Antidiabetic Medications & The Nursing Process Karen Ruffin RN, MSN Ed.
92
Antidiabetic Medications & The Nursing Process Karen Ruffin RN, MSN Ed.
-
Upload
shonda-henderson -
Category
Documents
-
view
220 -
download
0
Transcript of Antidiabetic Medications & The Nursing Process Karen Ruffin RN, MSN Ed.

Antidiabetic Medications
&The Nursing
Process
Karen Ruffin RN, MSN Ed.

IS THERE A DIFFERENCE AND
IF SO WHAT IS IT??
Is it Diabetes or is it Is it Diabetes or is it Hyperglycemia???????????????Hyperglycemia???????????????

What is ???????
HyperglycemiaHyperglycemia
InsulinInsulin
The primary source of energy for The primary source of energy for our bodiesour bodies

What is the difference between
Basel InsulinBasel Insulin
Prandial InsulinPrandial Insulin


Optimal Levels of Blood Sugars
Preprandial-110 mg/dlPreprandial-110 mg/dl
Postprandial-180 mg/dlPostprandial-180 mg/dl



What happens to our bodies when we are
hyperglycemic?

hypertensionVascular smoothmuscle cell growth
Release of chemokinesRelease of cytokinesExpression of cellular adhesion molecules
Hyper coagulationPlatelet ActivationDecreased Fibrinolysis

So what disease states are you at risk for???
MIMI DVTDVT PEPE StrokeStroke AAAAAA RetinopathyRetinopathy

What happens to our bodies when we are
hyperglycemic?
Increased Glucose Decreased Insulin

Increased Glucose Decreased Insulin

STUNS YOUR ???????? FOR 2WEEK
DID YOU KNOW ANY BLOOD DID YOU KNOW ANY BLOOD SUGAR >200 SUGAR >200

Criteria for Diagnosis of DM
DM Screening Symptoms of diabetes + casual plasma glucose level Symptoms of diabetes + casual plasma glucose level
less than or equal to 200 mg/dLless than or equal to 200 mg/dLOROR Fasting plasma glucose higher than or equal to Fasting plasma glucose higher than or equal to
126 mg/dL126 mg/dLOROR 2-hour postload glucose level higher than or equal to 2-hour postload glucose level higher than or equal to
200 mg/dL during an oral glucose tolerance test200 mg/dL during an oral glucose tolerance test Impaired glucose tolerance (IGT)Impaired glucose tolerance (IGT)
◦ FPG <110 mg/dL: normal fasting glucoseFPG <110 mg/dL: normal fasting glucose◦ FPG ≥110 mg/dL but <126 mg/dL: impaired fasting FPG ≥110 mg/dL but <126 mg/dL: impaired fasting
glucose (IFG)glucose (IFG)◦ FPG ≥126 mg/dL: provisional diagnosis of diabetes FPG ≥126 mg/dL: provisional diagnosis of diabetes
mellitusmellitus

What is a HbA1c?
It is a test that allows healthcare It is a test that allows healthcare providers to see how diabetics providers to see how diabetics have managed their blood glucose have managed their blood glucose level over the last 2-3 months….level over the last 2-3 months….
Why do you think this is Why do you think this is important????important????


At what blood glucose level do we At what blood glucose level do we start treating with sliding scale?start treating with sliding scale?
??????????????
So, what do you think So, what do you think we are doing to our we are doing to our
patients???patients???

What is the Difference??
Type 1 diabetesType 1 diabetes
Type 2 diabetesType 2 diabetes

Type 1 Diabetes
Lack of insulin production Lack of insulin production OROR
Production of defective insulinProduction of defective insulin
Affected patients need exogenous insulinAffected patients need exogenous insulin
ComplicationsComplications Diabetic ketoacidosis (DKA)Diabetic ketoacidosis (DKA) Hyperosmolar nonketotic syndromeHyperosmolar nonketotic syndrome
Oral antidiabetic drugs not effectiveOral antidiabetic drugs not effective

SymptomsSymptoms
PolyuriaPolyuria PolydipsiaPolydipsia PolyphagiaPolyphagia GlycosuriaGlycosuria Unexplained weight lossUnexplained weight loss FatigueFatigue HyperglycemiaHyperglycemia
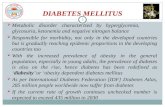
Diabetes Mellitus

