Antibiotics in icu
61
DR MAGED ABULMAGD,MD,EDIC CONSULTANT INTENSIVIST, EBGH ANTIBIOTICS IN ICU ANTIBIOTICS IN ICU
-
Upload
maged-abulmagd -
Category
Healthcare
-
view
74 -
download
4
Transcript of Antibiotics in icu

DR MAGED ABULMAGD,MD,EDICCONSULTANT INTENSIVIST, EBGH
ANTIBIOTICS IN ICUANTIBIOTICS IN ICU
Antibiotics are amongst the most commonly Antibiotics are amongst the most commonly used therapies in critical careused therapies in critical care
Optimising antibiotic use improves patient Optimising antibiotic use improves patient outcomesoutcomes
Optimising antibiotic use should minimise Optimising antibiotic use should minimise pressures on emerging antibiotic resistancepressures on emerging antibiotic resistance
Is antibiotic stewardship the answer?Is antibiotic stewardship the answer?

Stewardship “…the careful and responsible management of something entrusted to one's care Antimicrobial Stewardship
Healthcare institutional program to ensure appropriate antimicrobial usePrimary goal optimize clinical outcome while minimizing unintended consequenceSecondary reduce healthcare costs without adversely impacting quality of care
Antimicrobial Stewardship-- “Antimicrobial Management
Team”

Value of Stewardship Programs
Effective programs can be financially self supporting and improve patient care
Comprehensive programs have consistently demonstrated a decrease in antimicrobial use
51/66 (77%) studies of interventions to improve antibiotic use in hospitals had positive results
Davey P et al. Cochrane Database of Syst Rev 2005CID 2007;44:159-77.

Principles of antibiotic prescriptionPrinciples of antibiotic prescription
Right antibioticRight antibiotic guidelinesguidelines alert antibiotics alert antibiotics audit audit drug bug mismatchesdrug bug mismatches inappropriate antibiotics (dual anaerobic cover etc)inappropriate antibiotics (dual anaerobic cover etc) Right doseRight dose dose optimisationdose optimisation iv to oral switchiv to oral switch Right timeRight time golden hour of sepsisgolden hour of sepsis Right duration Right duration de escalationde escalation

Inappropriate Antimicrobial Use is Common
Antimicrobials account for up to 30% of hospital pharmacy budgetsAs many as 50% of antimicrobial regimens are considered “inappropriate”Wrong drug, route, interval, frequency, duration
Inappropriate use is associated with:Increased morbidity and mortalityIncreased length of stay (LOS)Increased adverse events and antimicrobial resistanceIncreased costs

