Antibiotic policy
40
Iman M. Fawzy; MD, MSc, PhD Consultant of Clinical Pathology
-
Upload
mona-mustafa -
Category
Health & Medicine
-
view
55 -
download
3
Transcript of Antibiotic policy

Iman M. Fawzy; MD, MSc, PhD
Consultant of Clinical Pathology

Rational Use of Antibiotics
The conference of experts on the rational use of drugs, by the WHO in 1985defined that
“Rational use of drugs requires that patientsreceive medications appropriately to theirclinical needs, in doses that meet their ownindividual requirements for an adequate periodof time, at the lowest cost to them and theircommunity”

Reasons for
Patient Concerns
• Want clear explanation
• Green nasal discharge
• Need to return to work
Physician Concerns
• Patient expects antibiotic
• Diagnostic uncertainty
• Time pressure
Antibiotic Prescription
Antibiotic Overuse
What is inappropriate use ?
Unnecessary prescription of antibiotics, such as for viral infections or for prolonged prophylaxis
Using broad-spectrum antibiotics when narrow-spectrum antibiotics are effective
Prescribing too low or too high dose
Continuing treatment for longer than necessary

What is inappropriate use ?
Not prescribing according to microbiology results
Omitting or delaying administration of doses
Prescribing intravenous therapy when oral therapy is known to be effective and clinically safe
Not taking antibiotics as prescribed

Antibiotic Resistance

New Resistant Bacteria
Emergence of Antibiotic Resistance
Susceptible
Bacteria
Resistant Bacteria
Resistance Gene Transfer

Resistant StrainsRare
Resistant Strains Dominant
Antimicrobial Exposure
Selection for Antibiotic-Resistant Strains
Antimicrobial resistance has emerged as a major public health problem all over the world
Infections by resistant microbes treatment fail↑morbidity ↑mortality.
Treatment failure longer infectivity, ↑infected people in community.
exposes general population to risk of resistant strains
Resistant to first-line antimicrobials, high cost of the second-line drugs treatment failure
Most alarming caused by multidrug-resistant microbes, which are virtually non-treatable and thereby create a “post-antibiotic era” scenario

Emergence of antibiotic resistance
5. Pray LA Insight Pharma Reports 2008, in Looke D ‘The Real Threat of Antibiotic Resistance’ 2012

Resistance spreads rapidly


Impact of resistance
Untreatable infections
Excess length of
stay
Increased morbidity/
mortality
Increased costs
Interference with patient’s normal flora.
Selection of drug resistant organisms
Increased side effects
Settings that favor antimicrobial resistance
Immune compromised patients e.g.
– ICU
– Oncology unit
– Dialysis unit
– Rehabilitation unit
– Transplantation unit
– Burn unit


Acute otitis
media
Respiratory tract
infection
AB resistance problem
Not only in hospitals
Urinary tract
infection
DiarrheaDental manipulation

we have to fight against the irrational use
save these important discoveries of man
Inappropriate use of antibiotics (life-saving (many problems
not many new antimicrobials
have been discovered since
the 1980th
funding on antimicrobial research is on
the decline

Antibiotic policy

Aim of Antibiotic Policy↓↓ morbidity and
mortality due to antimicrobial-resistant
infection
Preserve the effectiveness of antimicrobial agents in
treatment
Prevention of communicable diseases

Detect resistant microorganisms
Ensure effective treatment
Recognize trends in antimicrobial resistance within the institution
Assure infection control procedures
Plan for identifying,transferring, discharging andreadmitting patientscolonized with specificantimicrobial resistantpathogens
Incorporate the detection,prevention and control ofantimicrobial resistanceinto institutional strategicgoals
Rational use of antimicrobials
Objectives of Antibiotic Policy

