DESPRAD subproject Alvis Brazma EMBL-EBI Hinxton, October 20, 2003.

INFECTION AND IMMUNITY, Sept. 2009, p. 3661–3669 Vol. 77, No. 90019-9567/09/$08.00�0 doi:10.1128/IAI.00558-09Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Antibiotic Treatment of Clostridium difficile Carrier Mice Triggers aSupershedder State, Spore-Mediated Transmission, and Severe
Disease in Immunocompromised Hosts�†Trevor D. Lawley,1* Simon Clare,1 Alan W. Walker,2 David Goulding,1 Richard A. Stabler,3
Nicholas Croucher,2 Piero Mastroeni,4 Paul Scott,2 Claire Raisen,1 Lynda Mottram,1Neil F. Fairweather,5 Brendan W. Wren,3 Julian Parkhill,2 and Gordon Dougan1
Microbial Pathogenesis Laboratory1 and Pathogen Genomics,2 Wellcome Trust Sanger Institute, Hinxton, United Kingdom;London School of Hygiene and Tropical Medicine, University of London, London, United Kingdom3; Department of
Veterinary Medicine, University of Cambridge, Cambridge, United Kingdom4; and Center forMolecular Microbiology and Infection, Imperial College of London, London, United Kingdom5
Received 19 May 2009/Returned for modification 19 June 2009/Accepted 23 June 2009
Clostridium difficile persists in hospitals by exploiting an infection cycle that is dependent on humansshedding highly resistant and infectious spores. Here we show that human virulent C. difficile can asymptom-atically colonize the intestines of immunocompetent mice, establishing a carrier state that persists for manymonths. C. difficile carrier mice consistently shed low levels of spores but, surprisingly, do not transmitinfection to cohabiting mice. However, antibiotic treatment of carriers triggers a highly contagious supershed-der state, characterized by a dramatic reduction in the intestinal microbiota species diversity, C. difficileovergrowth, and excretion of high levels of spores. Stopping antibiotic treatment normally leads to recovery ofthe intestinal microbiota species diversity and suppresses C. difficile levels, although some mice persist in thesupershedding state for extended periods. Spore-mediated transmission to immunocompetent mice treatedwith antibiotics results in self-limiting mucosal inflammation of the large intestine. In contrast, transmissionto mice whose innate immune responses are compromised (Myd88�/�) leads to a severe intestinal disease thatis often fatal. Thus, mice can be used to investigate distinct stages of the C. difficile infection cycle and can serveas a valuable surrogate for studying the spore-mediated transmission and interactions between C. difficile andthe host and its microbiota, and the results obtained should guide infection control measures.
Clostridium difficile is a gram-positive, spore-forming, anaer-obic bacterium that can reside asymptomatically in the intes-tinal tract of humans (6, 11, 42). The use of antibiotics thatspare C. difficile but suppress the intestinal microbiota allowsC. difficile to proliferate (23), potentially leading to intestinaldamage, inflammation, and clinical disease (9). In most casesstopping antibiotic therapy is often sufficient to prevent orreverse disease symptoms in immunocompetent individuals (5,32). However, in immunocompromised hospital patients, par-ticularly the elderly, intestinal disease can quickly develop afterantibiotic treatment, with clinical outcomes ranging from milddiarrhea to pseudomembraneous colitis to multiple-organ dys-function syndrome (17, 31).
Unlike most pathogens, C. difficile produces a metabolicallydormant spore form that is excreted by infected patients (43,63). The infective spores persist in the environment and arehighly resistant to commonly used disinfectants (24). Indeed,environmental spore contamination in a hospital results in areservoir for transmission (21, 46) that can lead to a propor-tional increase in the percentage of the patient population
colonized by C. difficile (33). As a result, C. difficile is endemicin many hospitals, and outbreaks are difficult to contain, high-lighting the compelling need to understand the spore-mediatedinfection cycle and the factors that lead to C. difficile transmis-sion (24, 59).
Most studies of C. difficile pathogenesis in animals havefocused on the acute stage of infection (13, 38, 45, 57), so manyaspects of the C. difficile infection cycle have not been investi-gated in detail, including intestinal carriage, interactions withthe microbiota, the role of spores in transmission, and hostsusceptibility to severe disease. Recent reports that variousvirulent C. difficile ribotypes can colonize several mammalianhosts (25, 30, 48, 51, 52) led us to reinvestigate the mouse as amodel for the C. difficile infection cycle. We found that C.difficile strain M68, a representative ribotype that frequentlycauses human disease (19), was very proficient at persisting ininbred mice. Here we describe the impact of antibiotics on thecomposition of the intestinal microbiota of murine C. difficileM68 carriers and reveal that antibiotics can inadvertently trig-ger high-level spore excretion and remarkably efficient host-to-host transmission of C. difficile. Further, we demonstratethat transmission of C. difficile to immunocompetent miceleads to self-limiting intestinal disease, whereas transmission toMyd88�/� mice, which are defective in a key signaling pathwayin the innate immune response, leads to severe intestinal dis-ease and multiple-organ dysfunction syndrome, potentiallymimicking the situation in humans.
* Corresponding author. Mailing address: Microbial PathogenesisLaboratory, Wellcome Trust Sanger Institute, Hinxton, Cam-bridgeshire, United Kingdom CB10 1SA. Phone: 01223 495 391. Fax:01223 495 239. E-mail: [email protected].
† Supplemental material for this article may be found at http://iai.asm.org/.
� Published ahead of print on 29 June 2009.
3661
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

MATERIALS AND METHODS
C. difficile culture. C. difficile M68 is a PCR ribotype 17, toxinotype VIII,tcdAB� strain isolated from a multihospital outbreak of C. difficile disease inDublin, Ireland (19). C. difficile M68 was routinely grown for 24 to 48 h at 37°Cunder anaerobic conditions in a Whitley DG250 workstation (Don Whitley, WestYorkshire, United Kingdom). For mouse infection, C. difficile was grown stati-cally for 36 h in Wilson’s broth (62). To enumerate the total C. difficile in freshfeces, samples (100 mg feces/ml phosphate-buffered saline [PBS]) were imme-diately serially diluted in PBS and plated on Brazier agar (Bioconnections,Whetherby, United Kingdom) plates (90 mm or 140 mm; Bibby Sterilin Ltd.,Stone, Staffordshire, United Kingdom) supplemented with 0.5% taurocholate(Sigma, United Kingdom) to improve the C. difficile detection limit (62). Typi-cally, fresh fecal samples were processed and plates were placed in the anaerobiccabinet within 45 min after excretion. To enumerate spores in feces, 0.1-ml fecalsamples were mixed with 0.1 ml of 100% ethanol for 1 h at room temperature tokill the vegetative cells of C. difficile. Samples were pelleted, washed twice in PBS,resuspended in 0.1 ml of PBS, and cultured as described above.
