Anesthesia & Analgesia For the Laboring Woman
40
ANESTHESIA & ANALGESIA FOR THE LABORING WOMAN
Transcript of Anesthesia & Analgesia For the Laboring Woman

ANESTHESIA & ANALGESIA FOR THE LABORING WOMAN

A BETTER PAIN SCALE
0: Hi. I am not experiencing any pain at all. I don’t even know why I am here.
1: I am completely unsure whether I am experiencing painor itching, or maybe I just have a bad taste in my mouth.
2: I probably just need a Band Aid.3: This is distressing. I don’t want this to be happening to
me at all.4: My pain is not f----ing around.5: Why is this happening to me???6: Ow. Okay, my pain is super legit now.7: I see Jesus coming for me and I’m scared.8: I am experiencing a disturbing amount of pain.
I might actually be dying.9: I am almost definitely dying.10: I am actively being mauled by a bear.11: Blood is going to explode out of my face at any moment!

WHAT DO WE NEED TO KNOW ABOUT PAIN CONTROL IN LABOR?
• Explain how gate-control theory applies to non-pharmacologic pain management
• Identify medications and side effects used for analgesia during labor
• List complications that can occur to the patient undergoing general anesthesia
• Describe nursing management during neuraxial anesthesia

“PAIN WITH A PURPOSE”
”Unlike other acute and chronic pain experiences,
labor pain is not associated with pathology but with
the most basic and fundamental of life’s
experiences – the bringing forth of new life.”
-Nancy Lowe, Ph.D., CNM, FACNM, FAAN
PAIN CONTROL
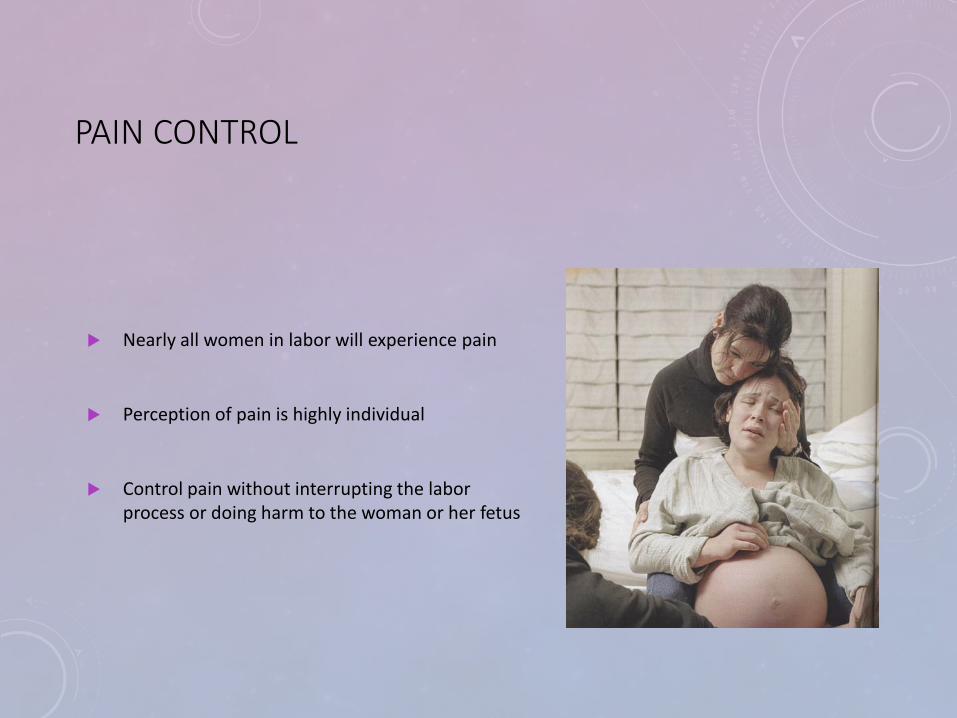
Nearly all women in labor will experience pain
Perception of pain is highly individual
Control pain without interrupting the labor process or doing harm to the woman or her fetus

FACTORS CONTRIBUTING TO PAIN IN LABOR
• Intensity and duration of contractions
• Rate of cervical dilation
• Perineal distention
• Size and position of fetus
• Procedures
• Fatigue


