Ankylosed primary mola.rs: Results and treatment recommendat,ons ...
11
PEDIATRIC DENTISTRY/Copyright (~) 1980 The American Academy of Pedodontics/Vol. 2, No, 1 Ankylosed primary mola.rs: Results and treatment recommendat,ons from an eight-year longitudinal study LouiseBrearley Messer, B.D.Sc., L.D.S., M.D.Sc. Jay T. Cline, D.D.S., M.A. Abstract A total of 263 ankyloscd primarymolars in 107 children aged three to 12 years was studied for four years. Forty-six children remained in the study for eight years. Observation of affected dentitions showed that the con- dition was likely to recur. Threeclinical pa~terns for the condition are described. Typically, maxillary molarsbe- came ankylosed earlier and demonstrated more severe in[raocclusion than mandibular molars. Mandibular first molars usually remained slightly or moderately in#a- occluded; mandibular second molars and maxillary first and secondmolars showed progressively severe infra- occlusion. Following either extraction or ex~oliation of the affected molars, the succedaneous bicuspids did not differ in either coronal morphology or in distribution of enamel surface defects from bicuspids preceded by non-ankylosed molars. Mandibular first molarsusually ex[oliated on schedule; failure to employ timed extraction for severely infraoccluded molars resulted in reduced alveolar bone support [or the bicuspid. Treatment recommendations are developed based.upon the molartype, clinical pattern, andthe severity of in#aocclusion. Introduction Dental ankylosis may be defined as an anatomical fusion of cementumwith alveolar bone, occurring at any time during the course of eruption. 1 Occasionally, the tooth may become ankylosed prior to emergence into the oral cavity, or may ankylose during active eruption before contact is made with the opposing dentition. 2 Clinically, the crown is located below the occlusal plane, while the eruption of adiacent teeth Accepted: December 3, 1979 continues concomitantly with vertical alveolar bone growth, ~,3 and the tooth is immobile to manual rock- ing.4, 5 The etiology of the condition remains unknown. Extrinsic causative factors implicated are local me- chanical trauma, ~ disturbed local metabolism, ~ local- ized infection, 6 chemical or thermal irritation 7 and tooth reimplantation, s Intrinsic factors cited include a genetic or congenital gap in the periodontal liga- ment. Since both erupting and exfoliating teeth show alternating periods of resorption and deposition of bone and cementum, ° aberrant deposition of these tis- sues may produce an area of ankylosing tissue.Z, I° In a summary of studies reporting the prevalence of ankylosed primary molars, Andlaw (1974) described a range from 1.3% to 38.5%. 11 The differences were attributed to ethnic factors, and also to differing diag- nostic criteria. Among healthy Caucasian children of predominantly Scandinavian descent residing in the Minneapolis-St. Paul area of Minnesota, we reported a prevalence of 6.9%. 12 Contrary to studies reporting the mandibular second primary molar to be most fre- quently affected, 4,z3,1~ our studies and others have implicated the mandil3ular first primary molar most frequently. 1~,15,16 Multiple instances of ankylosis oc- cur as frequently as single instances, ~7 and a patient with one or two ankylosed teeth is likely to have other teeth become ankylosed later. 1°,1v Radiographically, the zone of ankylosing tissue may not manifest as a localized obliteration of the periodontal ligament space, since the zone may be only a microscopic re- pair of cemental resorption by osteoid-like tissue con- tinuous with the alveolar bone. ~8-2° The presence of ankylosed primary molar teeth may complicate the eruption and development of the PEDIATRICDENTISTRY Vol. 2, No. 1 37
Transcript of Ankylosed primary mola.rs: Results and treatment recommendat,ons ...

PEDIATRIC DENTISTRY/Copyright (~) 1980 The American Academy of Pedodontics/Vol. 2, No, 1
Ankylosed primary mola.rs: Results andtreatment recommendat,ons from aneight-year longitudinal studyLouise Brearley Messer, B.D.Sc., L.D.S., M.D.Sc.Jay T. Cline, D.D.S., M.A.
AbstractA total of 263 ankyloscd primary molars in 107
children aged three to 12 years was studied for four years.Forty-six children remained in the study for eight years.Observation of affected dentitions showed that the con-dition was likely to recur. Three clinical pa~terns for thecondition are described. Typically, maxillary molars be-came ankylosed earlier and demonstrated more severein[raocclusion than mandibular molars. Mandibular firstmolars usually remained slightly or moderately in#a-occluded; mandibular second molars and maxillary firstand second molars showed progressively severe infra-occlusion. Following either extraction or ex~oliation of theaffected molars, the succedaneous bicuspids did not differin either coronal morphology or in distribution of enamelsurface defects from bicuspids preceded by non-ankylosedmolars. Mandibular first molars usually ex[oliated onschedule; failure to employ timed extraction for severelyinfraoccluded molars resulted in reduced alveolar bonesupport [or the bicuspid. Treatment recommendationsare developed based .upon the molar type, clinical pattern,and the severity of in#aocclusion.
