Androgenetic Alopecia 8-12
20
ANDROGENETIC ALOPECIA IN 3 RD DECADE -A PREDICTOR OF CARDIOVASCULAR RISK???
-
Upload
khalifa-al-wishahi -
Category
Documents
-
view
11 -
download
0
description
Androgenetic Alopecia
Transcript of Androgenetic Alopecia 8-12

ANDROGENETIC ALOPECIA IN 3RD DECADE -A PREDICTOR OF
CARDIOVASCULAR RISK???

INTRODUCTION• Androgenetic alopecia is the medical term for baldness, once known as male pattern baldness, but recently refers to both
men and women.• it is lost in a defined pattern and with men it usually begins above the temples along the hairline causing the hairline to begin
to recede.• The etiology and pathogenesis of AGA are not fully understood yet. Hamilton referred to mutual interplay of genetic factors,
androgens, and age factors in the origin of AGA • The etiology of coronary heart disease is related to multiple risk factors. The most common risk factors are family history of
premature CAD, hyperlipidemia including hypercholesterolemia, obesity, hypertension, cigarette smoking, diabetes mellitus, type-A personality, and emotional stress [18]. Although, for a long time, male gender has been suggested as a risk factor of CAD, the presence or absence of a hormonal (androgenic) relationship in both men and women is not well investigated.
• The etiology of coronary heart disease is related to multiple risk factors. The most common risk factors are family history of premature CAD, hyperlipidemia including hypercholesterolemia, obesity, hypertension, cigarette smoking, diabetes mellitus, type-A personality, and emotional stress [18]. Although, for a long time, male gender has been suggested as a risk factor of CAD, the presence or absence of a hormonal (androgenic) relationship in both men and women is not well investigated and there is not convincing evidence in favor of such a relationship in the medical literature.
• This type of baldness in men has on occasion been associated with other medical conditions such as coronary heart disease, an enlarged prostate, prostate cancer, diabetes as well as high blood pressure.
• Androgenetic alopecia(AGA) is an androgen induced disorder that is characterised by hair loss in genetically predisposed men.• It is considered to be associated with coronary heart disease(CHD) but the explanation of this association remains unknown.• Androgenetic alopecia (AGA) has been related to an increase in cardiovascular risk, but the mechanism of this association has
not been elucidated.• Several studies have confirmed a correlation between coronary heart disease and AGA. Early onset of AGA seems to be a risk
factor for early onset of coronary heart disease.• Most of the related studies have been done in 5thdecade but whether early onset androgenic alopecia is a marker of
cardiovascular risk factors can only be established if studied in younger age group.

• Many explanations have been proposed including overexpression of mineralocorticoid receptors targeted to the skin, insulin resistance, atherosclerotic processes, higher levels of androgen that may contribute to both atherosclerosis and thrombosis, adverse effects of lipid-lowering or antihypertensive drugs.
• IN THE LAST decade, several articles have indicated that bald men have a higher-than-normal risk for coronary artery disease (CAD) and that early-onset androgenetic alopecia (AGA), in particular, is somehow related to CAD. Such conclusions cannot be underestimated by dermatologists who treat with patients with AGA and who may prescribe systemic drugs. On the other hand, most of these articleshave been written by nondermatologists, without confirmation by specialists in dermatology.
• An epidemiological study with baldness as the primary hypothesis could also be undertaken. Progressing baldness can be considered as a manifest indicator of possible major risk for CAD, and balding young men may benefit from early aggressive screening of other better-known risk factors for CAD.

AIMS & OBJECTIVES
• To compare the level of lipid profile, body mass index, blood pressure and fasting sugar levels among cases of androgenetic alopecia and normal controls.
• To see whether these markers were significantly associated with androgenetic alopecia or not.
• To determine whether early onset androgenetic alopecia can be a first visible marker for adverse cardiovascular event.

