ANNEXES - National Health Insurance Scheme1).pdf · ANNEX 5: Directory of district mutual health...
60
Transcript of ANNEXES - National Health Insurance Scheme1).pdf · ANNEX 5: Directory of district mutual health...


2010 ANNUAL REPORT
i
TABLE OF CONTENTS
TABLE OF CONTENTS ..................................................................................................................... i LIST OF ACRONYMS ...................................................................................................................... iii VISION, MISSION AND CORE VALUES ....................................................................................... 1 PROFILE OF DIRECTORS ............................................................................................................... 6
CHAIRMAN’S ACKNOWLEDGEMENT ........................................................................................ 9 REPORT OF CHIEF EXECUTIVE.................................................................................................. 10 1.0 INTRODUCTION ....................................................................................................................... 13
1.1 GOVERNANCE ..................................................................................................................... 13 1.2 MANAGEMENT .................................................................................................................... 13
1.3 NHIS VALUE CHAIN ........................................................................................................... 13
2.0 CORPORATE GOALS AND OBJECTIVES ............................................................................. 15
2.1 CORPORATE GOALS ........................................................................................................... 15 2.2 CORPORATE OBJECTIVES FOR 2010-2014...................................................................... 15
3.0 OPERATIONAL ACTIVITIES .................................................................................................. 15 3.1 SUSTAINABILITY AND COST CONTAINMENT ............................................................. 15 3.2 MEMBERSHIP AND ID CARD MANAGEMENT .............................................................. 16
3.2.1 Membership trend ............................................................................................................. 16 3.2.2 Special registration exercise ............................................................................................. 18 3.2.3 Free maternal health care ................................................................................................. 19 3.2.4 ID cards production and distribution ................................................................................ 20
3.3 CLAIMS MANAGEMENT .................................................................................................. 21
3.3.1 Outpatient utilization ........................................................................................................ 21
3.3.2 Inpatient utilization ........................................................................................................... 21 3.3.3 Claims payment trend ....................................................................................................... 22
3.4 ICT AND DATA MANAGEMENT ....................................................................................... 23 3.5 PROVIDER ACCREDITATION AND QUALITY ASSURANCE ...................................... 23
3.5.1 Collaboration .................................................................................................................... 24
3.6 ADMINISTRATION AND HUMAN RESOURCE ............................................................... 25 3.7 PLANNING, MONITORING, EVALUATION, RESEARCH AND DEVELOPMENT ...... 25
3.8 PROJECTS AND PROCUREMENTS ................................................................................... 25 3.9 COMMUNICATION AND STAKEHOLDER ENGAGEMENT .......................................... 26
3.9.1 Stakeholder engagement ................................................................................................... 26 3.9.2 Policy fair ......................................................................................................................... 26
3.9.3 End of year get-together and awards night ....................................................................... 26 3.9.4 Media engagement ........................................................................................................... 27
4.0 ACHIEVEMENTS ...................................................................................................................... 29 4.1 INCREASED COVERAGE .................................................................................................... 29 4.2 UNDP/WHO EXCELLENCE AWARD ................................................................................. 29 4.3 FINANCIAL AND CLINICAL AUDITS .............................................................................. 29 4.4 REVIEW OF MEDICINES LIST ........................................................................................... 30
4.5 ACCREDITATION OF HEALTH FACILITIES ................................................................... 30 4.6 IMPROVED REIMBURSEMENT TO PROVIDERS ........................................................... 31 4.7 GATE-KEEPER SYSTEM AND FREE MATERNAL CARE PROGRAMME ................... 31 4.8 RISK ASSESSMENT ............................................................................................................. 31
5.0 CHALLENGES ........................................................................................................................... 32 5.1 FINANCIAL SUSTAINABILITY OF THE SCHEME ......................................................... 32 5.2 IDENTIFICATION OF THE POOR IN THE INFORMAL SECTOR .................................. 32
5.3 ID CARD MANAGEMENT ................................................................................................... 32 5.4 ICT ........................................................................................................................................... 32 5.5 CLAIMS MANAGEMENT .................................................................................................... 32

2010 ANNUAL REPORT
ii
6.0 OUTLOOK FOR 2011 ................................................................................................................ 33
6.1 ENHANCE FINANCIAL SUSTAINABILITY OF THE NHIS ............................................ 33 6.1.1 Defensive Strategy: .......................................................................................................... 33
6.1.2 Prudent fund management: ............................................................................................... 33 6.1.3 Sourcing Strategy: ............................................................................................................ 34
6.2 STRENGTHEN THE NHIS ICT ............................................................................................ 34 6.2.1 ICT deployment ................................................................................................................ 34 6.2.2 ICT governance ................................................................................................................ 34
6.2.3 Data integrity .................................................................................................................... 34 6.3 PROMOTE QUALITY IMPROVEMENT IN SERVICE PROVIDER FACILITIES ........... 35 6.4 STRENGTHEN CLAIMS MANAGEMENT ......................................................................... 35 6.5 IMPROVE ID CARD MANAGEMENT ................................................................................ 35
6.6 HUMAN RESOURCE CAPACITY AND ORGANISATIONAL REFORMS ..................... 35 6.6.1 Attracting, developing and retaining relevant human resource ........................................ 35 6.6.2 Organizational reforms ..................................................................................................... 36 6.6.3 Ghana Health Insurance Institute ..................................................................................... 36
6.7 Communication and marketing strategies ............................................................................... 36 6.7.1 Internal and external communication ............................................................................... 36 6.7.2 Communication with service providers ............................................................................ 37
7.0 CONCLUSION ........................................................................................................................... 38
ANNEXES ............................................................................................................................................ 39
ANNEX 1: Financial Statement .................................................................................................... 40
ANNEX 2: Minimum health care package under NHIS ............................................................... 43
ANNEX 3: Unit heads and managers ............................................................................................ 45 ANNEX 4: Regional Managers ..................................................................................................... 46 ANNEX 5: Directory of district mutual health insurance schemes .............................................. 47
ANNEX 6: Training programs organised in 2010 ........................................................................ 54
List of Figures
Figure 1: NHIS Value chain .............................................................................................................. 14
Figure 2: Active membership as percent of population by region in 2010 ....................................... 17 Figure 3: Active NHIS Subscribers by Category 2010 ..................................................................... 18 Figure 4: Outpatient Utilization Trend .............................................................................................. 21
Figure 5: Inpatient Utilization Trend ................................................................................................. 22
Figure 6: Claims Payment Trend ....................................................................................................... 22
List of Tables
Table 1: Active Membership ............................................................................................................. 16 Table 2: New Members, Renewing and Membership in 2010 Active .............................................. 17
Table 3: Total number of members registered under the special registration exercise ..................... 19 Table 4: ID Cards production and distribution by region ................................................................. 20
Table 5: Accreditation results ............................................................................................................ 24

2010 ANNUAL REPORT
iii
LIST OF ACRONYMS
1TP One-Time Premium
Act 650 National Health Insurance Act, 2003 (Act 650)
AMFm Affordable Medicine Facility – Malaria
CHAG Christian Health Association of Ghana
CPC Claims Processing Centre
DCEs Deputy Chief Executive
DMHIS District Mutual Health Insurance Scheme
DVLA Driver and Vehicle Licensing Authority
G-DRG Ghana Diagnostic Related Grouping
GH¢ Ghana Cedis
GHS Ghana Health Services
GMA Ghana Medical Association
HIP Health Insurance Project
ICT Information Communication Technology
IPD In-Patient Department
LEAP Livelihood Empowerment Against Poverty
LPM Live Presenter Mention
M&E Monitoring & Evaluation
MDAs Ministries, Departments and Agencies
MDGs Millennium Development Goals
MOH Ministry of Health
NGOs Non Governmental Organisations
NHIA National Health Insurance Authority
NHIL National Health Insurance Levy
NHIS National Health Insurance Scheme
OPD Out Patient Department
PDAs Personal Digital Assistance
PRMs Provider Relationship Managers
PRO Public Relations Officer
PW Pregnant women
RAC Risk Assessment Committee
R&D Research and Development
SCAD Strategy and Corporate Affairs Division
SSNIT Social Security and National Insurance Trust
UNDP United Nations Development Programme
WHO World Health Organization

2010 ANNUAL REPORT
1
VISION, MISSION AND CORE VALUES VISION
To be a model of a sustainable, progressive and equitable social health insurance scheme in Africa
and beyond.
MISSION
To provide financial risk protection against the cost of quality basic healthcare for all residents in
Ghana, and to delight our subscribers and stakeholders with an enthusiastic, motivated, and
empathetic professional staff who share the values of accountability in partnership with all
stakeholders.
CORE VALUES
Integrity
Accountability
Empathy
Responsiveness
Innovation

2010 ANNUAL REPORT
2
NATIONAL HEALTH INSURANCE COUNCIL
Hon. Doe Adjaho Chairman
Hon. Rojo Mettle-Nunoo (Dep. Minister of Health) Member
Mr. Sylvester A. Mensah Chief Executive
Dr. Elias Sory Member
Dr. Stephen Ayidiya Member
Mr. Samuel Akwei Member
Mrs. Czarina Baeta Ribeiro Member
Dr. Steve Ahiawordor Member
Mr. Kwame Owusu-Bonsu Member
Dr. Mercy Bannerman Member
Mrs. Nyamikeh Kyiamah Member
Mr. Kofi Asamoah Member
Dr. Edward Abbah Foli Member
Hajia Laadi Ayi Ayamba Member
Mr. Anthony Dzadzra Member
Dr. Hetty Asare Member
Mrs. Aimee Yuori Secretary

2010 ANNUAL REPORT
3
COUNCIL SECRETARY : MRS. AIMEE YUORI
REGISTERED OFFICE : CDH HOUSE, NORTH RIDGE,
ACCRA
AUDITORS : ERNST AND YOUNG,
CHARTERED ACCOUNTANTS
BANKERS : GHANA COMMERCIAL BANK
ECOBANK GHANA LTD,

2010 ANNUAL REPORT
4
EXECUTIVE MANAGEMENT
Mr. Sylvester A. Mensah Chief Executive
Mr. Nathaniel Otoo Director, Admin. & General Counsel
Dr. Nicholas A. Tweneboa Director, Operations
Mr. O. B. Acheampong Director, Research & Development
Dr. Gustav Cruickshank Chief Internal Auditor
Mr. Ben Kusi Director, ICT
Mr. Ahmed Imoro Ag. Director, Finance
Dr. Lydia Dsane-Selby Ag. Director, Clinical Audit
Mr. Perry Nelson Ag. Director, Claims
Mr. Winfred Agbeibor Ag. Director Strategy & Corporate Affairs
Mr. Francis-Xavier Andoh-Adjei Deputy Director, Strategy
Mr. Eric Ametor-Quarmyne Deputy Director, Corporate Affairs
Dr. Francis Mensah Asenso-Boadi Deputy Director, Research & Development
Mr. Rudolf Zimmermann Deputy Director, Finance
Mr. Anthony Gingong Deputy Director, Operations
Mrs. Adelaide Bunatal Deputy Director, Claims
Ms. Mary Owusu Deputy Director, Human Resource
Mr. Ben Yankah Deputy Director, Actuary
Mr. Sam Buabasah Deputy Director, Procurement & Projects
Mrs. Aimee Yuori Deputy Director, Legal (Council Secretary)

2010 ANNUAL REPORT
5
SSSYYYLLLVVVEEESSSTTTEEERRR AAA... MMMEEENNNSSSAAAHHH,,, CCCHHHIIIEEEFFF EEEXXXEEECCCUUUTTTIIIVVVEEE,,, NNNHHHIIIAAA ...
Sylvester A. Mensah is the Chief Executive of the National Health Insurance Authority. Prior to his
appointment, Mr. Mensah was the Head of Public Sector Banking at the Intercontinental Bank (GH)
Ltd., a full time lecturer at the Institute of Professional Studies (Ghana), and an Adjunct Lecturer at
the Central University Graduate School. He had earlier worked as District Co-ordinator of the
National Mobilization Program, rising through the ranks to the office of Greater Accra Regional
Director of same in 1987/88. He has 24 years working experience in the Public Services, Private
Sector, Banking and Academia. Mr. Mensah was elected Member of Parliament by the people of
Dadekotopon in the Greater Accra Region in 1997.
Mr. Mensah holds an MBA in Finance from the UK, Bsc. in Administration (Ghana), Diploma in
Political Economy (Germany) and a Diploma in Public Administration (Ghana). He is a Member of
the Institute of Business Consulting (MIBC), UK and a Council Member of the Global Marketing
Network, Ghana. He serves on a number of private and public boards including the National
Identification Authority of Ghana. He is an alumnus of the University of Ghana Business School,
the University of Leicester in the UK and the Harvard University School of Public Health, where he
pursued a number of health (insurance) financing related competency courses.