IntroductionDental ankylosis may be defined as an anatomical
fusion of cementum with alveolar bone, occurring atany time during the course of eruption.1 Occasionally,the tooth may become ankylosed prior to emergenceinto the oral cavity, or may ankylose during activeeruption before contact is made with the opposingdentition. 2 Clinically, the crown is located below theocclusal plane, while the eruption of adiacent teeth
Accepted: December 3, 1979
continues concomitantly with vertical alveolar bonegrowth,~,3 and the tooth is immobile to manual rock-ing.4,5
The etiology of the condition remains unknown.Extrinsic causative factors implicated are local me-chanical trauma,~ disturbed local metabolism,~ local-ized infection, 6 chemical or thermal irritation 7 andtooth reimplantation,s Intrinsic factors cited include agenetic or congenital gap in the periodontal liga-ment. Since both erupting and exfoliating teeth showalternating periods of resorption and deposition ofbone and cementum,° aberrant deposition of these tis-sues may produce an area of ankylosing tissue.Z,I°
In a summary of studies reporting the prevalence ofankylosed primary molars, Andlaw (1974) describeda range from 1.3% to 38.5%.11 The differences wereattributed to ethnic factors, and also to differing diag-nostic criteria. Among healthy Caucasian children ofpredominantly Scandinavian descent residing in theMinneapolis-St. Paul area of Minnesota, we reporteda prevalence of 6.9%.12 Contrary to studies reportingthe mandibular second primary molar to be most fre-quently affected, 4,z3,1~ our studies and others haveimplicated the mandil3ular first primary molar mostfrequently.1~,15,16 Multiple instances of ankylosis oc-cur as frequently as single instances,~7 and a patientwith one or two ankylosed teeth is likely to have otherteeth become ankylosed later. 1°,1v Radiographically,the zone of ankylosing tissue may not manifest as alocalized obliteration of the periodontal ligamentspace, since the zone may be only a microscopic re-pair of cemental resorption by osteoid-like tissue con-tinuous with the alveolar bone.~8-2°
The presence of ankylosed primary molar teethmay complicate the eruption and development of the
PEDIATRIC DENTISTRYVol. 2, No. 1 37

permanent dentition. Typically, there is delayed ex-foliation of affected teethzl with subsequent compli-cations such as deflected eruption paths for adiacentor opposing teeth, z impaction of succedaneous bicus-pids,%11 localized or generalized loss of needed archlength,21 and tipping of adiacent teeth over the anky-losed primary molar or supraeruption of opposingteeth. ]~,2~,2z These sequelae may result in malocclu-sion.
In the past, the treatment of ankylosed primarymolars has been largely empirical. Luxation,-° restor-ing the tooth to occlusion ~vith a variety of techniquesand materials,-0~,°’3 and extraction,~,z°,zl have all beenutilized. While the literature contains many anecdotalreports of the relative success of these treatment ap-proaches, clear documentation of indications, contra-indications and possible sequelae is lacking. In orderto develop more rational bases for treatment, a two-part clinical investigation comprising a short-term(four-year) study and a long-term (eight-year) studywas designed. A group of affected dentitions was fol-lowed longitudinally with periodic examinations, ra-diographs and study models, until complete erup-tion of all bicuspids, permanent cuspids, and perma-nent second molars. No attempt was made by theinvestigators to dictate treatment of the ankylosedmolars by the attending dentists in order that cur-rently-employed treatment regimes would be used un-hindered.
Study DesignStudy Population
A total of 107 healthy Caucasian children of pre-dominantly Scandinavian descent, ranging in age fromthree to 12 years and possessing one or more anky-losed primary molars, was studied in the PediatricDentistry Clinic of the University of MinnesotaSchool of Dentistry. Using periodic clinical and radio-graphic observations, the history of each ankylosedprimary molar (test molar), and non-ankylosed pri-mary molar in each dentition was followed and ob-servations recorded on these teeth and their succeed-ing bicuspids.
The majority of children received their dental carethroughout the study at the clinics of the Universityof Minnesota School of Dentistry; the remainder at-tended private dentists for regular dental care. In allinstances, the ankylosed molar either was ob.servedperiodically, or extracted and appropriate spacemaintenance instituted. No tooth was treated by lux-ation; only ankylosed teeth with congenitally-missingbicuspids ’were restored’ to occlusion with stainlesssteel crowns.
Purposes of Short-Term and Long-Term Studies
The purpose of the short-term study was to eluci-date the characteristics of ankylosis of individualmolars, ~vith respect to age at diagnosis, severity ofinfraocclusion, and distribution of the condition.
Dentitions in the long-term study were used tostudy the sequelae of ankylosis with respect to over-retention of the primary molar, and the clinical andradiographic appearance of the succeeding bicuspidin comparison with other bicuspids preceded by non-ankylosed primary molars in the same dentitions.
Diagnosis of Ankylosis
The diagnosis was based upon two essential cri-teria:
(1.) The entire occlusal surface of the primarymolar was located at least 1 mm below theexpected occlusal plane as judged from thenearest adjacent non-ankylosed teeth in thesame quadrant.5
(2.) The molar was immobile when subiected man-ually to a rocking movement,4 in contrast toother (non-exfoliating) primary molars in thedentition.
The emission of a sharp clear sound on percussionwas not an essential criterion because of its subiec-tivity, a9 Radiographic evidence of bony union wasnot required because of its variability.~z
Distribution of Primary Molars
The short-term study group comprised 107 denti-tions (45 males; 62 females) which at first examina-tion contained a total of 191 ankylosed molars (Table1). The group included six sibships each containingtwo affected children. Thirty-five dentitions eachcontained a single ankylosed molar and 72 dentitionseach showed two or more affected molars. The 107¯ dentitions were studied for four years, during whichtime 31 dentitions (29~) showed a recurrence ankylosis involving a further 72 primary molars (Ta-ble 1 ).
Thereafter, the long-term study group contained 46dentitions (23 males; 23 females; three sibships eachwith two affected children) totalling 116 ankylosedmolars (Table 1).~ These were followed for eightyears. No additional diagnoses were made duringthe second four years of the study. For this group,the bicuspids preceded by non-ankylosed primarymolars in the same dentitions were pooled as a com-parison group. These teeth were distributed as fol-lows: mandibular first: 9.8; mandibular second: 48 (afurther three teeth were congenitally absent); maxil-lary first: 86; and maxillary second: 86 (a further twoteeth were congenitally missing). Since many of thedentitions had contralateral molars affected with
ANKYLOSED PRIMARY MOLARS38 Messer and Cllne

Table 1. Distribution of ankylosed primary molars in i07 affected dentitions(short- and long-term studies)
Time of No. Ankylosed Primary MolarsStudy diagnosis Md 1st Md 2nd Mx 1st Mx 2nd Total
Short term at first exam 131 37 16 7 191at later exam 18 40 5 9 72
Total 149 77 21 16 263
Long term at first orlater exam 64 41 7 4 116
ankylosis, teeth could not be pair-matched for com-parisons. Therefore, the findings for each group ofankylosed molars were compared with those for thecorresponding group of pooled non-ankylosed molars.