METHODOLOGY• This study was designed and conducted as a case-control study with
25 cases in the patient and 15 cases in control group respectively. •We included all males with androgenetic alopecia (Grade III and higher according to Hamilton-Norwood) between age gp 25-35 yr attending skin opd. • We excluded males aged above 35 years or who are on lipid
lowering drugs.• We had taken detailed history and examine patient properly. • We had taken control from health check up scheme in our hospital
with minimal confounding factor error.• Serum lipid profile, body mass index, blood pressure and fasting
sugar levels were assessed in both groups.• We had applied Unpaired T- test for statistical analysis.

RESULTS• Patient and control groups each consisted of 25 male cases &
15 male cases respectively. • Comparison of cases and control:
CASES CONTROLS
MALES 25 15
AVERAGE AGE 26.2 26.5
H/O SMOKING 0 0
H/O ALCOHOL 0 0
F/H OF ALOPECIA 13 (52%) 2 (13.33%)
F/H OF HTN 10 (40%) 3 (20%)
F/H OF DM 6 (24%) 1 (6.66%)
F/H OF HYPERLIPIDEMIA 2 (8%) 0

Age group at the time of presentation
AGE OF ONSET TOTAL PERCENTAGE<15 0 0
15-20 1 4%
21-25 24 96%
26-30 0 0
31-35 0 0

Grade of androgenetic alopecia at time of presentation
GRADE OF ALOPECIA NO. OF PATIENTS PERCENTAGE
III 6 24%
IIIa 1 4%
IIIv 7 28%
IV 8 32%
IVa 2 8%
V 1 4%
• More than 50% cases were in grade IIIv &IV.

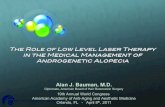
Comparison of means between cases and control
BMI(k
g/m2)
AG(cm)
BP(systo
lic)
BP(diasto
lic)
PULSE
FBS(m
g/dl)
0
20
40
60
80
100
120
140
CASESCONTROL

CASES CONTROLS
BMI (25) Elevated 3 (12%) 4 (26.67%)
Normal 22 (88%) 11 (73.33%)
Waist circum. (102) Elevated 1 (4%) 0
Normal 24 (96%) 15 (100%)
BP (130/85) Elevated (%) (%)
Normal (%) (%)
FBS (100) Elevated 8 (32%) 1 (6.67%)
Normal 17 (68%) 14 (93.33%)

CASES CONTROL
TOTAL CHOL. (200) Elevated 2 (8%) 3 (20%)
Normal 23 (92%) 12 (80%)
TG (150) Elevated 2 (8%) 2 (13.33%)
Normal 23 (92%) 13 (86.67%)
HDL (<40) Abnormal 9 (36%) 4 (26.66%)
Normal 16 (64%) 11 (73.34%)
LDL (100) Elevated 20 (80%) 7 (46.66%)
Normal 5 (20%) 8 (53.34%)
VLDL (30) Elevated 4 (16%) 2 (13.33%)
Normal 21 (84%) 13 (86.67%)
TC/HDL (5) Elevated 2 (16%) 1 (6.66%)
Normal 21 (84%) 14 (93.34%)
LDL/HDL (3.5) Elevated 3 (12%) 1 (6.66%)
Normal 22 (88%) 14 (93.34%)

PARAMETERSP value by
unpaired t-test (2- tailed)
Significance
BMI 0.558 Not significant
WAIST CIRCUMFERENCE
0.945 Not significant
BP (SYSTOLIC) 0.156 Not significant
BP (DIASTOLIC) 0.694 Not significant
FBS 0.185 Not significant

PARAMETERSP value by
unpaired t-test (2- tailed)
Significance
TOTAL CHOLESTEROL
0.564 Not significant
TRIGLYCERIDE 0.178 Not significant
HDL 0.418 Not significant
LDL 0.264 Not significant
VLDL 0.514 Not significant
TC/HDL 0.376 Not significant
LDL/HDL 0.232 Not significant

• No significant differences were present in mean values of age, waist circumference, BMI, blood pressure, FBS, lipid profile between patients with AGA and controls.

