Anticoagulation Therapy in Percutaneous Coronary...
46
Anticoagulation Therapy in Percutaneous Coronary Interventions
Transcript of Anticoagulation Therapy in Percutaneous Coronary...
-
Anticoagulation Therapyin Percutaneous Coronary Interventions
-
Disclosure Statement of Financial Interest
None
-
Thrombus Formation: Platelet Activation and Blood Coagulation
Coagulationcascade
FactorXa
Thrombin
Fibrinogen
fibrin
Platelets
Thrombin
ADP
Thromboxane
Collagen
Activated Platelet
Platelet Aggregation
GP IIb/IIIa
CLOT
InflammationCellular
proliferation
Hamm CW. et al.ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:
The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology.(ESC).
-
Coagulation Processes: Mostly Cell Surface-based
De Caterina R. et al.General mechanisms of coagulation and targets of anticoagulants (Section I).
Position Paper of the ESC Working Group on Thrombosis--Task Force on Anticoagulants in Heart Disease.Thromb Haemost.2013 Apr;109(4):569-79
INITIATION AMPLIFICATION PROPAGATION
-
Thrombin: Exertion of Multiple Biological Actions
TF/FVIIa
FX FIX
FIXa
FVIIIaFXa
FVa
thrombin inflammationProtein C activationand anticoagulation
FXI activationFXIII activation andfibrin stabilazation
Platelet activationAnti fibrinolysis
FV FVIII
FVa FVIIIa
Fibrinogen Fibrin
-
Thrombin: Actions on Blood Cells and Blood Vessels
Endothelium
Platelet
MonocyteLymphocyte
SmoothMusclecell
ThrombinCytokinesGrowth factorsAutocoidsProteases
Shape andpermeabilitychanges
Serine protease generated at sites of vascularinjury. Most effective platelet activator (PAR-protease activated receptor). Elicits host ofresponses in vascular endothelium: shape &permeability changes, mobilization of adhesivemolecules to endothelial surface & stimulation ofautocoid (small molecule mediators such asprostaglandins, PAF) & cytokine production.Chemotactic for monocytes. Mitogenic forlymphocytes & mesenchymal cells.
NeutrophilNeutrophil
Coughlin SR.Thrombin signalling and protease-activated receptors.
Nature.2000 Sep 14;407(6801):258-64
-
Thrombin: the Multi Faceted Enemy Within
In vivo arterial thrombosis involvesplatelet aggregation, tissue factorgeneration and fibrin formation
Falati S. et al.Real-time in vivo imaging of platelets, tissue factor and fibrin during arterial thrombus formation in the mouse.
Nat Med.2002 Oct;8(10):1175-81
-
Thrombus Composition in AMI:A Time Dependent Phenomenon
Silvain J. et al.Composition of coronary thrombus in acute myocardial infarction.
J Am Coll Cardiol. 2011 Mar 22;57(12):1359-67
Scanning Electron Micrograph at 3,000 Magnification
-
Thrombin Generation in ACS and Stable CAD
ACS
Control
CAD
Brummel-Ziedins K. et al.Thrombin generation in acute coronary syndrome and stable coronary artery disease: dependence on plasma factor composition.
J Thromb Haemost. 2008 Jan;6(1):104-10
-
Thrombin Levels in ACS: 6 Mo. F.U
Merlini PA. et al.Persistent activation of coagulation mechanism in unstable angina and myocardial infarction.
Circulation.1994 Jul;90(1):61-8
-
atherosclerosis pronecoronary segment
focal plaque formation
vascular remodeling response
Constrictiveremodeling
Compensatoryremodeling
Excessive expansiveremodeling
Flow limitationstable angina
quiescence potential forplaque rupture
High ESS
Subclinical Plaque Ruptureor Intraplaque Hemorrhage
Hypothesis of the Natural History ofVulnerable Plaque and CAD Progression
Low ESS
5-10%
95%
~5%
+
+
Stable CAD
Acute CoronarySyndromes/RapidPlaque Progression
PlaqueErosion
PlaqueRupture
+
Stone PH.TCT 2014
-
Rationale for antithrombotic therapy during PCI
Tissue Factor
Adhesion Molecules
ThrombinGeneration
PlateletActivation
Vessel Wall Injuryand Inflammation
David J. CohenFellows Course 2015
Mechanical vessel injury in PCI andspontaneous injury in ACS are thrombogenic
-
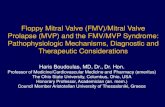
Heparins (UFH/LMWH): Mechanism of Action
Heparin/antithrombin (AT) complex inhibits thrombin and Factor XaMust have adequate AT present for anticoagulant effect
Thrombin inhibition requires“bridging” by heparin chain(at least 18 units)
LMWH has greater activityagainst Xa than thrombin
Heparin chains withpentasaccharide sequence(~30%) bind to AT causing aconformational change
Hirsh J. et al.Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics, dosing, monitoring, efficacy, and safety.
