
Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab
7
1. Introduction 2. Bevacizumab and ranibizumab 3. Anti-VEGF antibodies in neovascular glaucoma 4. Anti-VEGF antibodies in glaucoma filtration surgery 5. Conclusion 6. Expert opinion Review Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab Sung Chul Park, Daniel Su & Celso Tello † † Department of Ophthalmology, The New York Eye and Ear Infirmary, New York, NY, USA Introduction: Anti-VEGF therapy has been widely used in the treatment of ocular neovascular diseases. Because of their anti-angiogenic and anti-fibrotic properties, anti-VEGF antibodies such as bevacizumab and ranibizumab have emerged as an adjunctive treatment modality in glaucoma to improve success of conventional treatments. Areas covered: Ranibizumab is an anti-VEGF-A antigen binding fragment currently indicated in neovascular age-related macular degeneration as well as macular edema following retinal vein occlusion. Several off-label uses include the treatment of neovascular glaucoma to regress/suppress iris and iridocorneal angle neovascularization and the modulation of wound healing after glaucoma filtration surgery. Bevacizumab is a full-length anti-VEGF antibody, which is also being used in aforementioned eye conditions off-label. An overview of these anti-VEGF antibodies and the results of preclinical and clinical studies regarding their use in the treatment of glaucoma are presented. Expert opinion: Early studies on the utility of both bevacizumab and ranibi- zumab in neovascular glaucoma and filtration surgery reported promising results. However, a large-scale randomized clinical trial as well as comparative studies between the two anti-VEGF antibodies are currently lacking. A single dose of ranibizumab costs approximately 40 times as much as a single dose of bevacizumab. Clinicians should take this into account, in addition to their differences in the efficacy and safety, when treating patients. Keywords: anti-VEGF, bevacizumab, glaucoma filtration surgery, neovascular glaucoma, ranibizumab, trabeculectomy, vascular endothelial growth factor, wound healing Expert Opin. Biol. Ther. (2012) 12(12):1641-1647 1. Introduction First discovered in 1983 as a molecule secreted by tumor cells to increase vascular permeability [1], vascular endothelial growth factor (VEGF) was later found to be produced in tumors that outgrow their oxygen supply. The hypothesis that VEGF was responsible for hypoxia-mediated angiogenesis in ischemic tissue was streng- thened when VEGF mRNA levels were reported to be dramatically increased within a few hours of exposing different cell cultures to hypoxia and return to background when normal oxygen supply was resumed [2]. Furthermore, it was discovered that VEGF was consistently expressed in samples of intraocular neovascular membranes obtained from patients with proliferative diabetic retinopathy and that intravitreal VEGF levels were increased in patients with proliferative diabetic retinopathy as well as other ischemic retinal diseases [3-5]. These discoveries have led to the development of VEGF inhibitors in order to reduce pathologic angiogenesis. There are currently two anti-VEGF antibodies used in therapy. Bevacizumab, a humanized IgG1 monocolonal antibody against all isoforms of VEGF-A [6], is used in combination with intravenous 5-fluorouracil (5-FU)-based chemotherapy as the first- or second-line treatment of metastatic carcinoma of the colon and 10.1517/14712598.2012.721772 © 2012 Informa UK, Ltd. ISSN 1471-2598 1641 All rights reserved: reproduction in whole or in part not permitted Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by University of Connecticut on 05/22/13 For personal use only.
Transcript of Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab

1. Introduction
2. Bevacizumab and ranibizumab
3. Anti-VEGF antibodies in
neovascular glaucoma
4. Anti-VEGF antibodies in
glaucoma filtration surgery
5. Conclusion
6. Expert opinion
Review
Anti-VEGF therapy for thetreatment of glaucoma: a focus onranibizumab and bevacizumabSung Chul Park, Daniel Su & Celso Tello††Department of Ophthalmology, The New York Eye and Ear Infirmary, New York, NY, USA
Introduction: Anti-VEGF therapy has been widely used in the treatment of
ocular neovascular diseases. Because of their anti-angiogenic and anti-fibrotic
properties, anti-VEGF antibodies such as bevacizumab and ranibizumab have
emerged as an adjunctive treatment modality in glaucoma to improve success
of conventional treatments.
Areas covered: Ranibizumab is an anti-VEGF-A antigen binding fragment
currently indicated in neovascular age-related macular degeneration as well
as macular edema following retinal vein occlusion. Several off-label uses
include the treatment of neovascular glaucoma to regress/suppress iris and
iridocorneal angle neovascularization and the modulation of wound healing
after glaucoma filtration surgery. Bevacizumab is a full-length anti-VEGF
antibody, which is also being used in aforementioned eye conditions off-label.
An overview of these anti-VEGF antibodies and the results of preclinical and
clinical studies regarding their use in the treatment of glaucoma are presented.
Expert opinion: Early studies on the utility of both bevacizumab and ranibi-
zumab in neovascular glaucoma and filtration surgery reported promising
results. However, a large-scale randomized clinical trial as well as comparative
studies between the two anti-VEGF antibodies are currently lacking. A single
dose of ranibizumab costs approximately 40 times as much as a single dose of
bevacizumab. Clinicians should take this into account, in addition to their
differences in the efficacy and safety, when treating patients.