Comparison with other studies….
• Mantilainen, Koskela and Keinanen Kiukaanniemi reported an association between early-onset AGA and insulin resistance in males, but the mechanism of action has not been elucidated.
• An association between early-onset AGA and hyperglycemia /type 2 diabetes was observed in the Salvador Arias study.

Study Positive relation
1 Salvador Arias study early-onset AGA and hyperglycemia /type 2 diabetes
2 Trevisan et al. [5] in their study on CAD risk factors concluded that patients with
fronto-occipital baldness had on the average higher serum cholesterol and blood pressure compared to participants of similar age with no baldness.
3
4

CONCLUSION
• A statistical analysis between AGA and hypertension, obesity, hyperglycaemia and
hyperlipidaemia was not significant.• The study of wider sample would confirm these
findings and would permit analysis of the pathogenic mechanisms underlying the increase in cardiovascular risk in patients with AGA.
• If linked then balding-young men may benefit from early aggressive screening of other better-known risk factors for CHD.

• Progressing baldness can be considered as a manifest indicator of possible major risk for CAD
• Androgenetic alopecia could be considered as a clinical marker of a risk for hypertension,
• If this observation is extended and confirmed in additional studies, it may be prudent to
follow up patients with early onset AGA for the development of cardiovascular risk factors to permit an earlier diagnosis of an unknown hyperglycemia or diabetes and initiation of appropriate treatment.• Further studies must be conducted to determine the impact of
these changes on cardiac risk assessment.

• Our study is one of the few investigations about the association of AGA and CAD in women. Regarding the statistically significant correlation between female AGA and CAD, and between AGA and previous history of myocardial infarction, we suggest female androgenetic alopecia as a possible marker for increased risk of CAD events but many questions remain to be answered. Does AGA reflect CAD morbidity and mortality whether associated solely with CAD or metabolic syndrome or obesity? Can AGA be an important predictor of cerebrovascular accident? Is AGA associated with single vessel or multi-vessel CAD? Do patient with AGA respond less well than non-AGA counterparts with similar metabolic profile post-MI? larger studies in both men and women are needed to confirm our findings and to answer these questions.
• The relationship between AGA and CAD in men after more than 30 years of investigation is still a controversial issue; larger studies in both men and women are needed to confirm our findings

References 1. Salvador Arias-Santiago, María Teresa Gutiérrez-Salmerón et al. Sex hormonee binding
globulin and risk of hyperglycemia in patients with androgenetic alopecia J AM ACAD DERMATOL 2010:65: 48–53
2. Serge Ahouansou, Philippe Le Toumelin, Béatrice Crickx et al. Association of androgenetic alopecia and hypertension. European Journal of Dermatology 2007. 17; 3, 220-2.
3. Matilainen VA, Mäkinen PK, Keinänen-Kiukaanniemi SM. Early onset of androgenetic alopecia associated with early severe coronary heart disease: a population-based, case-control study. J Cardiovasc Risk. 2001 Jun;8(3):147-51.
4. Cotton SG, Nixon JM, Carpenter RG, Evans DW. Factors discriminating men with coronary heart disease from healthy controls. Br Heart J. 1972;34:458-464.
5. Hamby RI, Aintablian A, Hoffman I, et al. Is male baldness a coronary risk factor. Clin Res. 1977;25:226A.
6. Lesko SM, Rosenberg L, Shapiro S. A case-control study of baldness in relation to myocardial infarction in men. JAMA. 1993;269:998-1003.
7. Hombly RL, Aintablian A, Hoffman L, et al. Is male baldness a coronary risk factor? Clin Res 1977; 25:226A.
8. Trevisan M, Farinaro E , Krogh V, et al. Baldness and coronary heart disease risk factors. J Clin Epidemiol 1993; 46 (10): 1213-8.