33%32%
16%
10%
0%
5%
10%
15%
20%
25%
30%
35%
REASON UNNECESSARY
Dur. Of Therapy Longer thanNeeded
Noninfectious/NonbacterialSyndrome
Treatment ofColonization/Contamination
Redundant
Hecker MT. Arch Intern Med. 2003;162:972-978.
Unnecessary AntimicrobialsWhere Do We Go Wrong?
“Unnecessary” Antimicrobial Therapy • 129 patients/2 wk period• 576 (30%) of 1941Antimicrobial Day
% U
NN
EC
ES
SA
RY
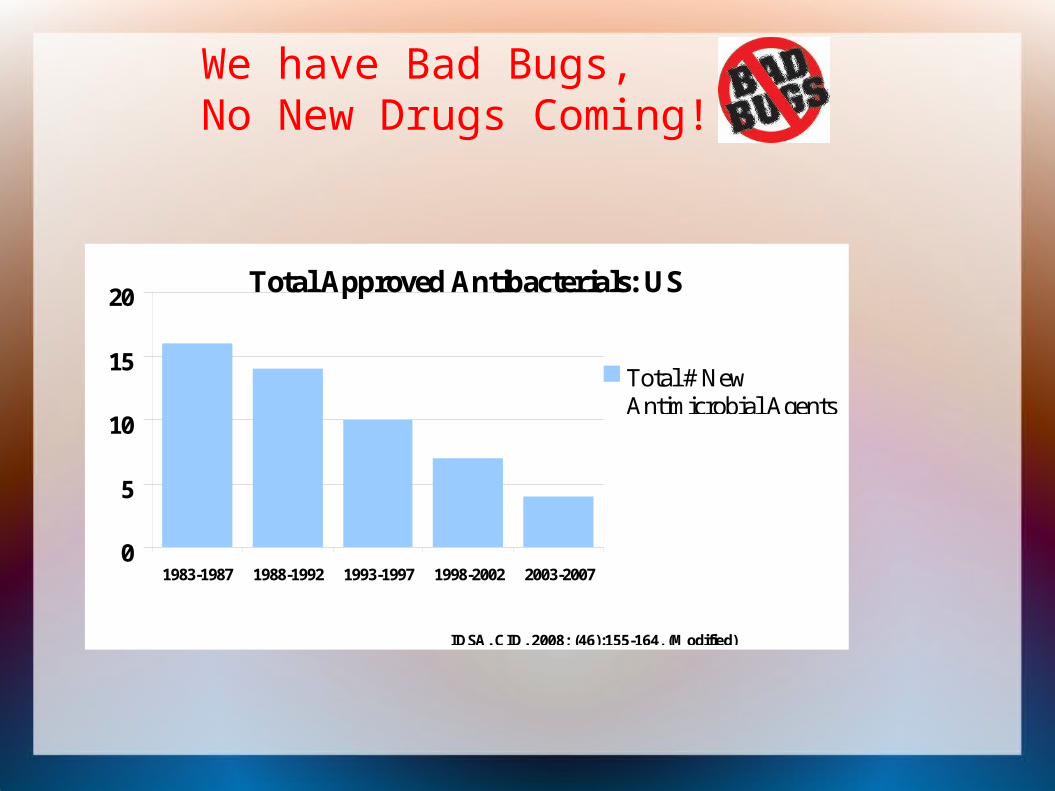
Total Approved Antibacterials: US
0
5
10
15
20
1983-1987 1988-1992 1993-1997 1998-2002 2003-2007
Total # NewAntimicrobial Agents
IDSA. CID. 2008; (46):155-164, (Modified)
We have Bad Bugs, No New Drugs Coming!

Conventional antibiotics
Penicillins Cephalosporins Carbapenems Quinolones Aminoglycosides Macrolides Tetracyclines
Metronidazole clindamycin Vancomycin Teicoplanin Cotrimoxazole

Newer Classes Cyclic lipopeptides (daptomycin)
Bactericidal against Gram-positive, including MRSA
Glycylcyclines (tigecycline) Bacteriostatic against Gram-pos, Gram-neg and
MRSA Oxazolidinones (linezolid)
Bacteriostatic and bactericidal against Gram-positive, including MRSA, VRE

Classes
Bacteriostatic vs Bactericidal Narrow vs Broad spectrum

Classes
Bacteriostatic Aminoglycosides (Streptomycin, Amikacin,
Gentamicin, Tobramycin) Lincosamides (Clindamycin) Macrolides (Azithromycin) Tetracyclines (Doxycycline) Linezolid

Bactericidal
Penicillins Cephalosporins Monobactams (Aztreonam) Carbapenems (Meropenem) Quinolones Sulfonamides
Aminoglycosides Glycopeptides (Vancomycin) Lipopeptides (Daptomycin) Metronidazole

THE IDEAL ANTIBIOTIC?:PENICILLIN
Narrow spectrum Bactericidal Very selective mode of action Low serum protein binding Widely distributed in body esp. CNS Excreted by the kidneys

B-Lactams: Penicillins
Penicillin Use: pneumococcus, strep, enterococcus, N. meningitidis, syphilis,
listeria, leptospirosis and oral anerobes: peptostreptococcus and prevotella
Amoxicillin Use: Covers same stuff as penicillin and expanded activity against
gram negatives ( E.coli, Proteus,H. influenza, H. pylori, N. meningitidis, shigella, klebsiella); covers most spirochetes including lyme disease. Clavulanate enhances the gram negative spectrum to include additional anaerobes such as bacteroides.
Oxacillin/Nafcillin/Dicloxacillin Use: Only good for staphylococcal spp (except MRSA),
pneumococcus and other streptococci Piperacillin and Ticarcillin
Use: Piperacillin covers pneumococcus, streptococcal spp including
enterococcus, gram negative including pseudomonas. Does not cover MRSA.