PSYCHOSOCIAL FACTORS CONTRIBUTING TO PAIN PERCEPTION
• Childbirth preparation
• Support persons
• Loss of control

CONTINUUM OF PAIN MANAGEMENT
Non-pharmacologic→→
Positioning
Walking
Massage
Relaxation
Hydrotherapy
Breathing techniques
Imagery
Music
Peanut/Birth Balls
Hypnosis
→→ Pharmacologic
Analgesics
Anesthetics

GATE-CONTROL THEORY OF PAIN TRANSMISSION
The gate control theory of pain asserts that non-painful input closes the "gates" to painful input, which prevents pain sensation from traveling to the central nervous system. Therefore, stimulation by non-noxious input is able to suppress pain.
Small and unmyelinated fibers: pain and pressure of uterus, cervix and pelvic joints
Large myelinated fibers: skin impulses
Habituation to sensation – use various techniques
PHARMACOLOGIC - ANALGESIA
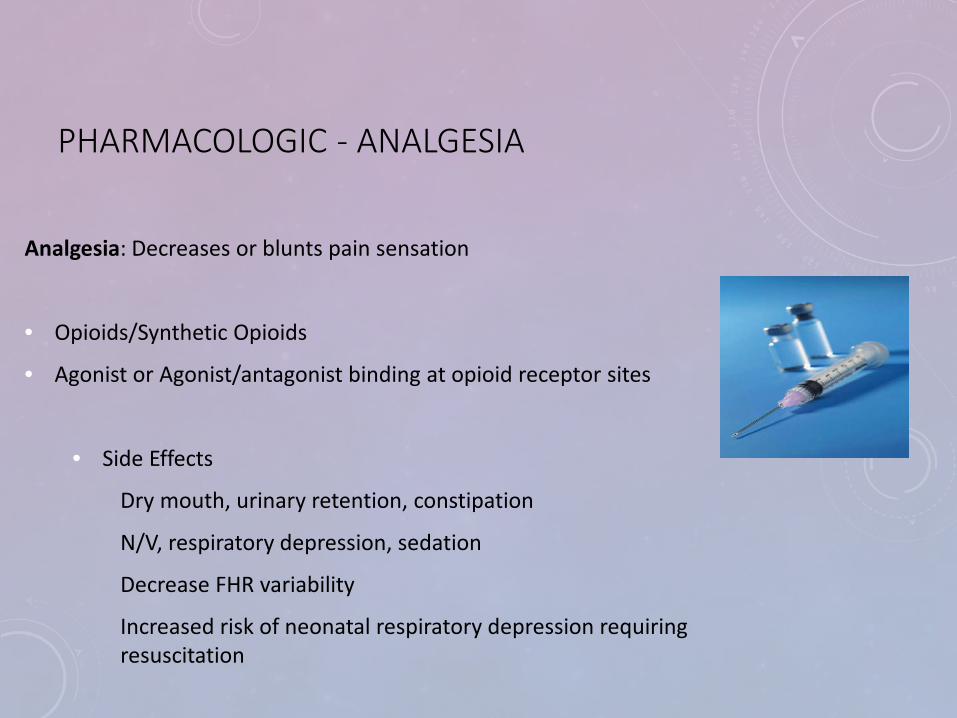
Analgesia: Decreases or blunts pain sensation
• Opioids/Synthetic Opioids
• Agonist or Agonist/antagonist binding at opioid receptor sites
• Side Effects
Dry mouth, urinary retention, constipation
N/V, respiratory depression, sedation
Decrease FHR variability
Increased risk of neonatal respiratory depression requiring resuscitation

FDA PREGNANCY CATEGORIES
A no risk demonstrated to the fetus in any trimester
B no adverse effects in animals, no human studies available
C only given after risks to the fetus are considered: animal studies have shown adverse reactions, no human studies available.
D definite fetal risks, may be given in spite of risks if needed in life-threatening conditions.
X absolute fetal abnormalities; not to be used anytime during pregnancy
FETAL DEVELOPMENT