Data Collected in Short-Term StudyAge at Diagnosis of Primary Molar Ankylosis
The age of each child at the time of diagnosis ofeach ankylosed molar was recorded, based on clinicalobservations and from existing clinical and radio-graphic records maintained by the clinic before com-mencement of the study.
Extent of Infraocclusion
Using study models, the extent of infraocclusion ofeach ankylosed molar was classified at diagnosis asone of the following:
Slight: The entire occlusal surface was lo-cated approximately 1 mm below theexpected occlusal plane as iudgedfrom the two nearest non-ankylosedteeth in the same quadrant.
Moderate: The entire occlusal surface was lo-cated with both marginal ridges ap-proximately level with, or iust cervi-cal to, the contact area of one or bothadiacent tooth surfaces. In instancesof ankylosis of two adiacent primarymolars, the contact area of the firstsecondary molar was used for refer-ence.
Severe: The entire occlusal surface was lo-cated level with or below the inter-proximal gingival tissue of one orboth adiacent tooth surfaces.
Distribution Characteristics of Ankylosis
Sequential study models for each child were ex-
amined in order to identify distribution characteristicsfor the condition.
Data Collected in Long-Term StudyOverretention of Ankylosed Primary Molars
A molar was deemed overretained if it was still inposition, and immobile, after the contralateral non-ankylosed primary molar had exfoliated. An ankylosedmolar which became mobile close to the expected ex-foliation time was not considered overretained. In in-stances of ankylosis of a contralateral pair of molars,reference was made to tables of chronology,z4 in con-iunction with an examination of the eruption se-quence for the particular dentition and the status ofroot development of the succedaneous bicuspids.
Clinical, Radiographic, Occlusal andPeriodontal Observations on Bicuspids
When all bicuspids, permanent cuspids and perma-nent second molars were fully erupted, each bicuspidwas air-dried and examined clinically using a mirrorand explorer* for the following: coronal and radicularmorphology, hypoplasia and hypomineralization, co-ronal position, and rotation. The periodontal tissueswere examined clinically and radiographically for evi-dence of pocket-formation, lamina dura thickening,and alveolar bone loss. Observations were made in-dependently by both authors, each unaware ofwhether the bicuspid was preceded by an ankylosedor non-ankylosed molar. Positive findings were re-corded only when there was unanimity between ex-aminers using the following criteria:
Coronal and radicular morphology:The morphological features of contralateral teethwere compared with each other and with those de-scribed by Wheeler (1974),~-5 and any marked dif-ferences recorded.
* No. 5DE explorer, Hu Friedy Manufacturing Co., Chi-cago, Illinois’ 60618.
PEDIATRIC DENTISTRYVol. 2, No. I 39

Table 2. Extent of infraocclusion of 263 ankylosed primary molars at initialdiagnosis (short-term study)
NO. Ankylosed Molars (%)Infraocclusion Md 1st Md 2rid Mx 1st Mx 2nd Total
Slight 111 (75) 36 (47) 9 (43) 6 (37) 162Moderate 36 (24) 32 (41) 10 (48) 7 (44) 85Severe 2 (1) 9 (12) 2 (9) 3 (19) 16
Total 149 77 21 16 263
Hypoplasia:Non-hereditary hypoplasia was defined after Sicher(1962)26 as localized, circumscribed pitting, fur-rowing or absence of enamel which may or maynot be associated also with hypomineralization.
H ypomineralization :Non-fluorotic surface enamel defects of hypominer-alization were asymmetrical round or oval lesionsclearly differentiated from adiacent normal enameland often creamy yellow or brown in color on nor-mally contoured enamel surfaces, z7 Very mildfluorosis was defined after Russell (1961)27 assymmetrical small spots or minute, lacy, horizontallines generally following the incremental lines ofenamel development and imperceptibly demar-cated from normal enamel and of a "paper white"color. The cusp tips may have a frosted appearanceand the condition usually affects the incisal or oc-clusal half, or more, of contralateral teeth. Theenamel is smooth to an explorer.
Coronal malposition:A bicuspid was deemed malpositioned if the en-tire crown was placed buccally, lingually or in in-fraocclusion from the expected position of thattooth in the dental arch contour.
Coronal rotation:This was classified as none, slight, moderate or se-vere, based upon the extent of deviation of thetooth from its expected angulation between the twoadiacent teeth, iudging on the positioning of themesial marginal ridge. A bicuspid was deemedslightly rotated if the position of this ridge was de-viated, but less than 20°, to either the buecal orlingual of its expected position between the ad-iacent teeth. If the mesial marginal ridge was devi-ated by more than 20°, but less than 90°, to eitherthe buccal or lingual, the bicuspid was deemedmoderately rotated; a bicuspid rotated 90° or morefrom its expected position was deemed severely ro-tated.
Periodontal pocket formation:Periodontal pocket depth was measured beneath
the mesial and distal contact areas using a perio-dontal probe.*
Thickening of lamina dura:Thickening of the lamina dura was diagnosed fromintraoral radiographs based on the description ofGoldman and Cohen ( 1973 ).~8
Alveolar bone loss:Vertical and horizontal bone loss was diagnosedfrom intraoral radiographs, based on the descrip-tion of Goldman and Cohen (1973).z8
A comparison of the binomial distributions ~9 wasused to test for any statistically significant differencebetween the distributions of observations for bicus-pids preceded by anl~ylosed and non-ankylosed mo-lars.
Results of Short-Term StudyAge at Diagnosis of Primary Molar Ankylosis
The mean ages at diagnosis were as follows: man-dibular first molar: 7.1 (range 5.2 - 9.2 yrs.); man-dibular second molar: 8.0 (range 5.1 - 10.4 yrs.);maxillary first molar: 6.2 (range 4.7 - 8.6 yrs.); max-illary second molar: 4.6 (range 3.0 - 9.4 yrs.). Thediagnosis of ankylosis of the maxillary first molarsfrequently coincided with the eruption of the maxil-lary first permanent molar, For several of the maxil-lary second molars in the study, the apparent failureof complete eruption of this tooth was the reason forthe patient presenting to the clinic. For all otherankylosed molars, the parents were unaware of thecondition until it was brought to their attention.
