ANTI CANCER DRUGS 1. 2 INTRODUCTION Definition: Cancer is a disease characterized by uncontrolled...
44
ANTI CANCER DRUGS 1
-
Upload
brent-baker -
Category
Documents
-
view
217 -
download
2
Transcript of ANTI CANCER DRUGS 1. 2 INTRODUCTION Definition: Cancer is a disease characterized by uncontrolled...

ANTI CANCER DRUGS
1

2
INTRODUCTIONDefinition: Cancer is a disease characterized by uncontrolled multiplication and spread of abnormal forms of the body's own cells.
The terms cancer, malignant neoplasm (neoplasm simply means 'new growth') and malignant tumor are synonymous.
TWO TYPES OF TUMOUR1 BENIGN TUMOUR2 MALIGNANT TUMOUR

3
THE PATHOGENESIS OF CANCER.
Cancer cells manifest four characteristics that distinguish them from normal cells1.uncontrolled proliferation 2.dedifferentiation and loss of function 3.invasiveness 4.Metastasis

Compartment A
• Continuously dividing cells
Compartment B
• Resting cells in G0 phase• Have an ability to enter the cell cycle
Compartment C
• No ability to divide
4
General principles for cancer therapy
• The cells of a solid tumour can be divided into 3 compartments:

• Only the cells in the compartment A i.e. the dividing cells are susceptible to the main currently available cytotoxic drugs. But these cells are only 5% of the entire tumour.
• The cells in the compartment B tend to pose a problem as they are not susceptible to cancer chemotherapy but are likely to enter the compartment A following the course of chemotherapy.
• Most of the currently available anti cancer drugs are antiproliferative. They have no specific inhibitory effect on invasiveness, the loss of differentiation or the tendency to metastatise. Their main action is on S phase of the cell cycle and hence results into the DNA damage causing apoptosis.
5

• Lastly , the cancer chemotherapy also acts on the normal tissues and thereby they produce a some general toxic effects like :• bone marrow suppression (myelosuppression) resulting in
decreased leucocyte production and hence increased resistance to infection.
• Impaired wound healing• Loss of hair• Damage to the gastrointestinal epithelium• Growth retardation in children• Sterility• Teratogenecity• They can themselves be carcinogenic• Kidney damage due to excess urate deposition in the tubules ( due
to extensive purine catabolism)• Severe nausea and vomitting ( reduced patient compliance)
6

DRUGS USED IN CANCER CHEMOTHERAPY1. Cytotoxic Drugs• Alkylating agents• Antimetabolites• Antimitotics• Cytotoxic antibiotics• Plant derivatives
2. Hormones 3. Miscellaneous agents
7

Alkylating agents
• The nitrogen at position 7 (N7) of guanine is strongly nucleophilic and is the main target for the alkylating agents. N1 and N3 of adenine and N3 of cytosine may also be affected. • Most of these agents are bifunctional i.e. they have
two alkylating groups and can cause inter as well as intrachain cross-linking.• This can not only interfere with transcription but
also replication .
8

• Other effects of alkylation at guanine N7 are excision of the guanine base with main chain scission, or pairing of the alkylated guanine with thiamine instead of cytosine and eventually substitution of the GC pair by an AT pair.• The effects of this alkylation are manifested during S
phase, resulting in block at G2 phase and subsequent apoptotic cell death.• Side effects:• bone marrow depression,• git disturbances at very high doses.• neurotoxicity• With prolonged use it can lead to sterility
9

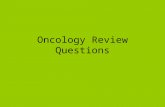
Intrastrand and interstrand crosslinking in DNA
10

Types of alkylating agents are:
1. Nitrogen MustardsCyclophosphamideIfosphamideChlorambucilMelphalanMecholrethamineBendamustineGlufosfamide
2. NitrosoureasLomustineCarmustineSemustineStreptozocine
3. Agents with trizene groupDacarbazineProcarbazineTimozolamide
4. EthelenaminesThiotepaHexamethylmelamine
5. Agents with sulfate groupBusulfan
Platinum compounds:Cisplatin, carboplatin 11

