Anti Ameobic Drugs
32
AMOEBIASIS Vipul Agarwal M.Pharm I Year BBAU Lucknow
-
Upload
vipul-agarwal -
Category
Health & Medicine
-
view
51 -
download
3
Transcript of Anti Ameobic Drugs

AMOEBIASISVipul Agarwal
M.Pharm I Year
BBAU
Lucknow

AMOEBIASIS
Amoebiasis is caused by E. histolytica, a protozoa parasite
Approximately 48 million individuals suffer from amoebiasis throughout the world
At least 40 thousand deaths are attributable to amoebiasis
Ranks third among parasitic causes of deaths, behind only malaria and schistosomiasis
1
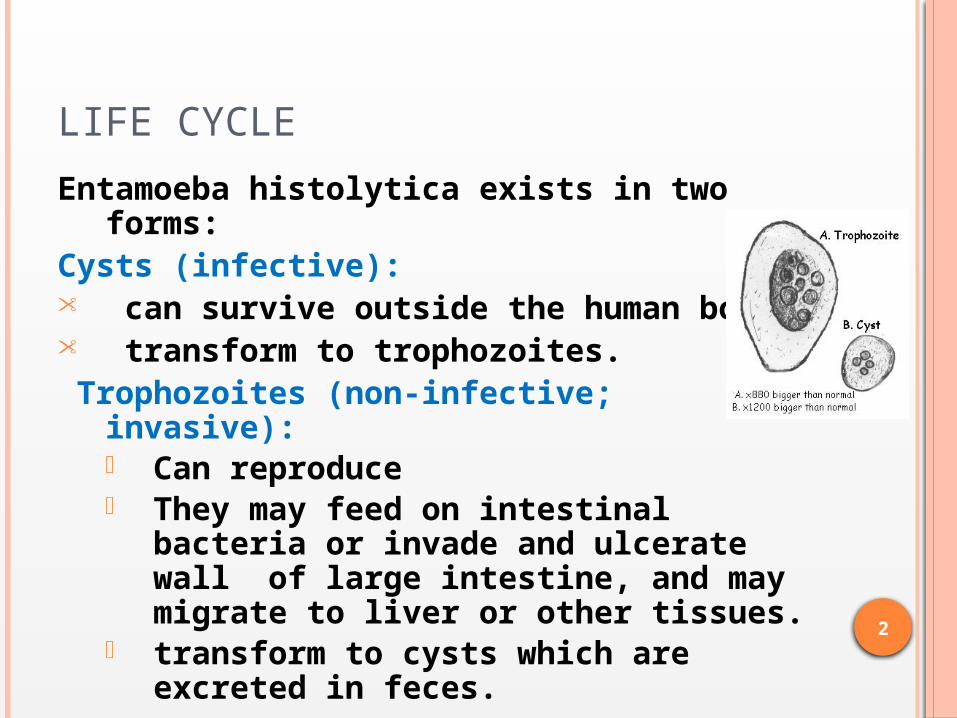
LIFE CYCLE
Entamoeba histolytica exists in two forms:
Cysts (infective):• can survive outside the human body.• transform to trophozoites. Trophozoites (non-infective; invasive):
• Can reproduce • They may feed on intestinal bacteria
or invade and ulcerate wall of large intestine, and may migrate to liver or other tissues.
• transform to cysts which are excreted in feces.
2

