Antibiotics use in the ICU/CCM Board review
61
ANTIBIOTIC USE IN THE CRITICALLY ILL Michael S. Niederman, M.D. Chairman, Department of Medicine WinthropCUniversity Hospital Mineola, NY Professor of Medicine ViceCChairman, Department of Medicine SUNY at Stony Brook
-
Upload
azmachamberazmacare -
Category
Documents
-
view
21 -
download
8
description
Critical care Board review
Transcript of Antibiotics use in the ICU/CCM Board review

!!
ANTIBIOTIC(USE(IN(THE(CRITICALLY(ILL(
Michael(S.(Niederman,(M.D.(Chairman,(Department(of(Medicine(
WinthropCUniversity(Hospital(Mineola,(NY(
(Professor(of(Medicine(
ViceCChairman,(Department(of(Medicine(SUNY(at(Stony(Brook(

Presenter(Disclosures(Related(To(This(PresentaKon(
• Michael!S.!Niederman,!M.D.!– Commercial!disclosures:!!
• Honorarium!and!consul8ng:!Bayer/Nektar,!Sanofi@!Aven8s,!Pfizer,!Merck,!Cubist!
– Non@commercial!disclosure:!Advisory!board!FDA,!IDSA/ATS!HAP!Guideline!CommiJee!
– Research!Grant:!Bayer/Nektar,!Sanofi@Aven8s,!Cubist!

ObjecKves(
ALer!this!course,!you!should!be!able!to:!• Explain!mechanisms!of!ac8on!of!common!an8bio8cs!• Use!pharmacokine8cs!and!pharmacodynamics!to!op8mize!therapy!against!drug@resistant!organisms!
• Apply!principles!of!responsible!an8bio8c!use!for!the!cri8cally!ill!and!principles!of!an8microbial!stewardship!
!!

4!
MECHANISMS(OF(ACTION((
• Bactericidal:!kill!bacteria!by!inhibi8ng!cell!wall!synthesis!or!key!metabolic!func8ons!– Penicillins,!cephalosporins,!aminoglycosides,!fluroquinolones,!vancomycin,!rifampin,!daptomycin,!metronidazole!
• Bacteriosta8c:!inhibit!growth!,!do!not!interfere!with!cell!wall!synthesis,!rely!on!host!defenses!to!eliminate!bacteria;!relevant!if!neutropenic!– Macrolides,!tetracycline,!sulfa!drugs,!chloramphenicol,linezolid,!!clindamycin!

MIC(and(MBC(
• MIC:!concentra8on!of!an8bio8c!that!inhibits!the!growth!of!90%!of!a!standard!sized!inoculum,!no!visible!growth!
• MBC:!minimum!concentra8on!killing!99.9%!of!a!standard!sized!inoculm!
• MIC!is!used!to!define!“sensi8vity”!of!an!organism!to!a!specific!an8bio8c,!but!considers!only!the!serum!concentra8on!and!NOT!the!concentra8on!at!the!site!of!infec8on.!!

!!
In(treaKng(severe(VAP(with(a(carbapenem,(efficacy(is(improved(if(A.!the!serum!concentra8on!exceeds!the!MIC!for!at!least!40%!of!the!dosing!interval!B.!the!area!under!the!concentra8on!8me!curve!divided!by!MIC!is!at!least!125!C.!!Dosing!is!once!daily!D.!dosing!is!given!by!con8nuous!infusion!E.!it!is!never!used!as!monotherapy!
Salma Akram

!!!
In(treaKng(severe(VAP(with(a(carbapenem,(efficacy(is(improved(if(A.!the!serum!concentra8on!exceeds!the!MIC!for!at!least!40%!of!the!dosing!interval!B.!the!area!under!the!concentra8on!8me!curve!divided!by!MIC!is!at!least!125!C.!!Dosing!is!once!daily!D.!dosing!is!given!by!con8nuous!infusion!E.!it!is!never!used!as!monotherapy!

!!!!!!!!!!!!!!
Cmax (peak)
Time above MIC
Half life
Time
Ant
ibio
tic
seru
m c
once
ntra
tion
MIC
AUC
Cmin (trough)
AUIC24= AUC24
MIC18
PharmacokineKc/Pharmacodynamic(Principles(

!!!!!
PHARMACODYNAMIC(CONSIDERATIONS(• Bactericidal!in!a!concentra8on@dependent!fashion:!aminoglycosides,!quinolones,!ketolides,!daptomycin!
• Bactericidal!in!a!8me@dependent!fashion!(if!>!MIC!for!at!least!40%!of!the!dosing!interval)!:!beta@lactams,!carbapenems,!aztreonam,!macrolides,!linezolid!!
• Time@dependent!with!prolonged!and!persistent!killing:!clindamycin,!vancomycin,!azithromycin,!tetracyclines.!(AUIC!and!trough!may!maJer!in!addi8on!to!8me!>!MIC)!
• Prolonged!PAE!against!gram@nega8ves:!aminoglycosides,!quinolones,!tetracyclines,!rifampin!
• LiJle!or!no!PAE!for!gram@nega8ves:!beta@lactams!(except!penems)!