Cyclophosphamide/ifosfamide are prodrugs
Metabolized to aldophosphamide
Tissues
Acrolein Phosphoramide mustard
causes hemorrhagic cystitis Alkyl group which causes N7 guanine and causes
inhibition of DNATreatment: Intake of fluids and
–SH group donors like Mesna
Hepatic cytochrome oxidase
12

Other imp points of alkylating agents:
Streptozocine: • destroys the beta cells of pancreas so approved for treatment of
insulinoma. Also used to induce diabetes mellitus in experimental animals.
Busulfan:• Selective action on bone marrow, depressing the formation of
granulocytes and platelets in low dose and red blood cells in high dose. • Use: chronic granulocytic leukemia, as a preparative for bone marrow
transplantation• Main side effect is pulmonary fibrosis and neurotoxicity (seizures)• Also can cause adrenal suppression
Estramustine: Estrogen + mechlorethamine• Approved for the treatment of prostatic carcinoma• S/E – Gynaecomastia, loss of libido, thromboembolism
13

Cisplatin: • M/A: • it has a platinum atom surrounded by two chloride atoms and two ammonia
groups. When it enters the cell the cl- group dissociates leaving the reactive complex to interact with DNA. It causes intrastrand crosslinking between N7 and O6 of adjacent guanine molecules leading to denaturation of DNA.
• Side effects: • nephrotoxicity,(hydration and diuresis required)• Severe nausea and vomiting (ondansetron given)• Tinnitus and hearing loss• Low myelotoxicity • Others: peripheral neuropathies, huperuricaemia, anaphylactic
reactions.• Use: solid tumours of testes and ovaryCarboplatin: derivative of cisplatin• More myelotoxicity• Less neurotoxocity, nephrotoxicity , ototoxicity, nausea and vomiting.• Cisplatin – max S/E and min potency• Carboplatin – intermediate• Oxaliplatin – min S/E and max potency
14

Antimetabolites • These drugs act in the s-phase of the cell cycle so only dividing
cells are responsiveFolic acid analogues Purine analogues Pyrimidine analoguesMethotrexate 6-mercaptopurine 5-flourouracilPemetrexed 6-thioguanine Capecitabine cladrabine Gemcitabine Pentostatin Cytarabine Fludrabine
Methotrexate:• Inhibitor of dihydrofolate reductase enzyme which is required
for synthesis of thymidylate and hence DNA formation.• At high dose – by diffusion enters the normal cells and inhibits
DNA formation in the normal cells 15

S/E: BM suppression, diarrhoea, mucositis due to inhibition of rapidly proliferating cells
Drug of choice for overdose: • Folinic acid or leucovorin or citovorum factor. It directly gets
converted to tetrahydrofolate bypassing the requirement of dihydrofolate reductase.
• On the surface of cancer cells, there is an influx pump which takes in methotrexate at low dose. Inside the cells it binds with polyglutamine
Forms methotrexate polyglutamine complex which serves as reservoir of methotrexate leading to long lasting effect.
• MTX has affinity for cells having high chromosome no. like placental, fetal and germ cells so it is drug of choice for choriocarcinoma in which single drug treatment is used.
16

• Eliminated by kidney- tubular secretion by acidic pumps.• NSAIDS can saturate these pumps leading to decreased secretion of MTX
causing toxicity.
Uses:• Almost all types of cancers, Burkitt’s lymphoma, choriocarcinoma, breast
carcinoma, osteosarcoma.• It also has immunosuppressive property so it is used for organ
transplant, RA, IBD, Psoriasis, Ectopic pregnancy.Resistance: - mutation of influx pumps - induction of efflux pumps - mutation of DHFRase enzyme
Pemetrexed:• inhibitor of thymidine synthase.• Folic acid or vit B12 can reduce the toxicity of pemetrexed• Approved for tumour of mesothelioma• S/E- peripheral neuropathy in hand and foot region called as hand-foot
syndrome.
17

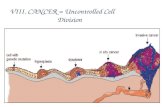
Mechanism of action methotrexate and fluorouracil18