Mouse infection and transmission experiments. Specific-pathogen-free femalewild-type, Igh6�/�, or Myd88�/� mice with a C57BL/6 genetic background thatwere 5 to 7 weeks old (from mouse colonies maintained at Wellcome TrustSanger Institute) were infected as indicated below by either oral gavage ortransmission. Mice were housed in sterile cages containing wood shavings, foodpellets, and water. Once a week, mice were aseptically moved to a sterile cage.Cage changing and mouse handling were performed in a sterile biosafety hood bya worker wearing a clean smock and gloves that were disinfected with 2% Virkon(potassium peroxymonosulfate). To establish the carrier state in the experimentwhose results are shown in Fig. 1, mice were pretreated with 1 mg of neomycin24 h prior to oral gavage with 107 CFU of C. difficile in 0.2 ml of PBS, althoughneomycin pretreatment is not necessary to establish the carrier state. For exam-ple, the carrier state in mice used for the experiment whose results are shown inFig. 2 was established without the antibiotic pretreatment. To induce the super-shedder state, carrier mice were treated with 1 mg clindamycin in 200 �l PBS viagavage (see Fig. 1 and 2) or clindamycin (250 mg/liter) was added to the drinkingwater (see Fig. 5).
To perform host-to-host transmission experiments, five naïve recipient micewere housed in a sterile cage with two infected donor mice or no donor mice for5 h. Immediately after this, the recipient mice were aseptically removed, housedindividually in sterile cages, and given water that contained clindamycin (250mg/liter) for 4 days. Mice drink 3 to 4 ml of water/day, so these mice typicallyingested 0.75 to 1 mg clindamycin/day. The transmission efficiency was assessedby culturing C. difficile from feces of recipient mice after 4 days of clindamycintreatment.
To contaminate polysulfone cages (with no bedding so mice were in directcontact) for environmental spore transmission experiments, supershedders (n �5) were placed in the cages (floor area, 800 cm2) for 1 h (1.5 to 1.8 g fecesexcreted/cage). Subsequently, the supershedders were removed, and the cageswere left for 16 h under ambient oxygen conditions to eliminate the vegetativeform of C. difficile (see Fig. 1c). Before experiments were performed, all feceswere removed from the cage to ensure that transmission did not occur viacoprophagy. To demonstrate spore contamination, naïve (untreated) mice wereaseptically placed in a cage for 1 h and then aseptically removed, placed in asterile cage, and given water containing clindamycin (250 mg/liter). Surfacedisinfection of contaminated cages was performed by adding 400 ml of a 2%Virkon solution to the cage for the periods of time indicated below. After theVirkon solution was removed, the surface was patted dry with sterile papertowels before naïve mice were placed in the cage. All animal infections wereperformed in accordance with the UK Home Office Animals (Scientific Proce-dures) Act of 1986.
Construction and analysis of 16S rRNA gene libraries. DNA was extractedfrom fresh, unfrozen fecal samples using a FastDNA Spin kit for soil and aFastPrep bead-beating instrument (both obtained from MP Biomedicals, Solon,OH). Preparation of 16S rRNA gene clone libraries and sequence analysis wereperformed as described previously (54), except that single reads for around 600to 650 bp spanning the V2 to V5 variable regions were generated for each cloneusing primer 926r (5�-CCGTCAATTC[A/C]TTT[A/G]AGT-3�). Sequences werealigned using the NAST aligner (15) and were subjected to extensive manualcorrection before further analysis. Shannon diversity indices (SDI) were calcu-lated for each sample using DOTUR (49).
Microscopy. Cecum tissue (0.5-cm tubular sections) was carefully excised,opened, and processed for transmission electron microscopy, scanning electronmicroscopy, and immunogold (66) or hematoxylin and eosin staining (54) aspreviously described.
Nucleotide sequence accession numbers. Sequences determined in this studyhave been deposited in the GenBank database under accession numbersGQ294716 to GQ300837.
RESULTS
Intestinal carriage of C. difficile in mice. Healthy immuno-competent C57BL/6 mice were orally challenged with the hu-man virulent strain C. difficile M68, and subsequently fecalshedding was monitored. Intriguingly, challenged mice repro-ducibly became carriers, shedding low levels of C. difficile(�500 CFU/g [fresh weight] feces) for many months (Fig. 1a).Further, low levels of C. difficile spores (�102 spores/g) wereconsistently detected in dried fecal pellets collected from thebedding of cages harboring carrier mice, which were asepticallymoved to sterile cages once a week. During the initial experi-ments mice were pretreated with neomycin; however, subse-quent experiments demonstrated that prior antibiotic treat-ment is not required for infection of mice with C. difficile (datanot shown). Importantly, the same strain of C. difficile (strainM68) that was used to infect mice was routinely isolated fromthe feces of carriers, based on comparative genomic hybridiza-tion results (see Fig. S1 in the supplemental material). Thecarrier mice appeared to be generally healthy and did notdevelop any obvious clinical symptoms or pathological lesionsin their intestinal tissues (data not shown). Therefore, C. dif-ficile M68 can asymptomatically and persistently colonize theintestine of mice at low levels in a manner reminiscent of thecolonization of human carriers (46).
Antibiotic induction of a supershedder state. In the clinicalsetting, treatment with antibiotics is the major risk factor for C.difficile disease (59). To determine the effect of antibiotic treat-ment on the dynamics of C. difficile shedding, we treated car-rier mice with clindamycin, to which C. difficile M68 is resistant.Between 2 and 3 days after treatment was initiated, we ob-served a dramatic 106-fold increase in the levels of C. difficileshedding for all of the treated mice, establishing what we referto as a supershedding state (Fig. 1a and b). Significantly, thesupershedding state was maintained as long as mice were beingtreated with clindamycin (see Fig. S2 in the supplemental ma-terial). Typically, 12 to 16 days after a 3-day course of clinda-mycin the levels of C. difficile shedding dropped abruptly to theprevious carrier shedding levels (Fig. 1b). After long-term ex-posure (17 days) to clindamycin, many mice were found to bein the carrier state 12 to 16 days after cessation of treatment(45 of 105 mice). However, a significant number of mice werepersistent supershedders for 3 to 5 weeks (55 of 105 mice) oroccasionally for months (5 of 105 mice) (see Fig. S2 in thesupplemental material). Thus, after longer-term antibiotictreatment mice were more prone to remain in the supershed-der state for extended periods. It is also noteworthy that col-onized mice were susceptible to multiple cycles of clindamycin-induced supershedding (Fig. 1b), indicating that mice do notclear the infection or become resistant to the supersheddingstate.
