
Anti-infective Drugs Advisory Committee (CABP) - InClin · 1 Anti-infective Drugs Advisory...
111
1 Anti Anti - - infective Drugs infective Drugs Advisory Committee Advisory Committee (CABP) (CABP) Ceftaroline fosamil Ceftaroline fosamil Cerexa, Inc. Cerexa, Inc. A subsidiary of Forest Laboratories, Inc. A subsidiary of Forest Laboratories, Inc. 07 September 2010 07 September 2010
Transcript of Anti-infective Drugs Advisory Committee (CABP) - InClin · 1 Anti-infective Drugs Advisory...

1
AntiAnti--infective Drugs infective Drugs Advisory CommitteeAdvisory Committee
(CABP)(CABP)
Ceftaroline fosamilCeftaroline fosamilCerexa, Inc.Cerexa, Inc.
A subsidiary of Forest Laboratories, Inc.A subsidiary of Forest Laboratories, Inc.07 September 201007 September 2010

2
IntroductionIntroductionCeftaroline fosamilCeftaroline fosamil
Dirk Thye, MDDirk Thye, MDPresidentPresident
Cerexa, Inc.Cerexa, Inc.

3
•• A novel intravenous cephalosporinA novel intravenous cephalosporin
•• BroadBroad--spectrum activity spectrum activity –– GramGram--positive bacteria positive bacteria (eg, Streptococcus pneumoniae, (eg, Streptococcus pneumoniae,
Staphylococcus aureus)Staphylococcus aureus)–– GramGram--negative bacteria (eg, negative bacteria (eg, Escherichia coli, Escherichia coli,
Klebsiella pneumoniae, Haemophilus influenzaeKlebsiella pneumoniae, Haemophilus influenzae))
•• Potent activity vs contemporary resistant pathogensPotent activity vs contemporary resistant pathogens–– MRSA, MDRSP MRSA, MDRSP
•• Demonstrated efficacy in CABP and cSSSI Demonstrated efficacy in CABP and cSSSI
•• Well tolerated with safety profile reflective of Well tolerated with safety profile reflective of cephalosporin classcephalosporin class
Ceftaroline DescriptionCeftaroline Description

4
Proposed IndicationsProposed Indications
•• Ceftaroline is indicated for patients with CABP Ceftaroline is indicated for patients with CABP caused by susceptible isolates of gramcaused by susceptible isolates of gram--positive positive and gramand gram--negative microorganisms:negative microorganisms:
–– S.S. pneumoniae pneumoniae (including MDRSP and cases with (including MDRSP and cases with concurrent bacteremia) concurrent bacteremia)
–– S.S. aureus aureus (MSSA) (MSSA) –– H.H. influenzae influenzae –– H.H. parainfluenzaeparainfluenzae–– K.K. pneumoniae (ceftazidime susceptible)pneumoniae (ceftazidime susceptible)–– E.E. coli (ceftazidime susceptible)coli (ceftazidime susceptible)
•• Proposed doseProposed dose–– 600 mg q12h IV over 1 hour600 mg q12h IV over 1 hour–– 400 mg q12h IV over 1 hour for subjects with moderate to 400 mg q12h IV over 1 hour for subjects with moderate to
severe renal impairment (CrCl < 50 mL/min)severe renal impairment (CrCl < 50 mL/min)

5
Program OverviewProgram Overview
2 CABP 2 CABP StudiesStudies
P903P903--08,08,P903P903--0909
Four Phase 3 Four Phase 3 StudiesStudies
2 cSSSI 2 cSSSI StudiesStudies
P903P903--06,06,P903P903--0707
2 cSSSI2 cSSSIStudiesStudies
Intravenous,Intravenous,IntramuscularIntramuscular
•• Healthy adultsHealthy adults•• Mild, moderate, Mild, moderate,
severe renal severe renal impairmentimpairment
•• ESRD receiving ESRD receiving hemodialysishemodialysis
•• Thorough ECGThorough ECG•• ElderlyElderly•• Adolescents Adolescents •• IM administrationIM administration•• Fecal microfloraFecal microflora
Two Phase 2 Two Phase 2 StudiesStudies
11 Phase 1 11 Phase 1 StudiesStudies
17 Studies17 Studies

6
20052005 20062006 20072007 20082008 20092009 20102010
Regulatory HistoryRegulatory History
DecemberDecemberIND submittedIND submitted
FebruaryFebruaryFast Track Fast Track
designationdesignationgrantedgranted
OctoberOctoberEndEnd--ofof--Phase 2Phase 2
meetingmeeting
JulyJulyPrePre--NDA NDA meetingmeeting
DecemberDecemberNDA submittedNDA submitted
JanuaryJanuarySPA submitted SPA submitted
for CABP for CABP studiesstudies
SeptemberSeptemberAgreement with Agreement with
FDA on FDA on 10% NI margin 10% NI margin
in CABPin CABPfor PORT III and for PORT III and
IV subjectsIV subjects
JuneJuneFDA requests FDA requests exploratory exploratory
populations & populations & endpointsendpoints
MarchMarchFDA updates FDA updates CABP Draft CABP Draft
Guidance for Guidance for Industry Industry

7
AgendaAgendaDirk Thye, MDDirk Thye, MDPresident President –– Cerexa, Inc.Cerexa, Inc.
IntroductionIntroduction
Donald E. Low, MD, FRCPCDonald E. Low, MD, FRCPCCABP: CABP: Therapeutic PerspectiveTherapeutic Perspective
David Friedland, MDDavid Friedland, MDVice President, Clinical Sciences Vice President, Clinical Sciences Cerexa, Inc.Cerexa, Inc.
Clinical SafetyClinical Safety
CABP:CABP:New Challenges New Challenges in Treatmentin Treatment
Donald E. Low, MD, FRCPCDonald E. Low, MD, FRCPCMicrobiologistMicrobiologist--inin--ChiefChiefMt. Sinai Hospital, TorontoMt. Sinai Hospital, Toronto
Microbiology and Microbiology and Clinical PharmacologyClinical Pharmacology
Ian Critchley, PhDIan Critchley, PhDVice President, MicrobiologyVice President, MicrobiologyCerexa, Inc.Cerexa, Inc.
Clinical Design and EfficacyClinical Design and Efficacy Dirk Thye, MDDirk Thye, MD
8
Experts Available to Advisory CommitteeExperts Available to Advisory Committee
Paul G. Ambrose, PharmD, FIDSAPaul G. Ambrose, PharmD, FIDSAPresidentPresidentInstitute for Clinical Pharmacodynamics Inc., Latham, NYInstitute for Clinical Pharmacodynamics Inc., Latham, NY
Robertson D. Davenport, MDRobertson D. Davenport, MDAssociate Professor and Director of the Blood Bank and Associate Professor and Director of the Blood Bank and Transfusion Service, Department of PathologyTransfusion Service, Department of PathologyUniversity of Michigan Health System, Ann Arbor, MIUniversity of Michigan Health System, Ann Arbor, MI
Jamie P. Dwyer, MDJamie P. Dwyer, MDAssistant Professor of MedicineAssistant Professor of MedicineDepartment of Medicine, Nephrology and Hypertension DivisionDepartment of Medicine, Nephrology and Hypertension DivisionVanderbilt University, Nashville, TNVanderbilt University, Nashville, TN
Gary Koch, PhDGary Koch, PhDProfessor of Biostatistics, Department of BiostatisticsProfessor of Biostatistics, Department of BiostatisticsUniversity of North Carolina, Chapel Hill, NCUniversity of North Carolina, Chapel Hill, NC

9
Financial Disclosure for External ConsultantsFinancial Disclosure for External Consultants
•• All have been paid (directly or through their All have been paid (directly or through their employer) for their time and travelemployer) for their time and travel
•• None own stock in Forest Laboratories, Inc.None own stock in Forest Laboratories, Inc.
•• Dr. Ambrose is a Cerexa consultant and Dr. Ambrose is a Cerexa consultant and current SGE serving as temporary member of current SGE serving as temporary member of AntiAnti--infective Advisory Committee, and here infective Advisory Committee, and here today with Agency approvaltoday with Agency approval

10
CommunityCommunity--Acquired Acquired Bacterial Pneumonia: Bacterial Pneumonia:
Medical NeedMedical Need
Donald E. Low, MD, FRCPCDonald E. Low, MD, FRCPCMicrobiologistMicrobiologist--inin--Chief, Chief,
Department of MicrobiologyDepartment of MicrobiologyMount Sinai Hospital, Toronto, OntarioMount Sinai Hospital, Toronto, Ontario

11
CABP: Burden of IllnessCABP: Burden of Illness
•• 77thth leading cause of death in USleading cause of death in USaa
•• ~ 5.6 million cases occur annually~ 5.6 million cases occur annuallybb
–– ~ 1.1 million require hospitalization~ 1.1 million require hospitalization–– Over 75% treated as outpatientsOver 75% treated as outpatients
•• Costs exceed US $8.4 Costs exceed US $8.4 –– $10 billion/$10 billion/yearyearaa
–– InpatientInpatient--care costs are ~ 25care costs are ~ 25--times higher than times higher than outpatientoutpatient--care costscare costs
a a Mandell LA, et al. Mandell LA, et al. Clin Infect DisClin Infect Dis 2007 2007 b b Am J Respir Crit Care Med Am J Respir Crit Care Med 20012001

12
CABP: Pathogens & Antimicrobial ResistanceCABP: Pathogens & Antimicrobial Resistance
•• Pathogens in moderatePathogens in moderate--toto--severe CABPsevere CABP–– Streptococcus pneumoniaeStreptococcus pneumoniae–– Staphylococcus aureusStaphylococcus aureus–– Haemophilus influenzaeHaemophilus influenzae–– Enteric gramEnteric gram--negative bacillinegative bacilli
•• Antibacterial resistance is commonAntibacterial resistance is common–– PenicillinPenicillin--nonsusceptible and multidrugnonsusceptible and multidrug--resistant resistant
S. pneumoniaeS. pneumoniae (PRSP, PISP, MDRSP)(PRSP, PISP, MDRSP)–– Nonvaccine Nonvaccine S. pneumoniaeS. pneumoniae serotypes (eg, 19A)serotypes (eg, 19A)
•• Emerging threatEmerging threat–– CommunityCommunity--acquired MRSAacquired MRSA
13
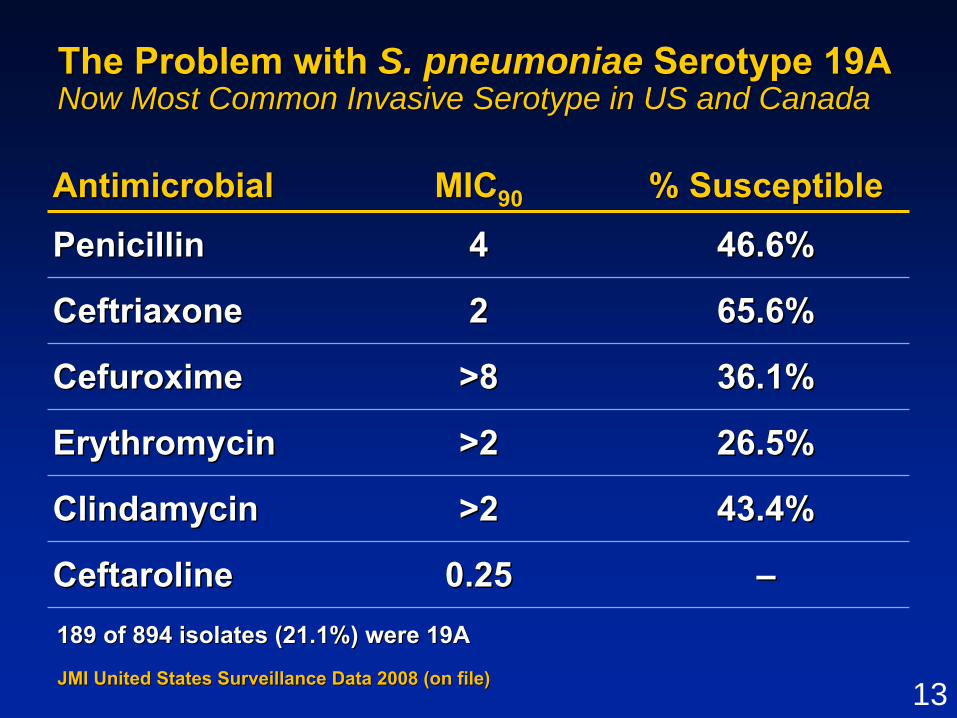
The Problem with The Problem with S. pneumoniaeS. pneumoniae Serotype 19ASerotype 19ANow Most Common Invasive Serotype in US and CanadaNow Most Common Invasive Serotype in US and Canada
AntimicrobialAntimicrobial MICMIC9090 % Susceptible% Susceptible
PenicillinPenicillin 44 46.6%46.6%
CeftriaxoneCeftriaxone 22 65.6%65.6%
CefuroximeCefuroxime >8>8 36.1%36.1%
ErythromycinErythromycin >2>2 26.5%26.5%
ClindamycinClindamycin >2>2 43.4%43.4%
CeftarolineCeftaroline 0.250.25 ––189 of 894 isolates (21.1%) were 19A189 of 894 isolates (21.1%) were 19A
JMI JMI United States Surveillance Data 2008United States Surveillance Data 2008 (on file)(on file)
14
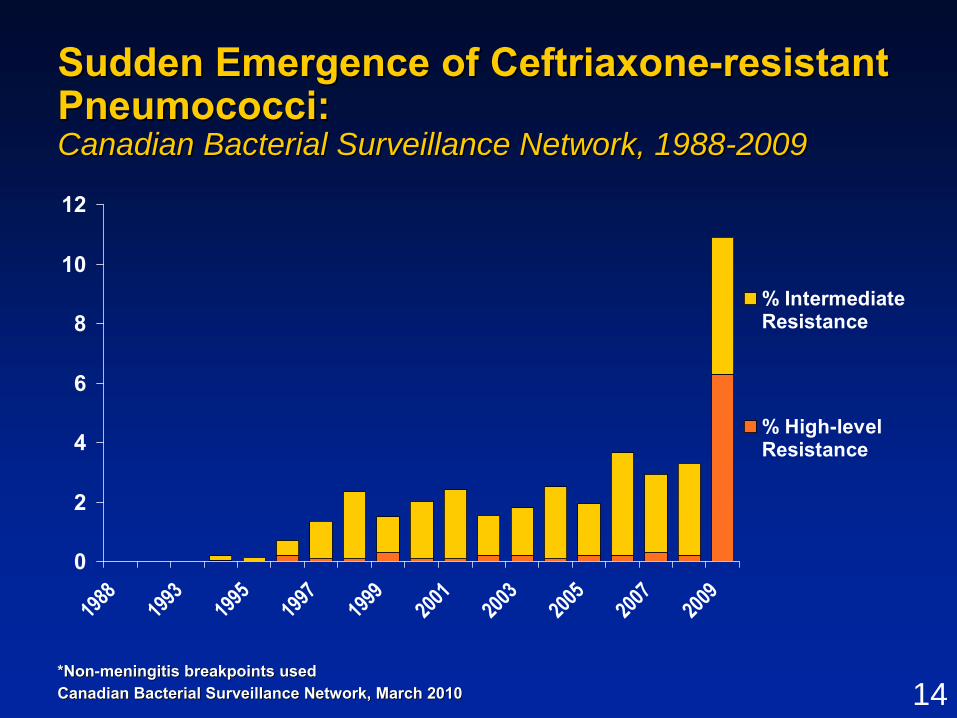
Sudden Emergence of CeftriaxoneSudden Emergence of Ceftriaxone--resistant resistant PneumococciPneumococci: : Canadian Bacterial Surveillance Network, 1988Canadian Bacterial Surveillance Network, 1988--20092009
0
2
4
6
8
10
12
1988
1993
1995
1997
1999
2001
2003
2005
2007
2009
% IntermediateResistance
% High-levelResistance
*Non*Non--meningitis breakpoints usedmeningitis breakpoints usedCanadian Bacterial Surveillance Network, March 2010Canadian Bacterial Surveillance Network, March 2010

