
Annual Reports (Nursing and Organization) Quality Plans ...
84
Annual Reports (Nursing and Organization) Quality Plans Patient Safety Plan Strategic Plan for the Organization and Nursing Services OO3: The following documents are provided: Nursing Annual Report (Attachment 1) (Note that 2014 is the most recent. The 2015 report is currently in production) Organizational Annual Report (Attachment 2) (Annual Report Document 2014) Quality & Patient Safety Plan 2016 (At Capital Health, the Quality Plan and the Safety Plan are combined in one document) (Attachment 3) Strategic Plans for the Organization (Attachment 4) Strategic Plan for Nursing Services (Attachment 5) Organizational Overview Source of Evidence - OO3
Transcript of Annual Reports (Nursing and Organization) Quality Plans ...

Annual Reports (Nursing and Organization)
Quality Plans
Patient Safety Plan
Strategic Plan for the Organization and Nursing Services
OO3: The following documents are provided:
Nursing Annual Report (Attachment 1) (Note that 2014 is the most recent. The 2015 report is currently in production)
Organizational Annual Report (Attachment 2) (Annual Report Document 2014)
Quality & Patient Safety Plan 2016 (At Capital Health, the Quality Plan and the Safety Plan are combined in one document) (Attachment 3)
Strategic Plans for the Organization (Attachment 4)
Strategic Plan for Nursing Services (Attachment 5)
Organizational Overview
Source of Evidence - OO3

Organizational Overview
Exhibits for SOE - OO3

AnnuAl RepoRt
2014
2-5yearson unit
3%MSNPhD
56% 13 %BSN 10
yearson unit
29%
<30: 12% >40: 68%
AGE<30: 14% >40: 69%
AGE
RMC
2-5yearson unit
7%MSNPhD
45% 18%BSN 10
yearson unit
28%
HW
NURSING
ndoolan
Text Box
OO3: Attachment 1
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE

Tr a n s f o r m a t i o n a l L e a d e r s h i p
A Letter from the Chief Nursing Officer ..................................................................................................................................... 1
Our Philosophy of Nursing ........................................................................................................................................................................ 2
Strategic Planning: EbOLA PrEPArEdNESS ....................................................................................................................... 3
S t r u c t u r a l e m p o w e r m e n t
Magnet recognition Program ............................................................................................................................................................... 5
Commitment to Professional development .......................................................................................................................... 6
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
Patient-Centered Care Model at Capital Health ...........................................................................................................10
5M Staff Improve Infection and Fall Safety rates .........................................................................................................12
rMC Earns 2014 Press Ganey Commitment to Excellence Award ...........................................................15 for Patient Experience
Improvement in Early Elective delivery (EEd) ..................................................................................................................16
Exclusive breastfeeding for Mothers ..........................................................................................................................................17
N e w K n o w L e d g e a n d i n n o vat i o n
Lung CT Screening Program for High-risk Patients ..................................................................................................19
New Observation Units in Ambulatory Care ......................................................................................................................20
NJ’s First Autism-Friendly Pediatric Emergency room ..........................................................................................22
Computerized Physician Order Entry (CPOE) ...................................................................................................................23
E m p i r i c a l o u t c o m e s
2014 research Highlights .........................................................................................................................................................................26
Ongoing research at Capital Health ..........................................................................................................................................27
2014 Conferences/Presentations/Publications ................................................................................................................28
2014 Excel lence in Nursing Pract ice award recipients ................back Cover
Capital HealtH 2014 Nursing annual Report table of CoNteNts

Colleagues:
The International Council of Nurses (ICN) theme for 2014 was Nurses: a force for Change — A Vital Resource for Health. As I reflect on the past year, I cannot imagine a more appropriate theme. Nurses are not just a vital, but a critically essential component to improving health.
One of the major tenets of the ICN’s 2014 focus was the need for an educated nursing workforce in a constantly changing healthcare environment. Our nurses at Capital Health had an amazing year in terms of educational achievements. Our rates of bSN and certified nurses continue to grow. In addition to the previous options for nurses continuing their education, Capital Health reached an agreement in 2014 with The College of New Jersey to begin an on-site bSN program. We needed 20 nurses to commit to the program. We got 30 for the first cohort, and as I write this, we are preparing to start our second cohort. Nurses have formed study groups to prepare and support each other in attaining professional nursing certification. Capital Health faculty and nursing staff who are educating the accelerated second degree nurses from Thomas Edison State College had another successful year with 100% of graduates achieving success in the NCLEX licensing exam.
Educational accomplishments in the practice areas are even more amazing. Not surprisingly, technology was likely the leading area requiring education. The past year saw the arrival of computerized physician order entry (CPOE) to the clinical areas. Teams also worked on updates to NTT and the implementation of additional documentation tools, upgrades to the Ob documentation system (Ob TraceVue) and building the new Or Information System (GE Centricity). documentation was created and implemented for use on our Observation Units. New technology like Avasure for monitoring 1:1’s and the expansion of uses for point-of-care-testing (POCT) also occurred in 2014.
And let’s not forget that 2014 brought a whole new healthcare concern in the US – Ebola. Countless hours were spent developing the safest protocols to protect staff and effectively care for patients. And we ended the year preparing the Emergency department staff at Capital Health regional Medical Center for a hospital without in-house obstetrics.
In the area of patient care and quality, there are endless examples of Capital Health nurses seeking knowledge and continually learning. We have teams working to reduce Catheter Associated Urinary Tract Infections (CAUTI), Central Line Associated blood Stream Infections (CLAbSI), Sepsis, falls and VTEs. These teams educate staff to identify evidence-based practices to improve patient outcomes.
I could continue with more examples but I think it is safe to say that nursing education and lifelong learning are alive and well at Capital Health. You will see more examples as you read through this report; 2014 was another year of major achievements. I cannot tell you how proud I am of the nurses at Capital Health. I hope you enjoy reading and reflecting on what a force for change our nurses are.
Sincerely,
Eileen M. Horton, MSN, MSM, rNVice President – Patient Services/Chief Nursing Officer
>>transformational leadeRsHip
a letter from the Chief Nursing officer Nurses: a force for Change–a Vital Resource for Health

Capital HealtH 2014 Nursing annual Report 2
Tr a n s f o r m a t i o n a l L e a d e r s h i p
The Capital Health department of Nursing is committed to the delivery of care through a shared vision of professionalism, integrity and caring. The philosophy of nursing at Capital Health is based on the teachings of Florence Nightingale. Florence Nightingale is the first theorist and founder of modern nursing. She stated in her nursing notes that “nursing” is an act of utilizing the environment of the patient to assist him in his recovery, (*Nightingale 1860/1969), that it involves the nurses initiatives to configure environmental settings appropriate for the gradual restoration of the patient’s health, and that external factors associated with the patient’s surroundings affect life or biological and physiological processes and development.
The nursing staff provides patient-centered care while focusing on patients’ needs and the environment in which they live. developing relationships through observation and interactions, as well as documenting
that information, helps provide a clear picture of an individual’s needs during hospitalization, while demonstrating the importance of his or her environment in improving health and recovery from illness. Capital Health nurses support patient/family-centered care, and as a result, developed CarePartners, a program designed to meet the patient’s personal, emotional, spiritual, physical and psychosocial needs. Each patient can choose up to three CarePartners who are actively involved in his or her care. They are encouraged to be the patient’s support system, and at times, advocate to protect and respect the patient’s sense of dignity and independence.
Notes on Nursing (1992). Florence Nightingale. Lippincott, Williams and Wilkins. Phil, Pa. (18)
our philosophy of Nursing

Capital HealtH 2014 Nursing annual Report 2 Capital HealtH 2014 Nursing annual Report 3
Tr a n s f o r m a t i o n a l L e a d e r s h i p
In September 2014, a multidisciplinary team met to address Capital Health’s response to an Ebola patient. This team soon became the Ebola Steering Committee with additional members added as needed. The team was divided into three committees, each working on specific aspects of care. The teams included Education and Communication, Clinical, and Equipment and Materials committees. Each committee identified tasks that needed to be accomplished in a very short period of time.
Education/Communication Committee
This committee addressed staff education related to Ebola through various media. Signs were developed for each entry point of the hospitals and each entry point person was trained to screen by asking the two key questions (travel/contact + fever = isolate).
A 24/7 on-call Ebola response Team was identified. Their purpose was to help relieve staff anxiety and provide support for staff working all shifts. The committee worked collaboratively with the Public relations/Marketing department to provide all Capital Health employees with consistent and up-to-date information on Ebola preparedness. Web-based online education for non-clinical and clinical staff was developed resulting in over 90% of staff completing the education. Public relations worked closely with the team and was instrumental in providing up-to-date information for all departments.
Clinical Committee
The primary focus of this committee was to train identified staff on the correct use of evidence-based personal protective equipment (PPE). The team decided that it was not feasible to train all staff on the correct use of donning and doffing PPE. Therefore, Emergency department (Ed), Pediatric department, Pediatric Ed, Intensive Care Unit and Labor and delivery rNs were identified as the focus group for PPE training. This proved to be a challenge as the Centers for disease Control & Prevention (CdC) constantly changed their recommendations for the type of PPE used. After a month of training in PPE, the use of powered air purifying respirator (PAPr), which includes a large hood with full face shield and battery packs for motorized air flow control, was highly recommended. This change in CdC recommendations occurred after reviewing outcomes for several Ebola-infected patients treated in the United States.
our philosophy of Nursing strategic planning—ebola pRepaRedNess

Capital HealtH 2014 Nursing annual Report 4
Tr a n s f o r m a t i o n a l L e a d e r s h i p
The Clinical Committee was also challenged with identifying care space for potential Ebola patients, which included identifying appropriate staff members as well as the supplies needed to care for the patient. All three committees collaborated to provide drills for designated staff. With each meeting, more concerns and processes were reviewed and identified as needing process improvement. One example includes the high risk associated with drawing blood and processing lab specimens. The decision was made to use point-of-care testing as the primary type of testing performed on this patient population. This led to a change in practice requiring additional staff education.
Equipment/Materials Committee
This committee was charged with management of waste/trash/linen/textiles that came in contact with the suspect/confirmed Ebola patient as well as the cleaning of equipment after use. In addition, the committee identified equipment needs, including the need for an increased supply of large and X-large PPE. One of its biggest challenges was assuring an adequate supply of PPE as every hospital was ordering PPE to prepare for the potential Ebola patient. demand was high and supplies were very hard to obtain. This committee persevered and the needed PPE was obtained.
Additional sub-committees were formed based on the community we serve and the potential types of patients we could be treating. A maternity sub-committee was formed to deal with issues specific to the pregnant woman who is positive for Ebola. Another sub-committee was formed to address ethical considerations for the critically ill patient with Ebola.
Each of these sub-committees reported back to the Ebola Steering Committee. After meeting for six weeks, it was identified that these committees could dissolve and a bi-monthly Ebola Steering Committee meeting was established. repetitive PAPrS training continues. Signage and ongoing educational updates are provided as well as identifying potential new care areas for Ebola patients. Ebola drills are planned and debriefed with process improvements initiated as needed. This multidisciplinary committee quickly developed a strategic plan that would allow Capital Health staff to safely care for patients who may present with Ebola. After six weeks, these committees were dissolved. The Ebola Steering Committee now meets bi-monthly and repetitive PAPr training continues. All of this work was accomplished as the result of the strong collaboration and work effort demonstrated by this multidisciplinary team.

Capital HealtH 2014 Nursing annual Report 4 Capital HealtH 2014 Nursing annual Report 5
Capital Health has held Magnet recognition Program® designation since 2002. recognized through the American Nurses Credentialing Center (ANCC), the program’s guiding principles advance three goals within healthcare organizations:
nPromote quality in a setting that supports professional practice
nIdentify excellence in the delivery of nursing services to patients
ndisseminate best practices in nursing services
The Magnet program criteria are organized into five model components and serve as the framework for the appraisal process.
Capital Health’s Magnet re-designation Timeline
The deadline for Capital Health’s fourth re-designation application is fast approaching. Teams are gathering data and collecting stories in preparation. The journey to re-designation requires teamwork, dedication and respect from the entire organization for a successful application.
> > s t r u c t u r a l e m p o w e R m e N t
magnet Recognition program
EMPIRICALOUTCOMES
STRUCTURALEMPOWERMENT
NEW KNOWLEDGE,INNOVATION ANDIMPROVEMENTS
TRA
NSF
OR
MA
TIO
NA
LLE
AD
ER
SHIP
EX
EM
PLARY
PRO
FESSIO
NA
LPR
AC
TICE

Capital HealtH 2014 Nursing annual Report 6
S t r u c t u r a l e m p o w e r m e n t
Commitment to professional development
Contact Hour Opportunities
Capital Health remains committed to the professional development of our nurses by providing opportunities that enhance their growth.
nThe Professional Nurse Education Fund awarded 16 nurses a total of $4,513.99 for off-site continuing education.
nOur New Jersey State Nurses Association (NJSNA) provider unit processed 59 CNE programs and awarded 4,422.61 contact hours to nurses in 2014.
nA new online Emergency Nurses Association (ENA) orientation program was implemented for Er nurses that complements the current roster of online learning systems – American Association of Critical-Care Nurses (AACN) Orientation, AACN EKG Interpretation Program, and Periop 101.
nUse of our CE direct Online contact hour program was robust. Our nurses completed 8,813.9 courses for 11,199.1 contact hours. Our top earners of nursing contact hours in CE direct:
name number of contact hours
Kim Moroz Neuro ICU 100
Andrea buchan Primary Care - Hamilton 79
Sudesh Joshi Chibbar Perioperative Services 77
Erika Sahrun Neuro ICU 76
Edith Scannella Case Management 74
Valerie Sampson Ambulatory Care/Clinic 73
Jonas Moulic Neuro ICU – rMC 69
Teresita Albano Steen 2 – rMC 63
Eugenia Tan Surgical Trauma Care Unit 61
Education and Certification
Capital Health supports the Institute of Medicine’s (IOM) recommendation to increase the number of bSN-prepared nurses and strives toward the Magnet goal of 80% by 2020. We continue to maintain and develop practice partner relationships with colleges and universities to offer reduced tuition rates to our nurses.
We created a new partnership with rider University for their online rN to bSN program. rider University, along with our current practice partners of Thomas Edison State College, drexel University, and The College of New Jersey, remain committed to supporting nurses who wish to return to school.
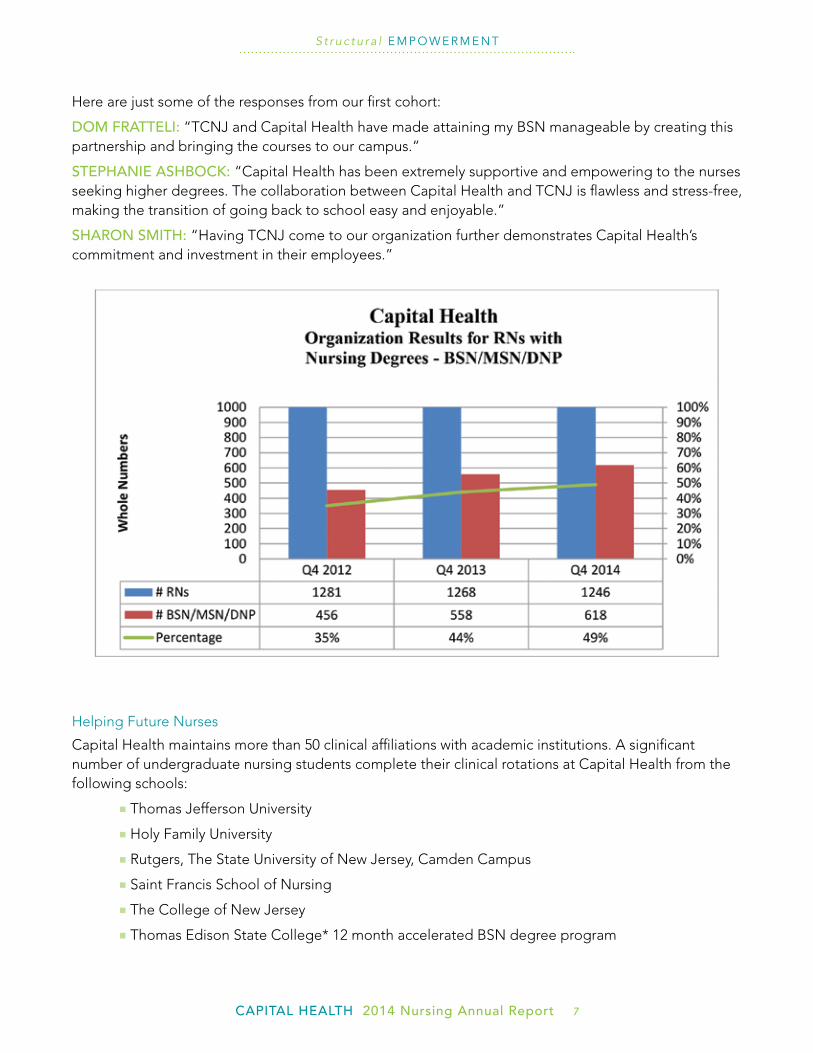
We collaborated with The College of New Jersey (TCNJ) to offer an on-site rN to bSN program at Capital Health Medical Center - Hopewell. The first cohort of 30 rNs was a success, and program interest was so high that an additional cohort class started in January 2015 with another 11 rNs enrolled.
Capital HealtH 2014 Nursing annual Report 6 Capital HealtH 2014 Nursing annual Report 7
S t r u c t u r a l e m p o w e r m e n t
Commitment to professional developmentHere are just some of the responses from our first cohort:
dom fRatteli: “TCNJ and Capital Health have made attaining my bSN manageable by creating this partnership and bringing the courses to our campus.”
stepHaNie asHboCk: “Capital Health has been extremely supportive and empowering to the nurses seeking higher degrees. The collaboration between Capital Health and TCNJ is flawless and stress-free, making the transition of going back to school easy and enjoyable.”
sHaRoN smitH: “Having TCNJ come to our organization further demonstrates Capital Health’s commitment and investment in their employees.”
Helping Future Nurses
Capital Health maintains more than 50 clinical affiliations with academic institutions. A significant number of undergraduate nursing students complete their clinical rotations at Capital Health from the following schools:
nThomas Jefferson University
nHoly Family University
nrutgers, The State University of New Jersey, Camden Campus
nSaint Francis School of Nursing
nThe College of New Jersey
nThomas Edison State College* 12 month accelerated bSN degree program