Total C. difficile cells (vegetative cells and spores) or onlyspores (ethanol resistant) in fecal samples can easily be enu-merated using CCEY selective medium in combination withthe ethanol shock method (47). We found that immediatelyafter excretion 10 to 20% of the total C. difficile vegetative cells
3662 LAWLEY ET AL. INFECT. IMMUN.
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

and spores shed in the feces of supershedders were spores (Fig.1c), representing a �105-fold increase (P � 0.005) comparedto the level excreted by carrier mice (Fig. 1a and c). Afterexcretion from supershedders, feces were maintained in theambient atmosphere for up to 30 days and periodically sam-pled to monitor the viability of environmental C. difficile totalcells and spores. After 7 h spores accounted for all of the
culturable C. difficile (Fig. 1c). Thus, while the vegetative formof C. difficile in excreted feces was short lived (�7 h), sporessurvived at a constant level over a 30-day period (Fig. 1c).Since sporulation requires vegetative growth (43, 55), theseobservations suggest that C. difficile sporulates in the intestinaltract prior to excretion. Together, these results demonstratethat antibiotic treatment per se of carrier mice induces a su-
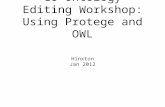
FIG. 1. Induction of high-level fecal shedding of C. difficile spores by clindamycin treatment of carrier mice shedding low levels of spores. (a)Long-term fecal shedding from individual mice (five mice per cage) infected with C. difficile M68. The horizontal dashed line indicates the detectionlimit, 101 CFU/g. (b) Clindamycin treatment (1 mg/day via oral gavage) (arrows) of carriers (five mice per cage) reproducibly resulted in rapidinduction of high-level shedding of C. difficile that gradually returned to low-level shedding 12 to 16 days after treatment was discontinued. Incontrast, PBS treatment of carrier mice (five mice per cage) (arrows) did not affect the levels of C. difficile cultured from feces, although these micewere prone to high-level shedding of C. difficile after clindamycin treatment (see panel a). In this experiment mice were pretreated with neomycin,although prior antibiotic treatment is not necessary to establish the carrier state, as shown in Fig. 2. (c) Levels of C. difficile vegetative and sporeforms (supershedder total) and spores (supershedder spores) excreted by supershedders and of spores excreted by carrier mice. Five mice wereused for each sample.
VOL. 77, 2009 INDUCTION OF C. DIFFICILE DISEASE AND TRANSMISSION 3663
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

pershedding state, resulting in the release of high levels of C.difficile spores into the environment, which can persist evenafter withdrawal of antibiotics. Importantly, the C. difficile su-pershedding state exists in the absence of obvious clinical dis-ease (lethargy, ruffled fur, hunched position, etc.).
Antibiotic disruption of C. difficile carrier microbiota. Sincewe established that C. difficile M68 can establish both a carrierstate and a supershedder state in mice, we decided to investi-gate the changes in the intestinal microbiota associated withthese states. Hence, we performed a detailed 16S rRNA genesequence analysis of a total of 6,122 clones amplified from thefeces of C. difficile-infected mice (n � 5) at five time pointsbefore and after clindamycin treatment (Fig. 2a and b; seeTable S1 in the supplemental material). This analysis con-firmed that in carrier mice C. difficile was a minor componentof the microbiota, as C. difficile 16S rRNA gene sequenceswere not detected even though �1,200 clones were sequenced(Fig. 2a and b). Given the low level of C. difficile shedding fromcarrier mice, we did not expect to detect any 16S rRNA clonesrepresenting this species. Indeed, the carrier mice maintaineda diverse microbiota community structure (SDI, 3.6) (Fig. 2c)dominated by members of the Firmicutes and Bacteroidetes
phyla (Fig. 2a), a typical profile for a stable mammalian intes-tinal microbiota (20, 35).
In contrast, a single exposure to clindamycin resulted indramatic alteration of the carrier microbiota (Fig. 2a and b; seethe supplemental material). Initially, the microbiota disruptionwas characterized by a tremendous loss of species richness(SDI, 1.5) (Fig. 2a and c), particularly in the Bacteroidetes andobligate anaerobic Firmicutes species, and a dramatic expan-sion of the facultative anaerobes Escherichia coli and Entero-coccus casseliflavis (Fig. 2b). Following a highly reproducible3-day lag period after clindamycin exposure, the C. difficilesupershedding state was established (Fig. 2a) and C. difficile16S rRNA genes accounted for �5% of the libraries (Fig. 2b).This time point coincided with partial recovery of the diversityof the microbiota (SDI, 2.5) (Fig. 2c), particularly for theFirmicutes phylum (Fig. 2b; see Table S1 in the supplementalmaterial). The subsequent decrease in the level of C. difficilecolonization was associated with a significant rebound in spe-cies diversity (SDI, 3.1) (Fig. 2c) typified by large increases inthe range of Firmicutes species and a slower recovery of therichness of the Bacteriodetes phylum (Fig. 2a). Our analysis wasdeep enough to monitor changes at the species level. However,we did not identify any specific genus or group of bacteria thatwere reproducibly associated with the reduction in C. difficileshedding (see Table S1 in the supplemental material). Finally,within 10 days after exposure to clindamycin both the compo-sition and the richness of the microbiota had recovered tolevels similar, but not identical, to the levels before clindamy-cin treatment (SDI, 3.3) (Fig. 2a and c).
C. difficile supershedders promote spore-mediated transmis-sion. Supershedders are the most contagious individuals innatural populations (36, 64). Consequently, we tested whetherC. difficile could be transmitted from colonized mice to naïvemice (i.e., mice that had never been colonized by C. difficile)and whether transmissibility was related to shedding levels.After naïve mice were housed with supershedding mice in thesame cage for 5 h, the majority (19 of 20) (Fig. 3a) of naïverecipient mice were colonized with C. difficile. In contrast, none(Fig. 3a) of the 15 naïve recipient mice housed with C. difficilecarriers were colonized even though we demonstrated that lownumbers of spores were present in the feces of the formermice. Thus, the high level of shedding of C. difficile fromsupershedder mice promotes efficient host-to-host transmis-sion, whereas the carrier state does not.
Next we investigated if direct contact was essential for C.difficile transmission by housing naïve mice in cages previouslyoccupied by supershedders. These investigations showed thatenvironmental spores are a very effective agent for C. difficiletransmission, as all 15 naïve mice were colonized when theywere housed in cages previously contaminated by supershed-ders (Fig. 3b). During these experiments the feces were re-moved from the cages to ensure that transmission was not dueto coprophagy. Indeed, we found that even short-term housingof supershedding mice in contaminated cages was sufficient totrigger transmission to naïve mice subsequently placed in thesame cages, suggesting that brief exposure to environmentalcontamination can result in infection (data not shown).
Since we could readily trigger transmission of C. difficilebetween mice, we were in a position to assess different disin-fection regimens for their potential to block transmission.