PENICILLIN IS GENERALLY VERY SAFE BUT….
Allergic reactions not uncommon-rashes Most severe reaction being anaphylaxis A history of anaphylaxis, urticaria, or rash immediately after
penicillin indicates risk of immediate hypersensitivity after a further dose of any penicillin or cephalosporin (therefore these must be avoided)
Allergy is not dependent on the dose given ie, a small dose could cause anaphylaxis
Very high doses of penicillin can cause neurotoxicity Never give penicillin intrathecally

What antibiotics can be used in penicillin allergy?
• Macrolides: erythromycin, clarithromycin (mainly gram positive cover)
• Quinolones: ciprofloxacin, levofloxacin (mainly gram positive cover)
• Glycopeptides (serious infections)
• Fusidic acid, rifampicin, clindamycin (mainly gram positive)

B-Lactams: Cephalosporins1st generation Cefazolin:
Use: staph, non-enterococal strep; prophylactic in clean surgeries, cellultis, folliculitis
Limitations: respiratory tract infections, animal bites or surgeries involving the colon
2nd Generation Cefuroxime:
Use: respiratory infections--Strep pneumoniae, H.influenzae and M.cattarhalis; , meningitis due to pneumococcus,H.flu and N.meningitidis.
Limitations: enteric organisms/abdominal anaerobes Cefoxitin/Cefotetan:
Use: intra-abdominal infections especially anerobes Limitations: staph and other gram positives

B-Lactams: Cephalosporins3rd Generation Cefotaxime & Ceftriaxone:
Use: Good for staph and non-enterococcal strep; broad coverage of gram negative and oral anaerobes, CNS, pulmonary, endovascular, GI infections (excluding gut anaerobes), sinusitis, otitis, head & neck.
Limitations: does NOT cover Pseudomonas; ceftriaxone can cause biliary sludging and limits its utility in treating biliary tree infections
Ceftazidime: Use: Good gram negative coverage including Pseudomonas;
febrile neutropenia CNS infections- good for Pseudomonas meningitis
Limitations: reduced activity against the gram positives and oral anaerobes.
4th Generation Cefepime & Cefpirome:
Use: Enterobacter, Citrobacter and Serratia;Pseudomonas; gram positives; used in neutropenic fever and CNS infections.
Beta-Lactams: Carbapenems
Imepenem: slightly more activity against gram positive
bacteria than meropenem or ertapenem Ertapenem:
Good for aerobic gram negatives poor coverage of pseudomonas ,E. faecalis,
nocardia Meropenem:
Good for aerobic gram negatives Doripenem:
Good for CNS coverage and pseudomonas

Beta-Lactams
Cautions: Beta-lactam allergy can occur in up to
10% 5%-10% cross-sensitivity in penicillin,
cephalosporins, and carbapenems Side effects:
diarrhea, nausea, rash

Quinolones: Ciprofloxacin:
Use: Covers most aerobic gram negatives including Pseudomonas.
penetrates CNS, prostate, lungs Limited against staph
Non-ciprofloxacin quinolones: Ofloxacin, Levofloxacin, Moxifloxacin: Gemifloxacin:
Use: Great for respiratory pathogens, most enteric gram negatives
Only levofloxacin covers pseudomonas Covers some atypicals: Mycoplasma, Chlamydia, Legionella
Cautions: Can cause Qt prolongation, tendon rupture, CNS toxicity Do not use in patients with epilepsy or existing CNS lesions or
inflammation Side effects:
Commonly causes C diff

Macrolides:Erythromycin, Clarithromycin, Azithromycin
Use: Broad spectrum against gram positives
including strep, staph aureus (MSSA) Good for atypical oganism such as
Mycoplasma, Chlamydia, Legionella Covers N.gonorrhea, H flu, Legionella
Caution: can interact with statin to cause myopathy Can cause Qt prolongation
Side effects: GI upset

Clindamycin
Use: Reasonable gram positive aerobic coverage
against strep and many staph including MRSA Special role in treating strep in necrotizing
fascitits Anaerobic coverage better then penicillin but
not as good as metronidazole Caution:
can interact with neuromuscular blocking agents and cyclosporine
Side effects: Diarrhea, commonly causes C difficile—avoid
clindamycin if other good options exist.

