Anemia and Peripheral Smears
62
Anemia and Peripheral Smears July 21, 2021 ACP Internal Medicine Board Review Joyce Wipf, MD, MACP University of Washington, VA Puget Sound
Transcript of Anemia and Peripheral Smears

Anemia and Peripheral Smears
July 21, 2021
ACP Internal Medicine Board Review
Joyce Wipf, MD, MACP
University of Washington, VA Puget Sound
ANEMIA
Definition: anemia represents a decrease in O-2 carrying capacity; not a dx but a sign of underlying disease
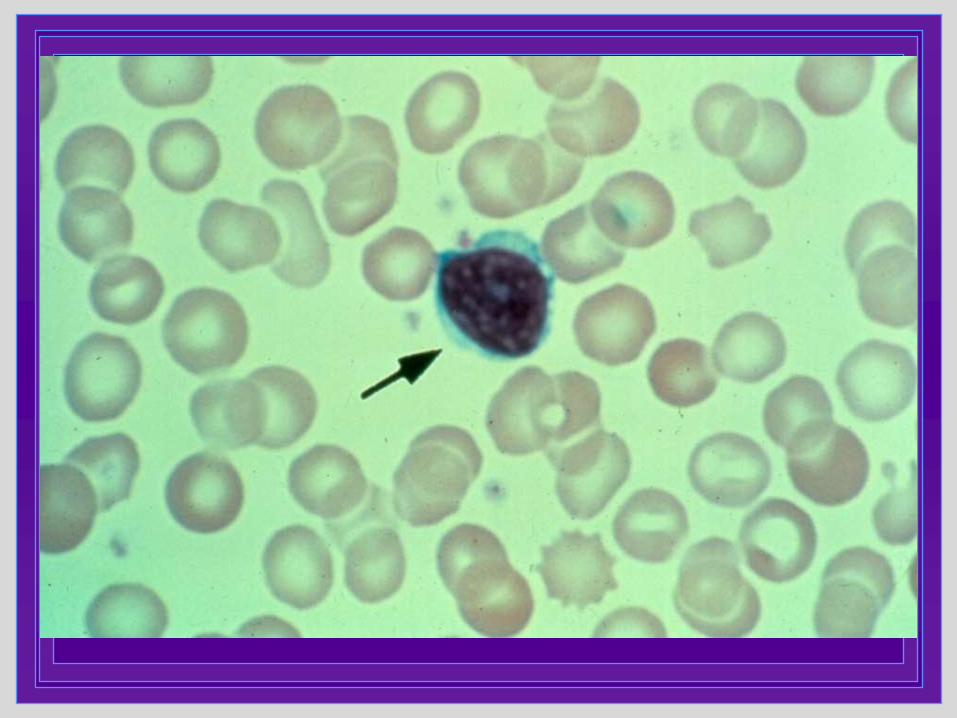
Peripheral smear is an important tool in diagnosis of type of anemia
Symptoms will vary depending upon:• Extent to which the O2 carrying capacity of the
blood is compromised
• Total change in blood volume/ rapidity of onset
• Manifestations of the underlying disorder that caused the anemia
•Coexistent disease that limits CV/pulm function
Case 1.The most common cause of anemia in women in the US is:
A. Anemia of chronic disease
B. Iron deficiency anemia due to low dietary intake
C. Iron deficiency due to blood loss
D. Macrocytic anemia due to alcohol
E. Vitamin B12 deficiency

Case 2. The most common cause of anemia in men in the US is:
A. Anemia of chronic disease
B. Iron deficiency anemia due to low dietary intake
C. Iron deficiency due to blood loss
D. Macrocytic anemia due to alcohol
E. Vitamin B12 deficiency
ETIOLOGY OF ANEMIA
Most common cause in US:– Women and children: Fe deficiency
• Blood loss in women, nutritional in children
– Men: anemia of chronic disease
• Fe deficiency is second
ETIOLOGY OF ANEMIA
1/3 of teens are anemic
Muscles are a prominent user of iron
Fe deficiency in Athletes:
▪ 50-80% of female athletes
▪ 10-17% of male athletes
CNS need for iron
▪ Test scores in young women improve after iron repletion

Mr. T. is admitted to Medicine with recurrent foot infection and gangrene.Diabetes Type 2, PVD
Labs: Hgb 10 Hct 30 MCV 80
What should be included in work-up of anemia in this pt? (not ARS case)
(note 1/3 of patients admitted to acute medicine are anemic)
What should be in the work-up of anemia?
Indices(MCV)
Retic indexPeripheral smear
Fe studies? Other (TSH, Bilirubin,
Macrocytic: B12, Folate)
Check other cell lines: wbc, plts

