ANNUAL SURVEILLANCE REPORT AND ANTIBIOTIC GUIDE · AND ANTIBIOTIC GUIDE ... program, allowing for...
26
ANNUAL SURVEILLANCE REPORT AND ANTIBIOTIC GUIDE Specialists | 2018
Transcript of ANNUAL SURVEILLANCE REPORT AND ANTIBIOTIC GUIDE · AND ANTIBIOTIC GUIDE ... program, allowing for...
ANNUAL SURVEILLANCE REPORT AND ANTIBIOTIC GUIDE
Specialists | 2018
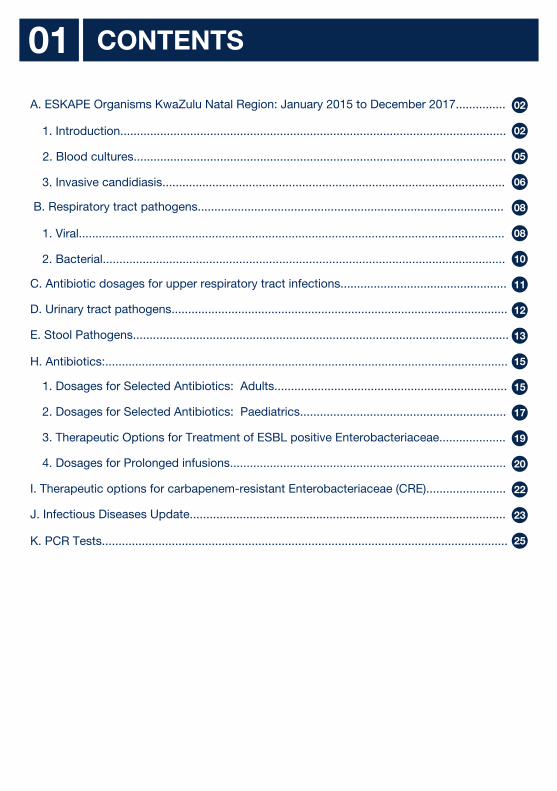
CONTENTS01
1. Introduction.................................................................................................................... 02
02A. ESKAPE Organisms KwaZulu Natal Region: January 2015 to December 2017...............
2. Blood cultures................................................................................................................ 05
3. Invasive candidiasis....................................................................................................... 06
08 B. Respiratory tract pathogens............................................................................................
1. Viral................................................................................................................................ 08
2. Bacterial......................................................................................................................... 10 C. Antibiotic dosages for upper respiratory tract infections.................................................. 11 D. Urinary tract pathogens..................................................................................................... 12
E. Stool Pathogens................................................................................................................. 13
H. Antibiotics:......................................................................................................................... 15
1. Dosages for Selected Antibiotics: Adults...................................................................... 15
2. Dosages for Selected Antibiotics: Paediatrics.............................................................. 17
3. Therapeutic Options for Treatment of ESBL positive Enterobacteriaceae.................... 19
4. Dosages for Prolonged infusions................................................................................... 20
I. Therapeutic options for carbapenem-resistant Enterobacteriaceae (CRE)........................ 22
J. Infectious Diseases Update............................................................................................... 23
K. PCR Tests.......................................................................................................................... 25
ESKAPE ORGANISMS KWAZULU NATAL REGION02
ESKAPE Organisms KwaZulu Natal Region: January 2015 to December 2017
IntroductionThe following microorganisms, forming the acronym ESKAPE CCC, have been listed among the most prioritized antimicrobial resistance threats, effectively escaping the currently available antimicrobial armamentarium: E: E nterococcus faecium (Vancomycin resistant) S: S taphylococcus aureus (Methicillin resistant) K: K lebsiella species A: A cinetobacter baumannii (Carbapenem resistant) P: P seudomonas aeruginosa (Carbapenem resistant) E: E nterobacter species C: C lostridium difficile C: C arbapenem resistant Enterobacteriaceae C: C andida species
Antimicrobial resistance (AMR) is a worldwide problem. New forms of AMR are crossing international boundaries and spreading between continents with ease and speed. World health leaders have described antibiotic resistant microorganisms as “nightmare bacteria” that “pose a catastrophic threat” to people in every country in the world. Antibiotic-resistant infections add considerable and avoidable costs to overburdened health care systems.
AMR estimates are an integral component of any antimicrobial stewardship program, allowing for informed appropriate selection of empiric therapy in an institute based on local epidemiology.
DEFINITIONS03
Extended spectrum beta lactamase producing (ESBL Positive) Extended spectrum beta-lactamases (ESBL) are enzymes that confer resistance to most beta-lactam antibiotics, including penicillins, cephalosporins, and the monobactam aztreonam. Carbapenems (meropenem, doripenem, imipenem and ertapenem) are the antimicrobial agents of choice for infections caused by such organisms.
Carbapenemase resistant Enterobacteriaceae (CRE) Carbapenem resistant Enterobacteriaceae (CRE) are Enterobacteriaceae that are resistant to the carbapenems. CRE are often resistant to multiple classes of antimicrobials substantially limiting treatment options. Infections caused by CRE are associated with high mortality rates. Many CRE possess carbapenemases (carbapenemase producing Enterobacteriaceae (CPE) which can be transmitted from one Enterobacteriaceae to another potentially facilitating transmission of resistance. Therapeutic options include combination therapy which can include colistin, tigecycline or any other antibiotic to which the organism is susceptible.
Clostridium difficile: Clostridium difficile (C. difficile) infections can cause illness ranging from diarrhoea to antibiotic-associated colitis, which can be fatal. Risk factors include recent medical care and antibiotics.
CRAc : carbapenem resistant acinetobacter
CRPs : carbapenem resistant pseudomonas
04
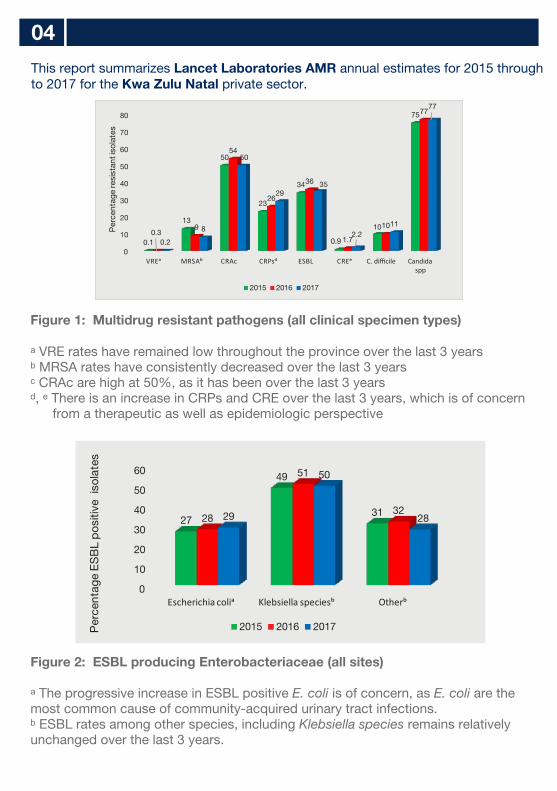
Figure 1: Multidrug resistant pathogens (all clinical specimen types)
ᵃ VRE rates have remained low throughout the province over the last 3 yearsᵇ MRSA rates have consistently decreased over the last 3 yearsᶜ CRAc are high at 50%, as it has been over the last 3 yearsᵈ, ᵉ There is an increase in CRPs and CRE over the last 3 years, which is of concern
from a therapeutic as well as epidemiologic perspective
Figure 2: ESBL producing Enterobacteriaceae (all sites)
ᵃ The progressive increase in ESBL positive E. coli is of concern, as E. coli are the most common cause of community-acquired urinary tract infections.ᵇ ESBL rates among other species, including Klebsiella species remains relatively unchanged over the last 3 years.
