
Anatomy of the Radial Nerve Motor Branches in the...
6
Anatomy of the Radial Nerve Motor Branches in the Forearm Reid A. Abrams, MD, Robert J. Ziets, MD, Richard L. Lieber, PhD, Michael J. Botte, MD, San Diego, CA Knowledge of radial nerve motor branch anatomy is important when performing surgery in its vicinity, neurorrhaphy, and nerve blocks and for understanding the rate and order of recovery of muscle function after injury. Twenty normal fresh cadaver arms were dissected to quantitate radial nerve motor branch anatomy in the forearm. Though variable in individual specimens, innervation order from proximal to distal (based on mean shortest branch lengths) was brachioradialis, extensor carpi radialis Iongus, supinator, extensor carpi radialis brevis, extensor digitorum communis, extensor carpi ulnaris, extensor digiti quinti, abductor policis Iongus, extensor policis Iongus, extensor policis brevis, and extensor indicis proprius. In 10 specimens, branches innervated the brachialis. Mean distances from a point 100 mm proximal to the lateral epicondyle to the muscle measured along the shortest nerve branch ranged from 97.2 mm for the brachioradialis to 299.8 mm for the EIP. The mean number of muscular branches ranged from 1.1 in the EIP to 4.6 in the EDC. Mean nerve length from the radial styloid to the last motor branch was 115.8 mm. (J Hand Surg 1997;22A:232-237.) Understanding radial nerve motor branch anatomy is necessary for performing surgery in its vicinity, undertaking nerve repair, performing motor nerve blocks, forecasting location of a compressive lesion and predicting rate and order of motor recovery. Some data in the English literature shed insight on these issues. 1-8 However, measurements of the motor branch points along the main nerve trunk without measuring the additional distances along the branches to muscle entry points will not accurately predict reinnervation order or rate (though useful for predicting the location of compressive or mass lesions), l Linell addressed the issue of muscle entry points, stating that his measurements were of the From the Hand and Microvascular Surgery Service, Department of Orthopedics, University of California, San Diego, and Veterans Administration Hospital, San Diego, CA. Received for publication April 26, 1996; accepted in revised form Oct. 1, 1996. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Reprint requests: Reid A. Abrams, MD, Department of Orthopedic Surgery, University of California, San Diego, 200 West Arbor Street, Suite 8894, San Diego, CA 92103. 232 TheJournal of Hand Surgery horizontal level at which the nerve entered the mus- cle with respect to the humeral lateral epicondyle and had no bearing on the actual course and length of the nerve and branches. 3 The calculations of Sed- don et al. of reinnervation rate and order are possibly flawed because they are based on Linell's data and similarly collected unpublished data of others. 2,3 Sunderland performed measurements on 10 paired cadavers (20 arms) along the radial nerve and branches to muscle entry points, providing the most useful data to predict innervation order and rate in the human upper extremity,t Radial nerve motor innervation order and its variability is controver- sial. 1,4 The purpose of our study was to delineate radial nerve motor branch anatomy, expanding upon Sunderland's data. Materials and Methods Measurements Twenty fresh cadaver arms (12 right and 8 left), with no history of disease or trauma, were harvested at the midbrachium and dissected under 3.5• loupe magnification. The radial nerve was identified in the interval between the brachioradialis (BR) and
Transcript of Anatomy of the Radial Nerve Motor Branches in the...

Anatomy of the Radial Nerve Motor Branches in the Forearm
Reid A. Abrams, MD, Robert J. Ziets, MD, Richard L. Lieber, PhD, Michael J. Botte, MD, San Diego, CA
Knowledge of radial nerve motor branch anatomy is important when performing surgery in its vicinity, neurorrhaphy, and nerve blocks and for understanding the rate and order of recovery of muscle function after injury. Twenty normal fresh cadaver arms were dissected to quantitate radial nerve motor branch anatomy in the forearm. Though variable in individual specimens, innervation order from proximal to distal (based on mean shortest branch lengths) was brachioradialis, extensor carpi radialis Iongus, supinator, extensor carpi radialis brevis, extensor digitorum communis, extensor carpi ulnaris, extensor digiti quinti, abductor policis Iongus, extensor policis Iongus, extensor policis brevis, and extensor indicis proprius. In 10 specimens, branches innervated the brachialis. Mean distances from a point 100 mm proximal to the lateral epicondyle to the muscle measured along the shortest nerve branch ranged from 97.2 mm for the brachioradialis to 299.8 mm for the EIP. The mean number of muscular branches ranged from 1.1 in the EIP to 4.6 in the EDC. Mean nerve length from the radial styloid to the last motor branch was 115.8 mm. (J Hand Surg 1997;22A:232-237.)