2010 ANNUAL REPORT
6
PROFILE OF DIRECTORS
NATHANIEL OTOO: DIRECTOR, ADMINISTRATION AND GENERAL COUNSEL
Mr. Otoo has over 19 years work experience spanning both the public and
private sectors. Prior to assuming the position of Director of Administration &
General Counsel at the Authority, he was Corporate Secretary at the Social
Security & National Insurance Trust, an Export Development Officer at the
Ghana Export Promotion Council and Projects Coordinator at Promasidor Ghana
Limited.
A Lawyer by profession, Mr. Nathaniel Otoo completed his Professional Law Studies in 1988 after
obtaining a Bachelor’s degree in law from the University of Ghana. He also holds a Master of Arts
Degree in International Relations from the International University of Japan, and has undertaken a
Professional Training Course in Marketing and Management under the auspices of the Carl
Duisberg Gesellschaft of Germany. He has participated in various health leadership courses.
DR NICHOLAS A. TWENEBOA: DIRECTOR, OPERATIONS. With over thirty years working experience spanning several fields, particularly
in the practice of medicine and in management, Dr Nicholas Tweneboa has
over the years gained deep insight into the health sector, having worked in
management capacity in several organizations and hospitals in the public,
private and quasi-public sub-sectors. He has facilitated many workshops and
undertaken consultancy services in health care quality management, strategy
and systems development on behalf of a number of local and international
organizations. He has intense interest in writing and health education which have won him a Valco
Literary Award in poetry and an international award in diabetes education.
Dr Nicholas A. Tweneboa holds an MB, ChB degree from the University of Ghana Medical School
and an MBA from the University of Leicester, UK.
OSEI B. ACHEAMPONG: DIRECTOR, RESEARCH AND DEVELOPMENT
Prior to joining NHIA, Mr. Acheampong worked for pharmaceutical companies
developing contracting and marketing strategies for hospitals and health
insurance companies. He also worked for health insurance companies where he
managed provider networks and contracts, and developed and managed drug
formularies.
Mr. Osei Boateng Acheampong holds a Master of Science degree in Health
Policy and Management from Harvard School of Public Health specializing in healthcare
financing, health insurance and international health. He had earlier studied at Brown University
where he obtained a Bachelor of Arts degree in Urban Studies/Planning and Yale School of
Management.

2010 ANNUAL REPORT
7
AHMED IMORO: AG. DIRECTOR, FINANCE
Mr. Ahmed Imoro joined the Controller and Accountant General Department in
1995 and was seconded to National Health Insurance Authority as Principal
Accountant in 2005. He was later appointed the substantive Deputy Director of
Finance and has since 2006 been the Acting Director of Finance.
Mr. Ahmed Imoro has a Masters Degree in Business Administration (MBA-
Finance) and a Bachelors degree in Business Administration (Accounting and
Finance) from European University of Lefke.
BEN KUSI: DIRECTOR, ICT
Prior to his present appointment, Mr. Ben Kusi worked with Bank of Ghana as
Head of Infrastructure and Project Manager on the IMPACT05 ICT project,
between 2004 and 2005. He had also worked with the British National Health
Service in the UK as ICT professional between 1998 and 2004. His expertise
ranges from People Management, Information Systems analysis and design,
project management and implementation of Enterprise Architecture solutions.
Mr. Ben Kusi holds a Bachelor of Science degree in Electronic Engineering
from Middlesex University, UK and a Post Graduate Diploma in Management Information Systems
Design from the University of Westminster, UK.
DR. LYDIA DSANE-SELBY: DIRECTOR, CLINICAL AUDIT
A Medical Doctor by profession, Dr. Lydia Dsane-Selby worked as Medical
Officer at Korle-Bu Teaching Hospital, Achimota Hospital and in the UK prior
to taking appointment at the NHIA,
She holds an MBChB from the University of Ghana Medical School, Korle-Bu
and a Post Graduate in ENT Surgery from the Royal College of England. She is
an ICT Trained Microsoft Certified Professional.
DR. GUSTAV G.L. CRUICKSHANK: CHIEF INTERNAL AUDITOR
Prior to his present appointment, Dr. Gustav G.L Cruickshank was a lecturer in
MBA, MSc and BSc degree programs in various institutions in the UK. He also
worked with organizations such as Arthur Andersen representative office,
Intercontinental Bank, LCBM (UK), Gabem Group (UK), Zenith Aegis Ltd
(UK and Ghana). He has over fifteen years international experience in
management consultancy, accounting, finance, auditing and operations and
strategic planning.
Dr. Gustav Cruickshank is a Chartered Accountant and has an MBA in Finance and PhD in
Strategic Management. He is a Fellow of the Association of Chartered Certified Accountants, UK

2010 ANNUAL REPORT
8
(FCCA), the Institute of Financial Accountants UK (FFA), the Institute of Business Consultancy
UK (FIBC), a member of the Institute of Chartered Accountants, Ghana (ICAG) and the Institute of
Internal Auditors (IIA).
PERRY NELSON: AG. DIRECTOR, CLAIMS
Mr. Perry Nelson was appointed Ag. Director of Claims in 2010 after serving
briefly as ICT Consultant to the NHIS and Deputy Director of ICT. He has over
21 years working experience in the ICT industry. He has been a key player in the
entire cycle of IT systems review, system requirements definition, design,
development, implementation and support in major IT projects across the USA,
United Kingdom, Africa, and Europe. Mr Nelson has been a freelance ICT
Consultant for over 15 years during which he worked on many multi-million pounds ICT projects
around the world.
Mr. Perry Nelson earned his Bachelor of Science degree in Computer Science from the Kwame
Nkrumah University of Science and Technology in 1980.
WINFRED AGBEIBOR: AG. DIRECTOR, STRATEGY & CORPORATE AFFAIRS
Winfred is a business planner and marketing communicator with over 12 years
experience in strategy, brand management, training and market research, from
Banking & Finance, through International Development & Medical Industry to
Consulting; both within and outside Ghana.
Before joining NHIA, he was the Commercial & Country Manager of The
Nielsen Company (ACNielsen) Ghana, and also served as Head of Strategy &
Corporate Affairs of Intercontinental Bank.
He has an MBA in Corporate Planning & Marketing from Vrije Universiteit Brussels, Belgium, a
Master of Human Ecology from same, and a BSc. Agriculture (Agricultural Economics) degree
from the University of Ghana.

2010 ANNUAL REPORT
9
CHAIRMAN’S ACKNOWLEDGEMENT
Many of the achievements mentioned in this report would not have been possible without the
support and selflessness of equally busy colleague Council members who take time off their
schedules to attend meetings and hold deliberations even at short notice. I appreciate their
commitment and contributions.
I am equally grateful to management and staff of the NHIS and the Ministry of Health for their
continued support. On behalf of the Council, I thank our subscribers, service providers and other
stakeholders for their cooperation.
Together, let’s look forward to a healthier and stronger NHIS in 2011.
Thank you.
Hon. Doe Adjaho
Council Chairman, NHIA

2010 ANNUAL REPORT
10
REPORT OF CHIEF EXECUTIVE
INTRODUCTION
The National Health Insurance Scheme (NHIS) is a social intervention program intended to provide
financial risk protection against out of pocket health care expenditure for all residents in Ghana.
The scheme is currently operational in 145 districts across the country with a total cumulative
membership of over 18 million, out of which over 8 million, representing 34% of Ghana’s current
population are active card bearing members.
RESTRUCTURING AND SIGNIFICANT ACHIEVEMENTS
Following on from 2009, Management continued the process of restructuring the NHIS in order to
secure the sustainability of the scheme. Some of the reforms that were made include the following:
Creation of Clinical Audit Division
The Clinical Audit Division was created and became operational in January 2010 to ensure the
provision of quality healthcare service to NHIS subscribers. The division is mandated to audit
claims at both the health facilities and at the scheme level. During the period under review, the
division, with the active collaboration of service providers, conducted audit in 450 health facilities
in 76 districts across the country. The audit exercise resulted in the recovery of GH¢16.8 million
from service providers. It also serves as a useful way of effecting behavioural change among health
care providers and district scheme officials.
Elevation of Internal Audit Unit
The Internal Audit Unit was elevated to a divisional status to empower it in order to deliver on its
mandate. During the period under consideration, the division conducted a full scale audit in all the
145 district schemes across the country. Scheme officials who were found to have misconducted
themselves were duly sanctioned.
Establishment of Claims Processing Centre
A world-class ultra modern Claims Processing Centre (CPC) was established to ease the burden of
claims management at the district schemes. The centre is fully staffed with qualified health
professionals to properly adjudicate claims submitted by accredited service providers. The centre
currently vets claims from all the eight (8) regional hospitals, the three teaching hospitals and some
selected health facilities across the country. The CPC has contributed to a considerable reduction in
claims processing turn-around time from an average of 90 days to 60 days. It has also contributed to
cost savings of 6.8 million Ghana Cedis representing 19% of total claims submitted in 2010.
Introduction of Capitation
NHIA had a successful negotiation for stakeholder acceptance of capitation as an additional
provider payment mechanism. It is expected that the new payment mechanism when introduced
would simplify claims management and improve the quality of care rendered to subscribers because
of continuity of care.
Capitation will be used to re-imburse providers for primary care OPD services while Ghana
Diagnostic Related Groupings (G-DRG) will continue to be used to re-imburse them for inpatient

2010 ANNUAL REPORT
11
and specialized services. For a start, capitation would be piloted in Ashanti Region. It is expected
that preparatory work would be completed for official launching in the third quarter of 2011.
One Time Premium Payment
The government has stated its commitment to assuring unhindered financial access to quality health
care for residents of Ghana through a universal health care programme that allows for a One Time
Premium Payment. To make the dream a reality, the Minister of Health commissioned a task force
comprising representatives from Ministry of Health, Ghana Health Service and NHIA to draft the
policy document for the implementation of the new policy. The committee has completed its work
and submitted the document to the Minister of Health for onward submission to Cabinet.
OUTLOOK FOR 2011
One Time Payment would be operational in 2011. In this regard, NHIA will focus on developing
implementation modalities and commence implementation as soon as official communication is
received from government.
It is also envisaged that the legislative review process would be completed in 2011 to streamline the
operations of the scheme. Other key activities that will be undertaken include the following:
1. Deploying the CPC to its full capacity with the introduction of all software and equipment.
2. Addressing the low claims management capacity outside the CPC operation/ coverage.
3. Strengthening the poor gatekeeper system.
4. Enforcing the MOH’s Medicine prescribing levels.
5. Implementing the new prescription form regime in collaboration with the GHS and the
MOH.
6. Addressing the low premium collection at the scheme level, accounting for less than 5% of
our total inflows.
7. Implementing the consolidated premium account regime.
8. Strengthening performance monitoring and measurement regime at the regional and scheme
levels.
9. Implementing Capitation pilot in Ashanti Region.
10. Developing an efficient ID card distribution regime.
11. Developing an operational asset allocation policy.
12. Engaging in equity investments for long term sustainability.
13. Establishing a Social Health Insurance Institute for South-South learning and income
generation for the National Health Insurance Fund.
14. Establishing an outsourced Call Centre to give a meaningful voice to customers and
stakeholders – subscribers, providers and the general public.
15. Develop an effective and efficient media communication strategy that would open up and
adequately ventilate the NHIS success story.
16. Improving data integrity.
17. Enhancing subscriber authentication.
18. Implementing a new claims module that links clinical diagnosis to therapy/ treatment.

