ANATOMY OF LARYNX - rameshhospitals.com · ANATOMY OF LARYNX. FUNCTIONS •Breathing •Sound...
66
MODERATOR:DR.K SAILAJA PRESENTOR:DR.M.MOUNIKA ANATOMY OF LARYNX
Transcript of ANATOMY OF LARYNX - rameshhospitals.com · ANATOMY OF LARYNX. FUNCTIONS •Breathing •Sound...

MODERATOR:DR.K SAILAJAPRESENTOR:DR.M.MOUNIKA
ANATOMY OF LARYNX


FUNCTIONS
• Breathing
• Sound Production
• Manipulation of Pitch and Volume
• Protecting Lungs against Food aspiration

SURFACE ANATOMY• A framework of articulating
cartilages linked together by ligaments and laryngeal muscles.
• Lies opposite 3rd – 6th Cervical vertebrae.
• It’s easily palpable, covered superficially by the Deep fascia in the midline and by thin strap muscles laterally.

SKELETAL ANATOMY• LARANGYAL FRAMEWORK;
• Cartilages• Ligaments and membranes• Muscles• Joints• Hyoid bone

CARTILAGES OF LARYNX• 3 Unpaired✔ Thyroid✔ Cricoid✔ epiglottis • 3 paired✔ Arytenoid✔ Corniculate✔ cuneiform

THYROID CARTILGE• located anterior to the 4th and
5th cervical vertebrae. • formed by 2 laminae which fuse
ventrally in the midline of the neck, forming a protuberance, the laryngeal prominence or "Adam's apple,“
• The 2 laminae meet at an angle of 90° in the male and 120° in the female.
• The upper limit of fusion of the two laminae forms the superior thyroid notch

THYROID CARTILAGE

THYROID CARTILAGE• 5 ligaments attach as
one to the posterior surfaces of the thyroid laminae near the union of the laminae (angle):
✔ The median thyroepiglottic ligament,
✔ The 2 vestibular ligaments, and
✔ The 2 vocal ligaments

CRICOID CARTILAGE❑ Shaped like a signet ring.❑ signet-shaped portion of the
cricoid faces posteriorly❑ the arch is located
anteriorly,❑ The cricoid cartilage is
situated at vertebral level C6 (occasionally reaching the middle of C6), just below the thyroid cartilage

CRICOID CARTILAGE✔ 2 superior facets– articulate with
the arytenoid cartilages and attach to them by the posterior cricoarytenoid ligaments
✔ 2 lower lateral facets of the lamina articulate with the inferior horns of the thyroid cartilage.
• The lower border of the cricoid cartilage is joined to the first tracheal ring by means of the thick cricotracheal ligament.

CRICOID CARTILAGE• Important from structural
& functional point of view– Base for entire larynx– Support to arytenoid– Attachment to intrinsic
muscles– Only part of
cartilagenous framework that forms the complete ring

EPIGLOTTIS• Oblong leaf shaped• Located behind the root of
the tongue and the body of the hyoid bone and in front of the laryngeal entrance (laryngeal aditus or vestibule).
• It has:✔ 2 ends— upper & Lower✔ 2 surfaces— Anterior &
Posterior✔ 2 Lateral borders❖ Upper end:broad

EPIGLOTTIS❖ lower end: narrow –“ petiolus / stalk ”
attaches to inner surface of thyroid cartilage below thyroid notch by the thyroepiglottic ligament
❖ It attaches to the posterior body of the hyoid bone via the hyoepiglottic ligament
❖ it lies dorsal to the thyroid cartilage and thyrohyoid membrane, guarding the laryngeal entrance.

EPIGLOTTIS.The epiglottis is attached to the thyroid
cartilage by the thyroepiglottic ligament.• The aryepiglottic folds and the
quadrangular membranes attach to the lower part of the lateral margins of the epiglottis.