Type 2 Diabetes
Most common typeMost common type
Caused by insulin deficiency and insulin Caused by insulin deficiency and insulin resistanceresistance
Many tissues are resistant to insulinMany tissues are resistant to insulin Reduced number insulin receptorsReduced number insulin receptors Insulin receptors less responsiveInsulin receptors less responsive These people respond to oral These people respond to oral
hypoglycemicshypoglycemics


Type 2 Diabetes
Several comorbid conditionsSeveral comorbid conditions• metabolic syndromemetabolic syndrome OR OR insulin-insulin-
resistance syndromeresistance syndrome OR OR syndrome Xsyndrome X
◦ ObesityObesity◦ Coronary artery diseaseCoronary artery disease◦ DyslipidemiaDyslipidemia◦ HypertensionHypertension◦ Microalbuminemia (protein in the urine)Microalbuminemia (protein in the urine)◦ Enhanced conditions for embolic events Enhanced conditions for embolic events
(blood clots)(blood clots)◦ Insulin ResistanceInsulin Resistance

Coronary Artery Disease

Treatment DIfferences Type 1Type 1
◦ Exogenous insulinExogenous insulin◦ Dietary controlDietary control
Type 2Type 2◦ Lifestyle changesLifestyle changes
Dietary controlDietary control Weight reductionWeight reduction ExerciseExercise
◦ May require oral hypoglycemic therapy or May require oral hypoglycemic therapy or exogenous insulinexogenous insulin
Insulin when oral hypoglycemic medications can Insulin when oral hypoglycemic medications can no longer provide glycemic controlno longer provide glycemic control

Gestational Diabetes
◦ Hyperglycemia that develops during pregnancyHyperglycemia that develops during pregnancy
◦ Insulin must be given to prevent birth defectsInsulin must be given to prevent birth defects
◦ 4% of all pregnancies4% of all pregnancies
◦ Must be reclassified if it persists 6 weeks post-Must be reclassified if it persists 6 weeks post-deliverydelivery
◦ Usually subsides after deliveryUsually subsides after delivery
◦ 30% of patients may develop Type 2 DM within 10 30% of patients may develop Type 2 DM within 10 to 15 yearsto 15 years

Major Long-Term Complications
of DM (Both Types)◦ Macrovascular (atherosclerotic Macrovascular (atherosclerotic
plaque)plaque) Coronary arteriesCoronary arteries Cerebral arteriesCerebral arteries Renal arteriesRenal arteries Peripheral vesselsPeripheral vessels
◦ Microvascular (capillary damage)Microvascular (capillary damage) RetinopathyRetinopathy NeuropathyNeuropathy NephropathyNephropathy

Complications Associated with Diabetes Mellitus
Cardiovascular disease, including Cardiovascular disease, including hypertensionhypertension
Peripheral vascular diseasePeripheral vascular disease Delayed healingDelayed healing
Visual defects, including blindnessVisual defects, including blindness Renal diseaseRenal disease InfectionInfection NeuropathiesNeuropathies ImpotenceImpotence

Oral Hypoglycemics
Sulfonylureas (oldest)Sulfonylureas (oldest)
MeglitinidesMeglitinides
BiguanideBiguanide
ThiazolidinedionesThiazolidinediones

Indications for Oral Hypoglycemics
They are used to lower blood They are used to lower blood sugar levels in patients that diet sugar levels in patients that diet and exercise have failed.and exercise have failed.
The patient must have some The patient must have some pancreatic function left.pancreatic function left.
They can be used as a They can be used as a monotherapy or in conjunction monotherapy or in conjunction with other oral hypoglycemics.with other oral hypoglycemics.