Capital HealtH 2014 Nursing annual Report 8
S t r u c t u r a l e m p o w e r m e n t
Table #
The following Capital Health nurses are committed to academic excellence by presenting lectures to nursing students at the request of our academic partners or by currently holding a formal faculty position:
nMichelle bostic MSN, APN, C; rNC-Ob Thomas Jefferson University
nVicki brzoza MbA, MSN, CCrN Thomas Edison State College
nMaria deCromar MSN, CNM Thomas Jefferson University
nKathy donaldson MSN, APN, C; CPLC, C-EFM The College of New Jersey/St. Francis SON
nLynne Capik MSN, APN,C Thomas Edison State College
nCarolyn Cooper bSN, rN-bC The College of New Jersey
nKim doney MSN, rNC-NIC Thomas Edison State College
nCookie Estlow MSN, rN, CPEN, PNP-bC The College of New Jersey
nGary Fassler MSN, rNC-Ob Thomas Edison State College
nAgnes Gallagher MSN, CCrN rutgers, State University of New Jersey/ burlington CC

Capital HealtH 2014 Nursing annual Report 8 Capital HealtH 2014 Nursing annual Report 9
S t r u c t u r a l e m p o w e r m e n t
nregina Kukulski MSN, APN,C; bC, CNE Thomas Edison State College
nVera Kunte MSN, APN,C; dNP Candidate Thomas Edison State College
nApril Lang MSN, APN,C The College of New Jersey
nCheryl Lang MSN, APN,C; CEN The College of New Jersey
nJill Mahony MSN, APN, C; rNC-Ob, C-EFM Thomas Jefferson University/ The College of NJ/St. Francis SON
nLisa McConlogue Phd, MSN, PMHCNS-bC Thomas Edison State College
nGary Oravsky bSN, CrN Jersey College of Nursing
nChris Saltzman MSN, rNC-NIC Thomas Jefferson University
nCaroline Steward MSN, APN,C; CCrN,CNN Thomas Edison State College/ Mercer County CC
nKatrina Sweeney MSN, rN-bC The College of New Jersey/ College of Saint Elizabeth
Capital HealtH 2014 Nursing annual Report 10
>>exemplary pRofessioNal pRaCtiCe
patient-Centered Care model at Capital Health
Capital Health commits to making patient satisfaction a priority. during 2014, a nursing work team was created at each of the hospital campuses – Patricia Michael, MSN spearheaded the team at Capital Health Medical Center - Hopewell and ruthann Tobolski, MA, bSN, NEA-bC led the team at Capital Health regional Medical Center. Work team members included representatives from both professional and technical staff.
The need to improve patient-centered care is supported in literature. According to The Advisory board Company, the benefits of patient-centered care delivery are:
Enhanced Operational Efficiency
ndecreased length of stay
nImproved care coordination, discharge planning
Appropriate resource Utilization
nLowered demand for specialty services
nreduced readmission rates
Improved Quality and Safety Outcomes
nreduced adverse events
ndecreased mortality rates
nIncreased quality of life post-discharge
nIncreased staff retention
nImproved staff engagement, satisfaction
nImproved unit culture, teamwork

Capital HealtH 2014 Nursing annual Report 10 Capital HealtH 2014 Nursing annual Report 11
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
>>exemplary pRofessioNal pRaCtiCe
patient-Centered Care model at Capital Health
patieNt-CeNteRed CaReAT CAPITAL HEALTH
bedsideRepoRt
Nurses conduct shift change report/handoff
in patient’s roomStandardized tool used
daily patient goals identified.
patieNteNgagemeNt
Patient/family participates in bedside shift report and become essential partners in their care
(CarePartners).
HouRlyRouNdiNgNursing staff rounds on all patients with
special attention to four specific care needs [4 P’s]:
Pain, Positioning, Potty (bathroom assisted),Personal Items in reach.
safetyHuddles
Occurs at the start of each shift. Led by
the charge nurse. A review of any safety or care
concerns. Help team focus on what is most
important for today.
Patient-Centered Care Model
Capital Health’s improvement strategies during the year focused on:
nbedside Shift reporting
nHourly rounding
nCare board Communication
nSafety Huddles
Each campus implemented select strategies for different nursing units based on campus outcome data, organizational culture and readiness. Team members meet monthly and share their successes and challenges with the group. Improvement activities are expected to continue throughout 2015.

Capital HealtH 2014 Nursing annual Report 12
5m staff improve infection and fall safety Rates
As the result of a nurse-driven “Call to Action,” the staff on 5M, a medical and oncology unit at Capital Health Medical Center – Hopewell, worked collaboratively to reduce Central Line Associated bloodstream Infections (CLAbSI) and patient falls.
Line rounds
In 2014, 5M sustained five CLAbSI’s. The unit’s CLAbSI rate was 7.87, well above the National Healthcare Safety Network (NHSN) benchmark of 0.9 per 1,000 patient days. Weekly IV line rounds began in January 2014. during these rounds, both central and peripheral lines are evaluated for care and maintenance. Weekly intravenous line rounds were in progress in January 2014. during these rounds, both central lines and peripheral lines were evaluated for care and maintenance.
Monitored central line issues included:
1) Was the dressing dated?
2) Were Curos Caps® on all ports?
3) Was the bIOPATCH® in place and correctly applied?
4) Was the correct dressing type being used specific to the location of line (e.g. sorbaview for internal jugular site)?
5) Was the dressing dry and intact?
6) Was the dressing less than seven days old?
Peripheral IV’s are checked for:
1) dressing date
2) Proper securement device (statlock or sterile chevron)
3) Curos Caps® on all ports
4) Site start date in compliance with Capital Health policy (i.e. less than 96 hours old)
5M nurses identified multiple issues during line rounds:
nChallenges in caring for lines on immunocompromised patients
nLack of consistency in utilizing Curos Caps® on all open connections
ndressings inadequate for site coverage causing breaks in the intact dressing
nLack of consistent documentation in the MAr for scheduled line changes
Changes were made between July and September 2014 to reduce the rate:
nLarger port dressings were purchased and utilized on all central lines.
n Chloralhexidine baths were initiated for all bedridden patients with end stage renal disease, liver disease or failure to thrive, and had a central line.
nFocused staff education on daily line assessment, line access and dressing changes.
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e

Capital HealtH 2014 Nursing annual Report 12 Capital HealtH 2014 Nursing annual Report 13
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
5m staff improve infection and fall safety RatesAfter implementing these changes and continuing IV line rounds, the CLAbSI rate decreased to zero between September and december and is below the national benchmark.
reducing Falls
5M experienced 52 falls in 2013 and 17 falls during the first quarter of 2014, which was above the National database of Nursing Quality Indicators (NdNQI) average. Part of the problem-solving process involved the Stryker bed Company who conducted an independent audit on adherence to fall prevention strategies on high-risk patients. Elements of the audit included: checking room signage, patients wearing fall Id bracelets, rooms free of clutter, call bell within patient reach, and bed alarms activated. The audit found that these elements were not consistently implemented.
In April 2014, the 5M staff and educators began an initiative to reduce falls with injury to meet or exceed the NdNQI benchmark of falls per 1,000 patient days with injury.
Hopewell 5M, CLABSI Rate ClABSI rate

Capital HealtH 2014 Nursing annual Report 14
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
The timeline for improvement that was followed by 5M nurses:
apRil 2014
—bedside shift report initiated, with an emphasis on hourly rounding.
—bathroom signage posted in each room.
—Wireless bed alarms installed on all beds to connect with the nurses’ Ascom telephones.
July 2014
—daily poster displayed identifying the number of days since the last patient fall on 5M.
oCtobeR 2014
—Telesitter patient monitoring camera initiated on high-risk patients.
—High-risk fall alerts documented on unit huddle sheets.
Falls on 5M decreased during the 4th quarter. The last fall occurred on November 17, 2014, and as of March 2, 2015, 5M staff celebrated 115 days with no falls.
Ho
url
y R
ou
nd
ing
Be
dsi
de
Re
po
rt

Capital HealtH 2014 Nursing annual Report 14 Capital HealtH 2014 Nursing annual Report 15
Capital Health regional Medical Center (rMC) recently became the only hospital in New Jersey and one of only six in the country to earn the 2014 Press Ganey Commitment to Excellence Award for Patient Experience.
The staff at rMC earned this award based on patient surveys collected from Press Ganey Associates, Inc. during a two-year span (2012 and 2013) and how patients responded specifically to the question of their likelihood to recommend regional Medical Center to others.
The Commitment to Excellence Award recognizes clients of Press Ganey who have consistently outpaced their peers in rates of performance improvement. The award was based on the data for the “recommend this Hospital” CAHPS question. The results were:
The award was presented to Capital Health regional Medical Center representatives at the Press Ganey National Conference in Orlando, Florida on November 4, 2014.
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
RmC earns 2014 press ganey Commitment to excellence award for patient experience oNly NJ Hospital, oNe of six iN tHe us
2012 2013 improvement
Quarter 1 62.2 69.8 7.6
Quarter 2 62.5 72.1 9.6
Quarter 3 55.7 69.7 14

Capital HealtH 2014 Nursing annual Report 16
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
research shows that more babies born between 37 and 39 weeks are admitted to a Neonatal Intensive Care Unit (NICU) for respiratory complications than those born at or after 39 weeks. In the three quarters prior to the changes made in October 2012, Capital Health had a total of 13 EEds between its two hospitals.
In July 2012, Katharine donaldson, MSN, APN, C, CPLC, C-EFM proposed a “hard stop” for scheduling inductions and cesarean births that involved use of two scheduling forms, one for inductions and the other for cesarean births. Three forms were evaluated by Capital Health’s Obstetrics Multidisciplinary Safety Committee, two of which were adapted from a form used by Oregon’s Health and Services and a third from the American College of Obstetricians & Gynecologists (ACOG, 2011). She proposed that the licensed independent provider (LIP) or designee would complete and fax the procedure-specific form to Labor & delivery at the time that the procedure was scheduled. A Labor & delivery nurse, usually the charge nurse, would then review the form and, if the timing and indication were appropriate, sign the form to authorize the procedure. If the procedure was not appropriately timed or the indication was questionable, the assistant nurse manager or nurse manager contacted the LIP. The forms would not be part of the permanent record but would be kept for future reference.
Capital Health’s Safety Committee approved the use of forms for inductions and cesarean births that incorporated items from the three example forms. They also approved a new policy and procedure titled, Scheduling of Inductions and Cesarean Births. Subsequently, the Obstetric Nursing Practice Council and the department of Obstetrics & Gynecology at Capital Health approved the process, forms, and policy in September 2012. The effective date was October 22, 2012.
data collection regarding EEds resumed in the first quarter of 2013. Following process implementation, there was an immediate and significant reduction in the number of EEds. The decrease has been sustained for more than two years.
In the second quarter of 2014, Capital Health had its first EEd in more than nine months. It was noted by the APNs that not all of the LIPs faxed the scheduling forms. Modification of the process was indicated. Instead of the charge nurses authorizing procedures, the APNs assumed this responsibility. The APN who initiated the process and the chairperson of the department of Obstetrics & Gynecology at Capital Health reminded the LIPs of the process at their monthly department meeting in August 2014.
Since the reminder and the implementation of the modification in August 2014, compliance with the faxing of scheduling forms has increased, and there have been no EEds.
improvement in early elective delivery (eed)

Capital HealtH 2014 Nursing annual Report 16 Capital HealtH 2014 Nursing annual Report 17
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
In 2007, the State of New Jersey initiated an effort to increase the rates of exclusive breastfeeding because of the high percentages of obesity and childhood obesity in age groups 2 – 5 years old (New Jersey has the highest rate of obesity in this population). Capital Health started its journey to achieve baby Friendly status by intensifying education to increase the rate of exclusive breastfeeding. baby Friendly© designation was achieved in March 2012 with an exclusive rate of 63% in 2011.
exclusive breastfeeding for mothers

