Chomba: Antenatal Corticosteroids for Threatened Preterm Delivery

Antenatal Steroids and Late Preterm Birth
T. Flint Porter, MDMaternal-Fetal MedicineIntermountain Healthcare
University of Utah Health Sciences
Disclosures• I have no relevant financial relationships to disclose or conflicts of
interest to resolve.
• I will not discuss any unapproved or off label, experimental or investigational use of a product, drug, or device.
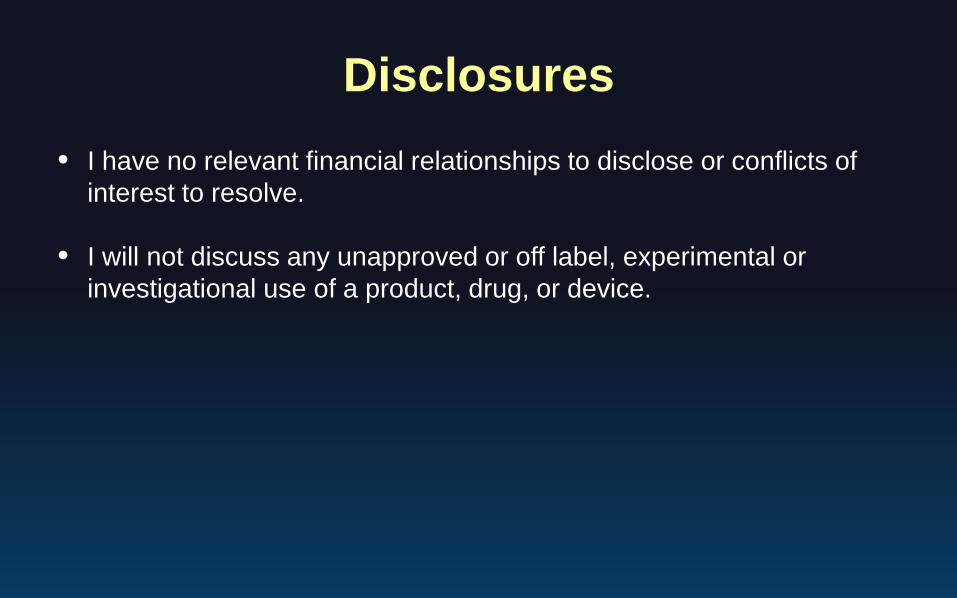
Antenatal Corticosteroids1972-1995
1972• Liggins & Howie, Pediatrics
⎯ < 32 weeks’⎯ RDS from 69.6 to 11.8%
• 14 RCT published• Steroid use 20-40%1973-1994
• Crowther, Meta-analysis, AJOG⎯ 50% reduction in RDS⎯ Best interval 24 hrs – 7 days
• Sinclair, Meta-analysis, AJOG⎯ NNTT prevent 1 RDS case⎯ < 31 weeks = 4⎯ 31-34 weeks = 15
1995

NIH Consensus StatementJAMA. 1995;273(5):413-418
• Antenatal corticosteroid therapy is indicated for women at risk of premature delivery with few exceptions and will result in a substantial decrease in neonatal morbidity and mortality, as well as substantial savings in health care costs.
• The use of antenatal corticosteroids for fetal maturation is a rare example of a technology that yields substantial cost savings in addition to improving health.

Antenatal Corticosteroids1995 - 2016
Steroid use increases to 70-90%!• 1996: 96% of US MFMs give more than one dose
− Protocols for steroids every week 24-34 weeks• 2001: NIH discourages repeat use
− IUGR, brain development, other long term effects• 2009: Single rescue course (Garite)
− < 34 weeks, > 14 days since last dose, delivery expected within 7 days
Antenatal CorticosteroidsOpening the GA Window
• 2011: Periviability− Expansion to 23 0/7 – 23 6/7 weeks− Reduction in death and neurodevelopmental
impairment at 18-20 months− Reduction in IVH, PVL, and NEC
• 2016: Late preterm birth (> 34 0/7 weeks)− 8% of all deliveries in late PTB period − Risks of PTB related morbidity low− Survival within 1% of survival at term