No(Benefit(From(Prolonged(Infusion(• Before!and!aLer!comparison!of!two!8me!periods!with!!30!minute!infusion!vs.!3!hour!infusion!!of!pip/taz,!cefepime,!carbapenem!
• Treatment!success!the!same!in!both!groups!(56%!vs!51%).!Same!mortality!!– Arnold!!HM!et!al.!Ann!Pharmacother!2013.!!
!!
Salma Akram

11
% o
f pat
ient
s re
mai
ning
cul
ture
-pos
itive
Days of treatment
0 2 4 6 8 10 12 14 0
100
75
50
25 AUIC 125-250
AUIC > 250
AUIC < 125
Ciprofloxacin: Eradication vs AUIC
Forrest A, Antimicrobial Agents Chemother 37:1073–1081, 1993.

!!!!!!!!The(following(anKbioKcs(penetrate(well(into(respiratory(secreKons(except(
A.!tetracycline!B.!erythromycin!C.!ciprofloxacin!D.!clindamycin!E.!vancomycin!
Salma Akram

!!
The(following(anKbioKcs(penetrate(well(into(respiratory(secreKons(except(A.!tetracycline!B.!erythromycin!C.!ciprofloxacin!D.!clindamycin!E.!vancomycin!

!!!!
PENETRATION((
• INFLAMMATION!INDEPENDENT!(LIPID!SOLUBLE)!GOOD!PENETRATION!– Chloramphenicol!– Macrolides!– Tetracyclines!– Quinolones!– Trimethoprim/sulfa!– Ketolides!– Linezolid!
• INFLAMMATION!DEPENDENT!(POORLY!LIPID!SOLUBLE)!POOR!PENETRATION!– Penicillins!– Cephalosporins!– Aminoglycosides!– Carbapenems!– Monbactams!– Vancomycin!

Factors(AffecKng(Clinical(Success(In(Pneumonia(Therapy(
!!
Lippman(et(al.(Curr(Opin(Infect(Dis(2013,(in(press(

FACTORS(AFFECTING(ANTIBIOTIC(CONCENTRATIONS(IN(THE(LUNG(
• Penetra8on,!Protein!Binding,!Volume!of!Distribu8on!(Vd),!Clearance!– OLen!enhanced!renal!clearance!(beta@lactams)!in!hyperdynamic!sep8c!pa8ents!(ARC,!augmented!renal!clearance)!
– Volume!of!distribu8on!>!3L!means!concentra8on!outside!of!plasma!• Lipophilic!drugs!have!a!high!Vd!• Hydrophilic!drugs!expand!their!Vd!with!sepsis!and!“leaky!capillaries”!(can!underdose)!
• Obesity:!If!use!IBW!can!underdose!(esp!lipophilic!drugs).!Generally!use!TBW,!!BUT!if!calculate!dose!on!TBW!can(overdose(hydrophilic!drugs!(extracellular!water!does!not!expand!as!much).!
– Free!drug!is!ac8ve!and!thus!with!low!serum!proteins,!may!increase!BOTH!Vd!and!Clearance!
!!
Salma Akram

BETACLACTAMS(• All!with!beta@lactam!ring:!penicillins,!cephalosporins,!monobactams,!
carbapenems!• Interfere!wiJhe!synthesis!of!bacterial!cell!wall!pep8doglycans!by!binding!
to!PBPs!• Penicillins:!an8@Staphylococcal,!an8@Pseudomonal!
– Can!also!extend!spectrum!by!combining!with!beta@lactamase!inhibitors!
• Cephalosporins:!First!to!fourth!genera8on!with!atrend!to!more!gram@posi8ve!coverage!with!earlier!agents,!more!specialized!with!later!agents!
• Carbapenems!(Imipenem,!meropenem,!doripenem):!the!broadest!spectrum!agents!;!resistance!can!emerge!during!monotherapy!vs.!P.!aeruginosa!
• Monobactam!(Aztreonam):!gram@nega8ve!ac8vity!only,!no!cross!reac8vity!to!PCN!allergy!
Salma Akram
Salma Akram

!!
QUINOLONES(• Interfere(with(DNA(gyrase(and(lead(to(cell(lysis(• Earlier(agents(marginal(vs.(gram(posiKves:(
ofloxacin,(ciprofloxacin(• Ciprofloxacin(is(most(acKve(against(P.(aeruginosa(
– Levofloxacin(750(mg(acKve(vs.(P.(aeruginosa(• Newer(agents(with(enhanced(gram(–posiKve(acKvity(
– Oral/(or(IV(agents:(Gemifloxacin((O)(>(Moxifloxacin(O,IV)(>(Levofloxacin((O,IV)(
• Moxifloxacin(with(anaerobic(acKvity(• Graveyard:(Temafloxacin,(trovafloxacin,(sparfloxacin,(
grepafloxacin,(gaKfloxacin(
Salma Akram