Contraindications
Know drug allergyKnow drug allergy Active hypoglycemiaActive hypoglycemia Usually not used during pregnancy Usually not used during pregnancy
subq insulin's are used then.subq insulin's are used then. Liver diseaseLiver disease Kidney diseaseKidney disease
Depending on the metabolic Depending on the metabolic pathways of the medicationpathways of the medication

Sulfonylureas
First generationFirst generation: :
chlorpropamide (Diabinese), chlorpropamide (Diabinese), tolazamide (Tolinase)tolazamide (Tolinase) tolbutamide (Orinase)tolbutamide (Orinase)
Second generationSecond generation: :
glimepiride (Amaryl) glimepiride (Amaryl) glipizide (Glucotrol)glipizide (Glucotrol) glyburide (DiaBeta, Micronase)glyburide (DiaBeta, Micronase)

Sulfonylureas Stimulate insulin secretiStimulate insulin secretion from the beta on from the beta
cells of the pancreas, thus increasing insulin cells of the pancreas, thus increasing insulin levelslevels
BetaBeta cell function must be present cell function must be present
Improve sensitivity to insulin in tissuesImprove sensitivity to insulin in tissues
Result: lower blood glucose levelsResult: lower blood glucose levels
First-generation drugs not used as frequently First-generation drugs not used as frequently nownow

Adverse Effects
SulfonylureasSulfonylureas
HypoglycemiaHypoglycemia hematologic effectshematologic effects nauseanausea epigastric fullnessepigastric fullness heartburnheartburn many othersmany others

Interactions SulfonylureasSulfonylureas
Hypoglycemic effect increases when taken with alcohol, Hypoglycemic effect increases when taken with alcohol, anabolic steroids, many other drugsanabolic steroids, many other drugs
Adrenergics (beta blockers) may mask many of the Adrenergics (beta blockers) may mask many of the symptoms of hypoglycemiasymptoms of hypoglycemia
Hyperglycemia: corticosteroids, phenothiazines, Hyperglycemia: corticosteroids, phenothiazines, diuretics, oral contraceptives, thyroid replacement diuretics, oral contraceptives, thyroid replacement hormones, phenytoin, diazoxide and lithium.hormones, phenytoin, diazoxide and lithium.
Allergic cross-sensitivity Allergic cross-sensitivity may occur with loop may occur with loop diuretics and diuretics and sulfonamide antibioticssulfonamide antibiotics
May May interact with alcohol/OTC medication interact with alcohol/OTC medication containing alcohol) - containing alcohol) - causing a disulfiram (Antabuse) -causing a disulfiram (Antabuse) -type reaction (facial flushing, pounding headache, feeling type reaction (facial flushing, pounding headache, feeling of breathlessness, and nausea) of breathlessness, and nausea)

Meglitinides
MeglitinidesMeglitinides repaglinide (Prandin)repaglinide (Prandin) nateglinide (Starlix)nateglinide (Starlix)
MeglitinidesMeglitinides Action similar to sulfonylureasAction similar to sulfonylureas Increase insulin secretion from the Increase insulin secretion from the
pancreaspancreas

Adverse Effects
MeglitinidesMeglitinides
HeadacheHeadache hypoglycemic effectshypoglycemic effects DizzinessDizziness weight gainweight gain joint painjoint pain upper respiratory infection or flu-like upper respiratory infection or flu-like
symptomssymptoms

Biguanides BiguanidesBiguanides
metformin (Glucophage) metformin (Glucophage)
BiguanidesBiguanides Decrease production of glucoseDecrease production of glucose
Increase uptake of glucose by tissuesIncrease uptake of glucose by tissues
Does not increase insulin secretion Does not increase insulin secretion from the pancreas (does not cause from the pancreas (does not cause hypoglycemia)hypoglycemia)

Adverse Effects MetforminMetformin
Primarily affects GI tract: Primarily affects GI tract: abdominal abdominal bloating, nausea, cramping, diarrhea, bloating, nausea, cramping, diarrhea, feeling of fullnessfeeling of fullness
May also cause metallic taste, reduced vitamin May also cause metallic taste, reduced vitamin BB1212 levels levels
Lactic acidosis is rare but lethal if it occursLactic acidosis is rare but lethal if it occurs
Does not cause hypoglycemiaDoes not cause hypoglycemia