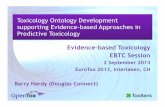
FIG. 2. Antibiotic-induced C. difficile supershedding state is asso-ciated with reduced intestinal microbiota diversity. (a) Average fecalshedding of C. difficile by carrier mice (five mice per cage) treated withclindamycin to induce a transient supershedder state. The error barsindicate standard deviations. DNA was extracted from fresh feces fromeach mouse at the indicated time points (green arrowheads) to create16S rRNA gene clone libraries. The detection limit was 103 CFU C.difficile/g feces. (b) Temporal shifts in the intestinal bacterial commu-nity after clindamycin treatment of carrier mice as determined by 16SrRNA gene analysis. The levels of predominant bacterial groups areexpressed as percentages of the clone libraries using pie charts. On day23 1,400 clones were included (average, 280 clones/mouse), on day 251,202 clones were included (average, 241 clones/mouse), on day 271,204 clones were included (average, 241 clones/mouse), on day 291,081 clones were included (average, 216 clones/mouse), and on day 331,167 clones were included (average, 233 clones/mouse). (c) SDI foreach phase of the microbiota community structure determined by 16SrRNA gene phylotypes.
3664 LAWLEY ET AL. INFECT. IMMUN.
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

Treatment of C. difficile spore-contaminated cages with alco-hol-based disinfectants did not prevent transmission (data notshown), reflecting the findings for clinical settings (59). In-stead, we found that a rigorous 20-min surface disinfectionregimen using the strong sporicidal agent Virkon was neces-sary to reduce environmental spore contamination enough toeliminate transmission (0 of 10 mice) (Fig. 3b). Importantly, 1-and 5-min Virkon-based surface disinfection regimens resultedin only 30% and 80% reductions in the transmission efficiency,respectively (Fig. 3b). Indeed, use of stringent precautions inour animal facility, such as proper disinfection and aseptichanding of mice, is required to prevent inadvertent C. difficiletransmission.
C. difficile supershedders transmit disease. The fact that C.difficile transmission was so efficient allowed us to investigateC. difficile colonization and host interactions following naturalinfection of mice rather than artificial challenge. When natu-rally infected mice were treated with clindamycin to induce thesupershedder state, they did not develop debilitating disease(see Fig. S3a in the supplemental material). However, an in-flammatory exudate was routinely found in the feces of thesesupershedders. We thus examined the gastrointestinal tracts ofsupershedder mice to identify any associated pathology. Clin-damycin-treated, uninfected control mice showed no sign ofpathological lesions (Fig. 4a and c). In contrast, during forma-tion of the supershedder state (days 4 to 7 postinfection), clearsigns of mucosal damage were evident in the large intestines(cecum and colon) of the majority of supershedding mice,including epithelial cell death, microvillus effacement, and dis-rupted epithelial tight junctions (Fig. 4d and e). Both thevegetative and spore forms of C. difficile were readily observedin the intestinal lumen, and sometimes large numbers were
observed (Fig. 4e). Individual cells or clumps of C. difficilecould be seen in close association with and sometimes attachedto or within damaged tissue (Fig. 4f). Importantly, immuno-gold labeling with a C. difficile antibody clearly demonstratedthat the bacteria observed were in fact C. difficile (Fig. 4e,inset).
On days 10 to 13 postinfection, as C. difficile shedding levelswere declining (see Fig. S3a in the supplemental material),supershedders continued to display obvious signs of intestinalinflammation. Pathological lesions consisting of hyperplasia,inflammatory cell infiltration, and submucosa edema were
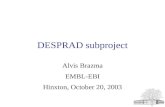
FIG. 3. Host transmission of C. difficile via supershedding mice andenvironmental spore contamination. (a) Transmission efficiency, indi-cating the percentage of naïve mice that acquired C. difficile infectionfrom donor mice. The number of naïve mice housed with no donor was10, the number of naïve mice housed with carrier mice was 15, and thenumber of naïve mice housed with supershedding mice was 20. (b)Percentage of naïve mice that acquired C. difficile infection from aspore-contaminated environment. The number of naïve mice housedin a contaminated environment with no sporicide was 15, the numberof naïve mice housed in a contaminated environment treated for 1 minwith sporicide was 10, the number of naïve mice housed in a contam-inated environment treated for 5 min with sporicide was 10, and thenumber of naïve mice housed in a contaminated environmenttreated for 20 min with sporicide was 10. Groups of 5 or 10 naïvemice were housed in cages previously contaminated by supershed-ders. The transmission efficiency was determined as described inMaterials and Methods.
FIG. 4. Supershedders efficiently transmit C. difficile disease tonaïve recipients. (a to f) Representative images that illustrate epithelialdamage and the inflammatory response in ceca of recipient mice (100mice) after clindamycin treatment (see Fig. S3 in the supplementalmaterial). (a) Toluidine blue staining of the cecum from a clindamycin-treated control mouse. (b) Toluidine blue staining demonstratingedema and immune cell infiltrate (arrows) within the cecal submucosaof a C. difficile-infected mouse. (c) Transmission electron micrographof the intact epithelial brush border (black arrow) and tight junctions(white arrows) of the cecum from a clindamycin-treated controlmouse. (d) Disrupted tight junction and microvillus effacement withinthe cecal submucosa of a C. difficile-infected mouse (arrow) (comparewith panel c). (e) C. difficile vegetative cells and spores associated withepithelial effacement and cellular invasion and immunogold labeling ofC. difficile within the lumen (inset). (f) Matt of C. difficile cells (arrows)overlaying damaged and necrotic microvilli.
VOL. 77, 2009 INDUCTION OF C. DIFFICILE DISEASE AND TRANSMISSION 3665
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

commonly observed (Fig. 4b). Regions of severe inflammationwere associated with large aggregates of C. difficile cells thatappeared to form exaggerated mats covering the epithelialsurface (see Fig. S3b in the supplemental material), which wasmarked by destroyed or necrotic microvilli (Fig. 4f). The typeof inflammatory lesions was variable, ranging from mild tosevere. Importantly, despite this clear intestinal damage, wild-type mice did not lose weight or succumb to C. difficile infec-tion. Indeed, these mice quickly recovered as no signs ofintestinal damage or pathology were evident following termi-nation of clindamycin treatment and the subsequent return ofsupershedding mice to the carrier state (data not shown).