!!
Quinolone(therapy(for(pneumococci(
A.!is!never!associated!with!an8bio8c!resistance!B.!is!more!likely!to!be!effec8ve!with!levofloxacin!than!with!moxifloxacin!C.!is!adequate!by!itself!for!ICU!admiJed!CAP!D.!can!have!efficacy!predicted!by!examining!the!peak!serum!concentra8on!rela8ve!to!the!MIC!of!the!target!organism!E.!is!equally!effec8ve!for!all!quinolones!
Salma Akram

!!
Quinolone(therapy(for(pneumococci(
A.!is!never!associated!with!an8bio8c!resistance!B.!is!more!likely!to!be!effec8ve!with!levofloxacin!than!with!moxifloxacin!C.!is!adequate!by!itself!for!ICU!admiJed!CAP!D.!can!have!efficacy!predicted!by!examining!the!peak!serum!concentra8on!rela8ve!to!the!MIC!of!the!target!organism!E.!is!equally!effec8ve!for!all!quinolones!

!!
Are(Quinolones(The(Therapy(of(Choice(for(Legionella(?(
• 6!clinical!trials!of!levofloxacin!for!CAP!included!75!with!Legionella.!– 500!mg!x!7@14!days;!750!mg!x!5!days!– 93.6%!success!in!mild@moderate,!91.6%!in!severe!– Yu!et!al:!Chest!2004;!125:2135@2139.!
• Pooled!data!from!8!trials!of!moxifloxacin:!4!p.o.,!4!IV/oral!– Moxi!400!mg/day!!for!7@14!– Success!:!95.2%!vs.!79.3%!,!moxi!vs.!comparators!– Garau!J!et!al,!J!Chemother!2010;!22:264@6!
Salma Akram
Salma Akram

!!!!Should(We(NOT(Use(Quinolones(For(A(First(ICU(InfecKon?((
• 239!ICU!pa8ents!with!no!prior!an8bio8c!exposure!
• Mul8variate!analysis!of!risks!for!acquiring!MDR!pathogens!– 77!pa8ents!with!ICU!acquired!MDR!organisms!(50!were!infec8on)!• Mul8variate!risks!for!MDR!acquisi8on:!FQ!use!(OR!3.3),!dura8on!an8bio8cs!(OR!1.1).!
• Maybe!reserve!quinolones!for!a!second!course!of!ICU!infec8on!
0
5
10
15
20
25
30
35
40
%MDR %MRSA %ESBL
CaseControl
Nseir(et(al.(Crit(Care(Med(2005;(33:283((Niederman.(Crit(Care(Med(2005;(33:443.(
Salma Akram

Empiric(Fluoroquinolone(Therapy(of(Severe(CAP(in(a(TB(Endemic(Area(
• 77!cases!TB!to!ICU!w/i!1!week!of!admit,!in!Taiwan,!treated!ini8ally!as!severe!CAP!– Empiric!FQ!in!43!
• Empiric!FQ!with!lower!100!day!mortality!(40!vs.!68%,!p=0.02).!OR!death=!0.36,!p<0.01.!!– 65%!!became!culture!nega8ve!
with!FQ!alone;!no!delay!in!star8ng!TB!rx!in!!empiric!FQ!group!
• Tseng!YT,!et!al.!Crit!Care!2012;!16:!R207!
!!
Salma Akram

!!!
CombinaKon(Regimens(Must(Account(For(Local(Microbiology(
• 111!pa8ents!with!HAP!• No!single!beta@lactam!more!than!80%!effec8ve,!adding!cipro!of!liJle!incremental!benefit!– Amikacin!more!ac8ve!vs.!gram!–nega8ves!than!quinolones!
• Beardsley!JR,!et!al.!Chest!2006;!130:!787@793.!
Salma Akram
Quinolones ate not appropriate second agent for ICU pneumonia due to resistant

AMINOGLYCOSIDES(• Bind!to!the!30!S!ribosomal!subunit!of!bacteria!and!
interfere!with!protein!synthesis!• Gram!–!nega8ve!spectrum!,!including!P.!aeruginosa!• Synergy!when!combined!with!an8@!Pseudomonal!beta@
lactams!• Amikacin!is!generally!the!most!ac8ve!since!it!is!less!
suscep8ble!to!enzyma8c!inac8va8on.!Tobramycin!more!ac8ve!than!gentamicin.!
• Poor!respiratory!penetra8on,!inac8ve!at!acid!pH,!nephrotoxic!
• Once!daily!dosing!possible!
Salma Akram
better second line agent in ICU pneumonia

!!!
Pharmacodynamics(of(Aminoglycosides((
• Concentra8on@dependent!bacterial!killing;!probably!best!given!once!daily!(?!Less!toxic,!more!effec8ve)!
• Peak/MIC!and!AUC/MIC!(AUIC)!correlate!with!outcome;!AUIC!target!for!good!result,!is!>!125.!
• Peak/MIC!ra8o!should!be!8!to!10@fold!for!a!clinical!response!of!!>!90%!and!AUIC!at!least!125.!
• Peak/MIC!ra8o!of!8@10!and!AUICs!>!100!can!also!reduce!the!rate!of!emergence!of!resistant!mutants!during!therapy!
• AUICs!of!!250!are!capable!of!killing!bacterial!pathogens!on!day!1!of!therapy!