15
CABP CABP –– SummarySummary
•• CABP is one of most common infectious CABP is one of most common infectious diseases, with heavy burden of illnessdiseases, with heavy burden of illness
•• Significant morbidity and mortality despite Significant morbidity and mortality despite advances in medical careadvances in medical care
•• Emerging antimicrobial resistance threatens Emerging antimicrobial resistance threatens the utility of our firstthe utility of our first--line agents line agents
–– MDRSPMDRSP–– CACA--MRSAMRSA
•• New safe and effective antibiotics are New safe and effective antibiotics are urgently needed for CABPurgently needed for CABP

16
Microbiology and Microbiology and Clinical PharmacologyClinical Pharmacology
Ian Critchley, PhDIan Critchley, PhDVice President, MicrobiologyVice President, Microbiology
Cerexa, Inc.Cerexa, Inc.

17
Key Microbiology AttributesKey Microbiology Attributes
•• BroadBroad--spectrum bactericidal activity spectrum bactericidal activity –– Resistant gramResistant gram--positive bacteria and common positive bacteria and common
gramgram--negative pathogensnegative pathogens–– Typical respiratory pathogens including Typical respiratory pathogens including
S. pneumoniae, H. influenzae, S. pneumoniae, H. influenzae, andand M. catarrhalisM. catarrhalis
•• Higher affinity for penicillinHigher affinity for penicillin--binding proteins binding proteins (PBPs) than other (PBPs) than other ββ--lactamslactams
•• Low potential for resistance induction in vitro Low potential for resistance induction in vitro
•• Excellent bactericidal activity against PRSP or Excellent bactericidal activity against PRSP or MRSA / VISA in animal efficacy modelsMRSA / VISA in animal efficacy models
18
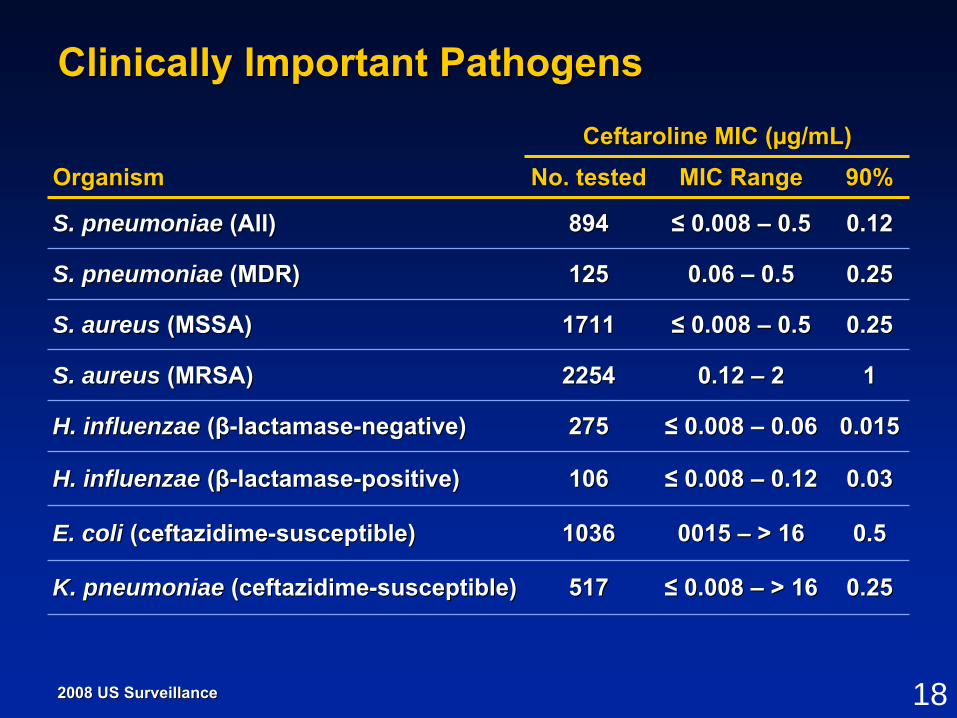
Clinically Important PathogensClinically Important Pathogens
0.250.250.06 0.06 –– 0.50.5125125S. pneumoniaeS. pneumoniae (MDR)(MDR)
0.120.12≤≤ 0.008 0.008 –– 0.50.5894894S. pneumoniaeS. pneumoniae (All)(All)
0.250.25≤≤ 0.008 0.008 –– > 16> 16517517K. pneumoniae K. pneumoniae (ceftazidime(ceftazidime--susceptible)susceptible)
0.50.50015 0015 –– > 16> 1610361036E. coliE. coli (ceftazidime(ceftazidime--susceptible)susceptible)
0.030.03≤≤ 0.008 0.008 –– 0.120.12106106H. influenzae H. influenzae ((ββ--lactamaselactamase--positive)positive)
0.0150.015≤≤ 0.008 0.008 –– 0.060.06275275H. influenzae H. influenzae ((ββ--lactamaselactamase--negative)negative)
110.12 0.12 –– 2222542254S. aureus S. aureus (MRSA)(MRSA)
0.250.25≤≤ 0.008 0.008 –– 0.50.517111711S. aureus S. aureus (MSSA)(MSSA)
90%90%MIC RangeMIC RangeNo. testedNo. testedCeftaroline MIC (Ceftaroline MIC (µµg/mL)g/mL)
OrganismOrganism
2008 US Surveillance2008 US Surveillance

19
Lower MICs than Comparators Against Lower MICs than Comparators Against S. pneumoniaeS. pneumoniaeUS Surveillance Isolates from 2008US Surveillance Isolates from 2008
40
50
60
70
80
90
100
≤ 0.008 0.015 0.03 0.06 0.12 0.25 0.5 1 2 4 > 4
Cum
ulat
ive
Isol
ates
, %
Ceftaroline Ceftriaxone Penicillin
MIC (µg/mL)
891 isolates
Arrows indicate MICArrows indicate MIC9090 values for each agentvalues for each agentJacobs RM et al. Jacobs RM et al. Antimicrob Agents Chemother Antimicrob Agents Chemother 2010 54(6):27162010 54(6):2716--9.9.

20
High Affinity for Modified PBPs in PRSP High Affinity for Modified PBPs in PRSP and MRSAand MRSA
408408128128OxacillinOxacillin0.790.791 1 –– 22PenicillinPenicillin
677677> 128> 128CeftriaxoneCeftriaxone0.640.641 1 –– 22CeftriaxoneCeftriaxone
0.160.160.5 0.5 –– 11CeftarolineCeftaroline0.170.170.120.12CeftarolineCeftaroline
PBP2aPBP2aICIC5050 ((μμg/mL)g/mL)
MICMIC((μμg/mL)g/mL)
PBP2xPBP2xICIC5050 ((μμg/mL)g/mL)
MICMIC((μμg/mL) g/mL)
MRSA MRSA Strain 67Strain 67--00
AntibioticAntibiotic
PRSPPRSPS. pneumoniae S. pneumoniae 20392039
AntibioticAntibiotic
Moisan H et al. Moisan H et al. J Antimicrob Chemother J Antimicrob Chemother 2010 65(4):7132010 65(4):713--6.6.
Higher affinity for modified PBPs results in lower MICsHigher affinity for modified PBPs results in lower MICs

21
Low Potential for Resistance Development Low Potential for Resistance Development In VitroIn Vitro•• No MIC shifts > 2 dilutions following serial passageNo MIC shifts > 2 dilutions following serial passage
(10 (10 –– 50 passages)50 passages)
•• Low spontaneous mutation frequenciesLow spontaneous mutation frequencies
0.120.120.060.06< 1.43 x 10< 1.43 x 10--99BLNARBLNARH. influenzaeH. influenzae 27972797
0.120.120.060.06< 4.98 x 10< 4.98 x 10--99H. influenzaeH. influenzae 12241224
0.250.250.120.12< 7.14 x 10< 7.14 x 10--99PRSPPRSPS. pneumoniaeS. pneumoniae 08840884
0.0150.0150.0080.008< 6.80 x 10< 6.80 x 10--99PSSPPSSPS. pneumoniaeS. pneumoniae 08690869
1111< 1.10 x 10< 1.10 x 10--1010CACA--MRSAMRSAS. aureusS. aureus 22022202
Final MIC After Final MIC After 10 Passages10 Passages
((µµg/mL)g/mL)Initial MIC Initial MIC ((µµg/mL)g/mL)4 x MIC4 x MIC
Serial Passage Resistance Serial Passage Resistance DevelopmentDevelopment
Spontaneous Spontaneous Mutation FrequencyMutation Frequency
PhenotypePhenotypeOrganismOrganism
•• Insignificant induction of AmpC Insignificant induction of AmpC ββ--lactamases at lactamases at ≤≤ 1 x MIC 1 x MIC among gramamong gram--negative bacillinegative bacilli

22* Simulated human dose regimen* Simulated human dose regimenMICs (MICs (µµg/mL) for PSSP (g/mL) for PSSP (0.015 vs. 0.060.015 vs. 0.06) , PISP () , PISP (0.125 vs. 10.125 vs. 1), and PRSP (), and PRSP (0.25 vs. 40.25 vs. 4) for ceftaroline and ) for ceftaroline and ceftriaxone, respectively (ceftriaxone, respectively (CroisierCroisier--Bertin D et al. Bertin D et al. 19th ECCMID19th ECCMID, Helsinki 2009 Abstract O382, Helsinki 2009 Abstract O382). ).
In Vivo Efficacy of Ceftaroline and In Vivo Efficacy of Ceftaroline and Ceftriaxone Against Ceftriaxone Against S. pneumoniaeS. pneumoniae in in Rabbit Pneumonia ModelRabbit Pneumonia Model
0123456789
10
PSSP PISP PRSP
p < .001 p < .001 p < .001
Bac
teria
l Cou
nts
Afte
r 2 D
ays
of T
hera
py(m
ean
log 1
0C
FU/g
lung
tiss
ue)
Ceftaroline 600mg/12h IV*Control Ceftriaxone 1g/24h IV*
p < .01
Ceftriaxone MIC = 4 Ceftriaxone MIC = 4 µµg/mLg/mL
Ceftaroline MIC = 0.25 Ceftaroline MIC = 0.25 µµg/mLg/mL

23
PharmacokineticsPharmacokinetics
•• Rapid prodrug conversion to ceftaroline in plasmaRapid prodrug conversion to ceftaroline in plasma
•• Approximately linear PK for doses of 50 Approximately linear PK for doses of 50 –– 1000 mg1000 mg
•• HalfHalf--life of 2.5 hourslife of 2.5 hours–– No drug accumulation on repeated dosesNo drug accumulation on repeated doses
•• Low protein binding ~ 20%Low protein binding ~ 20%
•• Low potential for drugLow potential for drug--drug interactions drug interactions –– No CYP450No CYP450--dependent metabolismdependent metabolism–– No inhibition or induction of CYP450 enzymesNo inhibition or induction of CYP450 enzymes
•• Elimination mainly through renal excretionElimination mainly through renal excretion–– Dose adjustment for moderate and severe renal Dose adjustment for moderate and severe renal
impairmentimpairment

24
S. pneumoniaeS. pneumoniae PK/PD PK/PD
•• %T>MIC is PK/PD parameter that best %T>MIC is PK/PD parameter that best predicts efficacy for cephalosporinspredicts efficacy for cephalosporins
•• Murine neutropenic thigh/ bacteremia Murine neutropenic thigh/ bacteremia infection model standard for determining infection model standard for determining magnitude of %T>MICmagnitude of %T>MIC
•• %T>MIC predicts efficacy for ceftaroline%T>MIC predicts efficacy for ceftaroline
•• ≥≥ 39% T>MIC required for efficacy for 39% T>MIC required for efficacy for S. pneumoniaeS. pneumoniae
Andes and Craig. Andes and Craig. Antimicrob Agents ChemotherAntimicrob Agents Chemother 2006 50(4):13762006 50(4):1376--13831383

25
PK/PD Target AttainmentPK/PD Target Attainment
S. pneumoniaeS. pneumoniae
* Bars represent percentage of isolates from US surveillance 200* Bars represent percentage of isolates from US surveillance 20088
MIC (μg/mL)
0
20
40
60
80
100
≤ 0.008 0.015 0.03 0.06 0.125 0.25 0.5 1 2 4 8 16
S. pneumoniae*
32
Org
anis
m F
requ
ency
, %
T>MIC = 39%
PK-P
D T
arge
t Atta
inm
ent,
%
> 90% PTA for > 90% PTA for MIC of 1 MIC of 1 µµg/mLg/mL
Monte Carlo simulationMonte Carlo simulation--predicted probability (%) of target predicted probability (%) of target attainment for 600 mg q12h dose as function of MICattainment for 600 mg q12h dose as function of MIC