Chest. 2001 Jan;119(1 Suppl):64S-94S
UFHbound
toAT
-
Heparin: A Disgusting ProductCombine 5,000 lbs. intestines, 200 gallons water, 10 gallons chloroform, and 5gallons toluene. Hold at 90°F for 17 hours.Add 30 gallons acetic acid, 35 gallons ammonia, sodium hydroxide toadjust pH, and 235 gallons water.Bring to a boil; then filter.Add 200 gallons hot water to filtrate and allowto stand overnight, then skim off the fat.Keep pancreatic extract at 100°F for three days,then bring to boil.Filter solids and assay for heparin content.
G.W. Stone, TCT 2014.Bivalirudin vs. Heparin Monotherapy in STEMI: Debating the merits.
-
Pharmacological Properties of Current Anticoagulants:UFH
UFHPredictability in pharmacological profile -
Cofactor required +++
Renal clearance -
Non-specific protein binding +++
Platelect activation +++
Rebound of thrombin generation after discontinuation +++
Inhibition of bound thrombin -
Neutralization by platelet factor 4 +++
Inhibition of thrombin generation +
-
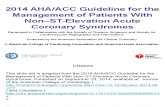
Unfractionated Heparin in PCI: a Meta-Analysis
Chew DP. et al.Defining the optimal activated clotting time during percutaneous coronary intervention: aggregate results from 6 randomized, controlled trials.
Circulation.2001 Feb 20;103(7):961-6
10.1%11.1%
8.6% 8.9%
6.6%7.5% 7.7%
9.8%
0.15
0.10
0.05
0.00250 300 350 400 450
Minimum ACT at device activation
Probability of 7 Day Death, MI or RevascPr
obab
ility
of d
eath
, MI,
orre
vasc
at 7
-day
s p = 0.001 between 11.1% and 7.7%
-
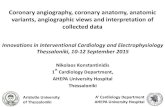
Unfractionated Heparin in PCI: a Meta-Analysis
16.9%
12.4%
8.6%9.9%
12.4%13.7%
12.4%
16.9%
Maximum ACT during PCI
0.20 Probability of TIMI major + minor hemorrhage
0.15
0.10
0.05
0.00250 300 350 400 450
Prob
abili
ty o
f maj
or o
r
min
or b
leed
ing
Chew DP. et al.Defining the optimal activated clotting time during percutaneous coronary intervention: aggregate results from 6 randomized, controlled trials.
Circulation.2001 Feb 20;103(7):961-6
-
Heparin + GP IIb/IIIa:Efficacy and Bleedingby Tertiles of Maximum ACT
Heparin + GP IIb/IIIa:Efficacy and Bleedingby Tertiles of Maximum ACT
10,0%11,5%
10,3%
0,6% 0,3% 0,4%
6,1%7,3% 7,0%
0,7%1,9% 1,4%
0%
5%
10%
15% placebo
eptifibatide39%39% 37%37%
ACT244 - 292
n=678
ACT244 - 292
n=678
ACT>292n=676
ACT>292n=676
32%32%
ACT292n=676
ACT
-
Pharmacological Properties of Current Anticoagulants:LMWH
LMWHPredictability in pharmacological profile ++
Cofactor required +++
Renal clearance ++
Non-specific protein binding +
Platelect activation +
Rebound of thrombin generation after discontinuation +
Inhibition of bound thrombin -
Neutralization by platelet factor 4 +
Inhibition of thrombin generation ++
-
Enoxaparin in PCIsimulated curve
1.0 mg/kg sc steady state + 0.3 mg/kg iv
0.00.20.40.60.81.01.21.41.61.82.0
0 2 4 6 8 10 12 14 16 18 20Time (h)
aXa I
U/m
l
0.3 mg/kg IV at 8 hours or more after lastsc. injection allows “optimal” therapeutic levels
Martin JL. et al.Reliable anticoagulation with enoxaparin in patients undergoing percutaneous coronary intervention:
The pharmacokinetics of enoxaparin in PCI (PEPCI) study.Catheter Cardiovasc Interv. 2004 Feb;61(2):163-70
-
Pharmacotherapy Across the Spectrum of CAD/ PCI:Enoxaparin
Ris
k/ (M
orta
lity)
Stableangina
Unstableangina
NSTEMI STEMI
N=18.452Randomized Patients
David J. CohenFellows Course 2015
-
Study Pts. Comparators Setting Main Results
STEEPLE 3528
IV UFHVs.