!!!!!!
Use(of(an(Aminoglycoside(Improves(VAP(Mortality((
• Prospec8ve!observa8onal!study!of!156!VAP!pa8ents!!
• Lower!mortality!if!ini8al!therapy!with!a!beta@lactam/BLI!and!also!a!trend!with!an!aminoglycoside.!!– Recommend!to!consider!using!aminoglycosides!in!combina8on!as!empiric!therapy,!IN!SPITE!OF!POOR!AG!PENETRATION!!
• Fowler!RA,!et!al.!Chest!2003;!123:835@844!
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
BL/BLI AG FQ Ceph
HR ofDeath
p=<0.01(
P=0.08(
P>(0.2(

!!
Tigecycline:(?(For(Acinetobacter(• Approved!for!SSSTi!(and!intra@abdominal!infec8ons)!– S8ll!no!compara8ve!data!on!severe,!bacteremic!infec8ons!(only!‘complicated’)!
– Not!approved!for!nosocomial!pneumonia!– Low!serum!concentra8ons:!empiric!therapy!for!less!severe!infec8ons,!where!MRSA!and!GNB!(Acinetobacter,!but!NOT!Pseudomonas!aeruginosa)!
Salma Akram
Salma Akram
carbepenams are the agents of choice.

Tigecycline(Vs.(Imipenem(For(HAP/VAP(• 945!pa8ents!,!randomized,!double@blind!,!mul8center!study.!!
– Tigecycline!100!mg,!then!50!mg!q12!h!with!op8onal!ceLazidime!– Imipenem!500@1000!mg!!q8!h!with!op8onal!vancomycin!
• Tigecycline!non@inferior!!for!!clinical!efficacy!– Tigecycline!significantly!worse!in!VAP!pa8ents!in!the!CE!popula8on!– Mean!AUC!15%!lower!in!VAP!than!non@VAP,!AUC/MIC!!was!60%!lower!
• Acinetobacter+baumanii!VAP:!Clinical!response!57%!Tigecycline,!95%!Imipenem!• Friere!AT,!et!al.!Diagnos8c!Microbiol!Infect!Dis!2010;!68:!140@51!

CombinaKon(Therapy(for(Acinetobacter(VAP(
• 33!pa8ents!with!carbapenem@resistant!Acinetobacter!– 19!with!VAP!
• 31!got!8gecycline!as!!combina8on!therapy!– 21!clinical!success!with!combina8on!therapy!
– Guner!R,!et!al.!Infec8on!2011;!39:515@518!!
!!

!!
Polymyxins(for(Acinetobacter(VAP(• Two!agents!have!been!used!:!Polymyxin!B!and!E!(colis8n)!
– IV!and!aerosolized!therapy!of!MDR!gram@nega8ves!• Binds!to!gram@nega8ve!outer!cell!membrane!leading!to!permeability!change!and!cell!death!
• Bactericidal!in!concentra8on@dependent!fashion!• Polymyxin!B:!1!mg=!10,000!IU!• Colis8n!2.5@5!mg/kg!per!day!in!2@4!divided!doses!
– 1!mg=!12,500U;!80!mg=!1!Million!U!– Reduce!dose!to!160!mg!(2!MU)!q!12,!24!and!36!h!with!renal!dysfunc8on!
• Toxicity:!renal!(ATN),!neurotoxicity!(neuromuscular!block,!confusion,!ataxia,!visual!disturbances,!dizziness)!
• Falagas!and!Kasiakou.!Clin!Infect!Dis!!2005;!40!:!1333@41!

Therapy(of(MRSA(infecKon((A.!Is!more!effec8ve!using!an!an8@Staphylococcal!penicillin!than!using!linezolid!B.!Can!be!accomplished!with!either!vancomycin!or!linezolid!C.!Can!be!accomplished!with!daptomycin,!regardless!of!the!site!of!infec8on!D.!!Will!likely!be!effec8ve!if!the!!trough!serum!concentra8on!is!10!mg/L!for!an!!organism!with!an!!MIC!>!1!mg/L!!E.!Can!be!done!by!maximizing!vancomycin!dose,!which!has!no!risk!of!nephrotoxicity!
!!