Myd88 protects against severe C. difficile disease. C. difficiledisease is normally associated with immunocompromised orelderly individuals, and although normal supershedder micedisplayed evidence of intestinal damage, they did not developovert disease. Therefore, we exposed groups of knockout micewith mutations in genes associated with immune defense tomicrobial pathogens. Igh6�/� mice, defective in B-cell re-sponses (29), that were infected with C. difficile maintainedtheir weight and remained asymptomatic during the experi-ment (Fig. 5a). Further, these mice did not exhibit severemucosal damage compared to similarly infected wild-type mice(Fig. 5b). In contrast, we found that on days 10 to 12 postin-fection Myd88�/� mice (1), deficient in innate signaling at the
mucosa, became moribund and began to rapidly lose weight(Fig. 5a). Analysis of the large intestine of infected mice re-vealed more pronounced intestinal disease in Myd88�/� micethan in wild-type and Igh6�/� mice (Fig. 5b), including in-creased hyperplasia, cellular infiltrate, and edema. Interest-ingly, 48% (28 of 60) of the Myd88�/� infected mice suc-cumbed to infection, whereas clindamycin-treated, uninfectedMyd88�/� mice (n � 15) remained healthy. Postmortem ex-amination revealed a variety of pathological lesions at systemicsites in moribund Myd88�/� mice that were not observed inwild-type infected mice, particularly in the kidneys and lungs(see Fig. S4 in the supplemental material). Therefore, micedeficient in Myd88 are susceptible to severe C. difficile intesti-nal disease and are prone to succumbing to an infection that isassociated with systemic pathologies.
DISCUSSION
We demonstrate here for the first time that human virulentC. difficile can establish an asymptomatic and persistent carrierstate in healthy mice, mimicking the situation with humancarriers (46) (Fig. 6). Further, we show that carrier mice arenot significantly contagious, even though they excrete low lev-els of C. difficile spores. However, using these carrier mice, weobtained the first experimental evidence that antibiotic treat-ment triggers a supershedding state involving high levels ofspore excretion, leading to C. difficile transmission in the ab-sence of obvious clinical disease. Symptomatic hospital pa-tients with overt C. difficile clinical disease are currently theprimary target of infection control measures in hospitals (24,59). However, our results suggest that antibiotic treatment ofC. difficile carriers per se triggers excretion of high levels ofspores. Thus, in hospitals it may be prudent to monitor patientsundergoing treatment with antibiotics for evidence of C. diffi-cile spore shedding.
A stable intestinal microbiota community protects the hostfrom both indigenous and exogenous pathogens through aphenomenon termed “colonization resistance” (53, 54, 58).Antibiotic-mediated disruption of colonization resistance canpromote intestinal overgrowth of pathogens such as Enterococ-cus (10, 18) and Salmonella enterica (4, 8, 14, 34, 50). Here weused 16S rRNA gene analysis to monitor the temporal shifts inthe bacterial community of carriers during the loss and subse-quent recovery of colonization resistance to C. difficile. Weshow that reduced bacterial diversity is one of the majorchanges in the intestinal microbiota that allows C. difficile toproliferate and sporulate within the intestinal tract. In additionto C. difficile proliferation after antibiotic treatment, we notedthat Enterococcus and E. coli also thrived. Although we did notmonitor the transmission of Enterococcus and E. coli in ourexperiments, it has previously been documented that transmis-sion of Enterococcus (18) and S. enterica (34) increases signif-icantly after treatment of infected hosts with antibiotics. Thus,bacterial groups associated with antibiotic-associated diarrheamay exploit common antibiotic-induced perturbations in theintestinal microbiota to cause contagious diarrhea and dissem-inate.
Disrupting the carrier microbiota with a short course ofclindamycin appears to result in ecological succession (37) inwhich the disturbance of the initial community is followed by
FIG. 5. Myd88�/� mice are susceptible to severe C. difficile disease.(a) Average weights of wild-type, Igh6�/�, and Myd88�/� mice thatwere infected with C. difficile via transmission (green arrow) and sub-sequently treated with clindamycin (red bar). Wt, wild type. (b) He-motoxylin- and eosin-stained sections of cecal mucosa from wild-type,Igh6�/�, and Myd88�/� mice that were treated with clindamycin butnot infected and from mice treated with clindamycin and infected withC. difficile. Infection with C. difficile results in moderate intestinalinflammation (cecum) in wild-type and Igh6�/� mice and more severeintestinal inflammation in Myd88�/� mice. Magnification, 20.
3666 LAWLEY ET AL. INFECT. IMMUN.
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

orderly changes in the composition and richness until a stableclimax community is reestablished. Recent analyses of murine(2) and human (16, 28) intestinal bacterial communities inresponse to longer-term antibiotic therapy revealed similarpatterns of biodiversity dynamics, although the stable, postan-tibiotic communities differed significantly from the preantibi-otic communities. Ecological succession is a fundamental con-cept in ecology that is used to understand and predict theimpact of a disturbance on ecosystems, and the classic exampleis the recovery of a forest after clear-cutting. Ecological suc-cessions are marked by distinct stages in which opportunisticorganisms exploit the reduced species diversity to proliferatebut are replaced by organisms that compete more efficiently asthe community diversity increases during recovery (37). Interms of antibiotic disruption of the mammalian intestinal mi-crobiota ecosystem, C. difficile, E. coli, and enterococci areconsidered opportunistic organisms that thrive in the intestinalmicrobiota community during periods when the biodiversity islow. This idea is consistent with a recent analysis of the intes-tinal microbiota of patients that are prone to relapsing with C.difficile overgrowth and disease (12).
Other workers have successfully used hamsters (38, 45) andmice (13, 41, 57) to investigate aspects of acute C. difficiledisease and protective immunity. Previous murine infectionmodels have relied on mice devoid of an intestinal microbiota(germfree or antibiotic depletion prior to infection), so thesemodels were not exploited to study the complete infectioncycle, including intestinal carriage and host-to-host transmis-sion. Further, previous work on other enteric infections hassuggested that bacteria grown in laboratory medium and ad-ministered by oral gavage may have a distinct pattern of colo-nization compared to the pattern seen following host-to-hosttransmission (39, 60, 61). Here, using direct environmental
transmission of C. difficile spores, we demonstrate that natu-rally infected immunocompetent mice develop intestinal dam-age and inflammation that resolve after the antibiotic is re-moved and the intestinal microbiota recovers. These resultsmimic the expected outcome of C. difficile infection in healthy,immunocompetent adult humans (5, 32). Our ability to triggerC. difficile transmission with relevant antibiotic treatment ofcarriers places in context the entire C. difficile infection andtransmission cycle and potentially has great significance.
