ANTIDEPRESSANT˜MINING A˜Z ˚AMAZ˛ DESIGNING A …
98
ANTIDEPRESSANT-MINING A-Z (AMAZ) DESIGNING A WEB-BASED ALGORITHM AND VISUAL LANGUAGE FOR ANTIDEPRESSANT DRUG SELECTION TO EDUCATE PRIMARY CARE PRACTITIONERS By Amy Zhong A thesis submitted to Johns Hopkins University in conformity with the requirements for the degree of Master of Arts Baltimore, Maryland March, 2016 © 2016 Amy Zhong All Rights Reserved
Transcript of ANTIDEPRESSANT˜MINING A˜Z ˚AMAZ˛ DESIGNING A …

ANTIDEPRESSANT-MINING A-Z (AMAZ) DESIGNING A WEB-BASED ALGORITHM AND VISUAL
LANGUAGE FOR ANTIDEPRESSANT DRUG SELECTION TO EDUCATE PRIMARY CARE PRACTITIONERS
ByAmy Zhong
A thesis submitted to Johns Hopkins University in conformity with the requirements for the degree of Master of Arts
Baltimore, MarylandMarch, 2016
© 2016 Amy ZhongAll Rights Reserved

ii
ABSTR ACTDepression is a common mental disorder that affects approximately 14.8 million American
adults each year. In addition to being a debilitating condition, depression often occurs in tandem
with other medical conditions such as diabetes, heart disease, and cancer. While psychiatric
professionals are essential for the management of mental health, majority of patients seek care
from their primary care practitioners. This phenomenon is of great concern because diagnosis of
depression within primary care settings has only been accurate 25-50% of the time.
The antidepressant drug selection algorithm utilizes a unique formula to integrate patient and
family medical histories, patient symptoms, and patient preferences to make optimal treatment
selections. The development of a visual language explores the use of graphic elements to improve
understanding of major pharmacological mechanisms, knowledge essential to making rational
void in resources available to primary care practitioners, and improve management of mental
health within the primary care setting.
By Amy Zhong
Chairpersons of the Supervisory Committee
Adam I. Kaplin, M.D., Ph.D., �esis Preceptor
Assistant Professor, Departments of Psychiatry and Neurology
�e Johns Hopkins University School of Medicine
Kristen Rahn Hollinger, Ph.D., �esis Preceptor
Instructor, Departments of Psychiatry and Neurology
�e Johns Hopkins University School of Medicine
Jennifer E. Fairman, M.A., C.M.I., F.A.M.I., Departmental Advisor
Assistant Professor, Department of Art as Applied to Medicine
�e Johns Hopkins University School of Medicine

iii
ACKNOWLEDGEMENTSI would like to take this opportunity to express how eternally grateful I am to have been
invited into the Hopkins family two years ago. I am thankful for the aspiring guidance, invaluable
constructive criticism and unyielding support that many have shown me over the past few years,
all of whom helped bring this thesis into fruition.
To Drs. Adam I. Kaplin and Kristen Rahn Hollinger from the Departments of Psychiatry and
Neurology, I owe a deep sense of gratitude to both as my thesis preceptors, my guidance counselors
and my friends. It was truly an honor to have had the opportunity to work with you both this year.
To my faculty advisor, Jennifer E. Fairman, I would like to express a special appreciation for being
my rock. Her optimism and enthusiasm helped me stay focused and motivated through the research
and writing of this thesis. I would also like to extend my sincere thanks to the rest of the thesis
team: Mark Kandrysawtz and Josiah Heigel from Benjamin & Bond and Mike Wang.
A shout out to everyone who helped fund my thesis on Experiment.com (Jason Zhong,
Kevin G Chen, Joanne Yuan, Steven Chen, Denny Luan, Adam Kaplin, John Sandford, Andrew
Kim, Wendy Yuan, Calvin Chan, Minna Chan, Andrew W. Lee, David Dickerman, Ada Lin,
Tiffany Liang, Andrew Wu, Rachel Zhou, John Megahan, Weiling Chou, Chris Chen, Claire
Vergara, Peter Yeung, Tim Su, Christine Lin, Pamela Krikorian, Wendy Luo, Harry Zhang,
Joe Samson, Jeremy Reppy, Lindaanne Donohoe, Patrick Chen, Louise Giam, Andy Li, Ashley
Chung, Ashley Jiang, Jeff Lin, Ray Lian, Clarice Chan, Richard Chen, Carmen Loo, Michael
Kim, Robin Muccari, Joseph Lee, Jeff G, Xuesi Li, Jeff Day, Ian Suk, Wenjing Wu, Kimberly
Stemp, Justine Mirasol, Joshua Gabriel, George Dong, Victoria Tsay, Robert Paul Malchow,
Kate Ray, April Koh, Ashley Lau, Tom Liang, Cindy Wu, Douglas A. Mata, Eric Damon
Walters, and Adam Davies) and the individuals who helped endorse my project (Corinne
Sandone, Justine Mirasol, Lynn Ngai, Felicia Hardi, and Cheri Dijamco).
I want to acknowledge the faculty and staff in the Department of Art as Applied to Medicine
who were an invaluable support system: Corinne Sandone, Tim Phelps, David Rini, Gary Lees,
Juan Garcia, Lydia Gregg, Dacia Balch, Carol Pfeffer, and Ed Philips.
I would like to thank my second family in Chicago, whose words of encouragement remind me
every day that I am capable of accomplishing anything I put my mind to. Thank you John Sanford,
Pamela Krikorian, Robin Muccari, Lindaanne Donohue, and Phil Martin.

iv
ACKNOWLEDGEMENTSThank you to my class, the Class of 2016, the classes of 2015 and 2017, and our wonderful
alumni Hannah Ahn and James Abraham for the weekly goodies, midnight critiques, spontaneous
food adventures and overall good times.
I want to thank my godparents Xiaoyu Jing and Kevin Chen for always looking out for me
and ensuring that I didn’t starve.
I would like to thank my dog Jamie for her unconditional love and enforcement of potty breaks
and playtime, which helped maintain my sanity throughout this thesis.
To Calvin J. Chan, I am so grateful for his love and support, and extraordinary patience.
This thesis is dedicated to my amazing parents Holly Xiong and Pingyu Zhong for whom I owe
everything I am today. To my baby brother Arthur Zhong whose creativity and enthusiasm for the
arts inspires me to be more fearless. To my grandparents I want to thank for their experiences and
words of wisdom. I am so blessed to have such inspiringly hardworking people in my life. You have
and will always be my role models. I love you.

v
TABLE OF CONTENTS
Abstract iiChairpersons of the Supervisory Committee iiAcknowledgements iiiTable of Contents vIndex of Tables viiIndex of Figures vii
Introduction 1
Overview of Mental Healthcare 1Depression with a capital “D” 2Psychiatric Consultations 3Existing Algorithms for Antidepressant Drug Selection 4Visuals for Teaching Psychopharmacology 5Potential for a Smartphone Accessible Resource 5Project Objective 6Disclaimer 6
Materials & Methods 8
Development of Antidepressant Charts 8Development of Application Flowchart 11Development of Drug Selection Algorithm 13Development of Visual Language 19Development of Application 22
Results 23
Access to Assets resulting from this thesis 28
Discussion 29
Conclusion 31

vi
TABLE OF CONTENTS
Appendices 32
Appendix A: Antidepressant Charts 32Appendix B: Drug Selection Flowchart 42Appendix C: Drug Selection Questions 43Appendix D: Visual Language 48Appendix E: Web Application Wireframe & Design 50Appendix F: Test Scenarios & Results 54Appendix G: IRB Pre/Post Questionnaires 64
References 65
Vita 68

vii
INDEX OF TABLESTable 1 9Table 2 10Table 3 14Table 4 16Table 5 20Table 6 21
INDEX OF FIGURESFigure 1 12Figure 2 17Figure 3 17Figure 4 21Figure 5 22Figure 6 25Figure 7 26

1
INTRODUCTION
Overview of Mental Healthcare
Depression is a life debilitating mood disorder that affects approximately 14.8 million
American adults each year (ADAA 2014). In addition to being a chronic mental illness, studies
have shown that depression is also a frequent comorbidity of other conditions such as HIV/
AIDS, diabetes, multiple sclerosis, and cancer. Though depression is a treatable condition, it is
frequently underdiagnosed and undertreated, and the disease is responsible for a 5-fold increased
risk of mortality of comorbid medical conditions (ESC 2015). In 2010, antidepressants were the
second most commonly prescribed drug in the US (IMS Health 2011). Between 1988-1994 and
2005-2008 their use increased by 400% (Pratt, et al. 2011). Meanwhile, disturbing evidence
shows a steady increase in suicide rates since 2005 with the US suffering nearly 43,000 deaths
in 2014 (AFSP 2014). This phenomenon has launched awareness of the increasing involvement
of primary care practitioners (PCPs) in mental health – 80% of psychotropic drug prescriptions
were made by PCPs in 2013 (Barkil-Oteo 2013) – and the evaluation of their abilities to detect
depression and implement the necessary treatment.
symptoms not only include depressed mood and anhedonia (inability to experience pleasure),
but can range from insomnia and anorexia to decreased cognition and suicidal behavior. The
comorbid diagnoses. Though screening tools such PHQ-9 and PHQ-2 exist to detect characteristics
points in depression screening questionnaires are typically based off data collected from a variety
leaving room for a margin of error. The situation, as Dr. Ramin Mojtabai, Associate Professor
in the Department of Mental Health at the Johns Hopkins Bloomberg School of Public Health
describes, “Without enough time to really talk to patients about depression and with some patients
increasingly open to the idea of an antidepressant for mild conditions, the primary care setting can
be vulnerable to overprescribing” (Katz 2012).

2
Depression with a capital “D”
The ability to detect clinical depression manifests in the understanding of the condition.
What is depression? Everyone experiences sadness, but what makes a patient clinically depressed?
despondency, sleeplessness, irritability, [and] restlessness” (Kaplin 2014). In a lecture made by
Dr. Adam Kaplin, Assistant Professor in the Departments of Psychiatry and Neurology at the
It is an intermittent, universal experience in response to one’s environment, where the degree
is not merely severe sadness, but a syndrome. “Sadness is to major depression what cough is
to pneumonia. A cough can be an indicator of pneumonia, but not every cough is the result of
pneumonia” (Kaplin 2014).
The use of the word “depression” can be confusing. Not only is the term associated with the
general state of unhappiness, but clinically, multiple terms are used interchangeably to describe
the condition: major depressive disorder (MDD), major depression, depressive disorder, major
depressive disorder, clinical depression, and clinically depressed. All these terms fall under the
umbrella term of “mood disorder.”
When diagnosing depression, psychiatrists use the mnemonic “SIGEMCAPS.” If the patient
has experienced at least 5 of the 9 symptoms for at least 2 weeks, it is likely that the patient is
clinically depressed. Those symptoms are:
Sleep (lack of/excessive sleep)
Interest (loss of interest and pleasure)
Guilt (feeling worthless or guilty)
Energy (fatigue, loss of energy)
Mood (sadness)
Concentration (trouble concentrating or making decisions)
Appetite (increased/decreased appetite, correlates with weight)
Psychomotor Retardation (or agitation)
Suicidal Thoughts

3
Unlike stimulant drugs, antidepressants do not work unless a patient is suffering from a major
depressive disorder. If an individual is not responding to antidepressants, the medication will do
one of three things: (1) nothing, (2) cause side effects, or (3) make the patient worse. For instance,
an individual with bipolar disorder may experience irritability with an incorrectly prescribed drug.
For this reason, the most critical step in treating mood disorder is an accurate diagnosis.
Psychiatric Consultations
This 3-4 hours initial meeting is designed to collect the necessary background and symptom
information to make a diagnosis and provide any medication. Every psychiatrist approaches
consultations differently, but standard practice involves providing patients with a preregistration
packet consisting of forms for general information, medical history, family history and brief
self-report psychometric questionnaires. Before meeting with the patient, the psychiatrist will
to formulate the problem (conducting mental status, neurological and physical examinations as
necessary); (2) a private conversation with an individual of close relation, typically a spouse, to
gain a different perspective; and (3) a group discussion with both the patient and close relation
regarding the differential diagnosis and treatment options.
While the ability to make a diagnosis through discussion is a method similar to that of a medical
doctor, the nature of drug selection can often be an enigma. Prior to attending a consultation with
Dr. Kaplin, initial research on antidepressants proved helpful for understanding drug options, but
hours of seemingly unstructured discussion about a patient’s life later, Dr. Kaplin had eliminated
condition. As Dr. Kaplin itemized the choices of medication, describing how and why treatments
were selected (and occasionally mentioning those that were not), the inspiration for this thesis was
born. The mind is a complex network, but no matter how complicated it may be, the results of the
consult proved that there exists a formula for antidepressant drug treatment selection.