Extent of Infraocclusion
Most maxillary first and second primary molarswere in moderate or severe infraocclusion when diag-nosed (Table 2). These teeth tended to show a rela-tively rapid progression toward more severe infraoc-clusion. Mandibular first molars were only slightly
* No. 0 periodontal probe, Hu Friedy Manufacturing Co.,Chicago, Illinois 60618.
ANKYLOSED PRIMARY MOLARS40 Messer and Cline

Table 3. Three clinical patterns of primary molar ankylosis in 107 dentitionsdiagnosed over four-year observation period (short-term study)
Ankylosis Pattern Arch Distribution (no. dentitions)Total
dentitions (%)
I Molar Pair Mand 1 contralateral pair (29)2 contralateral pairs (15)1 adjacent pair (2)
Max 1 contralateral pair (2)
48 (45%)
II Single Molar
III Multiple Molars
Mand 1st molar (24)2nd molar (6)
Max 1st molar (4)2nd molar (1)
Mand 3 teeth — 1 pair plus 1 single (8)and 4 teeth — 1 pair plus 2 singles (5)Max 5 teeth — 2 pairs plus 1 single (9)
6 teeth — 3 pairs (1)7 teeth — 3 pairs plus 1 single (1)
35 (33%)
24 (22%)
affected (Table 2) and rarely became more severelyinfraoccluded, whereas most mandibular second mo-lars showed a progressive development of more se-vere infraocclusion. No molar which became anky-losed late in the development of the succedaneous bi-cuspid became severely involved and these usuallyremained in slight or moderate infraocclusion.
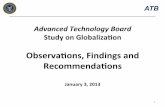
Figure 1 shows the intraoral radiographs of onepatient over a 55-month period. This patient illus-trates several salient features of molar ankylosis. Thefirst radiographs (Figure IA) show slight infraocclu-sion of the mandibular left and right first primarymolars. Interproximal lesions in these teeth were re-stored with amalgam (one tooth also later received astainless steel crown) and both teeth later exfoliatedon schedule. Meanwhile, the mandibular left andmandibular right second primary molars became mod-erately ankylosed (Figure IB), as did the maxillaryleft second primary molar (perhaps following the ec-topic eruption of the adjacent first permanent molar).The maxillary second primary molar was extractedand a space maintainer placed; the mandibular sec-ond molars exfoliated on schedule. A root fragmentof the mandibular right second primary molar re-mained (Figure 1C), probably related to the unequalresorption pattern of the mesial and distal roots.
Distribution Characteristics of Ankylosis
Three clinical patterns for the condition were ap-parent (Table 3). The most frequently occurring wasPattern I (48 dentitions, or 45%) where one or morecontralateral molar pairs, or an adjacent pair of mo-lars, were ankylosed. A single molar, Pattern II, was
Figure 1. A series of bitewing radiographs of a Cau-casian female showing progression of primary molarankylosis. (A) Note slight infraocclusion of mandibularfirst primary molars and ectopic eruption of the maxil-lary left first permanent molar. (B) Note loosening ofmandibular first primary molars, moderate infraocclu-sion of the mandibular second primary molars withan unequal resorption pattern of the roots of the man-dibular right second primary molar, and moderate in-fraocclusion of the maxillary left second primarymolar. (C) All bicuspids are fully erupted. Note theresidual primary molar root fragment mesial to themandibular right second bicuspid.
PEDIATRIC DENTISTRYVol. 2, No. 1 41

affected in 35 dentitions (3370). Pattern III com-prised multiple ankylosed molars ranging from threeto seven affected teeth (24 dentitions, or 2270). Thispattern was viewed as a combination of one, two, orthree molar pairs (as Pattern I), plus one or moresingle occurrences in any quadrant.
Results of Long-Term StudyOverretention of Ankylosed Primary Molars
The treatment histories are summarized in Table 4.Most mandibular first molars exfoliated on schedule,and none left residual root fragments. Mandibularsecond molars were less prone to exfoliation; residualroot fragments were shown by two molars that ex-foliated and by four molars that were extracted aheadof exfoliation. None of the 11 maxillary molars thatwere extracted early left root fragments. Five mandib-ular second molars without permanent successorswere restored with stainless steel crowns. During theobservation period, these teeth became severely infra-occluded and radiographically showed extensive re-placement of the periodontal ligament with mineral-ized tissue. Periodic replacement of the crowns wasrequired to maintain occlusion. Eventually, orthodon-tic treatment was instituted for one child and thetooth was extracted surgically.
Clinical and Radiographic Appearanceof Bicuspids
Table 5 summarizes the clinical and radiographicappearance of the test bicuspids.
Among test mandibular bicuspids, hypoplasia and/or hypomineralization defects were seen in 25 of the64 (39~) first bicuspids and in eight of the 36 (22g)second bicuspids. In all instances, similar multipleenamel surface defects were seen in other bicuspids inthe same dentition, and in no instance could the de-fects be clearly attributed to ankylosis of the pre-ceding primary molar or to the treatment procedure(observation until exfoliation, or extraction) that hadbeen followed. Very mild fluorosis was seen in 40gof the 46 dentitions studied.
On radiographic examination, four test bicuspidsshowed "V"-shaped notching of the root outline, lo-cated in the middle one-third. In three instances, thepreceding primary molar had been overretained andex-tracted. Of bicuspids preceded by non-ankylosedmolars, none showed "V" root notching. The distri-bution of apical root flexion did not differ signifi-cantly between bicuspids preceded by ankylosed ornon-ankylosed primary molars.