Thiazolidinediones ThiazolidinedionesThiazolidinediones
pioglitazone (Actos),pioglitazone (Actos), rosiglitazone (Avandia)rosiglitazone (Avandia) Also known as “glitazones”Also known as “glitazones”
ThiazolidinedionesThiazolidinediones Decrease insulin resistance Decrease insulin resistance ““Insulin sensitizing drugs”Insulin sensitizing drugs” Increase glucose uptake and use in Increase glucose uptake and use in
skeletal muscleskeletal muscle Inhibit glucose and triglyceride production in Inhibit glucose and triglyceride production in
the liverthe liver

Adverse Effects
ThiazolidinedionesThiazolidinediones
Moderate weight gainModerate weight gain Edema Edema Mild anemia Mild anemia Hepatic toxicityHepatic toxicity—monitor liver —monitor liver
function testsfunction tests

Alpha-glucosidase Inhibitors
Alpha-glucosidase inhibitorsAlpha-glucosidase inhibitors acarbose (Precose)acarbose (Precose) miglitol (Glysetmiglitol (Glyset))
Alpha-glucosidase inhibitorsAlpha-glucosidase inhibitors Reversibly inhibit the enzyme alpha-Reversibly inhibit the enzyme alpha-
glucosidase in the glucosidase in the small intestinesmall intestine Result: Result: delayed absorption of glucosedelayed absorption of glucose Must be taken with meMust be taken with meals to prevent als to prevent
excessive postprandial blood glucose excessive postprandial blood glucose elevations (with the “first bite” of a meal)elevations (with the “first bite” of a meal)

Adverse Effects
α-glucosidase inhibitorsα-glucosidase inhibitors
FlatulenceFlatulence diarrheadiarrhea abdominal painabdominal pain
Do not cause hypoglycemia, Do not cause hypoglycemia, hyperinsulinemia, or weight gainhyperinsulinemia, or weight gain

Insulins Mechanism of ActionMechanism of Action SubstituteSubstitute for & for & same effects same effects as as endogenous insulinendogenous insulin
Restores the diabetic Restores the diabetic patient’s ability patient’s ability to: to: Metabolize carbohydrates, fats, and proteinsMetabolize carbohydrates, fats, and proteins Store glucose Store glucose in the liverin the liver Convert glycogen Convert glycogen to fat storesto fat stores
Some derived from porcine sourcesSome derived from porcine sources
Most now human-derivedMost now human-derived, using recombinant DNA , using recombinant DNA technologiestechnologies
Goal: tight glucose control Goal: tight glucose control
To To reduce the incidence of long-term complicationsreduce the incidence of long-term complications

Indications
To treat both types of diabetesTo treat both types of diabetes
Each patient requires careful Each patient requires careful customization of the dosing customization of the dosing regimen for optimal glycemic regimen for optimal glycemic controlcontrol

Contraindications
Anyone who is hypoglycemic?????Anyone who is hypoglycemic?????

Adverse Effects
Are all signs and symptoms of Are all signs and symptoms of hypoglycemia including shock and hypoglycemia including shock and death.death.

Human-Based Insulins
Rapid-ActingRapid-Acting Most rapid onset of actionMost rapid onset of action Shorter durationShorter duration
May be given SC or via continuous SC May be given SC or via continuous SC infusioninfusionpump (but not IV)pump (but not IV)
Insulin Onset (mins)
Peak (hrs) Duration (hrs)
aspart (Novolog) 2-33 1-3 3-5
lispro (Humalog) 2-33 30mins – 2.5 3-6.5
glulisine (Apidra) 2-33 30mins – 1.5 1.-25


Human-Based Insulins
Short-ActingShort-Acting regular insulin (regular insulin (Humulin R, Novolin R)Humulin R, Novolin R)
Onset 30 – 60 minutesOnset 30 – 60 minutes The only insulin product that can be The only insulin product that can be
given by IV bolus, IV infusion, or even IMgiven by IV bolus, IV infusion, or even IM
Insulin Onset (mins) Peak (hrs)
Duration (hrs)
Humulin R 30 mins to 4 hrs 2.5-5 5-10
Novolin R 30 2.5-5 8