26
SummarySummary
•• Ceftaroline exhibits broadCeftaroline exhibits broad--spectrum antibacterial spectrum antibacterial activity against important respiratory pathogens activity against important respiratory pathogens
•• Activity against resistant gramActivity against resistant gram--positive bacteria positive bacteria mediated by highmediated by high--affinity binding to modified PBPsaffinity binding to modified PBPs
•• Low potential for resistance development in vitroLow potential for resistance development in vitro
•• Approximately linear PK profileApproximately linear PK profile
•• Low potential for drugLow potential for drug--drug interactionsdrug interactions
•• Dosing regimen of 600 mg q12h provides adequate Dosing regimen of 600 mg q12h provides adequate freefree--drug %T>MIC to cover key respiratory pathogensdrug %T>MIC to cover key respiratory pathogens
–– S. pneumoniaeS. pneumoniae with MICs with MICs ≤≤ 0.5 0.5 µµg/mLg/mL
27
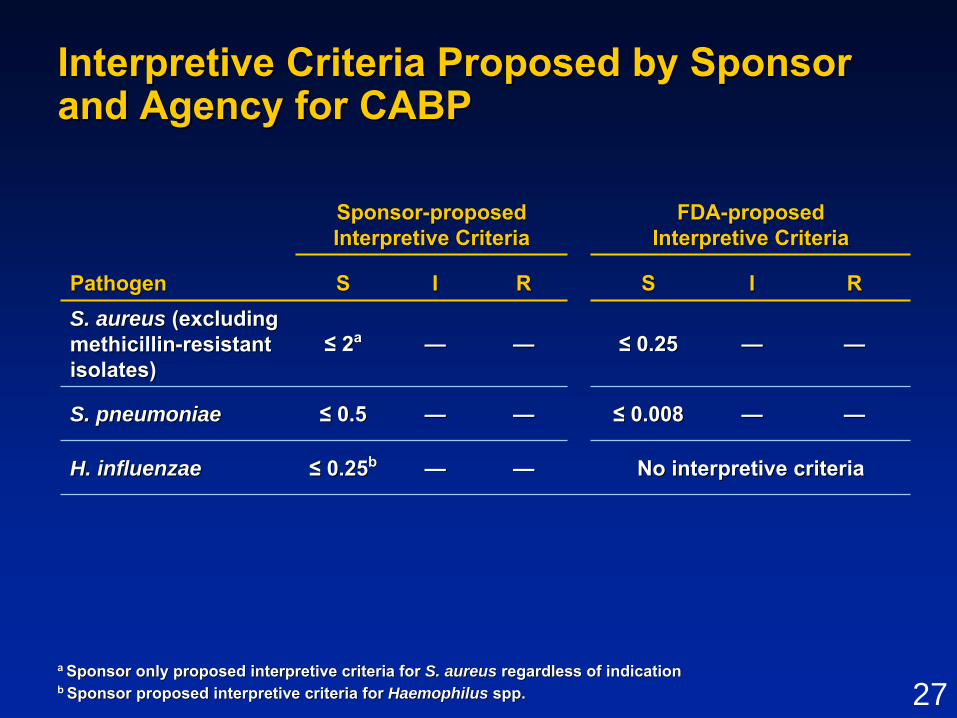
Interpretive Criteria Proposed by Sponsor Interpretive Criteria Proposed by Sponsor and Agency for CABPand Agency for CABP
———— No interpretive criteria No interpretive criteria ≤≤ 0.250.25bbH. influenzaeH. influenzae
————≤≤ 0.0080.008————≤≤ 0.50.5S. pneumoniaeS. pneumoniae
————≤≤ 0.250.25————≤≤ 22aaS. aureus S. aureus (excluding (excluding methicillinmethicillin--resistant resistant isolates)isolates)
RRIISSRRIISS
FDAFDA--proposed proposed Interpretive CriteriaInterpretive Criteria
SponsorSponsor--proposed proposed Interpretive CriteriaInterpretive Criteria
PathogenPathogen
a a Sponsor only proposed interpretive criteria for Sponsor only proposed interpretive criteria for S. aureus S. aureus regardless of indicationregardless of indicationb b Sponsor proposed interpretive criteria for Sponsor proposed interpretive criteria for Haemophilus Haemophilus spp.spp.

28
Interpretive CriteriaInterpretive Criteria
•• Important in guiding physicians in selecting Important in guiding physicians in selecting most appropriate agentmost appropriate agent
•• Susceptible implies a high probability that Susceptible implies a high probability that patient will respond to treatment with patient will respond to treatment with appropriate dosage of antimicrobial agentappropriate dosage of antimicrobial agent
•• Current FDACurrent FDA--proposed breakpointsproposed breakpoints–– Breakpoint divides wildBreakpoint divides wild--type MIC distributiontype MIC distribution–– 51% of US 51% of US S. pneumoniaeS. pneumoniae isolates nonsusceptible isolates nonsusceptible
despite adequate exposure and good clinical despite adequate exposure and good clinical efficacyefficacy
29
Clinical Design and EfficacyClinical Design and Efficacy
Dirk Thye, MDDirk Thye, MD

30
CABP CABP –– Study DesignsStudy DesignsP903P903--08 and P90308 and P903--0909
•• Phase 3, multicenter, randomized, doublePhase 3, multicenter, randomized, double--blindblind•• Noninferiority margin (10%) in clinical response at TOCNoninferiority margin (10%) in clinical response at TOC•• All subjects in Study P903All subjects in Study P903--08 in both groups received 08 in both groups received
2 doses adjunctive clarithromycin (500 mg q12h) on Day 12 doses adjunctive clarithromycin (500 mg q12h) on Day 1•• IV therapy only, no oral stepIV therapy only, no oral step--down therapydown therapy
CeftriaxoneCeftriaxone1 g IV q24h1 g IV q24h
CeftarolineCeftaroline600 mg IV q12h600 mg IV q12h
BaselineAssessment 55--7 days of therapy7 days of therapy
--24h24h
TOC
2121--35 days35 daysafter EOTafter EOT
LFU
88--15 days 15 days after EOTafter EOT
EOT

31
CABP DefinitionCABP Definition
•• New or progressive infiltrate on chest radiographNew or progressive infiltrate on chest radiograph
•• Acute illness (Acute illness (≤≤ 7 days) with 7 days) with ≥≥ 3 signs or 3 signs or symptomssymptoms
–– Fever > 38Fever > 38ººC oral or hypothermia < 35C oral or hypothermia < 35ººCC–– WBC count > 10,000 cells/mmWBC count > 10,000 cells/mm33 or < 4,500 cells/mmor < 4,500 cells/mm33
–– > 15% bands > 15% bands –– New or increased coughNew or increased cough–– Purulent sputum or change in sputum characterPurulent sputum or change in sputum character–– Auscultatory findings consistent with pneumoniaAuscultatory findings consistent with pneumonia–– Dyspnea, tachypnea, or hypoxemiaDyspnea, tachypnea, or hypoxemia

32
Main Inclusion CriteriaMain Inclusion Criteria
•• Adults aged 18 years or olderAdults aged 18 years or older
•• Infection requiring treatment with IV antibioticsInfection requiring treatment with IV antibiotics
•• Need for hospitalizationNeed for hospitalization
•• Only PORT Risk Class III or IV includedOnly PORT Risk Class III or IV included–– PORT I / IIPORT I / II Low mortality, outpatientLow mortality, outpatient–– PORT III / IVPORT III / IV Moderate mortality, hospitalizationModerate mortality, hospitalization–– PORT VPORT V High mortality, ICUHigh mortality, ICU
33
Main Exclusion CriteriaMain Exclusion Criteria
•• More than 1 dose of shortMore than 1 dose of short--acting prior acting prior antibioticantibiotic
•• Known or suspected ceftriaxoneKnown or suspected ceftriaxone--resistant resistant (eg, MRSA) or atypical pathogen(eg, MRSA) or atypical pathogen
•• Admission to ICUAdmission to ICU
•• HealthcareHealthcare-- or hospitalor hospital--acquired pneumoniaacquired pneumonia
•• Immediate lifeImmediate life--threatening disease or threatening disease or evidence of significant hepatic, hematologic, evidence of significant hepatic, hematologic, or immunologic diseaseor immunologic disease

34
Efficacy EndpointsEfficacy Endpoints
•• Primary Efficacy EndpointPrimary Efficacy Endpoint–– Clinical cure rate at TOCClinical cure rate at TOC
•• Secondary Efficacy EndpointsSecondary Efficacy Endpoints–– Clinical cure rate at EOTClinical cure rate at EOT–– Microbiological success rate at TOCMicrobiological success rate at TOC–– Clinical & microbiological response by Clinical & microbiological response by
pathogen at TOCpathogen at TOC–– Relapse at LFURelapse at LFU–– Reinfection/ recurrence at LFUReinfection/ recurrence at LFU

35
Primary Endpoint DefinitionsPrimary Endpoint DefinitionsDetermined at TOCDetermined at TOC
•• Clinical cureClinical cure–– Total resolution of all signs and symptoms of Total resolution of all signs and symptoms of
pneumonia or improvement to extent that further pneumonia or improvement to extent that further antimicrobial therapy not necessaryantimicrobial therapy not necessary
•• Clinical failure (any of following):Clinical failure (any of following):–– Persistence, incomplete clinical resolution, or Persistence, incomplete clinical resolution, or
worsening in signs and symptoms of CABP that worsening in signs and symptoms of CABP that required alternative antimicrobial therapyrequired alternative antimicrobial therapy
–– AE leading to discontinuation of study drug when AE leading to discontinuation of study drug when subject required alternative antimicrobial therapysubject required alternative antimicrobial therapy
–– AllAll--cause mortalitycause mortality•• IndeterminateIndeterminate

36
Analysis PopulationsAnalysis PopulationsPhase 3 CABP Studies CombinedPhase 3 CABP Studies Combined
ITTITT
MITTEMITTE
CECE mMITTEmMITTE
MEME
Study P903Study P903--08 (08 (N = 613)N = 613)Ceftaroline = 304Ceftaroline = 304 Ceftriaxone = 309Ceftriaxone = 309
Study P903Study P903--09 (09 (N = 627)N = 627)Ceftaroline = 317Ceftaroline = 317 Ceftriaxone = 310Ceftriaxone = 310
No drug received No drug received or PORT I, II, or Vor PORT I, II, or VFailed evaluability criteria Failed evaluability criteria
(eg, failed I / E, no outcome (eg, failed I / E, no outcome assessed, noncompliance), assessed, noncompliance), atypical pathogen only, or atypical pathogen only, or Legionella pneumophila Legionella pneumophila infectioninfection
No typical baseline No typical baseline pathogen, atypical pathogen, atypical pathogen only, or pathogen only, or Legionella pneumophilaLegionella pneumophilainfectioninfection

37
Demographics and Baseline CharacteristicsDemographics and Baseline CharacteristicsCABP Studies CombinedCABP Studies Combined
45.445.440.9 40.9 Prior antibiotics*, %Prior antibiotics*, %
74.274.274.874.8Met SIRS criteria, %Met SIRS criteria, %29.529.531.2 31.2
Met modified ATS severe CAP Met modified ATS severe CAP criteria, %criteria, %
3.53.54.04.0Bacteremia, %Bacteremia, %
CharacteristicCharacteristic
MITTE PopulationMITTE PopulationCeftarolineCeftaroline
N = 580N = 580CeftriaxoneCeftriaxone
N = 573N = 573AgeAge
Mean years Mean years ±± SD SD ≥≥ 65 years, % 65 years, % > 50 years, %> 50 years, %
60.8 60.8 ±± 16.416.447.147.175.575.5
61.6 61.6 ±± 15.615.649.0 49.0 77.777.7
Male, %Male, % 62.462.4 63.9 63.9 PORT Risk Class, %PORT Risk Class, %
IIIIIIIVIV
62.162.137.9 37.9
61.6 61.6 38.438.4
* Single dose of a short* Single dose of a short--acting antibioticacting antibiotic

38
Baseline Pathogens Baseline Pathogens Phase 3 CABP Studies CombinedPhase 3 CABP Studies Combined
60 (10.5)60 (10.5)70 (12.1)70 (12.1)Atypical onlyAtypical only
OrganismOrganism
MITTE Population, n (%)MITTE Population, n (%)CeftarolineCeftaroline
N = 580N = 580CeftriaxoneCeftriaxone
N = 573N = 573
Any pathogenAny pathogen 240 (41.4)240 (41.4) 235 (41.0)235 (41.0)
TypicalTypical 170 (29.3)170 (29.3) 175 (30.5)175 (30.5)