LIFE CYCLE
3
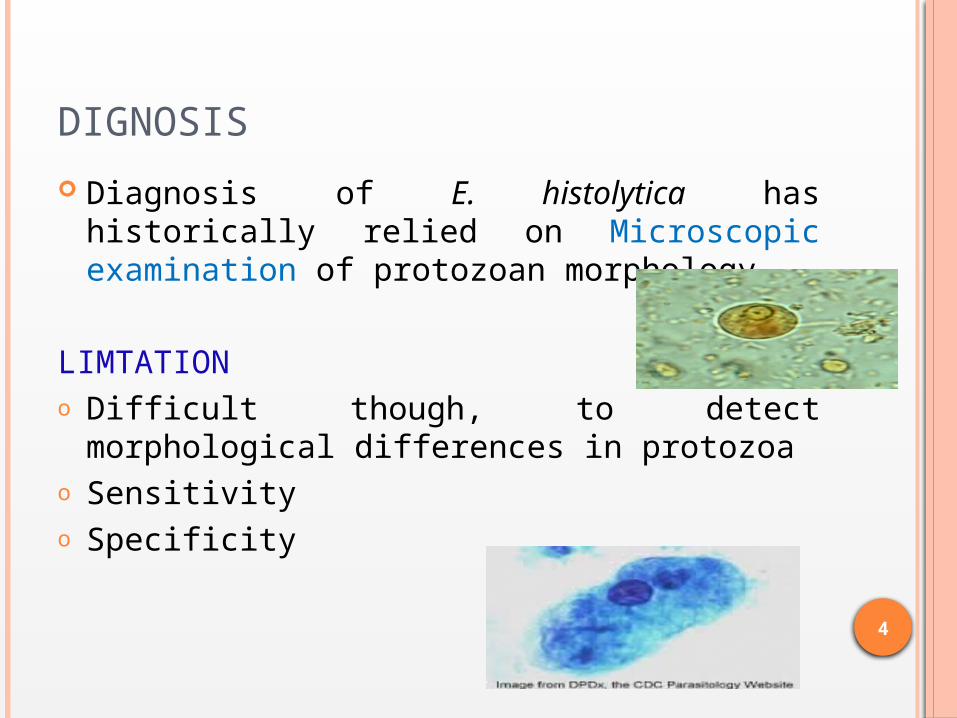
DIGNOSIS
Diagnosis of E. histolytica has historically relied on Microscopic examination of protozoan morphology
LIMTATIONo Difficult though, to detect morphological
differences in protozoao Sensitivity o Specificity
4

NEWER DIAGNOSTIC TECHNIQUE
DNA based methods:
The ability of Polymerase Chain Reaction (PCR) to specifically amplify minute amounts of pathogen DNA has revolutionized the diagnosis of amoebiasis
Most, but not all, rely on amplifying unique regions of the SSUrRNA
Coupled with antigen detection PCR, may offer the best way to diagnose patients
5

NEWER DIAGNOSTIC TECHNIQUE-CONTD
ELISA
Becoming increasingly popular in diagnoses symptomatic patients are thought to have
high levels of specific antibodies, serum anti-lectin immunoglobulin G (IgG), associated with the E. histolytica infection within one week of symptoms,
6

AVAILABLE DRUGS
1. Tissue amoebicides: Intestinal and extra-intestinal:
Nitroimidazoles – Metronidazole, Tinidazole, Secnidazole, Ornidazole, Satranidazole
Alkaloides – Emetine and Dihydroemetine Extra-intestinal –Chloroquine
2. Luminal amoebicides: Amides – Diloxonide furoate, Nitazoxamide 8-Hydroxyquinolines – Quinodochlor, Antibiotics - Tetracycline
7

METRONIDAZOLE – PROTOTYPE
Belongs to Nitroimiidazole CLass Mixed Amoebicide Originally discovered and used for
Trichomoniasis in 1959 Broad spectrum cidal activity against ---
Protozoa Acts on trophozoites. Has no effect on cysts.
8
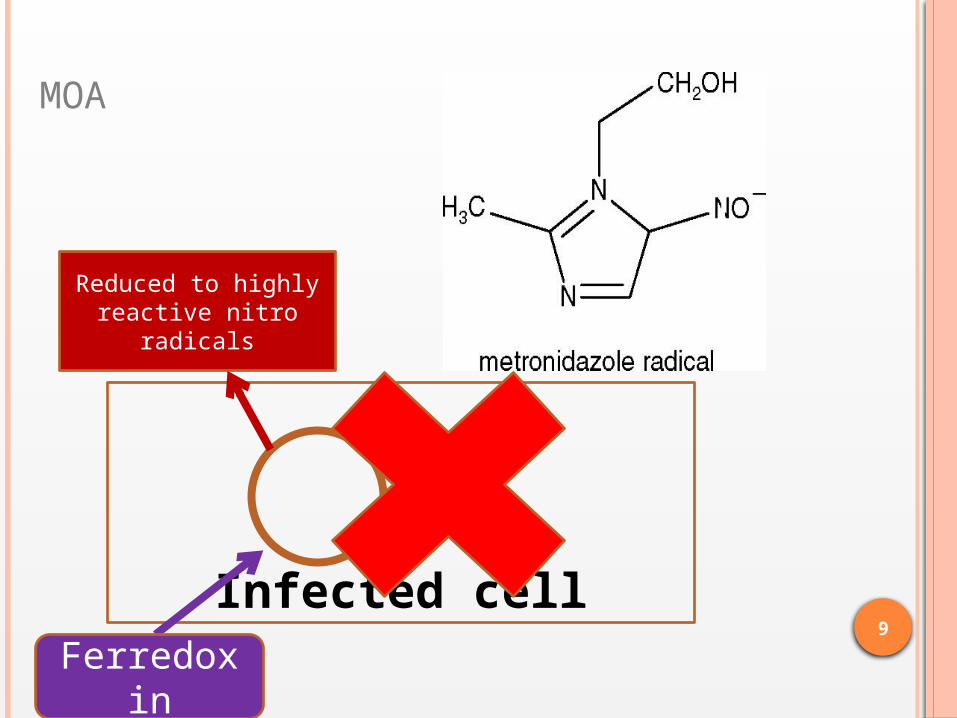
Infected cell
Reduced to highly reactive nitro
radicals
Ferredoxin
MOA
9