4
Existing Algorithms for Antidepressant Drug Selection
The prescription of antidepressant drugs is a dilemma due to perception of drugs being
of colleagues” (Zetin et al., 2006). For this reason, a proper understanding of how antidepressant
drugs work will allow for the ability to identify particular characteristics of antidepressant
medications that may make it a better choice for a patient.
In 2006, the authors of an article published in the Psychopharmacology Bulletin, titled “Rational
Antidepressant Selection,” discusses elements they found often understated. The article goes into
detail about the management of comorbidities and drug selection based on the co-effectiveness of
the drug to treat symptoms other than depression. Examples were provided describing situations
where certain antidepressants would be more effective than others. Though this information was
insightful and the tables informative, like other psychopharmacology textbooks, a 45-page paper is
not an effective resource in a busy clinical setting.
In 2008 the Texas Department of State Health Services produced “Major Depressive Disorder
Algorithms,” a procedural manual to facilitate clinical decision making in the management of
three conditions commonly encountered in the Texas public mental health system: schizophrenia,
bipolar I disorder, and major depressive disorder (Suehs et al., 2008). The treatment algorithms
provided sequential drug regimen options, driven by the evaluation of the patient’s response to
treatment. After assessment of the patient, “stage 1” treatment options included “SSRIs, BUP, SR/
XL, MRT, and SNRIs.” In translation, clinicians have a choice of 15 drugs for Stage 1: 7 SSRIs,
Bupropion - generic or brand, Mirtazapine, and 5 SNRIs. The next stage of action was determined
using results of the QIDS (Quick Inventory of Depressive Symptomatology), a test to assess the
severity of depressive symptoms. Though an evidence-based algorithm, this method not only fails
the same drug class until the medication charts listed in the Appendix.
In 2010, the National Health Service in England published prescribing guidelines for the
treatment of depression (Berkshire Healthcare 2010). Though the overall document covers
the necessary components for making a drug selection, the information was made available

5
via tables scattered throughout the packet. The information unfortunately did not translate
into the algorithm. While a helpful teaching aid, this packet is not useful for a fast-paced work
environment.
In 2015, the Eisenberg Center in Rockville, MD, developed a depression treatment decision
aid, called Depression Medication Choice (Kroenke 2015). This tool utilized decision aid
On average, 3-4 cards were used during a single clinical visit. This generated discussion about
educational resource, was designed primarily to improve patient experience, not teach primary
care physicians.
Visuals for Teaching Psychopharmacology
The availability of visuals for teaching drug side effects is currently limited to the textbook,
Stahl’s Essential Psychopharmacology. Nancy Muntner’s use of a circle with protruding polygonal
the same receptor required graphic elements to be placed in juxtaposition. Taken out of context, a
single drug’s diagrammatic representation could not be easily deciphered.
To communicate to a primary care audience, infographics also need to convey the relationship
to represent that relationship, the extensive variability in the use of color, shapes, and style grow
Potential for a Smartphone Accessible Resource
Originally marketed to executives on-the-go, the convenience of mobile-accessible services has
dramatically risen smartphone usage to approximately 84% of the US population in 2016 (Statista
2016). For those who cannot afford home broadband services, low income families have come to
rely on this platform for internet access. While the vast majority of smartphone owners use their

6
devices for texting and social media, 62% also use their mobile devices to access information about
health related conditions (Anderson 2015). We therefore chose to use a mobile-accessible platform
not only for its ability to disseminate information, but also for the ease of keeping up to date with
the evolution of psychopharmacology.
Project Objective
The objective of this thesis is to develop a decision support tool to educate and assist practitioners
with modest formal training in Psychiatry to make more informed decisions when prescribing
void, permitting easy and immediate access to clinically relevant information about antidepressant
patient the reasoning behind a diagnosis and drug treatment selection. We predict that improved
patient-practitioner communication will strengthen patient understanding and improve patient
compliance to antidepressant drug treatment, and, to a larger extent, improve management of
mental health within the primary care setting.
The web-based application is designed with a user-friendly interface to navigate a unique
algorithm constructed to take an evidence-based approach to drug selection. With education as
the primary intent for this creation, the application explores the use of a visual learning style to
The visual language is designed to communicate complex concepts, and bridge the gap between
mental health practitioners and PCPs. Not only will this channel of communication make side
Disclaimer
This resource does not yet cover depression in children or adolescents, postpartum depression,
or depression in patients with coexisting psychiatric disorders. The medications included in this
algorithm are FDA approved for depression and found to be clinically relevant to a practitioner
working in primary care. Psychotherapy, light therapy, and exercise were not considered in the
making of this application.

7
The drug selection tool is not intended to replace a practitioner’s clinical judgment, nor is it
and assist practitioners in decisions regarding mental healthcare. Primary care practitioners using
this resource are responsible for considering their patient’s unique condition to evaluate the
appropriateness of the algorithm’s results.

8
MATERIALS & METHODS
Development of Antidepressant Charts
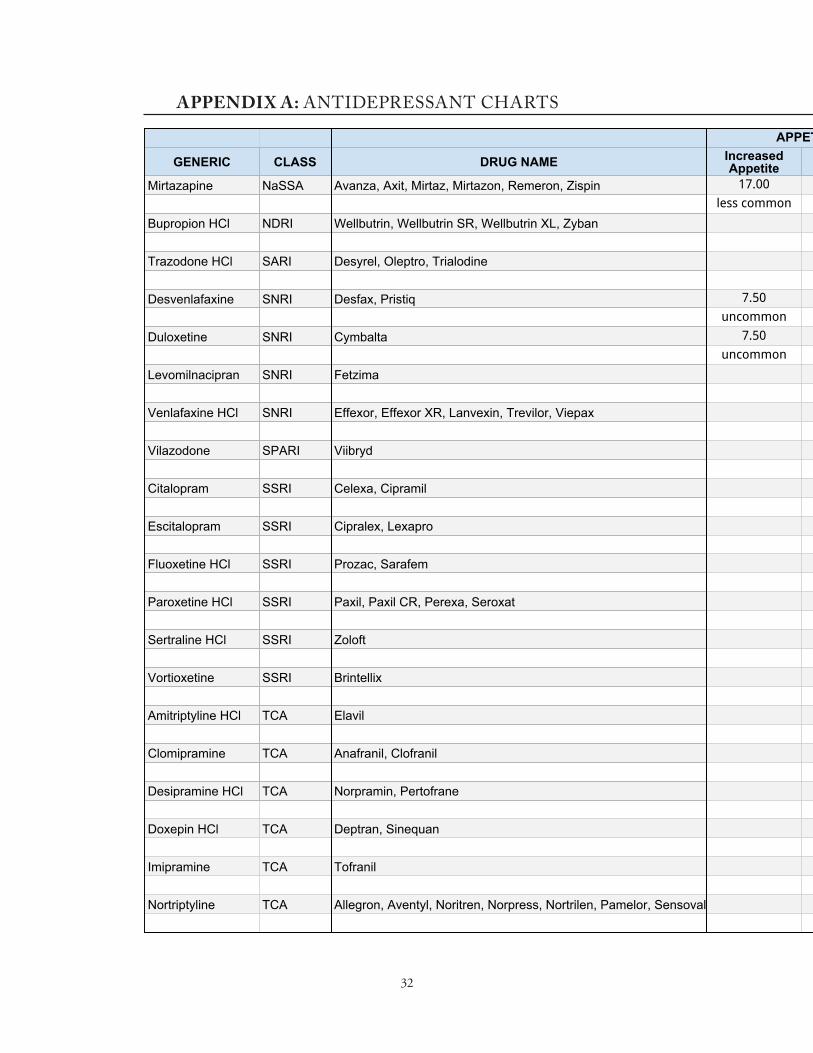
Initial research of antidepressant content was obtained by reading Stephen M. Stahl’s
Essential Psychopharmacology. A table was created created Microsoft Excel to organize facts
on 35 antidepressants. Data such as generic name, brand name, drug class, half life, side effect
availability of multiple drug databases, research papers and textbooks concerning the effects
of antidepressants. Ultimately, Medscape was chosen as the primary reference not only for
its reliability, but side effect frequency data, which was extracted from double-blind studies
published in The Physicians’ Desk Reference (PDR). The PDSP K1 Database supplied most
et al 2015) and Vortioxetine (Connolly, et al 2016) were found elsewhere.
efforts to simplify the antidepressant charts as much as possible were made by combining side
effects with similar implications. For example, drowsiness, sedation and hypnotic now fall under
the umbrella term of “somnolence.” Low energy, weakness and fatigue fall under “asthenia”
(Table 1). With the guidance of Dr. Kaplin, the list of antidepressants was also reduced to 20
to include only drugs most clinically relevant (Table 2). For instance, the class of monoamine
oxidase inhibitors (MAOIs) was removed due to dangerous drug interactions and serious dietary
restrictions, ultimately making MAOIs unfavorable among modern-day clinicians. Similarly, the
drawback of older tricyclic antidepressants (TCA) were removed due to their propensity to cause
serious side effects, many of which the mechanisms of action are not well understood.

9
Side Effect Category Umbrella Term Used Terms Listed on Medscape
Akathisia/Tremor Akathisia Agitation Akathisia Feeling Jittery Inner Restlessness Irritability Jittery Sensation Restlessness/AkathisiaAppetite Decreased Appetite Anorexia Decreased AppetiteBlood Pressure Orthostatic Hypotension Hypotension Orthostatic Hypotension VasodilationCognition Confusion Confusion Disorientation Lack of Concentration Decreased Concentration Disturbance in ThinkingEnergy Activating Activating Anxiety Nervousness Asthenia Asthenia Fatigue Low Energy WeaknessGastrointestinal Distress Dry Mouth Dry Mouth Xerostomia Nausea Nausea Nausea/VomitingHeart Rhythm Tachycardia Increased Heart Rate TachycardiaSensory Disturbances Blurred Vision Abnormal Vision Blurred Vision Vision Disturbances Dizziness Dizziness Lightheadedness Vertigo
Table . 1

10
Side Effect Category Umbrella Term Used Terms Listed on Medscape
Sexual Dysfunction Ejaculation Failure Ejaculation Disorder Delayed Ejaculation Decreased Libido Decreased Libido Libido Decrease Male Sexual DysfunctionSkin Edema of Lower Extremity Edema Swelling Peripheral Edema Sweating Diaphoresis Hyperhidrosis Increased Sweating SweatingSleep Disturbance Nightmares Abnormal Dreams Dream Disorder Somnolence Drowsiness Hypnotic Sedation
Original List Reason for Elimination
Isocarboxazid MAOIPhenelzine MAOISelegiline, transdermal MAOITranylcypromine MAOIMirtazapineBupropion Agomelatine foreign drug, not FDA approvedNefazodone sale of brand drug discontinued due to hepatotoxicity riskTrazodoneDesvenlafaxineDuloxetineMilnacipran FDA approved to treat Fibromyalgia, used off-label for DepressionLevomilnacipranVenlafaxine VilazodoneCitalopram
Table . 2