Occlusal Observation on Bicuspids
The occlusal observations for test bicuspids areshown in Table 5. Among mandibular first bicuspids,four test teeth (670) and three unaffected bicuspids(1170) were in infraocclusion; the difference was notstatistically significant. Inadequate mesiodistal spacewas present for 35 test mandibular first bicuspids(55g) and for 15 unaffected mandibular first bicus-pids (54g). This difference was not statistically sig-nificant. A total of 58 (90.6%) test mandibular firstbicuspids showed coronal rotation (slight: 41 teeth,moderate: 17 teeth, severe: none); among unaffectedbicuspids, only three (11~;) were rotated. Statistically,test mandibular first bicuspids were significantlymore frequently rotated than unaffected mandibularfirst bicuspids (Z=7.4672; p<0.01).
Among test mandibular second bicuspids, fourteeth (llg) were in infraocclusion. This distributiondid not differ significantly from that of unaffectedmandibular second bicuspids (four teeth or 8g werein infraocclusion). Eleven test mandibular second bi-cuspids (30g) and four unaffected bicuspids (8~;)showed inadequate mesiodistal space. This difference~vas statistically significant (Z=2.6327, p<0.01). Thedistribution of rotated mandibular second bicuspidsin the test group (21 rotated or 58g) did not differsignificantly from that of the unaffected group (29rotated or 60~o).
None of the eleven test maxillary bicuspids wereinfraoccluded; one showed mesiodistal space inade-quacy and four teeth were rotated. These sample sizeswere deemed too small for statistical comparison withunaffected maxillary bicuspids.
Periodontal Observations on Bicuspids
The periodontal observations on the test bicuspidsare shown in Table 5. Among the 64 test mandibularfirst bicuspids, none of those preceded by first pri-mary molars exfoliating on schedule showed any un-usual findings. Of the 11 in the extraction group, thet~vo bicuspids preceded by overretained mandibularfirst molars both showed periodontal pocketing (3-4mm), thickening of the lamina dura and inadequatevertical alveolar bone height. The latter two observa-tions were also recorded for one mandibular first bi-cuspid preceded by a primary molar which was ex-tracted early. Nbne of the unaffected mandibular firstbicuspids showed these periodontal findings.
Among the 16 test mandibular second bicuspids inthe exfoliation group, one bicuspid .showed pocketformation (3-4 mm) and this tooth, plus a second bi-cuspid in the same group, showed inadequate verticalalveolar bone height. Reduced alveolar bone heightwas ~Iso shown by a further three bicuspids in the
ANKYLOSED PRIMARY MOLARS42 Messer and Cline

Table 4. Treatment history for 116 ankylosed molars in 46 affected dentitions(long-term study)
NO. Ankylosed Primary Molars (%)Treatment History Md 1st Md 2nd Mx 1st Mx 2nd Total
Exfoliated onschedule 53 (83) 16 (39) 0 0 69
Extracted beforeexfoliation time 9 (14) 15 (37) 7 (100) 4 (100) 35
Overretained andextracted 2 (3) 5 (12) 0 0 7
Occlusion restoredwith steel crown* 0 5 (12) 0 0 5
Total 64 41 7 4 116
* Five mandibular second bicuspids were congenitally missing.
Table 5. Coronal, radicular and periodontal observations on 111" bicuspidspreceded by ankylosed primary molars in 46 affected dentitions (long-termstudy)
No. Affirmative Observations on BicuspidsMand 1st Mand 2nd Mx 1st Mx 2rid
Observation Extoliatedt Extractedtt Exloliated Extracted Extracted Extracted Total(n=53) (n=11) (n=16) (n=20) (n~-7) (n=4)
Crownhypoplasia 2 1 0 1 0 0 4hypomineralization 17 5 5 2 0 0 29
Root"v" notching 1 1 0 2 0 0 4apical flexion 8 2 1 2 1 0 14
Occlusioninfraocclusion 2 2 2 2 0 0 8m-d space inadequate 30 5 4 7 1 0 47rotation 47 11 13 8 3 1 83
Periodontalpocket formation 0 2 1 1 1 0 5lamina dura thickened 0 3 0 0 1 0 4alveolar bone loss 0 3 2 4 1 0 10
* Only 111 of the 116 teeth are shown since five mandibular second bicuspidswere congenitally absent.
t Preceding primary molar exfoliated on schedule.11 Preceding primary molar extracted either before exfoliation time or following
overretention.
PEDIATRIC DENTISTRYVol. 2, No. ! 43

late extraction group. None of the unaffected man-dibular second bicuspids showed similar periodontalfindings. Of the eleven test maxillary bicuspids, peri-odontal pathology was seen for one maxillary firstbicuspid. The periodontal pocket depth was 3-4 mm.None of the unaffected maxillary bicuspids showedperiodontal pocket formation, lamina dura thickeningor alveolar bone discrepancy.
DiscussionCharacteristics of Ankylosed Molars
As shown previously,12,1~ the mandibular first pri-mary molar was the tooth most frequently affected byankylosis in the present study. Since this tooth usuallyshows only slight and rarely moderate infraocclusion,and typically exfoliates on schedule, the diagnosis ofankylosis may be missed. Consequently, it is not sur-prising that the mandibular second molar, which isusually in more severe infraocclusion, has been con-sidered to be the tooth most frequently affected byankylosis.4,13,14 In the present study, maxillary molarswere affected less frequently than mandibular molars,and the maxillary second molar least of all, confirm-ing the observations of many other surveys on thisaspect of ankylosis.4,1"~-15
The present study appears to be one of very fewexamining the time of diagnosis .of ankylosis.~5,~6
Since a criterion for inclusion of the dentition in thestudy was the presence of at least one tooth alreadyankylosed, the actual onset of the condition for theseteeth cannot be determined. Also, the diagnostic cri-teria are applicable only after the tooth has begunto manifest the condition clinically, and presumablythe cellular changes occur considerably in advance ofthe clinical picture. Nevertheless, the approx.imationsmade in the present study serve to show that thefour different primary molars are prone to ankyloseat various times and that these are usually quite typi-cal for each molar.