IV enoxaparin 0.75 mg/kgVs.
IV enoxaparin 0.5 mg/kgElective PCI
Significant reduction in 48h non–CABG-related bleeding* with Enoxaparin 0.5.
Significant reduction in major bleeding withboth enoxaparin groups.
SYNERGY 10027
IV UFHVs.
Enoxaparin
NSTE-ACS No differences in 30-day death/MI*. No differences in procedural events. Bleeding modestly higher with enoxaparin. Relative advantage of enoxaparin when
therapy crossovers were censored.
ATOLL 910IV UFH
Vs.IV enoxaparin 0.5 mg/kg
STEMI Not significant reduction of 30-day ischemic
outcomes with enoxaparin. No differences in bleeding.
RCT comparing IV enoxaparin vs. UFH
-
ATOLL Per-Protocol Analysis:Primary End Point/ Main Safety End Point
Collet JP. Et al.A direct comparison of intravenous enoxaparin with unfractionated heparin in primary percutaneous coronary intervention (from the ATOLL trial).
Am J Cardiol. 2013 Nov 1;112(9):1367-72
-
Pentasaccharide (and Hexadecasaccharide):Fondaparinux anti Fxa
But…Wait! This is an interventional meeting!!!
-
(Gly)4
Bivalirudin: Bivalent Synthetic Direct Thrombin Inhibitor
Gly-Pro-Arg-Pro(active site binding region)
C-terminal dodecapeptide(exosite 1-binding region)
• Bivalent direct thrombininhibitor
• High specificity andpotency
• Lack of dependence onantithrombin-III
• Effect on clot-bound &free thrombin
• No platelet activation• No inhibition by PF4 and
others• t½ of 25 min
Adapted from:Eric J. Topol, Paul S. Ternstein.
Textbook of Interventional Cardiology, 6th Edition.Elsevier/ Expert Consult.
-
Pharmacological Properties of Current Anticoagulants:Bivalirudin
BivalirudinPredictability in pharmacological profile +++
Cofactor required -
Renal clearance ++
Non-specific protein binding -
Platelect activation -
Rebound of thrombin generation after discontinuation -
Inhibition of bound thrombin +++
Neutralization by platelet factor 4 +
Inhibition of thrombin generation +++
-
Pharmacotherapy Across the Spectrum of CAD/ PCI:Bivalirudin
Ris
k/ (M
orta
lity)
Stableangina
Unstableangina
NSTEMI STEMI
N=27.593Randomized Patients
David J. CohenFellows Course 2015
-
Study Pts. Comparators Setting Main ResultsACUITY(multicenter) 13819
Heparin + GPI Vs.Bivalirudin + GPI Vs.
Bivalirudin
NSTE-ACSPCI 56%
Similar ischemic events. Bleed reduction with bivalirudin monotherapy.
ISAR-REACT 4(multicenter) 1721
UFH + GPI Vs.Bivalirudin
NSTE-ACSPCI 100%⃰
No differences in ischemic events/major bleed. Bleed reduction with bivalirudin.
HORIZONS- AMI(multicenter) 3602
UFH + GPI vs.Bivalirudin (infusion
stopped at the end of PCI)
STEMIP- PPCI
Bleed and mortality reduction with bivalirudin. Similar MACE; acute ST higher with bivalirudin.
EUROMAX(multicenter) 2218
Heparin + optional GPI Vs.Bivalirudin (infusion
prolonged after PCI*)
STEMIP-PCI
Bleed and mortality reduction with bivalirudin. Similar MACE; Acute ST higher with bivalirudin.