Sliding-Scale Insulin Dosing
SC rapid or short-acting SC rapid or short-acting doses adjusted doses adjusted according to blood glucose test resultsaccording to blood glucose test results
Typically Typically used in hospitalized diabetic used in hospitalized diabetic patientspatients Or in Or in patients on TPN /patients on TPN / enteral enteral tube feedings tube feedings or or
receiving receiving steroidssteroids
Subcutaneous insulin is Subcutaneous insulin is ordered in an ordered in an amount that increases as the blood amount that increases as the blood glucose increasesglucose increases


Human-Based Insulins
Intermediate-ActingIntermediate-Acting isophane insulin suspension (isophane insulin suspension (also called NPH) also called NPH) (Humulin N, (Humulin N,
Novolin N)Novolin N)
isophane insulin suspension & insulin injectionisophane insulin suspension & insulin injection
(Humulin 50/50 , (Humulin 50/50 , Humulin 70/30, Novolin 70-30)Humulin 70/30, Novolin 70-30)
Lispro protamine suspension (Lispro protamine suspension (Humalog 75/25Humalog 75/25, Novolog Mix , Novolog Mix 70/30)70/30)
insulin zinc suspension (insulin zinc suspension (LenteLente, Novolin L), Novolin L)
CloudyCloudy appearance appearance Slower in onset and more prolonged duration than Slower in onset and more prolonged duration than
endogenous insulinendogenous insulin

Human-Based Insulins Intermediate-Acting
Insulin Onset (hrs)
Peak (hrs) Duration (hrs)
Isophane (NPH):
Humulin N 1-4 4-12 16-28
Novolin N 1-5 4-12 24
Isophane & Insulin:
Humulin 50/50 0.5 4-8 24
Humulin 70/30 0.5 4-12 24
Novolin70/30 0.5 2-12 24

Human-Based Insulins Intermediate-Acting
Insulin Onset (hrs)
Peak (hrs) Duration (hrs)
lispro protamine & lispro:
Humalog Mix 75/25 0.25-0.5 0.5-1.5 12-24
Novolog Mix 70/30 0.2-0.33 2.4 24
Insulin Zinc Suspension:
Lente Iletin II 1-1.5 8-12 24
Novolin L 1-4 7-15 20-28

Human-Based Insulins Combination Insulin ProductsCombination Insulin Products
NPH 70% and regular insulin 30% NPH 70% and regular insulin 30% (Humulin 70/30, (Humulin 70/30, Novolin 70/30)Novolin 70/30)
NPH 50% and regular insulin 50% NPH 50% and regular insulin 50% (Humulin 50/50)(Humulin 50/50)
insulin lispro protamine suspension 75% insulin lispro protamine suspension 75% and insulin lispro 25% (and insulin lispro 25% (Humalog Mix Humalog Mix 75/25)75/25)


Human-Based InsulinsLong-Acting
Insulin Onset Peak Duration
glargine (Lantus 1 No peak activity
24 (when administered at hs)
detemir (Levemir) 1 6-8 6-28



DM Monitoring – Daily AC & HS
Ante CibumAnte Cibum: before meals: before meals
HSHS: Hour of Sleep: prior to taking any HS snack: Hour of Sleep: prior to taking any HS snack
Rapid or short acting insulin used to cover any blood Rapid or short acting insulin used to cover any blood sugar (accucheck, chemstrip) sugar (accucheck, chemstrip) Dose by Dose by protocolprotocol (protocols are usually hospital- (protocols are usually hospital-
based)based)
for any result greater than 150mg/dL for any result greater than 150mg/dL Usually 1-2U for every 50mg/dL >150 with special Usually 1-2U for every 50mg/dL >150 with special
instructions to notify physician if >300 mg/dLinstructions to notify physician if >300 mg/dL

Injection Sites

Insulin PumpsExternal Internal

HypoglycemiaAdverse Effect of Insulin
EarlyEarly◦ Confusion, irritability, tremor, sweatingConfusion, irritability, tremor, sweating
LaterLater◦ Hypothermia, seizuresHypothermia, seizures◦ Coma and death will occur if not treatedComa and death will occur if not treated
Abnormally low blood glucose levelAbnormally low blood glucose level (<50 mg/dL(<50 mg/dL))
Mild cases Mild cases can be treated with diet—higher intake can be treated with diet—higher intake of protein and lower intake of carbs—to prevent a of protein and lower intake of carbs—to prevent a rebound postprandial hypoglycemiarebound postprandial hypoglycemia



Good way to remember!!!

