And other Health Care Insights from America’s Greatest Contemporary Songwriter
44
And other Health Care Insights from America’s Greatest Contemporary Songwriter For the Times They Are A’ Changin’ How ACP Is Helping Internists to Start Swimmin’ (so You Don’t Sink Like a Stone) Bob Doherty, SVP, Governmental Affairs and Public Policy American College of Physicians Maryland Chapter, ACP January 31, 2013
description
For the Times They Are A’ Changin’ How ACP Is Helping Internists to Start Swimmin’ (so You Don’t Sink Like a Stone) Bob Doherty, SVP, Governmental Affairs and Public Policy American College of Physicians Maryland Chapter, ACP January 31, 2013. - PowerPoint PPT Presentation
Transcript of And other Health Care Insights from America’s Greatest Contemporary Songwriter
State HPPC Webinar
And other Health Care Insights from Americas Greatest Contemporary Songwriter
For the Times They Are A ChanginHow ACP Is Helping Internists to Start Swimmin(so You Dont Sink Like a Stone)
Bob Doherty, SVP, Governmental Affairs and Public PolicyAmerican College of Physicians Maryland Chapter, ACPJanuary 31, 2013
If your time to you, Is worth savin'Then you better start swimmin'Or you'll sink like a stoneThe times they are a-changinThe Times They Are A-Changin 1963
Swim or sink?Will physicians, medical schools, and hospitals be able to successfully participate in new payment/delivery models?
Swim or sink? Will the ACA . . . Deliver on its promise of providing affordable care to nearly all Americans?Will the marketplaces work as expected?Will premiums be affordable or cost too much?Will the states expand Medicaid?Will there be enough doctors?Or will political opposition, complexity, and misunderstanding cause it to fail?And will physicians help it swim . . . or sink?Payment and Delivery System ReformsThe Medicare SGR and the Future of FFSValue-based paymentsAlternative ModelsMedicare payment reformIn December. bipartisan, bicameral bills reported out of Senate Finance and Ways and Means committeesSimilar bill reported unanimously out of House Energy and Commerce committee in JulyPuts Medicare on the pathway to value-based payments and alternative payment modelsAligning payments with valueInstead of being determined by the SGR and Medicare Economic Index (inflation), physicians could earn more/less above baseline based on Participation in a new budget-neutral Value Based Payment (VBP) incentive programOr participating in an approved Alternative Payment Model (APM)
Bicameral physician payment bill:Out with the old, in with the newOld:Updates determined by SGR (-25% on 1/1/14)Continued cutsNo matter what physicians do
Separate PQRS, Meaningful Use, and Value Index programsWith 2016 penalties
NewBaseline updates set by law*House: 0.5% in CYs 14-16; then 0% until 24Senate: 0.0% in CYs 14-23
New VBP Program: existing PQRS, MU and Value Index consolidated into one program2016 penalties canceled
*With opportunity to earn more or lessBicameral physician payment bill:Out with the old, in with the newOld:Same conversion factor for all physicians, plus/minus penaltiesLimited incentives for PCMHs and other Alternative Payment Models
NewPhysicians determine their own conversion factor, based on VBPs or APMsCertified PCMHs and PCMH specialty practices get higher scores under new VBP program and can bill for chronic care management, and advanced PCMHs get 5% annual bonuses
Value-Based Payment ProgramDateMaximum/minimum VBP updates2017-4% to +4%2018-6% to +6%2019-8% to +8%2020-10% to +10%2021HHS may increase to -/+ 10% but no higher than -/+12%Chronic care managementProposes to pay physicians in certified PCMHs and PCMH-specialty (neighbor) practices a chronic care management fee for most complex patients, beginning in 2015Tracks closely with CMS proposed rule to do the sameHow ACP is helping internists swim . . .Advocacy for better models (PCMH, PCMH-N, ACOs, other)Advocacy for better payFFS (transition of care management, chronic care codes) and in new models Resources to help you make changes in your practice (e.g. Practice Planner, PQRS Wizard)New principles on team-based careAnother Dylan insightHow does it feel, how does it feel, to be without a [medical] home, like a complete unknown, like a Rolling Stone.Like a Rolling Stone, 1965
Prediction: rapid growth in # of PCMH practicesGateway to reimbursement for chronic care management codesGateway to being paid better than the flat baseline updates
ACP Practice AdvisorThe Medical Home Builder was initially launched in 2009 in response to the challenge of disseminating the lessons learned through the grant-funded Center for Practice Innovation program. It was re-named Practice Advisor earlier this year.