Neonatal M&M and Late PTBMcIntire, Obstet Gynecol. 111:35-41,
2008Neonatal death rates 34 to 40 weeks of gestation in singleton infants without malformations.
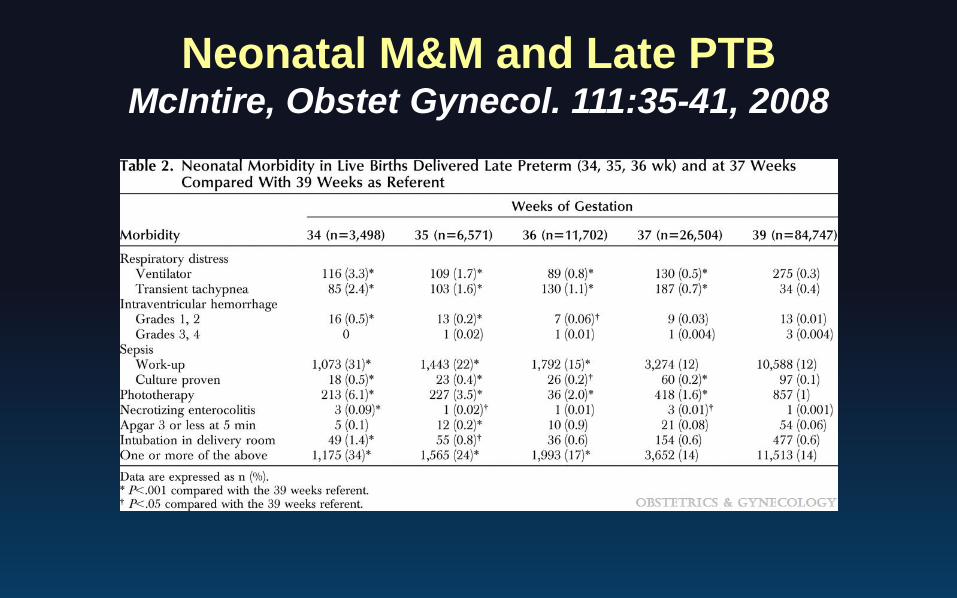
Neonatal M&M and Late PTBMcIntire, Obstet Gynecol. 111:35-41, 2008
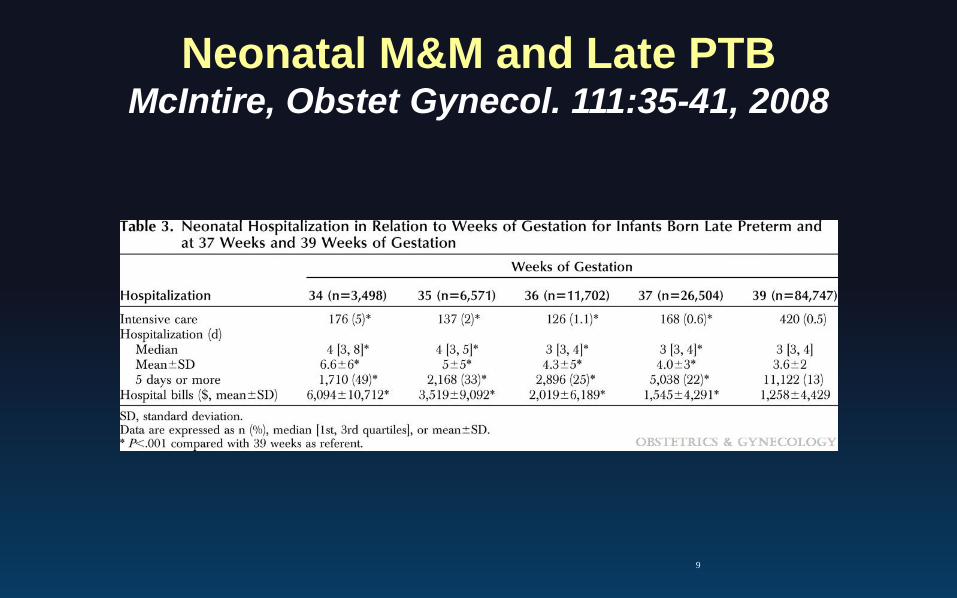
Neonatal M&M and Late PTBMcIntire, Obstet Gynecol. 111:35-41, 2008
9
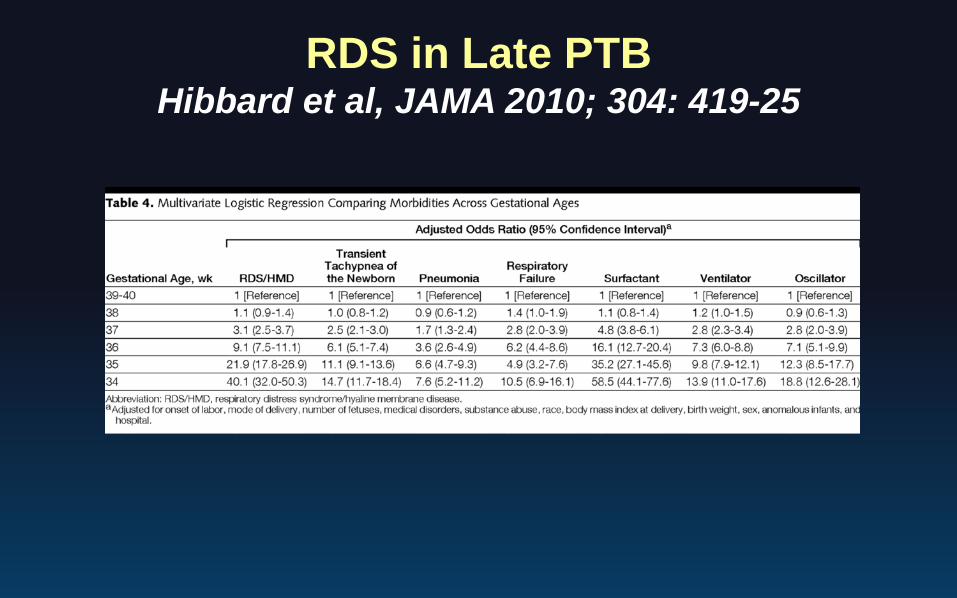
RDS in Late PTBHibbard et al, JAMA 2010; 304: 419-25