State of hyperglycemia State of hyperglycemia with with ketosisketosis Usually results from infection, environment, or emotional Usually results from infection, environment, or emotional
stressorstressor As a result of Lack of Insulin, Breakdown:As a result of Lack of Insulin, Breakdown:
Fat – free fatty acids in liver – ketone bodies – Fat – free fatty acids in liver – ketone bodies – ketones in urineketones in urine
Protein – to form new glucose / increased BUNProtein – to form new glucose / increased BUN Glycogen to glucose (decrease use of glucose Glycogen to glucose (decrease use of glucose
because of decreased insulin)because of decreased insulin) Osmotic diuresisOsmotic diuresis Dehydration / Electrolyte ImbalanceDehydration / Electrolyte Imbalance Hyperosmolality HemoconcentrationHyperosmolality Hemoconcentration AcidosisAcidosis DeathDeath
Diabetic Ketoacidosis

Sudden onsetSudden onset Factors: infection, stressors, inadequate insulinFactors: infection, stressors, inadequate insulin Kussmaul respiration / fruity odor to breath, nausea, Kussmaul respiration / fruity odor to breath, nausea,
abdominal painabdominal pain Dehydration, electrolyte imbalance, polyuria, polydipsia, Dehydration, electrolyte imbalance, polyuria, polydipsia,
weight loss, dry skin, sunken eyes, soft eyeballs, lethargy, weight loss, dry skin, sunken eyes, soft eyeballs, lethargy, comacoma
Glucose >300 mg/dLGlucose >300 mg/dL pH <7.35 / Bicarbonate < 15 mEq/LpH <7.35 / Bicarbonate < 15 mEq/L
Na – low / K+ </> / Na – low / K+ </> / Cr >1.5 mg/dLCr >1.5 mg/dL Blood & Urine Ketones - PositiveBlood & Urine Ketones - Positive
Diabetic Ketoacidosis


State of hyperglycemia State of hyperglycemia without without ketosisketosis Little breakdown of fat (little or no ketone Little breakdown of fat (little or no ketone
bodies)bodies) Breakdown Breakdown
Glycogen– formation of new glucose – Glycogen– formation of new glucose – hyperglycemiahyperglycemia Very high levels of glucose >800mg dLVery high levels of glucose >800mg dL
Osmotic diuresis – extracellular dehydrationOsmotic diuresis – extracellular dehydration Renal insufficiency – hyperosmolality – Renal insufficiency – hyperosmolality –
intracellular dehydrationintracellular dehydration Hypokalemia – shock – tissue hypoxia - ComaHypokalemia – shock – tissue hypoxia - Coma
Hyperglycemic-hyperosmolar nonketotic syndrome (HHNS)

Gradual onsetGradual onset Factors: infection, other stressors, poor fluid intakeFactors: infection, other stressors, poor fluid intake Altered CNS function – neurologic symptomsAltered CNS function – neurologic symptoms Dehydration / electrolyte lossDehydration / electrolyte loss Glucose > 800 mg/dLGlucose > 800 mg/dL pH >7.4 / Bicarbonate >20 mEq/LpH >7.4 / Bicarbonate >20 mEq/L Na & K+ normal or lowNa & K+ normal or low Bun & Cr – elevatedBun & Cr – elevated Blood & Urine Ketones - negativeBlood & Urine Ketones - negative
Hyperglycemic-hyperosmolar nonketotic syndrome (HHNS)

TreatmentTreatment Rehydrate with NS (if severe) or ½ NSRehydrate with NS (if severe) or ½ NS
Use CVP or PCWP / UO / blood pressure monitoringUse CVP or PCWP / UO / blood pressure monitoring
IV insulin According to Sliding ScaleIV insulin According to Sliding Scale Never Reduce hyperglycemia by 10% /hrNever Reduce hyperglycemia by 10% /hr
Replace Potassium (will not be as severe as Replace Potassium (will not be as severe as DKA)DKA)
Hyperglycemic-hyperosmolar nonketotic syndrome (HHNS