0
10
20
30
40
50
60
70
80
VREᵃ MRSAᵇ CRAc CRPsᵈ ESBL CREᵉ C. difficile Candidaspp
0.1
13
50
23
34
0.9
10
75
0.39
54
26
36
1.7
10
77
0.2
8
50
2935
2.211
77P
erce
ntag
e re
sist
ant i
sola
tes
2015 2016 2017
0
10
20
30
40
50
60
Escherichia coliᵃ Klebsiella speciesᵇ Otherᵇ
27
49
3128
51
3229
50
28
Per
cent
age
ES
BL
pos
itive
iso
late
s
2015 2016 2017
This report summarizes Lancet Laboratories AMR annual estimates for 2015 through to 2017 for the Kwa Zulu Natal private sector.
05
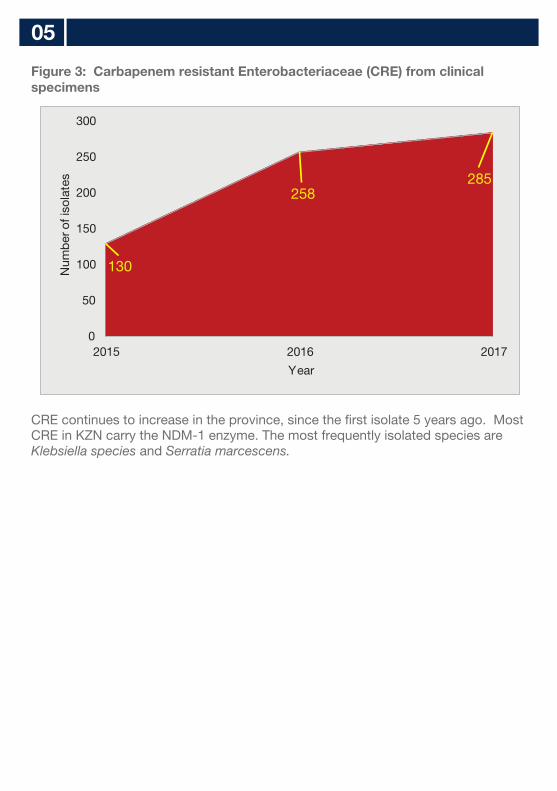
Figure 3: Carbapenem resistant Enterobacteriaceae (CRE) from clinical specimens
CRE continues to increase in the province, since the first isolate 5 years ago. Most CRE in KZN carry the NDM-1 enzyme. The most frequently isolated species are Klebsiella species and Serratia marcescens.
130
258285
0
50
100
150
200
250
300
2015 2016 2017
Num
ber o
f iso
late
s
Year
BLOOD CULTURES06
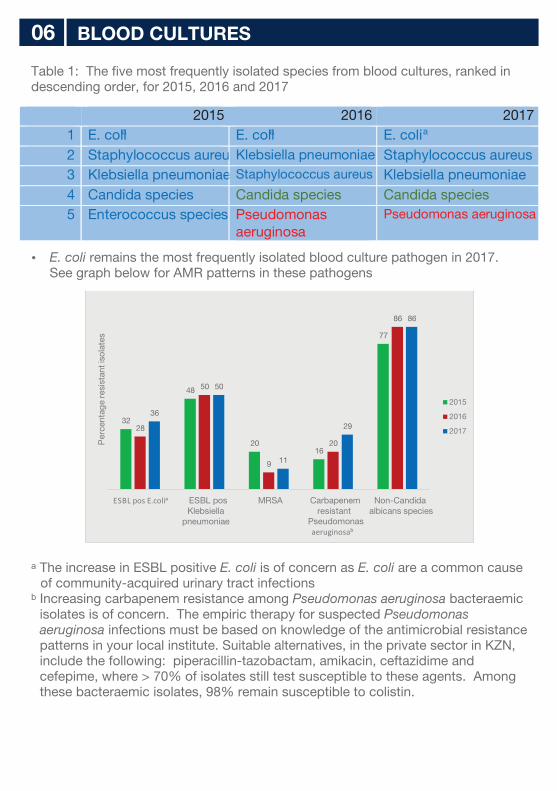
Table 1: The five most frequently isolated species from blood cultures, ranked in descending order, for 2015, 2016 and 2017
E. coli remains the most frequently isolated blood culture pathogen in 2017. See graph below for AMR patterns in these pathogens
ᵃ The increase in ESBL positive E. coli is of concern as E. coli are a common cause of community-acquired urinary tract infections
ᵇ Increasing carbapenem resistance among Pseudomonas aeruginosa bacteraemic isolates is of concern. The empiric therapy for suspected Pseudomonas aeruginosa infections must be based on knowledge of the antimicrobial resistance patterns in your local institute. Suitable alternatives, in the private sector in KZN, include the following: piperacillin-tazobactam, amikacin, ceftazidime and cefepime, where > 70% of isolates still test susceptible to these agents. Among these bacteraemic isolates, 98% remain susceptible to colistin.
2015 2016 20171 E. colia E. colia
E. colia
2 Staphylococcus aureus Klebsiella pneumoniae Staphylococcus aureus
3 Klebsiella pneumoniae Staphylococcus aureus Klebsiella pneumoniae
4 Candida species Candida species Candida species
5 Enterococcus species Pseudomonas aeruginosa
Pseudomonas aeruginosa
32
48
2016
77
28
50
9
20
86
36
50
11
29
86
ESBL pos E.coliᵃ ESBL posKlebsiella
pneumoniae
MRSA Carbapenem resistant
Pseudomonas aeruginosaᵇ
Non-Candidaalbicans species
Per
cent
age
resi
stan
t iso
late
s
2015
2016
2017
INVASIVE CANDIDIASIS07
0
10
20
30
40
50
60
Per
cent
age
2015
2016
2017
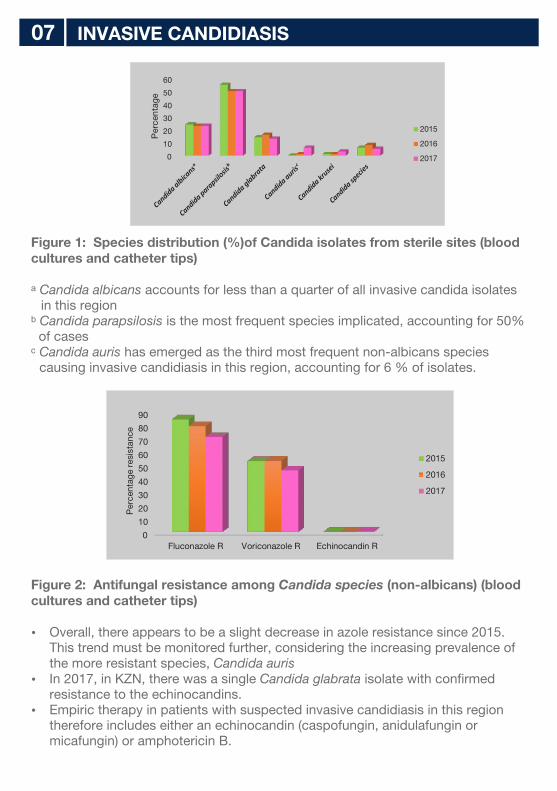
Figure 1: Species distribution (%)of Candida isolates from sterile sites (blood cultures and catheter tips)
ᵃ Candida albicans accounts for less than a quarter of all invasive candida isolates in this region
ᵇ Candida parapsilosis is the most frequent species implicated, accounting for 50% of cases
ᶜ Candida auris has emerged as the third most frequent non-albicans species causing invasive candidiasis in this region, accounting for 6 % of isolates.