11
Development of Application Flowchart
Following the model of general psychiatric consultation practices, the major themes relevant
Illustrator CC to illustrate where these major decision points of the algorithm would appear in
the application (Figure 1). Considerations were made for the possibility of saving patient records
as reference for future medical follow-ups.
Original List Reason for Elimination
EscitalopramFluoxetineFluvoxamine FDA approved to treat OCD, used off-label for DepressionParoxetine Sertraline VortioxetineAmitriptyline Amoxapine old TCAClomipramine Desipramine Dothiepin foreign drug, not FDA approvedDoxepin ImipramineLofepramine foreign drug, not FDA approvedMaprotiline old TCANortriptylineProtriptyline old TCATianeptine foreign drug, not FDA approvedTrimipramine old TCA

12
Figure . 1 Flowchart identifying the major decision points in the algorithm.

13
Development of Drug Selection Algorithm
Algorithm 1.0
Patient Medical History
conditions, life circumstances (pediatric, pregnancy, breast feeding), and drug interactions.
Contraindications were obtained via Medscape’s interactions, warnings and pregnancy sections.
drug would be eliminated from further algorithm calculations for a pregnant patient. Similarly, if
Drug selection questions were developed to elicit drug elimination therefore only conditions,
circumstances and drugs marked “contraindicated” on Medscape were listed as possible answer
choices (Appendix B).
Patient Symptoms
employed to weigh drug options using a point system. Drugs begin with a value of zero. One
point per side effect deductions were made for drugs yielding side effects patients were already
experiencing. Drugs yielding side effects opposite that of patient symptoms would increase by
one point. If a drug had no effect on patient symptoms, no points were deducted or added.
For example, if a patient suffered from insomnia, a drug such as Mirtazapine (which
causes somnolence) would increase by one point. A drug such as Bupropion (which also causes
insomnia) would be deducted by one point. For a drug like Vortioxetine (which causes neither
insomnia nor somnolence) no points were deducted or added. Side effects such as blurred vision
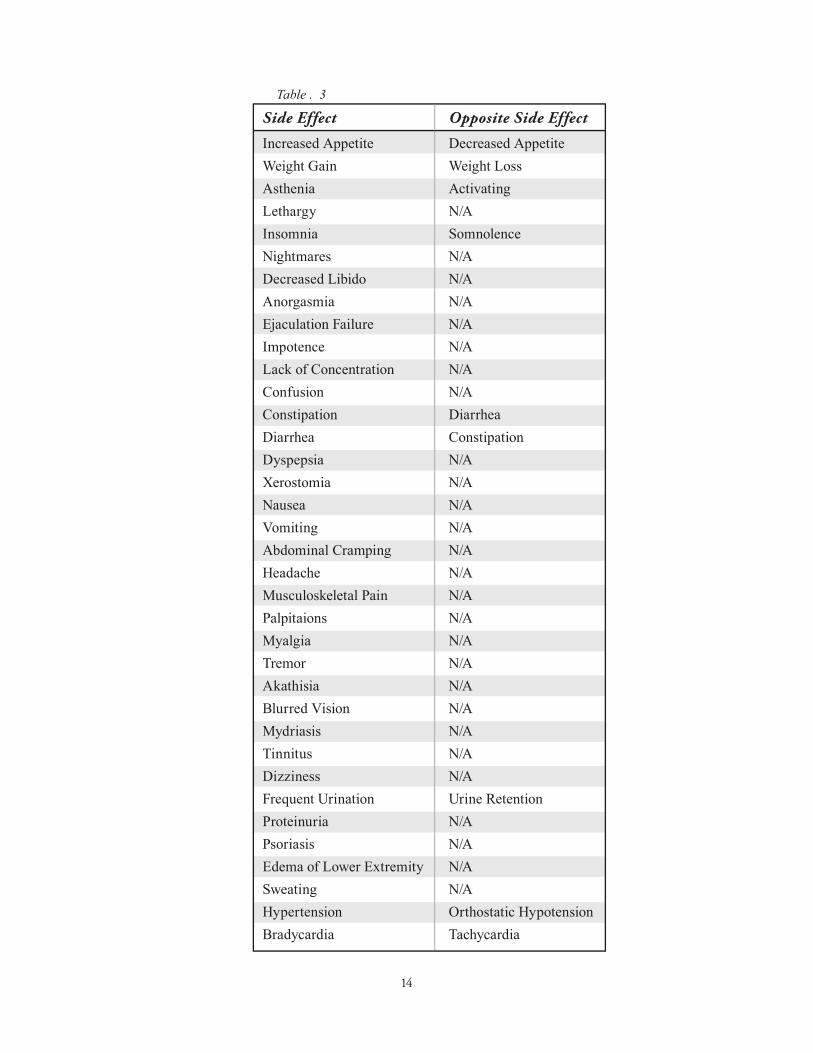
or vomiting, where there is no “opposite” side effect (Table 3), points can only be deducted.
14
Side Effect Opposite Side Effect
Increased Appetite Decreased AppetiteWeight Gain Weight LossAsthenia ActivatingLethargy N/AInsomnia SomnolenceNightmares N/ADecreased Libido N/AAnorgasmia N/AEjaculation Failure N/AImpotence N/ALack of Concentration N/AConfusion N/AConstipation DiarrheaDiarrhea ConstipationDyspepsia N/AXerostomia N/ANausea N/AVomiting N/AAbdominal Cramping N/AHeadache N/AMusculoskeletal Pain N/APalpitaions N/A Myalgia N/ATremor N/AAkathisia N/ABlurred Vision N/AMydriasis N/ATinnitus N/ADizziness N/AFrequent Urination Urine RetentionProteinuria N/APsoriasis N/AEdema of Lower Extremity N/ASweating N/AHypertension Orthostatic HypotensionBradycardia Tachycardia
Table . 3

15
Drug Weight Calculations
The number of added points (positive side effects) and deducted points (negative side effects)
from patient symptoms were used to arrange drugs into a list of ideal drug options, with the most
ideal drugs (higher drug weight) listed at the top.
Algorithm 2.0
Additional approaches to drug elimination and point adjustments were added to Algorithm 1.0.
General Information
Bupropion is the only drug FDA approved for smoking cessation. For patients indicated with
smoking cigarettes, one point was added for Bupropion. In addition, if an individual selected
“Yes” for regular alcohol use, the CAGE questionnaire was used to screen for alcoholism. If the
eliminated.
Patient Medical History
“The best predictor of future response is past response (Kaplin 2016).” If a patient had previously
taken an antidepressant, the drug will likely continue to yield successful or unsuccessful results.
Treatments yielding unsuccessful results in the past were eliminated from further drug selection.
Treatments yielding positive results were given one point.
Family Medical History
Patterns of heredity imply that having parents or family members with clinical depression
can increase the likelihood of an individual being diagnosed. Similar patterns have been observed
in patient response to antidepressant medication. If a blood relative had good results with an
antidepressant, the drug’s likelihood of working for the patient is high. In this algorithm, these
drugs received one point.

16
Patient Preferences
On Medscape, drug side effects are organized by frequency levels. Among a variety of drug
10% frequency, “less common” for side effects with 1-10% frequency, and “uncommon” for
side effects less than 1%. With the guidance of Dr. Kaplin, this scale was adjusted to emphasize side
as “common” and regarded with higher concern than that of 10%. Side effects only as low as 4%
frequency were recorded to accommodate for hypersensitive patients (Table 4). Using a scale
side effects unlisted.
dysfunction, gastrointestinal distress, and urinary function. Using the same scale (0-3), patient
preferences were ranked: 3 for high preference, 1 for little preference, and 0 for lack of preference.
These preferences were built into the algorithm by multiplying the patient preference by the drug
preferred by the patient, and a positive was used to denote drugs with side effects compatible to
those preferred by the patient. In the case of sexual dysfunction, patient preference denotes which
of the sexual side effects a patient would prefer if one was had (Appendix C). As each of the chief
Medscape Scale Algorithm Scale Frequency Side Effect Ranking
> 10% 31 - 45+% Common 3 1 - 10% 16 - 30% Less Common 2 < 1% 4 - 15% Uncommon 1 - < 4% unlisted 0
Table . 4

17
Example #1
A patient with insomnia expresses high preference for “increased sleep,” ranking it a 3.
Drug Option #1: Vortioxetine
Vortioxetine has no effect on sleep, therefore it’s side effect ranking is 0.
Patient Preference (3) x Side Effect Ranking (0) = 0
Drug Option #2: Mirtazapine
Mirtazapine has a 54% frequency of somnolence giving it a side effect ranking of +3.
Patient Preference (3) x Side Effect Ranking (+3) = +9
Drug Option #3: Bupropion
Bupropion has a 15.50% frequency of insomnia, therefore it’s side effect ranking is -2.
Patient Preference (3) x Side Effect Ranking (-2) = -6
Figure . 2 Sample patient preferences (sleep)
Figure . 3 Sample patient preferences

18
Example #2
Drug Option #2: Mirtazapine
Appetite: Patient Preference (2) x Side Effect Ranking (-2) = -4
Energy: Patient Preference (1) x Side Effect Ranking (-1) = 0
Sleep: Patient Preference (3) x Side Effect Ranking (+3) = +9
Sexual Dysfunction: Patient Preference (1) x Side Effect Ranking (0) = 0
Gastrointestinal Distress: Patient Preference (2) x Side Effect Ranking (+1) = +2
Urinary Function: Patient Preference (1) x Side Effect Ranking (0) = 0
Drug Score = (-4) + 0 +9 + 0 + 2 + 0 = 7
Patient Symptoms
Similar to algorithm 1.0, drugs will start with the arbitrary number of 0. Successful drugs
taken by family members with depression were given one point. Side effects that exacerbate
patient symptoms will deduct one point, s ide effects that alleviate patient symptoms will
gain one point, and side effects with no effect on existing symptoms will neither gain nor
lose points.
Drug Weight Calculations
The total number of deducted points (negative side effects) subtracted from the sum of the
added points (positive side effects, smoking cessation, and successful blood relative medications)
will generate a list of drugs from the most ideal drug selection to the least ideal drug selection.
Patient preferences is not integrated into any calculations.

