Antiarrhythmic Drugs Dr. Tom Murray Department of Pharmacology.
86
Antiarrhythmic Drugs Dr. Tom Murray Department of Pharmacology
-
Upload
dustin-burke -
Category
Documents
-
view
242 -
download
3
Transcript of Antiarrhythmic Drugs Dr. Tom Murray Department of Pharmacology.

Antiarrhythmic Drugs
Dr. Tom MurrayDepartment of Pharmacology

Voltage-gated ion channels
QuickTime™ and aSorenson Video 3 decompressorare needed to see this picture.

Nerbonne, J. M. et al. Physiol. Rev. 85: 1205-1253 2005;doi:10.1152/physrev.00002.2005
Action potential waveforms and underlying ionic currents in adult human and ventricular (left) and atrial (right) myocytes
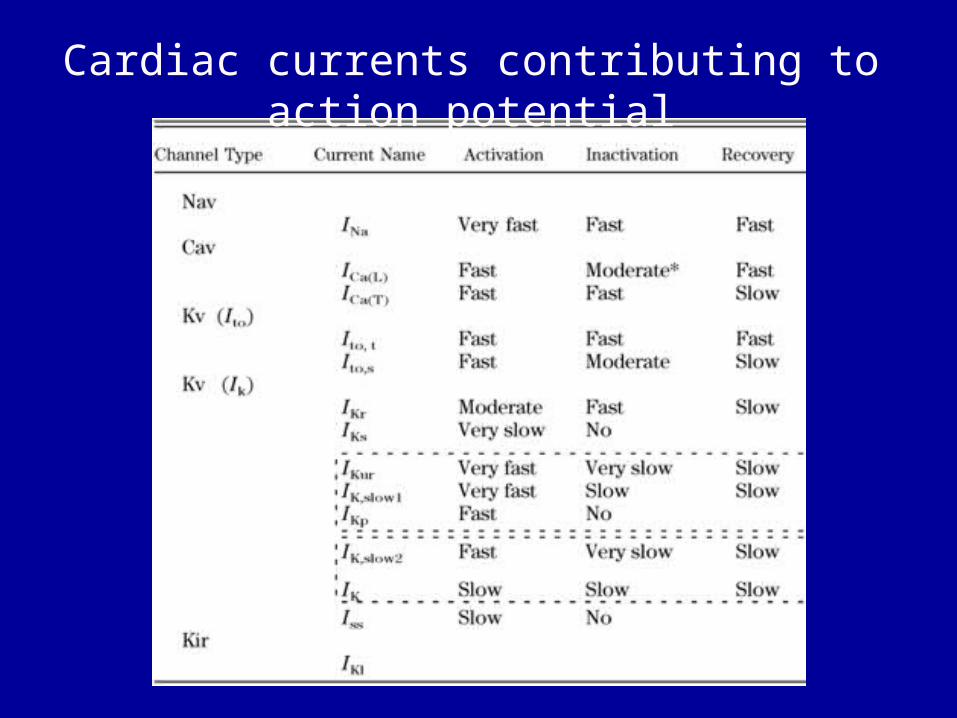
Cardiac currents contributing to action potential


Copyright ©2005 American Society for Clinical Investigation
George, A. L. J. Clin. Invest. 2005;115:1990-1999
Functional properties of NaVChs

Nerbonne, J. M. et al. Physiol. Rev. 85: 1205-1253 2005;doi:10.1152/physrev.00002.2005
Molecular assembly of cardiac Cav (Nav), Kv, and Kir channels

Nerbonne, J. M. et al. Physiol. Rev. 85: 1205-1253 2005;doi:10.1152/physrev.00002.2005
Pore-forming ({alpha}) subunits of cardiac Nav (A) and Kv (B and C) channels linked to inherited arrhythmias

