Antenatal Fetal Assessment 2013michigansonographerssociety.org/wp-content/uploads/2… · ·...
67
Antenatal Fetal Assessment The Old and the New 2017 1 Ivana M. Vettraino, M.D., M.B.A. Maternal Fetal Medicine Associate Professor, Michigan State University Here, There and Everywhere
-
Upload
nguyenmien -
Category
Documents
-
view
221 -
download
0
Transcript of Antenatal Fetal Assessment 2013michigansonographerssociety.org/wp-content/uploads/2… · ·...

Antenatal Fetal AssessmentThe Old and the New
2017
1
Ivana M. Vettraino, M.D., M.B.A.
Maternal Fetal Medicine
Associate Professor, Michigan State University
Here, There and Everywhere

Disclosures
O Speakers bureau
O March of Dimes
O Hologic, Inc
O Trainer
O Nexplanon
O I will not be discussing any of these organizations or products in this presentation
2

Objectives
O Define the role of antenatal fetal assessment
O List the methods of antenatal fetal assessment in common use
O Understand the application and interpretation of the various methods of fetal assessment
O State the limitations of the methods of assessment
O Review clinical indications and timing of the various methods
3

Introduction
O GoalO Identify fetuses at risk for intrauterine injury or death
to prevent these adverse outcomes
O Recognize the fetus that will benefit from early intervention/delivery without preterm delivery of the healthy fetus
O PremiseO Fetal hypoxia and acidosis is final common pathway to
fetal morbidity and mortality
O Fetus whose oxygenation in utero is challenged will respond with a series of detectable signs as hypoxemia progresses to metabolic acidemia 4

Example Indications
Maternal ConditionsPregnancy Related
Conditions
5
O Anti-phospholipid syndrome
O Chronic renal diseaseO Cyanotic heart diseaseO HemoglobinopathiesO Hypertensive disordersO HyperthyroidismO Systemic lupus
erythematosusO Type 1 diabetes mellitus
O Decreased fetal movementO Intrauterine growth restrictionO IsoimmunizationO Multiple gestation O OligohydramniosO PolyhydramniosO Post-term pregnancy
O 41 weeks’ gestation
O Pregnancy-induced hypertension
O Previous fetal demise

Introduction
O General limitations of tests of fetal surveillance
O In the 3rd trimester
O Fetuses spend 25% of time in a sleep state
O Increase the risk of non-reassuring fetal testing
O Which pregnancies should undergo antenatal fetal surveillance
O 30 to 50 percent of perinatal deaths occur in low risk pregnancies
O Acute catastrophic events such as abruptio placenta or cord accidents will not be detected
O Need to be able to identify fetal compromise in enough time to make a difference with an intervention 6

Introduction
O A combination of antenatal fetal assessment methods may be the optimal management strategy to balance the risks of false positive and false negative results
7
Common Methods of Antepartum Fetal Assessment
O Fetal movement assessment
O Nonstress test
O Biophysical profile
O Modified biophysical profile
O Contraction stress test
O Fetal vascular interrogation
O Umbilical artery
O Middle cerebral artery
O Ductus venosus
O Cerebral Placental Ratio (CBR)8

Fetal Movement Assessment
O Introduced by Sadovsky and Cardiff – 1970’s
O Fetal movement decreases in response to hypoxemia
O Maternal perception of decreased fetal movement may precede fetal death in some by several days
O Many methods for fetal “kick” counting
O No one method appears to be better/more predictive of a compromised fetus than another
O Initiated between 26 and 32 weeks’ gestation 9

10

Fetal Movement Assessment
O Common instructions
O Patient lies on her side to count fetal movement
O Count of 10 distinct fetal movements during a 2-hour period reassuring
O Count fetal movements for 1 hour 3 times per week
O Count is reassuring if it is at least equal to the previously established baseline count
O Review your individuals hospitals and/or office guidelines
11