Figure 2: Antifungal resistance among Candida species (non-albicans) (blood cultures and catheter tips)
Overall, there appears to be a slight decrease in azole resistance since 2015. This trend must be monitored further, considering the increasing prevalence of the more resistant species, Candida auris
In 2017, in KZN, there was a single Candida glabrata isolate with confirmed resistance to the echinocandins.
Empiric therapy in patients with suspected invasive candidiasis in this region therefore includes either an echinocandin (caspofungin, anidulafungin or micafungin) or amphotericin B.
0
10
20
30
40
50
60
70
80
90
Fluconazole R Voriconazole R Echinocandin R
Per
cent
age
resi
stan
ce
2015
2016
2017
CANDIDA AURIS08
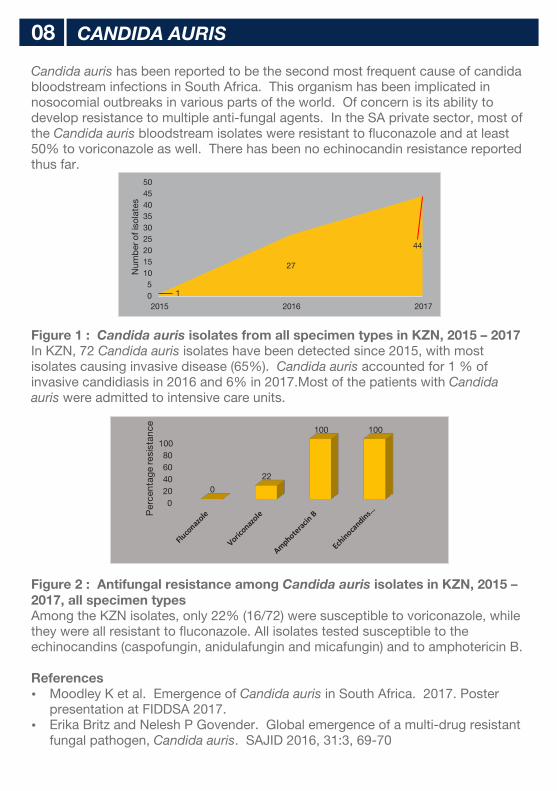
Candida auris has been reported to be the second most frequent cause of candida bloodstream infections in South Africa. This organism has been implicated in nosocomial outbreaks in various parts of the world. Of concern is its ability to develop resistance to multiple anti-fungal agents. In the SA private sector, most of the Candida auris bloodstream isolates were resistant to fluconazole and at least 50% to voriconazole as well. There has been no echinocandin resistance reported thus far.
Figure 1 : Candida auris isolates from all specimen types in KZN, 2015 – 2017In KZN, 72 Candida auris isolates have been detected since 2015, with most isolates causing invasive disease (65%). Candida auris accounted for 1 % of invasive candidiasis in 2016 and 6% in 2017.Most of the patients with Candida auris were admitted to intensive care units.
Figure 2 : Antifungal resistance among Candida auris isolates in KZN, 2015 – 2017, all specimen typesAmong the KZN isolates, only 22% (16/72) were susceptible to voriconazole, while they were all resistant to fluconazole. All isolates tested susceptible to the echinocandins (caspofungin, anidulafungin and micafungin) and to amphotericin B.
References Moodley K et al. Emergence of Candida auris in South Africa. 2017. Poster
presentation at FIDDSA 2017. Erika Britz and Nelesh P Govender. Global emergence of a multi-drug resistant
fungal pathogen, Candida auris. SAJID 2016, 31:3, 69-70
1
27
44
05
101520253035404550
2015 2016 2017
Num
ber
of i
sola
tes
020406080
100
0
22
100 100
Per
cent
age
resi
stan
ce
RESPIRATORY TRACT PATHOGENS 09
0100200300400500600700800900
895
614536
455405
363315
246201 192 172
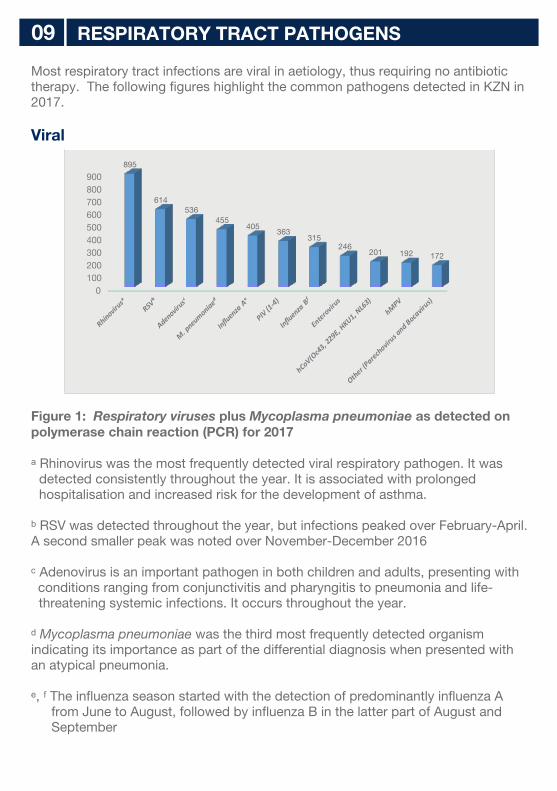
Most respiratory tract infections are viral in aetiology, thus requiring no antibiotic therapy. The following figures highlight the common pathogens detected in KZN in 2017.
Viral
Figure 1: Respiratory viruses plus Mycoplasma pneumoniae as detected on polymerase chain reaction (PCR) for 2017
ᵃ Rhinovirus was the most frequently detected viral respiratory pathogen. It was detected consistently throughout the year. It is associated with prolonged hospitalisation and increased risk for the development of asthma.
ᵇ RSV was detected throughout the year, but infections peaked over February-April. A second smaller peak was noted over November-December 2016
ᶜ Adenovirus is an important pathogen in both children and adults, presenting withconditions ranging from conjunctivitis and pharyngitis to pneumonia and life-threatening systemic infections. It occurs throughout the year.
ᵈ Mycoplasma pneumoniae was the third most frequently detected organism indicating its importance as part of the differential diagnosis when presented with an atypical pneumonia.