19
Development of Visual Language
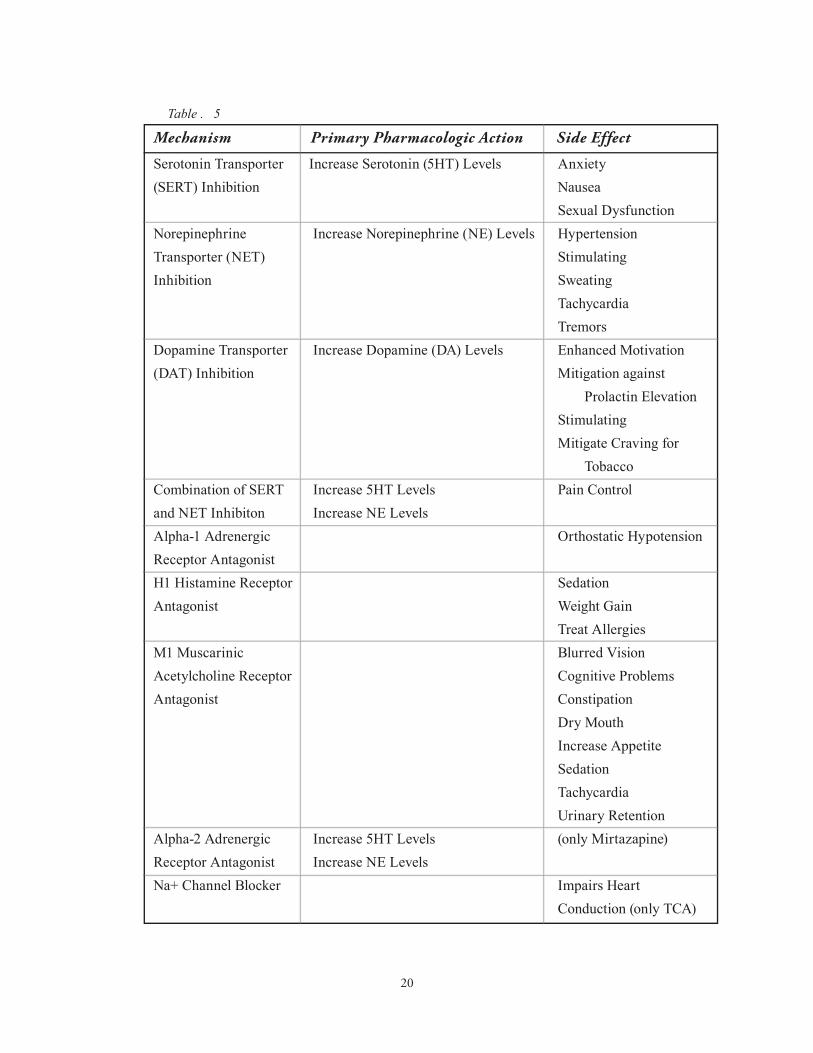
Side effects caused by antidepressant medication on key neurotransmitter systems were
Stahl’s Essential Psychopharmacology, the article “Interactions of
Antidepressants with Neurotransmitter Transporters and Receptors and their Clinical Relevance”
by Dr. Elliot Richelson (Richelson, 2003), and discussion with Dr. Kaplin (Table 5).
Side E�ect Icons
Icons were created using Adobe Illustrator CC. These icons correlate with the primary
pharmacologic action of the key mechanisms listed in Table 5. They do not encompass all
cataloged drug side effects in Appendix A, because many mechanisms are not yet well
understood. The objective in the creation of these graphic elements were to ensure easy
recognition and stylistic cohesiveness (Appendix D).
Receptor A�nity Levels
Ki
block 50% of human brain receptors. The lower the number, the higher the potency. To make this
relationship more intuitive, the inverse of each value was calculated.
This calculation was made with all receptors, with the exception of the H1 Histamine Receptor
Antagonist. Due to the extremely high potency levels of Mirtazapine and Doxepin for the
antihistamine receptor, normalizing H1
relevant antihistamine effects to be insubstantial. Therefore, H1
Amitriptyline’s H1
20
Mechanism Primary Pharmacologic Action Side Effect
Serotonin Transporter Increase Serotonin (5HT) Levels Anxiety(SERT) Inhibition Nausea Sexual DysfunctionNorepinephrine Increase Norepinephrine (NE) Levels HypertensionTransporter (NET) StimulatingInhibition Sweating Tachycardia TremorsDopamine Transporter Increase Dopamine (DA) Levels Enhanced Motivation(DAT) Inhibition Mitigation against Prolactin Elevation Stimulating Mitigate Craving for TobaccoCombination of SERT Increase 5HT Levels Pain Controland NET Inhibiton Increase NE LevelsAlpha-1 Adrenergic Orthostatic HypotensionReceptor AntagonistH1 Histamine Receptor SedationAntagonist Weight Gain Treat AllergiesM1 Muscarinic Blurred VisionAcetylcholine Receptor Cognitive ProblemsAntagonist Constipation Dry Mouth Increase Appetite Sedation Tachycardia Urinary RetentionAlpha-2 Adrenergic Increase 5HT Levels (only Mirtazapine)Receptor Antagonist Increase NE LevelsNa+ Channel Blocker Impairs Heart Conduction (only TCA)
Table . 5

21
adjustments were made by Dr. Kaplin to titrate certain values up and down to match what is
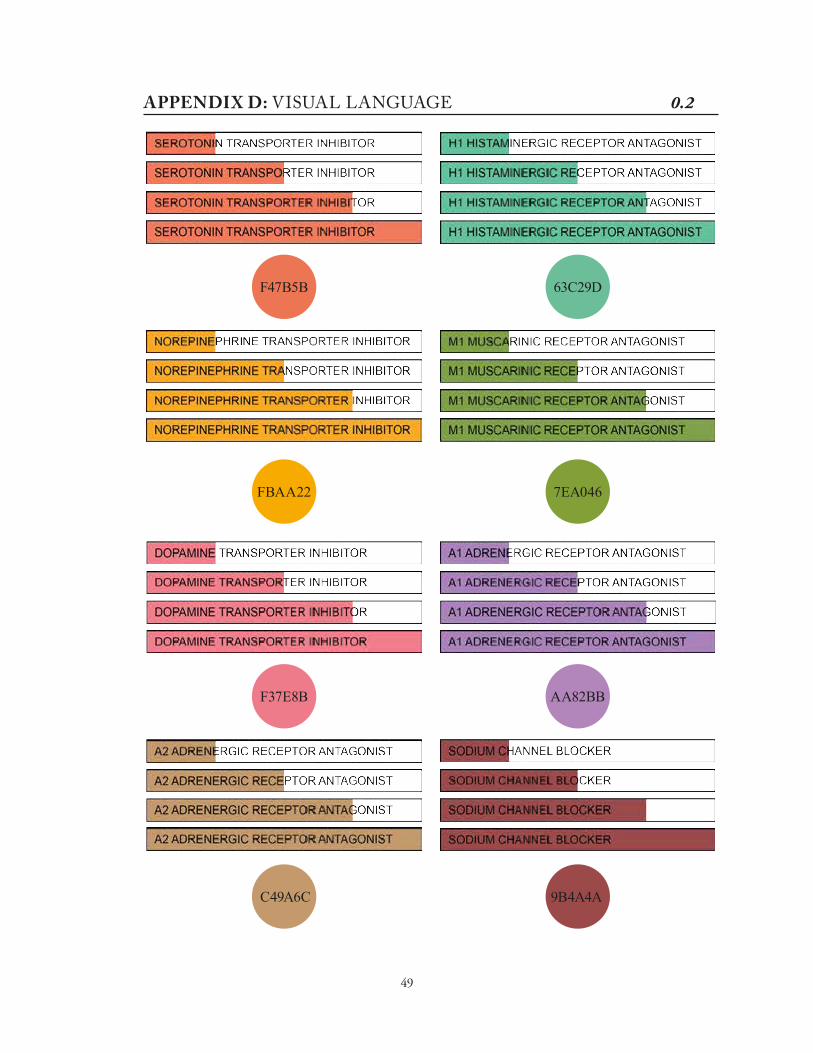
Visual Language
Each mechanism was assigned a color. Side effect logos were originally colorized with
their respective mechanisms. When considering layout design, the constant repetition of
graphic images if multiple mechanisms were to cause the same side effect, grew busy and hard
to comprehend. By allowing side effect logos to remain colorless, colored bars were used to
represent neurotransmitter inhibition potency levels that contribute to its respective side effect.
This not only reduced the amount of extraneous visuals, but enhanced readability (Figure 4).
Log Value Receptor Affinity Visual Scale
< 0 None 0 0 Little 1 1 Substantial 2 2 More Substantial 3 3 Maximum 4
Table . 6
Drug #1
1
1
1
1
2
2
33
2
Drug #1
1 11 1
Figure . 4 Side effect logo remains colorless to reduce extraneous visuals.

22
Development of Application
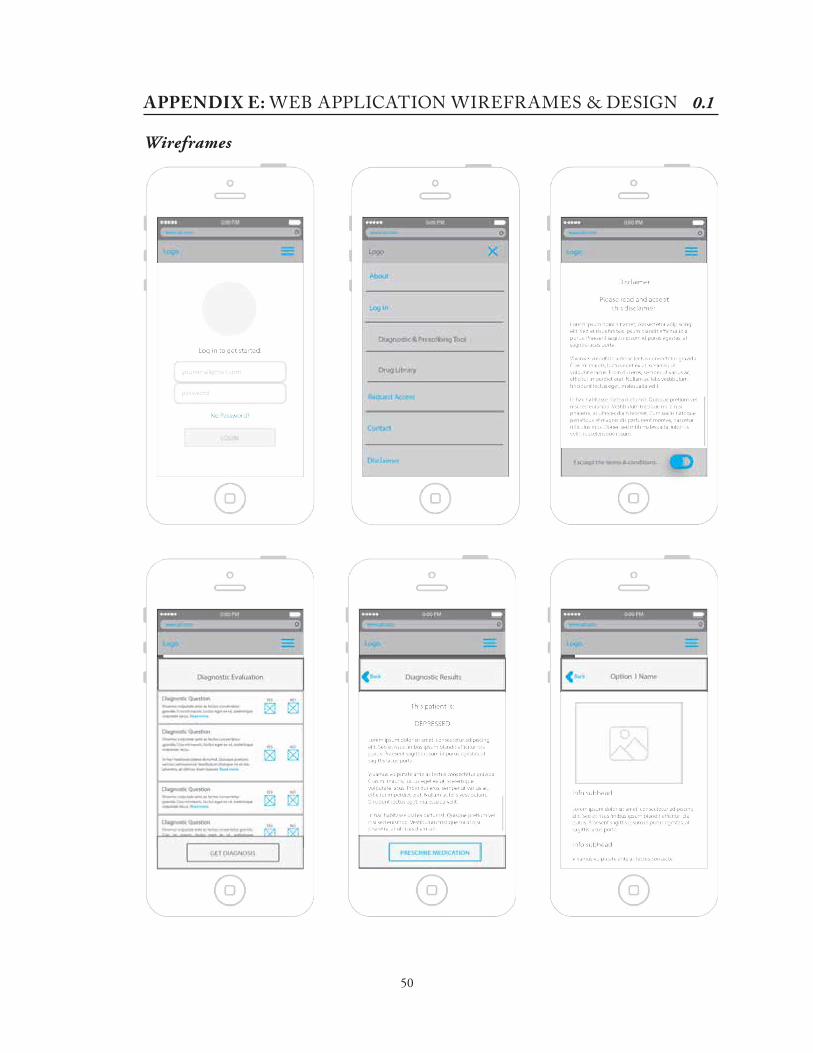
The mobile web application was designed to provide a sequential navigation structure that guides
the user through an abridged consultation to identify a list of ideal drug selections. Wireframes were
drafted by Benjamin & Bond (B&B) based on initial discussion of mobile web application goals and
objectives. Using the wireframes as a foundation, preliminary application designs were produced
using Adobe Illustrator CC (Appendix E). With the guidance of B&B, color palette and design
adjustments were made to create a more inviting platform. Wording of drug selection questions were
Example Question: Does the patient express concerns regarding sexual dysfunction? Y/N
If Yes, what side effects is the patient expressing concerns about? (Multiple Selection)
• Decreased Libido
• Inability to Achieve Orgasm
• Failure to Ejaculate
• Trouble Getting an Erection
Adjusted Question: Does the patient express concerns regarding sexual dysfunction?
(Multiple Selection)
• No Sexual Dysfunction Concerns
• Decreased Libido
• Inability to Achieve Orgasm
• Failure to Ejaculate
• Trouble Getting an Erection
option 1
option 2
option 3
option 4
Y N
none
option 1
option 2
option 3
option 4
Figure .