Fetal Movement Assessment
O Results of studies for reduction of stillbirth are inconsistent
O Randomized trial - Denmark
O Associated with 73% reduction in avoidable stillbirths
O Results of studies difficult to compare due to differences in methods
O No specific fetal movement threshold as a limit for concern
O Maternal sense that fetal activity is reduced may be the most important factor
O Cochrane database review concluded
O Insufficient evidence to recommend routine fetal movement
counting to prevent stillbirth in high risk or low risk pregnancies12

Fetal Movement Assessment
O ACOG July 2014 – Antenatal Fetal Testing
O Should all women perform daily fetal movement assessment?
O Multiple studies have shown decreased fetal movement increases risk of adverse perinatal outcomes
O Effectiveness of fetal kick counting in preventing stillbirth uncertain
O Evidence that formal program of fetal movement assessment in low-risk women results in reduction in fetal deaths is lacking
O Whether fetal movement assessment adds benefit to a program of regular fetal surveillance unknown
O Does not appear to increase number of antepartum visits or interventions (RCT)
O Although not all women need to perform daily fetal movement assessment, if a decrease in fetal activity is noted further assessment should be performed 13

Nonstress Test (NST)
O Physiology
O For reactivity an intact central nervous system -cardiac loop must be present
O Brain modulates the heart rate
14

Nonstress Test (NST)
O PremiseO Fetal heart rate of non-compromised fetus will accelerate with fetal
movementO Described in the 1970’s
O Predictive valueO Low false negative rate
O 0.19 % to 1%O High false positive rate
O 55 % to 90 %O Absence of reactivity not necessarily pathologic
O Sleep cycleO Acidosis
O 15% of all NSTs will be nonreactiveO 25% will have a positive contraction stress test O Stillbirth rate (corrected) was 1.9 per 1000 live births
O Negative predictive value is 99.8% 15

Interpretation Guidelines
O Follow a systematic approach
O Baseline rate
O Baseline FHR variability
O Presence of accelerations
O Periodic or episodic decelerations
O Changes or trends of FHR patterns over time
O Frequency and intensity of uterine contractions

Interpretation Guidelines
O ReactiveO Two or more fetal heart rate accelerations within a 20-
minute period
O Non reactiveO Lack of sufficient fetal heart rate accelerations over a
40-minute period
O <32 weeks‘ gestationO >10 BPM above baseline for >10 seconds
O >32 weeks‘ gestationO >15 BPM above baseline for > 15 seconds