Maxillary primary molars tended to ankylose early,either before the eruption of the maxillary first per-manent molar (as was shown by most of the secondprimary molars studied) or at approximately thesame time as the maxillary first permanent molarerupted (as seen for most of the maxillary first pri-mary molars studied). Mandibular primary molarstended to ankylose later than maxillary molars, themean age of diagnosis for mandibular first molars be-ing 7.1 years and 8.0 years for mandibular secondmolars. The majority of the mandibular first molarsbecame ankylosed soon after the eruption of the firstpermanent molar in the same quadrant, but this wasunusual among mandibular second molars. Ankylosisof mandibular first molars did not appear to occur
subsequent to ankylosis of the mandibular secondmolar in the same dentition, but there was a high in-cidence of ankylosis of the latter tooth subsequent toinvolvement of the former. Owent has observed thatankylosis of maxillary molars usually occurs coinci-dent with involvement of opposing mandibular mo-lars, and this is supported by the present observationswhere 30 of the 37 ankylosed maxillary molars werepresent in dentitions which also showed mandibularinvolvement. However, it is not an invariable findingas there were seven instances of affected maxillarymolars where no mandibular molar was involvedeither initially, or on longitudinal study.
The present study indicates that individual molarstend to show a somewhat typical pattern of severity.In comparison with mandibular molars, maxillary mo-lars tend to show severe, early involvement and therelative severity may be partially reflecting a spurt ofalveolar bone growth coincident with the eruption ofthe maxillary first permanent molars. The relativeslightness of the typical infraocclusion of the affectedmandibular first primary molar may reflect, in part,a lessened increment in vertical alveolar bone growthoccurring in the cuspid-first molar region prior to theexfoliation time of the first primary molar.
The decided tendencies seen toward multiple oc-currences, contralaterally affected teeth, and lack ofpredilection for the side of the arch first affected,confirm previous studies.4,14,~9 In the present study,only 35 of the 107 dentitions (33~g) in the four-yearstudy showed ankylosis limited to a single molar, andthe remaining 72 dentitions (67~o) each contained twoor more ankylosed molars totaling 228 affected teeth.The teeth were distributed in three distinct clinicalpatterns which serve to indicate where a contralateraloccurrence of the condition is likely to occur, andprovide a basis for treatment recommendations, asdescribed below. Contralateral occurrences are morelikely in the mandibular arch than in the maxillary,and single occurrences are more likely to occur inthe maxillary than in the mandibular arch.
Characteristics of Succeflaneous Bicuspids
The present study indicates that the presence of apreceding ankylosed primary molar is not likely toaffect coronal morphology or to initiate coronal hypo-plasia and/or hypomineralization of the succeedingbicuspid. This lends support to the opinion of Kollar(1972) 3° that the morphological template of thecrown is established very early in embryological de-velopment and is not readily altered. For the maiorityof the ankylosed teeth studied in the present report,the crowns of the succedaneous bicuspids were al-ready fully formed at the time described as the firstclinical diagnosis of the condition. Presumably the
ANKYLOSED PRIMARY MOLARS44 Messer and Cl|ne

cellular changes involved in the process of ankylosishad no effect on the coronal tissues of the formingsuccedaneous tooth. The lack of an increased preva-lence of enamel surface defects in the succeedingbicuspids is in contrast to the findings of Rule,Zacherl and Pfefferle (1972). 31 In a sample of 262bicuspids succeeding ankylosed primary molars, theseworkers described a statistically significant increasein the number of enamel surface defects over thoseseen in control bicuspids and speculated on a corre-lation between ankylosis and the coronal abnormali-ties. The present study examined a larger sample ofchildren with ankylosed teeth, and also identifiedthat 40~ of the dentitions demonstrated very mildfluorosis. This could have masked additional enameldefects of a non-fluorotic origin.
No clear association was found in the present studybetween apical flexion of the roots of succeeding bi-cuspids and "V"-shaped notches in the root periphe-ries, and ankylosis of the preceding molars. Notchingof the root outline on a radiograph is an equivocalfinding since the appearance of the root outline islargely dependent upon the radiographic techniqueemployed. These observations support the conclusionof Steigman, Koyoumdiisky-Kaye and Matrai (1974),that ankylosed teeth usually have no causative influ-ence on the rate of development of their successorsP2
Examination of the occlusion of the succedaneousbicuspids suggests that those preceded by an anky-losed primary molar are more likely to demonstrateinadequate mesiodistal space and to show coronal ro-tation. Although these differences were demonstratedto be significant statistically, it cannot be concludedto be more than a trend since the entire occlusion ofthe affected dentitions was not evaluated. In addition,the bicuspids used for comparison were located inthe same dentitions which showed ankylosed teeth,thereby introducing a bias into the statistical treat-ment of the data.
Bicuspids succeeding ankylosed primary molars ap-pear more likely to exhibit periodontal pathology(and particularly if the molar was overretained orrequired extraction) than bicuspids succeeding non-ankylosed molars. The lack of vertical alveolar boneheight coupled with periodontal pocket formation isthought to be due to a failure of alveolar bone devel-opment which normally occurs with exfoliation of theprimary tooth and eruption of the permanent tooth.An ankylosed primary molar is retained at its verticalposition by the ankylosin~ tissue while adjacent teethcontinue to move occlusally with appositional alveolarbone growth. The impedance of primary tooth move-ment serves to restrict vertical alveolar bone deposi-tion, hence there may be a reduced amount of bonesurrounding the bicuspid.
Prognosis and Treatment Recommendations
The present investigation did not seek to evaluatecomparatively the efficacy of several treatment re-gimens for ankylosed molars. Instead, the study soughtto observe the consequences of the three treatmentapproaches (observation; extraction; restoration to oc-clusion) utilized by the attending dentists. The lit-erature reveals widely divergent opinions on the treat-ment of ankylosed primary molars. Hovell (1966)z~stated that most cases require no treatment other thanobservation, while others recommend surgical extrac-tion as the usual treatment on the basis that ankylosedteeth neither exfoliate nor allow the eruption of thesucceeding permanent teeth.9, z4-3~ Andlaw (1974)11
has developed a more conservative series of treatmentrecommendations based upon the extent of infraoc-clusion of the affected tooth. The present study addsto those recommendations by taking into considera-tion also the three clinical patterns of ankylosis de-scribed and the recognized ankylosis characteristicsfor each type of primary molar.