23
RESULTSA prototype was delivered and assessed on March 16, 2016 (Appendix E).
Menu
Designed for mobile use, the menu of this web-based application was designated using a
three-line menu icon. Menu options include About, Login, Drug Selection Tool, Drug Library,
Request Access, Contact, and Logout. Upon each use of the drug selection algorithm, agreement
to the terms of the disclaimer was required before proceeding to the diagnostic evaluation. This
for a mental healthcare practitioner.
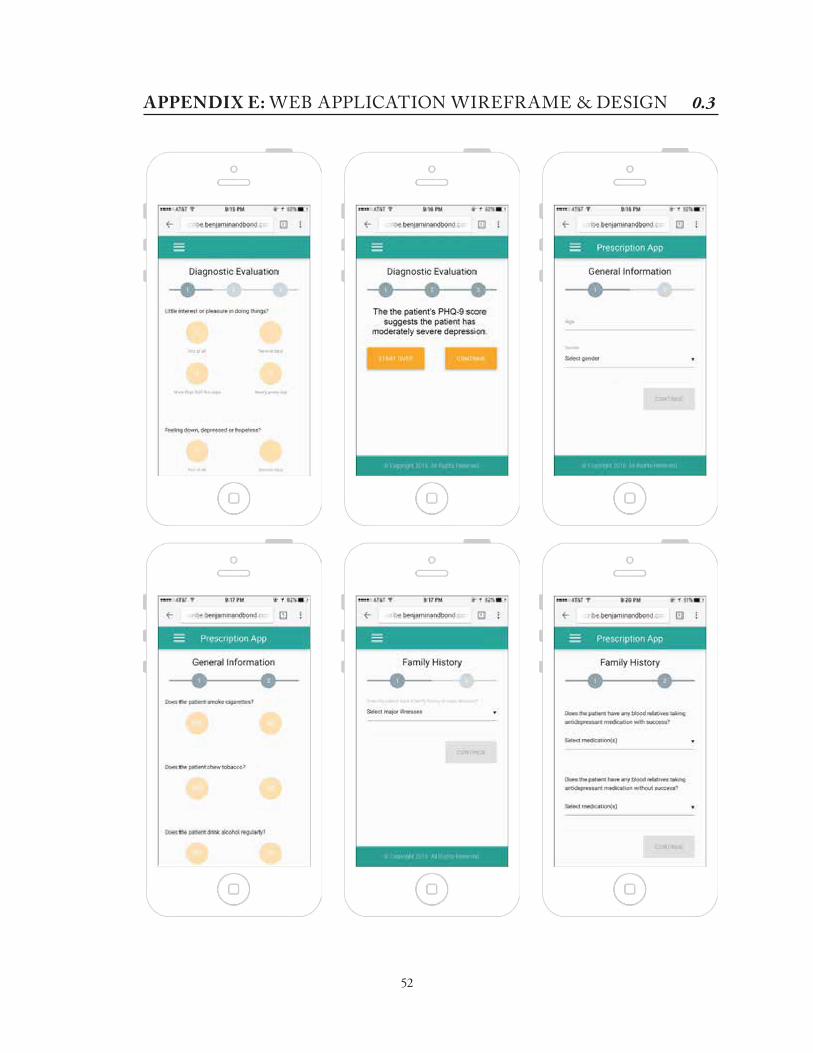
Diagnostic Evaluation
The mobile web application has a diagnostic evaluation function to screen for depression
before proceeding to the drug selection questions. Patient Health Questionnaire (PHQ) 2 was
used to assess whether patient symptoms warranted a diagnosis of major depression. Patients
who screened positive (>2) continued to PHQ-9 for further evaluation. PHQ-2 and PHQ-9 (a
total of 9 questions) are standardized assessment tools, but there remains a margin for error. For
this reason, the ability to override the results of the evaluation and proceed to the drug selection
algorithm were enabled.
Drug Selection Algorithm
A 35-year old male is diagnosed with clinical depression. He smokes cigarettes regularly,
does not drink alcohol, and has an aunt who was also diagnosed with major depression. The aunt
had been on two different antidepressants, Paroxetine (without success) and Bupropion (with
success). This man is quite healthy. He has no allergies, no preexisting conditions, no plans
to undergo surgery in the next 1-2 months, and has been on one antidepressant, Desvenlafaxine
(without success). When asked about symtpoms, the man says his appetite has increased and that
concentrate on work and says that he has a constant urg to urinate, but very little comes out.

24
drug options and generates a list (Figure 6). The representation of algorithm calculations is
values correlate with positive and negative symptoms, green and red respectively. The M value are
extra points given to medications for successful patient or blood relative use, and smoking cessation
(which only applies to Bupropion). W is the weighted number calculated by the subtraction of the
red S value by the sum of the green S and M values. Calculation details can be found on Appendix
A. The drug score value (DS) indicates level of adherence of each drug to the patient’s preferences.
The drug selection algorithm has four sets of questions: General Information, Family Medical
History, Patient Medical History and Patient Symptoms. Bupropion ranked highest in the list of
drug options due to the following calculations.
General Information (M value)
The patient smoked cigarettes so the M value increased by 1.
Family Medical History (M value)
The patient’s blood relative had success with Bupropion so the M value increased by 1.
Patient Medical History (M value)
There were no details entered in this section that contributed the points accumulated.
Patient Symptoms (S values)
The patient mentioned increased appetite, increased weight and somnolence. Bupropion
causes decreased appetite (+1), decreased weight (+1) as well as increased weight (-1),
and insomnia (+1). All (+1) points were indicated in the green S value, and all (-1) points
were indicated in the red S value.
Drug Weight Value (W value)
W = 1 + 1 + 1 + 1 – 1 + 1 = 4

25
Visual Language
From the generated list of drug options, medication details can be obtained by clicking
directly from the drug selection list or under the “Drug Library” option in the main menu. Drug
side effect icons are chosen to represent the drug in the generated drug option list.
Figure .

26
contributes to. If the user selected the “sedation” side effect icon, the page will scroll down to where
The visual language not only allows the user to identify which mechanisms are involved, but
also how potent. This information is advantageous when considering antidepressants to avoid
possible overdose. For example, if a patient is already taking a drug that increases serotonin levels,
antidepressants with high 5HT transporter inhibition should be avoided. In addition, the presence of
more than one mechanism per side effect indicates an increased severity of that side effect.
Figure . medication details based on side effect icon (Right)

27
Algorithm Results
Using a series of practice-based scenarios provided by Dr. Kaplin (Appendix F), the
algorithm has consistently ranked majority of the ideal drug selections at the top and less ideal
drug selections at the bottom. The patient preferences proved helpful in further differentiating
between drugs with the same weight value, but condition of information quality needs further
investigation.
Several drawbacks with this version of the algorithm include the elimination of
antidepressant medication options based on drug-drug interactions. Drug contraindications range
from chemotherapy to antihistamines so an elimination of an ideal drug choice will be made
over the use of an antihistamine. Using drug side effect frequencies to weigh patient symptom
calculations may yield more promising results.

28
the author at [email protected]. The author may also be reached through the Department of
Art as Applied to Medicine via the website www.medicalart.johnshopkins.edu.

29
DISCUSSION
void in resources available to primary care practitioners managing mental health. An application
prototype was successfully developed, establishing the infrastructure for a novel evidence-based
antidepressant prescribing algorithm with patient preference capabilities. Graphic elements
designed introduced a unique approach to communicating the effect of antidepressant drugs on
circuits and make rational antidepressant drug selections.
Further Development
Research during the production of the algorithm proved there are many aspects of drug
target PCP audience, expanding the algorithm would not only yield more precise drug selections,
but allow the algorithm to encompass a broader range of conditions. A sample list for further
development include:
• Inclusion of all antidepressants (especially those used off-label)
• Considerations for pediatric and geriatric depression
• Drug dosage and augmentation abilities
• Incorporation of drug cost and availability into patient preferences
• Consideration for other psychiatric comorbidities
• Ability to consider the co-effectiveness of antidepressants to
treat other symptoms and conditions besides depression
• Include more mechanisms, such as serotonin modulator and stimulators (SMS)

30
IRB Approved Study
To evaluate the effectiveness of the visual language an IRB approved study would need
to be conducted. The application’s ease of use as well as algorithm accuracy and helpfulness
would also be assessed. Feedback would provide necessary insight into how to teach PCPs about
psychopharmacology and whether a web-based algorithm would improve management of mental
health within primary care.
Integration into Johns Hopkins Point of Care Information Technology
The Johns Hopkins POC-IT Center is a web, mobile and print accessible collection of
evidence-based clinical decision guides developed for healthcare professionals. Integration of the
antidepressant drug selection algorithm would bring a unique interactive module to POC-IT, as
well as disseminate the contents of this resource to existing POC-IT users.

31
CONCLUSIONThe key to treating depression is to implement the proper management of mental health
into primary care. In 2003, Dr. Stephen Bartels, Associate Professor of psychiatry at Dartmouth
Medical School, said at least one-third of older adults in primary care presented with depression
or other mental illnesses (Rosack 2003). While depression is only accurately diagnosed 25-50%
of the time in primary care settings, physicians who do recognize depressive symptoms choose
not to enforce depression management (Gallo et al. 2015). On account of the multiple conditions
presented by older adult patients, treatment of depression often becomes secondary to the
management of “organic” diseases (Gallo et al. 2015). Studies have shown that the implementation
of a depression management program actually helps mitigate the combined effects of depression
and multimorbidities.
In creating this web-based application, we hope to have a number of effects on the treatment
of MDD by PCPs, which will be further tested and validated in future studies. Outcomes include
but are not limited to the following:
• PCPs will make more optimal treatment selections. They will be able to avoid subtle, but
important suboptimal or even dangerous treatments through the utilization of the drug
selection algorithm.
• The integration of patient preferences on the evidence-based selection of antidepressant
medication will result in treatment that patients will more likely tolerate and adhere to.
•
increased diagnosis and successful outcomes for patients with MDD.
32
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Side Effects 0.1

33
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Side Effects 0.2

34
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Side Effects 0.3

35
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Side Effects 0.4

36
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Side Effects 0.5

37
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Contraindications 0.1

38
APPENDIX A: ANTIDEPRESSANT CHARTS

Drug Contraindications 0.2
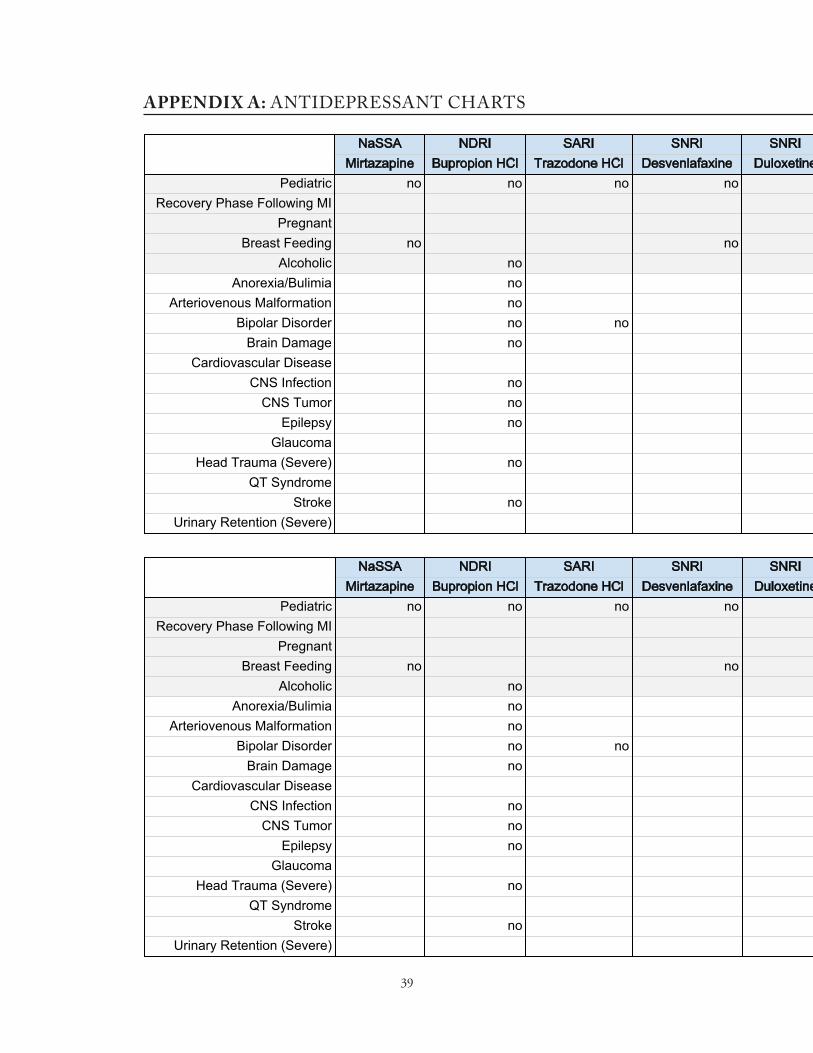
39
APPENDIX A: ANTIDEPRESSANT CHARTS

Ideal Patient

40
APPENDIX A: ANTIDEPRESSANT CHARTS

Receptor Affinities 0.1

41
APPENDIX A: ANTIDEPRESSANT CHARTS

Receptor Affinities 0.2

42
APPENDIX B: DRUG SELECTION FLOWCHARTAPPENDIX B: DRUG SELECTION FLOWCHART

43
APPENDIX C: DRUG SELECTION QUESTIONS 0.1
PHQ-2
Over the past 2 weeks, how often have you been bothered by any of the following problems?
1. Little interest or pleasure in doing things
2. Feeling down, depressed or hopeless
Scores < 3: �e patient has screened negative for someone who should be evaluated further for
depression.
Scores ≥ 3: �e patient has screened positive for someone who should be evaluated further for
depression.