Biophysical Profile (BPP)
O Combines NST with fetal ultrasound assessment
O More time intensive than NST alone and requires training
O Predictive value
O Low false negative rate
O ~0.07 %
O High false positive rate
O Slightly lower than NST alone
18
The Biophysical Profile
19
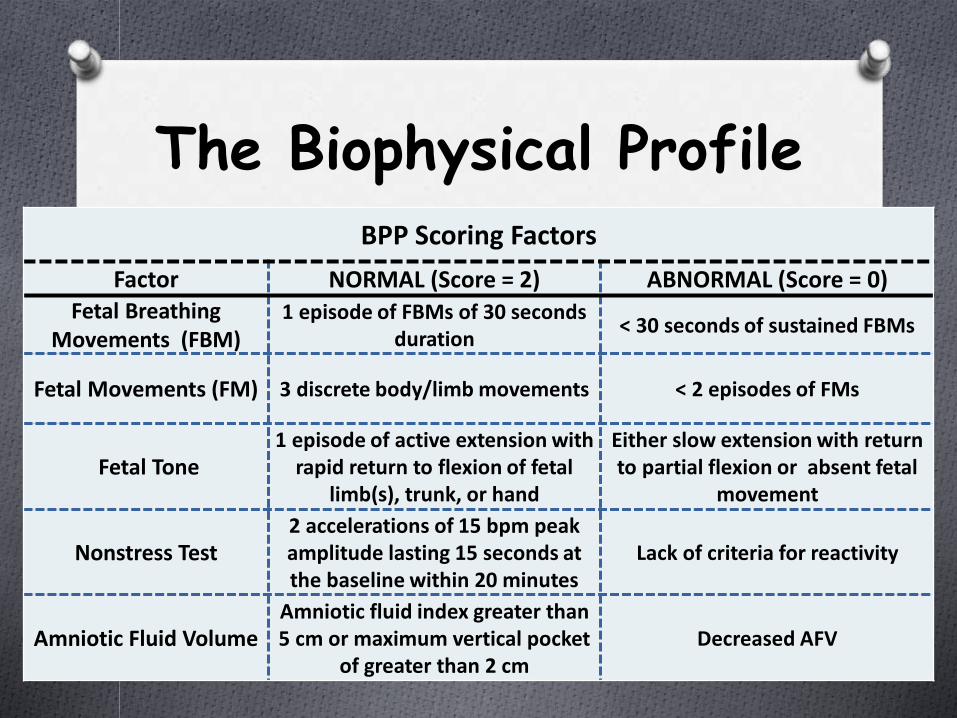
BPP Scoring Factors
Factor NORMAL (Score = 2) ABNORMAL (Score = 0)Fetal Breathing
Movements (FBM)1 episode of FBMs of 30 seconds
duration< 30 seconds of sustained FBMs
Fetal Movements (FM) 3 discrete body/limb movements < 2 episodes of FMs
Fetal Tone1 episode of active extension with
rapid return to flexion of fetal limb(s), trunk, or hand
Either slow extension with return to partial flexion or absent fetal
movement
Nonstress Test2 accelerations of 15 bpm peak amplitude lasting 15 seconds at the baseline within 20 minutes
Lack of criteria for reactivity
Amniotic Fluid VolumeAmniotic fluid index greater than 5 cm or maximum vertical pocket
of greater than 2 cmDecreased AFV

The Biophysical Profile
20
O Biophysical profile: 8-10 O Reassuring
O Follow-up as clinically indicated
O Biophysical Profile: 8O Reassuring
O Delivery considerations Oligohydramnios
O Biophysical Profile: 6 O Equivocal
O Repeat Biophysical Profile in 24 hours
O Biophysical Profile: 4O Non-reassuring
O Delivery considerations
O Gestational age >36 weeks
O Biophysical Profile: 0-2O Alarming
O Continue monitoring for max of 2 hours
O Calls for delivery
Oligohydramnios calls for further monitoring or delivery

Biophysical Profile
O Factors which may affect fetal parameters assessed
O Hypoxemia
O Acidosis
O Gestational age
O Maternal betamethasone administration
O Magnesium sulfate
O Excessive transducer pressure on the maternal abdomen
O Others
21

The Biophysical Profile
O No randomized trials have been performed comparing BPP with no testing
O Additional studies needed to make any reasonable conclusions regarding benefits of the BPP in high risk pregnancies to reduce fetal morbidity and mortality
22

Modified Biophysical Profile
O NST and amniotic fluid volume assessment
O Combination of short-term marker of fetal acid base status with the chronic marker of amniotic fluid
O Amniotic fluid assessment
O AFI
O Sum of measurements of deepest cord free amniotic fluid pocket in each of the uterine quadrants
O Single deepest vertical pocket without fetal parts or umbilical cord
O NormalO NST reactive and amniotic fluid volume greater than 2 cm
in deepest vertical pocket
O Negative predictive value similar to full BPP 23

Modified Biophysical Profile
O Adequate data does not exist to recommend or not recommend the modified BPP
O Similar reassuring false-negative rate and potentially a lower false-positive rate than the nonstress test alone
O Limitations
O False-positive rate high
O 60% of those delivered because of an abnormal antepartum test had no evidence of fetal compromise
O Led to preterm delivery in 1.5% of those tested before term
24

Contraction Stress TestO Fetal heart rate response to uterine contractions
O Premise
O Compromised fetus will have transient worsening in oxygen status with uterine contraction due to lack of reserve resulting in late decelerations
O Common Method
O External monitoring of FHR and uterine activity
O Three contractions of 40 seconds duration or longer in a 10-minute period
O Spontaneous or induced contractions
O Interpreted according to presence or absence of late decelerations 25

