ANTEPARTUM FETAL HEART RATE MONITORING IN MULTIPLE PREGNANCY
4
British Journalof Obstetrics and Gynaecology July 1980. Vol. 87. pp 561-564 ANTEPARTUM FETAL HEART RATE MONITORING IN MULTIPLE PREGNANCY BY DOROTHY BAILEY, Senior Research Technician ANNA M. FLYNN, Senior Research Fellow J. KELLY, Consultant Obstetrician AND MARIA O’CONOR, Research Midwife Department of Obstetrics and Gynaecology, Birmingham Maternity Hospital Queen Elizabeth Medical Centre, Edgbaston, Birmingham B15 2TG Summary The assessment of fetal wellbeing in patients with multiple pregnancy by non- stressed antepartum cardiotocography is technically feasible and of clinical value. In 50 patients (101 babies) who were monitored during the antepartum period, there were five patients in whom one of a pair of twins showed a non-reactive cardioto- gram. Four of these babies died (two intrauterine deaths and two neonatal deaths). All of these five babies were growth retarded at birth. The cardiotocograms from the other 96 fetuses were ‘reactive’ and these babies were normal. Cardiotocography seems to be a better predictor of perinatal mortality and morbidity than serial urinary oestrogens or serial biparietal diameter measurements in multiple pregnancy. THE perinatal mortality in multiple pregnancy is five times that of the singleton pregnancy (Chamberlain et al, 1975). Antepartum fetal deaths and intrauterine growth retardation are more common (Butler and Alberman, 1969). The clinical assessment of fetal wellbeing and/or size of each fetus, particularly if only one fetus is affected by placental insufficiency or growth retardation, is more difficult because of the multiplicity of fetal parts. Biochemical placental function tests in multiple pregnancy present problems. The results of 201, 24-hour urinary oestriol estimations in 50 twin pregnancies were studied by Duff and Brown (1974) who found that the urinary oestriol values were not low before or after intrauterine death of one fetus, or in pregnancies with intrauterine growth retardation. Oestriol production by the normal twin masked the deteriorating oestriol production by the twin in jeopardy. Human placental lactogen levels in multiple pregnancies have shown no consistent results (Josimovitch et al, 1970; Zlatnik et al, 1979). There is some evidence that the maturation of the lung in individual fetuses may proceed at different rates, even in identical twins (Picker et al, 1977; Goldkrand et al, 1977). The techniques used in obtaining the specimen are difficult and not readily repeatable. Divers and Hempsell (1979) found that ultrasound measurement of fetal biparietal diameter (BPD) was of limited use in the clinical diagnosis of intrauterine growth retardation in twin gestations, there being a significant number of false positives and false negatives. Relative head and abdominal measurements may be 561
-
Upload
dorothy-bailey -
Category
Documents
-
view
215 -
download
3
Transcript of ANTEPARTUM FETAL HEART RATE MONITORING IN MULTIPLE PREGNANCY

British Journalof Obstetrics and Gynaecology July 1980. Vol. 87. pp 561-564
ANTEPARTUM FETAL HEART RATE MONITORING IN MULTIPLE PREGNANCY
BY
DOROTHY BAILEY, Senior Research Technician
ANNA M. FLYNN, Senior Research Fellow
J. KELLY, Consultant Obstetrician
AND
MARIA O’CONOR, Research Midwife Department of Obstetrics and Gynaecology, Birmingham Maternity Hospital
Queen Elizabeth Medical Centre, Edgbaston, Birmingham B15 2TG
Summary The assessment of fetal wellbeing in patients with multiple pregnancy by non- stressed antepartum cardiotocography is technically feasible and of clinical value. In 50 patients (101 babies) who were monitored during the antepartum period, there were five patients in whom one of a pair of twins showed a non-reactive cardioto- gram. Four of these babies died (two intrauterine deaths and two neonatal deaths). All of these five babies were growth retarded at birth. The cardiotocograms from the other 96 fetuses were ‘reactive’ and these babies were normal. Cardiotocography seems to be a better predictor of perinatal mortality and morbidity than serial urinary oestrogens or serial biparietal diameter measurements in multiple pregnancy.
THE perinatal mortality in multiple pregnancy is five times that of the singleton pregnancy (Chamberlain et al, 1975). Antepartum fetal deaths and intrauterine growth retardation are more common (Butler and Alberman, 1969). The clinical assessment of fetal wellbeing and/or size of each fetus, particularly if only one fetus is affected by placental insufficiency or growth retardation, is more difficult because of the multiplicity of fetal parts.
Biochemical placental function tests in multiple pregnancy present problems. The results of 201, 24-hour urinary oestriol estimations in 50 twin pregnancies were studied by Duff and Brown (1974) who found that the urinary oestriol values were not low before or after intrauterine death of one fetus, or in pregnancies with intrauterine growth retardation. Oestriol production by the
normal twin masked the deteriorating oestriol production by the twin in jeopardy.