Therapy(of(MRSA(infecKon((A.!Is!more!effec8ve!using!an!an8@Staphylococcal!penicillin!than!using!linezolid!B.!Can!be!accomplished!with!either!vancomycin!or!linezolid!C.!Can!be!accomplished!with!daptomycin,!regardless!of!the!site!of!infec8on!D.!!Will!likely!be!effec8ve!if!the!!trough!serum!concentra8on!is!10!mg/L!for!an!!organism!with!an!!MIC!>!1!mg/L!!E.!Can!be!done!by!maximizing!vancomycin!dose,!which!has!no!risk!of!nephrotoxicity!
!!

Vancomycin(Resistance(and(Increased(Mortality(in(MRSA(HAP(
• 163!pa8ents!with!MRSA!HAP,!VAP!or!HCAP!– 73%!with!MIC!of!at!least!1.5!mcg/mL!
• OR!of!death!of!3.7!for!each!increase!of!1mcg/mL!in!vanc!MIC;!OR=2.97!aLer!propensity!adjustment!
– 79%!vanco!trough!>!10,!45%!at!least!15!mcg/mL!
– Haque!NZ!et!al.!Chest!2010;!138:1356@62!

Vancomycin(Nephrotoxicity(Increases(as(Trough(Levels(Are(Increased(
• Retrospec8ve!study!0f!166!pa8ents:!vancomycin!for!>!48!hours,!no!vasopressors!or!contrast!dye,!baseline!Cr!<!2.0!mg/dL!– 21!with!nephrotoxicity:!increase!in!Cr!by!0.5!or!by!>!50%!(whichever!greater)!
• In!mul8variate!model,!only!trough!level!correlated!with!toxicity.!!– Lodise!et!al.!CID!2009;!49:!507@14!

Vancomycin(Trough(ConcentraKons(Predict(Efficacy(and(Toxicity((
• 31!pa8ents!with!MRSA!pneumonia!!
• Nephrotoxicity:!increase!Cr!by!0.5!mg/dl!or!50%!from!baseline!
• Rela8onship!of!trough/MIC!with!success,!and!trough!levels!with!toxicity!– Suzuki!Y!et!al.!Chemotherapy!2012;!58:308@12!
Efficacy
Toxicity

!!
AlternaKves(to(Vancomycin(against(MRSA(
• Streptogramins!(quinupris8n/dalfopris8n)!• Oxazolidinones!(linezolid)!!• Glycopep8des!(teicoplanin)!• Daptomycin:!NOT!for!pneumonia!• Telavancin:!Just!approved!!for!VAP!due!to!MRSA!and!MSSA!
• CeLaroline:!4th!genera8on!cephalosporin!ac8ve!vs.!MRSA.!Approved!for!CAP!(not!MRSA)!
Salma Akram

!!
Daptomycin(
• Good!gram@posi8ve!drug!(including!MRSA!and!VRE)!– Bactericidal!drug!– Cyclic!lipopep8de!!
• Disrupts!cell!membrane!func8on!• Resistance!uncommon;!mechanism!unknown!• Not!used!for!pneumonia!due!to!low!respiratory!!tract!concentra8ons!and!inac8va8on!by!surfactant!– Use!in!endocardi8s,!SSTI,!bacteremia!
• Adverse!effects!–!reversible!myopathy!
Salma Akram

Vancomycin(vs.(Linezolid(• Vancomycin.!Glycopep8de,!disrupts!cell!wall/pep8doglycan!synthesis!
– Pros:!low!resistance!rates,!years!of!experience!– Cons:!slow!increase!in!MICs!(w/i!“sensi8ve”!range);!poor!lung!penetra8on!(12%!serum!levels);!slowly!bactericidal;!nephrotoxicity!
• May!overcome!poor!penetra8on!by!synergy!with!rifampin!• Linezolid(
– Pros:!good!lung!penetra8on;!IV/oral!available;!high!bioavailability!orally;!no!renal!dose!adjustment!
– Cons:!thrombocytopenia,!op8c!neuri8s,!lac8c!acidosis!(prolonged!therapy);!drug!interac8ons!(serotonin!syndrome)!
• Pletz!MW!,!et!al.!Eur!J!Med!Res!2010;!15:507@13!
Salma Akram

40!Linezolid(ConcentraKons(in(Serum(and(ELF(of(CriKcally(Ill(VAP(PaKents(
• 16!cri8cally!ill!VAP!pa8ents!studied!at!steady!state!– All!with!late!onset!VAP!– 12!with!organisms:!3!
MRSA,!1!MSSA,!8!Enteric!gram!nega8ves!
• Serum!and!ELF!concentra8ons!aLer!2!days!of!therapy!
• Blood!at!10,!20!30!and!45!min!and!1,2,4,8,12!hours!aLer!infusion!
• BAL!1!and!12!hours!aLer!infusion!• Similar!levels!in!serum!and!ELF!
– Range!of!Peak!penetra8on:!34@188%!
– Range!of!Trough!penetra8on:!28@220%!
• Boselli!et!al.!Crit!Care!Med!2005;!33;!1529@1533.!