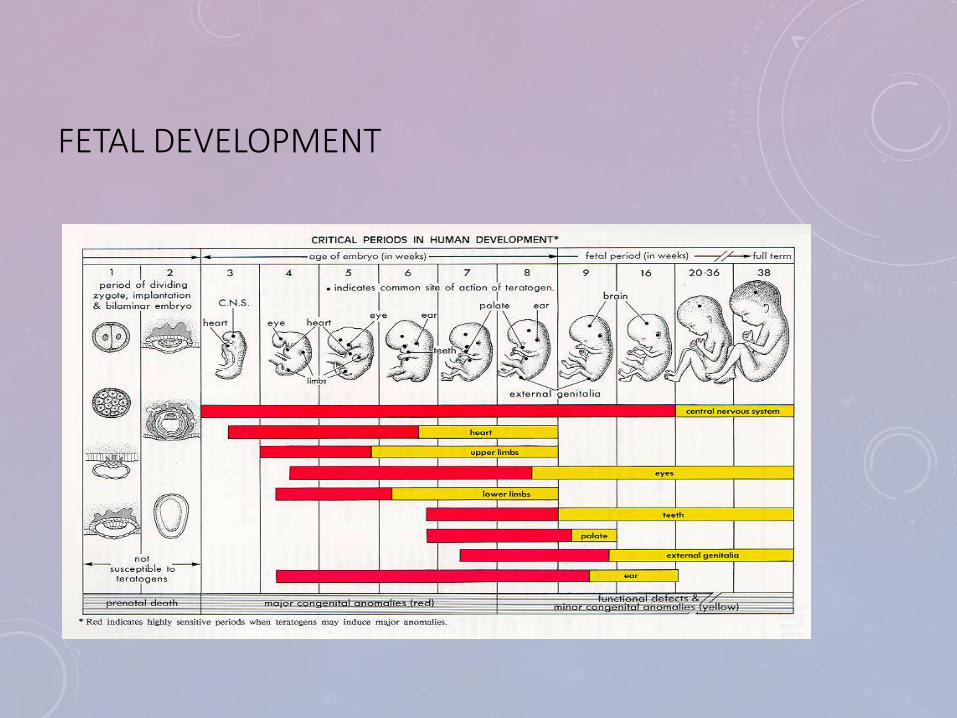
TIMING OF TERATOGENIC INSULT
• Week 1-2: all or nothing• Death or other cells assume its function
• No malformations
• Week 3-8: organogenesis• Major malformations
• Multiple systems are forming
• Week 9-term: organ systems damaged• IUGR
• Mental retardation
• Developmental / behavioral delays

COMMONLY USED PAIN MEDS IN LABOR
Drug Route Onset Duration Half-Life
Butorphanol 1-2 mg IV or IM 5-10 min IV30-60 min IM
4-6 hours 2-5 hours
Fentanyl 50-100 mcg IV or 2-4 minutes 30-60 minutes
3 hours
Morphine 2-5mg IV or5-10 IM
10 minutes IV30 minutes IM
1-3 hours 2 hours
Nalbuphine 10-20mg IM, IV, or SubQ 2-3 minutes IV15 minutes SubQ or IM
2-4 hours 2-5 hours
Remifentanil 0.15mcg-0.50 mcg/kg Q 2 minutes-PCA
20-90 seconds 3-4 minutes 9-10 minutes

PHARMACOLOGIC: INHALATIONAL ANALGESIA
Nitrous Oxide: 50:50 ratio of nitrous to oxygen• Colorless, Odorless• Administered via facemask or mouthpiece• Creates euphoric effect that decrease pain perception• Mostly used in UK, Australia, Finland, & Canada

CONTRAINDICATIONS TO NITROUS
• Inability to hold or self administer
• Recent collapsed lung, hx of gastric bypass
• Increased ICP or intraocular pressure
• Low B12 levels, Crohns disease, pernicious anemia

REMIFENTANIL
• Short acting opioid
• IV/PCA
• onset of action in 1minute, peak effects in 2 minutes, a constant half-life of 3 minutes, and complete elimination in 10 minutes
• 1:1, CEFM
• Side effect Respiratory Depression
EXTENDED – RELEASE EPIDURAL MORPHINE
• PF Morphine: achieves 12 to 24 hours of post-op for C/S
• Monitor at least hourly for 12 hours, then every 2 hours for 12 hours
• Adequacy of ventilations (RR, Depth)
• Oxygenation (Pulse Ox)
• Level of Consciousness
• Adverse effects
• Pruritis
• Nausea
• Respiratory Depression

PHARMACOLOGIC - ANESTHESIA
Anesthesia: Complete loss of sensation
Local anesthesia: Infiltration of perineum and vagina or pudendal nerve block
Potent vasodilators
Neuraxial anesthesia: Blocks sensation from a certain region of the body
General anesthesia: Complete unconsciousnessNurse assist with cricoid pressure during rapid
induction sequence.

