
Another case of congenital lobar emphysema fileCase Presentation •born term 40 weeks GA...
24
Another case of congenital lobar emphysema ?? Kamal Masarweh October 2018
Transcript of Another case of congenital lobar emphysema fileCase Presentation •born term 40 weeks GA...
Another case of congenital lobar
emphysema ??
Kamal MasarwehOctober 2018

Case Presentation
• born term 40 weeks GA
• spontaneous vaginal delivery
• birth weight – 3.57 kg, Apgar scores 9/10
• pregnancy:
• uneventful pregnancy
• normal antenatal ultrasound (13 and 26
weeks of gestation)
• firstborn to healthy non-consanguineous parents

• 15/2/2018
• 2 months old
• Presented in a northern hospital:
• 5 days URTI
• cough, dyspnea, cyanosis, restlessness
• afebrile
• ER: dyspneic, use of accessory muscles
• Vitals:
• tachypneic 70 BPM
• saturation 88% on room air, 98% +O2
• heart rate – 180 bpm, BP – 115/57
• Physical examination:
• moderate respiratory distress
• intercostal retractions
• decreased breath sounds on the left
• displaced heart sounds to the right side

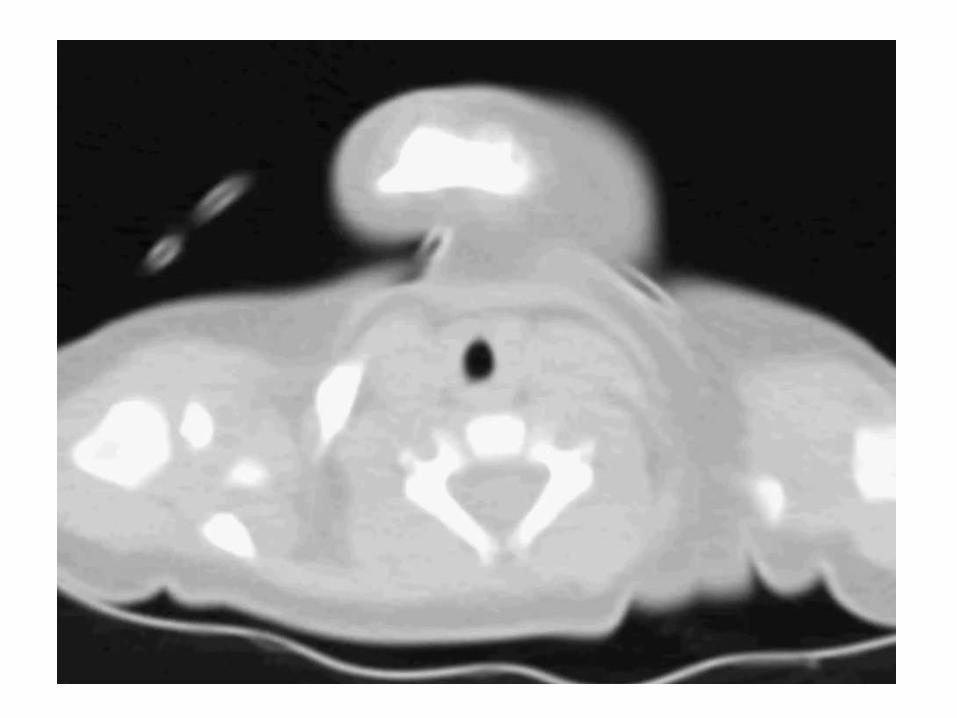


• Chest CT – hyperinflation on the left with septations, with a mediastinal shift to the right
• transferred to Rambam
• working diagnosis- CLE and significant respiratory compromise
• 16.2.2018 –
• left-sided thoracotomy
• lobectomy - left upper lobe
• uneventful surgery
• PICU
• extubated within one day
• analgesia and drainage
• post-operative pneumonia - antibiotics

Chest X-ray after surgery

• Is it congenital lobar emphysema??
typical age of presentation
typical location
typical herniation
× evidence of septations
× normal prenatal US (weeks 13 & 26) including revision after birth
Differential diagnosis
• Congenital Lobar Emphysema
• CPAM
• Pleuropulmonary Blastoma
• Bronchogenic cyst
• Others

• macroscopically - multiple septated cystic lesion measuring 9x6x2 cm
• microscopically - cystic lesions of various sizes, lined with a monolayer of endothelial cells
x40