ᵉ, ᶠ The influenza season started with the detection of predominantly influenza A from June to August, followed by influenza B in the latter part of August and September
Bacterial
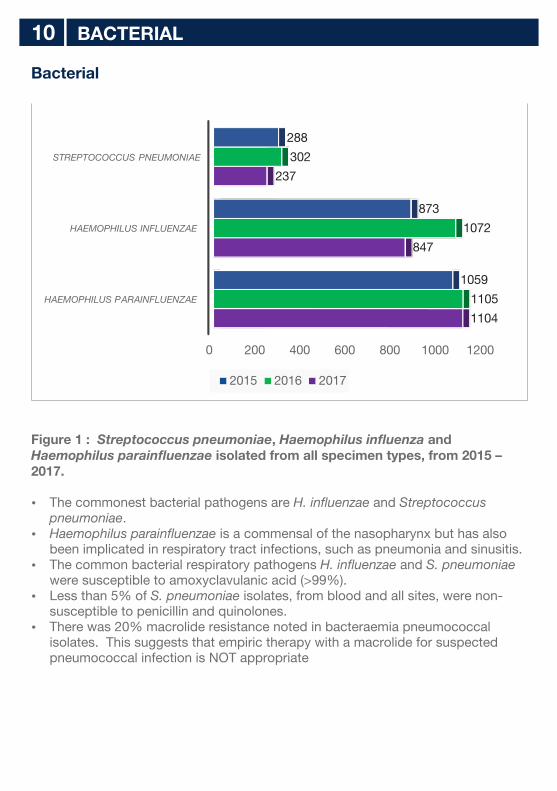
Figure 1 : Streptococcus pneumoniae, Haemophilus influenza and Haemophilus parainfluenzae isolated from all specimen types, from 2015 – 2017. The commonest bacterial pathogens are H. influenzae and Streptococcus
pneumoniae. Haemophilus parainfluenzae is a commensal of the nasopharynx but has also
been implicated in respiratory tract infections, such as pneumonia and sinusitis. The common bacterial respiratory pathogens H. influenzae and S. pneumoniae
were susceptible to amoxyclavulanic acid (>99%). Less than 5% of S. pneumoniae isolates, from blood and all sites, were non-
susceptible to penicillin and quinolones. There was 20% macrolide resistance noted in bacteraemia pneumococcal
isolates. This suggests that empiric therapy with a macrolide for suspected pneumococcal infection is NOT appropriate
BACTERIAL10
0 200 400 600 800 1000 1200
1104
847
237
1105
1072
302
1059
873
288
2015 2016 2017
HAEMOPHILUS PARAINFLUENZAE
HAEMOPHILUS INFLUENZAE
STREPTOCOCCUS PNEUMONIAE
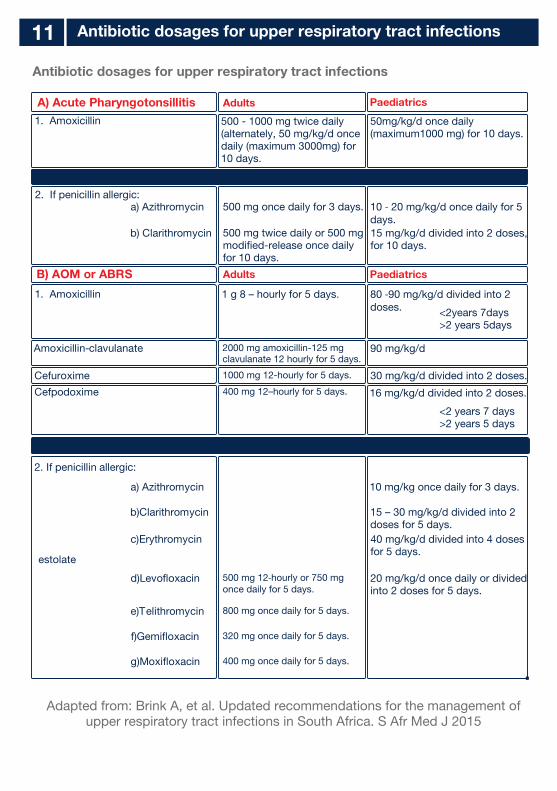
Antibiotic dosages for upper respiratory tract infections
Adapted from: Brink A, et al. Updated recommendations for the management of upper respiratory tract infections in South Africa. S Afr Med J 2015
Antibiotic dosages for upper respiratory tract infections11
A) Acute Pharyngotonsillitis
Adults
Paediatrics
1. Amoxicillin
1. Amoxicillin
2. If penicillin allergic:a) Azithromycin
b) Clarithromycin
500 mg once daily for 3 days.
B) AOM or ABRS Adults
Paediatrics
Amoxicillin-clavulanate
Cefuroxime
Cefpodoxime
2. If penicillin allergic:
a) Azithromycin
b)Clarithromycin
c)Erythromycin
estolate
d)Levofloxacin
e)Telithromycin
f)Gemifloxacin
g)Moxifloxacin
500 - 1000 mg twice daily(alternately, 50 mg/kg/d oncedaily (maximum 3000mg) for10 days.
50mg/kg/d once daily (maximum1000 mg) for 10 days.
10 ‐ 20 mg/kg/d once daily for 5days.15 mg/kg/d divided into 2 doses,for 10 days.
80 ‐90 mg/kg/d divided into 2doses.
16 mg/kg/d divided into 2 doses.
10 mg/kg once daily for 3 days.
15 – 30 mg/kg/d divided into 2doses for 5 days.40 mg/kg/d divided into 4 dosesfor 5 days.
20 mg/kg/d once daily or dividedinto 2 doses for 5 days.
90 mg/kg/d
30 mg/kg/d divided into 2 doses.
<2years 7days>2 years 5days
<2 years 7 days>2 years 5 days
500 mg twice daily or 500 mgmodified-release once daily for 10 days.
1 g 8 – hourly for 5 days.
2000 mg amoxicillin-125 mgclavulanate 12 hourly for 5 days.
1000 mg 12-hourly for 5 days.
400 mg 12–hourly for 5 days.
500 mg 12‐hourly or 750 mgonce daily for 5 days.
800 mg once daily for 5 days.
320 mg once daily for 5 days.
400 mg once daily for 5 days.
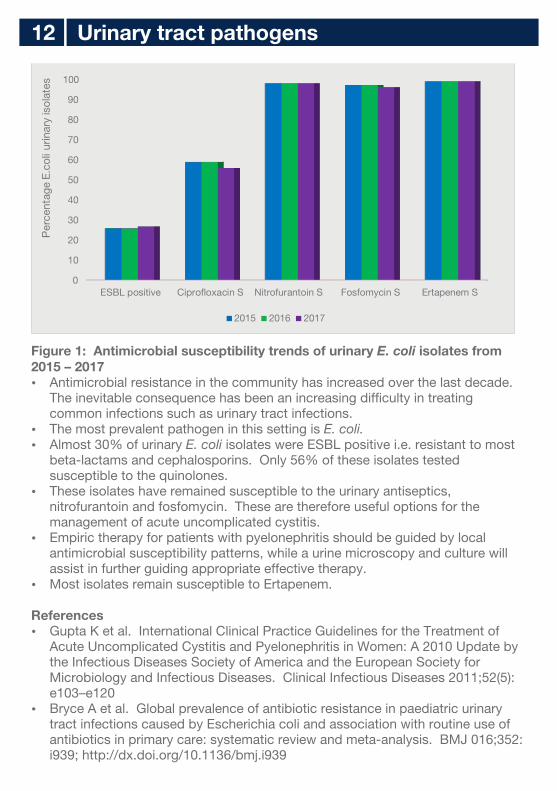
Figure 1: Antimicrobial susceptibility trends of urinary E. coli isolates from 2015 – 2017 Antimicrobial resistance in the community has increased over the last decade.
The inevitable consequence has been an increasing difficulty in treating common infections such as urinary tract infections.
The most prevalent pathogen in this setting is E. coli. Almost 30% of urinary E. coli isolates were ESBL positive i.e. resistant to most
beta-lactams and cephalosporins. Only 56% of these isolates tested susceptible to the quinolones.
These isolates have remained susceptible to the urinary antiseptics, nitrofurantoin and fosfomycin. These are therefore useful options for the management of acute uncomplicated cystitis.
Empiric therapy for patients with pyelonephritis should be guided by local antimicrobial susceptibility patterns, while a urine microscopy and culture will assist in further guiding appropriate effective therapy.
Most isolates remain susceptible to Ertapenem.