Metronidazole
Use: No aerobic activity Does not stand alone for mixed infections Good coverage of anaerobes Can be used for C diff, parasites
Caution: May require reduced dose in liver disease Can increase effect of warfarin
Side effects: Nausea, GI toxicity, antabuse reaction with
Etoh; headache, seizure, peripheral neuropathy with prolonged therapy.

Other major antibiotic groups: aminoglycosides
• Gentamicin, amikacin (tobramycin, streptomycin)
Mainly active against gram negative bacteria Mainly used to treat nosocomial infections Limiting factors are nephrotoxicity (and
ototoxicity) and resistance Also used in combination

How we give aminoglycosides
For serious nosocomial infections: “extended interval” or once daily dosing
Rationale based on concentration- dependent killing and post-antibiotic effect
Reduced risk of nephrotoxicity In infective endocarditis use lower doses to
give synergy with penicillin

Colistin
belongs to the polymyxin group of antibiotics used intravenously for otherwise panresistant
nosocomial infections, especially those due to Pseudomonas and Acinetobacter spp
The most important side effect of intravenous colistin is nephrotoxicity and neurotoxicity
Current major resistance problems: hospital infections
• MRSA: current strains are often multiply-antibiotic resistant
• VISA/GISA: intermediate resistance to glycopeptides (thickened cell wall)
• VRSA/GRSA: highly resistant (transferable on plasmids) from enterococci
• VRE: enterococci (multiply resis tant) Broad spectrum beta lactam resistant (ESBL) Esch
coli, Klebsiella Multiply antibiotic resistant enterobacteria:
Acinetobacter, Serratia
How to optimize antibiotic administration in critically ill How to optimize antibiotic administration in critically ill patientpatient
1) 1) ββ-lactams-lactams Active against most organisms recovered form ICU patientsActive against most organisms recovered form ICU patients
Drug levels are insufficient in patients with severe infections Drug levels are insufficient in patients with severe infections
Cefepime(2g taken every 12hr) concentrations were more than 70% above Cefepime(2g taken every 12hr) concentrations were more than 70% above target concetnrations in less than half of patients with sepsistarget concetnrations in less than half of patients with sepsis
Cefepime (2g every 8hr), recentlyCefepime (2g every 8hr), recently
Lipman J, Gomersall CD, Gin T, et al. Continuous infusion ceftazidime in intensive care: a Lipman J, Gomersall CD, Gin T, et al. Continuous infusion ceftazidime in intensive care: a randomized controlled trial. J Antimicrob Chemother. 1999;43:309–11.randomized controlled trial. J Antimicrob Chemother. 1999;43:309–11.
YUMC

How to optimize antibiotic administration in critically ill How to optimize antibiotic administration in critically ill patientpatient
1) 1) ββ-lactams-lactams Piperacillin concentration, above therapeutic levels for most of the time interval Piperacillin concentration, above therapeutic levels for most of the time interval
in patients with sepsisin patients with sepsis Administration of piperacillin by continuous infusion, with a loading dose, Administration of piperacillin by continuous infusion, with a loading dose,
achieved superior pharmacodynamic targets compared with conventional bolus achieved superior pharmacodynamic targets compared with conventional bolus dosing in septic patients dosing in septic patients
Meropenem concentration, adequate in Meropenem concentration, adequate in mostmost of the studies in critically ill of the studies in critically ill
patientspatients But in severe infection, meropenem had adequate serum concentration for at But in severe infection, meropenem had adequate serum concentration for at
least 50% of the time in patients with normal and impaired renal functionleast 50% of the time in patients with normal and impaired renal function
Kitzes-Cohen R, Farin D, Piva G, et al. Pharmacokinetics and pharmacodynamics of Kitzes-Cohen R, Farin D, Piva G, et al. Pharmacokinetics and pharmacodynamics of
meropenem in critically ill patients. Int J Antimicrob Agents. 2002;19:105–10meropenem in critically ill patients. Int J Antimicrob Agents. 2002;19:105–10..
YUMC