Pyrimidine analogues:• 5-FU is the prodrug• Active metabolite is 5- fluorodeoxyuridine monophosphate• Cells are unable to differentiate between 5F-dUMP and dUMP
5F-dUMP CH3 thymidine synthase
Fluorothymidine
Inhibits DNA synthesis because of incorporation of modified neucleotide
• Leucovorin given with 5FU increases formation of fluorothymidine causing increased effect of 5FU. This concept is used in colorectal cancer.
FOLFOX regimen of colorectal cancer. FOL- Folinic acidFOLFIRI F- 5FU, OX- oxaliplatin, IRI- irinotecan 19

• Metabolized at the level of lung tissue by endothelial enzymes.• Given by i.v route• Alternative: capecitabine which is prodrug of 5FU given by oral
route.
Gemcitabine/Cytarabine: • Act as prodrugs. Combines with 3PO4 groups and converts to
Gemcitabine triphosphate modified nucleotides which withCytarabine triphosphate the help of DNA polymerase gets
incorporated into DNA inhibiting DNA synthesis
Gemcitabine use: non beta cells cancer of pancreas S/E: flu like symptoms 20

Purine analogue: 6-MP ( prodrug)
6-methylmercaptopurine HGPRTase
Purine structure DNA polymerase
Incorporation in DNA. So inhibition of DNA synthesis.• Metabolized by xanthine oxidase to form uric acid.• Some part is metabolized by methyl transferase enzyme.
6-Tiagabine: acts in the same way as 6-MP but metabolized only by methyl transferase enzyme.
Azathioprine: prodrug of 6-MP. Used only as immunosuppressive. 21

Pentostatin: inhibitor of adenosine deaminase. Used in hairy cell leukemia.
Cladribine: used in hairy cell leukemia
Antimitotics1. Vinka alkaloids2. Texans3. Ixebepilone
Vinka alkaloids: • vincristine, vinblastine, vinorelbine• MOA: inhibition of spindle formation• S/E: - SIADH - Bone marrow suppression - Peripheral neuropathy. 22

Taxanes: Paclitaxel, docitexal, cabazitexal• MOA: inhibition of spindle formation• Approved for the treatment of breast carcinoma• Paclitaxel + carboplatin: treatment of choice in ovarian cancer.• S/E: Hypersensitivity reaction and to inhibit it paclitexal is
combined with albumin to form abpaclitaxel• bone marrow suppression• peripheral neuropathy
Ixebepilone: MOA same as texans but more potent than paclitexal so used in treatment of paclitexal resistant breast cancer
Advantage – no hypersensitivity reaction
23

Anti tumour antibiotics1. Anthracycline antibiotics2. Mitoxantrone3. Mitomycin c 4. Bleomycin5. Actinomycin D
Most imp mechanism of action – Free radicle formation
S/E: • Cardiotoxicity – cardiomyopathy after 2-3 months. Treatment– dexrazoxane, alpha – tocoferol – they are free
radicle scavengers• Bone marrow suppression
24

ANTHRACYCLINES:• Doxorubicin,Idarubicin, epirubicin, aclarubicin, mitoxantrone.• Mechanism of action of Doxorubicin: inhibits both DNA and
RNA synthesis by an effect on topoisomerase II (DNA gyrase)• Given by i.v. infusion • Epirubicin is less cardiotoxic than doxorubicin.• Mitoxantrone has dose-related cardiotoxicity .
Dactinomycin: Mechanism : it intercalates in the minor groove of DNA and interferes with the movement of RNA polymerase and thus prevents transcription.
25

• Red urine• Radiation recall phenomenon – seen after many years of
radiation. Epithelial damage and vesicles seen at the same site after taking drugs
• Most common S/E – Nausea, vomitting, diarrhoea
MITOXANTRONE• Same as above but cardiotoxicity is rarely seen.• Associated with blue urine, blue nails, blue sclera• Indication – Multiple sclerosis
26

MITOMYCIN C• Functions as a bifunctional alkylating agent• Very potent drug but causes toxicity when used systemically.• So not used via systemic route.Uses• Tracheal stenosis and • Oesophageal stenosis• Superficial bladder cancer
BLEOMYCIN• With the help of Fe2+ bleomycin converts O2 to free radicles
and causes DNA damage. It is the only anticancer drug that can be given via any route.
27