References Gupta K et al. International Clinical Practice Guidelines for the Treatment of
Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical Infectious Diseases 2011;52(5): e103–e120
Bryce A et al. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: systematic review and meta-analysis. BMJ 016;352: i939; http://dx.doi.org/10.1136/bmj.i939
Urinary tract pathogens12
0
10
20
30
40
50
60
70
80
90
100
ESBL positive Ciprofloxacin S Nitrofurantoin S Fosfomycin S Ertapenem S
Per
cent
age
E.co
li ur
inar
y is
olat
es
2015 2016 2017
Stool pathogens – KZN 201713
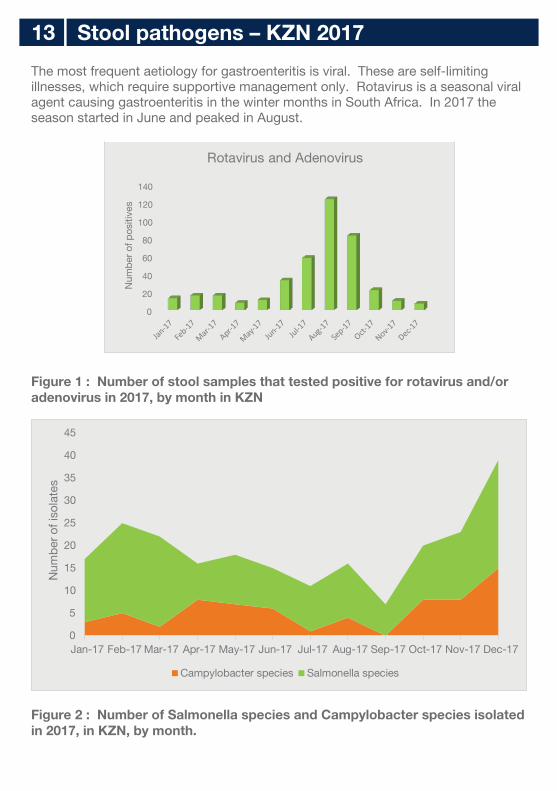
The most frequent aetiology for gastroenteritis is viral. These are self-limiting illnesses, which require supportive management only. Rotavirus is a seasonal viral agent causing gastroenteritis in the winter months in South Africa. In 2017 the season started in June and peaked in August.
Figure 1 : Number of stool samples that tested positive for rotavirus and/or adenovirus in 2017, by month in KZN
Figure 2 : Number of Salmonella species and Campylobacter species isolated in 2017, in KZN, by month.
0
20
40
60
80
100
120
140
Num
ber o
f pos
itive
s
Rotavirus and Adenovirus
0
5
10
15
20
25
30
35
40
45
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17
Num
ber o
f iso
late
s
Campylobacter species Salmonella species

14
The two most frequently isolated bacterial causes of diarrhoeal disease include the Campylobacter species and Salmonella species. These are most frequently detected in the summer months in South Africa.
Stool testing should be performed for patients presenting with diarrhoea accompanied by fever, bloody or mucoid stools, severe abdominal cramping or tenderness, or signs of sepsis.
Blood cultures should be obtained from infants <3 months of age, all patients with signs of septicemia and immunocompromised patients.
Molecular testing (PCR) is available for diagnosis of viral and bacterial causes of diarrhoeal illnesses.
Reference: Andi L Shane, Rajal K Mody, John A Crump, Phillip I Tarr, Theodore S Steiner,
Karen Kotloff, Joanne M Langley, Christine Wanke, Cirle Alcantara Warren, Allen C Cheng, Joseph Cantey, Larry K Pickering; 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea, Clinical Infectious Diseases, Volume 65, Issue 12, 29 November 2017, Pages e45–e80, https://doi.org/10.1093/cid/cix669
Gary R Fleisher et al. Approach to diarrhoea in children in resource-rich countries. Uptodate Literature review current through: Dec 2017
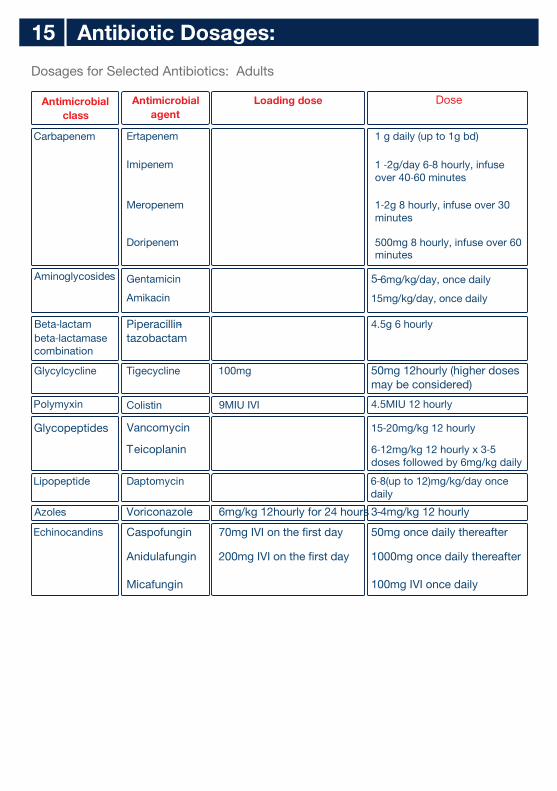
Dosages for Selected Antibiotics: Adults
Antibiotic Dosages:15
Antimicrobial class
Carbapenem
Aminoglycosides
Beta‐lactambeta‐lactamasecombination
Glycylcycline
Polymyxin
Glycopeptides
Lipopeptide
Azoles
Echinocandins
Antimicrobial agent
Ertapenem
Imipenem
Meropenem
Doripenem
Gentamicin
Amikacin
-
Piperacillintazobactam
Tigecycline
Colistin
Vancomycin
Teicoplanin
Daptomycin
Voriconazole
Caspofungin
Anidulafungin
Micafungin
Loading dose
100mg
9MIU IVI
6mg/kg 12hourly for 24 hours
70mg IVI on the first day
200mg IVI on the first day
Dose
1 g daily (up to 1g bd)
1 ‐2g/day 6‐8 hourly, infuseover 40‐60 minutes
1‐2g 8 hourly, infuse over 30minutes
500mg 8 hourly, infuse over 60minutes
-5 6mg/kg/day, once daily
15mg/kg/day, once daily
4.5g 6 hourly
50mg 12hourly (higher doses may be considered)
4.5MIU 12 hourly
15‐20mg/kg 12 hourly
6‐12mg/kg 12 hourly x 3‐5doses followed by 6mg/kg daily
6‐8(up to 12)mg/kg/day oncedaily
3- 4mg/kg 12 hourly
50mg once daily thereafter
1000mg once daily thereafter
100mg IVI once daily
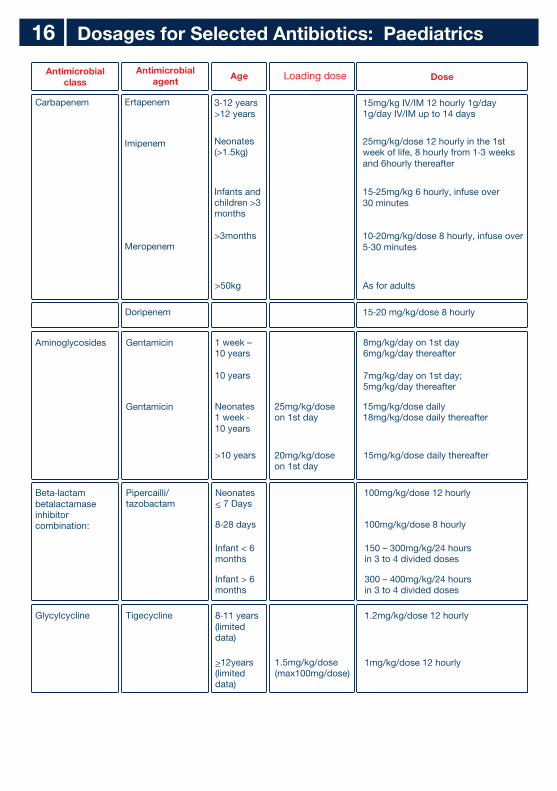
Dosages for Selected Antibiotics: Paediatrics16
Antimicrobialclass