Nerbonne, J. M. et al. Physiol. Rev. 85: 1205-1253 2005;doi:10.1152/physrev.00002.2005
Simulated human ventricular action potentials reveal the impact of gain of function (LQT3) and loss of function (Brugada) mutations in SCN5A


Loss of function mutation in hERG cause LQT1

Drugs That May Cause Torsade de Pointes


Mechanisms of Cardiac Arrhythmias
• Enhanced automaticity• Afterdepolarizations and triggered automaticity
• Re-entry

Afterdepolarizations and triggered activity

Reentry circuit in small branches of Purkinje system

Antiarrhythmic drug actions
• Alter function of ion channels
• Interfere with autonomic control

Electrophysiological Parameters
Conduction Velocity
Refractory Period

Curve relating Vmax to the resting membrane potential at the onset of action potential

ANTIARRHYTHMIC DRUGS• Class I – block Na+ channels
• IA – medium• IB – fast• IC – slow
– IA: quinidine, procainamide (reduce automaticity, delay conduction, increase refractory period)
– IB: lidocaine, mexilitine, tocainide (reduce ectopic automaticity)
– IC: flecainide, propafenone (reduce automaticity, delay conduction)

• Class II: -Adrenergic receptor blockers (propranolol, esmolol) (reduce automaticity, delay conduction)
• Class III Block K+ channels (amiodarone, ibutilide, sotalol) (delay repolarization, increase refractory period, reduce automaticity)
ANTIARRHYTHMIC DRUGS

• Class IV: Block Ca2+ channels (verapamil, diltiazem) (reduce conduction velocity, reduce automaticity)
• Adenosine: Stimulates adenosine A1 receptors ( reduces conduction velocity, reduces automaticity)
ANTIARRHYTHMIC DRUGS


Sites ofAction of
Drugs

Quinidine

Background• Discovered from effects of quinine
(from cinchona) - quinidine from same plant
• Beginning in the 1920s, quinidine was used as an antiarrhythmic agent

Quinidine pharmacological actions
• Inhibits VGSC (open channel blocker)
• Inhibits delayed rectifier K+ channels
• Muscarinic receptor antagonist• Alpha adrenergic receptor antagonist

Effects• Antimuscarinic – potential increase in AV nodal
transmission of atrial tachycardias• Increased threshold for excitability and
decreased automaticity• Reduces conduction velocity (decreases slope
of phase 0)• Increases duration of QRS (delays conduction)• Increases duration of QT interval (delays
repolarization)• Vasodilation

Adverse Reactions• Cinchonism: dizziness, tinnitus• Nausea, vomiting and diarrhea• Depressed myocardial contractility• Hypotension and syncope• Ventricular arrhythmia (2-8% of patients
develop torsades de pointes)

Uses of Quinidine• Maintain sinus rhythm in patients with atrial flutter or
atrial fibrillation prevent recurrence of ventricular tachycardia or ventricular fibrillation
• Prevent recurrence of ventricular tachycardia or ventricular fibrillation
• Use has diminished due to high incidence of proarrhythmias

Procainamide
•Similar to quinidine in electrophysiological effects – similar to procaine (Novocaine) in structure, weaker antimuscarinic and a-adrenergic effects compared to quinidine.•Blocker of open Na+ channels with an intermediate time constant of recovery from block. Also prolongs cardiac action potentials in most tissues probably by blocking outward K+ current(s).

Adverse reactions• Dose-related nausea is frequent during oral therapy
• Hypotension and marked slowing of conduction are major adverse effects of high concentrations
• Potentially fatal bone marrow aplasia in 0.2% of patients

Uses• Used in the acute therapy of many supraventricular and ventricular arrhythmias
Disopyramide•Electrophysiologic effects similar to quinidine•Prominent anticholinergic effects (precipitation of glaucoma, constipation, dry mouth, and urinary retention)•Commonly depresses contractility, which can precipitate heart failure•Used to maintain sinus rhythm in patients with atrial flutter or atrial fibrillation and to prevent recurrence of ventricular tachycardia or ventricular fibrillation