Linezolid(Vs.(GlycopepKdes(for(MRSA(NP(• Linezolid!vs.!glycopep8des!in!6!!trials!with!639!pa8ents!with!MRSA!proven!!• Clinical!success!with!!documented!MRSA!with!OR=1.23.!p=0.009!(from!0.09)!!
by!adding!Wunderink!2012!data!!• Thamlikitkul!V,!Tongsai!S.!Chest!2012;!142:!269!
Salma Akram
Vancomycin

!!
Aerosolized(AnKbioKcs(
• Target!delivery!to!site!of!infec8on!• Increase!concentra8ons!in!tracheobronchial!secre8ons!compared!to!parenteral!use!(esp.!aminoglycosides)!
• Avoid!exposure!to!systemic!an8bio8cs!• Reduce!poten8al!for!an8bio8c!resistance!• Reduce!systemic!side!effects!

How(To(OpKmize(Aerosol(Delivery(of(AnKbioKcs(in(VenKlated(PaKents(
• Ultrasonic!or!vibra8ng!plate!nebulizers!preferred!to!jet!nebulizers.!BUT!ultrasonic!nebs!may!heat!the!an8bio8c.!!– Vibra8ng!plates!can!synchronize!with!inspira8on!and!up!to!60%!of!reservoir!
dose!deposits!in!lung.!Par8cle!size!<!5!microns!– Place!!vibra8ng!plate!in!inspiratory!limb!before!the!!Y!connector!and!ETT!8p!
• Nebulized!dose=!systemic!IV!dose!+!extrapulmonary!deposi8on!(tubing,!expiratory!filter)!
• Limit!inspiratory!flow!turbulence!– Controlled!mode!ven8la8on!(NOT!assist,!and!may!need!seda8on),!!VT!of!7@9!
ml/kg,!constant!inspiratory!flow,!MV!<!6L/min,!R=12,!I/E!!ra8o!of!1:1,!end!inspir!pause!of!20%!of!the!duty!cycle!
• Remove!HME!filter!,!add!humidifica8on!if!delivery!8me!>!30!min!
Rouby!JJ,!et!al.!Anesthesiology!2012;!117:1364@1380!

AdjuncKve(Aerosolized(Amikacin(As(Part(of(CombinaKon(Therapy(of(MDR(GramCNegaKves?((• Prospec8ve!randomized,!controlled!trial!of!ADJUNCTIVE!aerosolized!amikacin!
400!mg!BID!vs.!QD!vs.!placebo,!all!with!adjunc8ve!systemic!an8bio8cs!• 49.1%!with!P.!aeruginosa!or!Acinetobacter!baumanii.!!• Use!of!proprietary!Pulmonary!Dose!Delivery!System!(Nektar)!• Up!to!day!7:!!an8bio8cs!were!added!(escalated)!in!14%,!38%!and!58%!of!the!
pa8ents!in!the!q12!h,!q24h,!and!placebo!groups!,!The!remainder!in!each!group!had!an8bio8cs!!either!stopped!or!subtracted!(de@escalated).!!
• Niederman(MS,(et(al.((Intensive(Care(Medicine(2012;((38:(263C271.(((
End=!Mean!of!7!days!

!!
THERAPY(PRINCIPLES(AND(DOSING(FOR(VAP(• Appropriate:!Matching!an8bio8c!sensi8vi8es!of!the!organism!to!the!an8bio8c!used.!!
• Adequate:!includes!appropriate!PLUS!correct!dose,!penetra8on!to!site!of!infec8on,!correct!route!and!combina8on!therapy!(if!needed)!– Need!proper!an8bio8c!dosing!(normal!renal!func8on)!
• Ciprofloxacin:!400!mg!q8h;!Levofloxacin!750!mg!qD!• Imipenem!1!gm!q!8H!or!500!mg!q!6h;Meropenem!1!gm!q!6@8!h!• Piperacillin/Tazobactam!4.5!gm!q!6h!• Cefepime!2!gm!q!8@12h!• CeLazidime!2!gm!q!8h!• Gentamicin!or!Tobramycin!7!mg/kg!/!day!or!Amikacin!20!mg/kg/
day!• Linezolid!600!mg!!q!12!h!• Vancomycin!15!mg/kg!q12h!
Salma Akram
Salma Akram
Salma Akram

!!
AnKCPseudomonal(AnKbioKcs(
• Aminoglycosides:!gentamicin,!tobramycin,!amikacin!• Quinolones:!ciprofloxacin,!high!dose!levofloxacin!!• Beta!lactams!
– An8@pseudomonal!penicillins!– Cephalosporins:!ceLazidime,!cefepime,!!– Imipenem,!meropenem,!doripenem!– Aztreonam!– Beta@lactam/beta@lactamase!inhibitor!combina8ons:!piperacillin/tazobactam,!8carcillin/clavulanate!