Keywords: anti-VEGF, bevacizumab, glaucoma filtration surgery, neovascular glaucoma,
ranibizumab, trabeculectomy, vascular endothelial growth factor, wound healing
Expert Opin. Biol. Ther. (2012) 12(12):1641-1647
1. Introduction
First discovered in 1983 as a molecule secreted by tumor cells to increase vascularpermeability [1], vascular endothelial growth factor (VEGF) was later found to beproduced in tumors that outgrow their oxygen supply. The hypothesis that VEGFwas responsible for hypoxia-mediated angiogenesis in ischemic tissue was streng-thened when VEGF mRNA levels were reported to be dramatically increased withina few hours of exposing different cell cultures to hypoxia and return to backgroundwhen normal oxygen supply was resumed [2]. Furthermore, it was discovered thatVEGF was consistently expressed in samples of intraocular neovascular membranesobtained from patients with proliferative diabetic retinopathy and that intravitrealVEGF levels were increased in patients with proliferative diabetic retinopathyas well as other ischemic retinal diseases [3-5]. These discoveries have led to thedevelopment of VEGF inhibitors in order to reduce pathologic angiogenesis.
There are currently two anti-VEGF antibodies used in therapy. Bevacizumab,a humanized IgG1 monocolonal antibody against all isoforms of VEGF-A [6], isused in combination with intravenous 5-fluorouracil (5-FU)-based chemotherapyas the first- or second-line treatment of metastatic carcinoma of the colon and
10.1517/14712598.2012.721772 © 2012 Informa UK, Ltd. ISSN 1471-2598 1641All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.

rectum [7]. It is also used in combination with a variety ofother anti-cancer drugs for advanced lung, breast, and kidneycancers [8]. Because of its size (molecular weight of 150 kDa),it was thought that penetration of bevacizumab through theretinal layers after intravitreal injection and its effect onpathologic conditions in the outer retina or choroid wouldbe limited. Therefore, ranibizumab, an antigen-binding frag-ment (Fab) of 48 kDa was developed for ocular indicationsand was affinity-matured to bind all isoforms of VEGF-A.On a molar basis, ranibizumab was 5- to 20-fold more potentthan full-length bevacizumab in bioassays measuring humanVEGF-induced endothelial cell mitogenesis [9]. In additionto the increased potency and enhanced penetration, ranibi-zumab’s absence of an Fc portion eliminated the possibilityof complement-mediated or cell-dependent cytotoxicity trig-gered by interaction with Fc receptors of inflammatorycells [10]. These advantages have increased the appeal of ranibi-zumab in the treatment of ocular diseases. Clinical trialsreported in 2006 established ranibizumab’s efficacy for thetreatment of neovascular age-related macular degeneration(AMD) [11,12]. In June 2006, ranibizumab was approvedby the US Food and Drug Administration (FDA) for thetreatment of wet AMD.Currently, anti-VEGF antibodies are also utilized as an off-
label treatment for ocular neovascular disease other than wetAMD, including neovascular glaucoma (NVG). Neovascularglaucoma is a severe form of glaucoma with devastating visualoutcomes. It is associated with neovascularization of the irisand iridocorneal angle structures secondary to posteriorsegment ischemic diseases such as proliferative diabeticretinopathy and central retinal vein or artery occlusion. Newblood vessel growth eventually obstructs aqueous humor out-flow, resulting in a high intraocular pressure (IOP) that isunresponsive to traditional glaucoma treatments [13,14]. Addi-tionally, patients often suffer from severe ocular pain due tohigh IOP. More invasive surgeries such as cyclophotocoagula-tion and glaucoma drainage device implantation than con-ventional glaucoma filtration surgery----trabeculectomy----areoften required in this devastating disease in combinationwith panretinal photocoagulation to eliminate the source of
VEGF. But the surgical outcome in NVG is much worsethan that in other types of glaucoma and far from satisfactory.
In addition, because of their potential inhibitory effect onpostoperative fibroblastic proliferation and wound healing, theutility of anti-VEGF antibodies in glaucoma filtration surgeryhave been investigated to reduce postoperative wound healing.Although trabeculectomy and glaucoma drainage deviceimplantation are effective methods of IOP reduction in patientswithmedically uncontrolled IOP, surgical outcome of these pro-cedures are often unpredictable. This lower predictability canlargely be attributed to individual variability in the postoperativewound-healing responses in the subconjunctival and sub-tenonspaces. Antifibrotic agents such as mitomycin C (MMC) and5-FU have improved the success rates of glaucoma filtration sur-gery but increased the rate of filtering bleb-related complicationsincluding leakage, blebitis, dysaesthesia, and endophthalmitis.Therefore, new wound-healing modulators are needed formore predictable and safer filtration surgery.
2. Bevacizumab and ranibizumab
2.1 ChemistryBevacizumab is a non-selective full-size anti-VEGF antibodyconsisting mainly of human IgG1 (93%) and a small amountof murine protein sequences (7%) in the complimentarity-determining region [15]. Bevacizumab is able to recognizeand inhibit all major isoforms of human VEGF-A [16].
Ranibizumab is the Fab moiety of a recombinant humanizedmonoclonal antibody rhuMAb accomplished by site-directedmutagenesis of a human IgG1 framework (95%) with murinecomplementarity-determining regions (5%). It has a molecularweight of approximately 48 kDa and is produced by an E. coliexpression system in a nutrient medium containing the anti-biotic tetracycline. Tetracycline is not detectable in the finalproduct. Ranibizumab binds with high affinity to the VEGF-A isoforms (e.g., VEGF110, VEGF121, and VEGF165) [17].The binding is strong (in the subnanomolar region), dissociatesslowly and it is likely that once the ranibizumab--VEGFcomplex is formed, it is very stable.
2.2 PhamacodynamicsVEGF-A has been shown to cause neovascularization (angio-genesis) and an increase in vascular permeability, which isthought to contribute to the progression of the neovascularform of AMD. A small study in rectal cancer demonstratedthat VEGF blockade by bevacizumab has a direct and rapidantivascular effect [18]. A single infusion of bevacizumabdecreased tumor perfusion, vascular volume, microvasculardensity, interstitial fluid pressure and the number of viable,circulating endothelial and progenitor cells and increased thefraction of vessels with pericyte coverage in rectal carcinomapatients [18].