Organizational structure of
antibiotic policy
Clinicians
Microbiologists
Pharmacists
Nurses
ANTIBIOTIC COMMITTEE
infection control
committee
Scope of hospital antibiotic policy
prophylaxis, empirical and definitive therapy.
high-risk/special groups e.g. immune compromised hosts;hospital-associated infections and community-associatedinfections.
The hospital antibiotic policy shall be based upon:
– spectrum of antibiotic activity
– pharmacokinetics/pharmacodynamics of antibiotic s
– adverse effects
– potential to select resistance
– cost
– special needs of individual patient groups.
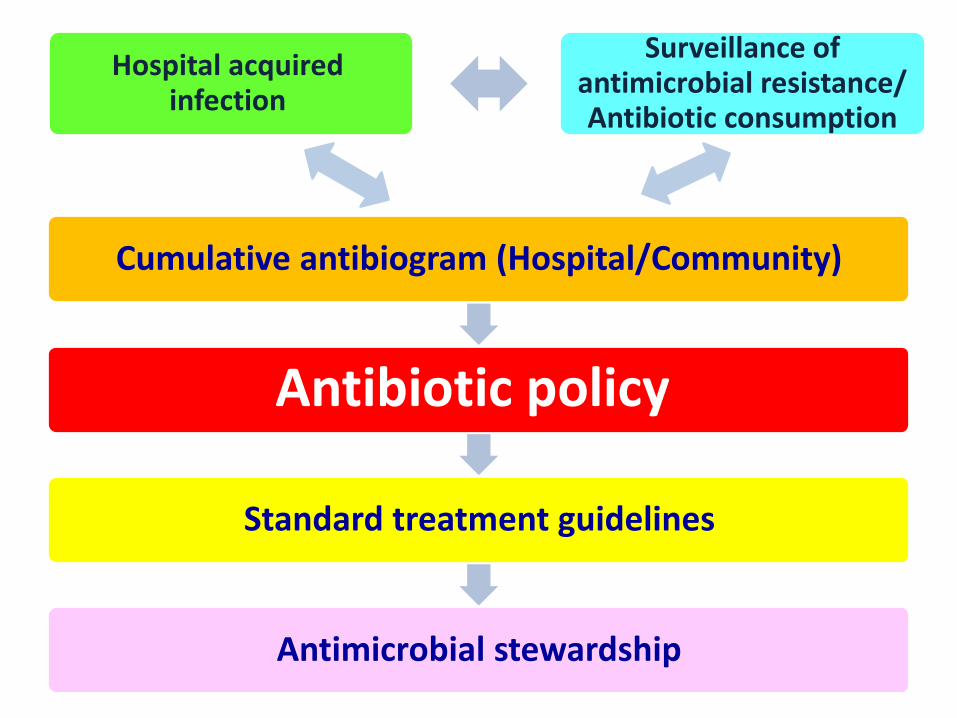
Cumulative antibiogram (Hospital/Community)
Antibiotic policy
Standard treatment guidelines
Antimicrobial stewardship
Hospital acquired infection
Surveillance of antimicrobial resistance/ Antibiotic consumption

Surveillance of antimicrobialresistance
• Use standards
• Generate reliable numerator: only the first positive culture from the patient for each disease episode should be reported for surveillance purposes.
• Express resistance as incidence rate
• Participate in external quality assessment schemes
• Prediction of evolution of antimicrobial resistance
• Surveillance of antimicrobial consumption

Cumulative antibiogram
• Analyses of data regularly, at least annually.
• Inclusion of diagnostic isolates.
• It is useful to stratify results by specimens type orinfection site, by nursing unit or site of care, byorganism’s resistance characteristics, by clinicalservice or patient population.
• Reviewing the cumulative antibiogram data if clinicalfailure occurs after empiric therapy.
• Comparing the cumulative antibiogram with nationaldata.

Development of standard treatment guidelines
• Should be based on local antibiograms.
• Should be syndrome/diseased based.
• Should specify type of clinical setting – Outpatientclinics, Inpatient units, ICU setting.
• Should involve treating physicians to bring ownershipto the guidelines
Direction of antibiotic policy
Frame the hospital own list of therapeutic antibioticcategories:• First-line• Reserved agents• Restricted agents• Withdrawn agentsfor example, first choice antibiotics can be prescribed by alldoctorswhile restricted choice antibiotics can only be prescribed afterconsulting the head of the department or the antimicrobialteam (AMT) representative.Reserve antibiotics, are prescribed only by designated experts.