RETICULOCYTE COUNT
Reticulocytes are immature RBCs recently released into peripheral circulation from the bone marrow
On peripheral smear appear as larger, slightly blue RBCs (polychromasia)
Retic count measured with special stain as a percentage
Must be corrected (indexed) for HCT• Elevation suggests hyperproliferative process
• Decrease suggests hypoproliferative process
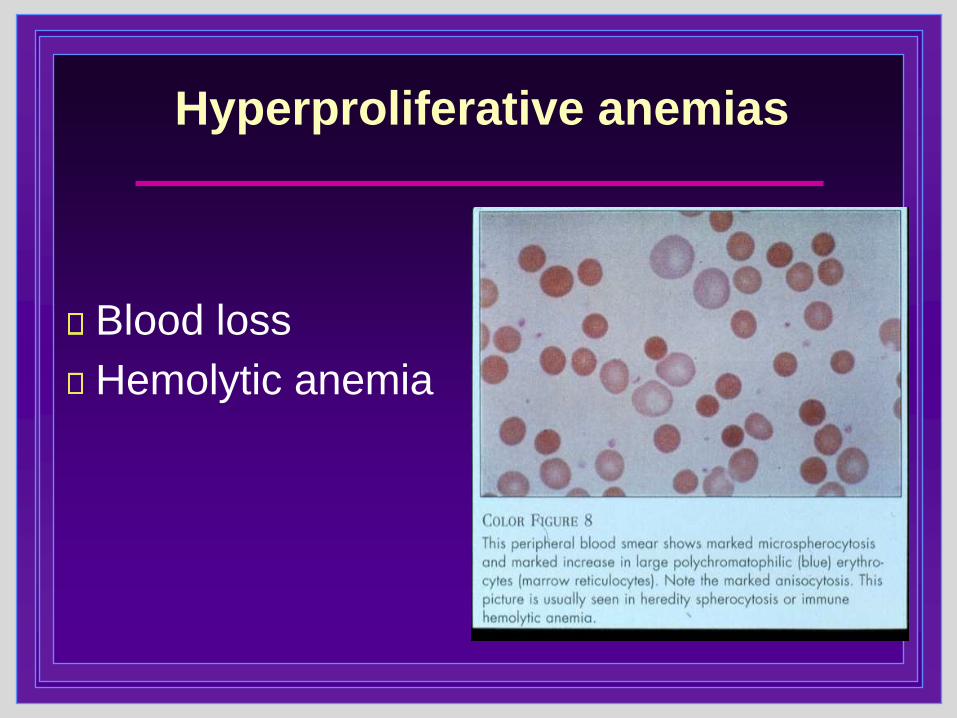
Hyperproliferative anemias
Blood loss
Hemolytic anemia
Harrison’s Principles of Internal Medicine
Hypoproliferative anemias
Early iron deficiency
Anemia of chronic disease
Anemia of renal failure
Anemia with endocrine conditions▪ ie hypothyroidism, adrenal insufficiency
hypogonadism
Marrow disorders ▪ myelofibrosis, myelodysplasia
HIV
Megaloblastic anemias