Ranibizumab, a VEGF-A antagonist, binds to the receptor-binding site of active forms of VEGF-A, including thebiologically active, cleaved form of this molecule, VEGF110.
Article highlights.
. Anti-VEGF antibodies may improve treatment outcomeof neovascular glaucoma by suppressing or regressingnew vessels.
. Anti-VEGF antibodies may help prevent excessive woundhealing after glaucoma filtering surgery and reduce theneed of conventional anti-fibrotic agents, thereforedecreasing the risk of postoperative hypotony orbleb-related complications.
. Large-scale randomized clinical trials as well ascomparative studies between ranibizumab andbevacizumab are needed.
This box summarizes key points contained in the article.
S. C. Park et al.
1642 Expert Opin. Biol. Ther. (2012) 12(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.
The binding of ranibizumab to VEGF-A prevents the interac-tion of VEGF-A with its receptors (VEGFR1 and VEGFR2)on the surface of endothelial cells, reducing endothelial cellproliferation, vascular leakage, and new blood vessel formation.
2.3 Pharmacokinetics and metabolismThe intraocular distribution, pharmacokinetics, and the safetyof full-length and Fab anti-VEGF antibodies were comparedfollowing intravitreal injection in Rhesus monkeys [19]. Tras-tuzumab (148 kDa), a humanized antibody with a similarframework to that of bevacizumab, was compared with theFab (48.3 kDa) version of bevacizumab. Microautoradio-graphy demonstrated that the full-length antibody did notpenetrate the internal limiting membrane, whereas the Fabantibody diffused through the retinal pigment epitheliumrapidly and persisted for up to 7 days. The intravitreal half-life was 3.2 days for the Fab antibody and 5.6 days for thefull-length antibody. An immune response was not evidentwith either full-length or Fab antibody. In these animalstudies, systemic exposure of ranibizumab is more than2000-fold lower than in the vitreous.
The half-life after a single intraocular injection ofranibizumab in monkey eyes was 3 days, whereas that of afull-length antibody in rabbit eyes is 5.6 days [20,21]. Usinga rabbit model, Bakri et al. found a half-life of 2.88 daysafter a single intravitreal injection of 0.5 mg of ranibizu-mab [22]. Concentrations > 0.1 µg/ml of ranibizumab weremaintained in the vitreous for a total of 29 days. No ranibi-zumab was detected in the serum or the fellow uninjectedeye, whereas small amounts of intravitreal bevacizumabhave been detected in the serum and the fellow eye in thesame rabbit model [23].
2.4 ToxicityWith intravitreally administered anti-VEGF antibody, themost common adverse reactions are conjunctival hemorrhage,eye pain, vitreous floaters, increased intraocular pressure andintraocular inflammation [24]. Other less frequent adverseevents include endophthalmitis and retinal detachment thatmay occur following intravitreal injection procedure, butnot specific to anti-VEGF antibody.
3. Anti-VEGF antibodies in neovascularglaucoma
3.1 Preclinical studiesIn 1996, it was demonstrated that intravitreal injections ofrecombinant human VEGF produced non-inflammatory irisneovascularization in a non-human primate and prolongedexposure led to NVG [25]. Various animal studies using differ-ent VEGF inhibitors have demonstrated the role of VEGFand the utility of anti-VEGF therapy in retinal neovasculari-zation caused by ischemia [26-29]. Furthermore, intravitrealinjections of ranibizumab prevented formation of clinicallysignificant choroidal neovascularization in cynomolgus mon-keys and decreased leakage of pre-existing choroidal neovascu-larization [30]. Because new formation of fibrovascularmembrane in the iridocorneal angle and resultant blockageof trabecular aqueous outflow pathway are key pathologiesin NVG, potential use of anti-VEGF antibody in the treat-ment of NVG was derived from these reports and thereforehuman clinical studies were subsequently performed.
3.2 Clinical studiesInvestigation on the use of anti-VEGF antibody in the treat-ment of NVG started with bevacizumab. Several case studiesreported a regression of iris neovascularization and/or reductionof IOP after intravitreal bevacizumab injections [31-33]. Anotherstudy noted a decrease in iris fluorescein angiography leakage asearly as one day after intravitreal injection of bevacizumab [34].Gheith et al. reported a case series of six patients who received1.25 mg/0.05 ml of bevacizumab followed by panretinal photo-coagulation, which resulted in complete regression of iris andangle neovascularization [35]. Two patients in this study hadrecurrence of iris neovascularization, which was resolved afteran additional bevacizumab injection.