The findings of the present study suggest that themaiority of ankylosed mandibular first primary molarscan be expected to become involved after the erup-tion of the mandibular first permanent molar, andthat the condition is likely to become bilateral. Anky-losis of other primary molars in the dentition is likely,especially of the mandibular second primary molars.The first primary molar is likely to demonstrate onlyslight, progressing but occasionally to moderate, infra-occlusion and can be expected to loosen and exfoliateon schedule. This expectation confirms the observa-tions of Steigman et al. 1~ on the ankylosis characteris-tics of the .mandibular first primary molar. For theseteeth, it is assumed that during the normal process ofexfoliation, the ankylosing tissue is resorbed, allowingthe tooth to become mobile and exfoliate. ]° Rarely isextraction or exfoliation of this tooth followed byresidual root fragments. Therefore, the clinician isrecommended to monitor dentitions with ankylosedmandibular first molars by employing study modelsand space measurements, and to extract these teethonly if they are severely infraoccluded and space lossis imminent. If supraeruption of opposing teeth ap-pears imminent, restoration of the occlusal surface tofull vertical dimension could be considered.
The ankylosed mandibular second primary molaris likely to be affected bilaterally, and onset is likelyto occur later than that of the mandibular first pri-mary molar. With time, mandibular second molarstend to become progressively more severely infraoc-cluded than mandibular first molars. Mesial tippingof the adiacent first permanent molar over the occlu-sal surface of the affected tooth may occur, resultingin loss of arch length. Failure to monitor these teeth
PEDIATRIC DENTISTRYVol. 2, No. 1 45

can result in overretention of the molar and a local-ized lack of vertical alveolar bone. Ankylosed mandib-ular second molars should be kept under close obser-vation with study mo~tels and arch length measure-ments. Extraction should be performed if the toothbecomes moderately infraoccluded and/or mesial tip-ping of the mandibular first permanent molar is im-minent, or if the molar fails to exfoliate on schedule forthat dentition. A passive lower lingual arch is a usefulspace maintainer in the former situation. Followingeither extraction or exfoliation of the mandibular sec-ond molar, the area should be examined closely forroot fragments as these may occur following the typi-cally uneven resorption of the mesial and distal roots.
Restoration of singly affected mandibular molarsshowing only slight infraocclusion with built-up res-torations or stainless steel crowns appears to be auseful interim treatment during the mixed dentitionperiod. There must be a permanent successor presentand both the vertical and mesiodistal dimensions ofthe crown of the ankylosed tooth need to be main-tained adequately. Active vertical alveolar bonegrowth related to the adjacent unaffected teeth islikely to necessitate the periodic replacement of therestoration. If however, the primary molar is in mod-erate or severe infraocclusion, the vertical alveolarbone growth may be hindered and lead to a poorperiodontal prognosis for the succeeding bicuspid.For such teeth, extraction and appropriate spacemaintenance is recommended.
In instances where the primary molar is ankylosedand the permanent molar is congenitally absent, earlyorthodontic and prosthodontic consultations should besought concerning the long-term treatment of the den-tition. While the vertical and mesiodistal dimensionsof the ankylosed molar can be maintained with res-torations throughout the mixed dentition, such res-torations can only be considered of interim nature.Also, after the permanent dentition is established, thesteady remodelling throughout life of alveolar bonesupporting adjacent teeth is likely to require periodicreplacement of such built-up restorations. Biederman(1968)-0 has observed that because of cessation ofalveolar bone growth in the immediate area of theankylosed tooth, the roots of adjacent teeth may be-come denuded of bone and the tooth lost. Such long-term restorative and periodontal consequences sug-gest that early consideration be given to extraction ofthe ankylosed tooth and space closure instituted inconjunction with orthodontic treatment of the denti-tion.
The findings of the present study suggest similarapproaches to treatment for both maxillary first andsecond primary molars. Maxillary second primary mo-lars tend to show a relatively fast progression towards
severe infraocclusion, with an onset which may pre-cede the eruption of the adjacent first permanentmolar. Maxillary first primary molars also tend to in-creasingly severe infraocclusion and the onset mayoccur close to the time of eruption of the first perma-nent molar. Additional ankylosed molars in the man-dibular arch are likely to follow. The obvious severityof the ankylosis of the maxillary primary molars in thepresent long-term study clearly indicated the need forearly extraction. It is likely that failure to extractthese teeth would have resulted in tipping of adja-cent non-ankylosed teeth and consequent loss of archlength and inadequate vertical alveolar bone growthleading to compromised periodontal support for thesucceeding bicuspids. Regardless of the severity ofthe infraocclusion, it is recommended that ankylosedand immobile maxillary molars be extracted as earlyas appears feasible. Since such extractions frequentlyrequire a surgical removal of the tooth on a childaged seven years or under, appropriate considerationshould be given to the behavior management of thechild. In our experience, a distal shoe space main-tainer is a useful appliance in the situation where anankylosed maxillary second primary molar requiresextraction prior to the eruption of the adjacent firstpermanent molar.
It is recommended that the treatment of dentitionswith multiple ankylosed teeth be treated by employ-ing a combination of the approaches recommendedabove for individual molars. Siblings in the familyshould also be monitored, since a familial tendencyfor the condition has been reported.5,1~
Acknowledgments
The assistance of Drs. David McKibben and John Hindingin the initial clinical phases of this study is gratefldly, acknowl-edged. This study ~vas supported in part by a Biomedical Re-search Support Grant from the National Institutes of Health.
References1. Owen, T. L.: "Ankylosis of Teeth," J Mich State Dent
Assoc, 47:347-350, 1965.2. Biederman, W.: "The Problem of the Ankylosed Tooth,"
Dent Clin North Am, July, 409-424, 1968.3. Darling, A. I. and Levers, B. G. H.: "Submerged Human
Deciduous Molars and Ankylosis," Arch Oral Biol, 18:1021-2040, 1973.