15ACP Practice AdvisorAgreement with NCQA to incorporate PCMH 2014 recognition criteriaEvaluating option to directly submit data from Practice Advisor to NCQA for recognitionPCSP 2013 modules launched 12/2013Also built with NCQA permission to use specific criteriaNew: Access to free modules (Mar 2014)New: MOC Part IV optionsThe Center for Practice Support is the home for ACP Practice Advisor the renamed Medical Home Builder. With guidance related to the medical home, a growing slate of clinical quality improvement modules for specific conditions, resources for office operations, Part IV Maintenance of Certification functionality, and a plan for adding a new category with six modules aligned with the NCQA Patient-Centered Specialty Practice recognition program in December of 2013Practice Advisor is poised to become the practice support equivalent of MKSAP. Later in this presentation, I will describe some of the ideas for further development that could make Practice Advisor invaluable for all types of practices, health systems, and training programs.16The ACA (Obamacare) and the Future of American MedicineWhat can you expect over the next six to twelve months? When it is finally fully implemented over the next decade?Obamacare implementation will:Be highly disruptive to insurance markets, employers and providers (as it was supposed to be)Political resistance and headlines on chaos, confusion, and problems will make it especially challenging (critics are rooting for failure)Will be confusing and not go smoothly on day one, but this is nothing new, same was true for Medicare Part D and original Medicare
New York Times, April 23, 1966http://www.washingtonpost.com/blogs/wonkblog/wp/2013/05/17/when-medicare-launched-nobody-had-any-clue-whether-it-would-work/
Source: Sarah Kliff, Washington Post, When Medicare Was Launched, Noboday Had Any Idea It Would Work, May 17, 2013ACA MilestonesDateMilestoneOctober 1, 2013Open enrollment period began to buy coverage from marketplaces
December 24, 2013Last date to sign up to be eligible for tax credits, subsidies on 1/1/14
January 1, 2014Marketplace coverage and tax credits went into effectJanuary 1, 2014Medicaid plans enroll persons with incomes up to 138% of FPL (participating states only)January 1, 2014Consumer protections implemented for all insurance plans (no lifetime limits, no pre-existing condition exclusioms)ACA MilestonesDateMilestoneMarch 31, 2014Open enrollment period closes, except for persons who have life changes that make them eligible to buy coverage later. Persons without qualified coverage in 2014 subject to tax penalty equal to $95 or one percent of taxable income, whichever is greater
January 1, 2015Employers with 50 or more FTEs must provide coverage that meets federal requirements or pay a penalty (delayed by one year from initial 1/1/14 deadline)
Premiums, cost-sharing in the marketplacesAverage of 53 qualified health plan choices in states where HHS will fully or partially run the MarketplacePremiums before tax credits will be more than 16 percent lower than projected. Premiums tend to be lower in states where there is more competition and transparencyAfter taking tax credits into account, fifty-six percent of uninsured Americans may qualify for health coverage in the Marketplace for less than $100 per person per month, including Medicaid and CHIP in states expanding Medicaidhttp://aspe.hhs.gov/health/reports/2013/MarketplacePremiums/ib_marketplace_premiums.cfm
Qualified health plans: cost-sharing levelsPlan% of actuarial cost of required benefitsBronze60-69%Silver70-79%Gold80-89%Platinum90-100%Catastrophic plan for under age 30$6350 deductibleAll plans cover same essential benefits. No cost-sharing for USPSTF screening tests.Maximum out-of-pocket expenses for all plans: $6350 for individuals, $12,700 for family of four . Individuals and families with incomes between 100 percent of the federal poverty line ($23,550 for a family of four) and 250 percent ($58,875 for a family of four) are eligible for cost-sharing reductions (or CSRs) if they are eligible for a premium tax credit and purchase a silver plan through the health insurance marketplace in their state. People with lower incomes receive the most assistance.What about so-called premium shock?Some will pay more (healthy and younger) but many will pay less (older, less healthy)Even those who pay more cant be turned down and will be getting better coverage (lower cost-sharing, better benefits) than usual plans in small and individual insurance marketAffects very small percentage of the population in small group and individual market