2010 ANNUAL REPORT
12
The following projects would be undertaken:
1) Complete and relocate into the new Head Office Premises.
2) Re-locate data centre from STL to NHIA head quarters premises.
3) Develop & maintain Data Recovery Site within STL for at least 12 months.
4) Construct ten (10) new regional offices.
5) Construct twenty (20) new schemes and satellites offices across the country.
CONCLUSION
The ongoing reforms in NHIS call for strategic thinking, benchmarking with best practices, team
work, efficient use of resources, sacrifice and commitment. Management of NHIA is determined to
build a scheme that would stand out as a model in Africa and beyond, providing access to
affordable and quality health care services for all residents in Ghana with highly motivated
professionals. I appreciate the team spirit and cordial working relationship with a technically
efficient management team who have always kept their “eyes on the ball”.
Let me use this opportunity to thank all NHIS stakeholders for your continued support and
commitment to building a sustainable health insurance scheme. All views on how to improve the
NHIS are welcome.
Thank you.
Sylvester A. Mensah
Chief Executive

2010 ANNUAL REPORT
13
1.0 INTRODUCTION The National Health Insurance Authority (NHIA) is a statutory body mandated to secure the
implementation of the National Health Insurance Scheme. It is responsible for the registration,
licensing and regulation of health insurance schemes in the country. It also has the role of
supervising the operations of District Mutual Health Insurance Schemes (DMHIS), grant
accreditation to healthcare providers and to monitor their performance for efficient and quality
service delivery. It is responsible for managing the National Health Insurance Fund and devising
mechanisms to ensure that indigents are adequately catered for under the NHIS.
1.1 GOVERNANCE
The scheme is governed by a 16-member Council drawn from various stakeholder organisations.
The Council is under the chairmanship of Hon. Doe Adjaho, First Deputy Speaker of Parliament
and Member of Parliament (MP) for Ave-Avenor constituency.
1.2 MANAGEMENT
The Executive Management of the scheme is led by Mr. Sylvester A. Mensah, the Chief Executive.
Other members include technical directors of various divisions, deputy directors and other senior
managers. To ensure accountability to stakeholders, NHIS is decentralised to the regional and
district levels. The full lists of Unit Heads and other Managers, including Regional Managers of the
NHIS are attached as Annexes 3 and 4.
1.3 NHIS VALUE CHAIN
The value chain demonstrates how NHIS delivers value to subscribers through its primary and
supporting activities.
The primary activities are membership registration and ID card management, provider accreditation
and quality assurance, claims management and provider payments. These are supported by
secondary activities which include research and development, monitoring and evaluation, an ICT
infrastructure and data management, financial and clinical audits, effective communication with
internal and external publics, human resource management, conflict resolution and stakeholder
management. Another key supporting activity is financing, which refers to how funds are mobilised
from different sources to pay for services rendered under the NHIS services.
Figure 1 shows the value chain captured in a framework for securing financial risk protection, client
satisfaction and improved health status for residents in Ghana.
Additionally, the NHIS in collaboration with stakeholders develops and maintains the NHIS
medicines list and tariffs system in accordance with the benefits package.

2010 ANNUAL REPORT
14
Figure 1: NHIS Value chain

2010 ANNUAL REPORT
15
2.0 CORPORATE GOALS AND OBJECTIVES
2.1 CORPORATE GOALS
The key corporate goals of the National Health Insurance Scheme are:
1. To attain a financially sustainable health insurance scheme.
2. To achieve universal financial access to basic health care.
3. To secure stakeholder satisfaction.
2.2 CORPORATE OBJECTIVES FOR 2010-2014
The NHIS has developed a strategic plan to provide direction for the period 2010-2014 to enable
management focus on its core mandate. The plan envisages to achieve the following corporate
objectives:
1. To mobilise 100% of the required funds by the end of 2014.
2. To increase efficiency in the financial operations of the scheme.
3. To increase active membership to 60% of the population by 2014.
4. To increase coverage of the vulnerable including the poor and the indigent to 70% by 2014.
5. To provide support to increase access to quality basic health care services in all districts.
6. To strengthen governance systems and improve human resource capacity.
7. To improve the quality of services accessed by members in the national health insurance
system.
8. To improve the level of provider experience within the NHIS.
9. To improve involvement and participation in health insurance programmes.
3.0 OPERATIONAL ACTIVITIES
Operational activities for the year 2010 are derived from the corporate objectives outlined above.
This section discusses the key activities undertaken within the year.
3.1 SUSTAINABILITY AND COST CONTAINMENT
Sustainability and cost containment were major issues that engaged management’s attention during
the year under review. Pursuant to that, a Clinical Audit Division was set up to embark on regular
claims verification exercises to assure provision of quality health care services and to minimize
financial leakages resulting from provider-side moral hazards.
The internal audit department was also upgraded to a division to empower it to effectively monitor
the financial and operational processes within the NHIS. The activities of these two divisions have
contributed immensely to the reduction in financial leakages and strengthening of internal controls.
They have also contributed to the stimulation of behavioural change among health care providers
and schemes officials. Providers and scheme officials who were found to have abused the system
were sanctioned.
The free maternal health policy was reviewed in order to inject some sanity into the system. An
ultra modern claims processing centre was established to process claims emanating from the
teaching and regional hospitals. The year under review also witnessed the commencement of
initiatives to introduce capitation as an additional provider payment mechanism to allow providers

2010 ANNUAL REPORT
16
and subscribers to share the risks associated with the provision and utilisation of health care
services at the health facilities.
3.2 MEMBERSHIP AND ID CARD MANAGEMENT
3.2.1 Membership trend
The NHIS has made significant progress towards extending health insurance coverage to residents
of Ghana. The cumulative membership of the scheme has increased from 1.3 million in 2005 to 18
million in 2010. This represents an average annual growth of 68% over the entire period.
The NHIA undertook methodology and data validation exercise, during the first quarter of 2011, to
ascertain the accuracy of the 2010 membership database. During the exercise, it was realized that
the old methodology of calculating active membership was riddled with inherent challenges. The
old methodology calculates active membership by subtracting the number of all expired ID cards
since inception of the scheme from the sum of all ID cards issued and ID cards renewed since
inception of the scheme.
The challenges indentified with this methodology are as follows:
1. The cumulative number of ID cards issued includes members who have engaged in
multiple registrations and thus over estimated the number of ID card holders.
2. The cumulative number of ID cards issued includes members who have died and thus also
over estimated the number of ID card holders.
3. The cumulative number of expired ID cards was not accurately tracked and therefore was
underestimated.
Clearly, due to these challenges, the number of active members reported over the years may be
inaccurate. In order to mitigate these challenges, a new and appropriate methodology was used to
determine the 2010 active membership. This new approach is based on the sum of the number of
new members registered for a given year and the number of renewals made for that year.
To further improve the quality of the data, the ICT platform was used in the extraction of the
number of new and renewing members for 2010. Previously, active membership reports were based
on manual reports submitted to Operations division from the schemes. Table 1 gives the trend for
active membership based on the old methodology up to 2009. Given that we could not apply the
new ICT-based methodology in retrospect to report active membership for the previous periods, the
new methodology was used for reporting only the 2010 active membership, and will be applied
going forward.
Table 1: Active Membership
Methodology 2005 2006 2007 2008 2009 2010
Old
1,348,160
2,521,372
6,643,371
9,914,256
10,638,119 N/A
New N/A N/A N/A N/A N/A
8,163,714
The new active membership figure of 8.16 million for 2010 does not necessarily represent a drop, as
there is no comparative historic data based on the new methodology.

2010 ANNUAL REPORT
17
While the perceived drop in active membership is largely due the application of the new
methodology for reporting, other sub-standard practices from the schemes such as the issuing of old
ID cards, the granting of validity period exceeding three months for temporary cards and the
printing of temporary ID cards outside the NHIS ICT system make the reported new active
membership data look lower than expected. Table 2 shows the number of new members, renewals
and active membership distribution by region.
Table 2: New Members, Renewing and Membership in 2010 Active
Region 2010
New Members
2010
Renewals
2010
Active Members
Ashanti 606,349 978,748 1,585,097
Brong Ahafo 323,092 691,462 1,014,554
Central 303,592 189,125 492,717
Eastern 316,861 613,482 930,343
Greater Accra 492,443 469,012 961,455
Northern 349,899 421,436 771,335
Upper East 238,935 278,932 517,867
Upper West 158,911 202,154 361,065
Volta 263,050 318,255 581,305
Western 466,458 481,518 947,976
Ghana 3,519,590 4,644,124 8,163,714
The total active membership of 8,163,714 as at December 2010 represents 34% of the total
population in 2010. Upper West Region had the highest active population coverage rate of 53%
whiles Central Region recording the lowest active coverage rate of 23%. Figure 2 shows the NHIS
active membership coverage by region.
Figure 2: Active membership as percent of population by region in 2010
34%
44%
23%
36%
25%
31%
50% 53%
28%
41%
0%
10%
20%
30%
40%
50%
60%
Ashanti BrongAhafo
Central Eastern GreaterAccra
Northern UpperEast
UpperWest
Volta Western

2010 ANNUAL REPORT
18
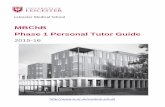
Figure 3 shows the distribution of active members of 8,163,714 as at December 2010 by category -
Informal, SSNIT Contributors, SSNIT Pensioners, Under 18 years, 70 years and above, Pregnant
women and indigents.
Figure 3: Active NHIS Subscribers by Category 2010
3.2.2 Special registration exercise
In September 2010, the National Health Insurance Authority embarked upon a special registration
exercise as a means of increasing NHIS membership coverage. The programme predominantly
targeted the poor and vulnerable in their local communities and at large congregation centres such
as churches, mosques and markets. The exercise was conducted across the country to allow new
members to register and old members to renew their membership. Registered members were issued
NHIS cards within a period of one month. This arrangement encouraged many people to patronise
the special registration exercise.
Under 18 years 47.7%
70 years & above 5.4% Indigents
1.4%
SSNIT contributors
4.7%
SSNIT pensioners
0.4%
Pregnant women
8.6%
Non-exempt group (Informal
sector) 31.8%

2010 ANNUAL REPORT
19
National Chief Imam, Sheikh Osman Nuhu Sharabutu (seated, middle), being registered at Old Fadama, Accra during the special registration exercise.
The special registration brought an additional 276,300 people unto the scheme. Regional
breakdown of members registered during the exercise is shown in table 3 below.
Table 3: Total number of members registered under the special registration exercise
Region Total number of members registered
ASHANTI 6,830
BRONG AHAFO 23,192
CENTRAL 31,882
EASTERN 4,993
GREATER ACCRA 39,048
NORTHERN 11,031
UPPER EAST 47,216
UPPER WEST 8,296
VOLTA 80,152
WESTERN 23,660
TOTAL (NATIONAL) 276,300
3.2.3 Free maternal health care
The free maternal care programme was introduced in July 2008 to help Ghana meet Millennium
Development Goals (MDG) 4 and 5. Under this programme pregnant women are to receive free
medical care. However, due to abuse of the system, NHIA revised the implementation guidelines in
2010 to encourage pregnant women to register with the scheme before accessing healthcare. As at
the end of 2010, a cumulative total of 1,394,445 pregnant women (PW) representing 7.7% of total
number registered had subscribed to the scheme.