Understanding radial nerve motor branch anatomy is necessary for performing surgery in its vicinity, undertaking nerve repair, performing motor nerve blocks, forecasting location of a compressive lesion and predicting rate and order of motor recovery. Some data in the English literature shed insight on these issues. 1-8 However, measurements of the motor branch points along the main nerve trunk without measuring the additional distances along the branches to muscle entry points will not accurately predict reinnervation order or rate (though useful for predicting the location of compressive or mass lesions), l Linell addressed the issue of muscle entry points, stating that his measurements were of the
From the Hand and Microvascular Surgery Service, Department of Orthopedics, University of California, San Diego, and Veterans Administration Hospital, San Diego, CA.
Received for publication April 26, 1996; accepted in revised form Oct. 1, 1996.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Reprint requests: Reid A. Abrams, MD, Department of Orthopedic Surgery, University of California, San Diego, 200 West Arbor Street, Suite 8894, San Diego, CA 92103.
232 TheJourna l of Hand Surgery
horizontal level at which the nerve entered the mus- cle with respect to the humeral lateral epicondyle and had no bearing on the actual course and length of the nerve and branches. 3 The calculations of Sed- don et al. of reinnervation rate and order are possibly flawed because they are based on Linell's data and similarly collected unpublished data of others. 2,3 Sunderland performed measurements on 10 paired cadavers (20 arms) along the radial nerve and branches to muscle entry points, providing the most useful data to predict innervation order and rate in the human upper extremity, t Radial nerve motor innervation order and its variability is controver- sial. 1,4 The purpose of our study was to delineate radial nerve motor branch anatomy, expanding upon Sunderland's data.
Materials and Methods
Measurements
Twenty fresh cadaver arms (12 right and 8 left), with no history of disease or trauma, were harvested at the midbrachium and dissected under 3.5• loupe magnification. The radial nerve was identified in the interval between the brachioradialis (BR) and
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 233
brachialis, proximal to the innervation of the BR. The nerve and branches were dissected and branch and muscle entry points were measured along the nerve with respect to a bony landmark 100 cm proximal to the lateral humeral epicondyle (LHE). The number of branches entering muscles was counted. The follow- ing measurements were performed: forearm length from the LHE to the radial styloid (RS), the distance from the LHE and the bifurcation of the posterior interosseous nerve (PIN) and the superficial branch of the radial nerve (SBRN), the location of the arcade of Frohse with respect to the LHE, the supinator length from the arcade of Frohse to the distal exit of the PIN, the distance between the RS and the point where the SBRN comes between the extensor carpi radialis longus (ECRL) and BR tendons and becomes subcutaneous, and the PIN length past the distal most motor branch. Measurements were made with an ana- log calipers (No. 505-633, Mitutoyo, Japan; accurate to 0.05 ram) to the nearest 0.1 mm.
Statistical Analysis
Data were pooled among all specimens (n = 20) to calculate mean and standard deviation. The mini- mum and maximum distance to each muscle was entered into a statistical software spreadsheet (Stat- view 4.1, Abacus Concepts, Berkeley, CA) for subse- quent analysis. All data were screened for normality and skew to justify the use of parametric statistics. Means were compared by one-way analysis of vari- ance. Subsequently, pairwise comparisons were done between all means using the Fisher's least squares
differences test, These pairwise comparisons were corrected for the fact that multiple paired compar- isons within a dataset tend to achieve significance given a greater number of comparisons. 9
In addition to analysis of variance, simple cor- relations were generated between the number of branches measured for each specimen and the archi- tectural properties of the selected muscles that were previously reported.10,1~ In all cases, significance was set to a = .05 and statistical power was calculated to be at least 80% (b = .8) in all cases where signifi- cance was greater than 0.05.