Antidiabetic Drugs:Nursing Implications
Before giving any drugs that alter Before giving any drugs that alter glucose levels, obtain and glucose levels, obtain and document:document:
A thorough historyA thorough history Vital signsVital signs Blood glucose levelBlood glucose level, HbA1c level, HbA1c level Potential complications and drug Potential complications and drug
interactionsinteractions

Antidiabetic Drugs:Nursing Implications
Before giving any drugs that alter glucose levels:Before giving any drugs that alter glucose levels:
Assess the patient’s ability to consume foodAssess the patient’s ability to consume food
Assess blood glucose levelAssess blood glucose level
Assess for nausea or vomitingAssess for nausea or vomiting
Hypoglycemia may be a problem if antidiabetic drugs are Hypoglycemia may be a problem if antidiabetic drugs are given and the patient does not eatgiven and the patient does not eat
If a patient is NPO for a test or procedure, consult physician to If a patient is NPO for a test or procedure, consult physician to clarify orders for antidiabetic drug therapyclarify orders for antidiabetic drug therapy

Antidiabetic Drugs:Nursing Implications
Keep in mind that overall concerns for any Keep in mind that overall concerns for any diabetic patient increase when the patient:diabetic patient increase when the patient:
Is under stressIs under stress
Has an infectionHas an infection
Has an illness or traumaHas an illness or trauma
Is pregnant or lactatingIs pregnant or lactating

Antidiabetic Drugs:Patient Education
Thorough patient education is essential regarding:Thorough patient education is essential regarding:◦ Disease processDisease process◦ Other Risk Factors:Other Risk Factors:
SmokingSmoking HTNHTN CADCAD
◦ Self-Care:Self-Care: MedicationMedication Psychological adjustmentPsychological adjustment NutritionNutrition Activity and ExerciseActivity and Exercise Blood-glucose testingBlood-glucose testing Self-administration of insulin or oral drugsSelf-administration of insulin or oral drugs
◦ Potential complicationsPotential complications How to recognize and treat hypoglycemia and hyperglycemiaHow to recognize and treat hypoglycemia and hyperglycemia

FIGURE 36-3 Diabetes health care plan.
Mosby items and derived items © 2007, 2004 by Mosby, Inc., an affiliate of Elsevier Inc.

Nursing ImplicationsInsulin
When insulin is ordered, ensure:When insulin is ordered, ensure:◦ Correct routeCorrect route◦ Correct type of insulinCorrect type of insulin◦ Timing of the doseTiming of the dose◦ Correct dosageCorrect dosage
Insulin order and prepared dosages are Insulin order and prepared dosages are second-checked with another nursesecond-checked with another nurse◦ Check blood glucose level before giving insulinCheck blood glucose level before giving insulin◦ Roll vials between hands them to mix suspensions – no shaking!Roll vials between hands them to mix suspensions – no shaking!◦ Ensure correct storage of insulin vialsEnsure correct storage of insulin vials◦ ONLY insulin syringes, calibrated in units, to administer insulinONLY insulin syringes, calibrated in units, to administer insulin◦ Ensure correct timing of insulin dose with mealsEnsure correct timing of insulin dose with meals

Nursing ImplicationsInsulin
InsulinInsulin
When drawing up two types of insulin in one syringe:When drawing up two types of insulin in one syringe: Always Always withdraw the regular or rapid-acting insulin withdraw the regular or rapid-acting insulin
firstfirst
Provide Provide thorough patient education thorough patient education regarding regarding self-administration of insulin injections, including self-administration of insulin injections, including timing of doses, monitoring blood glucoses, and timing of doses, monitoring blood glucoses, and injection site rotationsinjection site rotations

Nursing Implications Oral Antidiabetic drugs
Always check blood glucose levels before givingAlways check blood glucose levels before giving
Usually given 30 minutes before mealsUsually given 30 minutes before meals Administer the medication at exact time – Administer the medication at exact time –
with meal or when food is in sight*with meal or when food is in sight*
AlphaAlpha-glucosidase inhibitors are given with the first -glucosidase inhibitors are given with the first bite of each main mealbite of each main meal
Metformin is taken with meals to reduce GI effectsMetformin is taken with meals to reduce GI effects