How to optimize antibiotic administration in critically ill How to optimize antibiotic administration in critically ill patientpatient
Dose adjustments are necessary to optimize drug concentrations Dose adjustments are necessary to optimize drug concentrations
Early phase of sepsis, broad-spectrum Early phase of sepsis, broad-spectrum ββ-lactams should be administered more -lactams should be administered more frequently or in doses larger than suggested in non septic patients with a frequently or in doses larger than suggested in non septic patients with a dramatic increased of therapy costsdramatic increased of therapy costs
Continous infusion or extended Continous infusion or extended ββ-lactam infusion are required to optimize -lactam infusion are required to optimize pathogen exposure to bactericidal concentrations of these drugspathogen exposure to bactericidal concentrations of these drugs
Roberts JA, Lipman J: Pharmacokinetic issues for antibiotics in The critically ill patients. Roberts JA, Lipman J: Pharmacokinetic issues for antibiotics in The critically ill patients. Crit Care Med 2009, 37:840–851Crit Care Med 2009, 37:840–851
YUMC

How to optimize antibiotic administration in critically ill How to optimize antibiotic administration in critically ill patientpatient
2) Vancomycin2) Vancomycin Higher than recommended doses of vancomycin were necessary to optimize Higher than recommended doses of vancomycin were necessary to optimize
drug concentrations and rescue patients from septic shock drug concentrations and rescue patients from septic shock
Administration of the conventional dose of vancomycin(15mg/kg of BW every Administration of the conventional dose of vancomycin(15mg/kg of BW every 12hr) would probably fail to achieve therapeutic drug concentraions in the 12hr) would probably fail to achieve therapeutic drug concentraions in the majority of critically ill patientsmajority of critically ill patients
Continuous infusion with 30mg/kg daily dosage has been proposed to optimize PD Continuous infusion with 30mg/kg daily dosage has been proposed to optimize PD vancomycin vancomycin
Continuous infusion, faster time to achieve target drug concentrations, lower Continuous infusion, faster time to achieve target drug concentrations, lower daily dose, reduced therapy costs than intermittent dosedaily dose, reduced therapy costs than intermittent dose
YUMC
Duration of antibiotic therapyDuration of antibiotic therapy
The optimal duration of antibiotic therapy for The optimal duration of antibiotic therapy for bacteremia is unknown. bacteremia is unknown.
There appears to be some evidence that There appears to be some evidence that would suggest that there is no significant would suggest that there is no significant difference in mortality, clinical and difference in mortality, clinical and microbiological cure between shorter durations microbiological cure between shorter durations i.e. 5 – 7 days versus 8 -21 days in critically ill i.e. 5 – 7 days versus 8 -21 days in critically ill patients with bacteremia. patients with bacteremia.

Strategies to optimize the use of antimicrobials in the Strategies to optimize the use of antimicrobials in the ICUICU
1) De-escalation therapy1) De-escalation therapy
2) Antibacterial cycling2) Antibacterial cycling
3) Pre-emptive therapy3) Pre-emptive therapy
4) Use of pharmacokinetic/pharmacodynamic parameters 4) Use of pharmacokinetic/pharmacodynamic parameters for dose adjustmenfor dose adjustmentt
YUMC

De-escalation therapyDe-escalation therapy
Initial administration of broad spectrum empirical treatmentInitial administration of broad spectrum empirical treatment
Rapid adjustment of antibacterial treatment once the causative pathogen Rapid adjustment of antibacterial treatment once the causative pathogen has been identifiedhas been identified
ObjectiveObjective Lower morbidity and mortality by an early achievement of an appropriate Lower morbidity and mortality by an early achievement of an appropriate
empirical treatmentempirical treatment Limit the appearance of bacterial resistance by a reduced antibacterial pressureLimit the appearance of bacterial resistance by a reduced antibacterial pressure
YUMC