Results
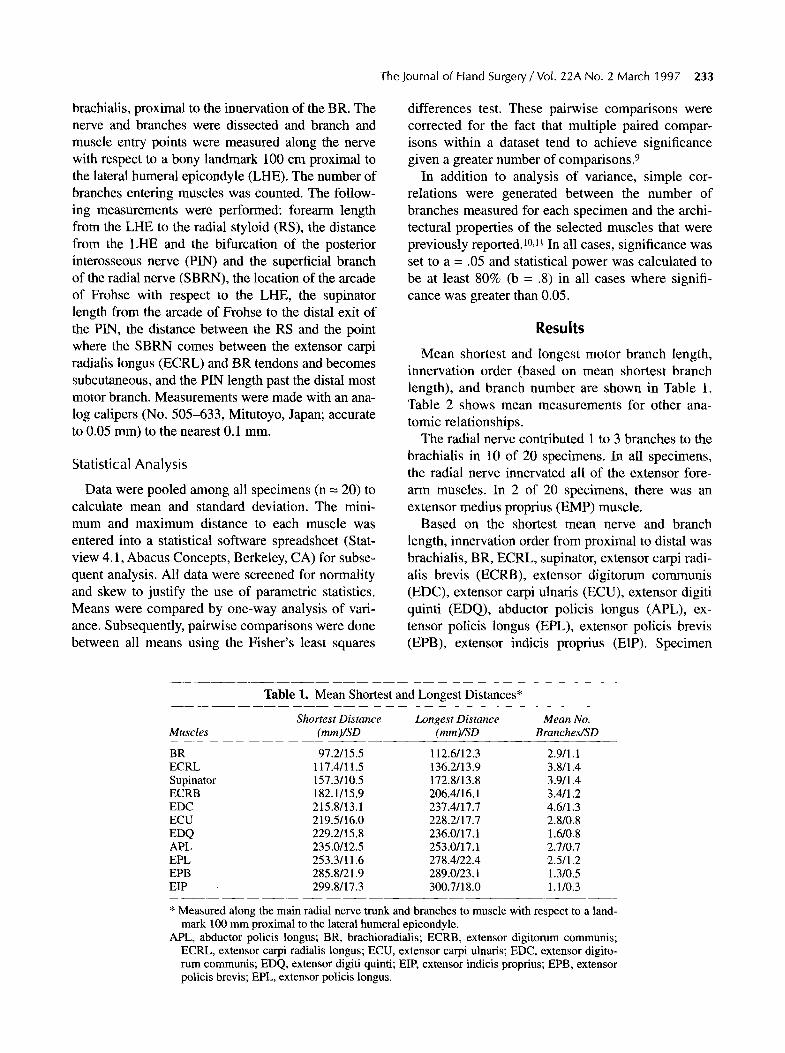
Mean shortest and longest motor branch length, innervation order (based on mean shortest branch length), and branch number are shown in Table 1. Table 2 shows mean measurements for other ana- tomic relationships.
The radial nerve contributed 1 to 3 branches to the brachialis in 10 of 20 specimens. In all specimens, the radial nerve innervated all of the extensor fore- arm muscles. In 2 of 20 specimens, there was an extensor medius proprius (EMP) muscle.
Based on the shortest mean nerve and branch length, innervation order from proximal to distal was brachialis, BR, ECRL, supinator, extensor carpi radi- alis brevis (ECRB), extensor digitorum communis (EDC), extensor carpi ulnaris (ECU), extensor digiti quinti (EDQ), abductor policis longus (APL), ex- tensor policis longus (EPL), extensor policis brevis (EPB), extensor indicis proprius (EIP). Specimen
Table 1. Mean Shortest and Longest Distances*
Shortest Distance Longest Distance Mean No. Muscles (mm )/S D (mm )/S D Branc he s/S D
BR 97.2/15.5 112.6/12.3 2.9/l. 1 ECRL 117.4/11.5 136.2/13.9 3.8/1.4 Supinator 157.3/10.5 172.8/13.8 3.9/1.4 ECRB 182.1/15.9 206.4/16.1 3.4/1.2 EDC 215.8/13.1 237.4/17.7 4.6/1.3 ECU 219.5/16.0 228.2/17.7 2.8/0.8 EDQ 229.2/15.8 236.0/ 17.1 1.6/0.8 APL 235.0/12.5 253.0/17.1 2.7/0.7 EPL 253.3/11.6 278.4/22.4 2.5/1.2 EPB 285.8/21.9 289.0/23.1 1.3/0.5 EIP 299.8/17.3 300.7/18.0 1.1/0.3
* Measured along the main radial nerve trunk and branches to muscle with respect to a land- mark 100 mm proximal to the lateral humeral epicondyle.