!!Monotherapy(of(nosocomial(pneumonia(in(venKlated(paKents(can(be(done(in(the(absence(of(highly(resistant(pathogens(with(all(of(the(following(except(
A.!ciprofloxacin!B.!imipenem!C.!cefepime!D.!piperacillin/tazobactam!E.!gentamicin!
Salma Akram

!!Monotherapy(of(nosocomial(pneumonia(in(venKlated(paKents(can(be(done(in(the(absence(of(highly(resistant(pathogens(with(all(of(the(following(except(
A.!ciprofloxacin!B.!imipenem!C.!cefepime!D.!piperacillin/tazobactam!E.!gentamicin!

!!
Why(EMPIRIC(CombinaKon(Therapy(in(VAP?((• Combina8on!therapy!does!NOT!!
– Improve!mortality!overall!– Prevent!the!emergence!of!resistance!during!therapy!
• BUT!combina8on!therapy!could!reduce!mortality!IF!– It!increases!the!chance!of!appropriate!therapy!
• Broader!spectrum!coverage!than!with!one!drug!alone!(gram!nega8ve!and!gram@posi8ve)!
• Mixed!infec8on:!cover!gram@posi8ves!and!gram@nega8ves!
– It!is!used!!in!Pseudomonal!bacteremia!– Pa8ent!is!sep8c:!More!rapid!bacterial!killing!
Salma Akram
Salma Akram
Salma Akram

!!
GENERAL(ISSUES(FOR((ANTIBIOTIC(USE(IN(THE(CRITICALLY(ILL((• General!Considera8ons!
– Know!local!microbiology!– Site!of!infec8on!– Pa8ent!risk!factors:!recent!hospitaliza8on,!prolonged!hospitaliza8on,!recent!an8bio8c!use,!immune!status,!origin!(community,!nursing!home,!hospital)!
– Emphasis!on!proper!dosing!– Specific!an8bio8c!issues!
• Avoid!dual!beta@lactam!therapy!!• Limit!use!of!third!genera8on!cephalosporins!• Consider!sequence!of!therapy:!?!Limit!quinolones!to!second!episode!of!ICU!infec8on!

!!
OTHER((PRINCIPLES(OF(ANTIBIOTIC(USE(IN(THE(CRITICALLY(ILL((• Limited!need!for!combina8on!therapy!
– Bacteremia,!neutropenia,!broad!spectrum!coverage!• Consider!5!day!aminoglycoside!therapy!in!combina8on!with!a!
beta@lactam!when!trea8ng!P.!aeruginosa!• Use!an!empiric!therapy!regimen!that!includes!agents!different!
from!what!the!pa8ent!has!recently!received!!• Re@evaluate!pa8ent!during!therapy!!
– Shorten!dura8on!of!therapy!– Stop!therapy!in!some!– Consider!aerosolized!therapy!as!an!adjunct!to!reduce!the!dura8on!of!therapy!
• Consider!aerosolized!an8bio8cs!as!adjunc8ve!therapy!for!VAP!with!MDR!pathogens!

!!
AnKbioKc(resistance(in(the(ICU(
A.!Is!commonly!due!to!the!presence!of!ESBL’s!among!S.!aureus!B.!Makes!appropriate!empiric!therapy!less!likely!C.!Mandates!never!using!vancomycin!for!empiric!therapy!of!VAP!D.!Can!be!prevented!by!regular!use!of!an8bio8c!rota8on!E.!Can!be!eliminated!by!prohibi8ng!the!use!of!an8bio8cs!such!as!the!third!genera8on!cephalosporins!
Salma Akram

!!
AnKbioKc(resistance(in(the(ICU(
A.!Is!commonly!due!to!the!presence!of!ESBL’s!among!S.!aureus!B.!Makes!appropriate!empiric!therapy!less!likely!C.!Mandates!never!using!vancomycin!for!empiric!therapy!of!VAP!D.!Can!be!prevented!by!regular!use!of!an8bio8c!rota8on!E.!Can!be!eliminated!by!prohibi8ng!the!use!of!an8bio8cs!such!as!the!third!genera8on!cephalosporins!

Increasingly(Common((MDR(Pathogens((not(all(causing(pneumonia)(
• ESKAPE!Pathogens!needing!beJer!therapies!than!currently!available!– E.+faecium+(VRE)!– S.+aureus+(MRSA)!– Klebsiella!spp.!and!E.+coli+with!ESBL’s!and!carbapenemases!(KPC’s)!
– Acinetobacter+– Pseudomonas+aeruginosa+with!mul8@drug!resistance!– Enterobacter!spp.!!
• Boucher!HW,!et!al.!CID!2009;!48:1@12!!