De-escalation therapyDe-escalation therapy
Applicability of this strategy, failedApplicability of this strategy, failed Absence of microbiological resultsAbsence of microbiological results Isolation of multi-resistant pathogens preventing de-escalation Isolation of multi-resistant pathogens preventing de-escalation Reluctance of some clinicians to change antibacterials in patients with a Reluctance of some clinicians to change antibacterials in patients with a
favorable clinical course despite persistence of severity of illnessfavorable clinical course despite persistence of severity of illness
Despite limitations, antibacterial de-escalation therapy has been Despite limitations, antibacterial de-escalation therapy has been recommended recommended
YUMC
Antibacterial cyclingAntibacterial cycling
The scheduled rotation of one class of antibacterials The scheduled rotation of one class of antibacterials One or more different classes with comparable spectra of activity One or more different classes with comparable spectra of activity Different mechanisms of resistanceDifferent mechanisms of resistance
Some weeks and a few monthsSome weeks and a few months
ObjectiveObjective Reduce the appearance of resistances by replacing the antibacterial before they Reduce the appearance of resistances by replacing the antibacterial before they
occur and preserving its activity to be re-introduced in the hospital in a later occur and preserving its activity to be re-introduced in the hospital in a later cyclecycle
YUMC
Pre-emptive therapyPre-emptive therapy
The administration of antimicrobials in certain patients at very high risk of The administration of antimicrobials in certain patients at very high risk of opportunistic infections opportunistic infections before the onset of clinical signs of infectionbefore the onset of clinical signs of infection
Developed in hematological patients and/or transplant recipients based on the Developed in hematological patients and/or transplant recipients based on the use of serological tests that advanced the diagnosis of some infectionsuse of serological tests that advanced the diagnosis of some infections
CMV, aspergillosisCMV, aspergillosis In critical illness patients to patients at high risk of candidemia or invasive In critical illness patients to patients at high risk of candidemia or invasive
candidiasis candidiasis
: In the absence of serological test to establish an early diagnosis of invasive : In the absence of serological test to establish an early diagnosis of invasive candidiasis, different scores based on clinical and/or microbiological datacandidiasis, different scores based on clinical and/or microbiological data
YUMC

Optimize Duration of Antibiotic Therapy
• Avoid automatic 10-14-day course of therapy
• New evidence for duration of therapy
– Uncomplicated urinary tract infection: 3-5 days
– Community-acquired pneumonia: 3-7 days
– Ventilator-associated pneumonia: 8 days
– CR-BSI Coagulase-negative staphylococci: 5-7 days
– Acute Hem Osteomyelitis in children-21 days
– Meningococcal meningitis-7 days
– Uncomplicated secondary peritonitis with source control: 4-7 days

• Nosocomial infection is an infection that is not present or incubating when a patient is admitted to a hospital

TYPES OF NCI BY SITE
1. Urinary tract infections (UTI)
2. Surgical wound infections (SWI)
3. Lower respiratory infections (LRI)
4. Blood stream infections (BSI)

CONSEQUENCES OF NOSOCOMIAL INFECTIONS
1. Prolongation of hospital stay: Varies by site, greatest with pneumonias and
wound infections2. Additional morbidity3. Mortality increases - in order - LRI, BSI, UTI4. Long-term physical &neurological
consequences5. Direct patient costs increased- Escalation of the cost of care

UTI
• Contribute to one third of NCI s
• 80% due to catheter
• 5-10% due to urinary tract manipulation
• Prolongs hospital stay by 1-2 days

BACTERIURIA
• PERIURETHRAL COLONIZATION WITH POTENTIAL PATHOGENS INCREASES BU BY THREE FOLD
• LATE CATHETERIZATION INCREASES BU

SURGICAL WOUND INFECTIONS
Incidence varies from 1.5 to 13 per 100 operations.
It can be classified as
1- Superficial incisional SWI
2-Deep incisional SWI and
3-Organ/Space SWI.

LOWER RESPIRATORY INFECTIONS
MOSTLY SEEN IN ICU
RISK FACTORS 1. TRACHEOSTOMY,
2. ENDOTRACHEAL INTUBATION, VENTILATOR,
3. CONTAMINATED AEROSOLS, BAD EQIPPMENT,
4. CONDENSATE IN VENTILATOR TUBING,
5. ANTIBIOTICS,
6. SURGERY,
7. OLD AGE ,
8. COPD,
9. IMMUNO SUPPRESSION

RISK FACTORS FOR DIARRHEAS
1. BY CLOSTRIDIUM DIFFICILE
2. OLD AGE
3. SEVERE UNDERLYING DISEASE
4. HOSPITALISATION FOR >1 WEEK
5. LONG STAY IN ICU
6. PRIOR ANTIBIOTICS