44
APPENDIX C: DRUG SELECTION QUESTIONS 0.2
PHQ-9
Over the past 2 weeks, how often have you been bothered by any of the following problems?
3. Trouble falling or staying asleep, or sleeping too much
4. Feeling tired or having little energy
5. Poor appetite or overeating
6. Feeling bad about yourself-or that you are a failure or have let yourself or your family down
7. Trouble concentrating on things, such as reading the newspaper or watching television
8. Moving or speaking so slowly that other people could have noticed. Or the opposite
9. Thoughts that you would be better off dead, or of hurting yourself in some way.
Scores ≤ 4: �e patient’s PHQ-9 score suggests the patient has minimal depression.
Scores 5 - 9: �e patient’s PHQ-9 score suggests the patient has mild depression.
Scores 10 - 14: �e patient’s PHQ-9 score suggests the patient has moderate depression.
Scores 15 - 19: �e patient’s PHQ-9 score suggests the patient has moderately severe depression.
Scores 20 - 27: �e patient’s PHQ-9 score suggests the patient has severe depression.

45
APPENDIX C: DRUG SELECTION QUESTIONS
General Information Questions
1. Age ____
2. Gender (Male, Female, Transgender)
3. If Female or Transgender and age 30+, is the patient in perimenopause? Y/N If No, ask following (yes or no) questions: a. Is the patient pregnant? b. Does the patient have plans to get pregnant in the next 6-12 months?
c. Is the patient currently breastfeeding? 3. Does the patient smoke cigarettes? Y/N 4. Does the patient drink alcohol regularly? Y/N
If Yes, ask following (yes or no) questions: a. Has the patient ever felt he/she needed to cut down on his/her drinking? b. Have people annoyed the patient by criticizing his/her drinking? c. Has the patient ever felt guilty about drinking? d. Has the patient ever felt he/she needed a drink �rst thing in the morning (eye-opener) to steady his/her nerves or to get rid of a hangover?
Family Medical History Questions
1. Does the patient have a family history of major illnesses? (Multiple Selection)• No major illness(es)• Alcoholism• Bipolar Disorder• Drug Abuse
• History of Suicides (or Suicide Attempts)• Major Depression• Neurologic• Schizophrenia
(if yes to either, make pregnancy elimination)
(if yes to either, make breastfeeding elimination)
(if yes to either, +1 to Bupropion)
(if 2 or more yes’s, make alcohol elimination)
(pediatric < 18, geriatric > 65)

3. Does the patient have blood relatives with negative experiences with any antidepressant medications? (Multiple Selection)
• No antidepressant(s)• Amitriptyline HCl• Bupropion HCl• Citalopram• Clomipramine• Desipramine HCl• Desvenlafaxine• Doxepin HCl• Duloxetine• Escitalopram• Fluoxetine HCl
• Imipramine• Levomilnacipran• Mirtazapine• Nortriptyline• Paroxetine HCl• Sertraline HCl• Trazodone HCl• Venlafaxine HCl• Vilazodone • Vortioxetine
2. Does the patient have blood relatives with positive experiences with any antidepressant medications? (Multiple Selection)
• No antidepressant(s)• Amitriptyline HCl• Bupropion HCl• Citalopram• Clomipramine• Desipramine HCl• Desvenlafaxine• Doxepin HCl• Duloxetine• Escitalopram• Fluoxetine HCl
• Imipramine• Levomilnacipran• Mirtazapine• Nortriptyline• Paroxetine HCl• Sertraline HCl• Trazodone HCl• Venlafaxine HCl• Vilazodone• Vortioxetine
Patient Medical History Questions
1. Has the patient su�ered a heart attack in the past 10 weeks? Y/N
2. Does the patient plan to undergo surgery in the near future (e.g. 1-2 months)? Y/N
0.3
(+1 for selected drug/s)
(if yes, eliminate drugs contraindicated for recovery phase following MI)

46
5. Has the patient taken any antidepressants with success?• No antidepressant(s)• Amitriptyline HCl• Bupropion HCl• Citalopram• Clomipramine• Desipramine HCl• Desvenlafaxine• Doxepin HCl• Duloxetine• Escitalopram• Fluoxetine HCl
• Imipramine• Levomilnacipran• Mirtazapine• Nortriptyline• Paroxetine HCl• Sertraline HCl• Trazodone HCl• Venlafaxine HCl• Vilazodone• Vortioxetine
3. Does the patient have any preexisting condition(s)? • No preexisting condition(s)• Anorexia/Bulimia• Arteriovenous Malformation• Bipolar Disorder• Brain Damage• Cardiovascular Disease• Chronic Pain Syndrome • CNS Infection
4. Is the patient currently taking any medication or receiving any of the following treatment? • No medication(s)/treatment(s)• Artemether/Lumefantrine• Astemizole• Cisapride• Disopyramide• Disul�ram• Dronedarone• Eliglustat• Flibanserin• Ibutilide• Indapamide• Linezolid• Lumefantrine
• Pentamidine• Pimozide• Procainamide• Procarbazine• Quinidine• Rasagiline• Saquinavir• Selegiline• Sotalol• Terfernadine• �ioridazine
• CNS Tumor• Epilepsy• Glaucoma• Head Trauma (Severe)• QT Syndrome• Stroke • Urinary Retention (Severe)
APPENDIX C: DRUG SELECTION QUESTIONS
(eliminate contraindicated)
(eliminate contraindicated)
(+1 for selected drug/s)

• Imipramine• Levomilnacipran• Mirtazapine• Nortriptyline• Paroxetine HCl• Sertraline HCl• Trazodone HCl• Venlafaxine HCl• Vilazodone• Vortioxetine
5. Has the patient taken any antidepressants without success?• No antidepressant(s)• Amitriptyline HCl• Bupropion HCl• Citalopram• Clomipramine• Desipramine HCl• Desvenlafaxine• Doxepin HCl• Duloxetine• Escitalopram• Fluoxetine HCl
0.4
Patient Symptom Questions
1. APPETITE: Has the patient’s appetite changed drastically? • No appetite change(s)• Decreased Appetite• Increased Appetite
(eliminate selected drug/s)

47
2. WEIGHT: Has the patient lost or gained an unhealthy degree of weight?• No weight change(s)• Decreased Weight • Increased Weight Loss
3. ENERGY/MOOD: Does the patient feel a change in energy or mood? • No energy/mood change(s)• Activating• Asthenia• Lethargy
4. SLEEP: Does the patient have issues regarding sleep (too much or too little)? • No sleep issue(s)• Insomnia• Nightmares• Somnolence
5. SEXUAL DYSFUNCTION: Does the patient express concerns regarding sexual dysfunction? • No sexual dysfunction issue(s)• Anorgasmia• Decreased Libido• Ejaculation Failure• Impotence
6. COGNITION: Does the patient have trouble with confusion or concentration? • No cognition issue(s)• Confusion• Lack of Concentration
7. GASTROINTESTINAL DISTRESS: Does the patient experience any gastrointestinal distress? • No gastrointestinal distress• Constipation• Diarrhea• Indigestion • Dry Mouth• Nausea• Vomiting
APPENDIX C: DRUG SELECTION QUESTIONS

8. PAIN: Does the patient experience pain anywhere in the body? • No pain issue(s)• Abdominal Cramping• Headache• Muscle Pain• Musculoskeletal Pain
9. AKATHISIA/TREMOR: Does the patient su�er from akathisia or tremor? • No akathisia or tremor• Akathisia• Tremor
10. SENSORY DISTURBANCES: Does the patient complain of sensory disturbances? • No sensory disturbance(s)• Blurred Vision• Dizziness• Mydriasis• Tingling• Tinnitus
11. URINATION: Does the patient raise concerns regarding urination frequency? • No urinary change(s)• Frequent Urination• Proteinuria• Urine Retention
12. SKIN: Has the patient complained of any of the following conditions? • No skin issue(s)• Edema of Lower Extremity• Psoriasis• Sweating
13. BLOOD PRESSURE: Is the patient’s blood pressure abnormally increased/decreased? • No blood pressure abnormalities• Hypertension• Orthostatic Hypotension
14. HEART RHYTHM: Does the patient have an abnormal heartbeat? • No heartbeat abnormalities• Bradycardia• Palpitations• Tachycardia
0.5

48
APPENDIX D: VISUAL LANGUAGE 0.1
Sexual Dysfunction Stimulating SweatingSedationPain Control
Anxiety Cognitive Problems
Blurred Vision Decreased Appetite
Constipation
Tachycardia Treat Allergies Tremors Urinary Retention Weight Gain
Nausea Orthostatic Hypotention
Mitigation Against Prolactin
Elevation
Increased Appetite
Mitigate Craving for Tobacco
HypertensionDry Mouth Enhanced Motivation
Impairs Heart Conduction
Gastrointestinal Distress
49
APPENDIX D: VISUAL LANGUAGE 0.2
F47B5B
FBAA22
9B4A4A
F37E8B
C49A6C
63C29D
7EA046
AA82BB
50
Wireframes
APPENDIX E: WEB APPLICATION WIREFRAMES & DESIGN 0.1

51
APPENDIX E: WEB APPLICATION WIREFRAME & DESIGN 0.2
Design
52
APPENDIX E: WEB APPLICATION WIREFRAME & DESIGN 0.3

53
APPENDIX E: WEB APPLICATION WIREFRAME & DESIGN 0.4

54
APPENDIX F: TEST SCENARIOS & RESULTS SCENARIO 1
General Information
1. Age: 60
2. Gender: Male
4. Does the patient smoke cigarettes? No
5. Does the patient drink alcohol regularly? No
Family Medical History
1. Does the patient have a family history of major illnesses?
History of Suicides and Major Depression
2. Does the patient have blood relatives with positive experiences with any antidepressant medications? No
3. Does the patient have blood relatives with negative experiences with any antidepressant
medications? Paroxetine HCl
Patient Medical History
1. Has the patient su�ered a heart attack in the past 10 weeks? No
2. Does the patient plan to undergo surgery in the near future (e.g. 1-2 months)? No
3. Does the patient have any preexisting condition(s)? QT Syndrome
4. Is the patient currently taking any medication or receiving any of the following treatment? No
5. Has the patient taken any antidepressants with success? No
6. Has the patient taken any antidepressants without success? Escitalopram
7.Is the patient hypersensitive to any antidepressants? No
Patient Preferences
Increase Sleep 3
Increase Appetite 3
Increase Energy 1
Reverse Hardened Stool 2

Patient Symptoms
1. Decreased Appetite
2. Decreased Weight
3. Lethargy
4. Insomnia
5. Decreased Libido
6. Lack of Concentration
7. Constipation
8. No Pain Issues
9. No Akathisia or Tremor
10. No Sensory Disturbances
11. No Urinary Changes
12. No Skin Issues
13. Hypertension
14. No Heartbeat Abnormalities
Dr. Kaplin’s RecommendationsMirtazapine (good)Duloxetine (ok)Levomilnacipran (ok)Sertraline (ok)Trazodone (ok)Vilazodone (ok) Vortioxetine (ok)Bupropion (less good)Citalopram (less good)Desvenlafaxine (less good)Escitalopram (less good)Fluoxetine (less good)Paroxetine (less good)Venlafaxine (less good)Amitriptyline (bad)Clomipramine (bad)Desipramine (bad)Doxepin (bad)Imipramine (bad)Nortriptyline (bad)
Algorithm RecommendationsMirtazapineTrazodoneCitalopramFluoxetineVortioxetineSertralineVilazodoneDesvenlafaxineBupropionLevomilnacipranParoxetineDuloxetineVenlafaxineEscitalopramAmitriptylineClomipramineDesipramineDoxepinImipramineNortriptyline