Contraction Stress Test
O InterpretationO Negative
O No late or significant variable decelerations
O Positive
O Late decelerations following 50% or more of contractions
O Equivocal
O Intermittent late decelerations/significant variable decelerations
O FHR decelerations with contractions more frequent than every 2 minutes or lasting longer than 90 seconds
O Unsatisfactory
O Fewer than 3 contractions in 10 minutes or an uninterruptable tracing 26

Contraction Stress Test
O Predictive value
O Negative predictive value of greater than 99.9%
O Time consuming
O Usually requires intravenous infusion of oxytocin
O Contraindications limit use of the contraction stress test in many high-risk situations
O Few demonstrated benefits over other methods of fetal assessment
O Should not be used routinely 27

Doppler Assessment

Doppler
• Doppler transducer placed
on skin and aimed at an
angle, θ
• Blood vessel contains blood
flowing with velocity of u m/s
• Transducer emits ultrasound
waves of frequency, fo
• Echoes generated by
moving reflectors in blood
have frequency, fr
• V is the sound wave in the
fluid

Fetal Doppler Assessment
O Uses ultrasound to measure blood flow velocities in fetal vessels that reflect downstream vascular resistance by calculations in differences between the peak systolic and the end-diastolic velocity within blood vessels of interest in each fetal cardiac cycle
30

Doppler Assessment
O Fetal-placental circulation is evaluated in the umbilical arteryO Measured by
systolic/diastolic (S/D) ratio
O S/D indirectly measures impedance or resistance downstream within the placental vessels
O As placental resistance increases, diastolic flow decreases and the S/D ratio rises

Fetal Vascular Doppler
O Primarily reserved for evaluation of the fetus with suspected or known growth restriction
O Most vigorously studied method to assess fetal well-being
O Almost all fetal vessels have been studied
O Umbilical artery Doppler interrogation most useful
O Directly reflects status of fetoplacental circulation
O systolic/diastolic ratio
O resistance index
O pulsatility index 32

IUGR
O Sonographic estimated fetal weight below 10th percentile or abdominal circumference less than 5th
percentile for gestational age
O Monitoring the growth-restricted fetus
O Serial assessment of fetal biometry
O Amniotic fluid volume
O Antenatal surveillance
O BPP
O NST
O Doppler flow assessment of the umbilical artery
O Antenatal surveillance should not begin before a gestational age when delivery would be considered 33

34
Fetal Vascular Doppler
O Abnormal flow velocity waveforms
O Correlated histopathologically with small-artery obliteration in placental tertiary villi
O Fetal hypoxemia and academia
O Increases in perinatal morbidity and mortality
35

Umbilical Artery Doppler
O Waveforms obtained near placental cord insertion site show higher end-diastolic flow velocity than waveforms obtained near abdominal cord insertion
O Due to the distance from point of resistance
O To optimize reproducibility, SMFM suggests interrogating umbilical artery at abdominal cord insertion
O S/D ratio and PI should be obtained in the absence of fetal breathing
O Waveforms should appear uniform 36