Subsequently, larger case series reported the value of bevaci-zumab in the treatment of NVG. Chalam et al. [36] reportedcomplete or partial reduction of leakage in iris fluoresceinangiography within 3 weeks after intracameral injection of bev-acizumab in 16 of 16 eyes.Wakabayashi et al. [37] retrospectivelyreviewed 41 cases with secondary iris neovascularization orNVG and found that initial treatment with intravitreal
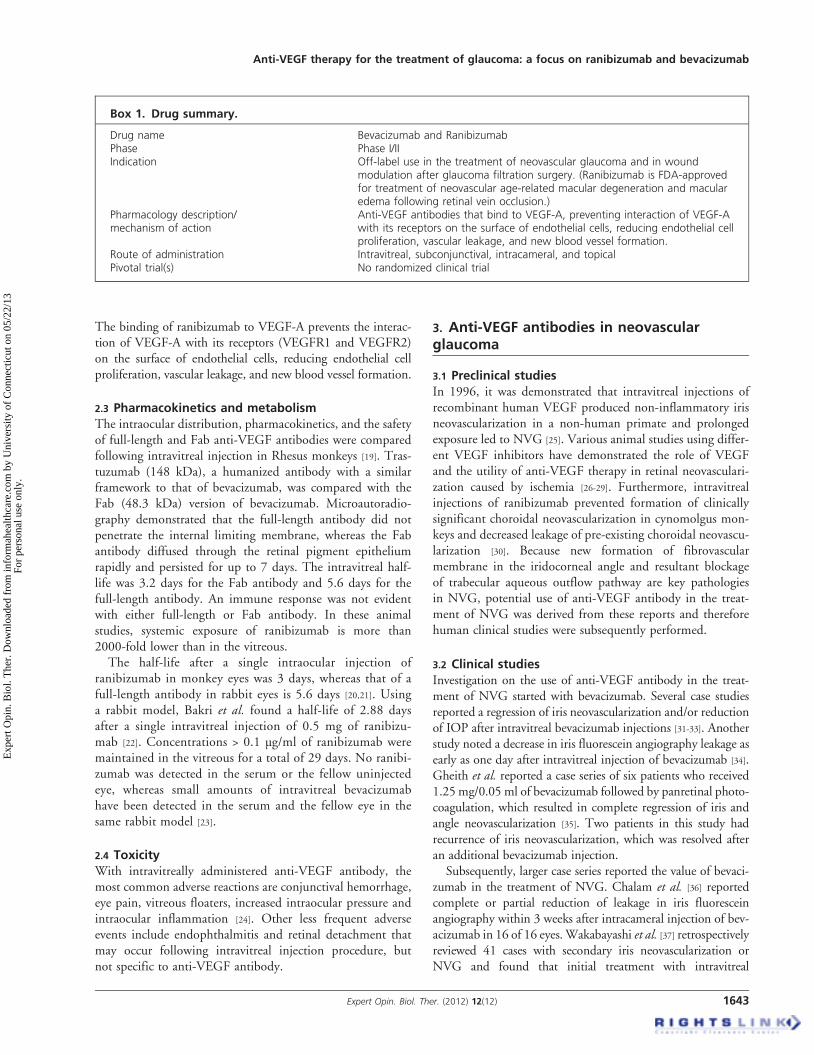
Box 1. Drug summary.
Drug name Bevacizumab and RanibizumabPhase Phase I/IIIndication Off-label use in the treatment of neovascular glaucoma and in wound
modulation after glaucoma filtration surgery. (Ranibizumab is FDA-approvedfor treatment of neovascular age-related macular degeneration and macularedema following retinal vein occlusion.)
Pharmacology description/mechanism of action
Anti-VEGF antibodies that bind to VEGF-A, preventing interaction of VEGF-Awith its receptors on the surface of endothelial cells, reducing endothelial cellproliferation, vascular leakage, and new blood vessel formation.
Route of administration Intravitreal, subconjunctival, intracameral, and topicalPivotal trial(s) No randomized clinical trial
Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab
Expert Opin. Biol. Ther. (2012) 12(12) 1643
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.

bevacizumab controlled IOP in patients with iris neovasculariza-tion alone or early-stageNVGwithout angle closure. Intravitrealbevacizumab resulted in more rapid decrease in IOP whencombined with panretinal photocoagulation [38].Investigations of ranibizumab in the treatment of NVG have
been scarce. Dunavoelgyi et al. reported a case of radiation-induced NVG successfully treated with ranibizumab [39]. Thepatient received radiation treatment for malignant melanomaof the uvea, which resulted in secondary NVG with an IOPof 26 mmHg. Iris angiography prior to ranibizumab treatmentshowed leakage from iris neovascularization, which improvedrapidly after a single intravitreal injection of 0.5 mg/0.05 mLof ranibizumab. IOP decreased to 16 mmHg 2 days after injec-tion. Both iris neovascularization and fluorescein leakagediminished to almost normal conditions 1 week after injection.In a case series of 14 eyes with NVG after proton therapy foruveal melanoma, Caujolle et al. [40] reported promising resultsusing intravitreal ranibizumab either alone or in combinationwith 180-degree ciliary body cryotherapy as a last-chancetreatment before enucleation. All patients suffered from un-controlled NVG despite maximal medical treatment. Irisneovascularization resolved in all cases and IOP was normalizedin 11 out of 14 patients after the treatment.These early results of bevacizumab and ranibizumab (Box 1)
in the treatment of NVG in human eyes are promising, espe-cially for ranibizumab when considering its substantiallyhigher potency on a molar basis and lower possibility ofcomplement-mediated or cell-medicated cytotoxicity thanthose of bevacizumab. Studies with a larger sample size anda longer follow-up time are needed to confirm the benefit ofanti-VEGF agent use in the treatment of NVG. There hasbeen no head-to-head study comparing the two anti-VEGFantibodies in treating NVG and further investigationsare needed.