Capital HealtH 2014 Nursing annual Report 18
E x e m p l a r y p r o f e s s i o n a L p r a c t i c e
The Joint Commission’s 2014 core measures for maternal child health stated that an exclusive breastfeeding rate of 90% should be possible. After designation, Capital Health’s rates of initiation were very good at over 80%, but exclusivity still lagged. Capital Health added a series of intense nursing competencies that emphasized the importance of the Ten Steps of Baby Friendly, including improved level of documentation for formula supplementation, skin-to-skin, and rooming in were added after designation in 2012.
While statistics are influenced by many factors, such as the decision to breastfeed, the report published in 2014 named Capital Health as the facility with the highest rate of exclusivity in the state of New Jersey at 84%.
It is important to note that the Electronic birth Certificate (EbC) program was used to calculate the statistics for this report. The EbC relies on what the mother reports for its data. Chart review actually estimated a lower rate of exclusivity, pointing to a discrepancy in what mothers perceive and what they actually do. In any case, all the hospitals were measured in the same system, thus putting all hospitals on equal footing. The data was measured based on predicted outcome for population as well, so that those hospitals having more difficulty to penetrate populations were credited with any achievements. An expected “average rate” based on the population was included in the report and a standardized score. Scores of “1” mean the average predicted score is achieved. “> or < 1” means a better than expected or lower than expected score. Capital Health achieved a 2 at Capital Health Medical Center – Hopewell and a 1.91 for Capital Health regional Medical Center.
(*Baby Friendly is an international designation awarded through WHO and UNICEF to facilities who practice the “Ten Steps” and do not engage in promotion of breast milk substitutes. The designation can only be used by those facilities that have passed the required standards of care and audit by Baby Friendly USA assessors.)
baby-friendly designated
Capital HealtH 2014 Nursing annual Report 18 Capital HealtH 2014 Nursing annual Report 19
> > N e w k N o w l e d g e , i N N o Vat i o N a N d i m p R o V e m e N t s
lung Ct screening program for High-Risk patients
Among the many 2014 highlights for the Capital Health Center for Oncology was the planning and implementation of the Lung CT Screening Program. The program launched in October 2014 and was the culmination of a year’s worth of planning by a multidisciplinary team.
Why Lung Cancer?
Lung cancer is the leading cause of cancer death in the United States in both men and woman, with more than 150,000 deaths per year and a five-year survival rate as low as 15%. Low-dose CT (LdCT) screening is the only path – outside of never smoking to begin with – that shows significant potential to reduce lung cancer morbidity. based on the findings of the Lung Cancer Screening Trial, the US Preventive Services Task Force (USPSTF) recommends annual lung cancer screening through LdCT screenings. The target population of those at highest risk for developing lung cancer includes current or former smokers, age 55-80 years with a 30-pack/year smoking history. The study’s results revealed that for every 100 screens, one early lung cancer will be discovered. In addition to USPSTF, many other well-respected oncology groups supported this landmark initiative. To support these new guidelines, Capital Health decided to offer the community this important screening tool.
A Nurse-driven Program
The role of nursing in this endeavor was very influential, spearheaded by rona remstein, MSN, rN, director of Oncology Services at Capital Health. Linda Andrzejewski, rN, an experienced oncology nurse volunteered to assist in this endeavor and was selected to be the LCSP’s nurse navigator. Prior to the opening of the program, Ms. Andrzejewski worked closely with the director of oncology services to operationalize the program. As the nurse navigator, Ms. Andrzejewski designed screening intake forms, created educational letters to referring physicians, and worked closely with the radiology department to establish a screening schedule. She also created a tracking system to monitor outcomes and necessary follow-up. The nurse navigator is the first person the patient speaks with to register into the program and meets the patient at the time of the screening. A lung screening nurse navigator was hired to guide patients through the screening process and be a liaison to the radiology department. She worked closely with remstein to operationalize the program by designing screening intake forms, creating educational letters to referring physicians, and working closely with the radiology department to establish a screening schedule. She also created a tracking system to monitor outcomes and necessary follow-up. The nurse navigator is the first person the patient speaks with to register into the program and meets the patient at the time of the screening.
A Good Start
From October through december, 62 individuals enrolled in the program and 43 received a LdCT by the end of the year. Of these, 20% were found to have results that needed further follow-up and one patient was identified with an early cancer. Patients have been referred to the program through a variety of methods. Through the coordination and leadership of our nurses, the objectives of the Lung CT Screening Program were successfully met and a group of interdisciplinary professionals worked together to create a meaningful endeavor.

Capital HealtH 2014 Nursing annual Report 20
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s
New observation units in ambulatory Care
Admission decisions are one of the most costly decisions made in the emergency department on a daily basis. Yet, issues of overcrowding and increased patient acuity have placed immense pressure on making the decision to admit or discharge in an expeditious manner.
The Need for Observation
Observation units are designed to allow for coordinated, structured and high-quality care for select diagnoses. Observation units are considered an extension of the emergency department for the purposes of further assessment, diagnosis and monitoring of patients for up to 48 hours. They have demonstrated improved outcomes while reducing resource utilization through shorter hospital stays and greater care coordination.
Efficient and effective management of the observation status patient can have a significant impact on hospital operations and costs. Studies of observation units demonstrate shorter lengths of stay, fewer inappropriate emergency department discharges, fewer adverse outcomes and lower readmission rates.
Opening Our Units at both Hospitals
In 2014, Capital Health opened observation units at both of its hospitals with focus on the following diagnoses:
nChest pain
nAbdominal pain
nAnemia
nAsthma
nCOPd
ndehydration
nElectrolyte and metabolic derangement
The units are staffed 24/7 with advanced practice nurses (APN), registered nurses (rN), and patient care technicians (PCT).

Capital HealtH 2014 Nursing annual Report 20 Capital HealtH 2014 Nursing annual Report 21
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s
New observation units in ambulatory CareStrengthened by APNs
The APNs function as the licensed independent practitioner who:
nScreens patients referred from the emergency department,
nAssesses patient condition upon arrival to the observation unit,
nOrders diagnostic and laboratory studies,
nPrescribes interventions,
nEvaluates response to interventions,
nCoordinates care with rNs,
nInitiates appropriate consulting physicians, and
nEnsures necessary discharge plans for continuity of care purposes.
In addition, the APN monitors patients’ throughput to ensure efficient and effective outcomes.
This APN model of care has been shown to provide comprehensive, efficient and effective management of patients admitted to our observation units. because the APNs are unit-based, continuity of care is seamless from admission to discharge with the APN being the point person for every aspect of patient care.
For decades, APNs have been recognized as cost-effective providers of high-quality healthcare, while at the same time, being considerably less expensive to train than physicians. research shows that healthcare organizations utilizing APNs as care providers see improved patient outcomes, reduction of healthcare costs and higher financial efficiency. In addition to these direct benefits, APNs also provide mentoring opportunities to rNs and a vital link between nursing and medical teams.
Our beds don’t rest
Eight beds within the Observation Unit at Capital Health Medical Center – Hopewell opened in June 2014 under Medical director Jessica Codjoe, Md; Patricia Michael, MSN, divisional director, Patient Care Services and Alex McConville, bSN, nurse manager. by december 31, 2014, the unit saw 1,187 patients (5.9% of the Emergency department volume) with an average length of stay of 13.5 hours.
Four beds within the Observation Unit at Capital Health regional Medical Center (rMC) opened on October 21, 2014 under Medical director Jessica Codjoe, Md; Lisa McConlogue, Phd, PMHCNS-bC, divisional director, Patient Care Services and deb Lenart, bSN, nurse manager. Volume increased to eight beds on december 22, 2014. by december 31, 2014, the unit at rMC saw 240 patients (1.9% of the Emergency department volume) with an average length of stay of 17 hours. The national average percent of emergency department patients seen in observation is 10%.

Capital HealtH 2014 Nursing annual Report 22
NJ’s first autism-friendly pediatric emergency department
In the spring of 2014, a decision was made to develop an Autism-Friendly Pediatric Emergency department at Capital Health Medical Center – Hopewell by a multidisciplinary team of physicians, neurology subspecialists, nurses and emergency department leadership. Nurse Manager Heather Keller collaborated with Scott Serbin, director of Education and research at Emergency Medical Associates, and developed an educational plan for the Pediatric department staff.
Tactile sensory boxes were created and items were purchased that would meet the sensory needs of this population. The boxes were labeled according to type of sensory (i.e. soft, shiny, squishy). These boxes were placed at the main nurse’s station in the Pediatric Emergency department (Ed), easily accessible to the staff for their autistic patients.
In order to provide communication tools for the autistic child, the nurse manager met with the Information Services department to download an application called Go Talk on to the current iPads that were being used by patients in the Pediatric Ed. In addition, a personalized additional application was installed to enhance Go Talk. This application provides both visual and auditory communication screens for the autistic child: what hurts, communication preference, what I like to talk about, steps that happen in the Ed (e.g. triage, put a gown on).
The interdisciplinary team, in coordination with divisional director of Marketing Strategy & Communications Jayne O’Connor, helped to form a discussion panel of local parents with autistic children. In September 2014, the Pediatric
leadership team, eight Pediatric department staff, Pediatric Neurologists dr. Olga Goldfarb and dr. Mitra Assadi met with five community parents. The main goal of this meeting was to discuss ideas, concerns, and perceptions of an emergency room visit with an autistic child from a parent’s point of view and for the pediatric staff to learn from the parents and their experiences and what their expectations were. It was an eye-opening experience and the conversation was very informational and educational for all who attended.
On October 14, 2014, the Pediatric Ed launched the autism-friendly Ed. In december, a question was added to Wellsoft (the Ed electronic medical record) as to a child being diagnosed with autism. A quarterly audit is scheduled to track if there is an increase of autistic children and their families using the Pediatric Emergency department.
developing this program to meet the special needs of this autistic population has been especially gratifying for everyone involved. The staff support this program and believe that providing this type of specialized medicine increases the quality of care provided each day in, what can be at times, a very stressful environment for both staff and the families for whom they care.
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s

Capital HealtH 2014 Nursing annual Report 22 Capital HealtH 2014 Nursing annual Report 23
NJ’s first autism-friendly pediatric emergency department Computerized physician order entry (Cpoe)
research indicates that Computerized Physician Order Entry (CPOE) has the potential to reduce medication errors, improve legibility, and decrease adverse drug events, thus improving the patient’s quality of care. Many organizations struggle with implementation due to complexity, physician workflow, and extremely robust resources it takes to be successful. The greatest challenges faced are implementation, managing evidence-based order sets, and ongoing maintenance.
The need for CPOE at Capital Health had several drivers:
1) Improve patient safety with clinical decision support.
2) Implement evidence-based practices.
3) Achieve Meaningful Use 1 and 2 requirements.
4) Improve communication among disciplines; quicker turnaround time to ordering and processing within the departments.
Capital Health decided to implement CPOE using a nursing-led approach that would collaborate with physician leaders and champions. barbara Grande, director of Nursing Informatics, formed a multidisciplinary team to evaluate existing workflow for nursing, ancillary departments, and physicians. She educated the team on:
nthe software being utilized for evidence-based order sets,
napproval process required for new order sets to be implemented, and
nthe roll-out process selected.
The team chose to implement in phases, starting with a closed unit that could be closely monitored. The decision was made to start with Maternal Child Health (MCH) (excluding Pediatrics, Newborn and NICU) due to this area currently succeeding with implementing paper evidence-based order sets. The MCH area willingly stepped up to the challenge and two physician champions, along with Kathy donaldson, MSN, APN, C, CPLC, C-EFM and Jill Mahony, MSN, APN, C, rNC-Ob, C-EFM, identified potential areas of weakness, conducted a Failure Mode Effective Analysis (FMEA) with registered nurses and pharmacy staff, and began to focus on evidence-based order sets.
The team established an expedited approval process for order sets. The plan was to work with clinical experts and physician champions to create order sets, have them reviewed and approved by the Obstetrics Section, Informatics Council, and then report up to Pharmacy and Medical Executive Committee. At each phase, the order set was presented by barbara Grande and the physician champions. The goal was to present as a united front and to enhance communication between nursing and physicians. The team developed a structured timeline and was able to successfully go live with 21 evidence-based order sets in February 2014.
As a result of the FMEA, several items were identified as potential patient safety issues and had to be escalated with the vendor to enhance the design. While the software did improve and send clinical decision support notifications to the pharmacy and the provider, a big safety item was identified. The system failed to have direct communication from documentation to the Pharmacy system for pregnant and lactating women. Since the MCH area was selected, this was a critical software item the vendor had to address.
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s
Capital HealtH 2014 Nursing annual Report 24
One of the issues with the existing software was that it did not allow Capital Health to make this a required field, so in order to enhance compliance, a daily report was created to notify the nursing units which patients fit the selected criteria (in this case, pregnant and lactating women) and need to have information entered. Upon initiation, this process did not exist so there was 0% compliance with Pharmacy being notified when a patient was pregnant or lactating.
With new software modifications, Capital Health quickly improved compliance. The project team set the goal for a minimum of 70% compliance within the first six months. Nursing Informatics continues to work with the vendor to make the existing functionality an embeddable data field so it can be required during the admission assessment. The goal will be to have greater than 90% compliance when this is completed. The vendor is targeting early 2016 for this.
After the trial unit (MCH) was completed, the implementation moved to the Mental Health department at Capital Health regional Medical Center. The system was quickly accepted, and the team continues to expand the system and drive compliance.
The CPOE project team selected to implement all Med-Surg, Telemetry, Critical Care and Neuroscience areas in September 2014. Within eight weeks, Capital Health successfully met the Meaningful Use 2 requirements of 60% medications, 30% labs, and 30% diagnostics.
As we continue to implement CPOE and expand order sets, the goal is to keep the focus on evidence-based order sets, improve physician compliance, enhance patient safety and outcomes, and successfully improve workflow for healthcare providers. The way to increase compliance is to develop disease-specific order sets and continue to work with physician champions. As an organization, physician leadership will be engaged in the process and measurable items put into place for reporting purposes.
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s

Capital HealtH 2014 Nursing annual Report 24 Capital HealtH 2014 Nursing annual Report 25
N E W K n o w L e d g e , i n n o vat i o n s , a n d i m p r o v e m e n t s

Capital HealtH 2014 Nursing annual Report 26
>>empirical outComes
2014 Research Highlights
The Capital Health research Council is a core council of the Capital Health professional practice model and partners with the Education and Professional development Council, the Practice Council and the Nursing Quality Council to ensure quality practice that is based on empirical evidence. The research Council exists to promote professional nursing practice through encouragement of scientific inquiry, use of research and literature, and evidence-based practice standards.
Nursing research has led to evidence-based changes in clinical practice at Capital Health. One example is Effects of Oxytocin Administration Checklists on Perinatal Safety (PI: Jill Mahony and deborah Moorhouse). This study resulted in a practice change that became policy for safer administration of oxytocin. The use of pre-oxytocin and oxytocin management safety checklists have been accepted as standard procedure at Capital Health when initiating oxytocin for any induction or augmentation of labor.
Currently, nurses are the principal investigators of 11 Irb (Institutional review board)-approved research protocols at Capital Health. Highlights include The Lived Experience of Nurses who Move to a New Hospital (PIs: Ann L. Curley and barbara Chamberlain) and Primary Postnatal Infant Weight Loss in Conjunction with Baby Friendly Hospital Practices (PI: diane Procaccini).
The moving study used phenomenology, a qualitative research method that helps researchers understand how individuals perceive and make sense of their lived experience. The focus of phenomenology is on the nature of the experience from the point of view of the person who experiences it. This is known as the lived experience. The goal of this study was to describe the lived experience of nurses who move to a new hospital. The results were presented at Capital Health research day in September 2014. A manuscript is being written on the results of the study and will be submitted to a peer-reviewed nursing journal.
The purpose of the postnatal infant study is to determine if baby Friendly practices affect term newborn weight loss. It will also analyze the implementation of evidenced-based maternal/newborn practices to determine if they have decreased hypoglycemic events within the first 96 hours after delivery. Term newborn birth weight, discharge weights, hypoglycemic events and type of birth are being collected for all full-term births that took place at Capital Health for the full year prior to baby Friendly designation (2010) and then compared to the full year after designation (2013). It is hoped that findings from this study provide valuable information on changes related to baby Friendly practices.