Umbilical Artery Doppler
37OBserver Record Review System

Umbilical Artery Doppler
O Normal wave form
38

Umbilical Artery Doppler
O Elevated umbilical artery Doppler
39
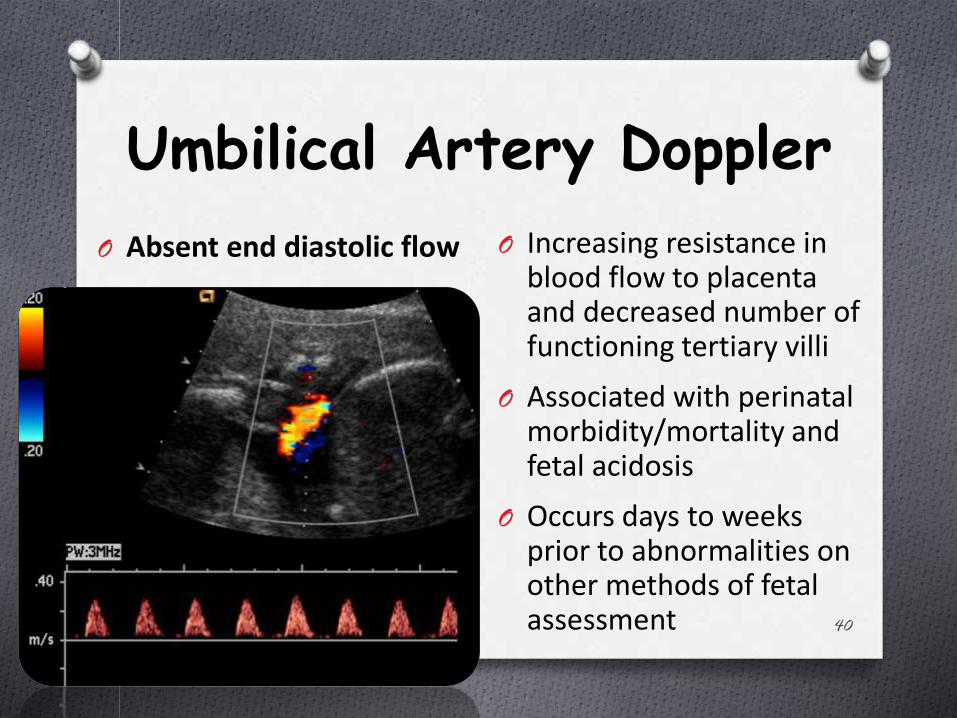
Umbilical Artery Doppler
40
O Absent end diastolic flow O Increasing resistance in blood flow to placenta and decreased number of functioning tertiary villi
O Associated with perinatal morbidity/mortality and fetal acidosis
O Occurs days to weeks prior to abnormalities on other methods of fetal assessment

Umbilical Artery Doppler
O Embolization experiments in the sheep placenta suggest that absent end-diastolic flow velocities are not achieved until more than 50% of functional villi have been obliterated
41

Umbilical Artery Doppler
42
O Reversed end diastolic flow
O Advanced stage of placental compromise
O Obliteration of 70% of arteries in placental tertiary villi
O Associated with severe IUGR (birth weight less than 3rd percentile) and oligohydramnios

Clinical Considerations
O Betamethasone administration in the growth-restricted fetus with abnormal umbilical artery Doppler studies
O Original trial showed increased risk of fetal deaths among women with hypertension and IUGR
O Due to transient increased physiologic and metabolic demands associated with administration of glucocorticoids
O Consider close observation for 48-72 hours following betamethasone administration
O Fetus with absent or reversed umbilical artery end-diastolic flow
O Betamethasone can result in transient return of end diastolic flow in about two thirds of the cases
O Due to altered tone of the placental vasculature43
Umbilical Artery Doppler
O Cochrane meta-analysis of randomized trials on use of umbilical artery Doppler in pregnancies with risk factors for adverse perinatal outcome demonstrates a clear reduction in perinatal mortality in normally formed fetuses
O This is the only form of fetal surveillance that has been shown to improve perinatal mortality in randomized controlled trials
44

Ductus Venosus
O Doppler waveforms from the fetal central venous circulation reflect the physiologic status of the right cardiac ventricle
O Continuous forward flow throughout the cardiac cycle is normal
O Decreased, absent, or reversed flow in the A wave (atrial contraction) can represent myocardial impairment (increased ventricular end-diastolic pressure)
O Associated with increased neonatal mortality rate in the fetus with growth restriction 45