Severe C. difficile disease likely occurs in immunocompro-mised or elderly individuals because of aberrant interactionsbetween the host immune system, the intestinal microbiota,and C. difficile. Presumably, specific elements of the immunesystem are compromised in such individuals, making themsusceptible to severe disease, although this hypothesis has notbeen formally addressed. We demonstrate here that the innateimmune system of mice protects against C. difficile severe dis-ease, specifically signaling through the Myd88 pathway (Fig. 6).Defective innate immune signaling has not previously beenimplicated in C. difficile disease susceptibility, but this pathwayhas been shown to play a role in a variety of intestinal disor-ders, such as Crohn’s disease and ulcerative colitis, due todisrupted signaling between the luminal bacteria and the in-testinal mucosa (65). The identification of Myd88�/� mice asmice that are susceptible to severe C. difficile disease generatesa number of testable hypotheses regarding the precise mech-anism(s) that the host uses to resist the potentially harmfuleffects of virulent C. difficile overgrowth, including the roles ofMyd88-mediated cytokine cascades (22), antimicrobial pep-tides (56), and the epithelial barrier function (44). Severe C.difficile intestinal disease in humans can culminate in multiple-organ dysfunction syndrome (17) that can be associated withrenal failure (3, 7) and acute respiratory distress syndrome
FIG. 6. Relationship between C. difficile carrier state and supershedding state in response to antibiotic treatment and role of the host immunesystem in severe disease. C. difficile carrier mice possess a stable and diverse intestinal microbiota community (small rods) which includes low levelsof C. difficile (red rods with spores). As a result, carrier mice excrete low levels of spores and are poor donors for C. difficile infection. Antibiotictreatment of carrier mice reduces the diversity of the intestinal microbiota community, allowing C. difficile to proliferate and sporulate (red circles).As a result, a supershedding state occurs with high levels of spore excretion and efficient host-to-host transmission. Withdrawing the antibioticallows the intestinal microbiota to rediversify and suppresses C. difficile levels, thereby reestablishing the carrier state and reducing the conta-giousness of the host. Transmission of C. difficile to Myd88-deficient mice, but not transmission of C. difficile to Igh6�/� mice, results in severedisease, implicating Toll-like receptor signaling in protection against virulent C. difficile overgrowth. Wt, wild type.
VOL. 77, 2009 INDUCTION OF C. DIFFICILE DISEASE AND TRANSMISSION 3667
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

(27). We observed these syndromes in many Myd88-deficientmice, demonstrating that transgenic knockout mice can beused to study host susceptibility to severe C. difficile disease.
Understanding the interactions between C. difficile, the in-testinal microbiota, and the host immune system in response todifferent antibiotic treatments and host genotypes is requiredto fully appreciate the mechanisms of C. difficile carriage, dis-ease, and transmission. The C. difficile strain used in our stud-ies represents only one clinically relevant ribotype, so it isimportant to test other strains (i.e., ribotype 027) in the mousemodel. Further, the ability to make targeted mutations in C.difficile (26, 40), as well as the availability of several C. difficilegenomes (http://www.sanger.ac.uk/Projects/C_difficile), shouldallow studies of toxin production and sporulation during C.difficile disease and transmission. Thus, the availability of amurine model for investigating the complete infection andtransmission cycle of C. difficile could be extremely valuable forassessing the potential of novel therapeutics, immunization,probiotics, and transmission prevention measures to control C.difficile.
ACKNOWLEDGMENTS
This work was funded by the Wellcome Trust. T.D.L. was funded bythe Royal Society of London.
We are grateful to Stanley Falkow and Bronwyn MacInnis for in-valuable input and thoughtful discussions, to Cordy Brandt and NicolaGoodwin for technical assistance with the animal infections, to theSanger Sequencing Team for 16S rRNA clone sequencing, and toDenise Drudy for supplying C. difficile strain M68.
REFERENCES
1. Adachi, O., T. Kawai, K. Takeda, M. Matsumoto, H. Tsutsui, M. Sakagami,K. Nakanishi, and S. Akira. 1998. Targeted disruption of the MyD88 generesults in loss of IL-1- and IL-18-mediated function. Immunity 9:143–150.
2. Antonopoulos, D. A., S. M. Huse, H. G. Morrison, T. M. Schmidt, M. L.Sogin, and V. B. Young. 2009. Reproducible community dynamics of thegastrointestinal microbiota following antibiotic perturbation. Infect. Immun.77:2367–2375.
3. Arrich, J., G. H. Sodeck, G. Sengolge, C. Konnaris, M. Mullner, A. N.Laggner, and H. Domanovits. 2005. Clostridium difficile causing acute renalfailure: case presentation and review. World J. Gastroenterol. 11:1245–1247.
4. Barthel, M., S. Hapfelmeier, L. Quintanilla-Martinez, M. Kremer, M. Rohde,M. Hogardt, K. Pfeffer, H. Russmann, and W. D. Hardt. 2003. Pretreatmentof mice with streptomycin provides a Salmonella enterica serovar Typhi-murium colitis model that allows analysis of both pathogen and host. Infect.Immun. 71:2839–2858.
5. Bartlett, J. G. 2002. Clinical practice. Antibiotic-associated diarrhea.N. Engl. J. Med. 346:334–339.
6. Bartlett, J. G. 2006. Narrative review: the new epidemic of Clostridiumdifficile-associated enteric disease. Ann. Intern. Med. 145:758–764.
7. Bishara, J., N. Peled, S. Pitlik, and Z. Samra. 2008. Mortality of patientswith antibiotic-associated diarrhoea: the impact of Clostridium difficile. J.Hosp. Infect. 68:308–314.
8. Bohnhoff, M., B. L. Drake, and C. P. Miller. 1955. The effect of an antibioticon the susceptibility of the mouse’s intestinal tract to Salmonella infection.Antibiot. Annu. 3:453–455.
9. Borriello, S. P. 1998. Pathogenesis of Clostridium difficile infection. J. An-timicrob. Chemother. 41(Suppl. C):13–19.
10. Brandl, K., G. Plitas, C. N. Mihu, C. Ubeda, T. Jia, M. Fleisher, B. Schnabl,R. P. DeMatteo, and E. G. Pamer. 2008. Vancomycin-resistant enterococciexploit antibiotic-induced innate immune deficits. Nature 455:804–807.
11. Brazier, J. S. 2008. Clostridium difficile: from obscurity to superbug. Br J.Biomed Sci. 65:39–44.
12. Chang, J. Y., D. A. Antonopoulos, A. Kalra, A. Tonelli, W. T. Khalife, T. M.Schmidt, and V. B. Young. 2008. Decreased diversity of the fecal microbiomein recurrent Clostridium difficile-associated diarrhea. J. Infect. Dis. 197:435–438.
13. Chen, X., K. Katchar, J. D. Goldsmith, N. Nanthakumar, A. Cheknis, D. N.Gerding, and C. P. Kelly. 2008. A mouse model of Clostridium difficile-associated disease. Gastroenterology 135:1984–1992.
14. Croswell, A., E. Amir, P. Teggatz, M. Barman, and N. H. Salzman. 2009.Prolonged impact of antibiotics on intestinal microbial ecology and suscep-tibility to enteric Salmonella infection. Infect. Immun. 77:2741–2753.
15. DeSantis, T. Z., P. Hugenholtz, N. Larsen, M. Rojas, E. L. Brodie, K. Keller,T. Huber, D. Dalevi, P. Hu, and G. L. Andersen. 2006. Greengenes, achimera-checked 16S rRNA gene database and workbench compatible withARB. Appl. Environ. Microbiol. 72:5069–5072.