Capital HealtH 2014 Nursing annual Report 26 Capital HealtH 2014 Nursing annual Report 27
E m p i r i c a l o u t c o m e s
>>empirical outComes
2014 Research Highlights
Does Blood Collection Technique Have an Effect on Hemolysis Rates?
principal investigator: Cheryl lang, msN, apN, C; CeN
Pediatric Resuscitation-“A to D Resuscitate Me”
The Team Approach: Development and Implementation of a Role Assignment Model in a Community Hospital
principal investigator: margaret “Cookie” estlow, msN, RN, CpeN, pNp-bC
Investigation of Methods to Reduce Hemolysis
principal investigators: Cheryl lang, msN, apN, C; CeN and april lang, msN, apN, C
The Impact of a Nursing-Connection Mentor Program on New Nurse Retention Rates, Professional Growth, and Nurse Satisfaction (dNP Project – dr. Sandra Quinn)
principal investigator: michelina king, phd, RN, Professor, duquesne University, School of Nursing
Co-investigators: sandra Quinn, RN, dNp and ann l. Curley, RN, phd
Evaluation of Patient Anticoagulation Therapy Knowledge and Compliance
principal investigator: ellen Clancey, apN-C
Co-investigator: Valerie sampson, RN, msN
Analysis of Factors Contributing to Heart Failure 30-Day Readmissions at Capital Health
principal investigators: therese prentice, msN, apN-C and donald Haas, md, mpH
Evaluation of the Reliability and Validity of a Tool to Assess Patients with Acute Stroke
principal investigator: Rosemary silva, RN, bsN, CmC, CCRN
Co-investigators: deborah tomaszewski, RN, bsN, msN, CCRN, CNRN and ann l. Curley, RN, phd
Establishing an Anticipatory Model for Anxiety and Depression through a Screening Tool for First Time Radiation Oncology Patients
principal investigator: Rona Remstein, RN, msN
Co-investigator: trish tatrai, RN, ms, oCN, CbCN
The Lived Experience of Nurses who Move to a New Hospital
principal investigators: ann l. Curley, RN, phd and barbara a. Chamberlain, RN, phd, apN, mba, CCRN, wCC
Co-investigators: mary Rosner, RN, msN and deborah tomaszewski, RN, bsN, msN, CCRN, CNRN
ongoing Research at Capital Health

Capital HealtH 2014 Nursing annual Report 28
Psychiatric Nursing Education: Does it Influence View of Psychiatric Nursing as a Career Choice
principal investigator: patricia smyer, phd, RN
Co-investigator: lisa mcConlogue, ph.d., RN, pmHCNs-bC
Primary Postnatal Infant Weight Loss in Conjunction with Baby Friendly Hospital Practices
principal investigator: diane procaccini, msN, RN
Co-investigator: martha goldman, ma, RN
A Study to Improve Patient Satisfaction: Stop, Sit, Speak (PSSST)
principal investigators: april lang, msN, apN, C and ann l. Curley, ph.d., RN
geri san fillippo, msN, RN sCRN
Early Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates the Recovery of FunctionInternational Stroke Conference 2014San diego, CA, February 2014Poster Presentation
Early Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates the Recovery of FunctionNew Jersey State Stroke ConferenceNew brunswick, NJ, April 2014Poster Presentation
barbara grande, msN, RN-bC
Computerized Physician Order Entry, An Organizational Approach. Development to Go-LiveNTT data National Client Conference Nashville, TN, June 2014Presenter
diane procaccini, msN, RN, ibClC
New Jersey Obstetrical & Gynecological Society: Breastfeeding as a Community Health Initiative Atlantic City, NJ, June 2014 Presenter
New Jersey Hospital Association: Maternal Child Health Summit –Baby Friendly Accomplishments and Difficulties Princeton, NJ, June 2014Panelist
Breastfeeding in the African American Community-How We Can Help2014 Children’s Futures Organization for Healthy Newborns and Families, Trenton, NJPresenter
E m p i r i c a l o u t c o m e s
2014 Conferences/presentations/publications

Capital HealtH 2014 Nursing annual Report 28 Capital HealtH 2014 Nursing annual Report 29 capitalhealth.org
Caroline steward, apRN
Capital Health regional Medical Center renal dialysis Services: The CUSP ExperienceNew Jersey Hospital Association: Quality Insights Renal Network 3Princeton, NJ, May 2014 Presenter
Chris saltzman, msN, RNC-NiC
Clinical, Operational & Satisfaction Outcomes After NICU Redesign27th Annual Gravens Conference Clearwater, FL, February 2014Presenter
ann Curley, phd, RN
Introduction to Population-Based NursingUniversity of Massachusetts dartmouth College of NursingFebruary 2014Presenter
kim Coleman msN, apN, C
The Impact of a Nursing Connection Mentor Program on New Nurse Retention Rates, Professional Growth and Nurse Satisfaction2014 ONE research day ConferencePrinceton, NJ, June 2014Poster Presenter
Cupp-Curley, a.l. (2014). Population-based data analysis. In J.S. Fulton, b.L. Lyon, & K.A. Goudreau (Eds.), Foundations of Clinical Nurse Specialist Practice (2nd ed.), (pp. 241-254). New York: Springer Publishing Company.
Greenberg, K., Maxwell, C.r., Moore, K.d., d’Ambrosio, M. Liebman, K., Veznedaroglu, E., sanfillippo, g., diaz, C., & binning, M.J. (2014). Improved door-to-needle times and neurological outcomes when IV-tPA is administered by emergency physicians with advanced neuroscience training. The American Journal of Emergency Medicine, 33 (2015) 234–237.
E m p i r i c a l o u t c o m e s
2014 Conferences/presentations/publications

Capital Health medical Center – Hopewell: Recipients included (from left): Allison Fanelli, rN, bSN, Medical Surgical/Telemetry Nursing; Suzanne Weilminster, rN, Maternal Child Nursing; rosely Kaduthodil, rN, Critical Care Nursing; Jonos Moulic, rN, bSN, Neuro Critical Care; Johanna Castro, rN, bSN, Ed Nursing; Antoniette derricottt, rN, Procedural Nursing; Erin bender, rN, Or Nursing; Elaine O’Connor, rN, Ambulatory Nursing
Capital Health Regional medical Center: From left, front row: Theresa Nixon, rN, bSN, Medical Surgical/ Telemetry Nursing; dianne Paterson, MSN, rNC-NIC, Maternal Child Nursing; Susan rudenstein, rN, Critical Care Nursing; Jolanda Hoegen, rN, bSN, Ed Nursing; dahlia dobson, rN, Ambulatory Nursing; Sharon Laliberte, rN, Psychiatric Nursing; Ann Schnerr, rN, Or Nursing
2014 exCelleNCe iN NuRsiNg pRaCtiCe award Recipients

Capital Health Annual Report: 2014
Background ==========
Capital Health System, Inc. ("Capital Health") operates a multi-hospital healthcare system which provides substantial community benefit through the provision of a comprehensive spectrum of healthcare services to the residents of New Jersey and surrounding communities. Capital Health is recognized by the IRS as an internal revenue code section 501(c)(3) tax-exempt organization. Pursuant to its charitable purposes, Capital Health provides medically necessary healthcare services to all individuals in a non-discriminatory manner regardless of race, color, creed, sex, national origin or ability to pay. Moreover, the hospitals operate consistently with the following criteria outlined in IRS revenue ruling 69-545:
1) Capital Health provides medically necessary healthcare services to all individualsregardless of ability to pay;
2) Capital Health operates emergency departments at both of its hospital campuses;Capital Health Regional Medical Center and Capital Health Medical Center - Hopewell;which are open 24 hours a day, 7 days a week, 365 days per year;
3) Capital Health maintains an open medical staff, with privileges available to allqualified physicians;
4) Control of Capital Health rests with its board of directors; which is comprised ofindependent civic leaders and other prominent members of the community; and
5) Surplus funds are used to improve the quality of patient care, expand and renovatefacilities and advance medical care, programs and activities.
With over a century of service to the greater Mercer and bucks county areas, Capital Health is comprised of 458 beds, employs approximately 4,500 individuals, and generates over 585 million dollars in annual net patient service revenue. Capital Health Regional Medical Center and Capital Health Medical Center - Hopewell are separately licensed acute care hospitals with 237 and 221 beds; respectively.
Capital Health also operates a new kind of healthcare center that puts family physicians and specialists, state-of-the-art technologies, and same-day surgical services all in one location. Capital Health in Hamilton, located at 1445 whitehorse-Mercerville road, and spanning 46,293 square feet, creates a "medical mall" where patients can seek a host of services such as outpatient surgery, radiological testing and specialized care.
The Family Health Center ("FHC") at Capital Health is located at 433 Bellevue Avenue in Trenton. The 14,000 square foot location helps to reduce patient wait time for appointments.
OO3: Attachment 2
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE

In addition to the CH Medical Clinic at the FHC there is also the Henry J. Austin Family Medicine Clinic at the same location, which also provides comprehensive primary care for families, including evaluations and same-day walk-in and sick appointments for adults and children, and patients have access to lower cost prescriptions, social service and patient navigation. Capital Health is guided by its dedication to the healthcare needs of the communities that it serves. That level of determination and commitment is an essential part of the culture at Capital Health. Capital Health provides healthcare services to all people in a non-discriminatory manner, regardless of race, color, creed, sex, national origins or ability to pay. Moreover, Capital Health provides healthcare services to patients who meet certain criteria under its charity care policy, as defined by the New Jersey state attorney general, without charge or at amounts less than established rates. Capital Health maintains records to identify and monitor the amount of charity care it provides. These records include the amount of charges foregone for services and supplies furnished under its charity care policy. Mission Statement ================ Capital Health is committed to providing comprehensive, quality healthcare services, which improve and sustain the health status of the residents throughout Central New Jersey and Lower Bucks County, Pennsylvania. Capital Health assures accessible, compassionate, culturally sensitive and preventative healthcare services that respect individual dignity. Capital Health addresses the region's evolving healthcare needs by providing comprehensive care including education, prevention, disease management and restorative health programs. Awards and Recognition ===================== Capital Health has received the following awards and recognitions: - Joint commission advanced certification for comprehensive stroke center (RMC) - Joint commission disease specific certification for acute stroke (CHMCH) Magnet Re-designation --------------------- The American Nurses Credentialing Center ("ANCC") has recognized Capital Health's exemplary nursing leadership and quality patient care by awarding its magnet recognition for excellence in nursing service. Magnet status is the highest level of recognition the ANCC can extend to a healthcare organization. Capital Health has earned this recognition three times, consecutively.

2014 Awards and Accreditations ------------------------------ Capital Health Medical Center-Hopewell was named a 2012 top performer on key quality measures by the joint commission for exemplary performance in using evidence-based processes to improve care for stroke, heart attack, heart failure and surgical care. Our Marjorie G. Ernest joint replacement center of excellence at Capital Health Medical Center-Hopewell received disease-specific care certification for total joint hip replacement from the joint commission. Capital Health Regional Medical Center was one of the first two hospitals in New Jersey to receive advanced certification as a comprehensive stroke center from the joint commission. The Bristol-Myers Squibb Trauma Center at Capital Health Regional Medical Center was reverified as a level ii trauma center by the Committee on Trauma (COT) of the American College of Surgeons (ACS). Comprehensive center for breast care was accredited by the National Accreditation Program for Breast Centers (NAPBC). Chest pain center accreditation from the society of cardiovascular patient care (SCPC). Regional Medical Center became the only hospital in New Jersey and only 1 of 6 in the country to earn a 2014 commitment to excellence award for patient experience from press Ganey Associates., Inc. Capital Health launched New Jersey's first "autism-friendly" pediatric emergency room. Accredited with commendation by the American College of Surgeons Commission on Cancer. Accreditation by COC is given only to those facilities that have voluntarily committed to providing the highest level of quality cancer care and that undergo a rigorous evaluation process and review of their performance. Capital Health earned the American Heart Association/American Stroke Association's "get with the guidelines" stroke gold plus performance achievement award. The American College of Radiology (ACR), an organization focused on the practice of radiology and the delivery of comprehensive health care services, designated Capital Health as a breast imaging center of excellence for earning four national accreditations in mammography, stereotactic breast biopsy, breast ultrasound and ultrasound-guided breast biopsy. Joint Commission's Gold Seal of Approval ----------------------------------------
The joint commission is an independent, not-for-profit, national body that oversees the safety and quality of healthcare and other services provided in accredited organizations. By awarding Capital Health their gold seal of approval, the joint commission confirmed that Capital Health improved the accuracy of patient identification, improved the effectiveness of communication among caregivers, and improved the safety of using medications. In addition, the joint commission confirmed that Capital Health reduced the risk of healthcare-associated infections, accurately and completely reconcile medications across the continuum of care, reduced the risk of patient harm resulting from falls, encouraged patients' active involvement in their own care as a patient safety strategy, and Capital Health identified safety risks inherent in the patient population. Statement for Community Health Improvement & Benefits ===================================================== To promote wellness, prevent illness, and remove barriers that hinder access to healthcare by working hand-in-hand with the communities served. Principles ---------- - Capital Health believes that community health improvement is essential to the Capital Health mission. - Capital Health believes community-based coalitions are uniquely qualified to achieve community health goals and Capital Health values partnerships with them. - Capital Health values evidence-based practices and seeks to model excellence in community health practice based on evidence. - Capital Health believes in applying continuous quality improvement to community health: measuring need, matching resources to need, measuring outcomes and making adjustments in processes. Operational values ------------------ Integrity: adheres to an appropriate and effective set of core beliefs including honesty and serving the greater good. Does not blame others for his or her own mistakes or misrepresent himself or herself for personal gain or protection. Perceived by others as a direct, truthful individual and is widely trusted, with the ability to present the truth in an appropriate and helpful manner. Excellence: provides the most efficient and effective work processes to meet the needs of patients and other customers, which leads to the highest quality services. Makes

sound decisions based upon knowledge, judgment, and experience, and is sought out by others for advice and solutions to issues and problems. Compassion: demonstrates caring and concern for the welfare of others, assisting wherever necessary. Uses understanding and insight when dealing with patients or other customers in all aspects of care or service delivery. Teamwork: displays a professional and collaborative spirit in fulfilling responsibilities and assisting others. Helps to create and maintain positive morale with his or her team, sharing in successes, working through problems. Fosters open dialogue and works towards creating an atmosphere where outcomes and success are beneficial to the team and/or the organization at large. Vision ------ Capital Health will be the premier community-based healthcare provider in Central New Jersey and Lower Bucks County, PA. Capital Health will constantly strive to maintain the highest professional standards, exceed expectations of those served and to promote a positive work environment. Capital Health's success will be built upon caring, compassion, creativity, integrity, respect, service, and teamwork. Capital Health's services will support the physical, emotional and psychological health of their communities. Service Culture Initiative -------------------------- Capital Health is dedicated to high quality performance, and to exceeding customer expectations within a supportive and friendly environment. Each employee has a responsibility and is accountable for providing optimum satisfaction to the patients and their families, physicians and coworkers. Service Culture Initiative Vision Statement ------------------------------------------- - Capital Health commits to the needs of the communities served. Through excellent service and care, Capital Health achieves successful patient outcomes. - Capital Health adheres to a standard of positive behavior. This must include positive first impressions, appropriate communication, professional appearance and the realization that they are dealing with people's lives. - Capital Health creates an environment conducive to positive relationships. By engaging employees in a partnership of teamwork, Capital Health is reinforcing their commitment to trust and respect.