APL, abductor policis longus; BR, brachioradialis; ECRB, extensor digitorum communis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor digito- rum communis; EDQ, extensor digiti quinti; EIP, extensor indicis proprius; EPB, extensor policis brevis; EPL, extensor policis longus.

234 Abrams et al. /Anatomy of Radial Nerve Motor Branches
Table 2. Mean Pertinent Distances
Distance Measured Mean Distance (range) in mm
LHE-RS LHE-Frohse Supinator length RS-SBRN RS-final PIN/SBRN branch point
264.7 (230.0-303.9) 51.0 (39.5~57.9) 36.1 (23.9--44.0) 96.4 (72.8-112.9)
115.8 (79.3-154.9) 89.7 (74.1-105.1)
LHE-RS, distance between lateral humeral epicondyle and radial styloid; LHE-Frohse, distance between the lateral epicondyle and the arcade of Frohse; Supinator length, supinator length at level where posterior interosseous nerve (PIN) passes beneath; RS-SBRN, distance between the radial styloid and where the superficial branch of the radial nerve (SBRN) becomes subcu- taneous along the radial forearm; RS-final, distance between radial styloid and the distal most motor branch of the PIN; PIN/SBRN, distance from 100 mm proximal to the lateral epi- condyle along the nerve to the PIN/SBRN branch point.
innervation order was quite variable (Table 3). Mean shortest branch lengths for the EDC and ECU (p = .5), ECU and EDQ (p = .08), and EDQ and APL (p = .3) were not significantly different. In the 10 cases where there were branches to the brachialis, there were 2 where the BR was innervated before the brachialis, in the rest, the brachialis was innervated
first. The only constant consecutive order in all but one of our specimens was ECRL, supinator, ECRB. In one specimen, the distance to the BR was longer than to the ECRL. The EDC and ECU were innervated very close to each other (with mean difference between shortest branches being 3.7 mm) with 12 of 20 specimens having the EDC innervated before the ECU. In 12 of 20, the EDQ was innervated before the APL (with the difference between mean branch lengths being only 5.8 ram). In 17 of 20 specimens, the EPL was innervated before the EPB and EIP, and in the remainder, the EPB preceeded the EPL and EIP. In 15 of 20 specimens, the EIP was the last muscle to be innervated, and in remaining specimens, the EPB was last. In 17 of 20, the EIP and EPB were the last two innervated muscles. When present, the extensor medius proprius was innervated close to the EIP.
Extensor carpi radialis longus branch origin was variable. In 9 of 20 (45%), the branch originated from the PIN. In 6 of 20 (30%), the branch emanated from the radial nerve as 1 branch of a trifurcation (with the other branches being the PIN and SBRN). In 5 of 20 (25%), the ECRB branch came from the SBRN.
Figure 1 demonstrates a typical radial nerve branch pattern in the forearm proximal to the PIN. The typical branch pattem of the PIN is shown in Figures 2 and 3.