• Metabolized by bleomycin hydrolase which is present all over the body except skin and lung. So the main S/E is lung and skin fibrosis.
• It causes little myelosuppression.
• RADIOACTIVE IODINE : I131: Used in treatment of thyroid tumours.
28

• TOPOISOMERASE INHIBITORS
Etoposide Irinotecan Teniposide Topotecan(Topoisomerase II) (TopoisomeraseI)
campothecins
• All drugs eliminated by kidney. Caution in CRF• Except Irinotecan which is a drug metabolized by liver to
active SN38 which is eliminated by kidney.
• Cholinergic properties – diarrhoea present since day 1 of therapy.
• USE – colorectal carcinoma.29

Hormones:• Glucocorticoids: They have inhibitory effect on lymphocyte
proliferation • Used in leukemias and lymphomas
• Estrogens: Fosfeterol (a prodrug which is activated by acid phosphatase in prostatic tissue ) block the effect of androgens in androgen-dependent prostatic tumours.
• Estrogen can also be used to recruit resting mammary cells from compartment B to compartment A thus allowing greater killing efficiency of cytotoxic drugs.
• Progesterons: Megesterol and medroxyprogesterone have been useful in endometrial neoplasms and renal tumours.
30

• Gonadotrophin- releasing hormone analogues:• Goserelin can inhibit gonadotrophin release. • Used to treat advanced breast cancer in postmenopausal women
and prostate cancer.
• Analogue of somatostatin:octreotide is used to treat various hormone secreting tumours of the git such as VIPomas, glucagonomas, gastrinomas. These tumors express somatostatin receptors, activation of which inhibits cell proliferation and hormone secretion.
31

Hormone antagonists:• Anti-estrogens: Tamoxifen is effective in hormone dependent
breast cancer. In breast tissue, Tamoxifen competes with endogenous oestrogens for oestrogen receptors and inhibits transcription of oestrogen- responsive genes.
• Also has cardioprotective effect by preventing oxidation of LDL.
• Anti-androgens: Flutamide and cyproterone are used in prostate tumours.
• Adrenal hormone synthesis inhibitor: Formestane acts at a late stage of sex hormone synthesis by inhibiting enzyme aromatase. Trilostane and aminoglutethimide also inhibit sex hormone synthesis.
32

Miscellaneous agents:L-ASPERGINASE(Crisantaspase)
• Only enzyme used as anticancer drug.• Metabolize aspergine to urea or ammonia• Normal cells can form all aspergine on their own but cancer cells
cannot form their own aspergine and depend on plasma aspergine. L-asperginase depletes plasma aspergine causing cancer cell death.
USE- LeukemiasS/E • Hyperammonemia• Protein deficiency• Clotting and anticlotting factors are proteins so clotting
disturbances• Hupoalbuminemia
33

HYDROXYUREA• Inhibitor of ribonucleotide reductase enzyme which converts
ribose sugar to deoxyribose sugar incorporated in DNA• Acts on the S phase of the cell cycle• Side-effect: myelosupression
34

Miscellaneous agents:• Imatinib mesylate: it is a small molecule which inhibits
signalling pathway kinases. It inhibits platelet- derived growth factor.
• It also inhibits cytoplasmic kinase which is a unique factor in pathogenesis of chronic myeloid leukemia and hence licensed for the treatment of this tumour.
• Biological response modifiers: agents which enhance the host response.
• Examples: interferon γ, aldesleukin and tretinoin.
35

Monoclonal antibodiesRituximab:• Attaches to CD20 proteins on B cells and kills B cells by
complement mediated lysis or by inducing apoptosis.• Use: B cell lymphoma• Side effects: hypotension, chills and fever initially • Hypersensitivity reaction• May make cardiovascular diseases worse
Trastuzumab:• Binds to a protein called Her2/neu. (member of the epidermal
growth factor receptor family- receptors with integral tyrosine kinase activity)
• Use: in some patients with breast cancer, these receptors are overexpressed
• Side effects : similar to rituximab
36