Original Article
Antenatal Betamethasone for Women at Risk for Late Preterm Delivery
Cynthia Gyamfi-Bannerman, M.D., Elizabeth A. Thom, Ph.D., Sean C. Blackwell, M.D., Alan T.N. Tita, M.D., Ph.D., Uma M. Reddy, M.D., M.P.H., George R. Saade, M.D., Dwight J. Rouse, M.D., David S. McKenna, M.D., Erin A.S. Clark, M.D., John M. Thorp, Jr., M.D., Edward K. Chien, M.D., Alan M. Peaceman, M.D., Ronald S. Gibbs, M.D., Geeta K. Swamy, M.D., Mary E. Norton, M.D., Brian M. Casey, M.D.,
Steve N. Caritis, M.D., Jorge E. Tolosa, M.D., M.S.C.E., Yoram Sorokin, M.D., J. Peter VanDorsten, M.D., Lucky Jain, M.D., for the NICHD Maternal–Fetal Medicine
Units Network
N Engl J MedVolume 374(14):1311-1320
April 7, 2016
Antenatal BMS for Late PTBGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320
• Singleton pregnancy 34 - 36 5/7 wks with high probability of delivery before 36 6/7 wks− Excluded if received BMS previously delivery expected
< 12 hours• Primary outcome: need for respiratory support
< 72 hours after birth• Other neonatal outcomes• Maternal morbidity
Antenatal BMS or Late PTBGyamfi-Bannerman C wholotta et al. N Engl J Med 2016;374
• MFMU, 17 centers− > 24,000 women screened
• 2831 women randomized− 1429 received BMS
• 860 – two doses• 568 – single dose• 2 lost to follow-up
− 1402 received placebo• 826 – two doses• 571 – single dose• 2 lost to follow-up

Antenatal BMS for Late PTBGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320
Indication for Delivery BMS (1429)
Placebo (1402)
PTL intact membranes 28% 28%PPROM 22.1% 21.7%GHTN or Pre 25.9% 27.5%IUGR 3.2% 3.4%Oligo 3.5% 3.0%Other 17.3% 16.5%