2010 ANNUAL REPORT
20
3.2.4 ID cards production and distribution
During the year under review, a total of 3,950,502 ID cards were printed, out of which 3,450,822,
representing 87.35% were distributed. A total of 499,680 ID were not distributed as at the close of
the year (see table 4).
Table 4: ID Cards production and distribution by region
Region
Number of ID Cards printed
Number of ID Cards distributed
Number of Undistributed cards
Ashanti
734,946 695,517 39,429
Brong Ahafo
379,099 350,449 28,650
Central
261,092 215,909 45,183
Eastern
476,746 410,743 66,003
Greater Accra
462,583 405,373 57,210
Northern
374,128 320,694 53,434
Upper East
223,774 164,063 59,711
Upper West
258,133 253,469 4,664
Volta
351,557 275,568 75,989
Western
428,444 359,037 69,407
Total (National)
3,950,502 3,450,822 499,680

2010 ANNUAL REPORT
21
3.3 CLAIMS MANAGEMENT
3.3.1 Outpatient utilization
Outpatient utilization has increased by over twenty-eight fold from 0.6 million in 2005 to 16.9
million in the year 2010. Figure 4 presents outpatient utilization trend from 2005 to 2010.
Figure 4: Outpatient Utilization Trend
3.3.2 Inpatient utilization
Inpatient utilization increased over thirty fold from 28,906 in 2005 to 973,524 in 2009 but dropped
to 724,440 in 2010. The decline in utilization in 2010 could be attributed to the following reasons;
Members are seeking early treatment and thereby reducing inpatient cases
Primary healthcare is becoming more efficient
Detentions were being billed as inpatients in prior years instead of outpatient
Providers are changing their behaviour due to effective clinical audit
Figure 5 presents Inpatient utilization trend from 2005 to 2010.
597,859
2,434,008
4,648,119
9,339,296
16,629,692 16,931,263
0
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000
14,000,000
16,000,000
18,000,000
2005 2006 2007 2008 2009 2010

2010 ANNUAL REPORT
22
Figure 5: Inpatient Utilization Trend
3.3.3 Claims payment trend
Claims payment is the major cost driver of the scheme. Claims payments has increased from
GH¢7.60 million in 2005 to GH¢ 394.27 million in 2010. The total amount of GH¢ 394.27 million
disbursed for the payment of claims represent 76.2% of the total expenditure of the scheme. Figure
6 shows the trend in claims payment from 2005 to 2010.
Figure 6: Claims Payment Trend (Ghøm)
28,906
135,221
303,930
627,795
973,524
724,440
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
1,000,000
2005 2006 2007 2008 2009 2010
7.60
35.48
79.26
198.11
322.91
394.27
0.00
50.00
100.00
150.00
200.00
250.00
300.00
350.00
400.00
450.00
2005 2006 2007 2008 2009 2010

2010 ANNUAL REPORT
23
3.4 ICT AND DATA MANAGEMENT
During the period under review, management sought to improve the ICT system and its data
management by improving existing claims module to encourage usage by the schemes, introducing
rule-based engine for effective electronic claims processing and rolling out electronic claims
submission.
Printing of temporary ID cards from the NHIS ICT application was started to minimize the
extension of benefit period of members. A template for linking diagnosis to treatment was also
designed.
3.5 PROVIDER ACCREDITATION AND QUALITY ASSURANCE
The National Health Insurance Scheme Act, 2003 (Act 650) mandates the NHIA to accredit service
providers before they can provide service to NHIS members. The primary goal is to ensure that
healthcare services offered to card bearing members are of good quality. In pursuance of this,
inspection of the first and second batches of health facilities was carried out in 2009. In 2010, a
third batch of 915 facilities were inspected out of which 849 were accredited. Total accredited
health facilities as at 31st December 2010 were 2,647. Table 5 summarizes the accreditation results.

2010 ANNUAL REPORT
24
Table 5: Accreditation results
SUMMARY OF NHIA ACCREDITED FACILITIES AS AT DECEMBER 2010
FACILITIES BY TYPES
1ST BATCH
2ND BATCH
3RD BATCH TOTAL
FACILITIES BY GRADE
1ST BATCH
2ND BATCH
3RD BATCH TOTAL
CHEMICAL SHOPS 50 69 60 178 GRADE A+ 2 4 0 6
CHPS ZONE 74 343 308 714 GRADE A 21 35 19 75
CLINICS 82 107 58 255 GRADE B 86 267 151 507
DENTAL CLINIC 0 0 2 3 GRADE C 139 536 380 1066 DIAGNOSTIC CENTRES 0 13 6 19 GRADE D 278 330 279 887
EYE CLINIC 0 3 3 6 PROVISIONAL 48 52 20 106 HEALTH CENTRES 73 347 242 658 TOTAL 574 1224 849 2647
LABORATORIES 22 21 15 59 MATERNITY HOMES 120 58 22 198
PHARMACIES 76 94 65 238
POLYCLINICS 1 9 2 12 FACILITIES BY REGIONS
1ST
BATCH 2
ND
BATCH 3
RD
BATCH TOTAL PRIMARY HOSPITALS 58 150 54 267 ASHANTI 138 268 50 456
PYHSIOTHERAPY 0 0 0 0 BRONG AHAFO 45 99 138 282
SECONDARY HOSPITAL 4 3 2 9 CENTRAL 107 82 28 217 TERTIARY HOSPITAL 0 1 0 1 EASTERN 86 181 91 358
ULTRASOUND 14 6 10 30 GREATER ACCRA 64 126 98 288
TOTAL 574 1224 849 2647 NORTHERN 27 161 83 271
UPPER EAST 38 77 40 155
FACILITY BY OWNERSHIP
1ST
BATCH 2
ND
BATCH 3
RD
BATCH TOTAL UPPER WEST 1 31 102 134
GOVERNMENT 167 741 564 1460 VOLTA 22 89 83 194
MISSION 11 106 29 149 WESTERN 46 110 136 292
PRIVATE 395 367 250 1022 TOTAL 574 1224 849 2647 QUASI GOVERNMENT 1 10 6 16
TOTAL 574 1224 849 2,647
3.5.1 Collaboration
NHIA is collaborating with PharmAccess, a Dutch Non Governmental Organization (NGO) in the
accreditation exercise. The NGO has supported the training of accreditation surveyors, provided
Personal Digital Assistance (PDAs) and software for analyzing the data as well as 10 laptop
computers for capturing data on the field, and a server to house accreditation data.

2010 ANNUAL REPORT
25
3.6 ADMINISTRATION AND HUMAN RESOURCE
In 2010, the National Health Insurance Council approved an organisational structure proposed by
management. As at the end of the year, 358 employees of diverse skills were at post at both the head
office and the regional offices. Employees also benefited from various training and development
programmes. In all, 48 different training programmes were organised for a total of 265 participants
(see annex 6).
The year also witnessed salary rationalisation exercise that sought to address distortions in the
salaries of employees. 75 employees faced various disciplinary actions, ranging from queries to
dismissals, on grounds of deviant behaviour.
3.7 PLANNING, MONITORING, EVALUATION, RESEARCH AND DEVELOPMENT
To provide strategic direction to the operations of NHIA, a ten-member Technical Committee was
formed by NHIA management with SCAD as the lead division to draft a strategic plan for the
NHIA. The committee started work in September and will continue in the ensuing year to complete
the process.
Weekly management meetings were held throughout the year to review activities and plan for
ensuing weeks to ensure management was on course. Two management seminars were also held as
part of the monitoring and evaluation process to keep the organization on course.
Besides routine monitoring and supervision by the regional office staff, the head office operations
division embarked on support visits to nine regions and 57 schemes. On the average, four health
facilities per region were also visited.
Research was conducted to find out the views of major stakeholders on the NHIS medicines list.
The results of the research informed the revision of the list and prices. Ministry of Health approved
prescribing levels were also incorporated into the NHIS medicines list. A uniform prescription form
was also designed in collaboration with the MOH and major provider groups. This will be piloted in
Greater Accra Region in 2011.
3.8 PROJECTS AND PROCUREMENTS
The construction of the Head Office continued and reached 93% completion during the year.
Contracts were awarded for the construction of ten regional office buildings. The Claims Processing
Centre was established and furnished for centralised claims processing to commence during the
year. Six million NHIS ID cards were procured during the year. 64 bicycles were also procured for
schemes who needed them for their outreach programmes.