TYPES OF ANESTHESIA
• Neuraxial Anesthesia/Analgesia:
Blocks sensation from a certain region of the body.
• Spinal Block:
Single injection of local anesthetic into subarachnoid space.
• Epidural Block:
Needle and catheter placement in the epidural space – before crossing the dura

NEURAXIAL ANESTHESIA
• ContraindicationsCoagulation disordersInfection at siteHypovolemia/shock/hypotension
• Relative contraindicationsFHR pattern associated with u/p insufficiencySpinal deformityVentricular outflow obstruction – aortic stenosis, hypertrophic
cardiomyopathy

NURSING CARE OF PATIENT UNDERGOING NEURAXIAL ANESTHESIA
• Insure informed consent is completed
• Insure patient’s questions are answered
• Bolus of IV fluid (LR, NS)

NURSING CARE OF PATIENT UNDERGOING NEURAXIAL ANESTHESIA
• Time out verification
Correct person
Correct procedure
Correct equipment
*(site & position)
• Positioning/ support of patient
Sitting or lateral
• Monitoring
VS
Pain perception
Fetal response
LOC & Level of Mobility
Site/tubing/pump functioning

NURSING CARE OF PATIENT UNDERGOING NEURAXIAL ANESTHESIA
RN can:
• Monitor mother & fetus
• Replace empty infusion bags with new of same medications & concentration according to anesthesia orders
• Stop infusion if there is safety concern or after the birth
• Remove catheter according to institutional policy after education
• Initiate emergency measures as indicated and notify anesthesia & OB care providers
• Communicate assessments and changes to maternal status to OB and Anesthesia care providers

NURSING CARE OF PATIENT UNDERGOING NEURAXIAL ANESTHESIA
RN cannot:
• Bolus or Re-bolus by injection or increasing infusion rate
• Increase or decrease infusion rate
• Re-initiate infusion once stopped
• Manipulate dose or interval rates of PCEA
• Obtain informed consent – however, may witness consentOBN Policy/Guideline # P-04

EPIDURAL PROCEDURE
• Site selection
L 3-5
• Prep and drape
• Local site infiltration
• Insertion of needle
16-18G
loss of resistance technique

ANATOMY OF SPINE

EPIDURAL PROCEDURE
• Insertion of catheter
• Test dose
Detect subarachnoid or intravascular injection
• Secure catheter
• Assessment of block
Sensory & motor
Onset of action
Missed segments (windows)
This Photo by Unknown Author is licensed under CC BY-SA

EPIDURAL PROCEDURE
Epidural Drugs
• Act on nerve fibers crossing the epidural space
• Bupivacaine & Ropivacaine
• Fentanyl
Reduces requirement of local anesthetic
Spares motor fibers
Reduces hypotension

COMPLICATIONS OF ANESTHESIAMALIGNANT HYPERTHERMIA
• Potentially lethal complication of inherited muscular disorder
• Administering volatile anesthetics or neuromuscular blocking agents triggers hypermetabolic state
• Symptoms:
Rise in end-tidal CO2
Muscle rigidity – masseter spasm
Tachycardia & tachypnea
Ventricular fibrillation
Hyperthermia (104 F)
Acidosis
Rhabdomyolysis – breakdown of muscle excreted in the urine – may result in renal failure
Organ Damage, DIC, Death
MALIGNANT HYPERTHERMIA ETIOLOGY
• Caused by imbalance of intracellular and extracellular Ca+.
• Increased breakdown of muscle extracellular K+ = dysrhythmia
• Sustained muscle contraction increase muscle work - load, oxygen consumption, lactic acid production acidosis and elevated temp. tachycardia, cardiac dysrhythmia, hypotension, reduced cardiac output and arrest.