4. Anti-VEGF antibodies in glaucomafiltration surgery
4.1 Preclinical studiesIn addition to the recruitment of blood vessels, VEGF alsoplays a pivotal role in normal embryonic development andwould healing [41]. Extensive scarring occurs when the balanceof wound-healing cell-mediators and growth factors such asVEGF is disturbed. In vitro over-expression of TGF-betaand VEGF was demonstrated in keloid fibroblasts, and bothin vitro and in vivo studies confirmed the higher angiogenicactivity of keloid fibroblasts compared with normal fibro-blasts [42]. Furthermore, suppression of endogenous VEGFexpression and fibroblast proliferation by dexamethasoneinduces keloid regression [43].The would-healing process and scar formation after glau-
coma filtration surgery is mediated by tenon fibroblasts [44],whose proliferation and migration have been shown to beinhibited by angiogenesis inhibitors in vitro [45]. Two in vitrostudies confirmed the direct effect of anti-VEGF on human
tenon fibroblast proliferation [46,47]. Li et al. [46] showed thatVEGF was upregulated in the aqueous humor of rabbit eyesafter trabeculectomy and stimulated tenon fibroblast prolifera-tion. O’Neill et al. [47] demonstrated that addition of VEGFinduced tenon fibroblast proliferation, which was inhibitedsubsequently by the addition of bevacizumab in a dose-dependent manner. A couple of animal studies demonstratedthat subconjunctival injections of bevacizumab improved theoutcomes of glaucoma filtration surgery as defined by blebsurvival [48,49]. Memarzadeh et al. [48] reported significantlyimproved bleb survival in rabbit eyes with subconjunctivalinjections of 1.25 mg of bevacizumab compared with 5 mgof 5-FU or 0.1 ml of balanced salt solution. In this study,histologic analysis revealed that eyes treated with bevacizumabhad significantly less postoperative scarring. How et al. [49]
investigated the effect of bevacizumab in combination with5-FU and found a greater antifibrotic effect compared witheither therapy alone. They reported 100% bleb survival in arabbit model at 28 days after combination therapy.
An in vitro study by Vasudevan et al. found that at concen-trations commonly used in clinical practice, ranibizumabinduced a greater dose-dependent reduction in the numberof human tenon fibroblasts as compared to bevacizumab [50].Therefore, it can be hypothesized that ranibizumab may havea better inhibitory effect against the subconjunctival encap-sulation and scar tissue formation after glaucoma filtrationsurgery. However, there have been no animal or humanstudies comparing ranibizumab with bevacizumab as woundmodulators after glaucoma filtration surgery.
4.2 Clinical studiesVEGF level was increased in the aqueous humor of glaucomapatients that underwent glaucoma filtration surgery, sugges-ting that it is involved in the postoperative scarring process [46].Bevacizumab was first used in clinical studies in humans toevaluate the effect of anti-VEGF antibodies on wound healingafter glaucoma filtration surgery. There have been reports ofsubconjunctival bevacizumab injection as an adjunct to trabe-culectomy, resulting in effective IOP reduction [51,52].Grewal et al. [51] performed subconjunctival injection of1.25 mg of bevacizumab at the end of trabeculectomy in12 patients, without use of other anti-fibrotic agents (MMCor 5-FU). They reported successful IOP reduction to a rangeof 8 -- 14 mmHg in 11 patients and hypotony in one patient,which resolved spontaneously. Bleb vascularity was increasedafter 3 months, but no patient had a thin cystic bleb at6 months. Nilforushan et al. [52] compared the effect of beva-cizumab and MMC on postoperative wound healing anddemonstrated that IOP was reduced successfully after surgeryin both groups but bevacizumab’s effect was less prominentthan that of MMC. Mean (± standard deviation) post-operative IOP was 13.6 (± 3.2) mmHg with 0.2 (± 0.5) anti-glaucoma medications in the bevacizumab group and9.6 (± 2.7) mmHg with no antiglaucoma medications in theMMC group.
S. C. Park et al.
1644 Expert Opin. Biol. Ther. (2012) 12(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.

A pilot study by Kahook [53] randomized 10 patients withprimary open-angle glaucoma to trabeculectomy with eitherintraoperative intravitreal ranibizumab injection and topicalMMC application or MMC alone. Looking at bleb morpho-logy and vascularity, he found that there were statisticallysignificant differences in peripheral bleb area, vascularity, andnon-bleb-related vascularity between the two groups, with theintravitreal ranibizumab and topical MMC group exhibitingmore diffuse blebs with a lower degree of vascularity. Bothgroups had similar IOP values prior to surgery and at 6 monthsafter surgery. Both groups experienced a statistically significantdecrease in IOP from baseline. There were no intravitrealinjection-related complications such as endophthalmitis oruveitis. A separate investigation into the efficacy of topicalranibizumab on patients after trabeculectomy with MMC isunderway [54].
In addition to reports of anti-VEGF agents as adjuncts inglaucoma filtration surgery, their use in needle revision offiltering blebs were also reported. A couple of reports demon-strated the utility of bevacizumab in bleb needling proceduresafter failed trabeculectomy [55,56]. Purcell et al. [57] reporteda reduction in IOP and bleb vascularity after bleb needlerevision with ranibizumab. There have been no published dataof comparative clinical studies between the two anti-VEGFantibodies.
5. Conclusion
Anti-VEGF therapy in glaucoma has focused on NVG andmodulation of wound healing after glaucoma filtrationsurgery. These applications were introduced because of theanti-angiogenic and anti-fibroblastic properties of anti-VEGF agents. Despite limited data, early reports on theutility of both bevacizumab and ranibizumab in the treatmentof NVG and filtering bleb survival and rescue have beenpromising. However, prospective randomized multicenterclinical trials are still lacking and future studies are neededto elucidate proper treatment protocols, including appropriatedosage, route of delivery, and timing/number/frequency ofinjections, as well as potential side effects.
6. Expert opinion
Based on published results, it is likely that anti-VEGF anti-bodies will play an important role in the treatment of NVG.Intraocular pressure can be controlled using medical or surgicaltreatments, but it is crucial to suppress VEGF’s angiogeniceffect for a long-term IOP control in NVG. Panretinal photo-coagulation is effective to eliminate the source of VEGF, ische-mic retina, but does not clear up VEGF molecules that preexistin the aqueous humor and vitreous. Bevacizumab and ranibi-zumab have an immediate effect to neutralize the VEGF andsuppress/regress neovascularization. Further long-term studiesare required on the timing and frequency of injections indifferent stages of NVG.