2010 ANNUAL REPORT
26
3.9 COMMUNICATION AND STAKEHOLDER ENGAGEMENT
Prior to 2010, irregular communication between NHIS and its major stakeholders was identified as
a challenge at almost all forums which were organized. Hence, management saw improvement in
communication with stakeholders as very important. Efforts were therefore made to enhance
communication and engagement with stakeholders.
3.9.1 Stakeholder engagement
In line with the objective of strengthening collaboration between NHIA and its key stakeholders, a
two-day stakeholders meeting was held in Kumasi in April. Participants for the meeting included all
Medical Superintendents of Ghana Health Service, Christian Health Association of Ghana, Private
Health facilities and representatives of Pharmacy Council. Key issues discussed were the clinical
audits findings, claims management experiences, abuse and fraud in the system, among others. The
meeting ended successfully with participants resolving to contribute positively towards the
sustainability of the scheme.
3.9.2 Policy fair
As a way of showcasing the achievements of NHIS, the Authority participated in a five-day policy
fair organized by the Ministry of Information from the 27th
April to 1st May, 2010. The purpose of
the fair was to offer Ministries, Departments and Agencies (MDAs) the opportunity to showcase
their policies, programmes and activities and to enable the general public have direct contact with
the leadership of those MDA’s. On display at NHIS stand were the NHIS benefit package, major
reform initiatives and other ongoing activities. The Chief Executive of NHIA made a presentation
at the policy fair during which he explained the operations of the NHIS to the general public.
Group picture of Chief Executive and Participants at NHIA stand
Directors at the fair
3.9.3 End of year get-together and awards night
NHIA held its maiden awards night to show appreciation to its cherished service providers and
district schemes that performed creditably during the year. The awards ceremony took place on the
10th
of December 2010 at the Dome, Accra International Conference Centre. In attendance were all

2010 ANNUAL REPORT
27
staff of NHIA, District Schemes in the Greater Accra Region, Council Members, Members of the
Parliamentary Select Committee on Health, Development Partners, Representative of Ghana Health
Service and Ministry of Health. One scheme and one service provider were selected from each
region for the award. Special awards were also given to the President of Ghana Medical Association
and the Director General of the Ghana Health Service. The night was also used by management to
socialize with district schemes staff, service providers, development partners and other invited
guests.
WHO Country Representative, Dr. Daniel Kertesz, (left) presenting an
award to GMA President, Dr. Adom Winful.
3.9.4 Media engagement
Several media (print and electronic) were used to market NHIS to the public. Special jingles were
developed on the importance of NHIS and the need to register with the scheme, free maternal care
programme and fraud and abuse. Live Presenter Mention (LPM) was also developed on providers
and client responsibilities. The jingles and the LPM were aired on popular radio/FM stations in
Accra and other parts of the country.
Various directors, deputy directors and managers in NHIA were used in the communication
process. The strategy was to allow managers to disseminate information on their areas of expertise
through radio and television interviews thereby stepping up the level of ownership of issues. To
ensure closer monitoring of the media landscape, the NHIA commenced daily media content
analysis of issues affecting NHIS. The analysis is circulated to all directors for their input and
comments and for the necessary actions.

2010 ANNUAL REPORT
28
WHO/UNDP EXCELLENCE AWARD

2010 ANNUAL REPORT
29
4.0 ACHIEVEMENTS
4.1 INCREASED COVERAGE
The major success story of NHIS is its high patronage by residents in Ghana. As at 31st December
2010, over 18 million Ghanaians had subscribed to the scheme out of which over 8 million
representing 34% of the population are active card bearers. The high patronage attests to the fact
that Ghanaians have embraced the NHIS as the preferred health care financing mechanism.
4.2 UNDP/WHO EXCELLENCE AWARD
Ghana received an award from the United Nations Development Programme and the World Health
Organization for showing leadership in health insurance implementation within the southern
countries. It was in recognition of Ghana’s leadership role in providing financial risk protection
against cost of health care services for its population, especially the poor and vulnerable in society.
Mr. Sylvester A. Mensah receiving the award in Geneva Switzerland
4.3 FINANCIAL AND CLINICAL AUDITS
The establishment of Clinical audit division and strengthening of the internal audit division in 2010
resulted in huge cost savings to NHIS. Clinical audit alone recovered a total of GH¢16.8 million
from service providers. The exercise also helped in ensuring quality service delivery to NHIS
members. Generally, the activities of the two divisions helped in reducing financial leakages and
strengthened internal controls at both the district schemes and service provider ends.

2010 ANNUAL REPORT
30
4.4 REVIEW OF MEDICINES LIST
The NHIS Medicines List was developed in 2008 to serve as a guide to health providers in
delivering healthcare services to NHIS subscribers. The List contains medications in the various
therapeutic groupings used in the management of disease conditions covered under the benefit
package of the National Health Insurance Scheme, which forms over 95% of disease conditions in
Ghana.
Since its inception, the Medicines List has had two reviews with the last review in the last quarter
of 2010. The current List has five hundred and fifty two (552) formulations. In reviewing the
Medicines List, all anaesthetics (both local and general) and programme drugs were removed from
the List. This is because the anaesthetics form part of the tariffs paid for the services rendered while
programme drugs are those used in public health programmes of the Ministry of Health and as such
health providers are not to charge NHIS clients for such medicines.
However, although Sulfadoxine + Pyrimethamine tablet, 525 mg, is a Programme drug, it has been
maintained on the List due to its unavailability at some facilities across the country. This has been
done to prevent malaria in pregnancy and aid the country’s attainment of the Millennium
Development Goal 5 (which is to improve maternal health).
In addition, the following formulations were added to the List. They include:
o Artemether Injection, 40 mg/mL
o Artemether Injection, 80 mg/mL
o Cetirizine softgel Capsule, 10 mg
o Ferrous Gluconate Syrup
o Zinc Tablet, 10 mg
o Zinc Tablet, 20 mg
The Artemether injection formulations were added because of its importance in the treatment of
severe malaria conditions. Cetirizine softgel capsule was added for the benefit of the aged whilst
Ferrous Gluconate syrup was added to the therapeutic group of drugs affecting blood on the List.
Furthermore, the Zinc formulations were added for the treatment of diarrhoea in children as
stipulated in the Standard Treatment Guidelines.
4.5 ACCREDITATION OF HEALTH FACILITIES
In pursuant of NHIA mandate to give accreditation to service providers prior to providing services
to NHIS subscribers, a total of 915 health facilities were inspected in 2010, out of which 849
received formal accreditation. Out of a total number of 2,915 facilities inspected, 2,647 of them
have received formal accreditation since the inception of the exercise in 2009.

2010 ANNUAL REPORT
31
4.6 IMPROVED REIMBURSEMENT TO PROVIDERS
Reimbursement to accredited health care providers improved tremendously during the year under
review. Funds were released to district Schemes for payment of claims on timely basis. NHIA
placed advertisers’ announcement in the dailies reminding providers to submit their claims for
prompt reimbursement and informing them of fund transfers to the various schemes with whom
they have signed service contract. Thus, the issue of delayed reimbursement resulting in withdrawal
of health care service to NHIS clients became a thing of the past.
4.7 GATE-KEEPER SYSTEM AND FREE MATERNAL CARE PROGRAMME
Non enforcement of the gatekeeper system and abuse of the free maternal care programme have
been identified as major contributors to escalating claims which currently accounts for 76.2% of
National Health Insurance Authority (NHIA) total expenditure. To address these challenges, two
stakeholders meetings were held in Koforidua and Kumasi in September and October 2010
respectively, to develop guidelines that are mutually acceptable to stakeholders. Participants at the
meetings included representatives from Ghana Health Service (GHS), Ministry of Health (MOH),
NHIA, Christian Health Association of Ghana (CHAG), Korle–Bu, Komfo Anokye and Tamale
Teaching Hospitals, Ghana Registered Nurses and Midwives Association and Association of
Community Pharmacies. The revised guidelines have been distributed for implementation.
4.8 RISK ASSESSMENT
NHIS is confronted with various risks leading to high operational cost, which emanates partly from
weak controls and non standardization of the entire NHIS operations. To adequately identify and
control these risks, and to make the scheme more sustainable, an eleven-member Risk Assessment
Committee was constituted by NHIA to identify, assess, document and evaluate the various risks
associated with the entire operations of NHIS. The Committee identified 81 risk areas out of which
17% were high, 46% medium and 37% low. The recommendations made by the team are
vigorously enforced by management of NHIA.

2010 ANNUAL REPORT
32
5.0 CHALLENGES
5.1 FINANCIAL SUSTAINABILITY OF THE SCHEME
Financial sustainability of the scheme remains a big challenge to management given the increasing
demand for health insurance and its consequent increase in health care service utilisation. It is
projected that without any additional sources of funding to the current sources, the NHIF risks of
dipping down by the close of year 2012. There is therefore the need to secure additional sources of
funding for the scheme while implementing cost containment strategies to minimise operational
cost.
5.2 IDENTIFICATION OF THE POOR IN THE INFORMAL SECTOR
The national health insurance scheme is a pro-poor programme that focuses much attention on
targeting the poor for exemption. The general perception, however, is that the poor are not
adequately covered by the scheme. The inadequate coverage could be attributed to the difficulty in
identifying them for exemption.
Management has initiated discussion with officials managing the LEAP programme on how best
NHIA and LEAP could collaborate in identifying as many poor as possible for health insurance
coverage. Other methods of targeting the poor for exemption may, however, have to be explored to
improve coverage of the poor.
5.3 ID CARD MANAGEMENT
ID card management is one key constraint facing the scheme. There are delays in members
obtaining their cards on time because there are delays along the entire ID card management chain,
comprising data entry, data batching, card production and distribution. Card distribution constraints
are occasioned by several factors including difficulty in locating places of residence particularly in
the urban centres, change of residence and double registration. 5.4 ICT
There are constraints with the ICT system which need to be addressed to make it more robust.
These include slowness of the system and frequent down time. These challenges, together with the
large numbers of subscribers and low numbers of scheme staff, mostly account for non regular use
of the system at the district scheme level.
5.5 CLAIMS MANAGEMENT
Several challenges have been identified with claims management within the NHIS. There have been
delays in the submission of claims by some service providers, which is frequently occasioned by
inadequate capacity within health facilities in the preparation of claims. The district scheme offices
also do not have adequate capacity to vet claims effectively.

2010 ANNUAL REPORT
33
6.0 OUTLOOK FOR 2011
In 2011, steps will be taken to enhance the financial sustainability of the NHIS, strengthen the ICT
platform, promote continuous service improvement in service provider facilities, strengthen claims
management, improve ID card management, improve human resource capacity and organisational
reforms and take steps to improve the internal and external communication of the NHIS.
To achieve these corporate objectives, the strategies described in the sections below will be
pursued.
6.1 ENHANCE FINANCIAL SUSTAINABILITY OF THE NHIS
Three areas have been identified for addressing the sustainability issue:
6.1.1 Defensive Strategy: Developing cost containment measures to minimise leakages. These will include:
i. Establishing and operationalizing a Consolidated Premium Account to centralise
premium payment into two designated accounts.
ii. Intensifying Clinical Audits in collaboration with provider groups.
iii. Introducing and piloting Capitation as an alternative payment mechanism.
iv. Collaborating with providers and subscribers to enforce the gatekeeper policy of the
Ministry of Health.
v. Linking treatment to diagnosis to improve rational use of medicines.
vi. Implementing uniform prescription forms to promote rational prescribing.
vii. Using mystery shopping to identify inefficiencies and abuse in the entire NHIS system
for redress.
It is also known that over 27% of the scheme’s medicines cost is attributable to anti-malarial
medicines. For example, in 2009 the scheme spent over GH¢ 51 million on anti-malarial medicines
alone. The NHIS will therefore liaise with the Global Fund/Malaria Control Program office in order
to benefit from the Affordable Medicines Facility – Malaria (AMFm) program. Savings from
AMFm is projected to be over 50% annually.
6.1.2 Prudent fund management:
Fund Management and Investment will be strengthened to ensure that NHIA funds are judiciously
managed to generate optimal returns on investments. One strategic investment initiative will be the
development and maintenance of an optimal asset allocation system, through tactical asset timing
and superior investment selection. This is because between 80% and 90% of the performance of the
portfolio is determined by the mix of investment assets held in the portfolio.
Additionally, the NHIS will develop a robust investment research team to continually review the
investment environment, economic policies and capital market expectations for optimal investment
decision making. NHIS will also identify and include in the portfolio, alternative investments with
very low or negatively correlated returns. This is aimed at diversifying away unsystematic risks, for
higher risk adjusted investment returns.