Case 3.Pt is a 33 yr old woman who comes in for evaluation after turned down for blood donation due to anemia. Last donation 1 unit 6 months ago.
Sx: diminished energy, trouble keeping up with her 3 yr old.ROS: menorrhagia x ~4 cycles.Exam: BP 110/56, HR 50, wt 149 lbsHEENT: pink mucous membranes
GYN exam nl.
Labs: WBC 6.0 Hgb 9.6 Hct 29% MCV 76TSH 43
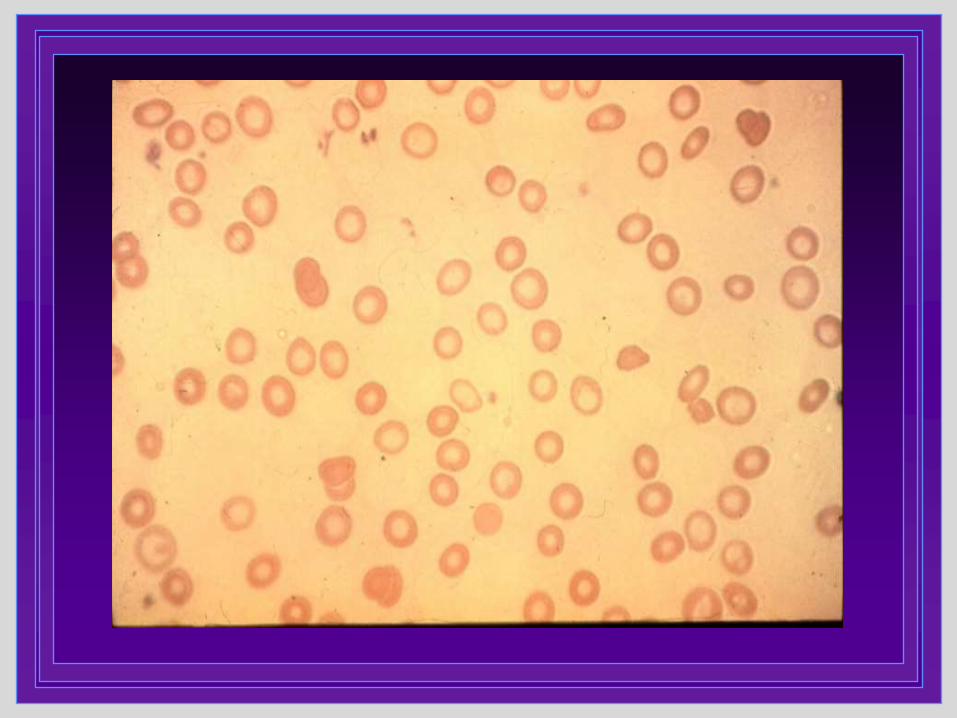
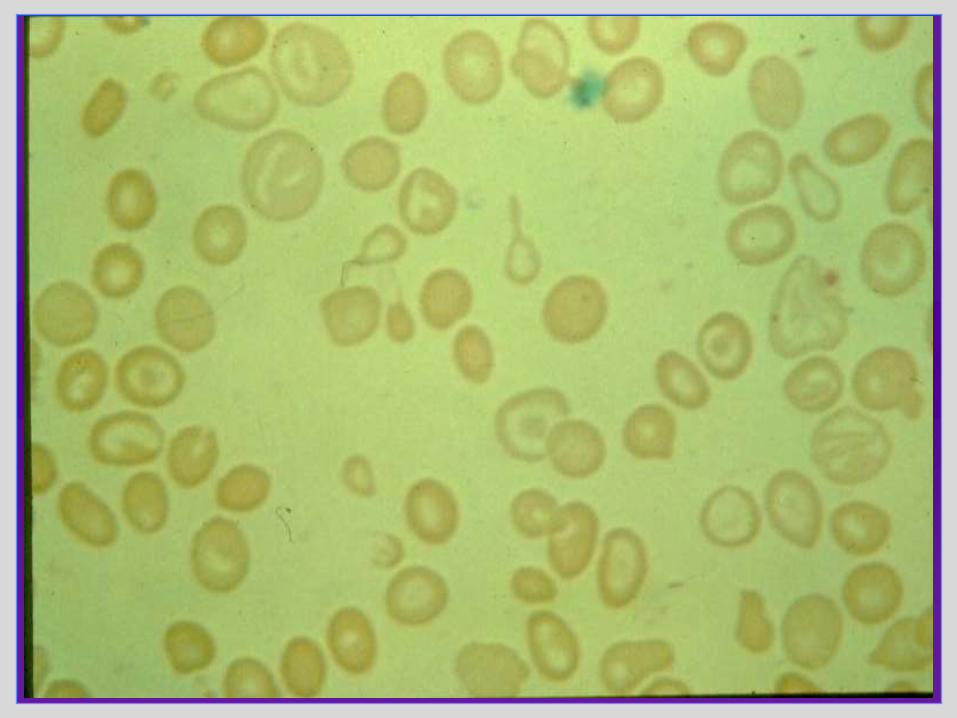
Peripheral smear is shown.
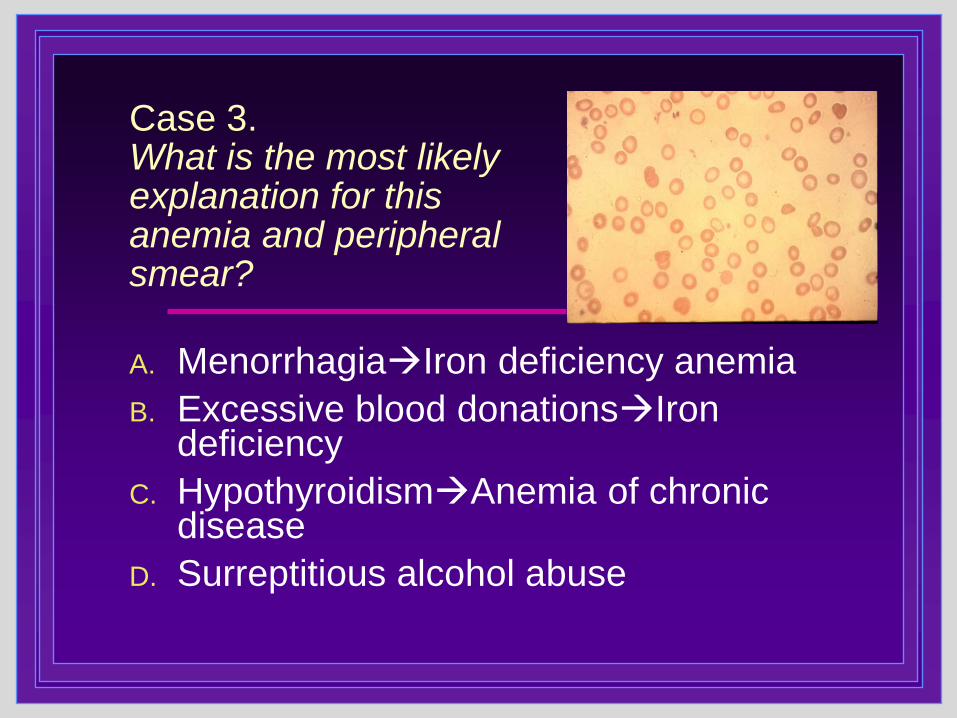
Case 3.What is the most likely explanation for this anemia and peripheral smear?
A. Menorrhagia→Iron deficiency anemia
B. Excessive blood donations→Irondeficiency
C. Hypothyroidism→Anemia of chronic disease
D. Surreptitious alcohol abuse
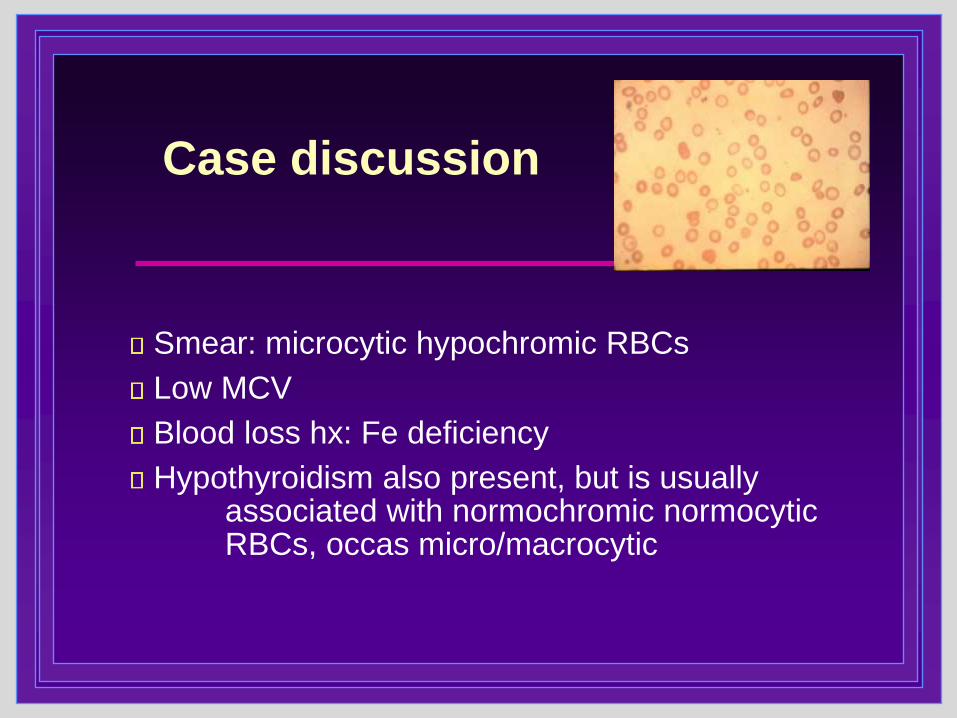
Case discussion
Smear: microcytic hypochromic RBCs
Low MCV
Blood loss hx: Fe deficiency
Hypothyroidism also present, but is usually associated with normochromic normocytic RBCs, occas micro/macrocytic