Antenatal BMS for Late PTBGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320
Other Characteristics (%) BMS (1429)
Placebo (1402)
< 34 wk 6 days 25.8 28.535 – 35 wk 6 days 40.0 37.9> 36 wks 34.2 33.6Nulliparous 32.0 32.0Preeclampsia or GHTN 30.3 31.4GDM 10.7 10.9Congenital Anomaly 0.8 1.5

Neonatal Respiratory OutcomesGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320

Other Neonatal OutcomesGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320
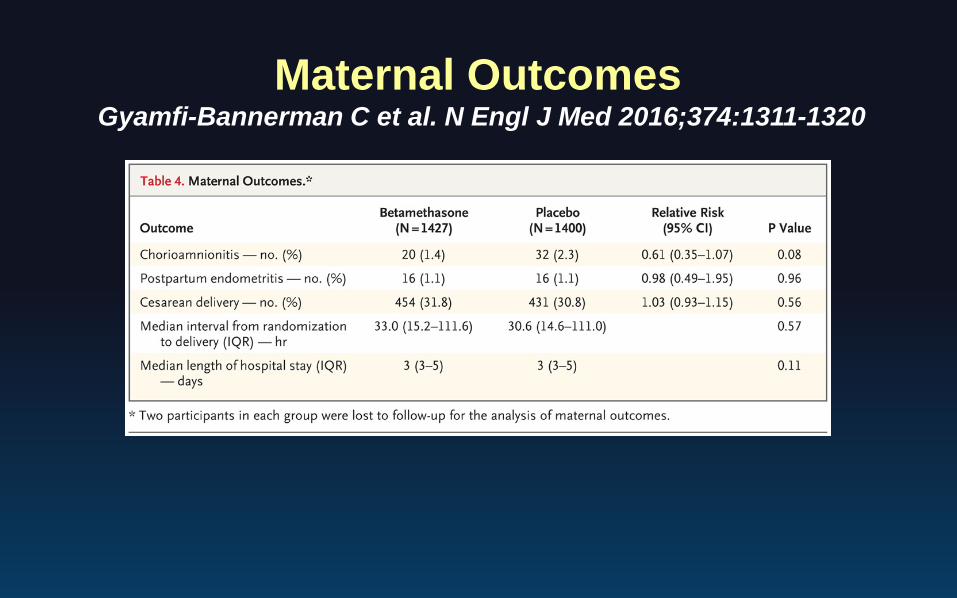
Maternal OutcomesGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320

Antenatal BMS for Late PTBGyamfi-Bannerman C et al. N Engl J Med 2016;374:1311-1320
• Administration of betamethasone to women at risk for late preterm delivery significantly reduced the rate of neonatal respiratory complications.
• Also resulted in decreased TTN, BPD, reduced rates of surfactant use, resuscitation, and prolonged hospital stay
• Betamethasone administration significantly increased the rate of neonatal hypoglycemia but no other maternal or neonatal complications

Antenatal Corticosteroid for FLMACOG, CO 677, Sep. 2016
• Single course 24 – 33 6/7 weeks− 23 weeks, delivery < 7 days, family decision
• Single course 34 – 36 6/7 weeks without prior steroids
• A single repeat course considered <34 weeks− Delivery considered imminent (< 7 days)− > 14 days since last dose− “Scheduled” repeated courses not recommended
• Repeated doses for patients with PPROM remains controversial