39
Key Baseline Pathogens Key Baseline Pathogens Phase 3 CABP Studies CombinedPhase 3 CABP Studies Combined
70 (41.7)70 (41.7)69 (41.8)69 (41.8)S. pneumoniaeS. pneumoniae
13 (7.7)13 (7.7)15 (9.1)15 (9.1)K. pneumoniaeK. pneumoniae
30 (17.9)30 (17.9)25 (15.2)25 (15.2)S. aureusS. aureus
13 (7.7)13 (7.7)12 (7.3)12 (7.3)E. coliE. coli
18 (10.7)18 (10.7)17 (10.3)17 (10.3)H. parainfluenzaeH. parainfluenzae
24 (14.3)24 (14.3)20 (12.1)20 (12.1)H. influenzaeH. influenzae
OrganismOrganism
mMITTE Population, n (%)mMITTE Population, n (%)CeftarolineCeftaroline
N = 165N = 165CeftriaxoneCeftriaxone
N = 168N = 168
40
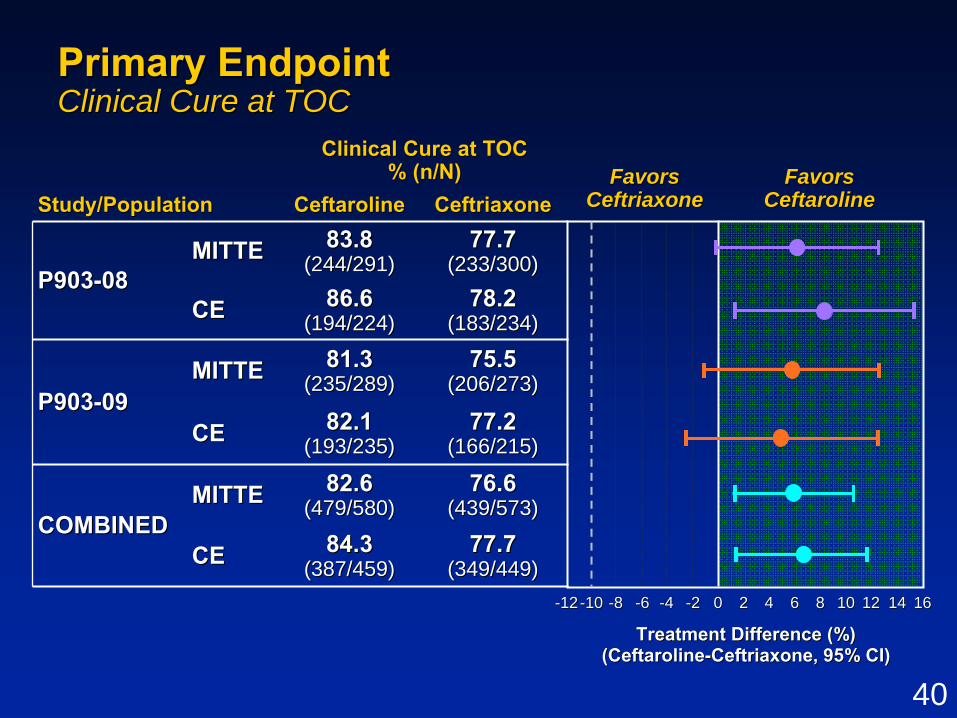
77.7 77.7 (233/300)(233/300)
83.8 83.8 (244/291)(244/291)MITTEMITTE
P903P903--0808
Clinical Cure at TOCClinical Cure at TOC% (n/N)% (n/N)
Study/PopulationStudy/Population Ceftaroline Ceftaroline CeftriaxoneCeftriaxone
CECE 86.6 86.6 (194/224)(194/224)
78.2 78.2 (183/234)(183/234)
P903P903--0909MITTEMITTE 81.3 81.3
(235/289)(235/289)75.5 75.5
(206/273)(206/273)
CECE 82.1 82.1 (193/235)(193/235)
77.2 77.2 (166/215)(166/215)
COMBINEDCOMBINEDMITTEMITTE 82.6 82.6
(479/580)(479/580)76.6 76.6
(439/573)(439/573)
CECE 84.3 84.3 (387/459)(387/459)
77.7 77.7 (349/449)(349/449)
Primary EndpointPrimary EndpointClinical Cure at TOCClinical Cure at TOC
Treatment Difference (%)Treatment Difference (%)(Ceftaroline(Ceftaroline--Ceftriaxone, 95% CI)Ceftriaxone, 95% CI)
FavorsFavorsCeftriaxoneCeftriaxone
FavorsFavorsCeftarolineCeftaroline
--1010 --88 --66 --44 --22 00 22 44 66 88 1010 1212 1414 1616--1212
41
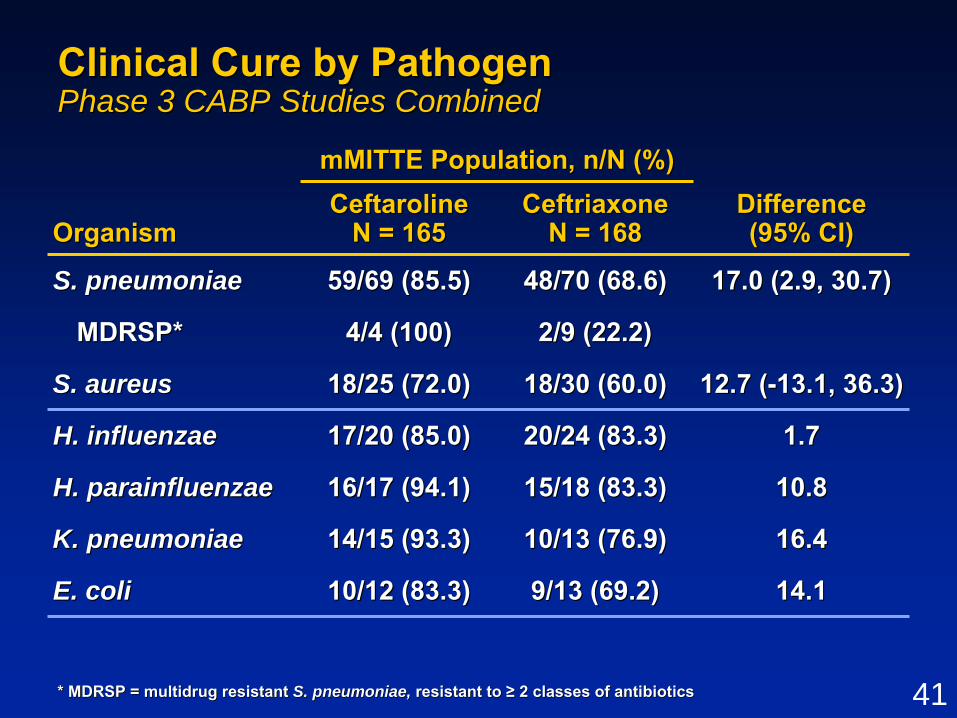
Clinical Cure by PathogenClinical Cure by PathogenPhase 3 CABP Studies CombinedPhase 3 CABP Studies Combined
16.416.410/13 (76.9)10/13 (76.9)14/15 (93.3)14/15 (93.3)K. pneumoniaeK. pneumoniae
14.114.19/13 (69.2)9/13 (69.2)10/12 (83.3)10/12 (83.3)E. coliE. coli
10.810.815/18 (83.3)15/18 (83.3)16/17 (94.1)16/17 (94.1)H. parainfluenzaeH. parainfluenzae
18/30 (60.0)18/30 (60.0)
OrganismOrganism
mMITTE Population, n/N (%)mMITTE Population, n/N (%)DifferenceDifference(95% CI)(95% CI)
CeftarolineCeftarolineN = 165N = 165
CeftriaxoneCeftriaxoneN = 168N = 168
S. pneumoniaeS. pneumoniae 59/69 (85.5)59/69 (85.5) 48/70 (68.6)48/70 (68.6) 17.0 (2.9, 30.7)17.0 (2.9, 30.7)
MDRSP*MDRSP* 4/4 (100)4/4 (100) 2/9 (22.2)2/9 (22.2)
S. aureusS. aureus 18/25 (72.0)18/25 (72.0) 12.7 (12.7 (--13.1, 36.3)13.1, 36.3)
H. influenzaeH. influenzae 17/20 (85.0)17/20 (85.0) 20/24 (83.3)20/24 (83.3) 1.71.7
* MDRSP = multidrug resistant * MDRSP = multidrug resistant S. pneumoniae, S. pneumoniae, resistant to resistant to ≥≥ 2 classes of antibiotics2 classes of antibiotics

42
Clinical Cure by SubgroupClinical Cure by SubgroupPhase 3 CABP Studies CombinedPhase 3 CABP Studies Combined
81.4 (158/ 194)81.4 (158/ 194)82.2 (152/ 185)82.2 (152/ 185)Yes*Yes*74.9 (191/ 255)74.9 (191/ 255)85.8 (235/ 274)85.8 (235/ 274)NoNo
79.2 (217/ 274)79.2 (217/ 274)86.8 (249/ 287)86.8 (249/ 287)IIIIII75.4 (132/ 175)75.4 (132/ 175)80.2 (138/ 172)80.2 (138/ 172)IVIV
78.5 (339/ 432)78.5 (339/ 432)84.9 (372/ 438)84.9 (372/ 438)NoNo58.8 (10/ 17)58.8 (10/ 17)71.4 (15/ 21)71.4 (15/ 21)YesYes
72.4 (71/ 98)72.4 (71/ 98)85.6 (83/ 97)85.6 (83/ 97)≤≤ 505079.2 (278/ 351)79.2 (278/ 351)84.0 (304/ 362)84.0 (304/ 362)> 50> 50
BacteremiaBacteremia
Prior antibioticsPrior antibiotics
PORT Risk ClassPORT Risk Class
SubgroupSubgroupCE Population % (n/N)CE Population % (n/N)
CeftarolineCeftarolineN = 459N = 459
CeftriaxoneCeftriaxoneN = 449N = 449
AgeAge
FavorsCeftriaxone
Treatment Difference (%) Treatment Difference (%) (Ceftaroline(Ceftaroline--Ceftriaxone, 95% CI)Ceftriaxone, 95% CI)
--1616 --1212 --88 --44 00 44 88 1212 1616 2020 2424 2828 3232 3636 4040 4444
FavorsCeftaroline
* No more than * No more than 1 dose of short1 dose of short--acting acting antibioticantibiotic
Shaded area = High risk of mortality subgroupsShaded area = High risk of mortality subgroups
43
FDAFDA--defined Exploratory Primary Analysis defined Exploratory Primary Analysis FDAFDA--mITT PopulationmITT Population
•• Subjects with Subjects with ≥≥ 1 acceptable pathogen1 acceptable pathogen–– Isolated from blood, pleural fluid, BALIsolated from blood, pleural fluid, BAL–– Isolated from adequate sputum specimen (Isolated from adequate sputum specimen (≤≤ 10 10
squamous epithelial cells/LPF and > 10 WBC/LPF)squamous epithelial cells/LPF and > 10 WBC/LPF)–– Positive urinary antigen test for Positive urinary antigen test for S. pneumoniaeS. pneumoniae–– Specific gramSpecific gram--negative rods and only if negative rods and only if ≥≥ PORT III PORT III
and isolate from appropriate sample and isolate from appropriate sample
•• Subjects with Subjects with H. parainfluenzaeH. parainfluenzae excludedexcluded
•• Subjects with sole atypical pathogens Subjects with sole atypical pathogens ((L. pneumophilaL. pneumophila, , M. pneumoniaeM. pneumoniae, or , or C. pneumoniae)C. pneumoniae) excludedexcluded
44
FDAFDA--defined Exploratory Primary Analysisdefined Exploratory Primary AnalysisClinical Responder at Study Day 4Clinical Responder at Study Day 4
•• Clinically stableClinically stable–– Temperature Temperature ≤≤ 37.837.8ooCC–– Heart rate Heart rate ≤≤ 100 bpm100 bpm–– Respiratory rate Respiratory rate ≤≤ 24 breaths per min24 breaths per min–– SBP SBP ≥≥ 90 mmHg90 mmHg–– Oxygen saturation Oxygen saturation ≥≥ 90%90%–– Confusion/ disorientation absentConfusion/ disorientation absent
ANDAND
•• SSymptoms criteria success (compared to baseline)ymptoms criteria success (compared to baseline)–– None of 4 symptoms (cough, dyspnea, chest pain, None of 4 symptoms (cough, dyspnea, chest pain,
sputum production) worseningsputum production) worsening–– ≥≥ 1 symptom improving1 symptom improving

45
56.9 56.9 (41/72)(41/72)
71.0 71.0 (49/69)(49/69)P903P903--0808
FDAFDA--mMITT PopulationmMITT Population% (n/N)% (n/N)
StudyStudy Ceftaroline Ceftaroline CeftriaxoneCeftriaxone
P903P903--0909 69.569.5(57/82)(57/82)
60.5 60.5 (49/81)(49/81)
COMBINEDCOMBINED 70.2 70.2 (106/151)(106/151)
58.8 58.8 (90/153)(90/153)
FDAFDA--defined Exploratory Primary Analysis defined Exploratory Primary Analysis Clinical Responders at Study Day 4Clinical Responders at Study Day 4
FavorsFavorsCeftriaxoneCeftriaxone
FavorsFavorsCeftarolineCeftaroline
Treatment Difference (%)Treatment Difference (%)(Ceftaroline(Ceftaroline--Ceftriaxone, 95% CI)Ceftriaxone, 95% CI)
--2020--1616--1212 --88 --44 00 44 88 1212 1616 2020 2424 2828 3232--2424--2828--3232

46
CABP Efficacy ConclusionsCABP Efficacy Conclusions
•• Ceftaroline efficacious for treatment of CABPCeftaroline efficacious for treatment of CABP–– PrePre--specified, traditional primary endpoint (TOC)specified, traditional primary endpoint (TOC)–– Exploratory, FDAExploratory, FDA--defined early time point (Day 4)defined early time point (Day 4)–– Secondary and subgroup analyses provide robust supportSecondary and subgroup analyses provide robust support
•• Efficacy demonstrated against important pathogensEfficacy demonstrated against important pathogens–– S. pneumoniaeS. pneumoniae–– S. aureusS. aureus–– H. influenzaeH. influenzae
•• Totality of data demonstrates trends favoring Totality of data demonstrates trends favoring ceftaroline over ceftriaxone for treatment of CABPceftaroline over ceftriaxone for treatment of CABP

47
Clinical SafetyClinical Safety
David Friedland, MDDavid Friedland, MDVice President, Clinical SciencesVice President, Clinical Sciences
Cerexa, Inc.Cerexa, Inc.