16. Dethlefsen, L., S. Huse, M. L. Sogin, and D. A. Relman. 2008. The pervasiveeffects of an antibiotic on the human gut microbiota, as revealed by deep 16SrRNA sequencing. PLoS Biol. 6:e280.
17. Dobson, G., C. Hickey, and J. Trinder. 2003. Clostridium difficile colitiscausing toxic megacolon, severe sepsis and multiple organ dysfunction syn-drome. Intensive Care Med. 29:1030.
18. Donskey, C. J., T. K. Chowdhry, M. T. Hecker, C. K. Hoyen, J. A. Hanrahan,A. M. Hujer, R. A. Hutton-Thomas, C. C. Whalen, R. A. Bonomo, and L. B.Rice. 2000. Effect of antibiotic therapy on the density of vancomycin-resistantenterococci in the stool of colonized patients. N. Engl. J. Med. 343:1925–1932.
19. Drudy, D., N. Harnedy, S. Fanning, R. O’Mahony, and L. Kyne. 2007.Isolation and characterisation of toxin A-negative, toxin B-positive Clostrid-ium difficile in Dublin, Ireland. Clin. Microbiol. Infect. 13:298–304.
20. Eckburg, P. B., E. M. Bik, C. N. Bernstein, E. Purdom, L. Dethlefsen, M.Sargent, S. R. Gill, K. E. Nelson, and D. A. Relman. 2005. Diversity of thehuman intestinal microbial flora. Science 308:1635–1638.
21. Fawley, W. N., S. Underwood, J. Freeman, S. D. Baines, K. Saxton, K.Stephenson, R. C. Owens, Jr., and M. H. Wilcox. 2007. Efficacy of hospitalcleaning agents and germicides against epidemic Clostridium difficile strains.Infect. Control Hosp. Epidemiol. 28:920–925.
22. Fukata, M., K. Breglio, A. Chen, A. S. Vamadevan, T. Goo, D. Hsu, D.Conduah, R. Xu, and M. T. Abreu. 2008. The myeloid differentiation factor88 (MyD88) is required for CD4� T cell effector function in a murine modelof inflammatory bowel disease. J. Immunol. 180:1886–1894.
23. Gerding, D. N. 2004. Clindamycin, cephalosporins, fluoroquinolones, andClostridium difficile-associated diarrhea: this is an antimicrobial resistanceproblem. Clin. Infect. Dis. 38:646–648.
24. Gerding, D. N., C. A. Muto, and R. C. Owens, Jr. 2008. Measures to controland prevent Clostridium difficile infection. Clin. Infect. Dis. 46(Suppl. 1):S43–S49.
25. Goorhuis, A., D. Bakker, J. Corver, S. B. Debast, C. Harmanus, D. W.Notermans, A. A. Bergwerff, F. W. Dekker, and E. J. Kuijper. 2008. Emer-gence of Clostridium difficile infection due to a new hypervirulent strain,polymerase chain reaction ribotype 078. Clin. Infect. Dis. 47:1162–1170.
26. Heap, J. T., O. J. Pennington, S. T. Cartman, G. P. Carter, and N. P. Minton.2007. The ClosTron: a universal gene knock-out system for the genus Clos-tridium. J. Microbiol. Methods 70:452–464.
27. Jacob, S. S., J. C. Sebastian, D. Hiorns, S. Jacob, and P. K. Mukerjee. 2004.Clostridium difficile and acute respiratory distress syndrome. Heart Lung33:265–268.
28. Jernberg, C., S. Lofmark, C. Edlund, and J. K. Jansson. 2007. Long-termecological impacts of antibiotic administration on the human intestinal mi-crobiota. ISME J. 1:56–66.
29. Kaisho, T., F. Schwenk, and K. Rajewsky. 1997. The roles of gamma 1 heavychain membrane expression and cytoplasmic tail in IgG1 responses. Science276:412–415.
30. Kawano, A., M. Ikeda, R. Iritani, A. Kinoshita, K. Watanabe, T. Hayao, T.Kokubo, and S. Matsushita. 2007. Colitis associated with Clostridium diffi-cile in specific-pathogen-free C3H-scid mice. J. Vet. Med. Sci. 69:973–975.
31. Kelly, C. P., and J. T. LaMont. 2008. Clostridium difficile—more difficultthan ever. N. Engl. J. Med. 359:1932–1940.
32. Kuipers, E. J., and C. M. Surawicz. 2008. Clostridium difficile infection.Lancet 371:1486–1488.
33. Kyne, L., M. Warny, A. Qamar, and C. P. Kelly. 2000. Asymptomatic car-riage of Clostridium difficile and serum levels of IgG antibody against toxinA. N. Engl. J. Med. 342:390–397.
34. Lawley, T. D., D. M. Bouley, Y. E. Hoy, C. Gerke, D. A. Relman, and D. M.Monack. 2008. Host transmission of Salmonella enterica serovar Typhi-murium is controlled by virulence factors and indigenous intestinal micro-biota. Infect. Immun. 76:403–416.
35. Ley, R. E., M. Hamady, C. Lozupone, P. J. Turnbaugh, R. R. Ramey, J. S.Bircher, M. L. Schlegel, T. A. Tucker, M. D. Schrenzel, R. Knight, and J. I.Gordon. 2008. Evolution of mammals and their gut microbes. Science 320:1647–1651.
36. Lloyd-Smith, J. O., S. J. Schreiber, P. E. Kopp, and W. M. Getz. 2005.Superspreading and the effect of individual variation on disease emergence.Nature 438:355–359.
37. Lockwood, J. L., M. F. Hoopes, and M. P. Marchetti. 2007. Invasion ecology,vol. 1. Blackwell Publishing, Oxford, United Kingdom.
38. Lyras, D., J. R. O’Connor, P. M. Howarth, S. P. Sambol, G. P. Carter, T.Phumoonna, R. Poon, V. Adams, G. Vedantam, S. Johnson, D. N. Gerding,and J. I. Rood. 2009. Toxin B is essential for virulence of Clostridiumdifficile. Nature 458:1176–1179.
39. Merrell, D. S., S. M. Butler, F. Qadri, N. A. Dolganov, A. Alam, M. B. Cohen,S. B. Calderwood, G. K. Schoolnik, and A. Camilli. 2002. Host-inducedepidemic spread of the cholera bacterium. Nature 417:642–645.
40. O’Connor, J. R., D. Lyras, K. A. Farrow, V. Adams, D. R. Powell, J. Hinds,
3668 LAWLEY ET AL. INFECT. IMMUN.
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from

J. K. Cheung, and J. I. Rood. 2006. Construction and analysis of chromo-somal Clostridium difficile mutants. Mol. Microbiol. 61:1335–1351.
41. Onderdonk, A. B., R. L. Cisneros, and J. G. Bartlett. 1980. Clostridiumdifficile in gnotobiotic mice. Infect. Immun. 28:277–282.