IRON DEFICIENCY:Clinical Features
Pica: an unusual desire to eat substances of little nutritional value: clay, ice, starch
Angular cheilitis
Glossitis with papillary atrophy of the tongue
Spoon nails (koilonychia) or brittle nails
CHF, dyspnea
New systolic murmur
Case 4.Pt is a 42 year old male with diabetes, recently started on hemodialysis for ESRD. He is chronically on anticoagulation for recurrent DVT. In routine evaluation, the patient notes six episodes of BRBPR x 3months. No postural sx.Exam: BP 138/88, pulse 84, alert, NAD. Abdomen benignRectal: brown stool, heme negative; no external hemorrhoids, no mass palpable
Labs: Hgb 10.2, hct 31%, WBC 6.2, plts 386KFe 42/ TIBC 199/ Sat 18%/ Ferritin 188Peripheral smear is viewed.

Case 4.The most likely cause of this patient’s anemia and smear findings:
A. Iron deficiency anemia secondary to GI blood loss
B. Anemia of chronic disease
C. Vitamin B12 deficiency
D. Hemolysis from dialysis

Case discussion
• Smear: normochromic normocytic RBCs
• Fe studies c/w anemia of chronic disease
• Other etiologies of anemia possible (has some blood loss, etc) but smear and MCV don’t fit Fe deficiency

Comparison of Fe def and ACD
Test Fe Deficiency ACD
Serum Iron (nl 50-150) Very low (<25) Low
- bound iron transported by transferrin
TIBC High nl or high Nl or low
- measures available transferrin binding sites
% Saturation <15% Slightly low
- Percent of transferrin sites bound by iron
Ferritin* Low (<50 mcg/L) Nl or high
- intracellular storage form of iron
Transferrin receptor High Normal- not acute phase reactant
Case 5.Which symptom is associated with ferritin levels <50?
A. Leg cramps
B. Numbness of the feet
C. Foot pain
D. Restless legs

Restless Leg Condition
Check a ferritin level (is the only useful blood test in patient with restless legs)
Rx for iron deficiency if ferritin <50
Anemia may or may not be present

Treatment of Iron Deficiency
Target Ferritin level? (>50)
Fe Gluconate or Fe Sulfate
• If can tolerate, Fe Sulfate better absorbed
• Takes 6 wks to correct anemia, 6-12 m to replete Fe Stores
Dose recommendations?
• Daily or QoD (not TID)
• Affects other meds, less Fe absorption with higher dose
Do you give with Vitamin C? (common practice, not strong evidence)
When to use IV Fe? Severe Fe def, sx

Ferritin levels: What is normal?
No physiologic reason why women would have lower ferritin levels than men
Normals set by lab
Study (BMJ 2003) of non-anemic women:
• Randomized to Fe Rx or none
• Energy level signif improved in treated group if ferritin <50
Consider Fe deficiency if ferritin <50 (regardless of lab setting normal at 10 or 30…)
Low Ferritin: GI disease?
Study of older patients with ferritin <50 (Am J Gastroenterol 1998)
• Serious GI pathology in over half
• Cancer 10%
Important to rule out GI disease in older patients, and in younger who have persistent sx