48
Safety PopulationSafety PopulationAll Clinical StudiesAll Clinical Studies
StudyStudy GroupingGrouping CeftarolineCeftaroline ComparatorComparator TotalTotal
Clinical PharmacologyClinical Pharmacology 275275 8484 305*305*
Combined Phase 2 Combined Phase 2 StudiesStudies 165165 7777 242242
Total PhaseTotal Phase 3 CABP 3 CABP and cSSSI Studiesand cSSSI Studies 13051305 13011301 26062606
Combined Combined PhasePhase 3 3 CABP StudiesCABP Studies 613613 615615 12281228
Combined Phase 3 Combined Phase 3 cSSSI StudiescSSSI Studies 692692 686686 13781378
Total All StudiesTotal All Studies 17451745 14621462 31533153
* 54 subjects in the TQT crossover study are counted only once i* 54 subjects in the TQT crossover study are counted only once in the total columnn the total column

49
Adverse Event OverviewAdverse Event OverviewPhase 3 CABP StudiesPhase 3 CABP Studies
2.02.02.42.4DeathDeath
Safety EventSafety Event
Safety Population, %Safety Population, %CeftarolineCeftaroline
N = 613N = 613CeftriaxoneCeftriaxone
N = 615N = 615
Any TEAEAny TEAE 47.047.0 45.745.7
Any SAEAny SAE 11.311.3 11.711.7
Discontinuations due Discontinuations due to TEAEto TEAE 4.44.4 4.14.1

50
Adverse Events Adverse Events ≥≥ 2% in Ceftaroline Group2% in Ceftaroline GroupPhase 3 CABP StudiesPhase 3 CABP Studies
Safety EventSafety Event
Safety Population, %Safety Population, %CeftarolineCeftaroline
N = 613N = 613CeftriaxoneCeftriaxone
N = 615N = 615
DiarrheaDiarrhea 4.24.2 2.62.6
HeadacheHeadache 3.43.4 1.51.5
InsomniaInsomnia 3.13.1 2.32.3
PhlebitisPhlebitis 2.82.8 2.12.1
HypertensionHypertension 2.32.3 2.62.6
HypokalemiaHypokalemia 2.32.3 2.42.4
NauseaNausea 2.32.3 2.32.3
51
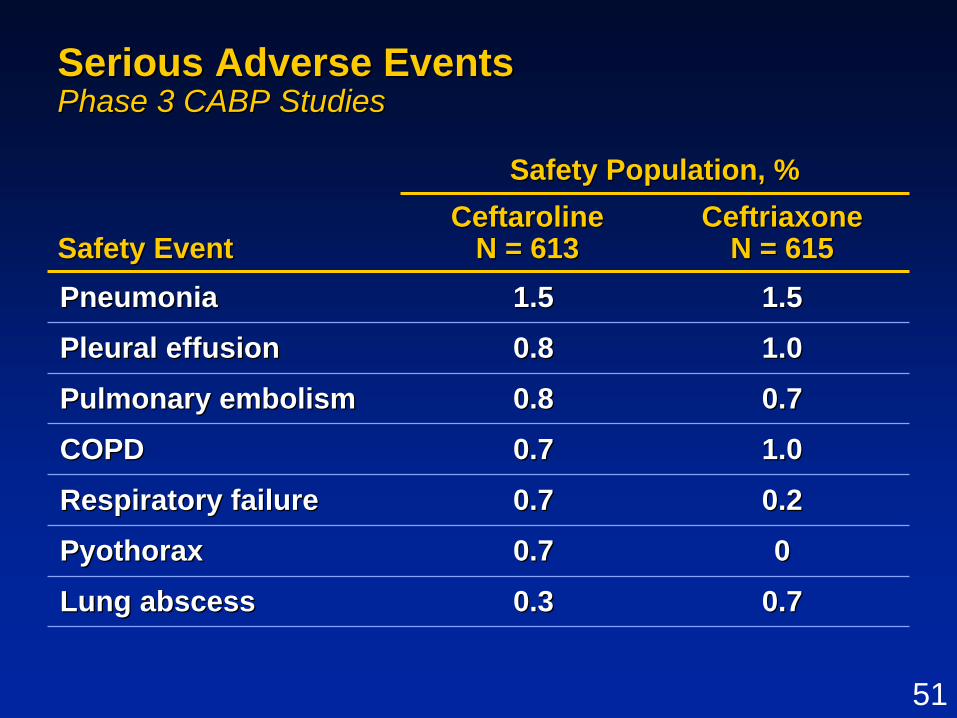
Serious Adverse EventsSerious Adverse EventsPhase 3 CABP StudiesPhase 3 CABP Studies
0.70.70.30.3Lung abscessLung abscess
Safety EventSafety Event
Safety Population, %Safety Population, %CeftarolineCeftaroline
N = 613N = 613CeftriaxoneCeftriaxone
N = 615N = 615Pneumonia Pneumonia 1.51.5 1.51.5
Pleural effusion Pleural effusion 0.80.8 1.01.0
Pulmonary embolism Pulmonary embolism 0.80.8 0.70.7
COPD COPD 0.70.7 1.01.0
Respiratory failure Respiratory failure 0.7 0.7 0.20.2
Pyothorax Pyothorax 0.70.7 00

52
Adverse Events Leading to Discontinuation Adverse Events Leading to Discontinuation of Study Drug or Studyof Study Drug or StudyPhase 3 CABP StudiesPhase 3 CABP Studies
•• Low and similar incidencesLow and similar incidences–– 4.4% ceftaroline vs 4.1% ceftriaxone4.4% ceftaroline vs 4.1% ceftriaxone
•• Few assessed as study drug relatedFew assessed as study drug related–– 0.8% ceftaroline vs 1.0% ceftriaxone0.8% ceftaroline vs 1.0% ceftriaxone
•• No individual AE leading to discontinuation in No individual AE leading to discontinuation in > 2 ceftaroline subjects> 2 ceftaroline subjects

53
Summary of DeathsSummary of DeathsPhase 3 CABP StudiesPhase 3 CABP Studies
•• Number of deaths low and similar between groupsNumber of deaths low and similar between groups–– 15 subjects (ceftaroline) vs 12 subjects (ceftriaxone)15 subjects (ceftaroline) vs 12 subjects (ceftriaxone)–– Potentially drugPotentially drug--related equal (1 subject each group)related equal (1 subject each group)–– Primary infectionPrimary infection--related similar (2 vs 3 subjects)related similar (2 vs 3 subjects)
•• Additional 5 deaths after LFU (1 vs 4 subjects)Additional 5 deaths after LFU (1 vs 4 subjects)
•• No predominant cause of death identifiedNo predominant cause of death identified
•• Timing of deathsTiming of deaths–– Few deaths while on therapy (2 vs 4 subjects)Few deaths while on therapy (2 vs 4 subjects)–– Day 14 mortality similar (6 vs 7 subjects)Day 14 mortality similar (6 vs 7 subjects)–– Day 30 mortality equal (12 subjects each group)Day 30 mortality equal (12 subjects each group)

54
Organ Systems or Events of Interest Organ Systems or Events of Interest Relevant to Cephalosporin ClassRelevant to Cephalosporin Class
Combined CABP and cSSSI Phase 3 Safety DataCombined CABP and cSSSI Phase 3 Safety DataComparator Agents: ceftriaxone (CABP)Comparator Agents: ceftriaxone (CABP)
vancomycin + aztreonam (cSSSvancomycin + aztreonam (cSSSI)I)

55
Summary of Organ SystemsSummary of Organ SystemsPooled Phase 3 CABP and cSSSI StudiesPooled Phase 3 CABP and cSSSI Studies•• Similar renal safetySimilar renal safety
–– TEAEs of potential renal impairment (1.5% vs 0.8%)TEAEs of potential renal impairment (1.5% vs 0.8%)–– PCS Cr increase (1.4% vs 1.9%)PCS Cr increase (1.4% vs 1.9%)–– PCS CrCl decrease (0.7% vs 1.3%)PCS CrCl decrease (0.7% vs 1.3%)
•• Similar hematological safetySimilar hematological safety–– Increased Coombs seroconversion (10.7% vs 4.4%)Increased Coombs seroconversion (10.7% vs 4.4%)–– TEAEs of potential drugTEAEs of potential drug--induced anemia (1.2% vs 1.3%)induced anemia (1.2% vs 1.3%)–– No hemolytic anemia or other hematological signalsNo hemolytic anemia or other hematological signals
•• No evidence of cardiac toxicityNo evidence of cardiac toxicity–– No cardiac signal (TEAEs and ECGs) in Phase 3 studies No cardiac signal (TEAEs and ECGs) in Phase 3 studies –– No QT prolongation (supratherapeutic dose)No QT prolongation (supratherapeutic dose)
•• Similar hepatic safetySimilar hepatic safety–– TEAEs of potential hepatic toxicity (2.5% vs 3.6%)TEAEs of potential hepatic toxicity (2.5% vs 3.6%)–– No ceftarolineNo ceftaroline--treated subject met Hytreated subject met Hy’’s Laws Law

56
Events of Interest Relevant to Events of Interest Relevant to Cephalosporin ClassCephalosporin ClassPooled Phase 3 CABP and cSSSI StudiesPooled Phase 3 CABP and cSSSI Studies
•• Seizures were uncommon (2 vs 1 subjects)Seizures were uncommon (2 vs 1 subjects)–– None related to study drugNone related to study drug
•• Lower incidence of potential allergic reactionsLower incidence of potential allergic reactions–– TEAEs of potential allergic reactions (5.4% vs 8.5%)TEAEs of potential allergic reactions (5.4% vs 8.5%)–– Serious/ severe TEAEs (3 vs 6 subjects)Serious/ severe TEAEs (3 vs 6 subjects)
•• Similar incidence of antibioticSimilar incidence of antibiotic--associated diarrheaassociated diarrhea–– TEAEs of potential antibioticTEAEs of potential antibiotic--associated diarrheaassociated diarrhea
(4.5% vs 3.2%)(4.5% vs 3.2%)–– C. C. difficiledifficile--associated diarrhea uncommonassociated diarrhea uncommon
(2 vs 1 subjects)(2 vs 1 subjects)

57
Safety ConclusionsSafety Conclusions
•• Safety results similar between ceftaroline Safety results similar between ceftaroline and ceftriaxone including:and ceftriaxone including:
–– TEAEsTEAEs–– SAEsSAEs–– Discontinuations due to AEDiscontinuations due to AE–– DeathsDeaths
•• No safety signal identified by Organ System No safety signal identified by Organ System or safety events of interest reviewor safety events of interest review
•• Ceftaroline well tolerated and safety profile Ceftaroline well tolerated and safety profile reflective of cephalosporin classreflective of cephalosporin class

58
Ceftaroline in CABPCeftaroline in CABPTherapeutic PerspectiveTherapeutic Perspective
Donald E. Low, MD, FRCPCDonald E. Low, MD, FRCPC
59
Ceftaroline Meets Urgent Medical NeedsCeftaroline Meets Urgent Medical Needs
•• Broad spectrum of activity against gramBroad spectrum of activity against gram--positives and grampositives and gram--negativesnegatives
•• Potent activity and proven effectiveness for Potent activity and proven effectiveness for treatment of CABPtreatment of CABP
•• Treatment advantage over ceftriaxone for Treatment advantage over ceftriaxone for CABP including CABP including S. pneumoniaeS. pneumoniae and and S. aureusS. aureus
•• Good safety profile consistent with Good safety profile consistent with cephalosporin classcephalosporin class
•• Ceftaroline represents significant Ceftaroline represents significant advancement in antibiotic treatment of CABPadvancement in antibiotic treatment of CABP

60
Where Would I Use CeftarolineWhere Would I Use Ceftaroline
•• FirstFirst--line empiric therapy for patients with line empiric therapy for patients with moderate to severe CABP requiring moderate to severe CABP requiring hospitalizationhospitalization
•• Alternative therapy for patients having failed Alternative therapy for patients having failed on other antibioticson other antibiotics

1
AntiAnti--infective Drugs infective Drugs Advisory CommitteeAdvisory Committee
(cSSSI)(cSSSI)
Ceftaroline fosamilCeftaroline fosamilCerexa, Inc.Cerexa, Inc.
A subsidiary of Forest Laboratories, Inc.A subsidiary of Forest Laboratories, Inc.07 September 201007 September 2010

2
Proposed IndicationsProposed Indications•• Ceftaroline is indicated for patients with cSSSI Ceftaroline is indicated for patients with cSSSI
caused by susceptible isolates of gramcaused by susceptible isolates of gram--positive and positive and gramgram--negative microorganismsnegative microorganisms
–– S. aureus S. aureus (including MSSA and MRSA) (including MSSA and MRSA) –– S.S. pyogenespyogenes, , S.S. agalactiae, S.agalactiae, S. dysgalactiae, S.dysgalactiae, S. anginosus anginosus
groupgroup–– E.E. coli coli (ceftazidime(ceftazidime--susceptible)susceptible)–– K.K. pneumoniaepneumoniae, , K.K. oxytoca oxytoca (ceftazidime(ceftazidime--susceptible)susceptible)–– M.M. morganii morganii (ceftazidime(ceftazidime--susceptible)susceptible)
•• Proposed doseProposed dose–– 600 mg q12h IV over 1 hour600 mg q12h IV over 1 hour–– 400 mg q12h IV over 1 hour for subjects with moderate to 400 mg q12h IV over 1 hour for subjects with moderate to
severe renal impairment (CrCl < 50mL/min)severe renal impairment (CrCl < 50mL/min)

3
AgendaAgenda
G. Ralph Corey, MDG. Ralph Corey, MDABSSSIABSSSITherapeutic PerspectiveTherapeutic Perspective
G. Ralph Corey, MDG. Ralph Corey, MDProfessor of MedicineProfessor of MedicineDuke Clinical Research InstituteDuke Clinical Research Institute
ABSSSI: New Challenges ABSSSI: New Challenges in Treatmentin Treatment
Dirk Thye, MDDirk Thye, MDPresident President –– Cerexa, Inc.Cerexa, Inc.
IntroductionIntroduction
David Friedland, MDDavid Friedland, MDVice President, Clinical Sciences Vice President, Clinical Sciences Cerexa, Inc.Cerexa, Inc.
Clinical SafetyClinical Safety
MicrobiologyMicrobiology Ian Critchley, PhDIan Critchley, PhDVice President, Microbiology Vice President, Microbiology Cerexa, Inc.Cerexa, Inc.
Clinical Design and EfficacyClinical Design and Efficacy Dirk Thye, MDDirk Thye, MD

4
Financial Disclosure for External ConsultantsFinancial Disclosure for External Consultants
•• All have been paid (directly or through their All have been paid (directly or through their employer) for their time and travelemployer) for their time and travel
•• None own stock in Forest Laboratories, Inc.None own stock in Forest Laboratories, Inc.
•• Dr. Corey is a Cerexa consultant for Dr. Corey is a Cerexa consultant for ceftaroline clinical trialsceftaroline clinical trials
•• Dr. Ambrose is a Cerexa consultant and Dr. Ambrose is a Cerexa consultant and current SGE serving as temporary member of current SGE serving as temporary member of AntiAnti--infective Advisory Committee, and here infective Advisory Committee, and here today with Agency approvaltoday with Agency approval

5
ABSSSI (cSSSI)ABSSSI (cSSSI)New Challenges in TreatmentNew Challenges in Treatment
G. Ralph Corey, MDG. Ralph Corey, MDProfessor of MedicineProfessor of Medicine
Duke Clinical Research InstituteDuke Clinical Research Institute

6
The Ongoing Epidemic of MRSAThe Ongoing Epidemic of MRSA--induced induced ABSSSI ABSSSI •• 14 million medical visits annually14 million medical visits annually
–– 600,000 hospitalizations each year600,000 hospitalizations each year
•• Most caused by Most caused by S. aureusS. aureus USA300USA300–– Reproduces every 30 mins (1 to 1 trillion in 20 hrs)Reproduces every 30 mins (1 to 1 trillion in 20 hrs)–– Genetically promiscuous and acquisitiveGenetically promiscuous and acquisitive
•• Resulting increase in virulence/ resistanceResulting increase in virulence/ resistance
Hersh et al. 2008; Hersh et al. 2008; DeFrances et al. 2008.DeFrances et al. 2008.