Human placental lactogen levels in multiple pregnancies have shown no consistent results (Josimovitch et al, 1970; Zlatnik et al, 1979).
There is some evidence that the maturation of the lung in individual fetuses may proceed at different rates, even in identical twins (Picker et al, 1977; Goldkrand et al, 1977). The techniques used in obtaining the specimen are difficult and not readily repeatable.
Divers and Hempsell (1979) found that ultrasound measurement of fetal biparietal diameter (BPD) was of limited use in the clinical diagnosis of intrauterine growth retardation in twin gestations, there being a significant number of false positives and false negatives. Relative head and abdominal measurements may be
561

562 BAILEY, FLYNN, KELLY AND O’CONOR
useful if the attendant technical problems can be overcome.
We have previously shown the value of non- stressed antepartum cardiotocography in the assessment of fetal wellbeing in 301 patients (Flynn and Kelly, 1977), and more recently used antepartum cardiotocography in the man- agement of the fetus suspected of intrauterine growth retardation (Flynn et al, 1979). Here we report the results of non-stressed antepartum fetal heart rate monitoring in patients with multiple pregnancy.
METHODS From 1st February, 1977 until 30th March,
1979, 50 patients with multiple pregnancy (49 with twins and one with triplets) were referred for antepartum cardiotocography. ‘At risk’ factors other than multiple pregnancy were present in 34 patients.
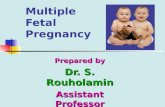
The position of the patient and the technique of antepartum cardiotocography were similar to those in patients with a singleton pregnancy (Flynn and Kelly, 1977), but two monitoring machines and two operators were required (Fig. 1). It was often necessary to hold the fetal heart sensor for each fetus on the maternal abdomen by hand, as well as using Tubigrip. When the fetus moved it was more common to
lose the signal in multiple pregnancy, than in a singleton pregnancy. When using ultrasono- graphy, the interference with the signal from each fetus could be avoided by changing the direction of the fetal heart sensor beam as the fetus moved.
The fetal heart monitors used were the Roche 540 or the Hewlett Packard 80/30. On some occasions two machines of the same kind were used, and sometimes one of each was used. As the mother could find it difficult to detect which fetus moved, the use of headphones by each operator in the Roche 540 helped to distinguish which fetus had moved and also the fetal heart rate response to that movement.
Ultrasonography was the method used to pick up the fetal heart signal.
The cardiotocograms were obtained at weekly intervals (apart from defaulters), and more frequently when requested by the clinician. The mean gestation at which recording commenced was 32 weeks, with a range of 29 to 35 weeks. The number of antepartum cardiotograms recorded on a patient varied from one to 27, with a mean of 4.7. In seven patients the cardiotocograms were obtained sequentially, rather than simultaneously, because of the poor quality of the simultaneous recording. There was only one patient on whom satisfactory
FIG. 1 Antepartum cardiotocography in multiple pregnancy. Two operators are observing (visually and by auscultation) fetal movements and the fetal heart response to such movements. The pressure and fetal heart transducers are held in place on the maternal abdomen by means of Tubigrip. The fetal heart transducer of the twin on the patient’s left
is also being held by hand, so that the direction can be altered when the baby moves.

MONITORING IN MULTIPLE PREGNANCY 563
simultaneous cardiotocograms could not be obtained at any time.
Twenty-four hour total urinary oestrogens were measured by the method of Simpkins and Worth (1975) in 37 patients.
Serial biparietal diameter (BPD) measure- ments were made in 44 patients.
RESULTS There were five patients in whom one of a
pair of twins showed a ‘non-reactive’ cardiotoco- gram. The cardiotocograms from the other 96 fetuses were ‘reactive’ and these babies are alive and well. Of the five fetuses with ‘non-reactive’ cardiotocograms, four died (two intrauterine deaths and two neonatal deaths). All five were growth retarded at birth (Table I). The intervals from the last cardiotocogram to intrauterine death or delivery in these five patients were two days in two patients (see Fig. 2), one day in one patient, and four hours in one patient. One patient defaulted and the interval between the last cardiotocogram and delivery was 24 days.
Of the 96 fetus with ‘reactive’ cardiotoco- grams, the mean Apgar score at one minute was
7.7 (range 6 to lo), and at five minutes the mean score was 9 - 3 (range 7 to 10). Twenty six of these babies were below the 10th centile of weight for gestation for singletons (Gairdner and Pearson, 1971).
The urinary oestrogens were measured in 37 patients and were within the normal limits for singleton pregnancies at our hospital.
Serial BPD measurements were in the normal range for singleton pregnancies in 43 of the 44 patients where such measurements were made. In one patient (Patient 1, Table I) the BPD was normal on three occasions and below the fifth centile on two occasions.