Anemia of Chronic Disease
ACD most common anemia among hospitalized patients; #1 cause in elderly US men
3 classic conditions: infection, inflammation, neoplasia
• Other: trauma, liver dz, renal dz, endocrine
• 70% pts with severe CHF have ACD
• COPD, DM
May coexist with other types of anemia
Anemia typically develops over months, but abnormalities in Fe studies over 2-3 wks
Labs: Anemia usually mild, Hgb 7-8, Hct >25%, occas severe;
1/3 microcytic

Anemia of chronic renal disease
ESRD: Erythropoetin Rx→
• Be sure not also Fe deficient: Rx Ferritin <100 in ESRD
• Recommend Hgb 10-12, partial correction
RCTs showed increased CV events/ CKD progression if correct anemia to normal
– NEJM 1998 (Besarab)
– CHOIR trial NEJM 2006 (Singh)
– CREATE trial NEJM 2006 (Dureke)
Transfusion
Expect Hgb/Hct to rise by 1 and 3 points respectively per unit
When to Transfuse: General rule is when Hgb <7/ Hct<21%; (vs <25%)
• Some situations where want to achieve higher levels
- if actively bleeding
- highly symptomatic
- severe cardiovascular disease (ie angina precipitated)
- planned surgery with anticipated significant blood loss
Case 6.A 27 yr old man with stated SE Asian ethnicity comes in for a routine exam required for employment. He is in good health, without weight loss, fatigue or bleeding symptoms.Exam is unremarkable and the pt has no hepatosplenomegaly. Negative stool FIT test.FH negative for anemia
Labs:
WBC 5.3, Hgb 11.4, Hct 35%, MCV 65,
Plts 330K.
Retic index 0.8%.

Case 6.What is the best test to confirm the most likely cause of this patient’s anemia?
A. Obtain CBC on siblings
B. Perform ultrasound for spleen size
C. Measure serum ferritin and iron studies
D. Check glucose-6-phosphate dehydrogenase screen
E. Perform hemoglobin electrophoresis
Evaluation of microcytic anemia
Thalassemia trait: suspect when mild anemia and marked microcytosis (MCV <70)
• Clues: ethnicity (Mediterranean, Asian)
lack of symptoms
(often negative FH)
• Dx thal trait: Hemoglobin electrophoresis
Thalassemia:• splenomegaly, abnormal smear, high retic
Iron deficiency anemia: usually more pronounced microcytic anemia than thal trait
• sx with exertion, bleeding hx, menorrhagia/metorrhagia

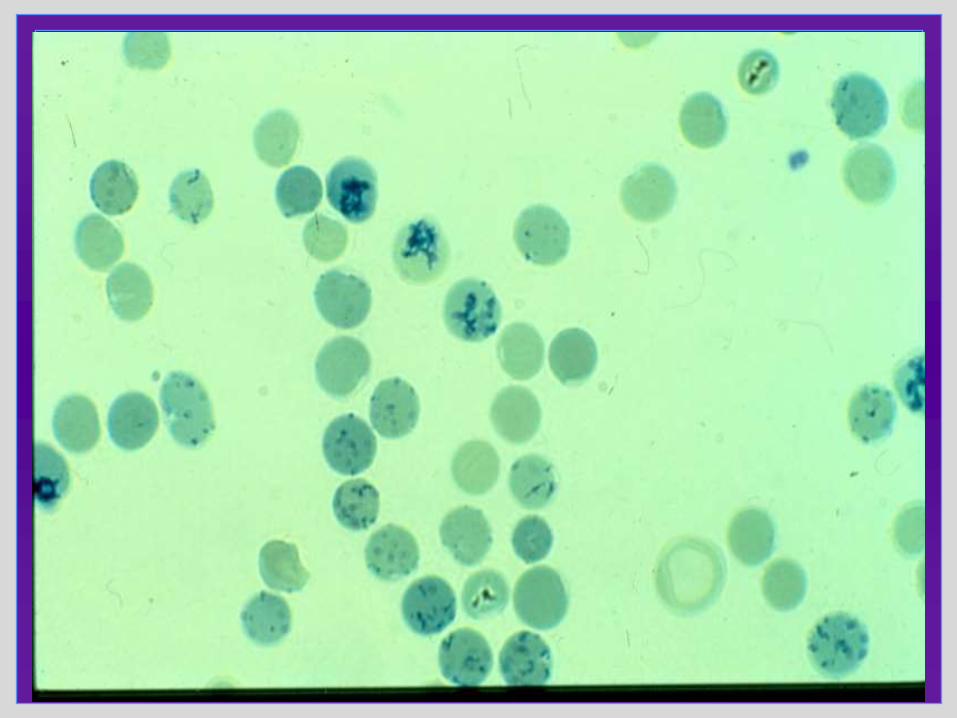
Case 7.The peripheral smear showed numerous abnormal speckled red cells.What is this patient’s diagnosis?
A. Mercury toxicity
B. Lead toxicity
C. Arsenic toxicity
D. Cadmium toxicity

Case 8.What percentage of outpatients >age 65 have macrocytosis without anemia?
A. 3%
B. 5%
C. 10%
D. 15%
E. 20%

