Anticoagulant Therapy in nstemi patients alwi - The Role of Anticoagula… · Szummer et al. JAMA....
37
Curriculum Vitae • Name : Prof. DR. Dr. Idrus Alwi SpPD, K-KV, FACC, FESC, FAPSIC, FINASIM, FACP. • Current Position : Professor of Internal Medicine, Faculty of Medicine, University of Indonesia. • Medical Student : Faculty of Medicine University of Indonesia 1986 • Internist : Faculty of Medicine University of Indonesia 1996 • Cardiovascular Consultant : The Indonesian Society of Internal Medicine , 2001 • PhD : Faculty of Medicine University of Indonesia, 2006 • FACC : American College of Cardiology, 2006 • FESC : European Society of Cardiology, 2008 • FAPSIC : Asia Pacific Society of Interventional Cardiology, 2009 • FINASIM : Indonesian Society of Internal Medicine, 2009 • FACP : American Colleague of Physician, 2013 • Advanced Course in Cardiology, Melbourne 1997 • Advanced Course on Echocardiography and Others Non Invasive Cardiology, Melbourne 1997 • Stem cell NOGA course, Cincinnatti, Ohio, 2009 • ASAN Interventional Cardiology Course, Seoul, 2011
Transcript of Anticoagulant Therapy in nstemi patients alwi - The Role of Anticoagula… · Szummer et al. JAMA....

Curriculum Vitae• Name : Prof. DR. Dr. Idrus Alwi SpPD, K-KV, FACC, FESC, FAPSIC,
FINASIM, FACP.
• Current Position : Professor of Internal Medicine, Faculty of Medicine,
University of Indonesia.
• Medical Student : Faculty of Medicine University of Indonesia 1986
• Internist : Faculty of Medicine University of Indonesia 1996
• Cardiovascular Consultant : The Indonesian Society of Internal Medicine , 2001
• PhD : Faculty of Medicine University of Indonesia, 2006
• FACC : American College of Cardiology, 2006
• FESC : European Society of Cardiology, 2008
• FAPSIC : Asia Pacific Society of Interventional Cardiology, 2009
• FINASIM : Indonesian Society of Internal Medicine, 2009
• FACP : American Colleague of Physician, 2013
• Advanced Course in Cardiology, Melbourne 1997
• Advanced Course on Echocardiography and Others Non Invasive Cardiology, Melbourne 1997
• Stem cell NOGA course, Cincinnatti, Ohio, 2009
• ASAN Interventional Cardiology Course, Seoul, 2011

Division of Cardiology, Department of Internal Medicine, Faculty of Medicine , University of Indonesia,
Jakarta , Indonesia
Prof. Idrus Alwi MD, PhD, FINASIM, FACP, FACC, FESC, FAPSIC
The Role of Anticoagulant in ACS Management

Outline
Spectrum of ACS, Therapy, Risk Stratification, Target of Anticoagulant
OASIS 5, Registry Data, OASIS 8
Recommendation of Anticoagulants
Conclusion

Outline
Spectrum of ACS, Therapy, Risk Stratification, Target of Anticoagulant
OASIS 5, Registry Data, OASIS 8
Recommendation of Anticoagulants
Conclusion

The spectrum of ACS
European Heart Journal (2011) 32, 2999–3054

STEMI
1. Revascularisation
2. Anti - Thrombotic
3. Anti - Ischemia
NSTEMI
1. Anti - Ischemia
2. Anti - Thrombotic
3. Revascularisation
Therapy of Choice

It is recommended to use established risk scores for prognosis and bleeding (e.g. GRACE, CRUSADE)
European Heart Journal (2011) 32, 2999–3054

European Heart Journal (2011) 32, 2999–3054

Fondaparinux Mechanism of Action
1. Olson et al. Role of the antithrombin-binding Pentasaccharide in heparin acceleration of antithrombin-proteinase reaction
J Biol Chem 1992;267:12528-38
2. Turpie et al. A synthetic Pentasaccharide for the Prevention of deep-vein trombosis after total hip replacement.
N Engl J Med 2001;344:619-25
Thrombin
Fibrinogen
Extrinsic pathway
Intrinsicpathway
AT
Fondaparinux
XaAT
Antithrombin
Fibrin clot
Xa
Pro-thrombin
Reutilized

Outline
Spectrum of ACS, Therapy, Risk Stratification, Target of Anticoagulant
OASIS 5, Registry Data, OASIS 8
Recommendation of Anticoagulants
Conclusion

OASIS 5: An International, Multicenter, Randomized, Double-Blind, Double-Dummy
Trial in 41 Countries
1. ArixtraTM PI BPOM 4 October 2010, GDS04/IPI04 (23 January 2007).2. Salim Yusuf, et al. Comparison of Fondaparinux and Enoxaprine in Acute Coronary Syndrome.
The fifth organization to assess strategies in Acute Ischemic Syndrome investigator. N Egl J Med 2006:354:1446-76.
20,078 patients with UA/NSTEMI20,078 patients with UA/NSTEMI
Fondaparinux2.5 mg s.c. od up to 8 days
Aspirin, Clopidogrel, anti-GPIIb/IIIa, planned Cath/PCI as per local practice
Randomization
Enoxaparin1 mg/kg s.c. bid for 2-8 days
1 mg/kg s.c. od if ClCr<30mL/min
Vital status ascertained in 20,066 (99.9%) Lost to follow-up at day 9: fondaparinux: n=7 and enoxaparin: n=5

Study Objectives and OutcomesObjectives
Primary efficacy objective: To demonstrate non-inferiority of fondaparinuxcompared with enoxaparin
Primary safety objective: To determine whether fondaparinux was superior to enoxaparin in preventing major bleeding
Objectives
Primary efficacy objective: To demonstrate non-inferiority of fondaparinuxcompared with enoxaparin
Primary safety objective: To determine whether fondaparinux was superior to enoxaparin in preventing major bleeding
Outcomes (centrally adjudicated)
Primary efficacy: 1st occurrence of the composite of death, MI, or refractory ischemia (RI) up to day 9
Primary safety: Major bleeding up to day 9
Risk benefit: Death, MI, refractory ischemia, major bleeds up to day 9
Secondary: Above & each component separately at days 30 and 180
1. ArixtraTM PI BPOM 4 October 2010, GDS04/IPI04 (23 January 2007).2. Salim Yusuf, et al. Comparison of Fondaparinux and Enoxaprine in Acute Coronary Syndrome.
The fifth organization to assess strategies in Acute Ischemic Syndrome investigator. N Egl J Med 2006:354:1446-76.