The role of anti-VEGF antibodies in glaucoma filtrationsurgery should be determined in interaction with conven-tional anti-fibrotic agents, MMC or 5-FU. Filtering surgerywith MMC or 5-FU better lowers IOP but is more likelyto cause postoperative hypotony or bleb-related complica-tions, compared to filtering surgery without such agents.Therefore, anti-VEGF antibodies may decrease not onlypostoperative wound-healing process but also hypotonyand bleb-related complications by reducing the dosage ofMMC and 5-FU. Further investigations are needed todetermine detailed protocols for the use of anti-VEGF anti-bodies in glaucoma filtration surgery in different types ofglaucoma, especially focusing on cases with a higher riskof surgical failure. Additionally, side effects of repetitiveinjections, including trabecular meshwork toxicity, shouldbe investigated in the future.
In vitro studies have demonstrated better tissue penetrationof ranibizumab when compared to bevacizumab, suggestingbetter efficacy of the former in the treatment of neovascularretinal diseases. However, investigations comparing theefficacy of the two anti-VEGF agents in the treatment ofNVG or in modulation of wound-healing process afterglaucoma filtration surgery are limited. The CATT researchgroup has recently published the results of a multicenterclinical trial comparing ranibizumab and bevacizumab in thetreatment of neovascular AMD [58]. They found that at1 year, bevacizumab and ranibizumab had equivalent effectson visual acuity when administered on the same schedule.Adverse effects between the two drugs require further investi-gation. Despite differences in pharmacokinetics, this reportsuggest similar efficacy of bevacizumab and ranibizumab inneovascular AMD. Future investigations of the two anti-VEGF agents in the treatment of glaucoma should be donein a similar fashion.
Currently, studies on the utility of bevacizumab in intrao-cular diseases are more abundant when compared to those onranibizumab even though ranibizumab is FDA-approved forintraocular diseases such as neovascular AMD and macularedema whereas bevacizumab is used off-label. One of thegreatest factors is cost. A single dose of ranibizumab costsapproximately 40 times as much as a single dose of bevacizu-mab. This difference in cost has enormous economic implica-tions. Clinicians should take this into serious considerationwhen treating patients.
Acknowledgement
Financial Support: SC Park is the Peter Crowley ResearchScientist and Assistant Professor at the New York Eye andEar Infirmary.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.
Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab
Expert Opin. Biol. Ther. (2012) 12(12) 1645
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.

Bibliography
1. Senger DR, Galli SJ, Dvorak AM, et al.
Tumor cells secrete a vascular permeability
factor that promotes accumulation of
ascites fluid. Science 1983;219:983-5
2. Shweiki D, Itin A, Soffer D, Keshet E.
Vascular endothelial growth factor
induced by hypoxia may mediate
hypoxia-initiated angiogenesis.
Nature 1992;359:843-5
3. Malecaze F, Clamens S,
Simorre-Pinatel V, et al. Detection
of vascular endothelial growth factor
messenger RNA and vascular endothelial
growth factor-like activity in proliferative
diabetic retinopathy. Arch Ophthalmol
1994;112:1476-82
4. Adamis AP, Miller JW, Bernal MT,
et al. Increased vascular endothelial
growth factor levels in the vitreous
of eyes with proliferative diabetic
retinopathy. Am J Ophthalmol
1994;118:445-50
5. Aiello LP, Avery RL, Arrigg PG, et al.
Vascular endothelial growth factor in
ocular fluid of patients with diabetic
retinopathy and other retinal disorders.
N Engl J Med 1994;331:1480-7
6. Presta LG, Chen H, O’Conner SJ, et al.
Humanization of an anti-vascular
endothelial growth facor monoclonal
antibody for the therapy of solid tumors
and other disorders. Cancer Res
1997;57:4593-9
7. Hurwitz H, Fehrenbacher L,
Novotny W, et al. Bevacizumab plus
irinotecan, fluorouracil, and leucovorin
for metastatic colorectal cancer. N Engl
J Med 2004;350:2335-42
8. Ferrara N, Kerbel RS. Angiogenesis
as a therapeutic target. Nature
2005;438:967-74
9. Ferrara N, Damico L, Shams N, et al.
Development of ranibizumab, an
anti-vascular endothelial growth factor
antigen binding fragment, as therapy
for neovascular age-related macular
degeneration. Retina 2006;26:859-70
10. Raghavan M, Bjorkman PJ.
Fc receptors and their interactions
with immunoglobulins. Annu Rev
Cell Dev Biol 1996;12:181-220
11. Rosenfeld PJ, Brown DM, Heier JS,
et al. Ranibizumab for neovascular
age-related macular degeneration. N Engl
J Med 2006;355:1419-31
12. Brown DM, Kaiser PK, Michels M,
et al. Ranibizumab versus verteporfin
for neovascular age-related macular
degeneration. N Engl J Med
2006;355:1432-44
13. Shazly TA, Latina MA. Neovascular
glaucoma: etiology, diagnosis and
prognosis. Semin Ophthalmol
2009;24:113-21
14. Shazly TA, Latina MA. Neovascular
glaucoma: etiology, diagnosis and
prognosis. Semin Ophthalmol
2009;24:113-21
15. Kim KJ, Li B, Houch K, et al. The
vascular endothelial growth factor
proteins: identification of biologically
relevant regions by neutralizing
monoclonal antibodies. Growth
Factors 1992;7:53-64
16. Cilley JC, Barfi K, Benson AB III,
Mulcahy MF. Bevacizumab in
the treatment of colorectal cancer.