BRIGHT(multicenter) 2194
UFH Vs.Bivalirudin Vs.UFH + Tirofiban
STEMINSTEMI
Ischemic events/bleed reduction with bivalirudincompared to both groups.
Bleed reduction with bivalirudin.
HEAT PPCI(single center) 1812
UFH Vs.Bivalirudin (infusion
stopped at the end of PCI)
STEMIP-PCI
Reduction in ischemic events with UFH No difference in bleeding Acute ST higher with bivalirudin.
RCT on Bivalirudin
-
Historical Trials of Bivalirudin vs. UFH in PCI
Trial ComparatorStrategyIschemicendpoints Bleeding
REPLACE 2 UHP+GPIequivalent
↓↓
ACUITY UHP+GPI equivalent ↓↓
HORIZONS AMI UHP+GPI equivalent ↓↓
ISAR REACT 3 UHP (high dose) equivalent ↓
ISAR REACT 4 UHP+GPI equivalent ↓↓
-
What about PCI has Changed Over the Last Decade?
Increased use of novel ADP antagonists–More potent and more rapid onset than clopidogrel
Marked decrease in use of GPIs
Development of 2nd and 3rd generation DES–Less thrombogenic than 1st gen DES or BMS
Increased use of transradial PCI
Taken together, these changes have dramatically alteredthe thrombotic and bleeding milieu in the cath lab:
Motivation to reassess antithrombotic therapy!
-
The Great Debate:UFH vs. Bivalirudin
-
Bivalirudin vs. Heparin Monotherapy During Primary PCI in STEMI:Three major RCTs
EUROMAX BRIGHT HEAT PPCIN centers 65 82 1N patients 2198 2194 1812-Bivalirudin 1089 735 905-Heparin 460 729 907-Heparin + GPI 649 730 -Heparin mono bolus 60 IU/Kg 100 IU/Kg 70 IU/KgBival. infusion None, low or
High doseMean 4.5 h
Low doseMean 4h -
GPI bailoutBiv. vs UFH 7.9% vs 25.4% 4.4% vs 5.6% 13.5% vs 15.5%
Prasugrel/ Ticagrelor 59% 0% 89%
-
0,0
2,0
4,0
6,0
8,0
10,0
0 5 10 15 20 25 30
Days from Randomization Date
Even
t Rat
e
Bivalirudin
Heparins with optional GPI 8.4%
Log-rank p = 0.002
Euromax Primary Endpoint:Death or Major Bleed, 30 day
5.1%
Zeymer U. et al.Bivalirudin is superior to heparins alone with bailout GP IIb/IIIa inhibitors in patients with ST-segment elevation myocardial infarction transported
emergently for primary percutaneous coronary intervention: a pre-specified analysis from the EUROMAX trial.Eur Heart J. 2014 Sep 21;35(36):2460-7
Stent thrombosis(ARC definition)
17 (1.6) 6 (0.5) 2.89 (1.14–7.29) 0.02
Definite 17 (1.6) 6 (0.5) 2.89 (1.14–7.29) 0.02Probable 0 (0) 0 (0) – n/aAcute (≤24 hours) 12 (1.1) 2 (0.2) 6.11 (1.37–27.24) 0.007Subacute
(>24 hours to 30 days)5 (0.5) 4 (0.4) 1.27 (0.34–4.73) 0.75
-
HEAT PPCI:Timing of First MACE Event
Shahzad A. et al.Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI):
an open-label, single centre, randomised controlled trial.Lancet.2014 Nov 22;384(9957):1849-58
Bivalirudin Heparinn % % n
All Events 24 3.4 % v 0.9 % 6
Relative risk = 3.91 (95% CI 1.6 - 9.5) P=0.001
-
Is HEAT-PPCI an Outlier or an Eye-Opener ?
Meta-analysis of 16 RCTs (n=33,958)comparing bivalirudin vs. heparin-basedanticoagulation for PCI
When pooled results indicated significantheterogeneity, results stratified byindication for PCI (STEMI, NSTEMI,elective) and use of GPIs (planned vs.provisional) in heparin and bivalirudinarms
Cavender MA., Sabatine MS.Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials.