4. Biederman, W.: "Etiology and Treatment of Tooth Anky-losis," Am ] Orthod, 48:670-684, 1962.
5. Via, W. F.: "Submer~ed Deciduous Molars: FamilialTendencies," ] Am Dent Assoc,-69:127-129, 1964.
6. Adamson, K. T.: "The Problem of Impacted Teeth inOrthodontics," Aust ] Dent, 56:74-84, 1952.
7. Atrizadeh, F., Kennedy, J., and Zander, H.: "Ankylosis ofTeeth Following Thermal Injury," I Periodont Res, 6:159-167, 1971.
ANKYLOSED PRIMARY MOLARS46 Messer and Cline

8. Finn, S. B.: Clinical Pedodontics, 4th Ed., Philadelphia:W. B. Saunders Co., 1973, p. 259.
9. Boyle, P. E., ed.: Histopathology of the Teeth and TheirSurrounding Structures, 4th Ed., Philadelphia: Lea andFebiger, 1955, p. 276.
10. Henderson, H. Z.: "Ankylosis of Primary Molars: A Clin-ical, Radiographic, and Histologie Study," J Dent Child,46:117-122, 1979.
11. Andlaw, R. J.: "Submerged Deciduous Molars: A Review,With Special Reference to the Rationale of Treatment,"Int Assoc Dent Child, 5:59-66, 1974.
12. Brearley, L. J. and McKibben, D. H.: "Ankylosis of Pri-mary Molar Teeth, I Prevalence and Characteristics; IILongitudinal Study," I Dent Child, 40:54-63, 1973.
13. Dixon, D. A.: "Observations on Submerged DeciduousMolars," Dent Pract Dent Rec, 13:303-316, 1963.
14. Lamb, K. A. and Reed, M. W.: "Measurement of SpaceLoss Resulting From Tooth Ankylosis,’" J Dent Child, 35:483-486, 1968.
15. Steigman, S., Koyoumdiisky-Kaye, E., and Matrai, Y.:"Subnaerged Deciduous Molars in Preschool Children: AnEpidemiologic Survey," ] Dent Res, 52:322-326, 1973.
16. Krakowiak, F. J.: "Ankylosed Primary Molars," I DentChild, 45:288-292, 1978.
17. Brearley, L. J. and McKibben, D. H.: "A LongitudinalStudy of Ankylosed Primary Molar Teeth," IADR Abstr,No. 678, 1972.
18. Noyes, F. B.: "Submerging Deciduous Molars," Ang/eOrthod, 2:77-87, 1932.
19. Thornton, M. and Zimmermann, E. R.: "Ankylosis ofPrimary Teeth," I Dent Child, 31:120-126, 1964.
20. Eichenbattm, I. W.: "Tooth Eruption and Ankylosis,"]Prev Dent, 4:39-45, 1977.
21. Konstat, M. M. and White, G. W.: "Ankylosed Teeth: AReview of the Literature," J Mass Dent Soc, 24:74-78,1975.
22. Gorelick, L. and Geiger, A. M.: "Direct Bonding in theManagement of an Ankylosed Second Deciduous Molar,"I Am Dent Assoc, 95:307-309, 1977.
23. Bonin, M.: "Simplified and Rapid Treatment of AnkylosedPrimary Molars With an Amalgam and Composite Resin,"] Dent Child, 43:159-162, 1976.
24. Logan, W. H. G. and Kronfeld, R.: "Development of thoHuman Jaxvs and Surrounding Structures From Birth to
the Age of Fifteen Years," I Am Dent Assoc, 20:397-427,1933.
25. Wheeler, R. C.: Dental Anatomy, Physiology and Occlu-sion, 5th Ed., Philadelphia: W. B. Saunders Co., 1974,pp. 195-236.
26. Sicher, H., ed.: Orban’s Oral Histology and Embryology,5th Ed., St. Louis: C. V. Mosby Co., 1962, pp. 100-102.
27. Russell, W. L.: "The Differential Diagnosis of Fluorideand Nonfluoride Enamel Opacities," I Public Health Dent,21:143-146, 1961.
28. Goldman, H. M. and Cohen, D. W., eds.: PeriodontalTherapy, 5th Ed., St. Louis: C. V. Mosby Co., 1973, pp.319-321.
29. Freund, J. E.: Modern Elementary Statistics, New York,Prentice-Hall, 1952, pp. 198-219.
30. Kollar, E. J.: "Histogenetic Aspects of Dermal-EpidermalInteractions," in Slavkin, H. C., and Baretta, L. A., eds:Developmental Aspects of Oral Biology, New York: Aca-demic Press, 1972, pp. 125-149.
31. Rule, J. T., Zacherl, W. A., and Pfefferle, A. M.: "TheRelationship Between Ankylosed Primary Molars and Mul-tiple Enamel Defects," ] Dent Child, 39:29-35, 1972.
32. Steigman, S., Koyoumdjisky-Kaye, E., and Matrai, Y.:"Relationship of Submerged Deciduous Molars to RootResorption and Development of Permanent Successors,"J Dent Res, 53:88-93, 1974.
33. Hovell, J. H.: In Walther, D. P. ed.: Current Orthodontics,Bristol: Wright, 1966, p. 203.
34. ShaIer, W. G., Hine, M. K., and Levy, B. M.: A Textbookof Oral Pathology, 3rd Ed., Philadelphia: W. B. SaundersCo., 1974, p. 66.
35. Schour, I. and Massler, M.: In Brauer, J. C.: Dentistry~or Children, New York: McGraw-Hill, 1964, p. 117.
DRS. MESSER and CLINE are affiliated with theDepartment of Pediatric Dentistry, University ofMinnesota, Minneapolis, Minnesota.
Requests for reprints may be sent to Dr, LouiseBrearley Messer, Department of Pediatric Dentistry,University of Minnesota, Minneapolis, MN 55455.
PEDIATRIC DENTISTRYVoh 2, No. 1 47