Competes with biological electron
acceptor
Acts as electron sink –electrons by
PFOR p/w
Energy metabolism disrupted
Reduced to highly reactive nitro
radicals
10

METRONIDAZOLE – CONTD. Pharmacokinetics: Well absorbed from the small intestine Metabolized in liver by oxidation and
glucoronidation Half life – 8 Hrs
ADRs: Most common - Nausea, Vomiting, abdominal
cramps and metallic taste Less frequent – headache,rashes and dryness of
mouth Seizures at high dose
Interactions:– Disulfiram-like intolerance with alcohol.
11
METRONIDAZOLE - USES
1. Ameobiasis – Kills E. histolytic trophozoites but not cysts. Treatment of all tissue infections with E histolytic. No effects against luminal parasites and so must be used with a luminal amebicide – for eradication
2. Giardiasis3. Anaerobic infections4. Pseudo-membranous enterocolitis5. Helicobacter pylori
12

OTHER NITROIMIDAZOLES
• Tinidazole:– Slower metabolism, duration of action longer (t1/2
12 hrs) – single dose– Higher cure rates – Better tolerated – lesser incidence of side effects
• Secnidazole: Rapid absorption, but slower metabolism – half life 17-29 hrs
• Ornidazole: 12 -24 hr
• Satranidazole: 14 hrs half life – better tolerated plus no nausea, vomiting and metallic taste - no disulfiram like reaction and neurological symptoms
13

EMETINE Emetine, alkaloid derived from Cephaelis ipecacuanha
and dehydroemetine, a synthetic analog, are effective against tissue trophozoites of E histolytica
Effects on trophozoites but not on cysts. Potent and rapid action – symptomatic relief in 1-3
days, but not curative Administered subcutaneously (preferred) or i.m. NO
ORAL because oral preparations are absorbed erratically and vomiting
MOA inhibits protein synthesis……arrest intraribosomal translocation of t RNA-AA complex
Uses: Seldom used now. Reserve drug for severe intestinal and extraintestinal amoebiasis or for patients not responding to metronidazole. Luminal amoebicide needed to be added
14

EMETINE - ADRS Pain and tenderness in the area of injection Gastrointestinal tract discomfort Cardiac toxicity: arrhythmias, congestive
heart failure, hypotension, ECG changes.
15

CHLOROQUINE
Kills trophozoites of E. histolytica Concentrates in liver – used in liver
amoebiasis Completely absorbed from upper intestine
– not effective in invasive or luminal dysentery
Efficacy in amoebic liver is equal to emetine, but longer treatment and relapse
Used after a course of Metronidazole – but a luminal amoebicide must be added
Dose - 600mg stat and next day &300mg for 2-3 days
16
CHLOROQUINE MOA Chloroquine probably acts by
concentrating in parasitic food vacuoles, preventing the polymerization of the hemoglobin breakdown product, heme into hemozoin, and thus eliciting parasite toxicity due to buildup of free heme.
17