- Capital Health is proactive rather than reactive. By having efficient and effective systems, Capital Health improves quality care and service delivery. - Capital Health accepts the challenge of service culture improvement as a business strategy. It is not only the nice thing to do, but the right thing to do to assure the growth of Capital Health. - Capital Health recognizes excellent service culture performance. Featured Services ================= Diabetes Services ----------------- Diabetes education at Capital Health is an outpatient comprehensive referral based diabetes education program that empowers patients to take control in the successful management of their disease. Capital Health's education model, where the patient is the central player, is widely recognized as the best model to use to help the patient achieve optimal health related outcomes. Capital Health works closely with primary care physicians who continue to monitor each individual's medical problems. Trauma and Emergency Services ----------------------------- The Bristol-Myers Squibb Trauma Center, the level ii trauma center at Capital Health regional medical center, is one of only 10 state designated trauma centers in New Jersey. Capital Health provides comprehensive care from the time of injury through rehabilitation. The trauma center meets high national standards for patient care and teaching. The designation process involves detailed regular inspections by national and state organizations to assure high standards of care. Capital Health is the regional referral center for injured patients in Mercer county and adjacent parts of Somerset, Hunterdon, Burlington, and Middlesex counties as well as nearby areas of Pennsylvania. Designated trauma centers care for severely injured patients as well as victims of accident types known to be associated with a high risk for injury. Trauma patients include persons involved in motor vehicle crashes, falls, and assaults with knives, guns, or blunt objects. Trauma centers have the latest technology and experienced staff available to care for your family member. Besides providing care to the injured, trauma centers are also active partners with the community in injury prevention and public education. Maternity --------- From routine deliveries to high-risk needs, Capital Health's great expectations program provides a full range of prenatal, obstetrical, postpartum, and neonatal care options to

make sure your new family has the greatest chance for a healthy beginning. The maternity unit at Capital Health medical center - Hopewell is Mercer county's only regional perinatal center and level iii neonatal intensive care unit. The Capital Health healthstart maternity program located at the FHC in Trenton provides care to over 1,000 pregnant women annually. Capital Health is the only healthcare provider in the region to have in-house coverage by obstetricians, midwives, neonatologists, and anesthesiologists 24 hours a day, seven days a week. And, Capital Health was chosen as New Jersey's first site to house a march of dimes family support program. The program provides information and emotional support to families of critically ill newborns being cared for in the neonatal intensive care unit. Also, comprehensive childbirth and parent education services are offered to help prepare individuals to be the best parents possible by teaching about the process of birth and how to care for their infants. Lactation Services ------------------ In 2012, Capital Health medical center-Hopewell was designated as a baby friendly hospital, the second hospital in New Jersey to attain this status. As a baby friendly hospital, Capital Health focuses on the entire obstetric population. In 2013, Capital Health demonstrated an overall 82 percent breastfeeding initiation rate and a 57 percent average exclusive breastfeeding rate. Exclusivity for breastfeeding mothers only was higher at an average 66 percent rate. Capital's healthstart clinic patient population breastfeeding rates were comparable to the overall obstetric population due to additional educational programs and one-to-one support with increases in services including prenatal group centering and collaborative efforts between Capital Health and specific community organizations directed toward this vulnerable population. Focused programs such as children's future and women's infants and children (WIC) have been instrumental to its demonstrated success. Institute for Neurosciences --------------------------- The Capital Institute for Neurosciences, has advanced the level of care available to patients in the region. Providing comprehensive, state-of-the-art diagnostics and treatments for a wide range of medical conditions involving the brain, spine and nervous system, the institute's highly trained and specialized physicians utilize cutting edge technology to deliver outstanding care. Physicians include board-certified and fellowship-trained specialists, and among them are dual-trained neurosurgeons treating patients using both endovascular and traditional neurosurgical approaches. At the institute, patients benefit from a multi-disciplinary team of specialists which can include neurologists, neurosurgeons, and other specialized physicians, as well as

anesthesiologists, physician assistants, critical care nurses, nurse anesthetists, speech pathologists, technicians, physical and occupational therapists, social workers, and other critical team members who provide an outstanding continuum of care from diagnosis to treatment and recovery at Capital Health. The institute includes many specialized centers of care. Among the conditions treated: - Stroke and transient ischemic attacks - Carotid stenosis - Aneurysm - Arteriovenous malformations (AVMS) - Chiari malformations - Traumatic brain injury - tumors of the brain and spine - both malignant and benign and including schwannomas, meningiomas, neurofibromas, pituitary, pineal, skull base, gliomas and others - Spinal diseases and injuries - such as herniated discs, spondylolisthesis, spinal compression fractures and spinal vascular malformations - Degenerative diseases and spinal trauma - Neurologic conditions including dementia, muscle and movement disorders, nerve disorders and headaches - Movement disorders, Parkinson’s, essential tremor, atypical Parkinson’s (multisystem atrohy, progressive supranuclear palsy, and corticobasilar degeneration), dystonia, ataxia and spasticity - Pediatric neurology, including developmental delays, autism, neurometabolic and genetic disorders, and attention deficit disorders - acute and chronic pain, including pain from spinal stenosis, nerve disorders, cancer, fibromyalgia, sciatica, migraines, trigeminal meuralgia, myofacial, shingles and other conditions - Epilepsy - Movement limitations due to stroke, arthritis, injury, amputation, or other conditions Center for Digestive Health --------------------------- The Capital Health Center for Digestive Health is advancing the level of care available to patients in the region by providing comprehensive, state-of-the-art diagnostics and treatments for a wide range of medical conditions involving the entire digestive system all in one location. The center's highly trained and specialized physicians utilize cutting-edge technology to deliver outstanding care. The center's medical director is a fellowship-trained and board-certified gastroenterologist with years of experience who helps patients and their referring doctors navigate the center and access the appropriate specialist or surgeon for the advanced testing or care required. The center's medical staff includes the region's pre-

eminent medical expert in interventional gastroenterology and therapeutic endoscopy, who has unmatched experience using advanced diagnostic techniques such as Endoscopic Ultrasound (EUS) and non-surgical treatments such as Endoscopic Retrograde Cholangiopancreatography (ERCP), Radiofrequency Ablation (BARRX), Endoscopic Mucosal Resection (EMR), and Enteral Stent Placement. The center also recently welcomed a specialist in irritable bowel diseases, such as Chron's and colitis. If surgery is an option, the center has direct access to a roster of highly trained laparoscopic (minimally invasive) surgeons, including the area's only hepatobiliary surgeon who specializes in advanced laparoscopic procedures of the liver, pancreas, and bile ducts. Center for Oncology ------------------- Capital Health has consistently offered patients a closely integrated team of medical, surgical, radiation, and allied cancer specialists who use their knowledge and experience to provide cutting-edge cancer treatment close to home. When one chooses Capital Health for cancer care, one selects board certified physicians who remain with the patient from diagnosis through treatment. Working together, Capital Health offers a compassionate approach to assist patients with every aspect of cancer care, including screening, diagnosis, treatment, recovery, and survivorship. The Capital Health, Center for Oncology is committed to providing comprehensive quality oncology healthcare services, to help improve and sustain the health status of residents living primarily in central New Jersey and lower bucks county. Capital Health strives to improve and extend the quality of life for the patient with cancer. The center for oncology is a leader in defining the community's cancer care needs by providing appropriate plans through a comprehensive continuum of care, which includes education, prevention, screening, diagnosis, treatment, clinical research, symptom management, supportive care and survivorship programs. Capital Health's success is built upon care, compassion, creativity, integrity, respect, service, state-of-the-art technology and multidisciplinary teamwork. The center for oncology is accredited by several esteemed bodies: * American College of Surgeons - Commission On Cancer * National Accreditation Program for Breast Centers (NAPBC) * American College of Radiology - Radiation Oncology Department * American College of Radiology - Imaging Center of Excellence Capital Health provides the most comprehensive lung screening through low dose cat scans and cancer treatment program in the region. This screening program is offered to patients at risk of developing lung cancer, those with a heavy smoking history. This includes cutting edge diagnostics, specifically their extremely low-dose 128- and 256-

slice CT scans. There is no contrast involved and no blood tests required, therefore, no needles are used. Capital Health physicians are licensed to offer a new FDA-approved treatment to patients with colorectal cancer that has metastasized to the liver. The Selective Internal Radiation Therapy (SIRT) is a proven technology for inoperable liver cancer that delivers doses of radiation directly to the site of tumors. The Capital Health's radiation oncology department recently added high dose radiation therapy (HDR) as one of its radiation options for oncology patients. HDR offers oncology patients an additional treatment option as it differs from traditional modalities. HDR treats cancer by placing radioactive sources directly into or next to the cancer. This enables clinicians to deliver a high dose with minimal impact to surrounding healthy tissues. HDR has proven to be a successful treatment for cancers of the prostate, cervix, endometrium, breast, skin, bronchus, esophagus, head and neck, and soft tissue sarcomas. At Capital Health, we plan to use HDR to treat all sites. Pediatrics ---------- Capital Health medical center - Hopewell is home to the only in-patient pediatric unit in Mercer Capital Health's pediatric emergency service is completely separate from the adult emergency department and is staffed by pediatric specialists. The pediatric hospitalist program gives pediatric patients and their physician's around-the-clock access to in-house pediatricians and pediatric trained nurses. Pediatrics is also provided for trauma patients at RMC. Radiology services ------------------ Capital Health has an abundance of the most state-of-the-art radiology services in the region. As the region's leader in diagnostic and treatment technology, Capital Health offers full-time, onsite PET scan technology and was the first hospital in the country to offer a molecular breast imaging device at Capital Health medical center-Hopewell. Full-service imaging suites at Capital Health locations boast the most advanced equipment available, including low dose, multi-slice dual energy CT scanners and large bore magnetic resonance imaging (MRI) machines that features the shortest high-field magnet in the industry ranging from a 1.5 to a 3.0 tesla and functional MRI capability. Sleep Center ------------ Capital Health has been providing comprehensive evaluation and treatment for sleep related problems for more than 20 years and Capital Health was the first provider in

Mercer County. At the present time, Capital Health is the largest fully accredited sleep center in Mercer and bucks counties. Between both campuses, Capital Health offers fourteen private rooms dedicated to sleep testing for patients who have a wide variety of problems related to sleep and wakefulness. In addition, Capital Health is the only area facility equipped to perform neurological monitoring for complex conditions such as nocturnal seizures. As sleep centers fully accredited by the American Academy of Sleep Medicine, Capital Health ensures that all patients treated at Capital Health benefit from a complete sleep evaluation and individualized treatment plan. Dialysis -------- Since 1970, the Capital Health renal dialysis services has been the only hospital owned and operated dialysis program in the area. The main objective of the service has been to deliver safe, effective treatment to patients with acute and chronic kidney failure in accordance with federal, state and joint commission regulations. Consisting of 28 hemodialysis and 3 home training stations, this pleasant, state-of-the-art facility provides inpatient and outpatient hemodialysis and peritoneal dialysis services. Our home program offers patients the opportunity to be educated in self-care to perform either dialysis modality in the home setting. It is the commitment of the service that no patient will be denied acceptance because of age, national origin, physical handicap, race, religion, sex or inability to pay. Also, all patients in the service are entitled to any and/or all ancillary services provided by Capital Health. Other needed services, not directly provided by Capital Health, are made available through a referral process. Treating diseases of the kidney require the right team to help the patient maintain his/her maximum level of health and activity. Our highly educated and experienced healthcare team, led by a medical director board certified in nephrology, also includes a director of renal dialysis, renal nurse manager, nephrology advanced practice registered nurse, renal clinical nurse specialist, registered and licensed practical nurses, dialysis patient care technician, renal dietitians and renal social workers. This team has successfully met the centers for Medicare & Medicaid services end stage renal disease quality incentive program goals since their inception. These goals were established to improve patient care by setting performance standards for quality of care. Definition of Community and Population Served --------------------------------------------- Capital Health defines its community as the city of Trenton, Mercer County and parts of Burlington, Monmouth, Middlesex and Bucks Counties. While it was once a center for industry in the late 1800's and early 1900's, Trenton has seen dramatic economic development challenges over the years. According to the 2010 U.S. census, its median

household income was $36,727, by far the lowest in Mercer County. Based on a population of 84,349, Trenton also has the highest number and percentage of minorities in Mercer County with a predominantly African-American population of 43,861 residents or 52.0 percent. Hispanics or Latinos of any race constituted 28,425 residents or 33.7 percent, while Caucasians were numbered at 22,436 or 26.6 percent. Community Benefits Programs =========================== Outlined below are a number of Capital Health community benefit programs. The information is not intended to be all-inclusive but rather provides additional information that further demonstrates how Capital Health benefits the surrounding community in furtherance of its charitable tax-exempt purposes. Capital Health Childbirth and Parent Education Program ------------------------------------------------------ Benefit Activity: Prepared Childbirth Classes in Spanish Language The childbirth and parent education program provides, free of charge, a full-day prepared childbirth class to Spanish-speaking expectant parents from their community. The class is held every other month and is taught by a Capital Health certified childbirth and parent educator who is fluent in Spanish. Culturally appropriate methods and audio-visual materials are utilized in the teaching of this class. Participants receive free breakfast and lunch. Participants receive Spanish language reference materials and an extensive handbook. Referrals to this class come from the Capital Health, health start prenatal clinic, a community partnership with CUNA, and by word-of-mouth. Trauma education ---------------- The Bristol-Myers Trauma Center at Capital Health Regional Medical Center offers free injury prevention programs to members of the community that include pedestrian safety, bicycle safety, seat belt safety, proper use of child safety seats, and home safety. Connecting with the Latino Community ------------------------------------ Enlace ("link" in Spanish) is a name for an innovative Capital Health program designed to create contacts and connections within the Latino community. Through enlace, Capital Health provides medical interpreting and has translated all vital medical documents and are now doing the same with patient education materials. Enlace also helps educate the Latino community about American customs and healthcare practices and provides Capital Health staff with information about Latino cultures. Another program, CUNA (which is Spanish for "crib"), connects Latino women with pre- and post-natal care, and helps new mothers overcome language barriers to better

understand health issues. Cuna also offers help with nutrition, coping skills and even babysitting for older children. Dsrip: Childhood Obesity ------------------------ Capital Health has partnered with the school district of Trenton and another local elementary school to develop, implement and provide a program to reduce the epidemic of childhood obesity in the region. The program has two aims: to instill an appreciation for healthy eating and active lifestyle in the impressionable child, and to reorient their parents to follow a similar path. We believe that a partnership and linkage must occur so that the child and parent see healthy eating and activity as a family activity. Therefore, while we focus directly on programs for the children, we have concurrently developing a tight linkage with education, weight monitoring and exercise inducement for the parents. The program's model follows the process outlined in shaping New Jersey and in serving up health, involving teaching children and their parents the basics of healthy eating and performance of daily aerobic exercise and monitoring of BMI. Dsrip: Substance Abuse ---------------------- Throughout our healthcare system, our staff sees a large number of individuals with substance abuse disorders and has developed an awareness of the impact of this health issue on other medical conditions. While Capital Health's dsrip substance abuse program seeks to improve the care of the patient with alcohol withdrawal syndrome by identifying the diagnosis in the early stages and prevent its progression into delirium tremens, capital's certified alcohol and drug abuse counselors focus on connecting diagnosed patients with post-acute substance abuse providers so that they can receive treatment and prevent recidivism. Community Health Education -------------------------- Capital Health's community health education program is dedicated to improving the health and well-being of the community, as well as to the prevention and early detection of disease among people living in our community. These goals are accomplished by providing health education and other related services to the general public, as well as to business organizations. These services consist of the speaker's bureau, health fairs/health screenings, health education lecture series and support groups. Programs are held in various locations throughout Mercer and bucks counties, with topics including diabetes education, peripheral vascular disease awareness, healthy eating, cancer genetics, and women's health issues and more. The community health education program provides a series of diverse health education programs, related to health maintenance, disease prevention, early detection, general wellness and personal development. A schedule of the programs, screenings and

support groups currently open for registration may be viewed online at:www.capitalhealth.org/events. Community Sponsorships ---------------------- Capital Health is proud to sponsor many local organizations in Mercer and bucks counties through in-kind and monetary donations. Capital Health supports a variety of civic and cultural organizations that work to improve the wellbeing of the community. Conclusion ---------- Capital Health is a non-profit organization that has an "open door" policy. This policy means that Capital Health provides necessary basic hospital care to everyone, regardless of their ability to pay for their care. Capital Health is committed to community outreach and education, offering numerous heath care related programs and activities, including community health fairs, health screenings, health education and medical lectures and seminars annually. Capital Health is proud of their many partnerships with local organizations. To further show how Capital Health is committed to benefiting its community, Capital Health, in November 2011, opened its $530 million 223-bed hospital in Hopewell Township, New Jersey to replace its existing facility, Capital Health - Mercer, in Trenton, New Jersey. In addition, Capital Health Regional Medical Center in Trenton underwent a complete renovation. Capital Health obtained a mortgage loan through the federal housing administration which enabled it to lower its cost of credit. This will allow Capital Health to use more of its resources to serve the medical needs of its community.
QUALITY & PATIENT SAFETY PLAN 2016
Hopewell & Regional Medical Center Approved: Board Quality and Safety Committee 3/9/15, 1/18/16
OO3: Attachment 3
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE

2
Purpose The Capital Health (CH) Quality and Patient Safety Plan aligns daily operations with the mission, vision and values of the organization to achieve excellence in clinical outcomes and patient satisfaction. The path to achieving the quality and patient safety initiatives involves defining and deploying high-impact innovations. The goal of excellence in clinical practice is measured by improvement in desired patient outcomes and excellence in organizational performance. The purpose of the Quality and Patient Safety Plan is to create an integrated structure that clearly defines the Capital Health’s approach to provide exceptional service, compassionate care, and high levels of safe patient care can be provided for every patient in every setting and service. The six aims of quality as published by the Institute of Medicine (IOM) in Crossing the Quality Chasm in 2001 provide the framework for the quality and patient safety plan reporting. To achieve the overall objective to improve patient-centered outcomes, the performance improvement program promotes processes that are reliable, decreases variation and defects (waste), focuses on the achievement of better outcomes, and uses evidence to ensure that service is satisfactory. Because patient safety is a central aim of quality, leadership supports a safety culture that validates methods to improve processes and systems, standardizes ways for interdisciplinary teams to communicate and collaborate, and safely integrates technology. Leadership promotes learning, motivates staff to uphold a fair and just safety culture, provides a transparent environment in which quality measures and patient harm are freely shared with staff, models professional behavior, removes intimidating behavior that might prevent safe behaviors, and provides the resources and training necessary to take on improvement initiatives. Transparency, accountability and mutual respect are valued. This plan outlines the aims, key performance indicators, organizational leadership structure and strategies used to interpret data, plan for improvement, and communicate need for change thereby sustaining performance resulting in high reliability and patient safety. Although the Quality and Patient Safety Plan provides the structure and the specific priorities are set annually, changes can be made at any time as new information from benchmarks, or changing trends are noted. All hospital and medical staff have the ability to request a reevaluation of priorities or process. In addition, Capital Health encourages the reporting of all patient safety events, near misses and unsafe conditions. All patient safety events are reviewed, investigated and trended. A consistent procedural framework is utilized by the Patient Safety Committee to facilitate an intensive assessment and analysis of adverse and sentinel events. A comprehensive systematic analysis identifies the causal and contributing factors associated with the event.