BLOOD STREAM INFECTIONS (BSI)
• PRIMARY = ISOLATION OF BACTERIAL BLOOD PATHOGEN IN THE ABSENCE OF INFECTION AT ANOTHER SITE
• SECONDARY = WHEN BACTERIA ARE ISOLATED FROM THE BLOOD DURING AN INFECTION WITH THE SAME ORGANISM AT ANOTHER SITE i.e. UTI, SWI OR LRI

BACTEREMIA (BSI)
BSI ARE INCREASING PRIMARILY DUE TO INCREASE IN INFECTIONS WITH GM+VE BACTERIA & FUNGI
MOST COMMON IN NEONATES IN HIGH RISK NURSERIES
MORTALITY RATE FOR NOSOCOMIAL BACTEREMIA IS HIGHER THAN FOR COMMUNITY ACQUIRED BACTEREMIA

Case 1
F/74, DM on oral hypoglycemic drugs Presented with fever and malaise, cough with sputum,
tachypnea; chest X-ray revealed bilateral infiltrates Travel history, occupation, contact and clustering non-
remarkable Received a course of amoxicillin for urinary tract infection
10 weeks ago Diagnosis: Community-acquired pneumonia
Question What is the empirical treatment for CAP?

Community-acquired pneumonia (CAP)
Microbiology “Typical” organisms
Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis
“Atypical” organisms Chlamydia pneumoniae Mycoplasma pneumoniae Legionella pneumophilia
Empirical therapy Beta-lactams to cover typical organisms Doxycycline / macrolides to cover atypical organisms Respiratory fluoroquinolones (levo, moxi) for beta-lactam
allergy

Community-acquired pneumonia (CAP)
Empirical therapy (as per IMPACT) CAP, out-patient
Augmentin/Unasyn PO ± macrolide PO Amoxicillin PO + clarithromycin / azithromycin PO
CAP, hospitalized in general ward Augmentin / Unasyn IV/PO ± macrolide Cefotaxime / ceftriaxone IV ± macrolide
CAP, hospitalized in ICU for serious disease Add cover to Gram-negative enterics Tazocin / cefotaxime / ceftriaxone IV + macrolide Cefepime IV + macrolide

Community-acquired pneumonia (CAP)
Empirical therapy Modifying factors
Allergy to beta-lactams Fluoroquinolone (levofloxacin / moxifloxacin)
Aspiration likely: anaerobes should be covered Augmentin / Unasyn / Tazocin already provide coverage Cephalosporins (except Sulperazon) is inactive Moxifloxacin
Bronchiectasis: Pseudomonas cover essential Tazocin / Timentin / cefepime + macrolide Fluoroquinolone + aminoglycoside
Case 2
M/56Presented with skin redness, warmth,
swelling, tenderness on his right lower limb, a pocket of fluid palpated
Diagnosis: cellulitis with pus formation
QuestionEmpirical treatment?
Skin and soft tissue infection
CellulitisMicrobiology
Staphylococcus, StreptococciStreptococci more likely when cellulitis is
well demarcated and there are no pockets of pus or evidence of vein thrombosis

Staphylococcus aureus
If susceptible, penicillinase-resistant penicillins are the drugs of choice for methicillin-susceptible Staphylococcus aureus (MSSA)
Drug of choice Cloxacillin, flucloxacillin Cefazolin, cephalexin (penicillin allergic but tolerate cephs) With beta-lactamase inhibitor
As two-agent combination in Augmentin, Unasyn Erythromycin, clindamycin (if penicillin allergic)
The above antibiotics also have good activity vs. Streptococci

Case 3
M/59 Presented with 2-day history of right upper quadrant pain,
fever, jaundice Emesis x 2 past 24 hours, dark color urine Elevated LFT Radiologic finding: dilated common bile duct, no increase
in gallbladder size Diagnosis: acute cholangitis
Question What is the empirical therapy?

Acute cholangitis/cholecystitis
MicrobiologyGram negative enterics
E. coli, Klebsiella spp., Proteus spp.Anerobes
Bacteriodes fragilis, Clostridium spp.Enterococcus

Acute cholangitis/cholecystitis
Adequate drainage is essentialEmpirical treatment complementary to
drainageAugmentin/Unasyn ± aminoglycosideCefuroxime + metronidazoleCiprofloxacin (if beta-lactam allergic)