Premium shock and joyReinhardt,
Reinhardt, Premium Shock and Joy under the Affordable Care Act, http://economix.blogs.nytimes.com/2013/06/21/premium-shock-and-premium-joy-under-the-affordable-care-act/
Traditionally, the premium in the nongroup market can be expressed as
Pi-premiumquoted to individual
Xi-expected outlaysfor covered healthbenefits for that Individual
L is a loading factoradded to cover thecost of marketing and administration, as well as a target profit margin
100887766472914Medicaid
736455392412Medicaid100
10053464028188Medicaid
10037322820126Medicaid
Source: The Henry J. Kaiser Family Foundation.
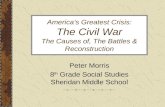
Percentage of premium paid by familyPercentage of premium covered by subsidy*For families of four purchasing coverage in the exchange, not through an employer; numbers reflect standard plan for coverageACA: A Closer LookFamily Health Insurance Premium Obligations Varyby Age, IncomePercentage of Premium Paid by Family of Four vs. Covered by SubsidyPolicyholder Age450%400%350%300%250%200%150%100%2040605030100978573523215MedicaidFamily Income as % of Poverty Level AnalysisA family of four is eligible for Medicaid at 133%, the same percentage below the poverty level as an individualA family of four buying coverage in new state-based health insurance exchanges will be eligible for federal subsidies if their joint income is below 400% of the poverty level; above 400%, families pay full cost26Premium shock and joyLess frequently noted in commentaries about the law certainly among its critics is that the law is likely to bring what I call premium joy to individuals and families with health problems. Many such people simply could not afford the high, medically underwritten premiums they were quoted in the traditional nongroup market. This joy will be shared by high-risk applicants who were refused coverage by the insurer, along with people now in high-risk pools.Uwe Reinhardt, Premium Shock and Joy under the Affordable Care Act, http://economix.blogs.nytimes.com/2013/06/21/premium-shock-and-premium-joy-under-the-affordable-care-act
Obamacare implementation is facing unprecedented political headwindsOrganized political effort to discourage people from signing upFailed effort to defund the law, tied to resolution to fund the government and/or debt ceilingState opposition to expanding Medicaid, setting up exchanges and helping people enrollIn most extreme cases, state opposition is bordering on nullification
Physicians should want Obamacare to swim, not sinkWill provide coverage to tens of millions of uninsured and better consumer protections for everyone elseState resistance to Medicaid expansion will result in 2 out of 3 poor and near-poor going without coverageCoverage associated with better outcomes and fewer preventable deathsIf Obamacare fails, nothing good will replace it
ACA: Resource for Members, ChaptersACA Implementation
Also available:Members can contact staff with issues and questions directly via e-mail.Additional FAQs for our members to help as the exchanges and Medicaid expansion rolls out (e.g., on the premium grace period, network adequacy, etc.)Identification of additional policy development needs related to the ACA rollout (e.g., Medicaid public-private partnerships)ACP AdvocacyFebruary 11 State of the Nations Health Care Report will recommend improvements to:Ensure continuity of care of physicians and hospitals for patients undergoing treatmentEnsure exchange plans meet letter and spirit of network adequacy standardsCreate exceptions/appeals for RXs not on the plans formularyComing Soon: Updated Medicaid Expansion Campaign
26 states + DC are expanding
25 states not expanding
Theres more work to be done!
Another Dylan insightThere must be some way out of here said the joker to the thief, There's too much confusion, I can't get no relief.