Ductus Venosus

Ductus Venosus
O Normal wave form
47
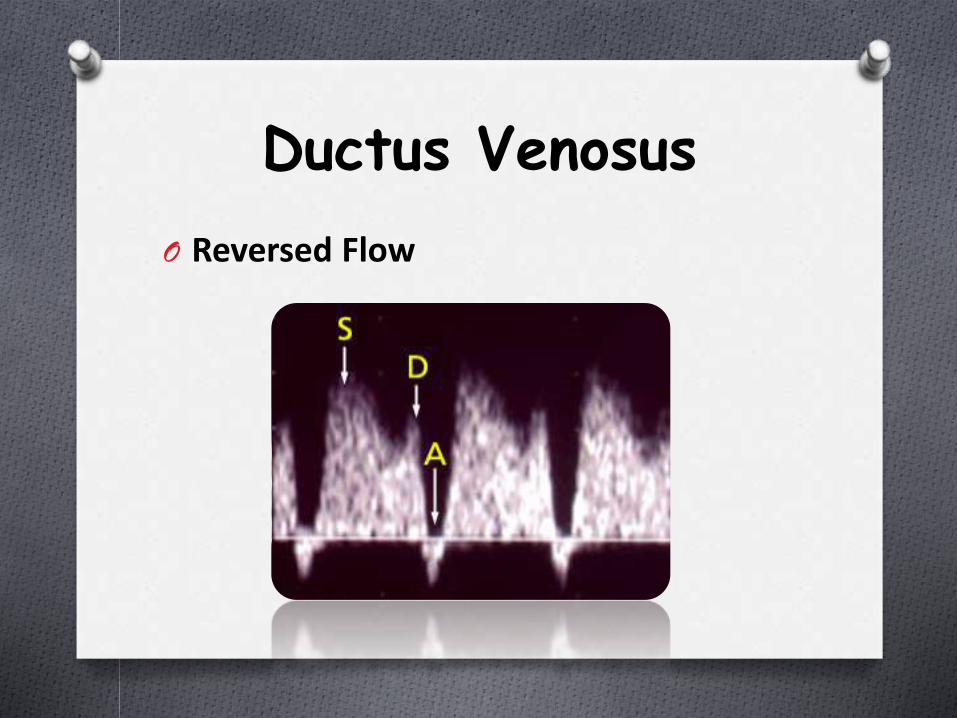
Ductus Venosus
O Reversed Flow

Fetal Vascular Changes in Hypoxemia
O Blood flow redistribution
O “Cerebral sparing” - MCA resistance indices fall as umbilical arterial resistance increases
O Does not correlate with final stages of asphyxia and not useful in choosing timing for delivery
O Increased resistance in umbilical arteries leads to increase in right ventricular (RV) end-diastolic pressure
O Deterioration of RV dilatation leads to tricuspid regurgitation
O Increased pulsatility in ductus venosus
O Highly correlated with impending asphyxia and acidosis
O Increased systemic venous pressures lead to dilatation of the ductus venosus and transmission of cardiac impulses to umbilical vein resulting in umbilical venous pulsations
O Highly correlated with severe acidosis and fetal demise 49

Progression of Abnormalities in Fetal Vessels
50
Ultrasound Obstet Gynecol 2002;19:140-146.
o = MCA PI
= UA AEDF
∆ = DV S/a
= UA RF
= DV RF

Outcomes
51
Ultrasound Obstet Gynecol 2002;19:140-146.

Middle Cerebral Artery Doppler
52

Fetal Middle Cerebral Arterial (MCA) Doppler
O Fetal cardiovascular distress
O Fetal anemia
O Fetal hypoxia
53

Fetal Middle Cerebral Arterial (MCA) Doppler
O Fetal head in the transverse plane
O Axial section of the brain, including the thalami and the sphenoid bone wings
O MCA vessels found with color or power Doppler overlying anterior wing of sphenoid bone near base of the skull
O Reading should be obtained close to origin of the circle of Willis
O Angle of insonation <15° should be used; typically
O Angle that approximates 0° is optimal54

Figure 1
American Journal of Obstetrics & Gynecology 2015 213, 5-15DOI: (10.1016/j.ajog.2015.05.024)
Copyright © 2015 Elsevier Inc. Terms and Conditions