Antimicrobial agent
Age Loading dose Dose
Carbapenem
Ertapenem 3‐12 years
>12 years15mg/kg IV/IM 12 hourly 1g/day1g/day IV/IM up to 14 days
25mg/kg/dose 12 hourly in the 1st week of life, 8 hourly from 1‐3 weeksand 6hourly thereafter
15‐25mg/kg 6 hourly, infuse over 30 minutes
10‐20mg/kg/dose 8 hourly, infuse over 5‐30 minutes
As for adults>50kg
Neonates(>1.5kg)
>3months
Infants andchildren >3months
Imipenem
Meropenem
Doripenem 15‐20 mg/kg/dose 8 hourly
Aminoglycosides Gentamicin
Gentamicin
1 week –10 years
10 years
Neonates1 week ‐ 10 years
>10 years
25mg/kg/doseon 1st day
20mg/kg/doseon 1st day
15mg/kg/dose daily thereafter
15mg/kg/dose daily18mg/kg/dose daily thereafter
8mg/kg/day on 1st day6mg/kg/day thereafter
7mg/kg/day on 1st day;5mg/kg/day thereafter
Beta‐lactam betalactamaseinhibitorcombination:
Pipercailli/tazobactam
Neonates< 7 Days
8‐28 days
Infant < 6months
Infant > 6months
150 – 300mg/kg/24 hoursin 3 to 4 divided doses
300 – 400mg/kg/24 hoursin 3 to 4 divided doses
100mg/kg/dose 8 hourly
100mg/kg/dose 12 hourly
Glycylcycline Tigecycline 8‐11 years(limited data)
>12years(limited data)
1.5mg/kg/dose(max100mg/dose)
1.2mg/kg/dose 12 hourly
1mg/kg/dose 12 hourly
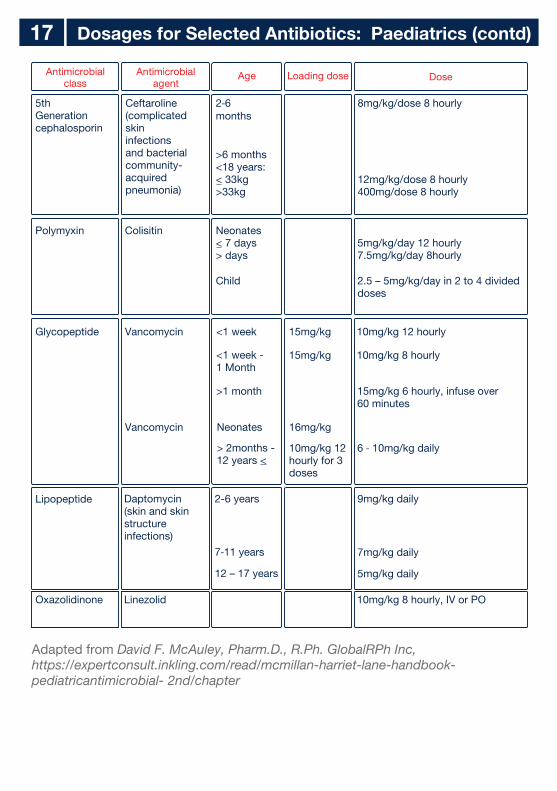
Dosages for Selected Antibiotics: Paediatrics (contd)17
Adapted from David F. McAuley, Pharm.D., R.Ph. GlobalRPh Inc,https://expertconsult.inkling.com/read/mcmillan-harriet-lane-handbook-pediatricantimicrobial- 2nd/chapter
Loading doseAntimicrobial class
Oxazolidinone
Lipopeptide
5thGenerationcephalosporin
Polymyxin
Glycopeptide Vancomycin
Vancomycin Neonates 16mg/kg
10mg/kg 12hourly for 3doses
> 2months -12 years <
<1 week
<1 week - 1 Month
>1 month 15mg/kg 6 hourly, infuse over60 minutes
6 ‐ 10mg/kg daily
15mg/kg
15mg/kg 10mg/kg 8 hourly
10mg/kg 12 hourly
Antimicrobial agent
Linezolid
Daptomycin(skin and skinstructureinfections)
Ceftaroline(complicatedskininfectionsand bacterialcommunity-acquiredpneumonia)
Colisitin
Dose
10mg/kg 8 hourly, IV or PO
9mg/kg daily
7mg/kg daily
5mg/kg daily
8mg/kg/dose 8 hourly
12mg/kg/dose 8 hourly400mg/dose 8 hourly
5mg/kg/day 12 hourly7.5mg/kg/day 8hourly
2.5 – 5mg/kg/day in 2 to 4 divideddoses
Age
2-6 years
7‐11 years
12 – 17 years
2‐6months
>6 months <18 years:< 33kg>33kg
Neonates< 7 days> days
Child
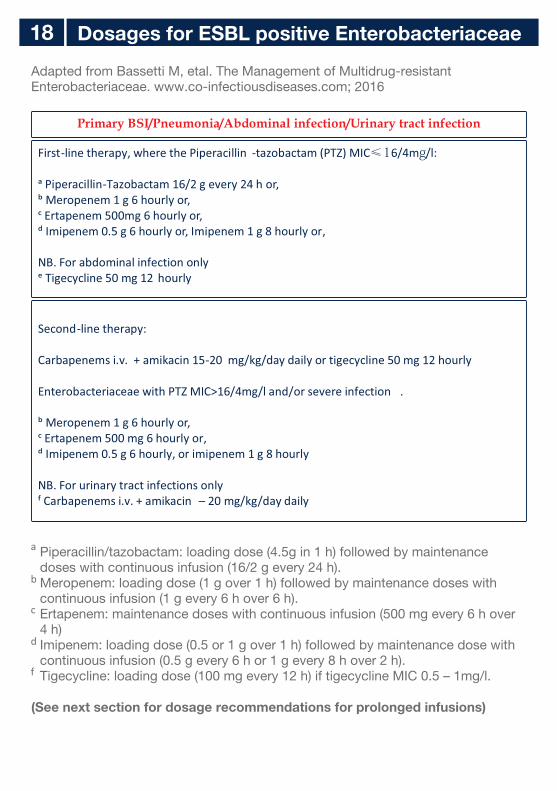
Dosages for ESBL positive Enterobacteriaceae18
Adapted from Bassetti M, etal. The Management of Multidrug-resistant Enterobacteriaceae. www.co-infectiousdiseases.com; 2016
Piperacillin/tazobactam: loading dose (4.5g in 1 h) followed by maintenance doses with continuous infusion (16/2 g every 24 h).Meropenem: loading dose (1 g over 1 h) followed by maintenance doses with continuous infusion (1 g every 6 h over 6 h).Ertapenem: maintenance doses with continuous infusion (500 mg every 6 h over 4 h)Imipenem: loading dose (0.5 or 1 g over 1 h) followed by maintenance dose with continuous infusion (0.5 g every 6 h or 1 g every 8 h over 2 h).Tigecycline: loading dose (100 mg every 12 h) if tigecycline MIC 0.5 – 1mg/l.
(See next section for dosage recommendations for prolonged infusions)
Primary BSI/Pneumonia/Abdominal infection/Urinary tract infection
First-line therapy, where the Piperacillin -tazobactam (PTZ) MIC≤16/4mg/l: a Piperacillin-Tazobactam 16/2 g every 24 h or,
ᵇ Meropenem 1 g 6 hourly or,
ᶜ Ertapenem 500mg 6 hourly or,
ᵈ
Imipenem 0.5 g 6 hourly or, Imipenem 1 g 8 hourly or,
NB. For abdominal infection only
ᵉ Tigecycline 50 mg 12 hourly
Second-line therapy:
Carbapenems i.v. + amikacin 15-20 mg/kg/day daily or tigecycline 50 mg 12 hourly
Enterobacteriaceae with PTZ MIC>16/4mg/l and/or severe infection .