Minimizing selection of resistant organisms
What should not be done• Treat non-infectious or nonbacterial
syndrome.
• Treat colonization or contamination.
• Treat longer than necessary.
• Fail to make adjustment in a timely manner.
• Prescribe antibiotic with spectrum of activitynot indicated.

Interventions
Continuous surveillance of bacterial infections.
Hospital acquired infection
Community acquired infection

Interventions
• Prohibiting the sale of antibiotics withoutmedical prescription.
• Development of regulations by Ministries ofHealth regarding responsible prescription ofantibiotics.
• Prohibition of advertising of antibiotics in thecommunity by industry and pharmaceuticalrepresentatives.

Community pharmacist
• Pharmacist should be able to prescribe certainantibiotics in appropriate circumstances topatients needing treatment for particularconditions
• Advice to patients to ensure that the patientunderstands that:– Antibiotic must be used properly
– Help and encourage Health Authorities.
– Ensure the implementation of the policies

Prevent Antimicrobial Resistance
12 Contain your contagion11 Isolate the pathogen
10 Stop treatment when cured9 Know when to say “no” to antibiotic
8 Treat infection, not colonization7 Treat infection, not contamination
6 Use local data5 Practice antimicrobial control
4 Access the experts3 Target the pathogen
2 Get the catheters out1 Vaccinate
Prevent Transmission
Use Antimicrobials Wisely
Diagnose and Treat Effectively
Prevent Infection
Clinicians hold the solution…

Antimicrobial Resistance:
Key Prevention Strategies
Optimize
Use
Prevent
Transmission
Prevent
Infection
Effective
Diagnosis
and Treatment
Pathogen
Antimicrobial-Resistant
Pathogen
Antimicrobial Resistance
Antimicrobial Use
Infection
Susceptible Pathogen

Antibiotic prescribing
Indication for use (definitive, empirical,
prophylaxis)
Route of administration,
dosage regimen, duration of
treatment, adverse effects
If the drug was on a
reserved list
Drug combinations
Whether it was approved by a microbiologist
Was culture and sensitivity
performed
Development of treatment
guidelines

ANTIMICROBIAL PRESCRIBING: GOOD PRACTICES
• Send for appropriate investigations in all infections.
• All antibiotic initiations would be done after sendingappropriate cultures
• Follow Hospital policy when choosing antimicrobial therapywhenever possible.
• Check for factors which will affect drug choice, eg, renalfunction, interactions, allergy.
• Check that the appropriate dose is prescribed.
• The need for antimicrobial therapy should be reviewed on adaily basis.
• Once culture reports are available, the physician shall stepdown to the narrowest spectrum, most efficacious and mostcost effective option.

Empiric Therapy
Where delay in initiating therapy to awaitmicrobiological results would be life threatening or riskserious morbidity, antimicrobial therapy based on aclinically defined infection is justified.
Where empiric therapy is used, the accuracy ofdiagnosis should be reviewed regularly and treatmentaltered/stopped when microbiological results becomeavailable.

Empiric Therapy
Side effects empirical antibiotics :
• Development of resistance in pathogens infecting thepatient.
• Risk for spread of resistance.
• Suppression of normal flora.
• Development of resistance in normal flora.
• Risk for super infection.

Hand Washing is Important Because…
Hand hygiene compliance rates of 10%-40% have been observed in the developed
countries.

• Policy should be reviewed by expertswho are not the members of thepolicy development group, but areexperts in the relevant field.
Revise policy
• Policy is not static. It is a livingdocument. It should be reviewed atperiodic intervals, updated accordingto current medical knowledge, clinicalpractice and local circumstances.
Revise policy

THANK YOU