Mission Creep
Corticosteroids After Immature FLMShanks et al, AJOG 2010;203:47
• Hypothesis: antenatal glucocorticoids accelerate fetal lung maturity 34-37 weeks with known immature FLM
• Inclusion Criteria− singleton gestation− 34-36 6/7 weeks with− immature TDx-FLM-II test (<45 mg/g)
• Randomized to steroids or no treatment• Primary outcome: percent with TDx-FLM-II >45
mg/g after 1 week
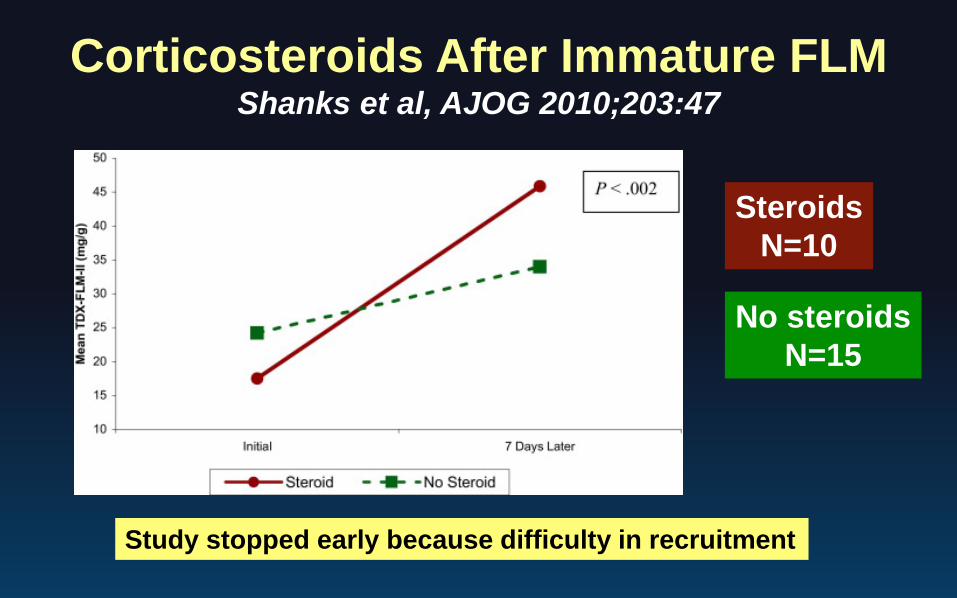
Corticosteroids After Immature FLMShanks et al, AJOG 2010;203:47
SteroidsN=10
No steroidsN=15
Study stopped early because difficulty in recruitment