55
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 1)

Total Points 0.1

56
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 1)

Total Points 0.2

57
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 1)

Patient Preferences 0.1

58
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 1)

Patient Preferences 0.2

59
APPENDIX F: TEST SCENARIOS & RESULTS SCENARIO 2
General Information
1. Age: 30
2. Gender: Male
4. Does the patient smoke cigarettes? Yes
5. Does the patient drink alcohol regularly? Yes
a. Has the patient ever felt he/she needed to cut down on his/her drinking? Yes
b. Have people annoyed the patient by criticizing his/her drinking? Yes
c. Has the patient ever felt guilty about drinking? Yes
d. Has the patient ever felt he/she needed a drink �rst thing in the morning (eye-opener) to steady
his/her nerves or to get rid of a hangover? Yes
Family Medical History
1. Does the patient have a family history of major illnesses?
Alcoholism, Drug Abuse, Major Depression
2. Does the patient have blood relatives with positive experiences with any antidepressant
medications? No
3. Does the patient have blood relatives with negative experiences with any antidepressant
medications? No
Patient Medical History
1. Has the patient su�ered a heart attack in the past 10 weeks? No
2. Does the patient plan to undergo surgery in the near future (e.g. 1-2 months)? No
3. Does the patient have any preexisting condition(s)? No
4. Is the patient currently taking any medication or receiving any of the following treatment? No
5. Has the patient taken any antidepressants with success? No
6. Has the patient taken any antidepressants without success? Escitalopram
7.Is the patient hypersensitive to any antidepressants? No
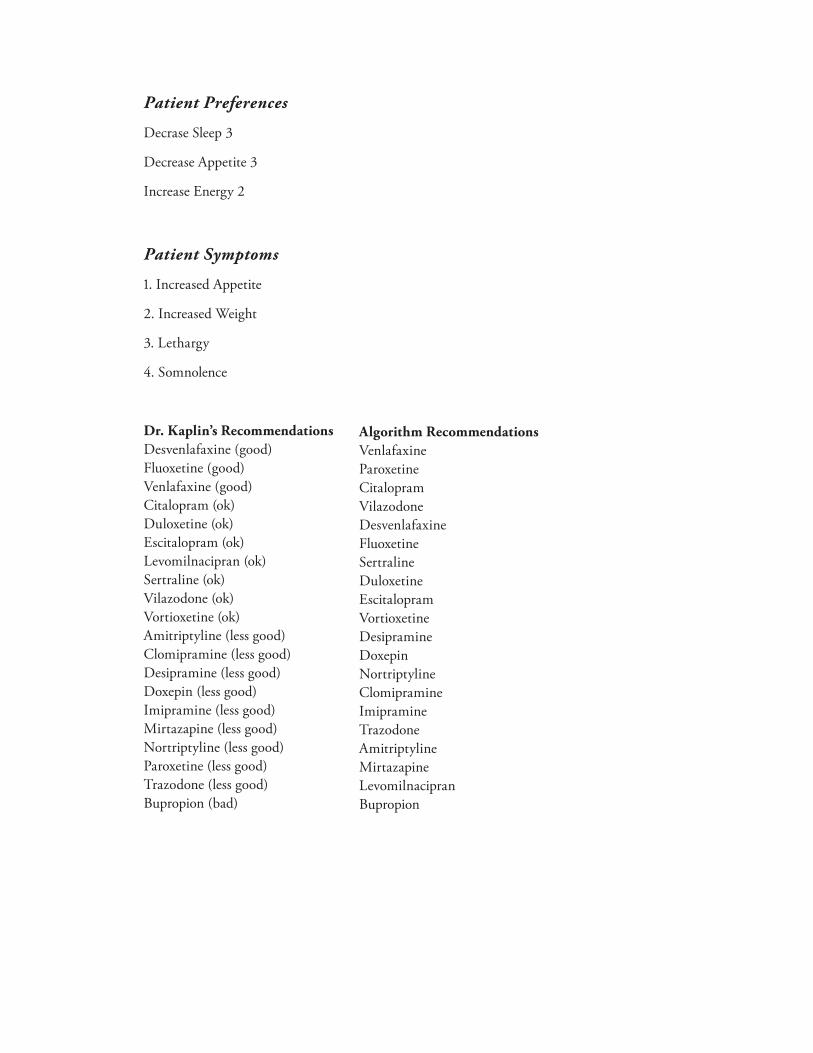
Patient Preferences
Decrase Sleep 3
Decrease Appetite 3
Increase Energy 2
Patient Symptoms
1. Increased Appetite
2. Increased Weight
3. Lethargy
4. Somnolence
Dr. Kaplin’s RecommendationsDesvenlafaxine (good)Fluoxetine (good)Venlafaxine (good)Citalopram (ok)Duloxetine (ok)Escitalopram (ok)Levomilnacipran (ok)Sertraline (ok)Vilazodone (ok)Vortioxetine (ok)Amitriptyline (less good)Clomipramine (less good)Desipramine (less good)Doxepin (less good)Imipramine (less good)Mirtazapine (less good)Nortriptyline (less good)Paroxetine (less good)Trazodone (less good)Bupropion (bad)
Algorithm RecommendationsVenlafaxineParoxetineCitalopramVilazodoneDesvenlafaxineFluoxetineSertralineDuloxetineEscitalopramVortioxetineDesipramineDoxepinNortriptylineClomipramineImipramineTrazodoneAmitriptylineMirtazapineLevomilnacipranBupropion
60
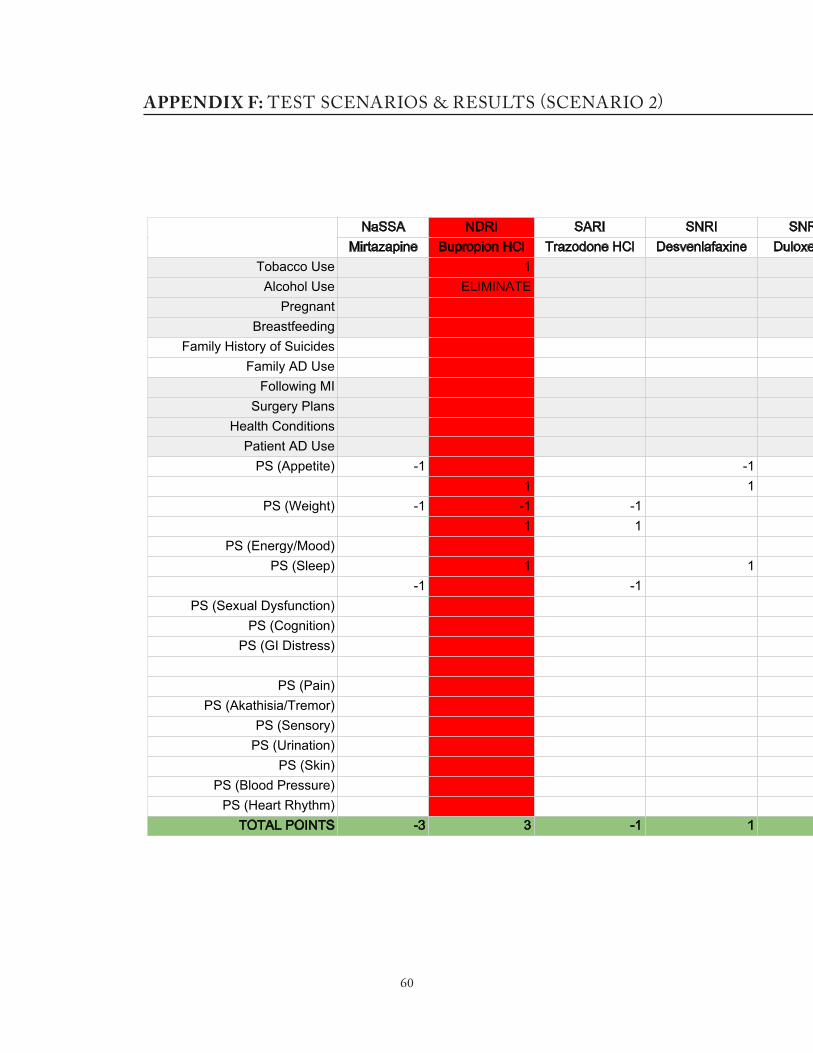
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 2)

Total Points 0.1

61
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 2)

Total Points 0.2
62
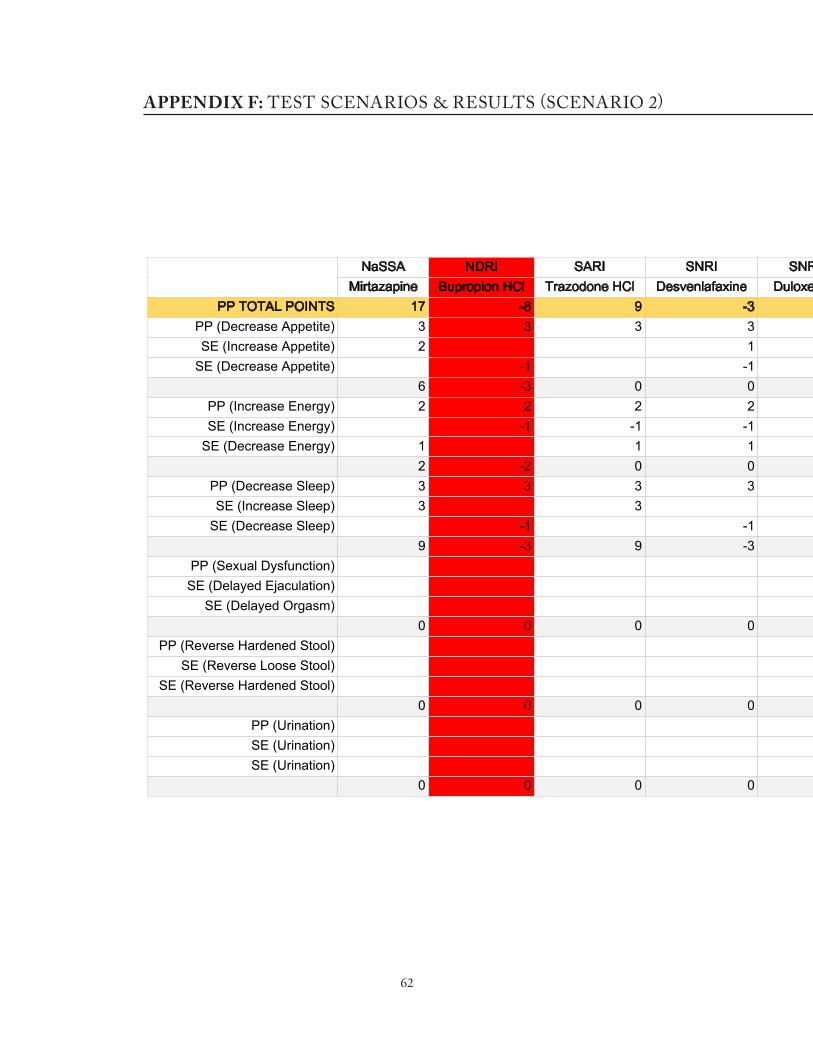
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 2)
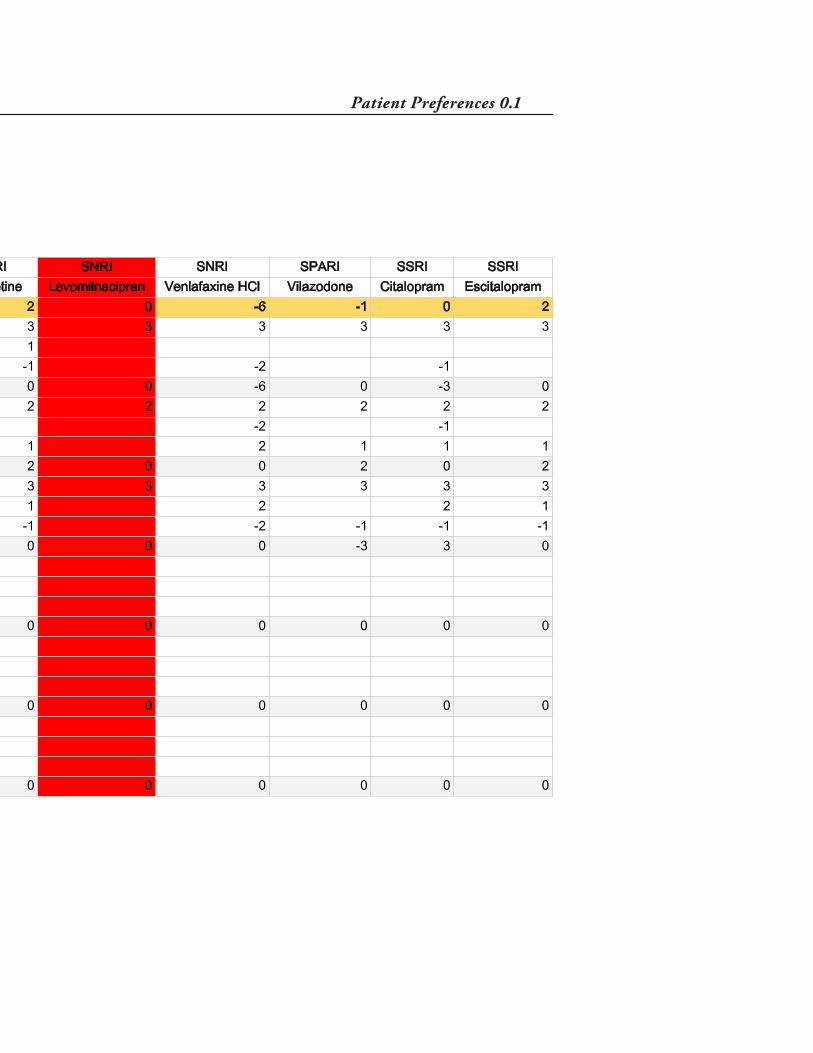
Patient Preferences 0.1