Cerebroplacental Doppler Ratio (CPR)
O Ratio of middle cerebral artery pulsatility index (MCA-PI) to the umbilical artery pulsatility index (UA-PI)
O Increasing use as a predictor of adverse pregnancy outcome in fetuses with suspected fetal growth restrictions
O Increase risk of abnormal fetal heart tones in labor
O Higher rate of cesarean delivery for fetal distress in labor
O Higher rate of Apgar scores less than 7 at 5 minutes
O Increased rate of neonatal acidosis
O Increased rate of newborn intensive care unit admissions and adverse neonatal outcome
O Greater incidence of perinatal death
O Earlier predictor of adverse outcome than the biophysical profile, umbilical artery, or middle cerebral artery 56

CBR Normal Ranges
57

Figure 4
American Journal of Obstetrics & Gynecology 2015 213, 5-15DOI: (10.1016/j.ajog.2015.05.024)
Copyright © 2015 Elsevier Inc. Terms and Conditions

ACOG Practice Bulletin 134 Fetal Growth Restriction May 2013
O Absent or reversed end-diastolic flow in the umbilical artery associated with an increased risk of perinatal mortality
O Rate of perinatal death reduced by ~ 29% with umbilical artery Doppler added to standard antepartum testing for suspected fetal growth restriction
O Doppler assessment of other fetal blood vessels not shown to improve perinatal outcome and role of these measures in clinical practice remains unclear59

60

Initiation of Surveillance
O Depends upon combination of several factors
O Prognosis for neonatal survival
O Severity of maternal disease
O Risk of fetal death
O Risks of iatrogenic prematurity complications
O Initiating testing at 32-34 weeks of gestation is appropriate for most at-risk pregnancies
O Fetal surveillance can be initiated earlier if multiple or very concerning high-risk conditions exist 61

Management of Abnormal Surveillance
O Abnormal antepartum fetal test result should be interpreted in the context of the overall clinical picture
O Certain acute maternal conditions can result in abnormal test results that normalize as maternal condition improves
O Stepwise approach for assessment of the fetal condition should be undertaken
O Antepartum fetal surveillance tests have high false-positive rates and low positive predictive values
O Minimizes the potential for unnecessary delivery based on a single false-positive test result
O Response to abnormal test result should be tailored to the clinical situation 62

Management of Abnormal Surveillance
O The growth restricted fetus
O No definitive RCTs to guide timing of delivery
O Umbilical artery Doppler velocimetry considerations
O Absent end-diastolic flow
O Delivery considered at or beyond 34 0/7 weeks of gestation
O Reversed end-diastolic flow
O Delivery considered at or beyond 32 0/7 weeks of gestation
O Elevated cord Doppler with end diastolic flow
O Delivery considered at or beyond 37 0/7 weeks of gestation
O In the absence of obstetric contraindications, a trial of induction of labor with continuous monitoring okay 63

Management of Abnormal Surveillance
O Umbilical artery Doppler velocimetry in addition to NSTs or BPPs, or both, is associated with improved outcomes
O Unclear if evaluation of middle cerebral artery or venous system improves perinatal outcome
O Role of these measures in clinical practice remains uncertain
64

Clinical Considerations
O Results can be affected by maternal behaviorsO Tobacco, alcohol, methadone
O Decrease fetal movement, breathing, and heart rate reactivity
O CorticosteroidsO Decrease movement, breathing, and heart rate reactivity
O Maternal medical conditions - DKA, pulmonary compromiseO Non-reassuring fetal surveillance
O Delivery of the infant in this precarious setting is often ill advised and dangerous
O Stabilize maternal status – fetal status also improves 65

Final ThoughtsO No large clinical trials to guide frequency of antenatal
testing
O Literature on ideal use of antenatal testing and benefit in reducing fetal morbidity and mortality based on observational studies and expert opinion
O No one ideal test for every high risk pregnancy/ fetus(es)
O Predictive value of test relies on the suspected underlying pathophysiology
O Before choosing a test of fetal well being – necessary to have an idea of the underlying pathophysiology placing the fetus at risk
66

67