Evaluation of macrocytosis in outpatients
➢ Present in 10% of adults in outpatient setting
(MCV to 96; 2-4% MCV >100)
Evaluation:
➢ ? Anemia present
➢ Mild: Consider hypothyroidism
➢ MCV > 110: vitamin B12/folate
➢ ETOH assessment, usually other clues

Case 9.You are working up a 74 yr old woman for anemia and mild cognitive impairment: Labs: Hgb 9.9, hct 31%, MCV 118 with 2+ anisocytosis, 2+ poikilocytosis. Vitamin B12 level is 210 (nl 200-900); Folate level is normal. Methylmalonic acid is high. Homocysteine level is high. What is the most likely diagnosis?
A. Folate deficiency
B. Vitamin B12 deficiency
C. Neither Vitamin B12 or folate deficiency


B12, Folate, MMA and Homocysteine: challenges
Low normal B12 levels are nonspecific
Serum folate levels return to normal after several good meals, and RBC folate levels may be unreliable
Decreased folate may cause low B12 concentrations due to metabolic blocks
Deficiency of either Vitamin B12 or folate can increase homocysteine, an amino acid
• Low B12 or folate and high homocysteine may be assoc with increased CV risk (Framingham data, other)
High Methylmalonic acid levels helpful in Dx Vit B12 deficiency: high MMA strong association with low or low normal (150-300 ng/ml) Vitamin B12 levels.
• MMA levels drop after 3m of Rx B12
If elevated Homocysteine and normal MMA→dx folate def.
Klee, Clin Chem 2000; 46:1277-83
Cochrane Review 2008

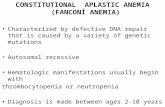
Vitamin B12 deficiency
Macrocytic anemia, MCV typically 110-140
Smear: macro-ovalocytes, hypersegmented PMNs
Neurologic sx (presenting sx in 30%):
• Stocking/glove paresthesias, poor proprioception & vibratory
• Dementia
• Loss of perception of smell
Glossitis with a beefy smooth-appearing tongue
Anemia may not be present or may be mild
Vitamin B12 deficiency - 2
B12 Deficiency common!
• One study of patients >60:
• 6% B12 deficiency
• 16% marginal stores
Causes: rarely dietary; usually decreased production of Intrinsic factor (autoimmune, gastrectomy), decreased ileal absorption
• Medications to decrease stomach acid can contribute to B12 deficiency (PPIs, antacids)
• Metformin Rx assoc with B12 deficiency
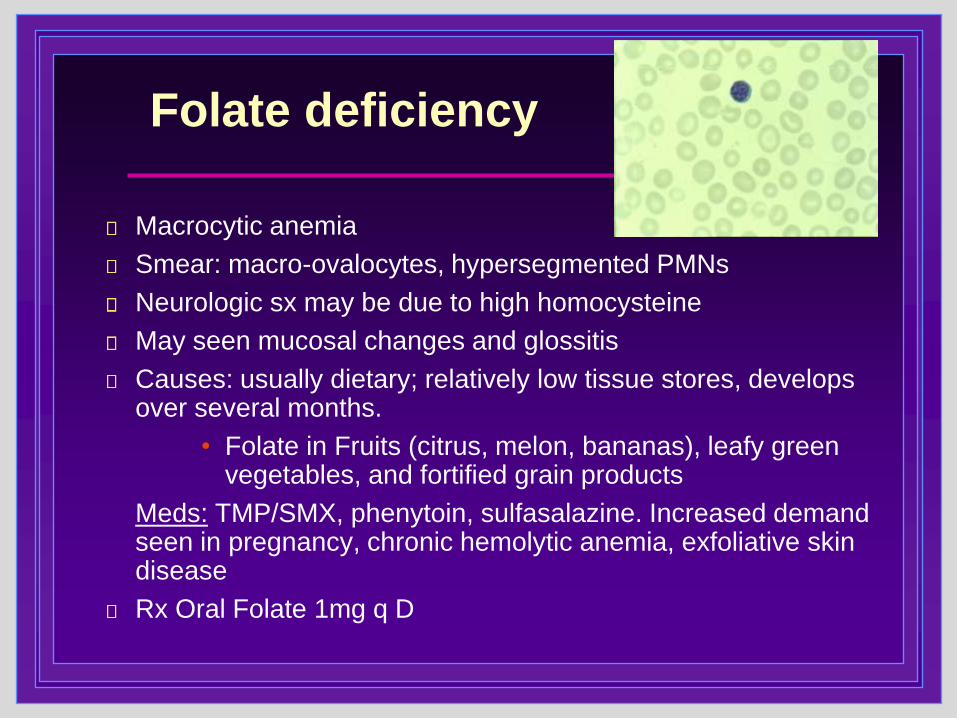
Folate deficiency
Macrocytic anemia
Smear: macro-ovalocytes, hypersegmented PMNs
Neurologic sx may be due to high homocysteine
May seen mucosal changes and glossitis
Causes: usually dietary; relatively low tissue stores, develops over several months.
• Folate in Fruits (citrus, melon, bananas), leafy green vegetables, and fortified grain products
Meds: TMP/SMX, phenytoin, sulfasalazine. Increased demand seen in pregnancy, chronic hemolytic anemia, exfoliative skin disease
Rx Oral Folate 1mg q D

Case 10.A 46 yo woman presents with severe jaundice and mild RUQ abdominal pain. She denies alcohol use.
Meds: Multivitamin, anti-histamines
PMH: Non-smoker, no substance use. FH: Neg for Cancer or liver disease
Exam: Pt alert, normal MSMarked icterusHepatomegaly to 16cm, Spleen not palpableNo fluid wave or shifting dullness
Labs:
WBC 7.3
Hgb 10.5, Hct32% MCV 86 Plts 86KTotal Bili 51 (direct 18)AST 650
ALT 588
Alk phos 350
Smear shown.