3
Framework for Quality
The Quality and Patient Safety Plan is designed to achieve outcomes identified by the Institute for Healthcare Improvement (IHI) triple aim to improve quality, cost, and value. Capital Health is committed to understanding our most productive opportunities to plan for higher value, and drive cost optimization through quality improvement with measures and metrics. By removing waste, harm, and variation, CH works to prioritize the most impactful interventions and methods to improve quality and reduce costs. The Institute of Medicine six aims of quality is utilized as the basis for reflecting activities and reporting:
1. Safe: Avoiding preventable injuries to patients from care that is intended to help them; reducing medical errors
2. Effective: Providing services based on scientific knowledge and evidence-based guidelines to all who could benefit and refrain from providing services to those not likely to benefit
3. Patient-Centered: Improving the overall care experience that is respectful and responsive to individual patient preferences, needs and values
4. Timely: Reducing wait times, improving the patient flow to promote accessibility 5. Efficient: Appropriate resource utilization by avoiding wasting time and other resources 6. Equitable: Providing quality and safe care that is consistent care regardless of patient
characteristics and demographics.
Key Performance Indicators
1. Maintenance and growth of accreditation, certifications, and third party recognitions 2. Promotion of patient participation and satisfaction with care and service 3. Promotion of staff engagement and retention 4. Promotion of a culture of safety and accountability to reduce variation, reduce risk and improve
quality. 5. Optimization of resource utilization and evidence-based practice to prevent penalties by CMS
a. Value based purchasing b. Readmission c. Hospital acquired conditions/ Hospital acquired infections d. Meaningful use
6. Participation in regional, state, and national quality and patient safety initiatives a. New Jersey Hospital Association Hospital Engagement Network (HEN) b. Quality Innovation Network – Quality Improvement Organization (QIN-QIO)
Organizational Leadership and Reporting Structure All members of CH are responsible for promoting safety and participating in quality initiatives. The Board of Directors (BOD) bears the ultimate responsibility for ensuring the quality of patient care services. The Board designates the Board Quality and Safety Committee to provide oversight and direction in setting the mission, vision, values, and strategic goals to support the culture of quality, safety and performance improvement.
4
The Management Team accepts personal accountability to ensure important internal processes and activities throughout the organization are systematically measured, assessed, and improved through implementation of the annual Quality and Patient Safety Plan. The Management Team allocates resources for assessing and improving the organization’s leadership, clinical and support services, analyzes and assesses the effectiveness of quality activities, and creates procedures for responding to system or process failures. The Management Team sets the organizational line-of-sight to unify efforts and afford a common goal. Annually, the Management Team reviews system or process failures, sentinel events, and activities to prioritize projects for the Quality and Patient Safety Committee in preparation for the next year. The Medical Executive Committee (MEC) is responsible for the ongoing quality of medical care provided by practitioners with clinical privileges. MEC provides leadership and participations in quality activities including professional practice evaluation. The MEC conducts quality activities and reviews data regarding implementation of evidence-based practices, utilization of resources, hospital acquired conditions, maintenance of medical record documentation, compliance with medical staff indicators, and quality & patient safety indicators to identify trends as potential opportunities for improvement. The Quality and Patient Safety Council, an interdisciplinary committee of the Hospital, has oversight to hospital-wide quality and patient safety initiatives. The Council evaluates aggregate performance data and quality outcomes, and makes recommendations to the BOD Quality and Safety Committee, the Management Team and MEC on indicators/measures for prioritization and review. The Quality and Patient Safety program’s effectiveness is documented in an annual report that is used by the BOD Quality and Safety Committee to recommend the annual Quality and Patient Safety Plan. The Patient Safety Team promotes a culture of safety within the organization by encouraging reporting of all occurrences ranging from near misses to adverse occurrences. Membership is from all clinical areas with representation of staff and leadership along with representation from the Quality/ Safety Department. Accountabilities include monitoring established metrics including National Patient Safety Goals, identifying risk reduction activities, implementing strategies to promote a culture of safety, and educating on organization-wide change. As per the New Jersey Patient Safety Act, an ad hoc Patient Safety Committee comprised of staff with knowledge of the event, and other medical, clinical and quality leaders review all adverse events to identify and resolve system and practice issues that may impact quality and patient safety. The Committee members have the competencies to conduct analyses of adverse events including near-misses, with particular attention to serious preventable adverse events to reduce the probability of recurrence through the application of evidence-based practices. The Patient Care Services Performance Improvement Committee coordinates and oversees Nursing performance improvement activities. Membership is from all areas of nursing, with equal representation of staff and educators. Each clinical department reviews the monthly Unit-based Quality Report to assess performance and identify opportunities for improvement. Data is collected using tracer methodology, chart abstraction, and performance improvement initiatives
5
allowing for education of staff. Accountabilities include monitoring unit-based quality reports, evaluation and recommendations related to structure, process and outcome measures. The Environment of Care Committee (EOCC) is an interdisciplinary committee with representatives from clinical, administrative, and support services responsible for promoting a safe, functional, and supportive environment within the hospital so that quality and safety are preserved. This committee stresses the importance of managing risks in the environment of care, which are different from the risks associated with the provision of care, treatment, and services. Representatives from clinical, administrative, and support services participate in the analysis of environment of care data and use the results of the data analysis to identify opportunities to resolve environmental safety issues. The EOCC is made up of teams representing safety, security, hazardous materials & waste, life safety, medical equipment, utilities, and emergency preparedness. Each of these teams is required by the Joint Commission to develop a written plan that manages these areas. These plans are reviewed annually, including a review of the the plan’s objectives, scope, performance, and effectiveness.
Methodology and Communication Strategies Using robust performance improvement methods and data from quality and patient safety initiatives, leadership assesses structures, processes and outcomes to develop plans that prioritize improvement initiatives. Areas needing improvement are communicated to the entire healthcare team. A rapid cycle improvement (RCI) methodology is employed to charge a team to develop an implementation plan including education and barriers identification; and to propose a methodology for data collection to assess compliance with the performance change. RCI Teams are chartered at all levels of the organization including unit-based and organization-wide. The Quality and Patient Safety Council charters the organization-wide RCI Teams to address broad based clinical, operational, and leadership processes. The primary methodology used for performance improvement is rapid cycle improvement utilizing PDCA (Plan-Do-Check-Act). A team or an individual can use other valid methodologies whenever the situation warrants. Through PDCA, knowledge of how a process is currently performing to meet customer needs and expectations is used to plan and test process changes. The purpose of these process changes is to improve the outcome. CH incorporates safety practices using risk assessment methodology such as Failure Mode and Effects Analysis (FMEA) or other Joint Commission methodologies to evaluate a process prior to implementation to prevent introduction of harm. Capital Health is committed to identifying organization-wide opportunities to improve care annually, and utilizes methodologies such as Failure Mode and Effects Analysis, Root Cause Analyses and Rapid Cycle Improvement Teams. The identified team utilizes a systematic, proactive method for evaluating a process to identify where and how it might fail and to assess the relative impact of failures, in order to identify the parts of the process that are most in need of change and reduce the likelihood of experiencing an adverse event. This proactive approach to patient safety identifies actionable common causes, avoids unintended consequences, identifies commonalities across departments/ services/ units, and identifies system solutions.

6
Root cause analysis (RCA) focused on systems is performed on all adverse events to identify cause(s) and design a risk-reduction program. RCAs are conducted when appropriate and charged by the Patient Safety Committee.
External Reporting
CH complies with all mandatory reporting of safety events to the State of New Jersey Department of Health (NJDOH), and reports clinical quality metrics to the Centers for Medicare and Medicaid Services (CMS), The Joint Commission (TJC), NJDOH, and NHSN (CDC). CH participates in voluntary reporting for Disease-specific Certification to TJC, The American Heart Association (Get with the Guideline Projects), the New Jersey Hospital Association Hospital Engagement Network, and the Leapfrog Group to promote quality and safety, and reduce adverse events.
Patient Safety Evaluation System The Patient Safety Evaluation System supports the implementation of best practice, redesign of faulty systems, transformation of culture and documentation of progress. Essential to producing safe care with quality outcomes is the organization-wide adoption of a Just Culture.
• Best practice is scientifically based and focused on high reliability including an understanding of risks, benefits and alternatives to treatment.
• Effective teamwork and communication in complex systems is required and necessary to improve the system.
• Incorporating mindful frontline provider in operational decisions demonstrates cultural transformation.
• Open communication between staff and patients surrounding errors defines opportunities for education and improvement.
Patient Safety Work Product All data, reports, memoranda, analyses or written/oral statements that could improve patient safety, healthcare quality or health care outcomes are privileged and confidential. Each patient safety work product is clearly labeled as “Confidential”. Patient Safety Work Product (PSWP) is retained separate from the patient’s medical record and documentation includes:
1. Events, near misses or unsafe conditions 2. Hospital acquired conditions, including infections 3. Peer review 4. Root cause analyses or other risk assessment

7
5. Quality improvement and performance improvement projects: structure, process or outcomes
Patient Safety Work Product may be used internally by the Medical Staff Professional Practice Committee ,
Patient Care Services Performance Improvement Committee, the Quality and Patient Safety Committee, the Patient Safety Committee/Team, and/or Continuing Medical Education Committee to raise awareness and educate on faulty systems and/or processes.
Confidentiality and Security
All activities of the Quality and Patient Safety Committee, and the respective committees and task forces, are performed with the purpose of performance improvement. Minutes and other work products are protected under the New Jersey Patient Safety Act of 2004 and the Health Care Quality Improvement Act of 1986. The information and recommendations generated by these bodies are therefore considered privileged.
CY2016 Priorities for Quality and Patient Safety Optimize resource utilization and clinical outcomes to eliminate CMS penalties for Value Based Purchasing, Readmissions, Hospital Acquired Conditions, and Meaningful Use by participating in CMS and Joint Commission quality initiatives. Participate in external Quality & Patient Safety Initiatives to improve clinical outcomes with Sepsis, Hospital Acquired Conditions, Hospital Acquired Infections, and Readmissions. Continue initiatives to improve Patient Experience in the inpatient and outpatient areas. Improve patient and family engagement through participation in committees and focused groups. Improve Patient Safety Culture through staff engagement in patient safety education programs and patient safety initiatives. Maintain The Joint Commission accreditation readiness, compliance and disease certifications. Pursue opportunities for Awards and Recognition.
8
COMMITTEE STRUCTURE TO SUPPORT QUALITY AND PATIENT SAFETY Committees lend experience and expertise in promoting the organizational culture of patient safety and performance improvement, evaluating clinical quality of care, and monitoring the organization-wide performance improvement and patient safety activities.
Board Quality and Safety Committee
Purpose: The Board Quality and Safety Committee oversees the quality and safety on behalf of the Board of Directors to assure the that there are appropriate and effective systems in place that cover all aspects of clinical quality and safety at Capital Health System Objectives:
• Facilitates the creation of a high reliability, cost-effective, and efficiently run healthcare system which promotes quality and safety through the proactive management of hospital processes and outcomes.
• Establishes quality and safety priorities to measure the effectiveness of the quality and patient safety program.
• Conducts annual reviews and suggest modifications to the Quality and Patient Safety Plan.
• Allocates resources necessary for safety, process improvement, and creation of performance improvement teams.
• Assess the integration of the strategic planning process with the organizational quality and patient safety functions.
• Act on recommendations generated through the patient safety and performance improvement activities, and allocate resources
• Delegate responsibilities to physician leaders and department heads. Chairperson: The committee is chaired by a member of the Board of Directors
Membership: The committee membership includes representatives from the Board of Directors, Medical Staff leadership, and senior executive leadership. The chairperson is selected by the Chairman of the Board.
Reporting/Accountability: The Board Quality and Safety Committee reports to the Board of Directors

9
Quality and Patient Safety Council
Purpose: The Quality and Patient Safety Council monitors, identifies and brings conclusion to quality and safety issues that exist within Capital Health System. By using reliable data and evidence-based practice and literature, the committee members drive evidenced-based change that improves the quality, safety, overall patient experience and public perception of Capital Health System. Objectives:
• Provide a mechanism for establishing/re-setting organization-wide patient safety and performance improvement priorities
• Develop performance measures to improve quality and safety and reduce preventable adverse events
• Measure the organization’s key outcomes, activities, and processes to support quality, safety, efficiency, improvement, innovation, and learning.
• Analyze patterns and trends of near-misses and adverse events to detect patterns and trends
• Address internal and external customers’ needs and expectations • Promote interdepartmental and multidisciplinary communication with a scientific
approach to problem solving • Facilitate dissemination, discussion, and understanding of clinical and management
data among medical staff and hospital staff members • Implement evidence-based safety practices to enhance patient safety that are
consistent with the organizational strategic plan • Obtain recognition for excellence in service and delivery of healthcare
Chairperson: The chairperson is appointed by the President & Chief Executive Officer (CEO) of Capital Health System
Membership: The committee membership is a multidisciplinary team of representatives from administration, clinical services, finance, guest relations, medical staff, patient care services, patient safety, pharmacy, risk management, regulatory affairs, and quality.
Reporting/Accountability: The Quality and Patient Safety Council reports to the Board Quality and Safety Committee.

10
Patient Safety Committee Purpose: The Patient Safety Committee ensures that all adverse events are reviewed to identify and resolve system and practice issues that impact quality and patient safety. The committee provides a forum for review of events that are potentially reportable to the NJDOH and The Joint Commission, and has appropriate competencies to conduct analyses of adverse events and near-misses, with particular attention to serious preventable adverse events to reduce the probability of reoccurrence through the application of evidence-based patient safety practice. Objectives:
• Establish and review timeline for all serious adverse occurrences and near misses to identify system and practice issues that impact quality and patient safety
• Comply with reporting requirements of the NJ Patient Safety Act and The Joint Commission
• Comply with Disclosure Policy • Conduct root cause analyses and develop action plans for organization wide change. • Recommend changes to the facility’s systems, technology, or policies and procedures
based on the RCA(s). Document whether the facility accepted, rejected, or modified their recommendations (including their rationale)
• Develop training program for all professional and direct care staff to enable them to recognize near-misses, adverse events, Serious Preventable Adverse Events (SPAEs), and distribution of information to employees regarding anonymous reporting of near misses and adverse events
• Analyze trends and make recommendations to enhance quality and safe patient care • Identify system and practice issues that impact quality and patient safety.
Chairperson: The committee is facilitated by a Quality/ Safety Leader Membership: Core members include CMO or designee, CNO, physician leaders, risk, and quality. Other members include the clinical leaders and staff from the area where the event occurred. Reporting/Accountability: The Patient Safety Committee reports to the Patient Safety Team.