7
MRSA among 422 ED Patients with ABSSSIMRSA among 422 ED Patients with ABSSSIAugust 2004August 2004
54%
51%
60%
60%
67%
74%
39%15%
55%
68%
72%
59%
Moran GJ et al. Moran GJ et al. N Engl J MedN Engl J Med 2006;355:666.2006;355:666.

8
ABSSSI Includes Primarily Moderate Infections ABSSSI Includes Primarily Moderate Infections

9
However, Occasionally Moderate Infections However, Occasionally Moderate Infections Develop Severe, LifeDevelop Severe, Life--threatening Complicationsthreatening Complications

10
Vancomycin: The Gold Standard for Rx of Vancomycin: The Gold Standard for Rx of MRSAMRSA•• A large hydrophilic moleculeA large hydrophilic molecule
–– Slowly bactericidalSlowly bactericidal–– Poor tissue penetrationPoor tissue penetration
•• Increasing resistance with worsening Increasing resistance with worsening outcomes outcomes
–– VISA (1996), hVISA (1997), VRSA (2002), VISA (1996), hVISA (1997), VRSA (2002), ↑↑MICsMICs
•• Increasing nephrotoxicity with high serum Increasing nephrotoxicity with high serum levelslevels
–– 22% with levels > 20 22% with levels > 20 μμg/Lg/L
Lodise P. CID 2009 209:507; Soriano. CIDLodise P. CID 2009 209:507; Soriano. CID 20082008; Bae 2010; Rybak CID; Bae 2010; Rybak CID 2009;2009;Hiramatsu K et al. Hiramatsu K et al. JAC JAC 1997;40:1351997;40:135--66; ; Hiramatsu K et al. Hiramatsu K et al. LancetLancet 1997;350:16701997;350:1670--3; CDC. 2002 MMWR 2002;51:5653; CDC. 2002 MMWR 2002;51:565--7. 7.
11
Clearly new antibiotics are needed toClearly new antibiotics are needed to
treat infections caused by atreat infections caused by a
resistant, evolving resistant, evolving
Staphylococcus aureusStaphylococcus aureus

12
MicrobiologyMicrobiology
Ian Critchley, PhDIan Critchley, PhDVice President, MicrobiologyVice President, Microbiology
Cerexa, Inc.Cerexa, Inc.

13
Broad Spectrum Activity vs Broad Spectrum Activity vs Clinically Important GramClinically Important Gram--positive Cocci positive Cocci and Gramand Gram--negative Pathogensnegative Pathogens
0.0150.015≤≤ 0.008 0.008 –– 0.030.031212S. dysgalactiaeS. dysgalactiae
0.0150.015≤≤ 0.008 0.008 –– 0.030.03157157S. agalactiaeS. agalactiae
0.50.50015 0015 –– > 16> 1610361036E. coliE. coli (ceftazidime(ceftazidime--susceptible)susceptible)
0.250.25≤≤ 0.008 0.008 –– > 16> 16517517K. pneumoniaeK. pneumoniae (ceftazidime(ceftazidime--susceptible)susceptible)
0.120.12≤≤ 0.008 0.008 –– 11110110Viridans group streptococciViridans group streptococci
≤≤ 0.0080.008≤≤ 0.008 0.008 –– 0.0150.015132132S. pyogenesS. pyogenes
110.12 0.12 –– 2222542254S. aureus S. aureus (MRSA)(MRSA)
0.250.25≤≤ 0.008 0.008 –– 0.50.517111711S. aureus S. aureus (MSSA)(MSSA)
90%90%MIC RangeMIC RangeNo. testedNo. testedCeftaroline MIC (Ceftaroline MIC (µµg/mL)g/mL)
OrganismOrganism
2008 US Surveillance2008 US Surveillance

14
Activities of Ceftaroline, Vancomycin and Activities of Ceftaroline, Vancomycin and Linezolid Against 2008 US Surveillance Linezolid Against 2008 US Surveillance Isolates of Isolates of S. aureusS. aureus
0
20
40
60
80
100
≤ 0.12 0.25 0.5 1 2 4 8 > 8
Ceftaroline Vancomycin Linezolid
Arrows indicate MICArrows indicate MIC9090 values for each agentvalues for each agentData from 2008 US Surveillance, JMI LaboratoriesData from 2008 US Surveillance, JMI Laboratories
MIC (µg/mL)
3965 isolates
Cum
ulat
ive
Isol
ates
, %C
umul
ativ
e Is
olat
es, %

15
Active Against Contemporary Resistant Active Against Contemporary Resistant Phenotypes of Phenotypes of S. aureusS. aureus
1 1 –– 44
0.5 0.5 –– 11
32 32 –– > 64> 64
0.12 0.12 –– 11
MIC Range MIC Range
VRSA VRSA (n = 10)(n = 10)
1 1 –– 2 2 2 2 2 2 LinezolidLinezolid
4 4 4411DaptomycinDaptomycin
1 1 –– 2 2 8811VancomycinVancomycin
0.25 0.25 –– 111111CeftarolineCeftaroline
MIC Range MIC Range MICMIC9090MICMIC9090
DAPDAP--NSNS(n = 7)(n = 7)
VISA VISA (n = 23)(n = 23)
CACA--MRSA MRSA (n = 92)(n = 92)Antimicrobial Antimicrobial
AgentAgent
Saravolatz L et al. Saravolatz L et al. Antimicrob Agents Chemother.Antimicrob Agents Chemother. 2010 54(7):30272010 54(7):3027--3030

16
High Affinity for Modified PBP2a in MRSAHigh Affinity for Modified PBP2a in MRSA
677677> 128> 128CeftriaxoneCeftriaxone
408408128128OxacillinOxacillin
0.160.160.5 0.5 –– 11CeftarolineCeftaroline
PBP2aPBP2aICIC5050 ((μμg/mL)g/mL)
MICMIC((μμg/mL)g/mL)
MRSA Strain 67MRSA Strain 67--00
AntibioticAntibiotic
Moisan H et al. Moisan H et al. J Antimicrob Chemother J Antimicrob Chemother 2010 65(4):7132010 65(4):713--6.6.
17
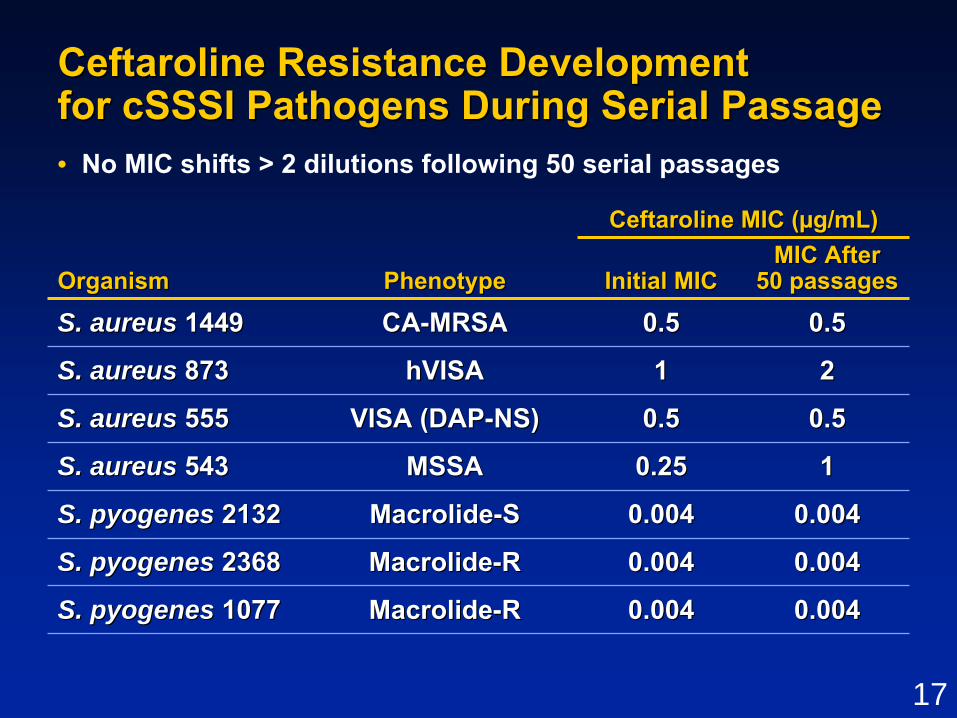
Ceftaroline Resistance Development Ceftaroline Resistance Development for cSSSI Pathogens During Serial Passagefor cSSSI Pathogens During Serial Passage
110.250.25MSSAMSSAS. aureusS. aureus 543543
0.0040.0040.0040.004MacrolideMacrolide--RRS. pyogenes S. pyogenes 23682368
0.0040.0040.0040.004MacrolideMacrolide--SSS. pyogenes S. pyogenes 21322132
0.50.50.50.5VISA (DAPVISA (DAP--NS)NS)S. aureusS. aureus 555555
2211hVISAhVISAS. aureus S. aureus 873873
0.50.50.50.5CACA--MRSAMRSAS. aureus S. aureus 14491449
0.0040.0040.0040.004MacrolideMacrolide--RRS. pyogenes S. pyogenes 10771077
OrganismOrganism Phenotype Phenotype
Ceftaroline MIC (Ceftaroline MIC (µµg/mL)g/mL)
Initial MICInitial MICMIC After MIC After
50 passages50 passages
• No MIC shifts > 2 dilutions following 50 serial passages

18
0
2
4
6
8
10
Control Linezolid Vancomycin CEFTAROLINE
MRSA hVISA
0
2
4
6
8
10
Control Linezolid Vancomycin CEFTAROLINE
Log 1
0C
FU/g
of V
eget
atio
n
Log 1
0C
FU/g
of V
eget
atio
n
**
**
* p * p ≤≤ 0.001 versus control and linezolid0.001 versus control and linezolid** p ** p ≤≤ 0.001 versus control, 0.001 versus control, linezolid,linezolid, and and vancomycinvancomycin
Efficacy of Ceftaroline and Comparators Efficacy of Ceftaroline and Comparators Against Against S. aureusS. aureus in Rabbit Endocarditis Model in Rabbit Endocarditis Model Simulated Human DosingSimulated Human Dosing
MIC = 1MIC = 1µµg/mLg/mL
MIC = 2MIC = 2µµg/mLg/mL

19
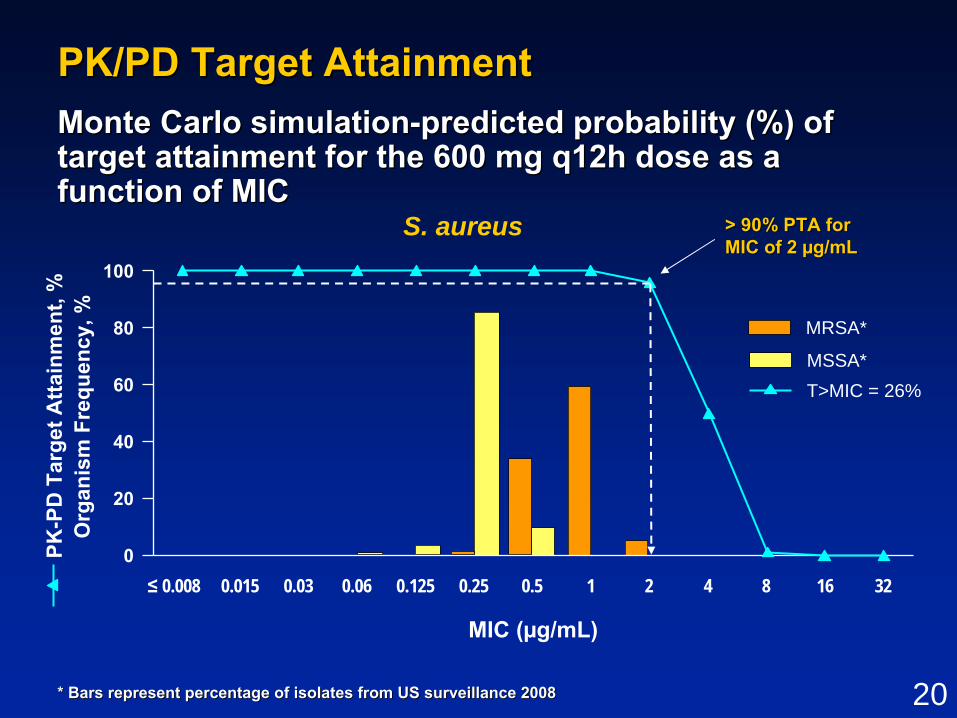
S. aureusS. aureus PK/PDPK/PD
•• %T>MIC is PK/PD parameter that best %T>MIC is PK/PD parameter that best predicts efficacy for cephalosporinspredicts efficacy for cephalosporins
•• Murine neutropenic thigh/ bacteremia Murine neutropenic thigh/ bacteremia infection model standard for determining infection model standard for determining magnitude of %T>MICmagnitude of %T>MIC
•• %T>MIC predicts efficacy for ceftaroline%T>MIC predicts efficacy for ceftaroline
•• ≥≥ 26% T>MIC required for efficacy for 26% T>MIC required for efficacy for S. aureusS. aureus
Andes and Craig. Andes and Craig. Antimicrob Agents ChemotherAntimicrob Agents Chemother 2006 50(4):13762006 50(4):1376--13831383
20
PK/PD Target AttainmentPK/PD Target Attainment
S. aureus
MIC (µg/mL)
MSSA*
MRSA*
* Bars represent percentage of isolates from US surveillance 200* Bars represent percentage of isolates from US surveillance 20088
0
20
40
60
80
100
≤ 0.008 0.015 0.03 0.06 0.125 0.25 0.5 1 2 4 8 16 32
Org
anis
mFr
eque
ncy,
%
Monte Carlo simulationMonte Carlo simulation--predicted probability (%) of predicted probability (%) of target attainment for the 600 mg q12h dose as a target attainment for the 600 mg q12h dose as a function of MIC function of MIC
T>MIC = 26%
PK-P
D T
arge
t Atta
inm
ent,
%
> 90% PTA for > 90% PTA for MIC of 2 MIC of 2 µµg/mLg/mL