DILOXANIDE FUROATE (DF) Highly effective luminal amoebicide Chemistry Ester of diloxanide + furoic acid . Kills trophozoites responsible for production of cyst – however
no antibacterial action MOA
Oral DF
Furoic hydrolyzed and Diloxanide is freed
90% Diloxanide is absorbed
Remaining 10% reaches Large intestine
Kills the trophozoites Absorbed D – low serum level – no therapeutic effects
18
DILOXANIDE FUROATE – CONTD
ADRs: Well tolerated, only falatulence, nausea, itching and rarely urticaria
For eradication of infection given along with all forms of amebiasis.
19

NITAZOXANIDE
Salicylamide congener of Niclosamide Also effective in E. Histolytica, T. Vaginalis, H.
Pylori etc. Converted to Tizoxanide after absorption MOA: Inhibition of PFOR enzyme,an esential
pathway of electron transport energy metabolism
Uses: Giardiasis, aboebiasis as luminal amebicide,diarrhoea
Dose: 500 mg BD for 3 days20
8-HYDROXYQUINOLINES Drugs – Iodoquinol, Clioquinol and Iodochlorohydroxyquin Luminal amoebicidal but no tissue action Effective in chronic intestinal amebiasis (but lesser than
DF) Absorbed very less amount (10-30%) - therapeutic conc.
Is not attained conjugated and excreted in urine
Once a popular drug – but less now because of ADRs ADRs – well tolerated – only nausea, green stools pruritus
etc. plus Iodism But Subacute myelo-optic neuropathy (SMON) - the
inflammation of the optic nerve causing a complete or partial loss of vision and also peripheral neuropathy
Uses: Alternative to DF in amoebiasis, Giardia and fungal and bacterial infections. 250 to 500 mg tds
21

TETRACYCLINES
Luminal amoebicide Disturbs the symbiosis between normal
intestinal flora & E .histolytica -----------amoebae grow at expense of normal intestinal flora .
Tetracyclines are broad spectrum antibiotics & kill these flora leading to death of E .histolytica also.
Used in resistant and chronic cases.
22

Infected cell
increased expression of iron-containing superoxide dismutase (Fe-SOD) and
peroxiredoxin
Ferredoxin
RESISTANCE Increased Antioxident enzyme activity so less radicle formation
23

RECENT DRUGS
Paromycin Auranofin Pyrimidine Analouges Etophamide
24
PAROMOMYCIN Aminoglycoside antibiotic. Not significantly absorbed Less toxic Superior to Diloxanide furoate in clearing
asyptomatic infections. No effect on extra-intestinal amoebic
infections.MOA Direct amebicidal action (causes leakage by its action on
cell membrane of parasite). Indirect killing of bacterial flora essential for
proliferation of pathogenic amoebae. S/E: Abdominal Distress & diarrhea.
25

AURANOFIN A gold-containing drug approved arthritis
drug In Phase IIa Identification by High-Throughput Screen
(HTS) Less Costly Effective against amoebas in lab and animal
studies Orphan Drug Status Ten times more potent than the current
treatment 26
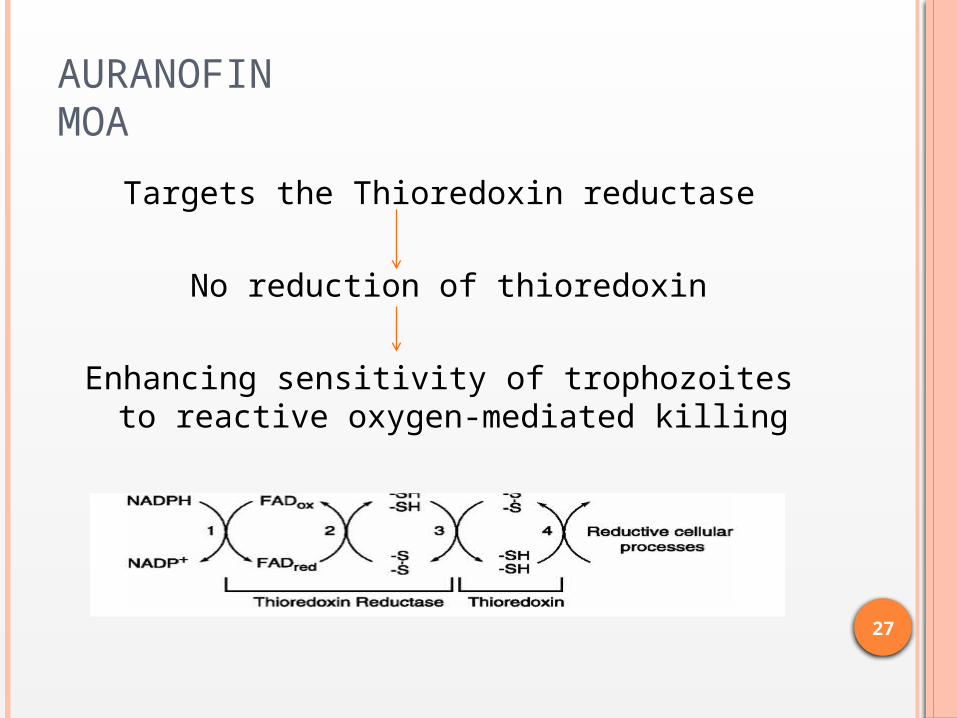
AURANOFIN MOA
Targets the Thioredoxin reductase
No reduction of thioredoxin
Enhancing sensitivity of trophozoites to reactive oxygen-mediated killing
27