11
Patient Safety Team Purpose: The Patient Safety Team promotes a culture of safety within the organization by encouraging reporting of all patient occurrences ranging from near misses to adverse occurrences. The team provides leadership in the identification of risk reduction activities and implements strategies to promote a culture of safety and organization wide change. Objectives:
• Promote multidisciplinary forums with staff involvement for review of safety events and implement policies and procedures to improve safety
• Identify educational needs and provide educational programs • Establish and review metrics to monitor patient safety • Review National Patient Safety Goals and ensure compliance • Identify high risk processes and conduct proactive risk assessment annually • Review the results of Root Cause Analyses and monitor action plans. • Implement patient safety in high risk areas to coordinate risk reduction activities. • Identify and communicate relevant clinical safety issues to medical staff and hospital
leadership. • Analyze trends and make recommendations to enhance quality and safe patient care • Identify system and practice issues that impact quality and patient safety. • Conduct ongoing review and application of evidence-based safety practices • Conduct periodic safety culture surveys
Chairperson: The committee shall be chaired by the Patient Safety Officer or designee appointed by the President & CEO. Membership: Membership shall be comprised of clinical and administrative leaders, medical staff, and clinical staff. Reporting/Accountability: The Patient Safety Team is accountable to the Quality and Patient Safety Council and provides on-going communications to the Medical Executive Committee.

12
Patient Care Services Performance Improvement Committee Purpose: The Patient Care Services Performance Improvement Committee systematically monitors, analyzes, and improves nursing performance and patient outcomes to enhance and promote the professional practice of the registered staff nurse. Objectives:
• All units collect, monitor, and analyze relevant NDNQI data: Adult units – falls, falls with injury, restraints, skin. Pediatrics and NICU – IV infiltrations and pain assessment cycles. Psychiatry – restraints and injury with assault.
• Each unit selects two (2) unit specific, nurse identified measures that relate to quality improvement collaboratives, Capital Health Quality and Patient Safety Plan, CMS Quality Measures, Disease Specific Certifications or other professional sources.
• Unit based indicators and compliance targets are approved by the Service Based Practice Council.
• Quarterly reports are submitted to the Shared Accountability Coordination Council (SACC).
Chairperson: The chairperson is appointed by the Chief Nursing Officer. Membership: Unit staff nurses and educators Reporting/Accountability: The Patient Care Services Performance Improvement Committee reports to the Quality and Patient Safety Council.

13
Environment of Care Committee Purpose: The Environment of Care Committee is committed to providing a safe, functional, supportive and effective environment for patients, staff members, and other individuals in the hospital.
Objectives:
• Create a system-wide program dedicated to the oversight and management of the hospital’s Environment of Care.
• Identify and promote improvement opportunities and process changes to facilitate the safety, security and comfort of patient; visitors; employees and their environment.
• Educate staff about the role of the environment in safely, sensitively, and effectively supporting patient care.
• Develop standards to measure staff and hospital performance in managing and improving the Environment of Care.
• Collect information, carry out analysis of and seek resolution of Environment of Care issues in a timely manner.
• Establish and maintain risk assessment and evaluation criteria to identify the priority of performance improvements and process changes.
• Make recommendations at least annually to the Board of Directors for performance improvement activities.
• Report activities and relative discussions/resolutions to the Board and to receive acceptance of these reports or requests for additional information back from the Board.
Chairperson: The committee is chaired by the Vice President, Professional Services or designee appointed by the President & CEO. Membership: Vice President, Facilities & Professional Services (Chairman), Director of Facilities ( Co-Chair, Safety Officer and chair of the Life Safety Management Team), Director of Human Resource Operations (chair of the Safety Management Team), Director of Safety & Security (chair of the Security Management Team), Director of Environmental Services/Escort ( chair of the Hazardous Materials & Waste Management Team), Director of Clinical Equipment (chair of the Medical Equipment Management Team), Manager of Plant Operations for both CHMCH & RMC ( chairs of the Utilities Management Team), Divisional Director of EMS/Patient Logistics (chair of Emergency Management Team), and representatives from each of the following areas; patient services, clinical education, risk management, infection prevention, project & property management and outside physician practices

14
Reporting/Accountability: The CEO/President delegates responsibility and the coordination of the Environment of Care Management Plans to the Environment of Care Committee (EOCC) under the direction of the Vice President, Professional Services.
The EOCC delegates responsibility for oversight of these management plans to six (6) individual management teams, Safety, Security, Hazardous Materials & Waste, Life Safety, Medical Equipment, and Utilities.
The CEO/President has designated the Director of Facilities as Safety Officer. The Safety Officer is charged to intervene whenever conditions exist that pose and immediate threat to life or health, or pose a threat of damage to equipment or buildings.

2015 Strategic Plan
Part I. Environmental Assessment
OO3: Attachment 4
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE

Affiliation Discussions and M&A Activity Continues to Rise and Activity in Our Market is at an All time High
Mergers and Acquisitions
Activity in Our Market is at an All‐time HighHospital Mergers and Acquisitions
M&A Plans for the Next 12 Months1
n=189
6589 95 98
12%
No M&A Activity Planned
2010 2011 2012 2013
Number of Hospitals Part of a Health System
2000‐2012
26262775
29213100
88%
Pl i t P
2000 2003 2006 2009 2012
2542 2626 Planning to Pursue M&A Within the Next
12 Months
Source: AHA Hospital Fast Facts, available at www.aha.org; GE Capital Survey, available at: www.gehealthcarefinance.com; Kaufman Hall, “Number of Hospital Transactions Grew in 2013,” available at: www.kaufmanhall.com; Advisory Board interviews and analysis.
September 2013.© The Advisory Board Co.
2000 2003 2006 2009 2012
2

The Number of Accountable Care Organizations Continues to Grow
Accountable Care Organizations
Total Number of Operating ACOsMay 2014
Widening Reach of ACOs
67%Portion of U.S. population living in a primary care service 210
74 13 626
area with an ACO
17%Portion of U.S. population treated by an ACO306
210
by an ACO
5.3MMedicare FFS beneficiaries treated by an ACO
23
MSSP Cohort Private Sector ACOs
ACOs without announced contracts
Pioneer ACO Model
TotalPrivate &PublicACOs contractsACOs
HHS Goal: 30% of Medicare FFS in alternative payment model by end of 2016 and 50% by end of 2018
Source: Oliver Wyman, “ACO Update: Accountable Care at a Tipping Point,” April 2014; Leavitt Partners, “Growth and Dispersion of ACOs,” June 2014; Marketing and Planning Leadership Council interviews and analysis.© The Advisory Board Co
As of April 2014.
3

Value Based Purchasing
Value Based Payments are Shifting Away from Process and Focusing on Experience Outcomes and EfficiencyExperience, Outcomes, and Efficiency
Medicare VBP Program Domain Weights
Clinical Process
Patient Experience25%45%
20%10%
g g
Patient Experience
Outcomes of Care30%
40%30%
30%
25%
70%
45%
Efficiency20% 25%25%
30%
30%
Source: The Advisory Board Company “Mortality Rates Are Only One of Many VBP Changes to Come ”
FY 2013 FY 2014 FY 2015 FY 2016
Source: The Advisory Board Company, Mortality Rates Are Only One of Many VBP Changes to Come, December 4, 2013, available at: www.advisory.com; CMS, “Request for Information on Specialty Practitioner Payment Model Opportunities,” February 2014, available at: www.innovation.coms.gov; Health Care Advisory Board interviews and analysis.© The Advisory Board Co
4

Commercial Payers
Public Health Exchange Participants Choosing High Deductibles: $Close to 70% of Enrollees have a Deductible of at least $3,000
Annual Deductibles of Individual Plans Selected on eHealth
October 2013 – March 2014
30%
39% $6 000+
$3,000-$5,999
13%
11%
5%39% $6,000+
$2,000-$2,999
$1,000-$1,999
Source: Breakaway Policy Strategies, “Eight Million and Counting: A Deeper Look at Premiums Cost Sharing and Benefit Design in the New Health Insurance Marketplaces ”
3%$500-$999 < $500
Premiums, Cost Sharing and Benefit Design in the New Health Insurance Marketplaces, May 2014; eHealth, “Health Insurance Price Index Report for Open Enrollment and Q1 2014,” May 2014; Health Care Advisory Board interviews and analysis.© The Advisory Board
5

Patients
Market Forces Are Turning Patients into Consumers and Catalyzing a Shift in Healthcare Network DemandsCatalyzing a Shift in Healthcare Network Demands
Traditional Market Retail Market
1P i l Activist employer
Characteristics of a Traditional vs. Retail Market
Growing number of buyers1
2
Passive employer, price-insulated employee
Activist employer, price-sensitive individual
Broad open networks Narrow, custom networksProliferation of product options
Increased transparency3
Broad, open networks ,
No platform for apples-to-apples plan comparison
Clear plan comparison on exchange platforms
Increased transparency
Reduced switching costs4
apples plan comparison
Disruptive for employers to change benefit options
Easy for individuals to switch plans annually
Greater consumer cost exposure5Constant employee
premium contribution, low deductibles
Variable individual premium contribution, high deductibles
Source: Health Care Advisory Board interviews and analysis.© The Advisory Board
6