Expert Opin Biol Ther 2007;7:739-49
17. Lowe J, Araujo J, Yang J, et al.
Ranibizumab inhibits multiple forms of
biologically active vascular endothelial
growth factor in vitro and in vivo.
Exp Eye Res 2007;85:425-30
18. Willett CG, Boucher Y, di Tomaso E,
et al. Direct evidence that the
VEGF-specific antibody bevacizumab
has antivascular effects in human rectal
cancer. Nat Med 2004;10:145-7
19. Mordenti J, Cuthbertson RA, Ferrara N,
et al. Comparisons of the intraocular
tissue distribution, pharmacokinetics, and
safety of 125I-labeled full-length and fab
antibodies in rhesus monkeys following
intravitreal administration.
Toxicol Pathol 1999;27:536-44
20. Gaudreault J, Fei D, Rusit J, et al.
Preclinical pharmacokinetics of
ranibizumab (rhuFabV2) after a
single intravitreal administration.
Invest Ophthalmol Vis Sci
2005;46:726-33
21. Mordenti J, Thomsen K, Licko V, et al.
Intraocular pharmacokinetics and safety
of a humanized monoclonal antibody in
rabbits after intravitreal administration
of a solution or a PLGA microsphere
formulation. Toxicol Sci 1999;52:101-6
22. Bakri SJ, Snyder MR, Reid JM, et al.
Pharmacokinetics of intravitreal
ranibizumab (Lucentis). Ophthalmology
2007;114:2179-82
23. Bakri SJ, Snyder MR, Reid JM, et al.
Pharmacokinetics of intravitreal
bevacizumab (Avastin). Ophthalmology
2007;114:855-9
24. Schmucker C, Loke YK, Ehlken C, et al.
Intravitreal bevacizumab (Avastin) versus
ranibizumab (Lucentis) for the treatment
of age-related macular degeneration:
a safety review. Br J Ophthalmol
2011;95:308-17
25. Tolentino MJ, Miller JW, Gragoudas ES,
et al. Vascular endothelial growth
factor is sufficient to produce iris
neovascularization and neovascular
glaucoma in a nonhuman primate.
Arch Ophthalmol 1996;114:964-70
26. Aiello LP, Pierce EA, Foley ED, et al.
Suppression of retinal neovascularization
in vivo by inhibition of vascular
endothelial growth factor (VEGF)
using soluble VEGF-receptor chimeric
proteins. Proc Natl Acad Sci USA
1995;92:10457-61
27. Adamis AP, Shima DT, Tolentino MJ,
et al. Inhibition of vascular endothelial
growth factor prevents retinal
ischemia-associated iris neovascularization
in a nonhuman primate. Arch
Ophthalmol 1996;114:66-71
28. Robinson GS, Pierce EA, Rook SL, et al.
Oligodeoxynucleotides inhibit retinal
neovascularization in a murine model of
proliferative retinopathy. Proc Natl Acad
Sci USA 1996;93:4851-6
29. Ozaki H, Seo MS, Ozaki K, et al.
Blockade of vascular endothelial cell
growth factor receptor signaling is
sufficient to completely prevent retinal
neovascularization. Am J Pathol
2000;156:697-707
30. Krzystolik MG, Afshari MA, Adamis AP,
et al. Prevention of experimental
choroidal neovascularization with
intravitreal anti-vascular endothelial
growth factor antibody fragment.
Arch Ophthalmol 2002;120:338-46
31. Davidorf FH, Mouser JG, Derick RJ.
Rapid improvement of rubeosis iridis
from a single bevacizumab (Avastin)
injection. Retina 2006;26:354-6
32. Iliev ME, Domig D,
Wolf-Schnurrbursch U, et al. Intravitreal
bevacizumab (Avastin) in the treatment
S. C. Park et al.
1646 Expert Opin. Biol. Ther. (2012) 12(12)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.
of neovascular glaucoma.
Am J Ophthalmol 2006;142:1054-6
33. Oshima Y, Sakaguchi H, Gomi F,
Tano Y. Regression of iris
neovascularization after intravitreal
injection of bevacizumab in patients
with proliferative diabetic retinopathy.
Am J Ophthalmol 2006;142:155-8
34. Grisanti S, Biester S, Peters S, et al.
Intracameral bevacizumab for iris
rubeosis. Am J Ophthalmol
2006;142:158-60
35. Gheith ME, Siam GA, de Barros DS,
et al. Role of intravitreal bevacizumab
in neovascular glaucoma. J Ocul
Pharmacol Ther 2007;23:487-91
36. Chalam KV, Gupta SK, Grover S, et al.
Intracameral Avastin dramatically resolves
iris neovascularization and reverses
neovascular glaucoma. Eur J Ophthalmol
2008;18:255-62
37. Wakabayashi T, Oshima Y, Sakaguchi H,
et al. Intravitreal bevacizumab to treat
iris neovascularization and neovascular
glaucoma secondary to ischemic retinal
diseases in 41 consecutive cases.
Ophthalmology 2008;115:1571-80
38. Ehlers JP, Spirn MJ, Lam A, et al.
Combination intravitreal bevacizumab/
panretinal photocoagulation versus
panretinal photocoagulation alone in
the treatment of neovascular glaucoma.
Retina 2008;28:696-702
39. Dunavoelgyi R, Zehetmayer M,
Simader C, Schmidt-Erfurth U. Rapid
improvement of radiation-induced
neovascular glaucoma and exudative
retinal detachment after a single
intravitreal ranibizumab injection.