2010 ANNUAL REPORT
34
6.1.3 Sourcing Strategy:
i. Seeking additional funding through policy
The approach is to further diversify our sources of funds by securing additional stable sources of
funds by December 2011, and collaborate with stakeholders to increase the value derived from
these sources by December 2014. Sources to be considered include petro-chemical levy, ‘sin tax’,
DVLA, NHIL increase.
ii. Review premiums
Since they were set in 2004, premiums have not been reviewed. With effect from 2011 premiums
would be reviewed annually to reflect changes in the domestic economy.
iii. Internally-driven fundraising activities
This activity would be treated as ad-hoc programs aimed at raising funds for specific purposes and
activities.
iv. Support from development partners
The NHIS will continue to welcome support from Development Partners (DP). For example, the
Health Insurance Project (HIP) is expected to maintain support for the strengthening of the
purchasing policies and mechanism, and the integrated claims management systems.
6.2 STRENGTHEN THE NHIS ICT
6.2.1 ICT deployment
In 2011, it is expected that nationwide down time of ICT platform will not exceed 5%. A minimum
of 105 additional terminals will be provided to serve key service providers.
To improve service delivery to SSNIT contributors especially at the time of registration and
renewal, business rules between NHIS and SSNIT will be harmonised. Monthly meetings between
the two institutions will be re-introduced effective January 2011.
6.2.2 ICT governance
In view of the strategic role of ICT in the operations of the NHIS, an ICT steering committee
chaired by the Chief Executive will be set-up to help optimise the realisation of value from ICT
investments. At the Council level, a sub-committee on ICT will be set up to provide strategic
direction.
6.2.3 Data integrity
To enhance the integrity of the membership database, the NHIS will embark on a database cleaning
process by incorporating biometric features into its applications. In this regard, the NHIS will
continue discussions and collaboration with other institutions.

2010 ANNUAL REPORT
35
6.3 PROMOTE QUALITY IMPROVEMENT IN SERVICE PROVIDER FACILITIES
One of the key mandates of the NHIS is the assurance of quality within NHIS-accredited health
care service provider facilities. This notwithstanding, at the inception of the scheme, public, quasi-
government and mission health facilities were given blanket provisional accreditation, while private
health care facilities were required to apply for accreditation. Under this arrangement, the health
care facilities were not inspected before being given provisional accreditation.
Since 2009, however, a formal accreditation system has been instituted under which health care
facilities are inspected to ensure that they meet pre-determined criteria before being granted
accreditation. To date, over 2,600 providers have been formally accredited. PharmAccess of the
Netherlands has provided significant support to the accreditation programme of the NHIS.
To promote quality improvements in health care service provision, NHIS will continue with
accreditation and strengthen post-accreditation monitoring. A further 1,000 health care facilities
will be inspected in 2011.
6.4 STRENGTHEN CLAIMS MANAGEMENT
To ensure timely payment of claims to providers, NHIS will implement a claims management
system that is complete with a rules-based engine and workflow management software. To support
the migration to electronic processing, the current claims module used at the schemes will be
enhanced to make it more user-friendly. The pilot for this enhanced module has been completed in
three schemes in the Greater Accra Region and rollout to the other regions will be completed by
July 2011.
The NHIS intends to centralize claims at three zones. The first zonal CPC will become operational
in 2011. This initiative is expected to bring efficiency and effectiveness in the processing of claims.
6.5 IMPROVE ID CARD MANAGEMENT
NHIA will institute measures to improve the production and distribution of ID cards in order to
make the NHIS card the most respected and trusted local card. The internal processes will be
reviewed and streamlined to clearly define roles and responsibilities at all levels of the production
and distribution chain. A manual will be developed to serve as a guideline to improve the processes
involved in ID card management.
6.6 HUMAN RESOURCE CAPACITY AND ORGANISATIONAL REFORMS
The following activities shall be undertaken as part of capacity strengthening within the NHIS:
6.6.1 Attracting, developing and retaining relevant human resource
The NHIA will attract, develop and retain relevant human resource capacity by providing a positive
and engaging working environment. It will recognise, reward and reinforce the right behaviour and
attitudes. It will also involve and engage employees through communication and feedback
mechanisms in the daily administration of the scheme. NHIS will utilise robust and focused training
and career development programs to create a match between training needs, people opportunities
and corporate goals while conducting continuous monitoring, evaluation and measurement of
progress to remove de-satisfiers and reinforce what satisfies people.

2010 ANNUAL REPORT
36
NHIA will continue with the revision of the entire conditions of service for staff. New schemes
such as a provident fund will be included in line with best practice with the view to securing
financial security of staff. Other welfare packages, such as annual medical checkups and
counselling services, will be implemented to motivate staff.
6.6.2 Organizational reforms
The successful implementation of the strategies highlighted in the preceding sections calls for some
organisational reforms in structure and function. The case for an organisational review is further
strengthened by the proposed new law that makes the scheme unitary.
A new structure that allows for the creation of two Deputy Chief Executives (DCEs) is proposed.
The creation of two DCEs calls for a thinning of the total number of directorates currently within
the NHIS. In this regard, the NHIS intends to reduce the total number of divisions to nine by the
end of 2011.
To make up for any gap that would be created by the above arrangements, and to strengthen staff
quality and capacity at the district/scheme level, District Director (DD) positions will be created in
all 145 districts across the country by the end of 2011.
6.6.3 Ghana Health Insurance Institute
The National Health Insurance Scheme has been acclaimed worldwide for showing leadership in
social health insurance implementation within the South-South regions, culminating in an
international award in 2010. The design of the scheme is an innovation and several other innovative
systems have been developed and implemented within the NHIS. These include the accreditation
system, institutionalised clinical audits, the Ghana Diagnosis Related Groupings, the NHIS
Medicines List, the Claims Processing Centre and a nationwide ICT platform. Members of staff
within the scheme have also had the opportunity of exposure to best practices and to present papers
around the world.
Thus the NHIS has experiences worth sharing with Africa and the world at large. There are
therefore plans to develop a Ghana Health Insurance Institute for in-country capacity building and
for sharing ideas and experiences with practitioners in Africa and beyond.
As a first step, a committee will be set up to develop a proposal that outlines the roadmap for the
establishment of the institute.
6.7 Communication and marketing strategies
6.7.1 Internal and external communication
The communication strategy takes cognisance of the need to be proactive in educational,
sensitisation and general information activities. It differentiates between internal and external
communications. Internal communications would be targeted at staff and council, while external
communications would be targeted at the general public and the international community.

2010 ANNUAL REPORT
37
Through monitoring and evaluation of the activities of the various divisions, there will be timely
internal communications to draw attention to shortfalls. Standards will be developed for this.
All types of media, from drama and information services vans at the community level to new media
such as mobile telephony and the internet, will be engaged.
Specifically, the following will be done:
i. Preparation and submission of monthly snapshot reports to the Ministry of Health,
Parliamentary Select Committee on Health (PARSCOM/Health) and to the NHIA Council
ii. Quarterly presentations/interaction with parent Ministry, Ministry of Information and other
relevant MDAs
iii. Quarterly press interactions
iv. Semi-annual staff durbars
v. Semi-annual interaction with the Press
vi. Annual interaction with stakeholders – providers and members, separately.
6.7.2 Communication with service providers
To improve communication between the scheme and service providers, management will develop
direct communication relationships with them. To retain technical links with providers, M&E
Manager for Claims/Provider Services and M&E Manager for Membership will be appointed in all
10 regional offices in 2011. These managers will serve as the main contact and information bank
through which other divisions will relate to providers, subscribers and other stakeholders.
A call centre will also be established to facilitate communication with subscribers and other
stakeholders and to resolve issues and challenges promptly. Public Relations Officers in the district
schemes will be empowered to play active roles in the mainstream communication and public
education at the district and regional levels.
As part of measures to position the NHIS website as a key communication medium and to facilitate
quicker update on the initiatives envisaged for 2011 and beyond, management will re-engineer the
NHIS website to match up to the task and to give the NHIS a reputable global image.
As part of its international marketing strategy, the NHIS will do some publications in international
journals, attend conferences and workshops to share experiences with the global community. Management will also, continuously engage staff through staff durbars, one-on-one interactions and
get-togethers. Opportunities will also be created to receive feedback on policies, programmes and
decisions.

2010 ANNUAL REPORT
38
7.0 CONCLUSION Over the past six years, particularly the last one-and-half years, the NHIA has seen significant
improvement in its operational results culminating in the attainment of an international award from
UNDP/WHO in November 2010. There was significant reduction in claims re-imbursement period
from over 90 days to 60 days on average. Other achievements include increase in membership
enrolment and increase in number of accredited facilities to improve physical access to healthcare.
These achievements have been recorded in the midst of numerous challenges, giving testimony to
the effectiveness of prudent strategies adopted by management.
To consolidate the gains made so far, management is determined to meet the aspirations of
Ghanaians by introducing far reaching innovations that will ensure an efficient and responsive
scheme.

2010 ANNUAL REPORT
39
ANNEXES

2010 ANNUAL REPORT
40
ANNEX 1: Financial Statement
NHIA FINANCIAL STATEMENT (UNAUDITED)
NATIONAL HEALTH INSURANCE AUTHORITY (NHIA)
INCOME AND EXPENDITURE ACCOUNT FOR THE YEAR ENDED
31 DECEMBER, 2010
2010 2009
GH ¢ GH ¢
Levies 401,848,524.08 329,459,128.92
Investment Income 58,708,664.99 75,638,686.50
Other Income 308,784.37 2,412,772.32
460,865,973.44 407,510,587.74
Subsidies and Claims 397,610,425.00 359,956,868.90
Administrative &
Logistical 23,300,837.11 8,346,070.31
Support to Partner
Institutions 65,080,841.83 41,870,416.36
Operational &
Administrative Expenses 22,133,809.61 16,883,796.75
508,125,913.55 427,057,152.32
Deficit Transferred to
Accumulated Fund (47,259,940.11) (19,546,564.58)
NATIONAL HEALTH INSURANCE AUTHORITY (NHIA)
ACCUMULATED FUND FOR THE YEAR ENDED
31ST DECEMBER, 2010
2010 2009
GH ¢ GH ¢
Balance b/f 443,263,968.13 462,495,574.80
Prior Year Adjustment
314,957.91
Deficit Transferred from
Income & Expenditure (47,259,940.11) (19,546,564.58)
Accumulated Fund For
the year 396,004,028.02 443,263,968.13

2010 ANNUAL REPORT
41
NATIONAL HEALTH INSURANCE AUTHORITY (NHIA)
BALANCE SHEET AS AT THE YEAR ENDED
31ST DECEMBER, 2010
2010 2009
Fixed Asset GH ¢ GH ¢
Property, Plant and
Equipment 48,011,901.46 35,943,972.47
Investments 284,487,882.28 437,818,825.16
332,499,783.74 473,762,797.63
Current Assets
Interest Receivable 15,902,358.94 37,528,128.94
NHIL Receivable 179,207,690.75 63,612,196.55
Other Receivable 1,330,417.37 906,445.95
Bank and cash 13,508,602.25 5,715,260.29
Total Current Assets 209,949,069.31 107,762,031.73
Total Assets 542,448,853.05 581,524,829.36
Funds & Liabilities
Accumulated Fund 396,004,028.02 443,263,968.13
Current Liability
Claims Payable 114,459,682.43 110,261,804.23
Accured Support to
Partner Institutions 23,973,822.18 23,417,000.00
Other Accounts Payables 8,011,320.42 4,582,057.00
Total Current Liabilities 146,444,825.03 138,260,861.23
Total Fund and
Liabilities 542,448,853.05 581,524,829.36