Immediate Access for Lower Acuity Care is a Huge Growth Area and Unmet Need in a Consumer‐Driven Healthcare market
Primary Care Network7
Need in a Consumer Driven Healthcare market
Consumer-Oriented Service Delivery Sites Filling the Gap
Traditional Access Points Primary Care
Office
Low Acuity High Acuity Emergency Department
Consumer-Oriented Access Points
Retail
Urgent Care Center
Virtual Visit
RetailClinic
Driving Provider Questions:
Sh ld t t t bli h t il li i ?• Should we build or expand our urgent care footprint?
Source: Mehrota A et al, "Visits To Retail Clinics Grew Fourfold From 2007 To 2009, Although Their Share Of Overall Outpatient Visits Remains Low " Health Affairs August 2012; Health
• Should we partner to establish retail clinics?• Is virtual care something that we should provide?• When should we enter into partnerships to meet patient demands?
Their Share Of Overall Outpatient Visits Remains Low, Health Affairs, August 2012; Health Care Advisory Board interviews and analysis.© The Advisory Board Co.
7
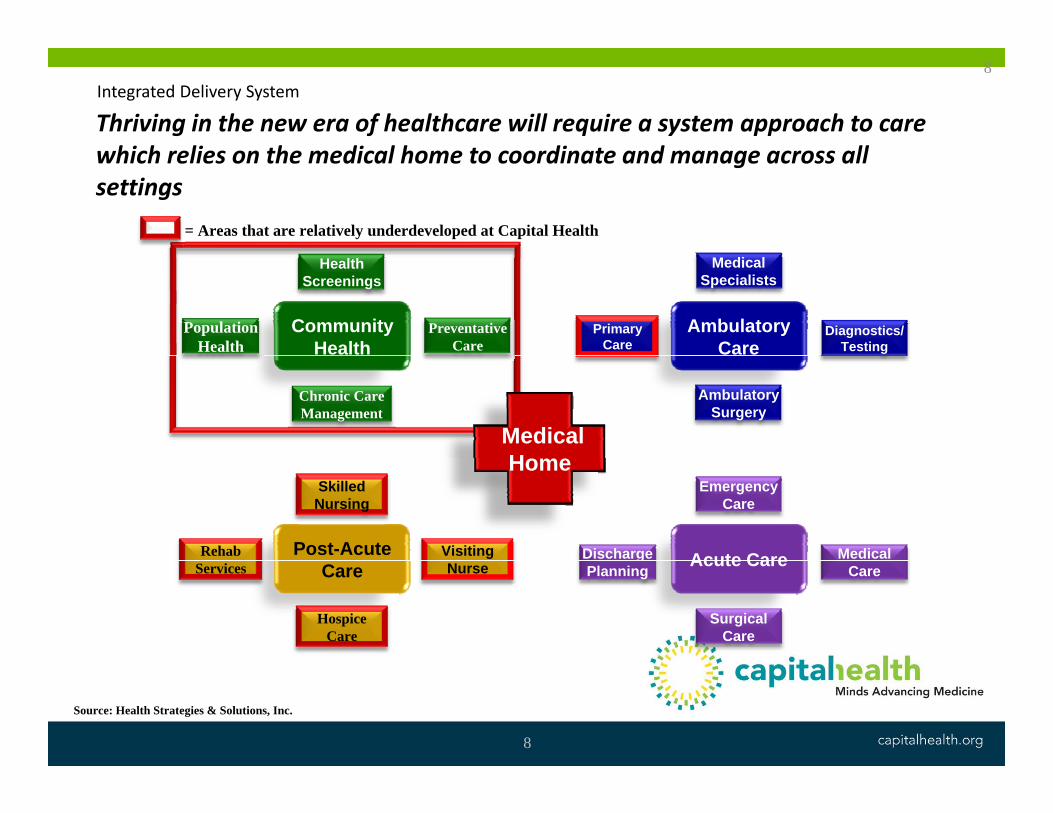
Thriving in the new era of healthcare will require a system approach to care hi h li th di l h t di t d ll
8Integrated Delivery System
which relies on the medical home to coordinate and manage across all settings
= Areas that are relatively underdeveloped at Capital Health
Community Health
Ambulatory Care
Primary Care
Medical Specialists
Diagnostics/Testing
Population Health
Health Screenings
Preventative Care
Medical H
Ambulatory Surgery
Chronic Care Management
Home
Post-Acute Acute CareDischarge
Emergency Care
Medical Rehab
Skilled Nursing
Visiting Care Acute Careg
Planning Care
Surgical Care
Services Nurse
Hospice Care
Source: Health Strategies & Solutions, Inc.
8
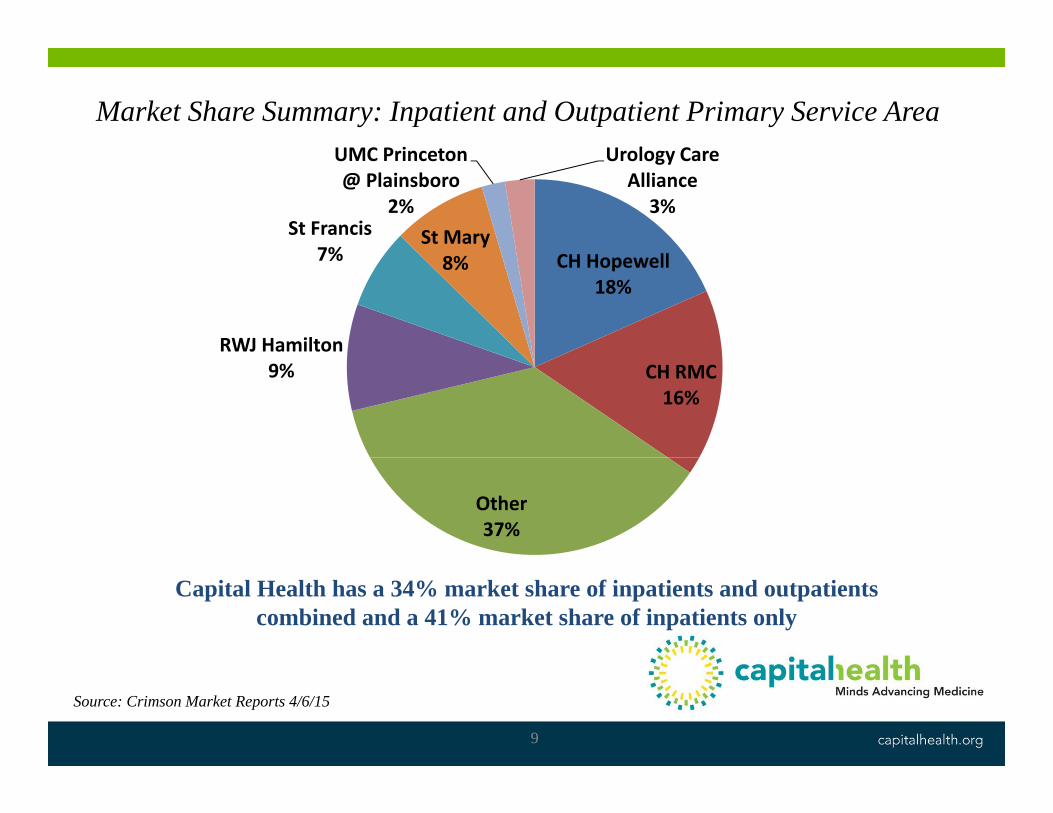
Market Share Summary: Inpatient and Outpatient Primary Service AreaUMC P i t U l C
St Francis7%
St Mary
UMC Princeton @ Plainsboro
2%
Urology Care Alliance
3%
CH Hopewell18%
RWJ Hamilton
7% 8%
CH RMC16%
9%
Other37%
Capital Health has a 34% market share of inpatients and outpatients combined and a 41% market share of inpatients only
Source: Crimson Market Reports 4/6/15
9
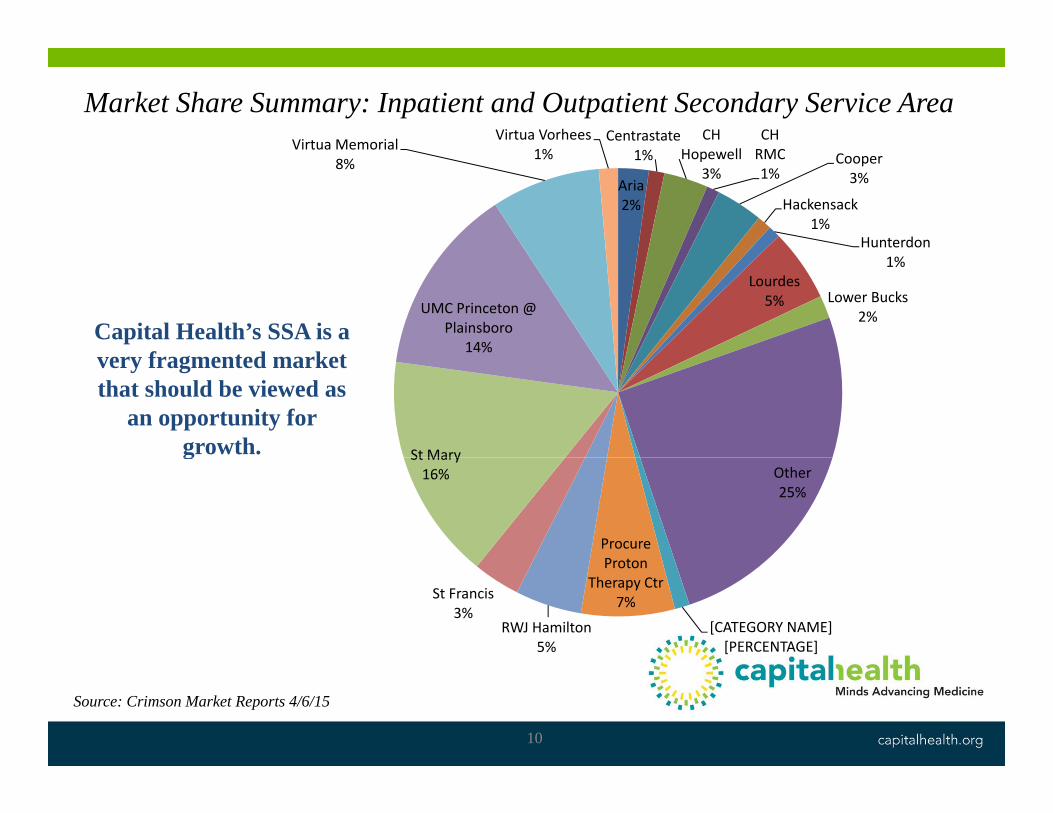
Market Share Summary: Inpatient and Outpatient Secondary Service AreaCentrastate
1%CH
H llCH RMCVirtua Memorial Virtua Vorhees
1%
Aria2%
1% Hopewell3%
RMC1%
Cooper3%
Hackensack1%
Hunterdon
8% 1%
1%Lourdes5% Lower Bucks
2%UMC Princeton @ Plainsboro
14%Capital Health’s SSA is a
f t d k t
St Mary
very fragmented market that should be viewed as
an opportunity for growth.
Other25%
Procure Proton
St Mary16%
g
[CATEGORY NAME][PERCENTAGE]
Proton Therapy Ctr
7%
RWJ Hamilton5%
St Francis3%
Source: Crimson Market Reports 4/6/15
10
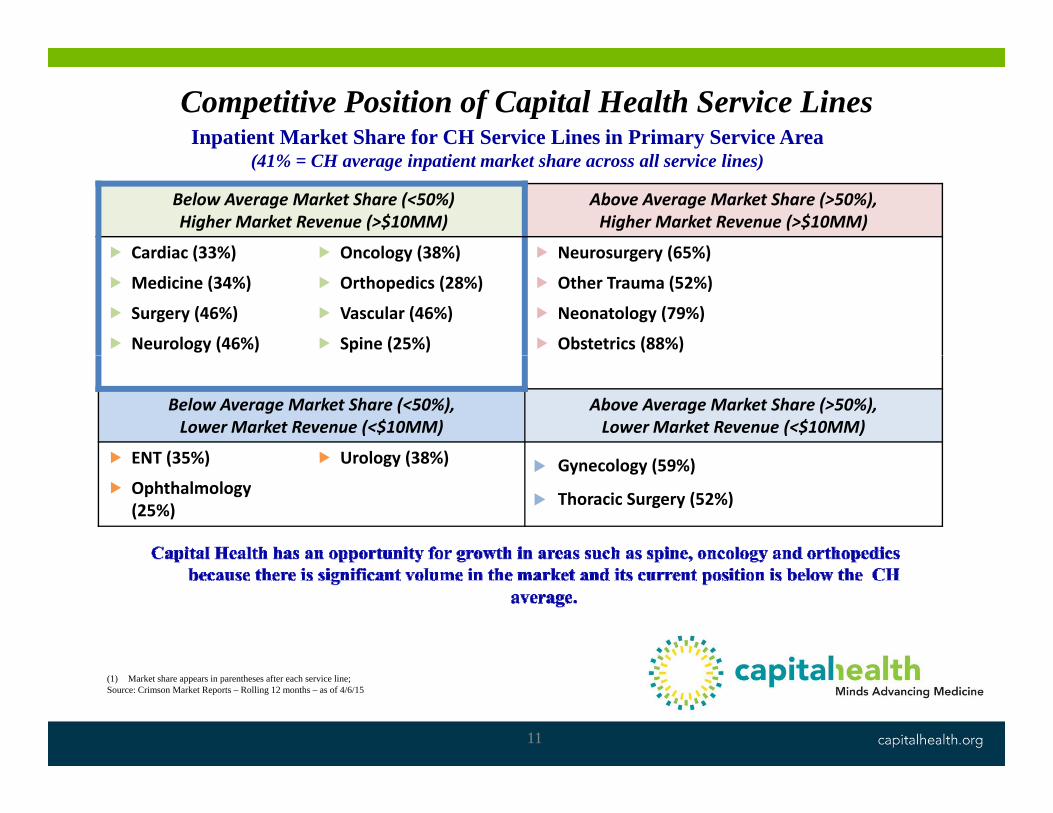
Competitive Position of Capital Health Service LinesInpatient Market Share for CH Service Lines in Primary Service Area
Below Average Market Share (<50%)Higher Market Revenue (>$10MM)
Above Average Market Share (>50%), Higher Market Revenue (>$10MM)
Cardiac (33%) Oncology (38%) Neurosurgery (65%)
(41% = CH average inpatient market share across all service lines)
Cardiac (33%)
Medicine (34%)
Surgery (46%)
Neurology (46%)
Oncology (38%)
Orthopedics (28%)
Vascular (46%)
Spine (25%)
Neurosurgery (65%)
Other Trauma (52%)
Neonatology (79%)
Obstetrics (88%)
Below Average Market Share (<50%),Lower Market Revenue (<$10MM)
Above Average Market Share (>50%),Lower Market Revenue (<$10MM)
ENT (35%) Urology (38%) ENT (35%)
Ophthalmology (25%)
Urology (38%) Gynecology (59%)
Thoracic Surgery (52%)
(1) Market share appears in parentheses after each service line;Source: Crimson Market Reports – Rolling 12 months – as of 4/6/15
11

Capital Health Key Operating Statistics 2012 - 2014% i
2012 2013 2014% increase ’12‐’14
Outpatient visits 298,253 302,453 299,466 0.4%
OR major cases 10,455 9,801 8,997 ‐14%
Same day surgery cases 6,962 8,072 7,855 13%
Radiology studies 159,230 162,131 159,751(x‐ray, MRI, CT scans) 0.3%
Inpatient discharges 24,763 25,510 24,798 0.1%
Births 2,357 2,881 2,860 21.3%
Emergency room visits 93,626 95,781 97,907 4.6%
Rehabilitation treatments 110,907 122,663 136,887 23.4%Capital Health’s volumes have held steady in most areas over the past 3 years withCapital Health s volumes have held steady in most areas over the past 3 years with
the exception of births, ED visits, and rehabilitation treatments which all experienced significant growth.
12

Capital Health’s Financial Status
2012 2013 2014 (unaudited)
Cash, investments and mortgage
$160,125,000 $163,806,000 $167,037,000
reserve fund cash equivalent
Long term debt $754,548,000 $748,276,000 $731,684,000
Current liabilities $67,206,000 $77,394,000 $90,512,000
Net income ($68,499,000) ($44,264,000) ($19,989,000)
HighlightsNet income and cash equivalents areNet income and cash equivalents are improving. Shifting from long term mortgage debt to current mortgage li bili iliabilities.
13

Payer Mix by Discharge 2014
Commercial / Other, 2%
Charity Care, 4%Self Pay, 4%
Medicare, 28%
Blue Cross, 16%
Managed Medicare, 4%
Medicaid, 9%
Managed Care / PPO, 17%
Managed Medicaid, 16%
1414

Competitive Threat Summary
Competitor Threat posed to Capital Health
► Merger with St. Barnabas leaves an uncertain future for RWJ Hamilton
► Strong financial position and increased access to capital due to new Trinity affiliation
► Expect intensified efforts to employ or affiliate with primary care physicians in the marketphysicians in the market
► Potential for a merger or affiliation with a larger, health system that would require all tertiary volume be kept within the system
► Recent instability in financial position may result in Trinity deciding to► Recent instability in financial position may result in Trinity deciding to pare down clinical services or close the facility over time; this will result in RMC being the only provider in the downtown Trenton market
► Current affiliation with Atlantic Health makes it virtually impossible to y pseek a clinical relationship for tertiary volume
15

Competitive Threat Summary, continued
Competitor Threat posed to Capital Health
► New Jersey’s largest health systems will continue to act as market consolidators and while this will increase their scale, they may beconsolidators and while this will increase their scale, they may be challenged to determine how to prioritize attention and resources among multiple entities
► The scale of these health systems’ pose a threat that Capital will need to address by ensuring that it owns its local marketto address by ensuring that it owns its local market.
► Virtua is one of the strongest financial health systems in New Jersey and the new hospital they plan to build will be a threat to CH’s ability to grow in northern Burlington Countygrow in northern Burlington County
► Dialysis, diagnostic, and rehabilitation competitors in the service area constantly seek to capture high‐margin ancillary volume from CH
`
16

CONCLUSIONSCONCLUSIONS
17
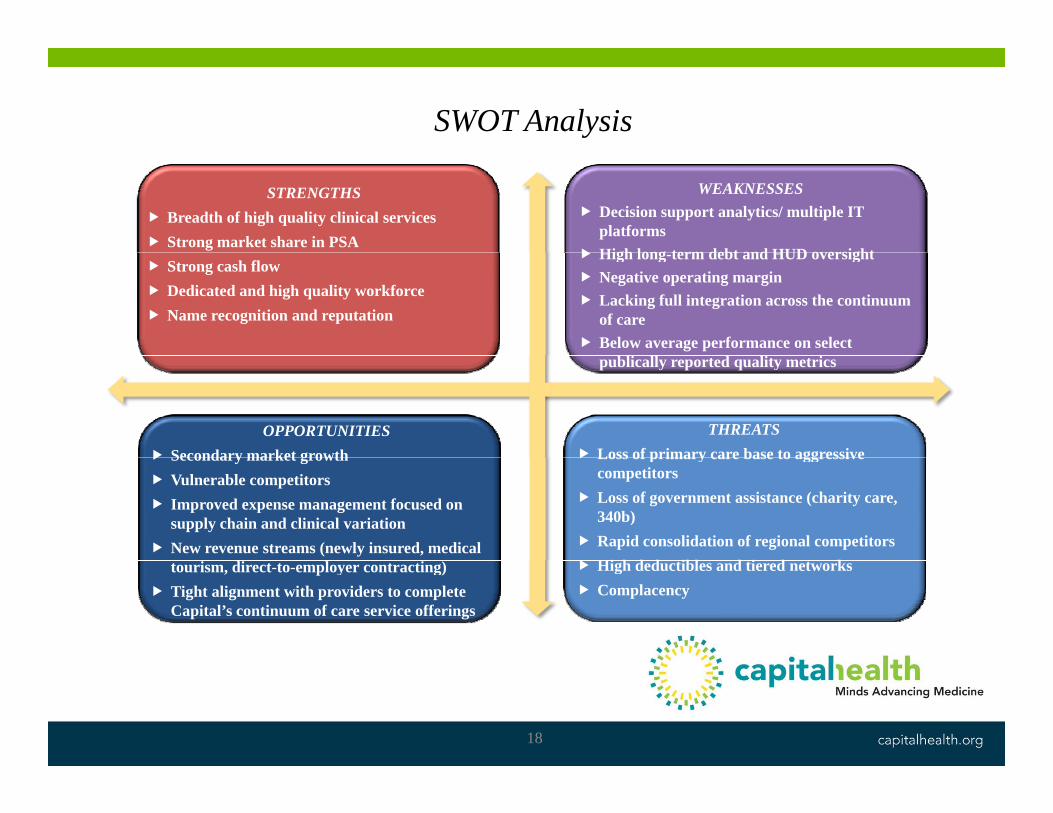
SWOT Analysis
STRENGTHS Breadth of high quality clinical services Strong market share in PSA
WEAKNESSES Decision support analytics/ multiple IT
platforms High long term debt and HUD oversight
Strong cash flow Dedicated and high quality workforce Name recognition and reputation
High long-term debt and HUD oversight Negative operating margin Lacking full integration across the continuum
of care Below average performance on select
publically reported quality metrics
THREATS Loss of primary care base to aggressive
OPPORTUNITIES Secondary market growth Loss of primary care base to aggressive
competitors Loss of government assistance (charity care,
340b) Rapid consolidation of regional competitors Hi h d d ibl d i d k
Secondary market growth Vulnerable competitors Improved expense management focused on
supply chain and clinical variation New revenue streams (newly insured, medical
High deductibles and tiered networks Complacency
tourism, direct-to-employer contracting) Tight alignment with providers to complete
Capital’s continuum of care service offerings
18

Capital Health’s Overall StrategyCapital Health s Overall Strategy
Th h t t i l ti hi C it l H lth illThrough strategic relationships, Capital Health will position itself as the region’s provider of choice
reflective of the evolving marketplace while maintaining local control
1919

Capital Health FY2018 Draft GoalsCapital Health FY2018 Draft GoalsStrategic Priorities FY2018 Goals
Quality and Service Excellence
► Capital Health is the top performer among its direct competitors in publically available quality indicators and patient satisfactionExcellence publically available quality indicators and patient satisfaction
Efficiency/ Clinical Variation
► Capital Health attains a better than average expense per admission
► Capital Health is not penalized by CMS for value‐based purchasing
C it l H lth i it b f d li d h dPopulation Health Capital Health increases its number of covered lives and earns shared savings dollars in numerous pay for performance programs
Partnerships/ New Business Development
Capital Health enters into mutually beneficial partnership opportunities and new revenue streams which result in the Business Development generation of a profit from operations
Stakeholder Development
Become the preferred health system/hospital employer in Capital Health’s local market
2020

Questions and DiscussionQuestions and Discussion
21

OO3: Attachment 5
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE


