Table 3. Proximal-to-Distal Innervation Order for 20 Specimens Based on Actual Nerve and Muscular Branch Lengths
Specimen No. Innervation Order
1 2 3 4 5 6 7 8 9
10
BR, ECRL, SUP, ECRB, EDC, APL, ECU, EPL, EDQ, EPB, EIP BC, BR, ECRL, SUP, ECRB, ECU, EDC, EDQ, APL, EPB, EPL, EIP BR, ECRL, SUP, ECRB, EDC, ECU, EDQ, APL, EPB, EPL, EIP BR, ECRL, SUP, ECRB, ECU, EDC, EDQ, APL, EPL, EPB, EIP BR, ECRL, SUP, ECRB, ECU, EDC, EDQ, APL, EPB, EPL, EIP BR, ECRL, SUP, ECRB, EDC, ECU, APL, EDQ, EPL, EIP, EMP, EPB BR, ECRL, SUP, ECRB, ECU, EDQ, EDC, APL, EPL, EPB, EIP BR, ECRL, SUP, ECRB, ECU, EDC, EDQ, EPL, APL, EIP, EPB BR, ECRL, SUP, ECRB, EDC, ECU, EDQ, APL, EPL, EPB, EIP BC, BR, ECRL, SUP, ECRB, EDC, ECU, EDQ, APL, EPL, EPB, EIP
11 BC, BR, ECRL, SUP, ECRB, ECU, EDC, APL, EDQ, EPL, EPB, EIP 12 BC, ECRL, BR, SUP, ECRB, EDC, ECU, APL, EDQ, EPL, EIP, EPB 13 BC, BR, ECRL, SUP, ECRB, ECU, EDC, APL, EDQ, EPL, EPB, EIP 14 BC, BR, ECRL, SUP, ECRB, ECU, EDC, EDQ, APL, EPL, EPB, EIP 15 BR, BC, ECRL, SUP, ECRB, EDC, EDQ, ECU, APL, EPL, EIP, EPB 16 BC, BR, ECRL, SUP, ECRB, EDC, ECU, EDQ, APL, EPL, EPB, EIP 17 BC, BR, ECRL, SUP, ECRB, EDC, EDQ, ECU, APL, EPL, EPB, EIP 18 BR, BC, ECRL, SUP, ECRB, EDC, ECU, EDQ, APL, EPL, EPB, EMP, EIP 19 BR, ECRL, SUP, ECRB, EDC, ECU, APL, EDQ, EPL, EPB, EIP 20 BR, ECRL, SUP, ECRB, EDC, ECU, APL, EDQ, EPL, EIP, EPB
APL, abductor policis longus; BC, brachialis; BR, brachioradialis; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor dig- itorum communis; EDQ, extensor digiti quinti; EIP, extensor indicis proprius; EMP, extensor medius proprius; EPB, extensor policis brevis; EPL, extensor policis longus; SUP, supinator.

Figure 1. Typical branch pattern of the radial nerve in the forearm proximal to the posterior interosseous nerve (PIN). Proximal is to the fight. Large arrow points to the arcade of Frohse. Nerve branches are encircled by black suture attached to labels. BR, brachioradialis; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radi- alis longus; SBRN, superficial branch of the radial nerve.
Figure 3, Example of branching of the posterior inter- osseous nerve (PIN). Proximal is to the fight. Large white arrow, PIN. Small black arrowheads, branches to the supina- tot (which has been cut to expose the PIN). Medium black arrowheads, branches to the extensor digitorum communis, extensor carpi ulnaris, and extensor digiti quinti. Small white arrow, branches to the extensor policis longus and extensor indicis proprius. Large black arrowhead, branches to the abductor policis longus and extensor policis brevis.
2 ,,4..- - - BR-97,2 f
3.4-.- E C R L - 1 1 7 . 4 ~
4 -49- -- -- ~ S U P - 1 5 7 . 3
5 -4- ECRB-182.1 I f l
6 ~ E D C - ~
tl .-,e- . . . . . . . EP8-285.8 \
A 12 .,4- EIP-299.8 B
Figure 2. Schematic of the typical branch pattern of the posterior interosseous nerve (PIN). Numbers represent distances in millimeters along the nerve and branches from a landmark on the humerus 100 mm proximal to the lateral epicondyle (symbolized by *). (In the 10 specimens where branches to the brachialis [BC] were found, they were distal to the reference point. If we had had more proximal specimens, other BC branches might have been found proximal to the reference point.) The lateral epicondyle is near the branch point of the PIN and superficial branch of the radial nerve (SBRN), but it is not labeled, because it can be proximal or distal to this branch point. Artist's drawing of the extensor forearm with an overlay showing PIN anatomy. APL, abductor pollicis longus; BR, brachioradialis; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor digitorum communis; EDQ, extensor digiti quinti; EIE extensor indicis proprius; EPB, extensor policis brevis; EPL, extensor policis longus; SUE supinator.