Clin Experiment Ophthalmol
2007;35:878-80
40. Caujolle JP, Maschi C, Freton A, et al.
Treatment of neovascular glaucoma after
proton therapy for uveal melanomas with
ranibizumabinjection: preliminary results.
Ophthalmic Res 2012;47:57-60
41. Gariano RF, Gardner TW. Retinal
angiogenesis in development and disease.
Nature 2005;438:960-6
42. Fujiwara M, Muragaki Y, Ooshima A.
Upregulation of transforming growth
factor-beta1 and vascular endothelial
growth factor in cultured keloid
fibroblasts: relevance to angiogenic
activity. Arch Dermatol Res
2005;297:161-9
43. Wu WS, Wang FS, Yang KD, et al.
Dexamethasone induction of keloid
regression through effective suppression
of VEGF expression and keloid fibroblast
proliferation. J Invest Dermatol
2006;126:1264-71
44. Skuta GL, Parrish RK II. Wound
healing in glaucoma filtering surgery.
Surv Ophthalmol 1987;32:149-70
45. Wong J, Wang N, Miller JW,
Schuman JS. Modulation of human
fibroblast activity by selected angiogenesis
inhibitors. Exp Eye Res 1994;58:439-51
46. Li Z, Van Bergen T, Van de Veire S,
et al. Inhibition of vascular endothelial
growth factor reduces scar formation
after glaucoma filtration surgery.
Invest Ophthalmol Vis Sci
2009;50:5217-25
47. O’Neill EC, Qin Q, Van Bergen NJ,
et al. Antifibrotic activity of bevacizumab
on human Tenon’s fibroblasts in vitro.
Invest Ophthalmol Vis Sci
2010;51:6524-32
48. Memarzadeh F, Varma R, Lin LT, et al.
Postoperative use of bevacizumab as an
antifibrotic agent in glaucoma filtration
surgery in the rabbit. Invest Ophthalmol
Vis Sci 2009;50:3233-7
49. How A, Chua JL, Charlton A, et al.
Combined treatment with bevacizumab
and 5-fluorouracil attenuates the
postoperative scarring response after
experimental glaucoma filtration surgery.
Invest Ophthalmol Vis Sci
2010;51:928-32
50. Vasudevan SK. Anti-VEGF anti-fibrosis -
a comparison of ranibizumab and
bevacizumab in vitro. Invest Ophthalmol
Vis Sci 2009;50:E-Abstract 466
51. Grewal DS, Jain R, Kumar H,
Grewal SP. Evaluation of subconjunctival
bevacizumab as an adjunct to
trabeculectomy a pilot study.
Ophthalmology 2008;115:2141-5; e2
52. Nilforushan N, Yadgari M, Kish SK,
Nassiri N. Subconjunctival bevacizumab
versus mitomycin C adjunctive to
trabeculectomy. Am J Ophthalmol
2012;153:352-7; e1
53. Kahook MY. Bleb morphology and
vascularity after trabeculectomy with
intravitreal ranibizumab: a pilot study.
Am J Ophthalmol 2010;150:399-403; e1
54. Bochmann F, Kaufmann C, Becht CN,
et al. ISRCTN12125882 - Influence
of topical anti-VEGF (Ranibizumab)
on the outcome of filtration surgery
for glaucoma - study Protocol.
BMC Ophthalmol 2011;11:1
55. Coote MA, Ruddle JB, Qin Q,
Crowston JG. Vascular changes after
intra-bleb injection of bevacizumab.
J Glaucoma 2008;17:517-18
56. Kahook MY, Schuman JS, Noecker RJ.
Needle bleb revision of encapsulated
filtering bleb with bevacizumab.
Ophthalmic Surg Lasers Imaging
2006;37:148-50
57. Purcell JM, Teng CC, Tello C, et al.
Effect of needle bleb revision with
ranibizumab as a primary intervention in
a failing bleb following trabeculectomy.
Invest Ophthalmol Vis Sci
2008;49:E-Abstract 4165
58. CATT Research Group. Martin DF,
Maguire MG, Ying GS, et al.
Ranibizumab and bevacizumab for
neovascular age-related macular
degeneration. N Engl J Med
2011;364:1897-908
AffiliationSung Chul Park1,2 MD, Daniel Su3,4 BS &
Celso Tello†5,6 MD†Author for correspondence1Assistant Professor,
Einhorn Clinical Research Center,
New York Eye and Ear Infirmary,
310 East 14th Street,
New York, NY 10003, USA2New York Medical College,
Department of Ophthalmology,
Valhalla, NY, USA3Research Fellow,
Einhorn Clinical Research Center,
New York Eye and Ear Infirmary,
310 East 14th Street,
New York, NY 10003, USA4Mount Sinai School of Medicine,
New York, NY, USA5Associate Professor,
New York Eye and Ear Infirmary,
310 East 14th Street,
New York, NY 10003, USA6Department of Ophthalmology,
New York Medical College,
New York, NY, USA
Tel: +1 212 477 7540;
Fax: +1 212 420 8743;
E-mail: [email protected]
Anti-VEGF therapy for the treatment of glaucoma: a focus on ranibizumab and bevacizumab
Expert Opin. Biol. Ther. (2012) 12(12) 1647
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 05
/22/
13Fo
r pe
rson
al u
se o
nly.




![Amino acid transporter LAT1 in tumor-associated vascular ...patients with bevacizumab, an anti-VEGF antibody, increased the PlGF in plasma [3]. FGF-2 and PlGF were increased in glioblastoma](https://static.fdocuments.us/doc/165x107/609eaca54cba15523b358952/amino-acid-transporter-lat1-in-tumor-associated-vascular-patients-with-bevacizumab.jpg)