21
Interpretive Criteria Proposed by Sponsor Interpretive Criteria Proposed by Sponsor and Agency for and Agency for S. aureusS. aureus
——≤ 0.5——≤ 2S. aureus (includes methicillin-resistant isolates)
RISRIS
FDA-proposed Interpretive Criteria
Sponsor-proposed Interpretive Criteria
Pathogen

22
SummarySummary
•• Ceftaroline exhibits broadCeftaroline exhibits broad--spectrum antibacterial spectrum antibacterial activity against important skin pathogens activity against important skin pathogens
•• Activity against resistant gramActivity against resistant gram--positive bacteria positive bacteria mediated by highmediated by high--affinity binding to modified affinity binding to modified PBPsPBPs
•• Low potential for resistance development Low potential for resistance development in vitroin vitro
•• Dosing regimen of 600 mg q12h provides Dosing regimen of 600 mg q12h provides adequate freeadequate free--drug %T>MIC to cover key skin drug %T>MIC to cover key skin pathogenspathogens
•• Data support breakpoint of Data support breakpoint of ≤≤ 2 2 µµg/mL for g/mL for S. aureusS. aureus

23
Clinical Design and EfficacyClinical Design and Efficacy
Dirk Thye, MDDirk Thye, MDCerexa, Inc.Cerexa, Inc.

24
cSSSI cSSSI –– Study DesignStudy Design
•• Phase 3, multinational, randomized, doublePhase 3, multinational, randomized, double--blindblind•• Noninferiority margin (10%) in clinical response Noninferiority margin (10%) in clinical response
at TOCat TOC•• IV therapy only, no oral stepIV therapy only, no oral step--down therapydown therapy
IV VancomycinIV Vancomycin1 g q12h1 g q12h
plus IV aztreonam 1 g q12hplus IV aztreonam 1 g q12h
IV CeftarolineIV Ceftaroline600 mg q12h600 mg q12h
BaselineAssessment 55--14 days of therapy14 days of therapy
--24h24h
TOC
2121--35 days35 daysafter EOTafter EOT
LFU
88--15 days15 daysafter EOTafter EOT
EOT

25
cSSSI DefinitioncSSSI Definition•• Involving deep soft tissue or requiring significant Involving deep soft tissue or requiring significant
surgical interventionsurgical intervention–– Major abscess required Major abscess required ≥≥ 2 cm of cellulitis extending from 2 cm of cellulitis extending from
abscess marginabscess marginORORInvolving cellulitis/ abscess of lower extremity in Involving cellulitis/ abscess of lower extremity in subjects with DM or PVDsubjects with DM or PVD
•• In addition: In addition: ≥≥ 3 clinical signs and symptoms3 clinical signs and symptoms–– Fever > 38Fever > 38°°C oral or C oral or
hypothermia < 35hypothermia < 35°°CC–– WBC count > 10,000/mmWBC count > 10,000/mm33
–– > 10% bands> 10% bands–– Purulent or seropurulent drainagePurulent or seropurulent drainage
–– ErythemaErythema–– FluctuanceFluctuance–– HeatHeat–– Pain or tendernessPain or tenderness
to palpationto palpation

26
Main Inclusion CriteriaMain Inclusion Criteria
•• Adults aged 18 years or olderAdults aged 18 years or older
•• Need for hospitalization or treatment in Need for hospitalization or treatment in emergency room or urgent care settingemergency room or urgent care setting
•• Expected to require Expected to require ≥≥ 5 days of IV 5 days of IV antimicrobial therapyantimicrobial therapy

27
Main Exclusion CriteriaMain Exclusion Criteria
•• > 24 hours of prior antibiotics for treatment > 24 hours of prior antibiotics for treatment of current cSSSIof current cSSSI
–– Unless treatment failure with microbiological Unless treatment failure with microbiological persistencepersistence
•• Decubitus ulcers and diabetic foot ulcers Decubitus ulcers and diabetic foot ulcers involving osteomyelitis or requiring surgery involving osteomyelitis or requiring surgery
•• Necrotizing fasciitis or gangreneNecrotizing fasciitis or gangrene
•• Immediate lifeImmediate life--threatening disease or threatening disease or evidence of significant hepatic, hematologic, evidence of significant hepatic, hematologic, or immunologic diseaseor immunologic disease

28
Efficacy EndpointsEfficacy Endpoints
•• Primary Efficacy EndpointPrimary Efficacy Endpoint–– Clinical cure rate at TOC in MITT and Clinical cure rate at TOC in MITT and
CE PopulationsCE Populations
•• Secondary Efficacy EndpointsSecondary Efficacy Endpoints–– Clinical cure rate at EOTClinical cure rate at EOT–– Microbiological success rate at TOCMicrobiological success rate at TOC–– Clinical and microbiological response Clinical and microbiological response
by pathogen at TOCby pathogen at TOC–– Relapse at LFURelapse at LFU–– Reinfection / recurrence at LFUReinfection / recurrence at LFU

29
Primary Endpoint DefinitionsPrimary Endpoint DefinitionsDetermined at TOCDetermined at TOC
•• Clinical cureClinical cure–– Total resolution of signs and symptoms or Total resolution of signs and symptoms or
improvement to extent that further antibiotics improvement to extent that further antibiotics not necessarynot necessary
•• Clinical failure (any of the following)Clinical failure (any of the following)–– Persistence, incomplete resolution, or worsening that Persistence, incomplete resolution, or worsening that
requires alternative antibioticsrequires alternative antibiotics–– Surgical intervention due to failure of study drugSurgical intervention due to failure of study drug–– New signs and symptoms at infection siteNew signs and symptoms at infection site–– AE leading to study drug discontinuation when AE leading to study drug discontinuation when
subject required alternative antimicrobial therapysubject required alternative antimicrobial therapy–– Death wherein cSSSI considered causativeDeath wherein cSSSI considered causative
•• IndeterminateIndeterminate

30
Analysis PopulationsAnalysis PopulationsPhase 3 cSSSI Studies CombinedPhase 3 cSSSI Studies Combined
No drug receivedNo drug received
No baseline No baseline pathogenpathogen
Failed evaluability criteria Failed evaluability criteria (eg, failed I / E, no (eg, failed I / E, no outcome assessed, outcome assessed, nonnon--compliance)compliance)
Study P903Study P903--06 (06 (N = 702)N = 702)Ceftaroline = 353Ceftaroline = 353 Vanco/Az = 349Vanco/Az = 349
Study P903Study P903--07 (07 (N = 694)N = 694)Ceftaroline = 348Ceftaroline = 348 Vanco/Az = 346Vanco/Az = 346
ITTITT
MITTMITT
CECE mMITTmMITT
MEME

31
Demographics and Baseline CharacteristicsDemographics and Baseline CharacteristicsPhase 3 cSSSI Studies CombinedPhase 3 cSSSI Studies Combined
3.83.84.24.2Bacteremia, %Bacteremia, %
CharacteristicCharacteristic
MITT PopulationMITT PopulationCeftarolineCeftaroline
N = 693N = 693Vanco/AzVanco/AzN = 685N = 685
AgeAgemean years mean years ±± SDSD≥≥ 65 years, %65 years, %
47.5 47.5 ±± 17.017.017.317.3
48.4 48.4 ±± 16.616.619.019.0
Male, %Male, % 64.164.1 61.261.2
BMI, mean kg/mBMI, mean kg/m2 2 ±± SDSD 28.4 28.4 ±± 7.1 7.1 28.7 28.7 ±± 7.07.0
Diabetes, %Diabetes, % 17.617.6 17.517.5
PVD, %PVD, % 13.413.4 13.613.6

32
Baseline Infection Type: Baseline Infection Type: Wound, Abscess, Cellulitis Wound, Abscess, Cellulitis Individual Phase 3 cSSSI Studies Individual Phase 3 cSSSI Studies ((MITT)MITT)
40%
29%
14%
8%6% 2% 1%
Cellulitis Abscess Infected woundInfected ulcer Infected burn Infected biteOther
36%
40%
13%
2%<1%8%
1%
Study P903Study P903--0606 Study P903Study P903--0707

33
Key Baseline PathogensKey Baseline PathogensPhase 3 cSSSI Studies CombinedPhase 3 cSSSI Studies Combined
151 (28.9)151 (28.9)179 (33.1)179 (33.1)MRSAMRSA
62 (11.9)62 (11.9)63 (11.7)63 (11.7)S. pyogenesS. pyogenes
21 (4.0)21 (4.0)23 (4.3)23 (4.3)E. coliE. coli
21 (4.0)21 (4.0)27 (5.0)27 (5.0)S. agalactiaeS. agalactiae
18 (3.3)18 (3.3)
245 (45.4)245 (45.4)
425 (78.7)425 (78.7)OrganismOrganism
mMITT Population, n (%)mMITT Population, n (%)
CeftarolineCeftarolineN = 540N = 540
Vanco/AzVanco/AzN = 522N = 522
S. aureusS. aureus 409 (78.4)409 (78.4)
MSSAMSSA 258 (49.4)258 (49.4)
K. pneumoniaeK. pneumoniae 19 (3.6)19 (3.6)
S. anginosusS. anginosus groupgroup 15 (2.8)15 (2.8) 18 (3.4)18 (3.4)
S. dysgalactiaeS. dysgalactiae 14 (2.6)14 (2.6) 17 (3.3)17 (3.3)
K. oxytocaK. oxytoca 12 (2.2)12 (2.2) 8 (1.5)8 (1.5)
M. morganiiM. morganii 12 (2.2)12 (2.2) 7 (1.3)7 (1.3)
34
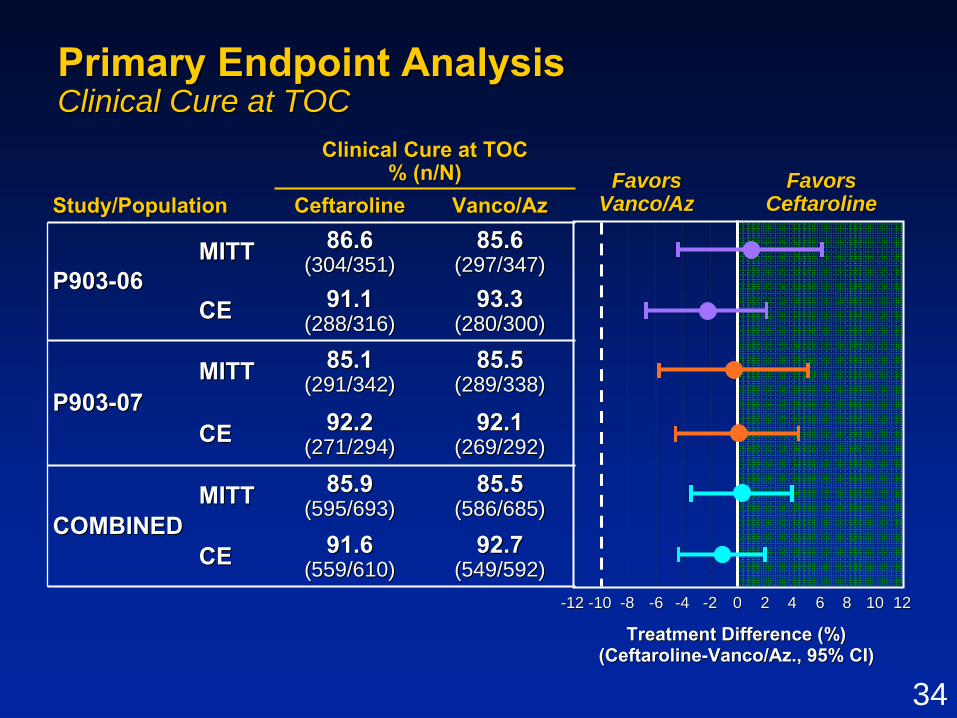
85.6 85.6 (297/347)(297/347)
86.686.6(304/351)(304/351)MITTMITT
P903P903--0606
Clinical Cure at TOCClinical Cure at TOC% (n/N)% (n/N)
Study/PopulationStudy/Population Ceftaroline Ceftaroline Vanco/AzVanco/Az
CECE 91.191.1(288/316)(288/316)
93.3 93.3 (280/300)(280/300)
P903P903--0707MITTMITT 85.185.1
(291/342)(291/342)85.5 85.5
(289/338)(289/338)
CECE 92.292.2(271/294)(271/294)
92.1 92.1 (269/292)(269/292)
COMBINEDCOMBINEDMITTMITT 85.985.9
(595/693)(595/693)85.5 85.5
(586/685)(586/685)
CECE 91.691.6(559/610)(559/610)
92.7 92.7 (549/592)(549/592)
Primary Endpoint AnalysisPrimary Endpoint AnalysisClinical Cure at TOCClinical Cure at TOC
Treatment Difference (%)Treatment Difference (%)(Ceftaroline(Ceftaroline--Vanco/Az., 95% CI)Vanco/Az., 95% CI)
FavorsFavorsVanco/AzVanco/Az
FavorsFavorsCeftarolineCeftaroline
--1010 --88 --66 --44 --22 00 22 44 66 88 1010 1212--1212

35
Clinical Cure by Pathogen Clinical Cure by Pathogen Phase 3 cSSSI Studies CombinedPhase 3 cSSSI Studies Combined
mMITT Population, n/N (%)mMITT Population, n/N (%)Difference Difference (95% CI)(95% CI)
--1.8 (1.8 (--13.3, 9.5)13.3, 9.5)57/62 (91.9)57/62 (91.9)56/63 (88.9)56/63 (88.9)S. pyogenesS. pyogenes
4.4 (4.4 (--3.4, 12.6)3.4, 12.6)124/151 (82.1)124/151 (82.1)155/179 (86.6)155/179 (86.6)MRSAMRSA
--0.1 (0.1 (--5.5, 5.2)5.5, 5.2)233/258 (90.3)233/258 (90.3)221/245 (90.2)221/245 (90.2)MSSAMSSA
1.6 (1.6 (--2.8, 6.1)2.8, 6.1)356/409 (87.0)356/409 (87.0)377/425 (88.7)377/425 (88.7)S. aureusS. aureus
Vanco/AzVanco/AzN = 522 N = 522
CeftarolineCeftarolineN = 540N = 540