ᵇ
Meropenem 1 g 6 hourly or,
ᶜ
Ertapenem 500 mg 6 hourly or,
ᵈ
a
b
c
d
f
Imipenem 0.5 g 6 hourly, or imipenem 1 g 8 hourly
NB. For urinary tract infections only
ᶠ
Carbapenems i.v. + amikacin –
20 mg/kg/day daily
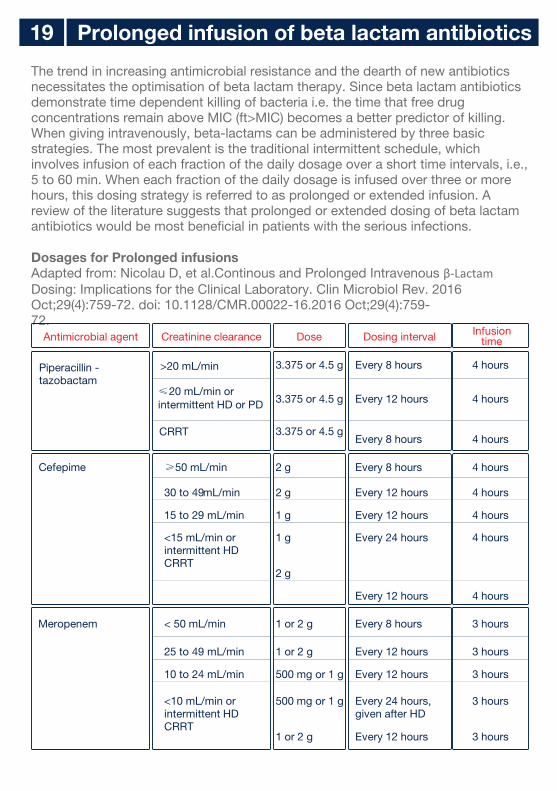
The trend in increasing antimicrobial resistance and the dearth of new antibiotics necessitates the optimisation of beta lactam therapy. Since beta lactam antibiotics demonstrate time dependent killing of bacteria i.e. the time that free drug concentrations remain above MIC (ft>MIC) becomes a better predictor of killing. When giving intravenously, beta-lactams can be administered by three basic strategies. The most prevalent is the traditional intermittent schedule, which involves infusion of each fraction of the daily dosage over a short time intervals, i.e., 5 to 60 min. When each fraction of the daily dosage is infused over three or more hours, this dosing strategy is referred to as prolonged or extended infusion. A review of the literature suggests that prolonged or extended dosing of beta lactam antibiotics would be most beneficial in patients with the serious infections.
Dosages for Prolonged infusionsAdapted from: Nicolau D, et al.Continous and Prolonged Intravenous β-Lactam Dosing: Implications for the Clinical Laboratory. Clin Microbiol Rev. 2016 Oct;29(4):759-72. doi: 10.1128/CMR.00022-16.2016 Oct;29(4):759-72.
Prolonged infusion of beta lactam antibiotics 19
Antimicrobial agent Creatinine clearance Dose Dosing interval Infusion time
Piperacillin - tazobactam
>20 mL/min
3.375 or 4.5 g Every 8 hours 4 hours
≤20 mL/min orintermittent HD or PD
3.375 or 4.5 g Every 12 hours 4 hours
CRRT
3.375 or 4.5 gEvery 8 hours 4 hours
Cefepime
≥50 mL/min
2 g
Every 8 hours 4 hours
30 to 49 mL/min
2 g
Every 12 hours 4 hours
15 to 29 mL/min
1 g
Every 12 hours 4 hours
<15 mL/min orintermittent HDCRRT
1 g
2 g
Every 24 hours 4 hours
Every 12 hours 4 hours
Meropenem < 50 mL/min 1 or 2 g Every 8 hours 3 hours
25 to 49 mL/min 1 or 2 g Every 12 hours 3 hours
10 to 24 mL/min 500 mg or 1 g Every 12 hours 3 hours
<10 mL/min orintermittent HDCRRT
500 mg or 1 g
1 or 2 g
Every 24 hours,given after HD
Every 12 hours
3 hours
3 hours
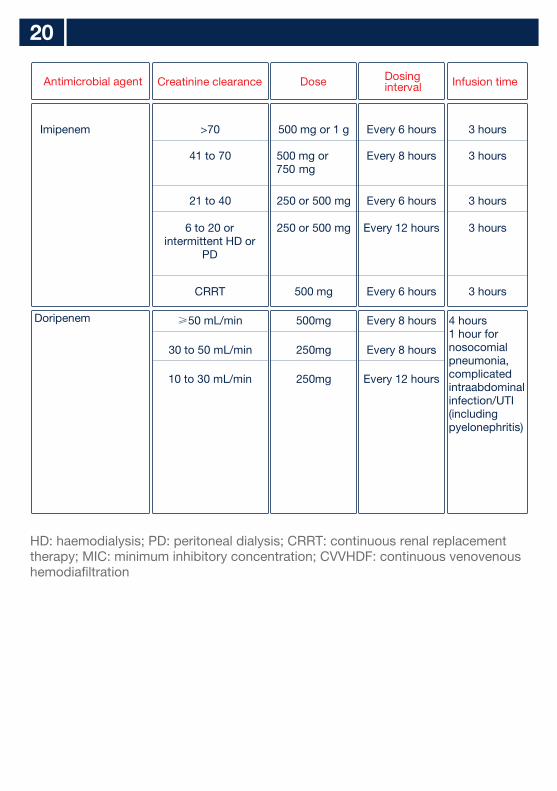
20
Antimicrobial agent
Creatinine clearance Dose Dosinginterval Infusion time
Imipenem
>70
500 mg or 1 g
Every 6 hours 3 hours
41 to 70
500 mg or 750 mg
Every 8 hours 3 hours
21 to 40
250 or 500 mg
Every 6 hours 3 hours
6 to 20 orintermittent HD or
PD
250 or 500 mg
Every 12 hours 3 hours
CRRT
500 mg
Every 6 hours 3 hours
Doripenem
≥50 mL/min 500mg
Every 8 hours 4 hours1 hour fornosocomialpneumonia,complicatedintraabdominalinfection/UTI(includingpyelonephritis)
30 to 50 mL/min
250mg
Every 8 hours
10 to 30 mL/min
250mg
Every 12 hours
HD: haemodialysis; PD: peritoneal dialysis; CRRT: continuous renal replacement therapy; MIC: minimum inhibitory concentration; CVVHDF: continuous venovenous hemodiafiltration
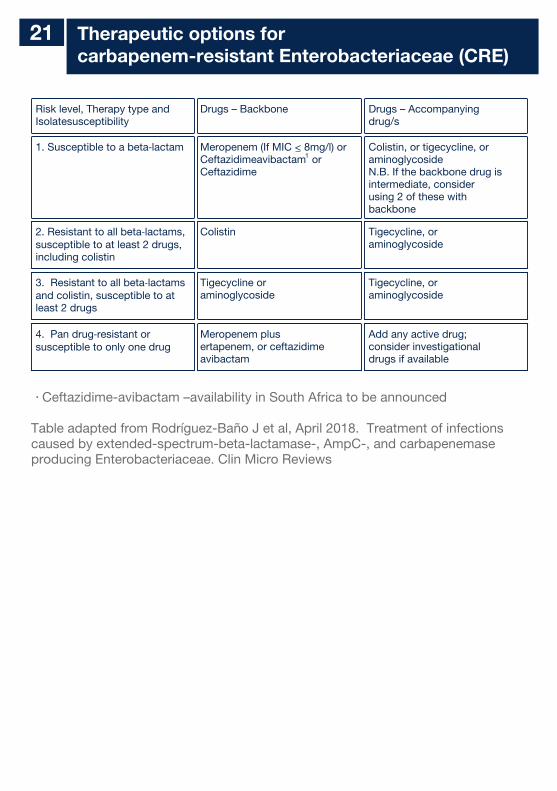
Therapeutic options for carbapenem-resistant Enterobacteriaceae (CRE)
21
Risk level, Therapy type and Isolatesusceptibility
Drugs – Backbone Drugs – Accompanyingdrug/s
1. Susceptible to a beta‐lactam
2. Resistant to all beta‐lactams,susceptible to at least 2 drugs,including colistin
3. Resistant to all beta‐lactams and colistin, susceptible to at least 2 drugs
4. Pan drug‐resistant or susceptible to only one drug
Meropenem (If MIC < 8mg/l) or Ceftazidimeavibactam or Ceftazidime
Colistin
Tigecycline oraminoglycoside
Meropenem plusertapenem, or ceftazidimeavibactam
Colistin, or tigecycline, oraminoglycosideN.B. If the backbone drug isintermediate, considerusing 2 of these withbackbone
Tigecycline, oraminoglycoside
Tigecycline, oraminoglycoside
Add any active drug;consider investigationaldrugs if available
1
Ceftazidime-avibactam –availability in South Africa to be announced
Table adapted from Rodríguez-Baño J et al, April 2018. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase producing Enterobacteriaceae. Clin Micro Reviews
22 INFECTIOUS DISEASES UPDATE
A.MALARIA TREATMENT UPDATE: Artesunate has replaced quinine as the treatment of choice for severe malaria and has been available from October 2017 as the registered product GARSUN®. The Section 21 application and reporting is no longer required.Compared to parenteral quinine, artesunate reduces death from severe malaria by 39% in adults and 24% in children.Advantages:1) Rapid antimalarial action with activity against early to late stages of the parasite
life cycle, preventing sequestration of parasite-infected red cells, and attendant complications.