• GEMTUZUMAB-OZAGAMYCIN COMBINATION• MOA – DNA inhibition by formation of free radicles.
CELL CYCLE SPECIFIC agents NON CELL CYCLE SPECIFIC agents
G1/S –Etoposide Topoisomerase inhibitors
S – Antimetabolite Hydroxyurea
Alkylating agents
G2/M – Etoposide Bleomycin
All anticancer antibiotics except bleomycin
M – vinka alkaloids taxens Ixebepilone Estramustine
Platinum compounds
37

REGIMENS FOR DIFFERENT TUMOURS:REGIMEN DRUGS
COAP Cyclophosphamide+Vincristine+ cytarabine+prednisolone
POMP Prednisolone+Oncovin(Vincristine)+ Mtx+Purinethol(6-MP)
CART Cytarabine+Asparginase+Rubidomycin(daunorubicin)+ 6-TG
MOPP Mechlorethamine+Oncovin+ Procarbazine+Prednisolone
VAMP Vincristine+Amethopterine(MTX)+ 6-MP+Prednisolone
38

MALIGNANCY FIRST LINE THERAPY
SECOND LINE DRUGS
Acute leukaemias VAMP Cytarabine, L-asparginase, Mtx, Doxorubicin
Hodgin’s Disease MOPP Bleomycine, Procarbazine, lomustine, ifosphamide, doxorubicin
Prostate carcinoma Flutamide+GnRH agonist
Doxorubicin, cisplatin, cyclophophamide, 5-FU
Breast carcinoma Tamoxifen, Mtx, 5-FU
Prednisolone, Vincristine, Paclitaxel, cyclophosphamide, Mitoxantrone
39

Malignancy First line drugs Second line drugs
Ovarian carcinoma Cisplatin, carboplatin, paclitaxel, cyclophosphamide, Doxorubicin
Melphalan, Chlorambucil, 5-FU, Mtx, Vincristine, Topotecan
Endometrial cancer Progestin, tamoxifen
Doxorubicin, cisplatin
Testicular tumours Mtx, bleomycin, etoposide, cisplatin, carboplatin
Actinomycin, ifosfamide, doxorubicin, vinblastine, melphalan
Lung cancer Cyclophosphamide, Vincristine, Doxorubicin
Carboplatin, Mtx, Lomustine, topotecan, etoposide
40

Dealing with side effects:
• EMESIS:• Mainly seen with cisplatin and other alkylating agents.• Treatment: ondansetron or granisetron can be used• Metoclopromide can also be used . But since it causes extra-
pyrimidal side effects, diphenhydramine can be used instead.
41

• MYELOSUPPRESSION• Removing some of the patients bone marrow prior to giving
cytotoxic drugs, purging it of the cancer cells and replacing it later• Administration of Molgramostim, then harvesting stem cells from
blood and multiplying them in-vitro with the relevant heomopoietic growth factors.
• Introducing mutated gene into the extracted bone marrow which confers multidrug resistance so that when this marrow is replaced the normal cells remain resistant to cytotoxic drugs but the cancer cells don’t .(a possibility)
42

Newer anti cancer targets• The Ras proteins- Farnesyl transferase inhibitors are in
development• Tyrosine Kinase : Agents interfering with the epidermal growth
factor receptor tyrosine kinase activity can be developed.• Cyclin and cyclin dependent kinases: Flavopiridol• Telomerase inhibitors• Angiogenesis and matrix metalloproteinase inhibitors: • Cyclo-oygenase inhibitors: COX-2 is overexpressed in many
cancer cells. Cox-2 inhibitor celecoxib has shown to reduce mammary tumours in animal models.
• P53 gene: cancer cells carry a mutated p53 gene• Antisense oligonucleotides: inhibit gene expression in tumour
cells.Example : augmerosen downregulates Bcl-243

REFERENCES:
1. Rang HP, Dale MM, Ritter JM, Moore PK Pharmacology. 5th edition. New Delhi: Elsevier publication; 2002, p. 693-709
2. Joel HG, Lee LE, Gilmann Ag. Goodmann and Gillmann’s The pharmacological basis of Therapeutics. 11th edition.Mc-Graw-Hill publication; 2006, p.670-680
3. Tripathi KD, Essentials of Medical Pharmacology. 6th edition. Jaypee Brothers Medical Publishers(P)LTD; 2008, p.:819-836
44