2010 ANNUAL REPORT
42
NATIONAL HEALTH INSURANCE AUTHORITY (NHIA)
CASH FLOW STATEMENT FOR THE YEAR ENDED 31ST DECEMBER, 2010
2010 2009
Cashflow from Operating
Activities GH ¢ GH ¢
Deficit (47,259,940.11) (32,518,697.37)
Add Depreciation 9,286,605.74 449,813.94
Increase in Receivables (94,393,695.62) 55,883,103.27
Increase Payables 8,183,963.80 133,179,199.24
Decrease in Premium
Deposits - 964,394.25
Net inflow from operating
activities (124,183,066.19) 157,957,813.33
Decrease in Fixed
Deposits (Short Term) 153,330,942.88 (158,287,910.97)
Investing Activities
Property, Plant &
Equipment Acquisition (21,354,534.73) (21,801,885.34)
Net Decrease in Cash &
Cash Equivalent 7,793,341.96 (22,131,982.98)
Cash & Cash Equivalent as
at 01/01/10 5,715,260.29 27,847,243.27
Net Cash & Cash
Equivalent as at 31/12/09 13,508,602.25 5,715,260.29

2010 ANNUAL REPORT
43
ANNEX 2: Minimum health care package under NHIS
1. Out-Patient Services
A) Consultation including reviews. These include both general and specialist
consultations.
B) Requested investigations including laboratory investigation, x-rays and ultrasound
scanning for general and specialist out-patient services.
C) Medication, namely, prescription drugs on National Health Insurance Drugs List,
traditional medicines approved by the Food and Drugs Board and prescribed by
accredited medical and traditional practitioners.
D) HIV/AIDS symptomatic treatment for opportunistic infection.
E) Out-patient/Day Surgery Operations including hernia repairs, incision and drainage,
haemorrhoidectomy.
F) Out-patient Physiotherapy.
2. In-Patient Services
A) General and Specialist in-patient care
B) Requested investigations including laboratory investigations, x-rays and ultrasound
scanning for in-patient care.
C) Medication; namely, prescription drugs on National Health Insurance Drugs List,
traditional medicines approved by the Food and Drugs Board and prescribed by
accredited medical and traditional medicine practitioners, blood and blood products.
D) Cervical and Breast Cancer Treatment
E) Surgical Operations
F) In-patient Physiotherapy
G) Accommodation in general ward
H) Feeding (where available)
3. Oral Health Services
A) Pain Relief which includes incision and drainage, tooth extraction and temporary
relief.
B) Dental Restoration which includes, Simple Amalgam Fillings and Temporary
Dressing.
4. Eye Care services
A) Refraction
B) Visual Fields
C) A-Scan
D) Keratometry
E) Cataract Removal
F) Eye lid Surgery

2010 ANNUAL REPORT
44
5. Maternity Care
A) Antenatal Care
B) Deliveries; namely, normal and assisted
C) Caesarian Section
D) Postnatal care
6. Emergencies
A) All emergencies shall be covered. These refer to crisis health situation that demand
urgent intervention and include:
B) Medical emergencies
C) Surgical emergencies including brain surgery due to accidents.
D) Paediatric emergencies
E) Obstetric and Gynaecological emergencies including caesarian sections
F) Road Traffic Accidents
G) Industrial and workplace accidents
H) Dialysis for acute renal failure
EXCLUSION LIST The following health care services are excluded:
A) Rehabilitation other than physiotherapy
B) Appliances and prostheses including optical aid, hearing aids, orthopedic aids,
dentures
C) Cosmetic surgeries and aesthetic treatment
D) HIV retroviral drugs
E) Assisted Reproduction e.g. Artificial insemination and gynaecological hormone
replacement therapy
F) Echocardiography
G) Photography
H) Angiography
I) Orthoptics
J) Dialysis for chronic renal failure
K) Heart and Brain surgery other than those resulting from accidents.
L) Cancer treatment other than cervical and breast cancer
M) Organ transplanting
N) All drugs that are not listed in the NHIS Drug list
O) Diagnosis and treatment abroad
P) Medical examinations for purposes of visa applications, educational, institutional,
driving license
Q) VIP ward (Accommodation)
R) Mortuary Services

2010 ANNUAL REPORT
45
ANNEX 3: Unit heads and managers
UNIT HEADS AND MANAGERS
# NAME DIVISION POSITION
1 Amadu Ali Claims Claims Manager
2 Collins Danso Akuamoah Strategy & Corporate Affairs Strategy Manager
3 Daniel K. Amekudzi Admin & Gen. Counsel HR Manager -Talent &
Recruitment
4 Diana Oye Ahene (Ms.) Admin. / CE's Secretariat Personal Assistant to CE
5 Abena Agyeiwaa Amoako (Dr.) Operations Provider Relations Manager
6 Edward Buckman ICT Information Systems
Manager
7 Francis Sampana Zuure Internal Audit Audit Senior
8 George Omaboe Internal Audit Audit Manager
9 George Asamoah Baah Finance Finance Manager
10 George G. Amoo Clinical Audit Clinical Audit Manager
11 Iddrisu Hudu Claims Claims Manager
12 Isaac Marful Dapaah ICT ICT Applications Manager
13 Ismail Osei Clinical Audit Clinical Nurse
14 Maxwell Addico Internal Audit I.T. Auditor
15 Constance Addo-Quaye Adjetey
(Mrs)
Clinical Audit Pharmacist
16 Nicholas Afram Osei Claims Senior Claims Manager
17 Nii Anang Adjetey (Dr.) Strategy & Corporate Affairs Communications Manager
18 Prince Debrah Internal Audit Audit Manager
19 Rebecca Akatue (Mrs.) Operations Operations Manager
20 Stella Adu-Amankwa (Mrs.) Strategy & Corporate Affairs Publications Manager
21 Stephen N. Bewong Claims Business Systems Manager
22 Thomas Adoboe ICT IT Infrastructure Manager
23 Vivian Addo-Cobbiah (Mrs.) Operations Accreditation & Quality
Manager
24 Washington Komla Darke Finance Fund Manager
25 William Sabi Operations Operations Manager

2010 ANNUAL REPORT
46
ANNEX 4: Regional Managers
# NAME REGION
1 Afrifa Yamoah Ponko Ashanti
2 Foster Agyei-Korang Brong Ahafo
3 Francis Asante Mensah Western
4 James Mettle Central
5 John Bosco Zury Upper West
6 Lawrence Amartey Greater Accra
7 Nester Akototse Volta
8 Rashid Tanko Northern
9 Roger Aposs Upper East
10 Windham Emil Afram Eastern

2010 ANNUAL REPORT
47
ANNEX 5: Directory of district mutual health insurance schemes
Name of Region Name of scheme Address/location Telephone number
Ashanti
Adansi North Box 21, Fomena Ashanti 0302-216970 EXT 5510/6510
Adansi South Box 1, New Adubiase 0302-216970 EXT 5511/6511
Afigya Sekyere Box 1, Agona Ashanti 0302-216970 EXT 5512/6512
Ahafo - Ano North Box 39, Tepa - Ashanti 0302-216970 EXT 5513/6513
Ahafo - Ano South
Box 9, Mankranso -
Ashanti
0302-216970 EXT
5514/6514
Amansie Central Box 7 Jacobu 0302-216970 EXT 5515/6515
Amansie East
Box 350, Bekwai -
Ashanti 0302-216970 EXT 5516/6516
Amansie West Box 1, Manso Nkwanta 0302-216970 EXT 5517/6517
Asante Akim North Box 214, Konongo 0302-216970 EXT 5518/5518
Asante Akim South Box 12, Juaso 0302-216970 EXT 5519/6519
Asokwa Sub - Metro Box 1916, Kumasi 0302-216970 EXT 5520/6520
Atwima Nwabiagya
Box 17, Nkawie -
Ashanti 0302-216970 EXT 5521/6521
Atwima Mponoa 0302-216970 EXT 5522/6522
Bantama Sub - Metro
Box Kj- 508,Kejetia -
Kumasi 0302-216970 EXT 5523/6523
Bosomtwe - Atwima-
Kwanwoma Box 24, Kuntanase 0302-216970 EXT 5524/6524
Ejisu – Juaben Box 144, Ejisu 0302-216970 EXT 5525/6525
Ejura Sekyeredumase Box 9, Ejura 0302-216970 EXT 5526/6526
Kwabre Box 8, Mamponteng 0302-216970 EXT 5527/6527
Manhyia Sub - Metro Pmb, Adum - Kumasi 0302-216970 EXT 5528/6528

2010 ANNUAL REPORT
48
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Ashanti
Obuasi Municipal Box 32,Obuasi 0302-216970 EXT 5529/6529
Offinsoman Box 281, Offinso 0302-216970 EXT 5530/6530
Sekyere West
Box 360, Mampong -
Ash 0302-216970 EXT 5532/6531
Sekyere East –
Effiduase Box 302, Effiduase 0302-216970 EXT 5532/6532
Subin Sub - Metro
Box Kj - 509, Kejetia -
Kumasi 0302-216970 EXT 5533/6533
Brong Ahafo
Asunafo North Box 237, Goaso 0302-216970 EXT 5534/6534
Asunafo South Box 14, Kukuom 0302-216970 EXT 5535/6534
Asutifi Box 23, Hwidiem 0302-216970 EXT 5536/6536
Atebubu Box 125, Atebubu 0302-216970 EXT 5537/6537
Berekum Box 21, Berekum 0302-216970 EXT 5538/6538
Dormaa Box 94, D - Ahenkro 0302-216970 EXT 5539/6539
Jaman North Box 62, Sampa 0302-216970 EXT 5540/6540
Jaman South Box 56, Drobo 0302-216970 EXT 5541/6541
Kintampo North Box 130, Kintampo 0302-216970 EXT 5542/6542
Kintampo South Box 50, Jema 0302-216970 EXT 5543/6543
Nkoranza District Box 169, Nkoranza 0302-216970 EXT 5544/6544
Pru Box 115, Yeji 0302-216970 EXT 5545/6545
Sene Box 11, Kwame Danso 0302-216970 EXT 5546/6546
Sunyani Municipal Box 2640, Sunyani
0302-216970 EXT
5547/6547
Tain Box 2, Nsawkaw 0302-216970 EXT 5548/6548