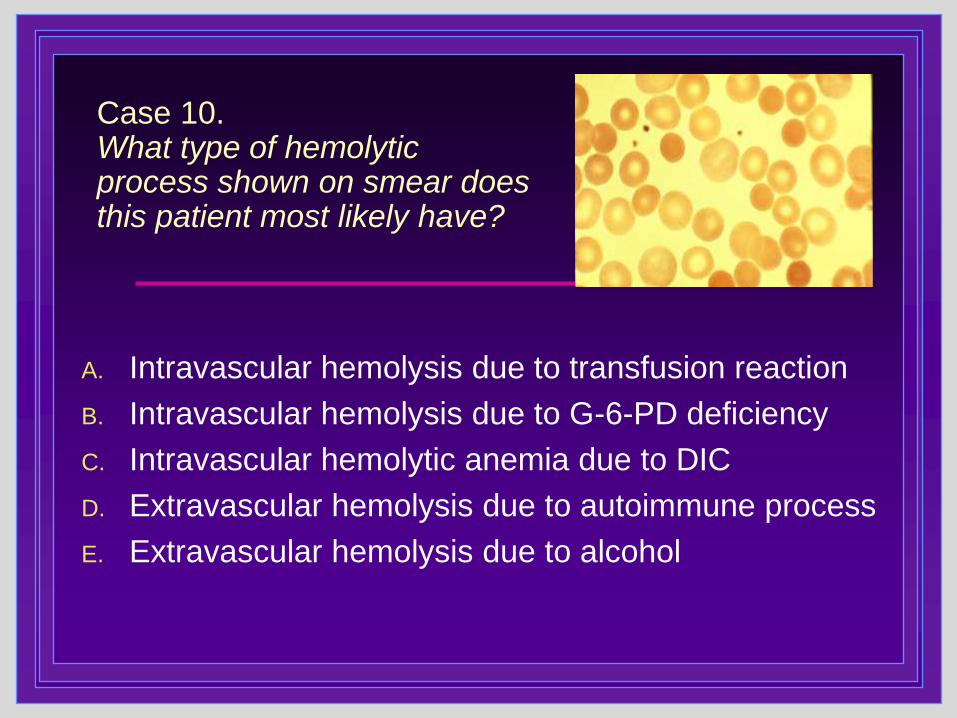
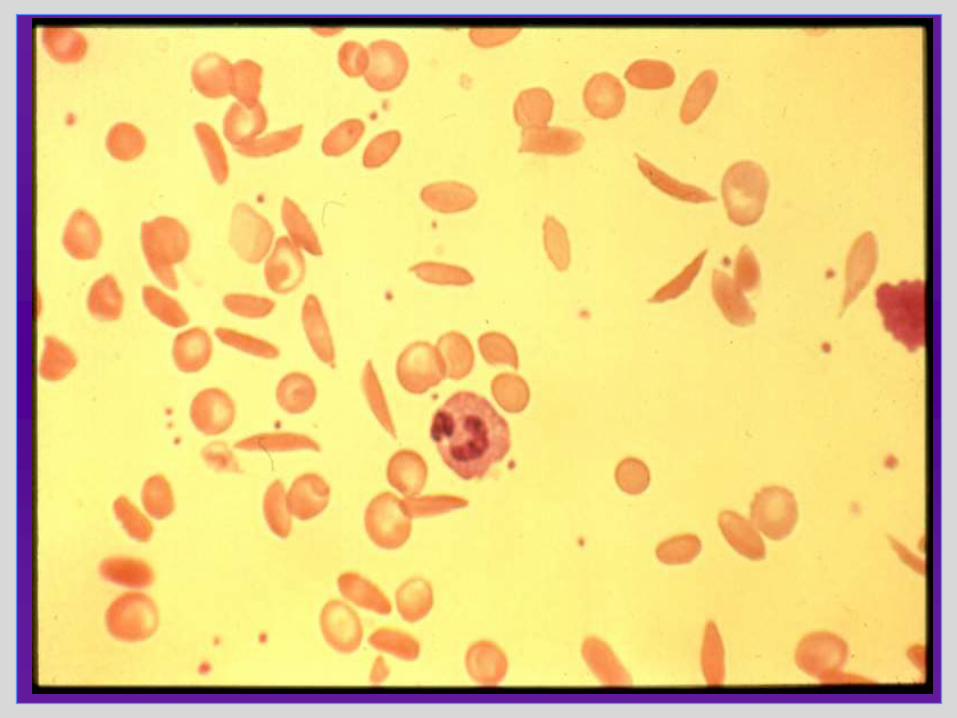
Case 10. What type of hemolytic process shown on smear does this patient most likely have?
A. Intravascular hemolysis due to transfusion reaction
B. Intravascular hemolysis due to G-6-PD deficiency
C. Intravascular hemolytic anemia due to DIC
D. Extravascular hemolysis due to autoimmune process
E. Extravascular hemolysis due to alcohol
Hemolytic anemia
Extravascular hemolysis
More common than intravascular hemolysis
RBCs sequestered in spleen and liver, then destroyed by macrophages
RBCs abnormal:
Coated with AB or structurally abnl and not released by the spleen
Haptoglobin declines, but detectable
NO hemosiderinuria or hemoglobinuria
Mild elevation of LDH
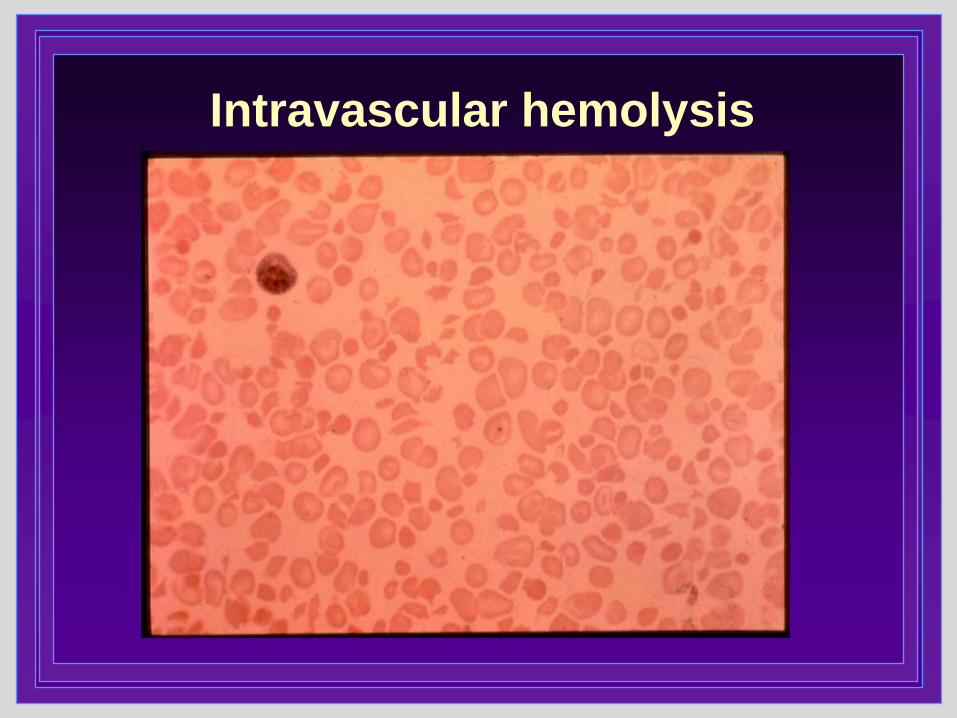
Intravascular hemolysis