42. Ozaki, E., H. Kato, H. Kita, T. Karasawa, T. Maegawa, Y. Koino, K. Ma-tsumoto, T. Takada, K. Nomoto, R. Tanaka, and S. Nakamura. 2004. Clos-tridium difficile colonization in healthy adults: transient colonization andcorrelation with enterococcal colonization. J. Med. Microbiol. 53:167–172.
43. Paredes, C. J., K. V. Alsaker, and E. T. Papoutsakis. 2005. A comparativegenomic view of clostridial sporulation and physiology. Nat. Rev. Microbiol.3:969–978.
44. Rakoff-Nahoum, S., J. Paglino, F. Eslami-Varzaneh, S. Edberg, and R.Medzhitov. 2004. Recognition of commensal microflora by Toll-like recep-tors is required for intestinal homeostasis. Cell 118:229–241.
45. Razaq, N., S. Sambol, K. Nagaro, W. Zukowski, A. Cheknis, S. Johnson, andD. N. Gerding. 2007. Infection of hamsters with historical and epidemic BItypes of Clostridium difficile. J. Infect. Dis. 196:1813–1819.
46. Riggs, M. M., A. K. Sethi, T. F. Zabarsky, E. C. Eckstein, R. L. Jump, andC. J. Donskey. 2007. Asymptomatic carriers are a potential source for trans-mission of epidemic and nonepidemic Clostridium difficile strains amonglong-term care facility residents. Clin. Infect. Dis. 45:992–998.
47. Riley, T. V., J. S. Brazier, H. Hassan, K. Williams, and K. D. Phillips. 1987.Comparison of alcohol shock enrichment and selective enrichment for theisolation of Clostridium difficile. Epidemiol. Infect. 99:355–359.
48. Rupnik, M. 2007. Is Clostridium difficile-associated infection a potentiallyzoonotic and foodborne disease? Clin. Microbiol. Infect. 13:457–459.
49. Schloss, P. D., and J. Handelsman. 2005. Introducing DOTUR, a computerprogram for defining operational taxonomic units and estimating speciesrichness. Appl. Environ. Microbiol. 71:1501–1506.
50. Sekirov, I., N. M. Tam, M. Jogova, M. L. Robertson, Y. Li, C. Lupp, and B. B.Finlay. 2008. Antibiotic-induced perturbations of the intestinal microbiotaalter host susceptibility to enteric infection. Infect. Immun. 76:4726–4736.
51. Songer, J. G., and M. A. Anderson. 2006. Clostridium difficile: an importantpathogen of food animals. Anaerobe 12:1–4.
52. Stabler, R. A., D. N. Gerding, J. G. Songer, D. Drudy, J. S. Brazier, H. T.Trinh, A. A. Witney, J. Hinds, and B. W. Wren. 2006. Comparative phylog-enomics of Clostridium difficile reveals clade specificity and microevolution ofhypervirulent strains. J. Bacteriol. 188:7297–7305.
53. Stecher, B., and W. D. Hardt. 2008. The role of microbiota in infectiousdisease. Trends Microbiol. 16:107–114.
54. Stecher, B., R. Robbiani, A. W. Walker, A. M. Westendorf, M. Barthel, M.Kremer, S. Chaffron, A. J. Macpherson, J. Buer, J. Parkhill, G. Dougan, C.
von Mering, and W. D. Hardt. 2007. Salmonella enterica serovar Typhi-murium exploits inflammation to compete with the intestinal microbiota.PLoS Biol. 5:2177–2189.
55. Stragier, P., and R. Losick. 1996. Molecular genetics of sporulation in Ba-cillus subtilis. Annu. Rev. Genet. 30:297–341.
56. Vaishnava, S., C. L. Behrendt, A. S. Ismail, L. Eckmann, and L. V. Hooper.2008. Paneth cells directly sense gut commensals and maintain homeostasisat the intestinal host-microbial interface. Proc. Natl. Acad. Sci. USA 105:20858–20863.
57. Vernet, A., G. Corthier, F. Dubos-Ramare, and A. L. Parodi. 1989. Rela-tionship between levels of Clostridium difficile toxin A and toxin B and cecallesions in gnotobiotic mice. Infect. Immun. 57:2123–2127.
58. Vollaard, E. J., and H. A. Clasener. 1994. Colonization resistance. Antimi-crob. Agents Chemother. 38:409–414.
59. Vonberg, R. P., E. J. Kuijper, M. H. Wilcox, F. Barbut, P. Tull, P. Gastmeier,P. J. van den Broek, A. Colville, B. Coignard, T. Daha, S. Debast, B. I.Duerden, S. van den Hof, T. van der Kooi, H. J. Maarleveld, E. Nagy, D. W.Notermans, J. O’Driscoll, B. Patel, S. Stone, and C. Wiuff. 2008. Infectioncontrol measures to limit the spread of Clostridium difficile. Clin. Microbiol.Infect. 14(Suppl. 5):2–20.
60. Wiles, S., W. P. Hanage, G. Frankel, and B. Robertson. 2006. Modellinginfectious disease—time to think outside the box? Nat. Rev. Microbiol.4:307–312.
61. Wiles, S., K. M. Pickard, K. Peng, T. T. MacDonald, and G. Frankel. 2006.In vivo bioluminescence imaging of the murine pathogen Citrobacter roden-tium. Infect. Immun. 74:5391–5396.
62. Wilson, K. H. 1983. Efficiency of various bile salt preparations for stimula-tion of Clostridium difficile spore germination. J. Clin. Microbiol. 18:1017–1019.
63. Wilson, K. H., M. J. Kennedy, and F. R. Fekety. 1982. Use of sodiumtaurocholate to enhance spore recovery on a medium selective for Clostrid-ium difficile. J. Clin. Microbiol. 15:443–446.
64. Woolhouse, M. E., C. Dye, J. F. Etard, T. Smith, J. D. Charlwood, G. P.Garnett, P. Hagan, J. L. Hii, P. D. Ndhlovu, R. J. Quinnell, C. H. Watts, S. K.Chandiwana, and R. M. Anderson. 1997. Heterogeneities in the transmissionof infectious agents: implications for the design of control programs. Proc.Natl. Acad. Sci. USA 94:338–342.
65. Xavier, R. J., and D. K. Podolsky. 2007. Unravelling the pathogenesis ofinflammatory bowel disease. Nature 448:427–434.
66. Yu, J., R. Rossi, C. Hale, D. Goulding, and G. Dougan. 2009. Interaction ofenteric bacterial pathogens with murine embryonic stem cells. Infect. Im-mun. 77:585–597.
Editor: R. P. Morrison
VOL. 77, 2009 INDUCTION OF C. DIFFICILE DISEASE AND TRANSMISSION 3669
on October 30, 2020 by guest
http://iai.asm.org/
Dow
nloaded from