Corticosteroids After Immature FLMKamath-Rayne et al, Obstet Gynecol 119:909-916
• Do steroids given after immature FLM at > 34 weeks improve neonatal outcomes
• Retrospective cohort study of neonates− 102 born after immature FLM and given steroids− 184 born after mature FLM− 76 born after immature FLM, expectant management
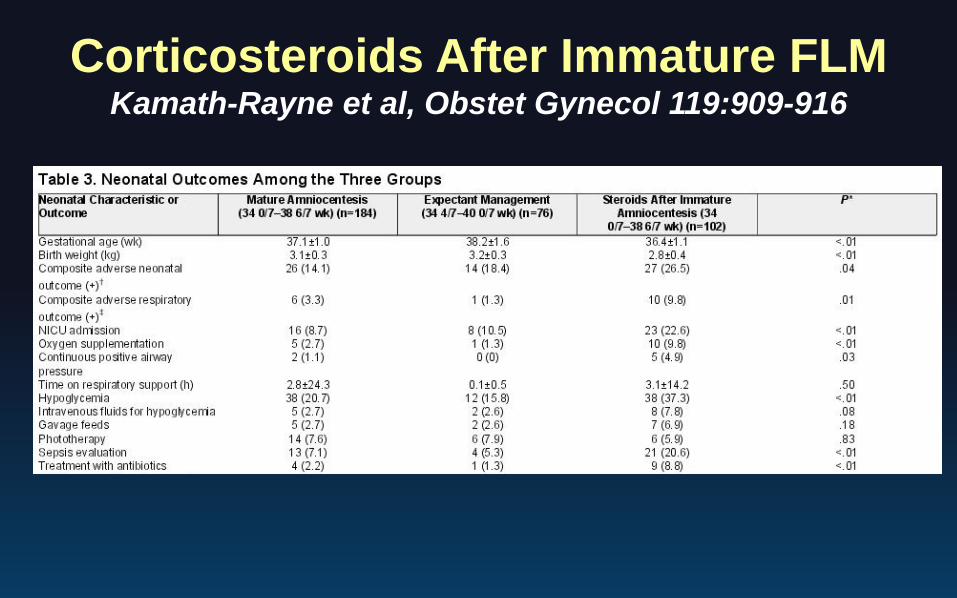
Corticosteroids After Immature FLMKamath-Rayne et al, Obstet Gynecol 119:909-916
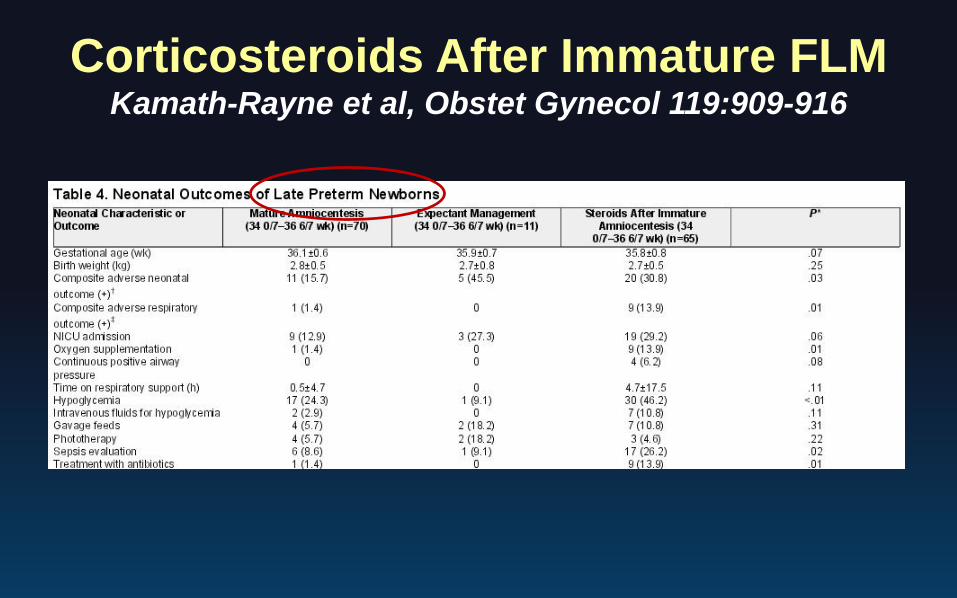
Corticosteroids After Immature FLMKamath-Rayne et al, Obstet Gynecol 119:909-916
Steroids Before Elective CS at TermStutchfield P et al, BMJ 2005;331:662
• ASTECS Trial: Antenatal Steroids for Term Elective Cesarean Section
• 998 women with planned elective CS < 37 wks• Primary outcome: admission to SCN for RDS• “Multicenter pragmatic randomized trial”
− Not blinded

Steroids Before Elective CS at TermStutchfield P et al, BMJ 2005;331:662
NICU (%) RDS (%) TTN (%)
Respiratory Morbidity
(%) Hypoglycemia
6.9 vs 7.1Not
Significant
0.2 vs 1.1RR = 0.21(0.03-1.32)
2.1 vs 4.0RR = 0.54; (0.26-1.12)
2.4 vs 5.1(RR = 0.46(0.23-0.93)
Not Reported
Steroids Before Elective CS at TermAhmed et al, J Mat Fet Neo Med 2015
• Non-blinded RCT• 2 doses of antenatal dexamethasone given at 37
wks before elective cesarean• RDS decreased in the treatment group
− (7.9%vs 23.2%; P< .01)− Most due to TTN

Steroids Before Elective CS at TermNada et al, Eur J Obstet Gynecol 2016
• Randomized, placebo controlled trial• 3 doses of dexamethasone 48 hours prior to
elective cesarean
NICU (%)RDS (%)
TTN (%)
Respiratory Morbidity (%) Hypoglycemia
3.1 vs 6.7P<.01
0.6 vs 1.6P<.01
1.3 vs 3.4P<.01
1.6 vs 3.9P<.01 Not Reported
Long Term Effects of Late Preterm Antenatal Corticosteroids
Worth the risk?• Poorly understood• Exposure to ACS shown to decrease stress
response in exposed preterm infants• Implications for Cardiovascular and mental
health implications

Continuing Challenges and Unintended Consequences
• Prediction of preterm birth− When do we give the corticosteroids
• Quality control measures− Are we giving them at the right time?− Are they given too often?
• Neonatal hypoglycemia− Does this risk outweigh benefit in some cases?− Trading one morbidity for another
• Delaying delivery unnecessarily