Nursing ImplicationsInsulin & hypoglycemic
medications Assess for signs of hypoglycemiaAssess for signs of hypoglycemia If hypoglycemia occurs:If hypoglycemia occurs:
Give glucagon orGive glucagon or Have the patient eat glucose tablets Have the patient eat glucose tablets
or gel, corn syrup, honey, fruit juice, or gel, corn syrup, honey, fruit juice, or nondiet soft drink oror nondiet soft drink or
Have the patient eat a small Have the patient eat a small snack such as crackers or half a snack such as crackers or half a sandwichsandwich
Monitor blood glucose levelsMonitor blood glucose levels


Nursing Implications Monitor for therapeutic responseMonitor for therapeutic response
Decrease in blood glucose levels to the Decrease in blood glucose levels to the level prescribed by physicianlevel prescribed by physician
Measure hemoglobin A1c to monitor long-Measure hemoglobin A1c to monitor long-term compliance to diet and drug therapyterm compliance to diet and drug therapy
Watch for hypoglycemia and hyperglycemiaWatch for hypoglycemia and hyperglycemia


Review
When administering insulin, the nurse When administering insulin, the nurse must keep in mind that the most must keep in mind that the most immediate and serious adverse effect of immediate and serious adverse effect of insulin therapy is which of the following?insulin therapy is which of the following? A: HyperglycemiaA: Hyperglycemia B: HypoglycemiaB: Hypoglycemia C: BradycardiaC: Bradycardia D: Orthostatic HypotensionD: Orthostatic Hypotension

Review
A dose of long acting insulin has been A dose of long acting insulin has been ordered for bedtime for a diabetic ordered for bedtime for a diabetic patient. The nurse expects to give which patient. The nurse expects to give which type of insulin?type of insulin? A: RegularA: Regular B: LenteB: Lente C: NPHC: NPH D: Glargine (Lantus)D: Glargine (Lantus)

Review
A Patient is to be placed on an insulin drip A Patient is to be placed on an insulin drip to control his high blood glucose levels. to control his high blood glucose levels. The nurse knows that which of the The nurse knows that which of the following is the only type of insulin that following is the only type of insulin that can be given IV?can be given IV? A: RegularA: Regular B: LenteB: Lente C: NPHC: NPH D: UltralenteD: Ultralente

Review
While monitoring a patient who is While monitoring a patient who is receiving insulin therapy, the nurse receiving insulin therapy, the nurse observes for signs of hypoglycemia, such observes for signs of hypoglycemia, such as which of the following?as which of the following? A: Decreased pulse and respiratory rate and A: Decreased pulse and respiratory rate and
flush skin.flush skin. B: Increased pulse rate and a fruity, acetone B: Increased pulse rate and a fruity, acetone
breath odor.breath odor. C: Weakness, sweating, and confusion.C: Weakness, sweating, and confusion. D: Increased urine output and edema.D: Increased urine output and edema.

Review
When giving oral acarbose When giving oral acarbose (Precose), the nurse should (Precose), the nurse should administer it at what time?administer it at what time? A: 15 minutes before mealA: 15 minutes before meal B: 30 minutes before mealB: 30 minutes before meal C: with the first bite of a mealC: with the first bite of a meal D: 1 hour after eatingD: 1 hour after eating

Review
A patient taking rosiglitazone (Avandia) A patient taking rosiglitazone (Avandia) tells the nurse, “There’s my insulin pill!” tells the nurse, “There’s my insulin pill!” The nurse describes the mechanism of The nurse describes the mechanism of action of Avandia by explaining that this action of Avandia by explaining that this drug is not insulin but it works by:drug is not insulin but it works by: A: Stimulating the beta cells of the pancreas A: Stimulating the beta cells of the pancreas
to produce insulin.to produce insulin. B: Decreasing insulin production.B: Decreasing insulin production. C: Inhibiting hepatic glucose production.C: Inhibiting hepatic glucose production. D: Decreasing intestinal absorption of glucose.D: Decreasing intestinal absorption of glucose.