Lidocaine
Effects• Blocks both open and inactivated cardiac Na+
channels• Decreases automaticity especially in ectopic
pacemakers• Not useful in atrial arrhythmias possibly
because atrial action potentials are so short that the Na+ channel is in the inactivated state only briefly

Adverse Reactions• Large intravenous doses of lidocaine administered rapidly may produce seizures
• Tremor, dysarthria, and altered levels of consciousness more common

Uses•Acute intravenous therapy of ventricular arrhythmias

Mexilitine

Mexilitine - Effects• Congener of, and similar to,
lidocaine
• Orally effective
• Used in treatment of ventricular arrhythmias

Flecainide

Effects• Reduces conduction velocity (phase 0)
• Very long recovery from Na+ channel block
• Prolongs the duration of PR, QRS, and QT intervals
• Decreases sinus node automaticity

Adverse Effects• Dose-related blurred vision is the most
common noncardiac adverse effect
• Cardiac risk in patients with recent myocardial infarction – reentrant tachycardia

Use• Maintenance of sinus rhythm in patients with supraventricular arrhythmias
• In the CAST study, flecainide increased mortality in patients convalescing from myocardial infarction
Propafenone

Effects• Depresses inward sodium current
(phase 0) - Reduces conduction velocity
• Reduces automaticity
• S-(+)-propafenone is a -adrenergic receptor antagonist

Adverse Effects• Contraindicated in severe heart failure,
disorders of conduction, bradycardia
• Increased frequency or severity of episodes of re-entrant ventricular tachycardia
• Adverse effects of -adrenergic blockade, such as sinus bradycardia and bronchospasm

Indications• Used to maintain sinus rhythm in patients with supraventricular tachycardias
• It also can be used in ventricular arrhythmias

adrenergic receptor blockers - propanolol
• Effectsblockade• Quinidine-like effect• Reduces automaticity of SA node• Reduces automaticity and
conduction velocity in AV node, His Purkinje and ventricles

Adverse effects• Reduced myocardial contractility
• Bradycardia
• Angina upon sudden withdrawal
• Bronchospasm

Uses• Supraventricular tachycardia
• Many studies indicate that, unlike flecainide, blockers provide prominent beneficial effect after myocardial
infarction.

Esmolol
• Short-acting -adrenergic receptor blocker
• Given IV for a rapid effect

Amiodarone

Amiodarone effects• Blocks K+, Na+ and Ca2+ channels and eta
adrenoceptors• Delays repolarization and increases the
refractory period• Decreases automaticity• Slows conduction• A vasodilator• Increased coronary blood flow

Amiodarone (adverse effects)• Conduction abnormalities• Pulmonary fibrosis• Reduced contractility of heart• Thyroid abnormalities • Hypotension with IV use • Skin (photosensitivity), cornea, peripheral neuropathy• Despite the marked QT prolongation and bradycardia typical of chronic amiodarone therapy, torsades de pointes and other drug-induced tachyarrhythmias are unusual.

Amiodarone (uses)• Recurrent ventricular tachycardia or fibrillation resistant to other drugs
• Maintaining sinus rhythm in patients with atrial fibrillation
• IV dosage form supplanting lidocaine as first-line therapy for out-of-
hospital cardiac arrest

Sotalol• A Class III drug• Prolongs cardiac action potentials by inhibiting delayed rectifier and possibly other K+ currents
• l-enantiomer is a much more potent -adrenergic receptor antagonist than the d-enantiomer, but the two are equipotent as K+ channel blockers
• Used in patients with both ventricular tachyarrhythmias and atrial fibrillation or flutter
• Torsades de pointes is the major toxicity with sotalol overdose

Ibutilide
• An IKr blocker that in some systems also activates an inward Na+ current
• Administered as a rapid infusion (1 mg over 10 minutes) for the immediate conversion of atrial fibrillation or flutter to sinus rhythm
• Major toxicity with ibutilide is torsades de pointes, which occurs in up to 6% of patients