COMPLICATIONS OF ANESTHESIA
MALIGNANT HYPERTHERMIA TREATMENT• Discontinue triggering anesthetic agents
• 100% oxygen
• Dantrolene sodium (Dantrium)/Ryanodex to restore Ca+ balance
• Cool – ice packs, cooling blanket, lavage
• Antiarrhythmics – no calcium channel blockers (may cause hyperkalemia)
• Post emergency care:
Blood gases, electrolytes, coag profile and UA
ICU 12-48 hours
Family education and referral for testing
MH Hotline: 1-800-644-9737

COMPLICATIONS OF ANESTHESIA
POST DURAL PUNCTURE HEADACHE
• 1-2% with epidural
• 70% of Dural puncture with 16G Tuohy needle
• Symptoms
Severe HA - sitting/standing, supine
Nausea/vomiting
Vertigo
• Treatment goal: replace lost CSF, seal puncture, control cerebral vasodilatation
Caffeine & opioids
Hydration
Epidural blood patch – 90+% effective

COMPLICATIONS OF ANESTHESIA
INTRATHECAL INJECTION
• Anesthesia level ascends toward the brain stem resulting in:
Severe hypotension
Bradycardia
Apnea
Cardiac arrest
Reversal within 1-2 hours with proper support ; IV fluids, ventilation, vasopressors

COMPLICATIONS OF ANESTHESIA
INTRAVASCULAR INJECTION
• Epidural space is richly vascular – negative aspiration is not a guarantee
Test dose – observe closely – wait 5 min – inject in small increments
Large doses of LA intravenously cause seizures, arrhythmias, and cardiac arrest
Act quickly: ABCD’s of resuscitation
Meds: thiopental or propofol for seizure activity
amiodarone, vasopressin, or epinephrine for arrhythmia
Bupivacaine Toxicity: intralipid emulsion

COMPLICATIONS OF ANESTHESIA
OTHER COMPLICATIONS• Spinal hematoma
Pain, muscle weakness, bowel/bladder dysfunctionMRISurgical intervention
• Spinal abscessHigh temperature, backache, malaiseRequires urgent surgical intervention
• Anaphylaxis SymptomsTreatment :Epinephrine & IV fluids
* Don’t Forget Fall
Risk
SPECIAL CONSIDERATIONS IN OPIOID DEPENDENT WOMEN WITH NEURAXIAL LABOR PAIN MANAGEMENT
• Avoid antagonists and agonist like Nalbuphine, Naloxone, or butorphanol
• If taking methadone or buprenorphine, should be continued at the usual dose during the peripartum period

SUMMARY
All have pros and cons & risk & benefits
Women who received neuraxial
anesthesia still need and can benefit from nonpharmacological
nursing interventions
Labor Pain is unique and individual with added components
of physiological, social, and
emotional stressors.Burke (2021). pg. 503

REFERENCES
ACOG (2019). Practice Bulletin 209. Obstetric Anesthesia and Analgesia.
American Society of Anesthesiologists. 2018. Statement on the role of registered nurses in the management of continuous regional analgesia. https://www.asahq.org/standards-and-guidelines/statement-on-the-role-of-registered-nurses-in-the-management-of-continuous-regional-analgesia
Association of Women’s Health, Obstetric and Neonatal Nurses. (2020) Analgesia and Anesthesia in the Intrapartum period. Washington, DC: Author. doi: 10.1016/j.nwh.2019.12.002
Association of Women’s Health, Obstetric and Neonatal Nurses. 2015. Role of the registered nurse (RN) in the care of the pregnant woman receiving analgesia/anesthesia by catheter techniques (epidural, intrathecal, spinal, PCA catheters) (Position Statement). Washington, DC:Author.
Burke, C.(2021). Pain in Labor: Nonpharmacologic and Pharmacologic Management. In Simpson, K.R., Creehan, P.A., O’Brien-Abel, N., Roth, C.K., & Rohan, A. J. (4th Eds), Perinatal Nursing (pp 466-508). Philadelphia: Lippincott Williams & Wilkins.
Oklahoma Board of Nursing (2018). Registered Nurse Monitoring Obstetrical Patients Receiving Analgesia/Anesthesia by Catheter Techniques (Epidural, PCEA, and Intrathecal Catheters) Guidelines. Retrieved from: https://nursing.ok.gov/prac-epidurob.pdf.

Don’t forget to completeYour evaluation athttp://opqic.org/opnf/bootcamp/