235

236 Abrams et al./Anatomy of Radial Nerve Motor Branches
The EDC had significantly more branches than all other radially innervated muscles. Branch number to four groups of muscles was not significantly differ- ent within the groups: (1) ECRB, ECRL, and supina- tor; (2) BR, ECU, APL, and EPL; (3) EDQ, EPB, and EIP; and (4) EDC. Other than for the BR and ECRB (p = 12), all other muscles between groups had significantly different branch numbers. Signifi- cant correlations (p < .0001) were found between branch number and muscle mass and physiologic cross-sectional area (PCSA).I0.11
Discussion This project augments quantitative anatomic data
for the motor branches of the radial nerve. Many authors have studied the radial nerve in the distal brachium and forearm; however, we are aware of no studies measuring distances along the radial nerve and branches to muscle entry points since the work of Sunderland in 1946. ~-Sa2a3 When attempting to forecast order and time to reinnervation following injury and nerve recovery, knowledge of the actual length of the shortest branch to each reinnervated muscle should be the best predictor. 1 We have cor- roborated and supplemented Sunderland's data.
Linell's work in 1921 studied levels of muscle inner- vation for the radial and other nerves. His measure- ments were longitudinal distances along the extremity to muscle entry points with respect to bony landmarks (for the radial nerve in the forearm, he used the LHE as the bony landmark). Linell did not measure the actual length of the nerve and its branches. It was assumed forearm length correlated to innervation distances (which may not be the case), and ratios of innervation distances to forearm length were made. This also assumes average innervation distances are valid, which further assumes that innervation order is fairly constant (with which we and Sunderland disagree). 1
Seddon's discussion of nerve regeneration rate in humans uses Linell's and other unpublished data (using a similar measurement technique as Linell's), and consequently predictions are probably flawed. 2,3 Seddon believed, however, that there may not be consistency of nerve branch points and that a rela- tionship of branch point measurements and limb length is therefore unlikely.2, 3 Seddon addressed variables that confound accurate prediction of rein- nervation rate. He presented evidence showing nerve regeneration was asymptotic rather than truly linear but over moderate durations and distances, recovery rate was relatively constant. 3 Other variables affect- ing regeneration rate were the type of nerve injury (axonotmesis vs neurotmesis) and, in the case of
neurotmesis, length of time to repair. In 12 cases of axonotmesis cited, the regeneration rate ranged from 0.70 to 2.00 mm/d and for neurotmesis and subse- quent suture, the regeneration rate ranged from 0.96 to 2.42 mm/d.
Unlike Sunderland's data, in which 18 of 20 speci- mens had a brachialis innervated by the radial nerve, we found 10 of 20 brachialis muscles radially inner- vated, a We think our data may be faulty because our specimens were distal to the midbrachium. We may have missed more proximal brachial innervation by the radial nerve.
We agree with Sunderland that innervation order is quite variable (Table 3). Our only constant order from proximal to distal was ECRL-supinator-ECRB, cor- roborating Sunderland's data. The EDC was always innervated before the EIP, APL, and EPL, and almost always before EDQ (in 1 of 20 of our specimens and 4 of 20 of Sunderland's specimens, the EDQ was before the EDC). Like Sunderland, all of our specimens had innervation of the EDQ before the EIP and of the APL before the EPB. In all of Sunderland's and 19 of 20 of ours, the APL was innervated before the EPL. In Sun- derland's and our data, mean shortest branch distances to the APL compared to the EDQ, and to the EDC compared to the ECU, were not significantly different. In 13 of 20 of our specimens (and in 7 of 20 of Sun- derland's specimens), the EDQ was innervated before the APL. In 11 of 20 of our and Sunderland's speci- mens, the EDC was innervated before the ECU, and in the rest, the branch lengths were equal or slightly longer in the ECU. Of note is that our mean shortest and longest distances were always longer than Sun- derland's (and Linell's) data. Also, Sunderland's reported muscle branch numbers were usually lower than ours. These discrepancies might possibly be explained if we measured branch lengths further dis- tally than Sunderland might have measured, closer to the motor end plates (where one would expect to find more nerve branching). Despite the variability between specimens, there is little deviation in our "average specimen" innervation order compared to the conclusions of others. 1,3
Many authors have found ECRB branch variation, originating from the radial nerve proper, the SBRN, or the PIN. Differences in the incidence of each variation is found in the literature, with the ECRB branch com- ing from the PIN in 2% and 60%, the SBRN in 16% and 43%, and the radial nerve proper in 24% and 55%. 4,8 Our data showed the ECRB branching from the PIN, SBRN, and radial nerve proper in 45%, 25%, and 30%, respectively. One explanation for discrepan- cies between studies may be inconsistency of dissec-

The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 237
tion and measurement techniques. The ECRB branch is frequently a separate fascicle adherent to the SBRN or PIN. Variation may occur depending on how far proximally the fasicle is dissected before measuring.