Calcium channel blockers –Verapamil, Diltiazem
• Block slow inward Ca2+ current• Reduce automaticity• Increase refractory period and decrease
conduction velocity of AV Node• Inhibit contractility• Vasodilatation

Calcium channel blockers (adverse effects)
• Flushing etc.• Reduced contractility of the heart• AV node conduction defects• Constipation
Use• Supraventricular arrhythmias

Adenosine
• Adenosine released by most cells
• Normal plasma levels ~300 nM• Can reach micromolar levels in ischemic tissue

Adenosine Metabolism

Adenosine Receptors
• Four receptor subtypes have been classified:– A1, A2A, A2B, A3 (Fredholm, 1993)
• All four subtypes are G-protein coupled receptors
• Methylxanthines such as caffeine and theophylline are competitive antagonists
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Adenosine receptors

G-Protein Coupled Receptors
• Seven-spanning transmembrane proteins
QuickTime™ and aSorenson Video 3 decompressorare needed to see this picture.
QuickTime™ and aSorenson Video 3 decompressorare needed to see this picture.
QuickTime™ and aSorenson Video 3 decompressorare needed to see this picture.

Adenosine (effects)
• Stimulates adenosine receptors (A1 receptors in the heart)
• Increases K+ conductance
• Inhibits opening of Ca2+ channels
• Reduces norepinephrine release
• Reduces automaticity and AV nodal conduction

Adenosine (adverse effects)
• Flushing
• Asthma – dyspnea – chest pain
• SA nodal arrest, AV nodal block

Other Drugs• Dofetilide
– A “pure” class III antiarrhythmic – Potent and "pure" IKr blocker– Can prolong the QT interval– Maintenance of sinus rhythm in patients with atrial
fibrillation
• Moricizine– A class IC antiarrhythmic– A phenothiazine– Used for ventricular arrhythmias– Has active metabolites


Appendix

Nerbonne, J. M. et al. Physiol. Rev. 85: 1205-1253 2005;doi:10.1152/physrev.00002.2005
Electrical activity in the myocardium


Diversity of inward rectifying potassium channels



Control of membrane potential
* if the membrane potential (Em) equals Nernst potential for an ion (Eion), there will be no net flux of that ion across the membrane * illustration: * vary membrane potential of cell (Em) while measuring flux of K+ * when Em = EK, no flux * when Em is more negative (-65 mV) than EK (-55 mV) as in hyperkalemia, influx of K+ (K+ flows into of cell) * influx of K+ makes the membrane potential less negative = depolarization * when Em (-65 mV) is more positive than EK (-90 mV), efflux of K+ (K+ flows out of cell) * efflux of K+ makes the membrane potential more negative = hyperpolarization
* thus, when the the equilibrium potential for a permeant ion differs from the membrane potential, that ion will tend to flow across membrane so as to draw the membrane potential closer to its equilibrium potential

Ionic currents• Each current is distinguished by ion selectivity, time course and voltage dependence
• Properties conferred by transmembrane proteins: ion channels
• Ion channels permit passage of 100,000 ions per second per channel due to passive movement of ions down their concentration gradient
• When ion channels open they bias membrane potential towards the equilibrium potential for that ion (eg. K+ channels -90 mV; Na+ channels +60)
• Channels are gated by voltage and may display rapid inactivation (eg. Na+ channels)

Diversity of voltage-gated sodium channels


Voltage-
gated sodium channe
l
QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.



Cardiac ion
channels

Differences in responses of fast- and slow-response tissues to
premature stimuli

Requirements for induction of reentryRequirements for induction of reentry
trigger unidirectional block excitable gap
exctitable gap(non-refractory tissue)
unidirectional block(prevents wavefronts collision)
trigger

Influence of hyperkalemia on cardiac action
potential