Hemolytic anemia
Common features:
• Splenomegaly
• Jaundice
• Elevated unconjugated bilirubin
• Marked reticulocytosis
Intravascular hemolysis
RBCs destroyed directly in the circulation
Hgb released and binds haptoglobin-->
low or absent serum haptoglobin
Renal filtration of hgb-->urinary hemosiderin
Hemoglobinuria
Very high serum LDH levels

Hemolysis: Peripheral Smear
Extravascular hemolysis
• Subtle
• Spherocytes (small round RBCs without central pallor)
(as in case)
Intravascular hemolysis
• Dramatic
• Fragmented RBCs



Case 11.
A 54 yr old man is transferred from Alaska for further
work-up of anemia. He works as a railway attendant,
healthy until fatigue 2m ago. At that time, he had a
Hgb of 6.9, Hct 21%, MCV 94, platelets 160K.
He was transfused 2 units of prbcs→Hgb 8.7.
He became asymptomatic and declined work-up;
returned to work for six weeks. Symptoms
recurred→Hgb 6.8%
Exam: Pallor of mucous membranes and palmar
creases, No adenopathy; +Hepatosplenomegaly.
Bone marrow was performed on admit, results
pending.
Case 11, cont.Admission reticulocyte index 15%. Hgb 6.5→8.7 after transfused 2 u prbcs.Hgb 8.6% the next morning.
Now 12 hrs later, the lab calls with critical result: PM Hgb drawn by the nurse = 5.0 (rechecked by lab). Pt evaluated: asymptomatic. Stool heme neg.
What is the best explanation for the decrease in Hgb?
A. The patient has increased hemolysis
B. The patient is bleeding
C. Blood sample was drawn from vein with IV fluids
D. Hematology lab error
Google image, CDC website


Anemia Summary
Use MCV, retic, and smear to help identify cause of anemia
Common to have more than one cause of anemia co-existing
Iron studies important, may be hard to interpret
• Ferritin best readily available test, but has limitations
• Fe, TIBC and % sat helpful in ACD
B12 deficiency common in elderly; absorption affected by meds
Check other cell lines to be sure not pancytopenia

Anemia Answer Sheet
Case 1. C Case 7. B
Case 2. A Case 8. C
Case 3. A Case 9. B
Case 4. B Case 10. D
Case 5. D Case 11. C
Case 6. E
Good luck!