2010 ANNUAL REPORT
49
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Brong Ahafo
Tano North Box 24, D/Nkwanta 0302-216970 EXT 5549/6549
Tano South Box 179, Bechem 0302-216970 EXT 5550/6550
Techiman Municipal Box 522, Techiman 0302-216970 EXT 5551/6552
Wenchi Box 75, Wenchi 0302-216970 EXT 5552/6552
Central
Abura-Asebu-
Kwamankese C/O District Assembly 0302-216970 EXT 5615/6615
Agona Box 595, Swedru 0302-216970 EXT 5616/6616
Ajumako Enyan Box 1, Ajumako 0302-216970 EXT 5617/6617
Asikuma Odoben
Brakwa Box 36, B, Asie 0302-216970 EXT 5618/6618
Assin North Box 102, Foso 0302-216970 EXT 5619/6619
Assin South
Box 18,Nsuaem-
Kyekyeware 0302-216970 EXT 5620/6620
Awutu - Effutu –
Senya Box 1, Winneba 0302-216970 EXT 5621/6621
Oguaman – Capecoast C/O District Assembly 0302-216970 EXT 5622/6622
Gomoaman Box Ap 162, Apam 0302-216970 EXT 5623/6623
Komenda-Edina-
Eguafo-Abirem
Box 29,
Elimina0243167295 0302-216970 EXT 5624/6624
Mfantsiman Box 28, Saltpond 0302-216970 EXT 5625/6625
Twifo Hemang Lower
Denkyira Box 182, Twifo - Praso 0302-216970 EXT 5626/6626
Upper Denkyira Box 89, Dunkwa - Offin 0302-216970 EXT 5627/6627
Eastern
Afram Plains Box 43, Donkorkrom 0302-216970 EXT 5598/6598
Akuapem North Box 154, Nsawam 0302-216970 EXT 5599/6599
Akuapem South Box Nw 602, Nsawam 0302-216970 EXT 5600/6600

2010 ANNUAL REPORT
50
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Eastern
Asuogyaman Box Ab 457, Akosombo 0302-216970 EXT 5601/6601
Atiwa Box 14, Kwabeng 0302-216970 EXT 5602/6602
Birim North Box 1, New - Abirem 0302-216970 EXT 5603/6603
Birim South Box 939, Akim Oda 0302-216970 EXT 5604/6604
East Akim Box Ky 174, Kibi 0302-216970 EXT 5605/6605
Fanteakwa Box 113, Begoro 0302-216970 EXT 5606/6606
Kwaebibirem Box 114, Kade 0302-216970 EXT 5607/6607
Manya Krobo
Box 266, Odumasi
Krobo 0302-216970 EXT 5608/6608
New Juaben Boxkf518, Koforidua 0302-216970 EXT 5609/6609
Okwawuman South Box 26, Mpraeso 0302-216970 EXT 5610/6610
Okwawuman West Box 770, Nkawkaw 0302-216970 EXT 5611/6611
Suhum Kraboa Coalta Box Su 260, Suhum 0302-216970 EXT 5612/6612
Yilo Krobo Box 102, Somanya 0302-216970 EXT 5613/6613
West Akim Box 136, Asamankese 0302-216970 EXT 5614/6614
Greater Accra
Ablekuma Box 228, Abossey Okai 0302-216970 EXT 5485/6485
Ashiedu Keteke Box Gt 2152, Accra 0302-216970 EXT 5486/6486
Ayawaso Box 473, Nima 0302-216970 EXT 5487/6487
Dagme East Box Af 179, Ada - Foah 0302-216970 EXT 5500/6500
Dagme West Box Dd 195, Dodowa 0302-216970 EXT 5501/6501
Ga District Box 1, Amasaman 0302-216970 EXT 5502/6502

2010 ANNUAL REPORT
51
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Greater Accra
Kpeshie Box Os 1979, Osu 0302-216970 EXT 5503/6503
Okaikoi Box 101, Sakum - Estate 0302-216970 EXT 5488/6488
Osu- Klottey Box Ad 133, Adabraka 0302-216970 EXT 5489/6489
Tema Box 301, Tema 0302-216970 EXT 5505/6505
Northern
Bole Box 72, Bole 0302-216970 EXT 5553/6553
Bunkpurugu Box 11, Nakpanduri 0302-216970 EXT 5554/6554
Central Gonja 0302-216970 EXT 5556/6556
East Gonja Box 9, Salaga 0302-216970 EXT 6555/7555
East Mamprusi Box 41,Gambaga 0302-216970 EXT 5557/6557
Gushegu Box 1, Gushegu 0302-216970 EXT 5558/6558
Karaga 0302-216970 EXT 5559/6559
Nanumba Box 1, Bimbilla 0302-216970 EXT 5560/6560
Nanumba South Box 1, Wulensi 0302-216970 EXT 6561/7561
Saboba/Cherekponi Box 42, Saboba 0302-216970 EXT 5562/6561
Savelugu/ Nanton B0x 1, Savelugu 0302-216970 EXT 5562/6563
Sawla-Tuna-Kalba 0302-216970 EXT 5643/6643
Tamale 0302-216970 EXT 5564/6543
Tolon/Kumbungu Box 2531, Tamale 0302-216970 EXT 5565/6565
West Gonja Box Dm 97, Damongo 0302-216970 EXT 6566/7566
West Mamprusi Box 6, Walewale 0302-216970 EXT 5567/6567
Yendi B0x 1, Yendi 0302-216970 EXT 5568/6568
Zabzugu/Tatale Box 1, Zabzugu 0302-216970 EXT 5569/6569

2010 ANNUAL REPORT
52
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Upper East
Bawku Municipal Box 1, Bawku 0302-216970 EXT 5570/6570
Bawku West Box 1, Zebella 0302-216970 EXT 5571/6571
Bolga 0302-216970 EXT 5572/6572
Bongo Box 1, Bongo 0302-216970 EXT 5573/6573
Builsa Box 3, Sandema 0302-216970 EXT 5574/6574
Kasena-Nankana Box 94, Navrongo 0302-216970 EXT 5575/6575
Upper West
Jirapa Box 1, Jirapa 0302-216970 EXT 5576/6576
Lawra Box 23, Lawra 0302-216970 EXT 5577/6577
Nadowli Box 40, Nadowli 0302-216970 EXT 5578/6578
Sissala East Box 107, Tumu 0302-216970 EXT 5579/6579
Sissala West C/O Box 107, Tumu 0302-216970 EXT 5580/6580
Wa Municipal Box 587, Wa 0302-216970 EXT 5581/6581
Wa West C/O Box 587, Wa 0302-216970 EXT 5582/6582
Wa East C/O Box 587, Wa 0302-216970 EXT 5583/6583
Volta
Adaklu Anyigbe Box Ap 47, Kpetoe 0302-216970 EXT 5644/6644
Akatsi Box 55, Akatsi 0302-216970 EXT 5584/6584
Ho Box 47, Ho 0302-216970 EXT 5585/6585
Hohoe Box 126, Hohoe 0302-216970 EXT 5586/6586
Jasikan Box 20, Jasikan 0302-216970 EXT 5587/6587
Kadjebi
Box 50, Kadjebi-
Akan 0302-216970 EXT 5588/6588

2010 ANNUAL REPORT
53
DIRECTORY OF DISTRICT MUTUAL HEALTH INSURANCE SCHEMES
Name of Region Name of scheme Address/location Telephone number
Volta
Keta Box Kw, 231 0302-216970 EXT 5589/6589
Ketu Box De 189, Denu 0302-216970 EXT 5590/6590
Kpando Box 45, Kpando 0302-216970 EXT 5591/6591
Krachi East Box11, Damba 0302-216970 EXT 5592/6592
Krachi West Box 42, Krachie 0302-216970 EXT 5593/6593
Nkwanta Box 1, Nkwanta 0302-216970 EXT 5594/6594
South Dayi Box 3, Kpeve 0302-216970 EXT 5595/6595
North Tongu Box 19, Adidome 0302-216970 EXT 5596/6596
South Tongu Box 46, Sogakope 0302-216970 EXT 5597/6597
Western
Ahantaman Box 10, Agona - Ahanta 0302-216970 EXT 5630/6630
Amenfiman Pmb, Asankragua 0302-216970 EXT 5631/6631
Aowin- Suaman Box 32, Enchi 0302-216970 EXT 5632/6632
Bia 0302-216970 EXT 5636/6636
Bibiani-Anhwiaso Box 49, Bibiani 0302-216970 EXT 5633/6633
Jomoro Box 176, Half - Assini 0302-216970 EXT 5634/6634
Juaboso Box 1, Juaboso 0302-216970 EXT 5635/6635
Mpohor Wassa East Box 1008, Daboase 0302-216970 EXT 5637/6637
Nzema East Box 25, Axim 0302-216970 EXT 5638/6638
Sefwi Wiawso Box 183, S/Wiaso 0302-216970 EXT 5640/6640
Sekondi Box Ax 43, Takoradi 0302-216970 EXT 5639/6639
Shama Box 5, Shama 0302-216970 EXT 5629/6629
Takoradi Box Ax 43, Takoradi 0302-216970 EXT 6641/7641
Wassa Amenfi East Box 10, Wasa Akropong 0302-216970 EXT 5628/6628
Wassa West Box 1, Tarkwa 0302-216970 EXT 5642/6642

2010 ANNUAL REPORT
54
ANNEX 6: Training programs organised in 2010
PROGRAM NO.
NUFFIC
FUNDED
TRAINING
1. ICT Training All 10 Regions
2. Introduction to HR Principles
3. Job Description & constructive Feedback
4. Performance Appraisal
5. Fraud Detection & Controls
6. Knowledge of the Ghanaian Health System
7. Leadership & Management
8. Change Management
9. Master of Public Health (Amsterdam)
Sub Total
95
5
6
16
6
12
16
5 1
158
OTHER
LOCAL
TRAINING
10. Basic Auditing for Internal Auditors
11. Hardware & Networking Training
12. Public Sector IFRS
13. Making Change Fun & Successful
14. Forensic Auditing
15. Planning Management
16. Training Selection of Consultant Services
and Stores Management
17. Managing HR Records: Files & Records
Generated by HR Function
18. Training Selection of Consultants’ Services
19. Computer Based Auditing Management
20. Training on Stores Inventory Management
21. Fraud Detection. Prevention & Controls
22. Efficiency & Effectiveness in Government
Expenditure Sub Total
3
6
2
23
2
2
6
2
3
2
2
1
2
6
1
61
EXTERNAL
TRAINING
23. Result-Based Management: Performance
Indicators
24. Public Procurement Management
25. Financial & Budgetary Management of
Projects & Organizations
26. Improving the Quality of Health Services
27. ITIL
28. Strengthening Human Resource for Health
29. Public –Private Investment Partnerships:
Innovations & Efficiency in Health
Systems
30. Health Insurance (Quality, Provider
Management, ICT & Contracting
31. Health Insurance Portability &
Accountability
32. White Collar Crime
33. Procurement Auditing
34. Conflict Prevention
1
1
1
3
2
1
2
2
1
2
1
1

2010 ANNUAL REPORT
55
35. Company Secretary & Corporate Advisors
Course
36. Combating Corruption & Developing
Organizational Integrity
37. Advanced Audit Skills
38. International Ministerial Conference on
Health System Financing
39. First Global Symposium on Health
Research
40. Capitalizing on the Strategic Shift &
Elevation of the Human Resource
Component
41. Strategic Planning, Budgeting &
Forecasting Training Workshop
42. 2nd Financial Management Conference
Optimizing Public & Private Sector
Financial Performance
43. Strategic Skills Development for Africa
Conference
44. Joint Learning for Universal Coverage
Workshop on Provider Payment Systems
45. Financial Access to Healthcare for the Poor
46. Strategic HR Africa Forum Kenya
47. African Healthcare Management
Conference
48. Financial Modeling & Reporting
49. Health Sector Reform & Sustainable
Financing
Sub Total
GRAND TOTAL
1
2
1
1
2
2
1
2
2
1
2
2
1
2
3
2
1
45
266