The distance along the PIN from the radial styloid proximally to the last motor branch point was mea- sured. This practical information indicates the length of available PIN usable for nerve graft. Our mean length was 11.6 cm (range, 7.9-15.5 cm). This corre- lates with the findings of Waters and Schwortz. 13
Our calculated bifurcation level of the SBRN and PIN was a mean of 10.3 mm above the LHE (range, 25.9 mm above to 5.1 mm below the LHE), which correlates well with the findings of other studies. 4,12,13
Table 1 shows the number of branches the radial nerve gives to each muscle. An interesting question is why there is such variation in branch number. Plausible influences may be differences in muscle architecture (eg, PCSA, fiber length [FL], and mass), the number of joints a muscle crosses, and variations in need for isolated control of different parts of a common muscle belly. Regression analysis demon- strated a positive nonlinear correlation between both muscle mass and branch number and PCSA and branch number (p < .0001).ml By contrast, there was not a significant correlation between FL and branch number. The muscle with the highest branch number was the EDC. Aside from architectural con- siderations, high branch number may be a mecha- nism for regional muscle control unique to the EDC, which has multiple independently functioning ten- don slips originating from a common muscle belly. The number of joints a muscle crosses may also put demands upon a muscle for more isolated regional control and may explain why a larger-mass uniartic- ular muscle such as the BR has fewer branches than the ECRL, which is biarticular.10,u
References 1. Sunderland S. Metrical and non-metrical features of the
muscular branches of the radial nerve. J Comp Neurol 1946;85:93-111.
2. Seddon HJ, Medawar PB, Smith H. Rate of regeneration of peripheral nerves in man. J Physiol 1943;102:191-215.
3. Linell EA. The distribution of nerves in the upper limb, with reference to variabilities and their clinical signifi- cance. J Anat 1921;55:79-112.
4. Fuss FK, Wurzl GH. Radial nerve entrapment at the elbow: surgical anatomy. J Hand Surg 1991;16A:742-747.
5. Rath AM, Perez M, Mainguene C, Masquelet AC, Chevrel JR Anatomic basis of the physiopathology of the epicon- dylalgias: a study of the deep branch of the radial nerve. Surg Radiol Anat 1993;15:15-19.
6. Spinner M. The arcade of Frohse and its relationship to posterior interosseous nerve paralysis. J Bone Joint Surg 1968;50B:809-812.
7. Papadopoulas A, Paraschos A, Pelekis R Anatomical observations on the arcade of Frohse and other structures related to the deep radial nerve: anatomical interpretation of deep radial nerve entrapment neuropathy. Folia Morphol 1989;37:319-327.
8. Prasartritha T, Liupolvanish P, Rojanakit A. A study of the posterior interosseous nerve (PIN) and the radial tunnel in 30 Thai cadavers. J Hand Surg 1993;18A:107-112.
9. Sokal RR, Rohlf FJ. Biometry. San Francisco: WH Free- man, 1981:354-360.
10. Lieber RL, Fazeli BM, Botte MJ. Architecture of selected wrist flexor and extensor muscles. J Hand Surg 1990; 15A:244-250.
11. Lieber RL, Jacobson MD, Fazeli BM, Abrams RA, Botte MJ. Architecture of selected muscles of the arm and fore- arm: anatomy and implications for tendon transfer. J Hand Surg 1992;17A:787-798.
12. Abrams RA, Brown RA, Botte MJ. The superficial branch of the radial nerve: an anatomical study with surgical implications. J Hand Surg 1992;17A:1037-1041.
13. Waters PM, Schwartz JT. Posterior interosseous nerve: an anatomic study of potential grafts. J Hand Surg 1993;18A: 743-745.


