DISCUSSION The technical difficulties of antepartum cardio-
tocography in multiple pregnancy can be over- come by the methods we have described. When one fetus is positioned behind the other, it is usually more difficult to obtain a satisfactory recording than when both fetuses are side by side. In certain patients, it may only be possible to perform tests sequentially after identifying each fetal heart; there were seven such patients
TABLE I Urinary oestrogens, fetal biparietal diameter measurements and fetal heart abnormalities in the five pregnancies showing a
‘non-reactive ’ cardiotocogram
Fetal heart rate abnormality in the affected twin Outcome
Serial urinary Loss of Absence of
Patient oestrogens Serial biparietal diameters variability accelerations Decelerations Twin 1 Twin 2
SB IUGR IUGR
d (late)
1 Normal Both normal on 3 occasions d d Both below 5th centile on
2 occasions
- 2 Normal Bothnormal d d IUGR SB& IUGR
- 3 Normal Both normal d d Normal N N D & IUGR
4 Normal Not measured d N N D & Normal IUGR
d (late)
d
5 Normal Bothnormal d - d Normal IUGR (a single variable)
IUGR = Intrauterine growth retardation SB = Stillbirth NND = Neonataldeath

564 BAILEY, FLY", KELLY AND O'CONOR
I I I I. Q
sao I " iol I.
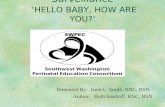
."....,"-. L. _ _ " . FIG. 2
Cardiotocograms in a multiple pregnancy Twin 2 died. The upper recording is from the fetal heart of normal Twin 1, and shows fetal heart accelerations due to fetal movements (marked by crosses). The middle recording is from the fetal heart of Twin 2, which died within 48 hours of this being made. There are repetitive late decelerations and loss of 'baseline variability'. The lower recording is of uterine action and shows Braxton-Hicks
contractions.
in our study. It is particularly important in twin pregnancy to avoid the supine position.
In multiple pregnancy, one fetus might show an abnormal cardiotocogram, the other one being normal. The decision about the timing of delivery requires then careful clinical judgement. To us it would seem wise that if both babies are mature and the one cardiotocogram shows repetitive late decelerations, delivery should be effected within 12 hours. Where the cardiotoco- gram of one fetus is 'non-reactive' but shows no late decelerations, pregnancy may be allowed to continue provided that there are no adverse
clinical features and frequently repeated cardio- tocograms show no deterioration.
As with other special tests, any correctable cause for an abnormal cardiotocogram, such as maternal treatment with sedatives reducing the number of fetal movements should be sought. A major fetal abnormality should also be considered.
In conclusion, it would seem that non-stress cardiotocography in the assessment of fetal wellbeing in patients with multiple pregnancy is feasible and of clinical value. It is a better predictor of perinatal mortality and morbidity than serial urinary oestrogens or serial biparietal diameter measurements in multiple pregnancy.
REFERENCES Butler, N. R., and Alberman, E. D. (1969): Perinatal
Problems. Livingston, E. S . , London, 12840. Chamberlain, R., Chamberlain, G., Howlett, B., and
Claireaux, A. (1975): British Births, 1970, Vol. 1, Heinmann Medical Books Ltd., London.
Divers, W. A., and Hempsell, D. L. (1979): The use of ultrasound in multiple gestations. Obstet Gynecol, 53 ,50W.
Duff, G. B., and Brown, J. B. (1974): Urinary oestriol excretion in twin pregnancies. J Obstet Gynaecol Br Commonw, 81,695-700.
Flynn, A. M., and Kelly, J. (1977): Evaluation of fetal wellbeing by antepartum fetal heart monitoring. Br MedJ, 1,936-9.
Flynn, A. M., Kelly, J., and O'Conor, M. (1979): Unstressed antepartum cardiotocography in the management of the fetus suspected of growth retardation. Br J Obstet Gynaecol, 86,10610.
Gairdner, D., and Pearson, J . (1971): A growth chart for premature and other infants. Arch Dis Child, 46,
Goldkrand, J. W., Varki, A., and McClurg, J. E. (1977): Surface tension of amniotic fluid lipid extracts: prediction of pulmonary maturity. Am J Obstet Gynecol, 128,591-8.
Josimovitch, J. B., Kosor, B., Boccella, L., Mintz, D. H., and Hutchinson, D. L. (1970): Placental lactogen in maternal serum as an index of fetal health. Obstet Gynecol, 36,244-50.
Picker, R. H., Smith, D. H., and Saunders, D. M. (1977): A new method of amniocentesis using ultrasound in multiple pregnancy to assess the second twin. Obstet Gynecol, SO, 489-94.
Simpkins, A., and Worth, H. G. J. (1975): An investi- gations into the automated measurement of urinary oestrogens in pregnancy. Ann Clin Biochem, 12, 233-43.
Zlatnik, F. J., Varner, M. W., and Hauser, K. S. (1979): Human placental lactogen: a predictor of perinatal outcome? Obstet Gynecol, 54,205-10.
783-7.