All Along the Watchtower, 1967
Too much confusionE-Rx, PQRS, Meaningful use, rewards and penaltiesICD-10Transitional Care Management CodesAnd many more!What do our Members want?Administrative Complexities survey closed on 1/10/2014Included only big M members low response rate (13%), but appears representative of our overall membership (will be supplementing with a panel survey)93% spend 50% or more of their time in direct patient care79% provide all or mostly outpatient care61% in practices of 10 or fewer physiciansWhat do our Members want?
Physician & Practice Timeline
www.acponline.orgMore from Bob DylanYou dont need a weatherman to know which way the wind blowsSubterranean Homesick Blues, 1965
Which way is the wind blowing?Away from pure FFS to new models that put physicians (potentially) in more control in patient-centered systems of care, but with more risk and accountabilityFrom a health system that leaves tens of millions without coverage to one that insures nearly everyone (even if it takes longer than originally planned) with better protections for allAnother Dylan insightHow many times must a man look upBefore he can see the sky?Yes, n how many ears must one man haveBefore he can hear people cry?Yes, n how many deaths will it take till he knowsThat too many people have died?The answer, my friend, is blowin in the windThe answer is blowin in the windBlowin in the Wind, 1963
3Dorn, Uninsured and Dying Because of It: Updating the Institute of Medicine Analysis on the Impact of Uninsurance on Mortality, Urban Institute, 2008Age
U.S.population(millions)
Percent
uninsuredwithin agegroupTotal deaths
Uninsuredexcess deaths
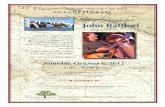
).:2000200120022003200420052006Total:21,00023,00YearNumber of deaths due to uninsurance2000 20,0002001 21,0002002 23,0002003 24,0002004 24,0002005 25,0002006 27,000Total165,000Why is it important to get Obamacare successfully implemented? Because too many people have died.Dorn, Uninsured and Dying Because of It: Updating the Institute of Medicine Analysis on the Impact of Uninsurance on Mortality, Urban Institute, 200843A Final Dylan InsightEverything passesEverything changesJust do what you think you should doTo Ramona, 1964
Chart1010.120.880.240.760.390.610.550.450.640.360.730.2710
Percentage of premium paid by familyPercentage of premium covered by subsidy
Sheet1Percent Above the Poverty LevelPercentage of premium paid by familyPercentage of premium covered by subsidy100%0%100%150%12%88%200%24%76%250%39%61%300%55%45%350%64%36%400%73%27%450%100%0%
Chart1010.080.920.180.820.280.720.40.60.460.540.530.4710
Percentage of premium paid by familyPercentage of premium covered by subsidy
Sheet1Percent Above the Poverty LevelPercentage of premium paid by familyPercentage of premium covered by subsidy100%0%100%150%8%92%200%18%82%250%28%72%300%40%60%350%46%54%400%53%47%450%100%0%
Chart1010.060.940.120.880.20.80.280.720.320.680.370.6310
Percentage of premium paid by familyPercentage of premium covered by subsidy
Sheet1Percent Above the Poverty LevelPercentage of premium paid by familyPercentage of premium covered by subsidy100%0%100%150%6%94%200%12%88%250%20%80%300%28%72%350%32%68%400%37%63%450%100%0%
Chart1010.150.850.320.680.520.480.730.270.850.150.970.0310
Percentage of premium paid by familyPercentage of premium covered by subsidy
Sheet1Percent Above the Poverty LevelPercentage of premium paid by familyPercentage of premium covered by subsidy100%0%100%150%15%85%200%32%68%250%52%48%300%73%27%350%85%15%400%97%3%450%100%0%
Chart1010.140.860.290.710.470.530.660.340.770.230.880.1210
Percentage of premium paid by familyPercentage of premium covered by subsidy
Sheet1Percent Above the Poverty LevelPercentage of premium paid by familyPercentage of premium covered by subsidy100%0%100%150%14%86%200%29%71%250%47%53%300%66%34%350%77%23%400%88%12%450%100%0%