Cumulative Risk through Day 9
Yusuf et al. N Engl J Med 2006;354:1464-76

Cumulative Risk through Day 180
Yusuf et al. N Engl J Med 2006;354:1464-76
Death through Day 180 Death, Myocardial Infarction, or Stroke through Day 180

Results of Subgroup Analyses of Efficacy
Yusuf et al. N Engl J Med 2006;354:1464-76
Primary Efficacy at 9 Days Major Bleeding at 9 Days

Treatments, Complications, and Outcomes among Patients Undergoing PCI within the First Eight Days after Randomization
Yusuf et al. N Engl J Med 2006;354:1464-76

Summary of OASIS 5
• Fondaparinux at a dose of 2.5 mg daily is similar to enoxaparin in the short term in preventing ischemic events among patients with acute coronary syndromes without ST-segment elevation, but it is associated with substantially less bleeding — an effect that translates into lower long-term mortality and morbidity

Brazilian Registry Data
de Matos Soeiro et al. Arq Bras Cardiol. 2016; 107(3):239-244

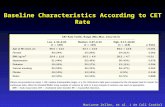
SWEDEHEART Registry
Szummer et al. JAMA. 2015;313(7):707-716

Mehta et al. J Am Coll Cardiol 2007;50:1742–51

Is fo
nd
apar
inu
x sa
fer
than
en
oxap
arin
for
pat
ient
s u
nd
ergo
ing
P
CI?
Antman EM. Nat Clin Prac Cardiovasc Med. 2007Mehta et al. J Am Coll Cardiol 2007;50:1742–51

Study Design OASIS 8
NSTEACSFonda
2.5 mg sc
AngioNo PCI
30 Day Follow-Up
Angiowith PCI R
Std Dose UFH
(85 U/kg or 60 U/kg with GP IIb/IIIa)
ACT guided*
30 Day Follow-Up
Low Dose UFH
(50 U/kg irrespective of GP IIb/IIIa) –
without ACT
30 Day Follow-Up
With at least 2 of following:
• Age>60
• elevated biomarkers
• ECG changes
Patients were not eligible if
required urgent coronary
angiography (<120 min) due
to clinical instability
Adjunctive therapy
during PCI
Double
Blind
Registry
*ACT Targets consistent with current guidelines
Coronary Angiography/PCI to be
performed within 72 hours
Jolly et al. JAMA. 2010;304(12):1339-1349

Study Outcome DefinitionsMajor Bleeding (OASIS 5)
• Fatal
• Symptomatic ICH
• Retroperitoneal hemorrhage
• Intraocular bleeding leading to significant vision loss
• Requiring surgical intervention
• Hb drop of ≥3 g/dL
• Blood transfusion of > two units RBCs
Minor Bleeding Any other significant bleeding leading to transfusion of one unit of blood or discontinuation of antithrombotic therapy.
Major Vascular Access Site Complications
• Large hematoma (≥5 cm or requiring intervention)
• Pseudoaneurysm requiring treatment
• Arterio-venous fistula
• Other vascular surgery related to the access site
Jolly et al. JAMA. 2010;304(12):1339-1349

Results
Jolly et al. JAMA. 2010;304(12):1339-1349
Death, myocardial infarction, or target vessel revascularisationMajor Bleeding

Treatment Effect for Primary Outcome
Jolly et al. JAMA. 2010;304(12):1339-1349

Treatment Effect for Death, Myocardial Infarction, or Target Vessel Revascularization
Jolly et al. JAMA. 2010;304(12):1339-1349


Outline
Spectrum of ACS, Therapy, Risk Stratification, Target of Anticoagulant
OASIS 5, Registry Data, OASIS 8
Recommendation of Anticoagulants
Conclusion

Recommendations for anticoagulants
Eur Heart J.2015

Recommendations for anticoagulants
Eur Heart J.2015

Recommendations for anticoagulants
Eur Heart J.2015

Recommendations for anticoagulants
Eur Heart J.2015

Recommendations for anticoagulants
Eur Heart J.2015

Recommendations for anticoagulants in patients with normal and impaired renal function
Eur Heart J.2015

Outline
Spectrum of ACS, Therapy, Risk Stratification, Target of Anticoagulant
OASIS 5, Registry Data, OASIS 8
Recommendation of Anticoagulants
Conclusion

In management of ACS, the efficacy and safety of antithrombotic are
primary concern
Anticoagulant options in management of UA/NSTEMI: UFH, LMWH &
Fondaparinux
Based on OASIS 5, fondaparinux is a selective factor Xa inhibitor which
offers similar efficacy with less bleeding risk compared to enoxaparin for
management UA/NSTEMI
Fondaparinux 2.5 mg SC once daily is preferable than enoxaparin as
recommended by ESC guideline for UA/NSTEMI patients
Adding UFH during PCI to fondaparinux preserves the benefits and safety
of fondaparinux (ie. reduced bleeding) while minimizing catheter thrombus
Conclusion