63
APPENDIX F: TEST SCENARIOS & RESULTS (SCENARIO 2)

Patient Preferences 0.2

64
APPENDIX G: IRB PRE/POST QUESTIONNAIRES
PRE-QUESTIONAIRE
1. What is your highest level of education? (Categories: MD, Psychiatry resident, Psychiatrist, Other)
2. How much experience do you have in psychiatry?
3. What did you �nd most di�cult when learning about antidepressants? Categories:
pharmacodynamics, names of antidepressants, side e�ect pro�les, drug drug interactions,
keeping up with current events (ie. newly approved medication) Rate 1-10.
4. How con�dent are you prescribing antidepressants to patients?
5. How helpful do you think an application would help prescribe antidepressants? Rate 1-10.
POST-QUESTIONAIRE
1. How con�dent are you prescribing antidepressants to patients with the application? Rate 1-10.
2. Do you agree with the results of the app? Rate 1-10.
3. Do you trust the application? Rate 1-10.
4. Do you like using the application? Rate 1-10.
3. Do you think this application would be helpful for healthcare professionals? Rate 1-10.
4. How likely would you be to use this application when prescribing antidepressants? Rate 1-10.
5. Was the application easy to navigate? Rate 1-10.
6. What improvements would you make with this application? (Categories: Login/Disclaimer
Options, Diagnosis, Drug Selection, Overall Design, Visual Language, Descriptions, Other
with blank) Based on categories checked, please elucidate.
7. How well did this application help with the understanding of the following categories:
pharmacodynamics, names of antidepressants, side e�ect pro�les, drug drug interactions,
keeping up with current events (ie. newly approved medication) Rate 1-10.

65
REFERENCESADAA Anxiety and Depression Association of America. “Facts & Statistics.” [2014,
Accessed via the Web, 19 February 2016]. <http://www.adaa.org/about-adaa/press-room/facts-statistics>.
American Foundation for Suicide Prevention. “Suicide Statistics.” [Accessed via the Web, 19 February 2016]. <https://afsp.org/about-suicide/suicide-statistics/>.
Anderson, Monica. “6 facts about Americans and their smartphones.” Pew Research Center. [1 April 2015, Accessed via the Web, 5 March 2016]. <http://www.pewresearch.org/fact-tank/2015/04/01/6-facts-about-americans-and-their-smartphones/>.
Barkil-Oteo A. Collaborative Care for Depression in Primary Care: How Pychiatry Could “Troubleshoot” Current Treatments and Practice. Yale Journal of Biology and Medicine [2013, Accessed 14 March 2016].
Berkshire Healthcare / National Health Service (2010). Antidepressant Guidelines: Treatment of Depression. 6.2th ed. 4. Print.
Berardi D, Leggieri G, Ceroni G B, Rucci P, Pezzoli A, Paltrinieri E, Grazian N, Ferrari G. Depression in primary care. A nationwide epidemiological survey. Family Practice. [2002, Accessed 14 March 2016].
European Society of Cardiology (ESC). “Depression associated with 5-fold increased mortality risk in heart failure patients.” Science Daily, [23 May 2015, Accessed via the Web, 19 February 2016]. <https://www.sciencedaily.com/releases/2015/05/150523081918.htm>.
Connolly K, Thase M. Vortioxetine: a New Treatment for Major Depressive Disorder. Taylor Francis Online. [11 Feb 2016, Accessed via the Web, 19 March 2016]. <http://www.tandfonline.com/doi/full/10.1517/14656566.2016.1133588#.Vu3afBIrIUE>.Medscape. “Drugs & Diseases.”
DBSA Depression and Bipolar Support Alliance. “Depression Statistics.” [Accessed via the Web, 5 March 2016]. <http://www.dbsalliance.org/site/PageServer?pagename=education_statistics_depression>.
Gallo J J, Hwang S, Joo J H, Bogner H R, Morales K H, Bruce M L, Reynolds III C F. Multimorbidity, Depression, and Mortality in Primary Care: Randomized Clinical Trial of an Evidence-Based Depression Care Management Program on Mortality Risk. Journal of General Internal Medicine. [2015, Accessed 14 March 2016].
Healy, Melissa. Antidepressants in primary care: is this any way to treat depression?. Los Angeles Times. [04 August 2011, Accessed 20 February 2016]. <http://articles.latimes.com/2011/aug/04/health/lat-he-depression-treatment-20110804>.

66
IMS Institute for Healthcare Informatics (2011). The Use of Medicines in the United States:
imshealth/Global/Content/IMS%20Institute/Static%20File/IHII_UseOfMed_report.pdf>
College of Physicians. [2012, Accessed via the Web, 1 Nov. 2015]. <http://www.acpinternist.org/archives/2012/01/antidepressants.htm>.
Kaplin, Adam. “What is the Connection Between Depression and Stroke?” Lecture, Johns Hopkins University School of Medicine, Baltimore, MD, September 19, 2014.
Kessler RC, Berglund P, Demler O, et al. The Epidemiology of Major Depressive Disorder: Results From the National Comorbidity Survey Replication (NCS-R). JAMA. [18 June 2003, Accessed 5 March 2016]. <http://jama.jamanetwork.com/article.aspx?articleid=196765>.
Kroenke K. The Role of Decision Aids in Depression Care. JAMA Internal Medicine. [2015, Accessed 14 March 2016].
LeBlanc A, Bodde A E, Branda M E, Yost KJ, Herrin J, Williams M D, Shah N D, Houten H V, Ruud K L, Pencille L J, Montori V M. Translating comparative effectiveness of depression medications into practice by comparing the depression medication choice decision aid to usual care: study protocol for a randomized controlled trial. Trials. [2013, Accessed 14 March 2016].
Man C, Nguyen C, Lin S. Effectiveness of a Smartphone App for Guiding Antidepressant Drug Selection. Society of Teachers of Family Medicine. [September 2014, Accessed via the Web, 19 February 2016]. <http://www.stfm.org/FamilyMedicine/Vol46Issue8/Man626>.
Martin, Taylor. The evolution of the smartphone. Pocketnow. [28 July 2014, Accessed 5 March 2016]. <http://pocketnow.com/2014/07/28/the-evolution-of-the-smartphone>.
NIH National Institute of Mental Health. “Major Depression Among Adults.” [Accessed via the Web, 19 February 2016]. <http://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adults.shtml>.
Pratt L A, Brody D J, Gu Q. Antidepressant use in persons aged 12 and over: United States, 2005–2008. Centers for Disease Control and Prevention, [1 October 2011, Accessed via the Web, 1 Nov. 2015]. <http://www.cdc.gov/nchs/data/databriefs/db76.htm>.
Rendgen, Sandra. Information Graphics. Taschen, 2013.
Richelson, Elliot. Interactions of Antidepressants with Neurotransmitter Transporters and Receptors and their Clinical Relevance. The Journal of Clinical Psychiatry. [2003, Accessed 14 March 2016].
Rosack J. Collaboration Key to Integrating Depression Treatment in Primary Care. Psychiatric News. [2003, Accessed 14 March 2016].

67
Samples H, Mojtabai R. Antidepressant Self-Discontinuation: Results From the Collaborative Psychiatric Epidemiology Surveys. Psychiatric Services. [2015, Accessed 14 March 2016].
Applications. New York: Cambridge University Press, 2012.
Statista The Statistics Portal. “Number of smartphone users in the United States from 2010 to 2019.” [Accessed via the Web, 5 March 2016]. <http://www.statista.com/statistics/201182/forecast-of-smartphone-users-in-the-us/>.
Suehs B, Argo T F, Bendele S D, Crismon M L, Trivedi M H, Kurian, B. (2008) Texas Medication Algorithm Project Procedural Manual: Major Depressive Disorder Algorithm. Texas Medication Algorithm Project, 2008. pp 45-59. Print.
Thombs B D, Benedetti A, Kloda L A. et al. The diagnostic accuracy of the Patient Health Questionnaire-2 (PHQ-2), Patient Health Questionnaire-8 (PHQ-8), and Patient Health Questionnaire-9 (PHQ-9) for detecting major depression: protocol for a systematic review and individual patient data meta-analyses. Systematic Reviews 3. [27 October 2014, Accessed via the Web, 1 November 2015]. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4218786/>.
Wang S, Han C, Lee S, Patkar A, Masand P, Pae C. Vilazodone for the Treatment of Major Depressive Disorder: Focusing on Its Clinical Studies and Mechanism of Action. KoreaMed Synapse. [18 March 2015, Accessed via the Web, 19 March 2016]. <http://synapse.koreamed.org/DOIx.php?id=10.4306/pi.2015.12.2.155>.
Weisberg R B, Dyck I, Culpepper L, Keller M B. Psychiatric Treatment in Primary Care Patients With Anxiety Disorders: A Comparison of Care Received From Primary Care Providers and Psychiatrists. American Journal of Psychiatry. [2017, Accessed 14 March 2016].

68
VITAAmy Zhong was born on July 22, 1988 in Washington, DC. She spent her childhood and
charcoal illustration. In 2010, Amy graduated with a Bachelor of Fine Arts degree for her work
in 2D animation from the University of Michigan in Ann Arbor, Michigan. While working the
(CMG) branch of Carus Publishing in Chicago, Illinois, Amy had the opportunity to illustrate for
CMG’s science and arts magazine Muse. It was the challenge of this assignment that led Amy to
illustration. In the fall of 2014, Amy moved to Baltimore, Maryland to study in the Department of
Art as Applied to Medicine at the Johns Hopkins School of Medicine, where she is to be awarded
with a Master of Arts degree in Medical and Biological Illustration in May 2016.