2) Administration as a slow intravenous injection over several minutes rather than a slow rate-controlled intravenous infusion over 4-6 hours.
3) A favourable safety profile and without causing hypoglycaemia4) No dosage adjustment in renal failure.
Artesunate can be used in all trimesters of pregnancy, and there is no lower age or weight limit. It can also be administered intramuscularly if intravenous administration not possible.
Dosage of artesunate is 2.4 mg/kg for patients weighing >20 kg stat, and again at 12 and 24 hours, and then once daily until patients can take oral treatment. For patients weighing <20 kg, the dose is 3 mg/kg stat following the same schedule.
Artesunate must be given for at least 24 hours (i.e. 3 doses), and should be followed by a full course of artemether-lumefantrine (Coartem®) to avoid recrudescence.
MALARIA PROPHYLAXISThe past 2016/2017-malaria season in southern Africa was particularly busy and made local and international news.
Malaria preventive measures include chemoprophylaxis with mefloquine, doxycycline, or atovaquone/proguanil, which should be taken strictly according to pharmacist instructions. Mosquito bites may be prevented by washing clothes in pyrethroid insecticides, covering exposed areas especially at dawn and dusk by wearing long sleeves and pants, using mosquito nets and mosquito repellent, and staying indoors between dusk and dawn. Chemoprophylaxis is not 100% effective and travelers to malaria areas must be alert for the development of symptoms on return. Symptoms of malaria include fever, malaise, headaches and extreme tiredness. Danger signs are drowsiness, deep heavy breathing, yellow eyes, inability to eat or drink, and vomiting. Returned travelers, and residents in malaria-endemic areas that experience these symptoms should be investigated for malaria urgently. For more information on malaria in South Africa please visit www.nicd.ac.za
Source: Division of Public Health, Surveillance and Response, NICD-NHLS ( ) [email protected]
23 LISTERIA
An update on the outbreak of Listeria monocytogenes outbreak, South Africa, 2018
As of 20 February 2018, 915 laboratory-confirmed listeriosis cases have been reported to NICD since 01 January 2017 (Figure 1). Most cases have been reported from Gauteng Province (59%, 541/915) followed by Western Cape (12%, 112/915) and KwaZulu-Natal (7%, 66/915) provinces. Cases have been diagnosed in both public (64%, 587/915) and private (36%, 328/915) healthcare sectors. Diagnosis was based most commonly on the isolation of Listeria monocytogenes in blood culture (73%, 669/915), followed by CSF (22%, 198/915). Where age was reported (n=886), ages range from birth to 92 years (median 20 years) and 41% (361/886) are neonates aged ≤28 days (Figure 2). Of neonatal cases, 97% (351/361) had early-onset disease (birth to ≤6 days). Females account for 56% (499/886) of cases where gender is reported. Final outcome data is available for 67% (617/915) of cases, of which 28% (172/617) died. This suggests that most cases in this outbreak have been exposed to a widely available, common food type/source. The most likely source of the current outbreak has been determined. Further information on Listeria treatment and prevention is available on our Lancet newsletter or via the NICD website ( www.nicd.ac.za)
Source: Centre for Enteric Diseases, and Division of Public Health Surveillance and Response, NICD-NHLS
24 PCR Tests
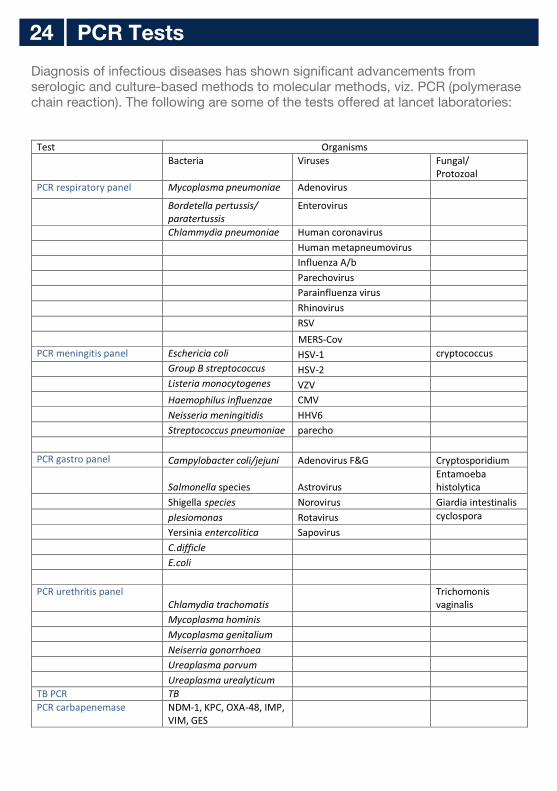
Diagnosis of infectious diseases has shown significant advancements from serologic and culture-based methods to molecular methods, viz. PCR (polymerase chain reaction). The following are some of the tests offered at lancet laboratories:
Test Organisms
Bacteria
Viruses
Fungal/Protozoal
PCR respiratory panel
Mycoplasma pneumoniae
Adenovirus
Bordetella
pertussis/ paratertussis
Enterovirus
Chlammydia
pneumoniae
Human coronavirus
Human metapneumovirus
Influenza A/b
Parechovirus
Parainfluenza virus
Rhinovirus
RSV
PCR meningitis panel
Eschericia coli
HSV-1
cryptococcus
Group B streptococcus
HSV-2
Listeria monocytogenes
VZV
Haemophilus influenzae
CMV
Neisseria meningitidis
HHV6
Streptococcus pneumoniae
parecho
PCR gastro panel
Campylobacter coli/jejuni
Adenovirus F&G
Cryptosporidium
Salmonella species
Astrovirus
Entamoeba histolytica
Shigella
species
Norovirus
Giardia intestinalis
plesiomonas
Rotavirus
cyclospora
Yersinia
entercolitica
Sapovirus
C.difficle
E.coli
PCR urethritis panel
Chlamydia trachomatis
Trichomonis vaginalis
Mycoplasma hominis
Mycoplasma genitalium
Neiserria gonorrhoea
Ureaplasma parvum
Ureaplasma urealyticum
TB PCR TB
PCR carbapenemase NDM-1, KPC, OXA-48, IMP, VIM, GES
MERS-Cov
Google playANDROID APP ON
www.lancet.co.za
@LancetLabApp StoreAvailable on the
LancetLaboratories
corporate branding/booklets/annual surveillance report and antibiotic guide/2018/ep00111 booklet annual surveillance specialist practitioners a5 eng duplex 170gsm taurus mar2018.cdr | rev001
ITEM CODE: EP00111