36
Clinical Cure by Pathogen Clinical Cure by Pathogen (cont(cont’’d)d)Phase 3 cSSSI Studies CombinedPhase 3 cSSSI Studies Combined
17/18 (94.4)17/18 (94.4)
21/23 (91.3)21/23 (91.3)
25/27 (92.6)25/27 (92.6)OrganismOrganism
mMITT Population, n/N (%)mMITT Population, n/N (%)CeftarolineCeftaroline
N = 540N = 540Vanco/AzVanco/AzN = 522N = 522
S. agalactiaeS. agalactiae 19/21 (90.5)19/21 (90.5)
E. coliE. coli 19/21 (90.5)19/21 (90.5)
K. pneumoniaeK. pneumoniae 14/19 (73.7)14/19 (73.7)
S. anginosusS. anginosus groupgroup 12/15 (80.0)12/15 (80.0) 16/18 (88.9)16/18 (88.9)
S. dysgalactiaeS. dysgalactiae 14/14 (100.0)14/14 (100.0) 15/17 (88.2)15/17 (88.2)
K. oxytocaK. oxytoca 10/12 (83.3)10/12 (83.3) 7/8 (87.5)7/8 (87.5)
M. morganiiM. morganii 11/12 (91.7)11/12 (91.7) 5/7 (71.4)5/7 (71.4)
37
FDAFDA--defined Exploratory Primary Analysisdefined Exploratory Primary AnalysisClinical Response at Study Day 3Clinical Response at Study Day 3
•• FDAFDA--MITT PopulationMITT Population–– Lesion size Lesion size ≥≥ 75 cm75 cm22
–– Infection type: Infection type: •• Infected woundInfected wound•• Major abscess (surrounding erythema Major abscess (surrounding erythema ≥≥ 5 cm)5 cm)•• Deep/ extensive cellulitisDeep/ extensive cellulitis•• Lower extremity SSSI in subjects with DM or PVDLower extremity SSSI in subjects with DM or PVD
•• Clinical respondersClinical responders–– Cessation of lesion spread at Day 3 (based on both Cessation of lesion spread at Day 3 (based on both
length and width compared to baseline)length and width compared to baseline)ANDAND–– Afebrile at Day 3 (Afebrile at Day 3 (≤≤ 37.637.6ooC)C)

38
64.6%64.6%(135/209)(135/209)
74.0%74.0%(148/200)(148/200)P903P903--0606
FDAFDA--MITT PopulationMITT Population% (n/N)% (n/N)
StudyStudy Ceftaroline Ceftaroline Vanco/AzVanco/Az
P903P903--0707 74.0%74.0%(148/200)(148/200)
68.1%68.1%(128/188)(128/188)
COMBINEDCOMBINED 74.0%74.0%(296/400)(296/400)
66.2%66.2%(263/397)(263/397)
FDAFDA--defined Exploratory Primary Analysidefined Exploratory Primary AnalysissClinical Responders at Study Day 3Clinical Responders at Study Day 3
FavorsFavorsVanco/AzVanco/Az
FavorsFavorsCeftarolineCeftaroline
Treatment Difference (%)Treatment Difference (%)(Ceftaroline(Ceftaroline--Ceftriaxone, 95% CI)Ceftriaxone, 95% CI)
--1010 --88 --66 --44 --22 00 22 44 66 88 1010 1212 1414 1616 1818

39
cSSSI Efficacy ConclusionscSSSI Efficacy Conclusions
•• Ceftaroline Ceftaroline noninferiornoninferior to vancomycin + aztreonam to vancomycin + aztreonam for treatment of cSSSIfor treatment of cSSSI
–– PrePre--specified, traditional primary endpoint (TOC)specified, traditional primary endpoint (TOC)–– Exploratory, FDAExploratory, FDA--defined early time point (Day 3)defined early time point (Day 3)–– Secondary and subgroup analyses supportiveSecondary and subgroup analyses supportive
•• Efficacy demonstrated against important pathogensEfficacy demonstrated against important pathogens–– S. aureus, S. aureus, including MRSAincluding MRSA–– S. S. pyogenespyogenes and otherand other StreptococcusStreptococcus spp.spp.–– EnterobacteriaceaeEnterobacteriaceae
•• Totality of data provides robust evidence for the Totality of data provides robust evidence for the effectiveness of ceftaroline for treatment of cSSSIeffectiveness of ceftaroline for treatment of cSSSI
40
Clinical SafetyClinical Safety
David Friedland, MDDavid Friedland, MDVice President, Clinical SciencesVice President, Clinical Sciences
Cerexa, Inc.Cerexa, Inc.
41
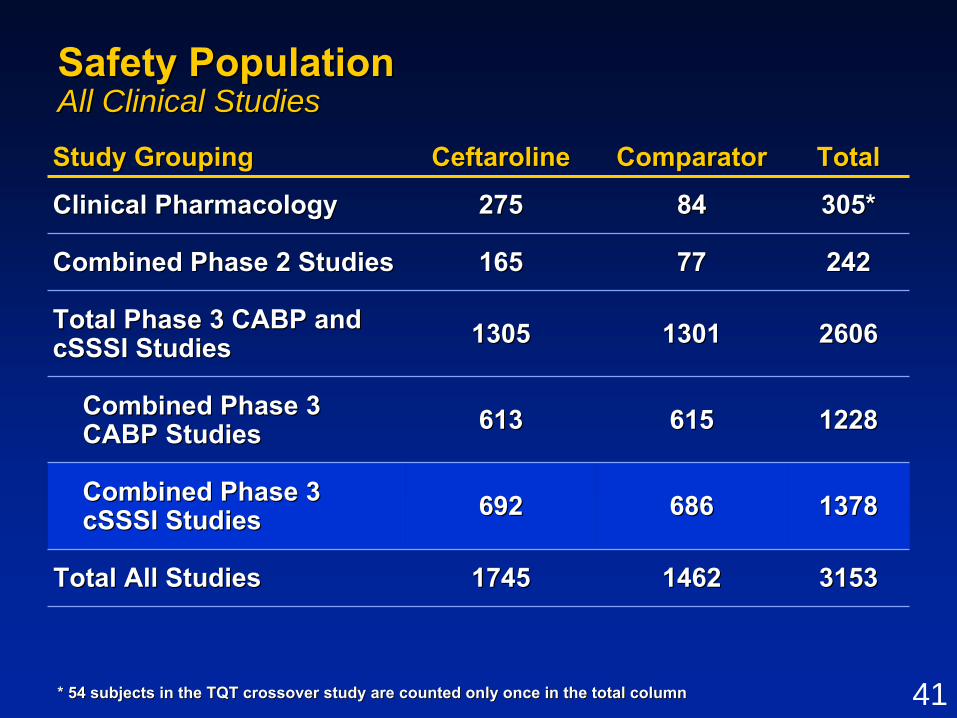
Safety PopulationSafety PopulationAll Clinical StudiesAll Clinical Studies
315331531462146217451745Total All StudiesTotal All Studies
StudyStudy GroupingGrouping CeftarolineCeftaroline ComparatorComparator TotalTotal
Clinical PharmacologyClinical Pharmacology 275275 8484 305*305*
Combined Phase 2 StudiesCombined Phase 2 Studies 165165 7777 242242
Total PhaseTotal Phase 3 CABP and 3 CABP and cSSSI StudiescSSSI Studies 13051305 13011301 26062606
Combined Combined PhasePhase 3 3 CABP StudiesCABP Studies 613613 615615 12281228
Combined Phase 3 Combined Phase 3 cSSSI StudiescSSSI Studies 692692 686686 13781378
* 54 subjects in the TQT crossover study are counted only once i* 54 subjects in the TQT crossover study are counted only once in the total columnn the total column

42
Adverse Event OverviewAdverse Event OverviewPhase 3 cSSSI StudiesPhase 3 cSSSI Studies
000.40.4DeathDeath
Safety EventSafety Event
Safety PopulationSafety Population, %, %
CeftarolineCeftarolineN = 692N = 692
Vancomycin + Vancomycin + AztreonamAztreonam
N = 686N = 686
Any TEAEAny TEAE 44.744.7 47.547.5
Any SAEAny SAE 4.34.3 4.14.1
Discontinuations Discontinuations Due to TEAEDue to TEAE 3.03.0 4.84.8

43
Adverse Events Adverse Events ≥≥ 2% in Ceftaroline Subjects2% in Ceftaroline SubjectsPhase 3 cSSSI Studies Phase 3 cSSSI Studies
1.21.22.02.0DizzinessDizziness2.82.82.22.2Pruritus generalizedPruritus generalized2.52.52.52.5InsomniaInsomnia
2.62.62.92.9VomitingVomiting
5.15.15.95.9NauseaNausea
8.28.23.53.5PruritusPruritus3.83.84.94.9DiarrheaDiarrhea4.54.55.25.2HeadacheHeadache
2.62.62.62.6ConstipationConstipation
2.52.53.23.2RashRash
Safety EventSafety Event
Safety Population, %Safety Population, %
CeftarolineCeftarolineN = 692N = 692
Vancomycin + Vancomycin + AztreonamAztreonam
N = 686N = 686

44
Serious Adverse EventsSerious Adverse EventsPhase 3 cSSSI StudiesPhase 3 cSSSI Studies
•• Low and similar incidenceLow and similar incidence–– 4.3% ceftaroline vs 4.1% vancomycin + aztreonam4.3% ceftaroline vs 4.1% vancomycin + aztreonam
•• Few were assessed as study drug relatedFew were assessed as study drug related–– 0.6% ceftaroline vs 0.4% vancomycin + aztreonam0.6% ceftaroline vs 0.4% vancomycin + aztreonam
•• No individual SAE occurred in > 2 ceftaroline No individual SAE occurred in > 2 ceftaroline subjectssubjects

45
AEs Leading to Discontinuation of AEs Leading to Discontinuation of Study Drug or StudyStudy Drug or StudyPhase 3 cSSSI StudiesPhase 3 cSSSI Studies
•• Low and similar incidenceLow and similar incidence–– 3.0% ceftaroline vs 4.8% vancomycin + aztreonam3.0% ceftaroline vs 4.8% vancomycin + aztreonam
•• Skin and Subcutaneous Tissue Disorders was Skin and Subcutaneous Tissue Disorders was only body system with incidence > 1% only body system with incidence > 1%
–– 1.2% ceftaroline vs 2.5% vancomycin + aztreonam1.2% ceftaroline vs 2.5% vancomycin + aztreonam
•• Only AE leading to discontinuation in > 2 Only AE leading to discontinuation in > 2 subjects in ceftaroline group was subjects in ceftaroline group was hypersensitivityhypersensitivity
–– 0.4% ceftaroline vs 0.9% vancomycin + aztreonam0.4% ceftaroline vs 0.9% vancomycin + aztreonam

46
Summary of DeathsSummary of DeathsPhase 3 cSSSI StudiesPhase 3 cSSSI Studies
•• 3 deaths prior to LFU visit3 deaths prior to LFU visit–– 3 ceftaroline vs 0 vancomycin + aztreonam3 ceftaroline vs 0 vancomycin + aztreonam–– None study drug relatedNone study drug related–– Due to underlying disease: Due to underlying disease:
•• Single cases of: respiratory failure; neoplasm Single cases of: respiratory failure; neoplasm progression; cardiopulmonary failureprogression; cardiopulmonary failure
–– Deaths occurred between 3 and 23 days after EOTDeaths occurred between 3 and 23 days after EOT
•• Additional 4 deaths after LFU visitAdditional 4 deaths after LFU visit–– 2 ceftaroline vs 2 2 ceftaroline vs 2 vancomycin + aztreonamvancomycin + aztreonam–– None study drug relatedNone study drug related

47
Safety ConclusionsSafety ConclusionsPhase 3 cSSSI StudiesPhase 3 cSSSI Studies
•• Safety results similar between ceftaroline Safety results similar between ceftaroline and vancomycin + aztreonam including: and vancomycin + aztreonam including:
–– TEAEsTEAEs–– SAEsSAEs–– Discontinuations due to AEDiscontinuations due to AE–– DeathsDeaths
•• No safety signal identified by review of No safety signal identified by review of Organ System or safety events of interestOrgan System or safety events of interest
•• Ceftaroline well tolerated and safety profile Ceftaroline well tolerated and safety profile reflective of cephalosporin classreflective of cephalosporin class

48
Ceftaroline in ABSSSICeftaroline in ABSSSITherapeutic PerspectiveTherapeutic Perspective
G. Ralph Corey, MDG. Ralph Corey, MDProfessor of MedicineProfessor of Medicine
Duke Clinical Research InstituteDuke Clinical Research Institute

49
Ceftaroline CharacteristicsCeftaroline Characteristics•• Demonstrated EfficacyDemonstrated Efficacy
–– Against wide range of pathogensAgainst wide range of pathogens–– Across varying infections and populationsAcross varying infections and populations–– ProtocolProtocol--defined endpointsdefined endpoints–– New FDANew FDA--defined early endpointsdefined early endpoints
•• Cessation of spread and resolution of feverCessation of spread and resolution of fever•• Percent reduction in infection areaPercent reduction in infection area
•• Safe and well toleratedSafe and well tolerated

50
When Would I Use Ceftaroline for ABSSSI?When Would I Use Ceftaroline for ABSSSI?
•• In communityIn community--acquired infections acquired infections –– When MRSA suspectedWhen MRSA suspected–– When gramWhen gram--negative bacilli suspectednegative bacilli suspected
•• In nosocomial infections when MRSA is In nosocomial infections when MRSA is suspectedsuspected
•• As a replacement for double coverage for As a replacement for double coverage for patients with suspected/ proven MRSA patients with suspected/ proven MRSA infections involving SSSinfections involving SSS
•• I would use in patients in my practiceI would use in patients in my practice

51
Infectious Diseases Society of AmericaInfectious Diseases Society of America


