X100
• Markers used in immunohistochemical staining for differentiating lymphatic lesions from other etiologies:
• D2-40- monoclonal antibody to podoplanin, highly reliable lymphatic endothelial marker. Stains the endothelium of lymphatic channels but not that of blood vessels
• CD31, CD34, ERG, factor VIII-related antigen – endothelial markers
• Minato H , Solitary intrapulmonary cystic lymphangioma in an infant: a case report with literature review. Pathol Res Pract. 2010 Dec 15;206(12):851-6

• Immunohistochemical staining - specific lymphatic vessel marker D2-40 -positive
x100

•Diagnosis:
Intrapulmonary macrocystic
lymphangioma
Pulmonary lymphatic system disorders
• rare lesions
• occur in a variety of non-neoplastic and neoplastic settings
• classification challenging
• inconsistent terminology
• mostly case reports and case series

Intrapulmonary Lymphangiomas
• extremely rare
• approximately 20 cases in literature
• patient ages – neonates (3 cases) to 54 yr
• frequently in the lower lobes of the lung, probably associated with a rich lymphatic supply
Clinical features
• symptoms vary widely depending on the age of the patient and the extent of disease
• neonates and infants - often present with pneumothorax and respiratory distress
• may remain asymptomatic until compression of vital structures
• may present as incidental findings on roentgenograms
Radiology
• Chest X-rays, US, CT scan, and MRI
• CT appearance - cystic mass with smooth margins
• no published data about antenatal US
• hypothesis that lymphangiomas become clinically significant in later stages of pregnancy or even after birth, possibly due to obstruction of lymphatic vessels

Intrapulmonary Lymphangiomas
• Treatment:
• surgical resection - frequently mandated both to confirm the diagnosis, and to prevent complications that arise from compressive effects on vital structures
• CT-guided Sclerosis
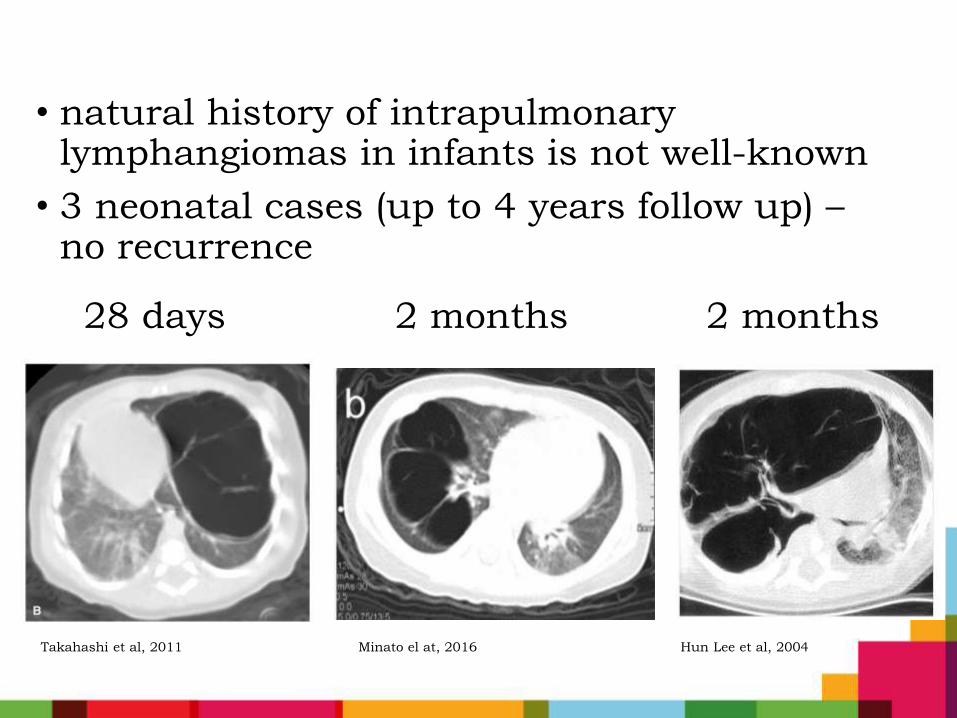
• natural history of intrapulmonary lymphangiomas in infants is not well-known
• 3 neonatal cases (up to 4 years follow up) –no recurrence
28 days 2 months 2 months
Takahashi et al, 2011 Minato el at, 2016 Hun Lee et al, 2004

Take home message
• Not all that looks like CLE is actually CLE
• Intrapulmonary lymphangioma mimics CLE and CPAM
• Does is it really matter to diagnose??
• is natural history of pulmonary lymphangiomas different than CLE/CPAM?
• is there a chance of recurrence?
• tendency for multiple lesions?
• is there a need for a different follow up?


