!!
Grayson(ML,(Eliopoulos(GM.(Semin(Respir(Infect.(1990;5:204C214.(
Mechanisms(of((AnKmicrobial(Resistance(
• Decreased!permeability!of!microbial!cell!wall!– altered!porin!channels!– primary!mechanism!of!gram@nega8ves!to!!β@lactamases!
• An8bio8c!inac8va8on!– beta@lactamases,!AG!inac8va8ng!enzymes,!other!inac8va8ng!enzymes!
• Altera8on!of!an8bio8c!target!site!– PBP,!DNA!gyrase,!RNA!polymerase!
• Ac8ve!efflux!of!the!an8bio8c!

!!
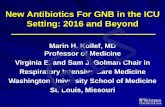
Mechanisms(of(Resistance:(Pseudomonas*and*Efflux*Pumps*
!Adapted!from!Livermore!DM.!Clin+Infect+Dis.+2002;34:634@640.
βClactams(Enter(Thru(
Porin(Channels Meropenem(is(pumped(out(while(imipenem(is(not(Efflux(System(
Exit(Portal((OprM)
Outer(Membrane
Periplasm Linker(Lipoprotein((Mex(A)
Cytoplasmic(Membrane
Efflux(System(Pump((Mex(B)
Porin

!!!!Risks(for(ESBL(Producing(Organisms(and(Appropriate(Therapy(
• Prospec8ve!observa8onal!study!of!455!episodes!of!K.!pneumoniae!bacteremia!(253!nosocomial)!in!12!hospitals!– 30.8%!nosocomial,!43.5%!in!ICU!with!ESBL’s!– Risks!for!ESBL’s:!previous!an8bio8c!rx.!(>2!days!in!last!14!days)!with!B@lactam!containing!oxyimino!group!(OR=!3.9).!No!risk!with!cefepime,!carbapenem,!quinolone,!aminoglycoside.!Other!risks:!TPN,!renal!failure,!burns.!!
Paterson!et!al:!Ann!Intern!Med!2004;!140:26@32.!

!!
AnKbioKc(Therapy(in(the(Presence(of(an(ESBLCproducing(Organism(
• Carbapenem!use!associated!with!significantly!lower!14@day!mortality!due!to!ESBL@producing!K+pneumoniae!bacteremia!
• Carbapenem!monotherapy!superior!to!that!of!quinolone!or!non@carbapenem!β@lactams!
• Use!of!a!carbapenem!≤5!days!onset!of!bacteremia!due!to!ESBL@producing!organism!associated!with!significantly!lower!mortality!!
Paterson(DL(et(al.(Clin*Infect*Dis.(2004;39:31C37.(
0 10 20 30 40 50 60 70 80 90
100
% M
orta
lity
BLIC=β@lactam/β@lactamase!inhibitor!combina8on!AMG=aminoglycoside!No!Abx=no!an8bio8cs!

!!The(Root(of(The(Problem(Is(Using(Too(Many(AnKbioKcs.(Is(RestricKon(the(Answer??(

!!
AnKmicrobial(Stewardship(• Mul8disciplinary!approach:!ID,!pharmacy,!microbiology,!epidemilogy,!!(!CRITICAL(CARE:((NOT(MENTIONED)!• 2!CORE!STRATEGIES!
– Prospec8ve!audit!with!interven8on!and!feedback!(!A@I)!– Formulary!restric8on!and!preauthoriza8on!to!control!resistance!(B@II)!
• Supplemental!strategies!– Educa8on!– Guidelines!with!local!microbiology!(A@I)!– An8microbial!cycling!(C@II)!– An8bio8c!order!forms!(B!II),!Combina8on!therapy!!(C@II)!– De@escala8on!(A@II)!– Dose!op8miza8on!(A@II)!– IV!to!oral!conversion!(A@III)!
• Dellit!TH,!et!al.!CID!2007;!44:!159@77!

Summary(of(Key(Points(• Drugs!that!kill!in!a!concentra8on!dependent!fashion!need!to!have!Peak/MIC!
ra8o!or!AUIC!op8mized:!aminoglycosides,!quinolones.!Once!daily!dosing.!!• Drugs!that!kill!in!a!8me!dependent!fashion!need!to!have!serum!concentra8on!
above!the!MIC!of!the!target!organism!for!at!least!40%!of!the!dosing!interval:!beta@lactams,!cephalosporins,!carbapenems.!Prolonged!or!con8nuous!infusion.!!
• Limita8ons!of!older!agents:!quinolones!vs.!P.+aeruginosa,!quinolones!for!VAP,!vancomycin!vs.!MRSA!with!MIC!>!1!mcg/ml!
• Dis8nguish!appropriate!from!adequate!therapy!• Benefits!of!combina8on!therapy:!empiric!rx!of!MDR!pathogens,!bacteremic!P.!
aeruginosa,!sep8c!shock!• ESBL!producers:!induced!by!third!gen!cephs,!best!rx!is!carbapenem!• An8microbial!stewardship:!de@escala8on,!local!protocols!for!therapy,!dose!
op8miza8on,!NOT!restricted!access!to!an8bio8cs!
!!