Etophamide
Dose of 1 g per day, for three consecutive days
Tolerance of a new antiamebic drug was excellent
Cure rate obtained 92% Used for treatment of chronic intestinal
amebiasis. MOA is Unkown
28

PYRIMIDINE ANALOUGES Pyrazolo[3,4-d]pyrimidine analogues Active against HM1:IMSS strain of Entamoeba
histolytica Comparable to MTZ Low Side effect
30
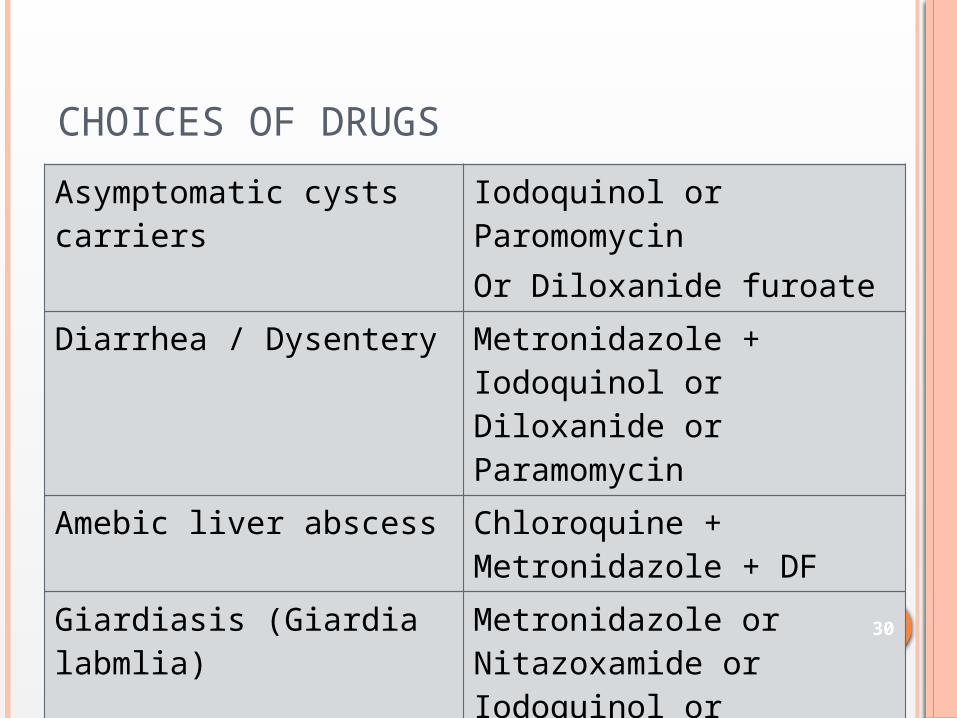
CHOICES OF DRUGS
Asymptomatic cysts carriers
Iodoquinol or ParomomycinOr Diloxanide furoate
Diarrhea / Dysentery Metronidazole + Iodoquinol or Diloxanide or Paramomycin
Amebic liver abscess Chloroquine + Metronidazole + DF
Giardiasis (Giardia labmlia)
Metronidazole or Nitazoxamide or Iodoquinol or Furazolidone 30

THANK YOU