Lancet.2014 Aug 16;384(9943):599-606
-
Stent Thrombosis: STEMI Trials
Cavender MA., Sabatine MS.Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials.
Lancet.2014 Aug 16;384(9943):599-606
-
Bleeding: According to Pattern of GPI Use
Cavender MA., Sabatine MS.Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials.
Lancet.2014 Aug 16;384(9943):599-606
Findings suggest that reduced bleeding with bivalirudin is directlyrelated to the rate of use of GPI in the comparison group
-
MACE: All Indications
Cavender MA., Sabatine MS.Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials.
Lancet.2014 Aug 16;384(9943):599-606
No evidence of between-trial heterogeneity (Q-stat 12.1, p=0.79)Pooled OR 1.09 (95% CI 1.01-1.17) P= 0.0204
-
Mortality: All Trials
Cavender MA., Sabatine MS.Bivalirudin versus heparin in patients planned for percutaneous coronary intervention: a meta-analysis of randomised controlled trials.
Lancet.2014 Aug 16;384(9943):599-606
No difference in mortality across trialsHORIZONS results appear to be an outlier
-
What Do the Guidelines Say?Enoxaparin UFH Bivalirudin
Elective PCI (EU 2014) IIa B I B IIa⃰ A
Elective PCI (U.S. 2011) IIb B I C I B
NSTE-ACS (EU 2014) IIa⃰⃰⃰ ⃰ B I C I A
NSTE-ACS (U.S. 2011) IIb B I C I B
STEMI (EU 2014) IIa B I C IIa A
STEMI (U.S. 2013) - - I C I B
B
-
The Future So Bright:Factor IX Inhibition Aptamers
Aptamers encode their own control agents
Aptamer Control Agent
Woodruff RS., Sullenger BA.Modulation of the Coagulation Cascade Using Aptamers.
Arterioscler Thromb Vasc Biol.2015 Aug 27. pii: ATVBAHA.115.300131. [Epub ahead of print]
pegnivacoginAnticoagulant aptamer
anivamersenActive control agent
-
Aptamer and Reversal Agent: Mode of Action
ActivatedProtein function
proceeds unimpeeded
InactivatedAptamer with high
specificity and highaffinity selectively
inhibits protein
ActivatedControl agent binds to
aptamer, complex is incapableof inhibiting
target protein andfunction returns to normal
Woodruff RS., Sullenger BA.Modulation of the Coagulation Cascade Using Aptamers.
Arterioscler Thromb Vasc Biol.2015 Aug 27. pii: ATVBAHA.115.300131. [Epub ahead of print]
REG-1 Aptamer Anticoagulant2-Component Controllable Factor IX Inhibitor
-
Guidelines: or else…Where Is The Knowledge We Have Lost In Information?
2014 ESC/EACTS Guidelines on myocardial revascularization:the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for
Cardio-Thoracic Surgery (EACTS).Eur J Cardiothorac Surg. 2014 Oct;46(4):517-92
Roughly 5 different antiplatelet drugs × roughly 5 differentanticoagulants × 4 major different clinical settings:
DO THE MATH.!
-
Balancing Risks and Benefits in ChoosingAdjunct Pharmacological Therapy for PCI
IschemiccomplicationsRecurrent ischemiaMyocardial infarctionIschemia-driven TVRStent thrombosis
HemorrhagicComplicationsAccess site relatedNon-access siteIntracranialGI,GU, otherBlood transfusions
Survival and QOL
-
Thank you
-
Months After Randomization
Is there a Need for Ongoing Factor Xa inhibition?
Rivaroxaban(both doses)
HR 0.84(0.74-0.96)ARR 1.7%
mITT p = 0.008ITT p = 0.002
NNT = 59
10.7%
8.9%
Estim
ated
Cum
ulat
ive
Rat
e (%
) Placebo
5113 4307 3470 2664 1831 1079 42110229 8502 6753 5137 3554 2084 831
PlaceboRivaroxaban
2 Yr KM Estimate
No. at Risk
Mega JL. et al.Rivaroxaban in patients stabilized after a ST-segment elevation myocardial infarction: results from the ATLASACS-2-TIMI-51 trial (Anti-Xa Therapy toLower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome-Thrombolysis In Myocardial Infarction-51).
J Am Coll Cardiol. 2013 May 7;61(18):1853-9