ARYTENOID CARTILGE• Almost pyramidal in shape,• with ❖ 3 surfaces,❖ a base, and❖ an apex.• Each triangle-shaped base articulates
with the cricoid cartilage by way of a diarthrodial joint.
• Base has 2 processes:✔ Anteromedially directed vocal process
– vocal ligament is attached✔ Short, broad, laterally projecting
Muscular process – lateral and posterior cricoarytenoid muscles are attached

ARYTENOID CARTILAGE• Arytenoid has 3 surfaces
1. Posterior surface —Transverse and oblique arytenoid muscles attach
2. Medial surface – covered with mucous-secreting laryngeal mucosa.
3. Anterolateral surface –insertion of
✔ thyroarytenoid muscle,✔ part of the vocalis muscle,and✔ the vestibular ligament.

CORNICULATE CARTILAGES (SANTORINI)
• small fibroelastic nodules that sit on the apices of the arytenoid cartilages.
• It has little functional importance in humans
• CUNEIFORM CARTILAGES (OF WRISBERG)
❑ rod-shaped (like ancient cuneiform script).
❑ situated in the aryepiglottic folds anterior to the corniculate cartilages,❑ may be entirely absent.

LIGAMENTS&MEMBRANESMembranes — Extrinsic – Thyrohyoid membrane Crico tracheal membrane
Intrinsic — Quadrangular membrane
Conus elasticus • Ligaments & Folds ❑ Epiglottic ligaments❑ Aryepiglottic fold ❑ Vestibular ligament (vestibular folds or false vocal
cords)❑ Vocal ligaments

EXTRINSIC MEMBRNES

CONUS ELASTICUS• Conus Elasticus connects the
cricoid cartilage with the thyroid and arytenoid cartilages.
• composed of dense fibroconnective tissue with abundant elastic fibers.
• Having 2 parts 1 .Medial cricothyroid ligament —connects the anterior part of the arch of the cricoid cartilage with the inferior border of the thyroid membrane.

CONUS ELASTICUS 2. Lateral cricothyroid membranes originate on the superior surface of the cricoid arch and rise superiorly and medially to insert on the vocal process of the arytenoid cartilages posteriorly, and to the interior median part of the thyroid cartilage anteriorly.• Its free borders form the
VOCAL LIGAMENTS

QUDRANGULAR MEMBRANE• Extends from the sides of
the epiglottic cartilage anteriorly to the anterolateral surface of the arytenoid cartilage and posteroinferiorly to the corniculate cartilage.
• With its covering of mucous membrane forms the aryepiglottic fold superiorly and vestibular ligament inferiorly.
• it forms the medial wall of the piriform recess

QUADRANGULAR MEMBRAANE• The paired Quadrangular Membranes
connect the epiglottis with the arytenoid and thyroid cartilages.
• Course posteriorly downward and attach to the corniculate cartilages and the lateral surfaces of the arytenoids.
• The cuneiform cartilages are embedded within the aryepiglottic folds.
• The free inferior borders of the quadrangular membranes form the ventricular ligaments, also known as the false vocal folds.

LARYNGEAL SPACES• Internal laryngeal spaces :✔ vestibule,✔ ventricles, o subglottic or infraglottic spaceso External laryngeal spaces ✔ Paraglottic space✔ pre-epiglottic. Space

INTERNAL LARYNGEAL SPCES

EXTERNAL LARYNGEAL

LARYNGEAL MUSCLES
• Extrinsic muscles — which move the entire larynx,
• Intrinsic muscles — which move the vocal cords.

• ELEVATORS OF THE LARYNX• The Suprahyoid Muscles
▪ Digastric▪ Stylohyoid▪ Mylohyoid▪ Geniohyoid
• The Longitudinal Muscles of the Pharynx▪ Stylopharyngeus▪ Salpingopharyngeus▪ Palatopharyngeus
DEPRESSORS OF THE LARYNX:
• The Infrahyoid Muscles▪ Sternohyoid▪ Sternothyroid▪ Omohyoid

INFRAHYOID GROUP

SUPRAHYOID GROUP



MUSCLES OF LARYNGEAL INLET

MUSCLES OPEN &CLOSE GLOTTIS

MUSCLES CONTROLLING TENSION OF CORDS

BLOOD SUPPLY• ARTERIAL SUPPLY• Upper Larynx• External carotid artery • Superior thyroid artery• Superior laryngeal artery
• Lower Larynx• Subclavian artery• Thyrocervical artery• Inferior thyroid artery• Inferior laryngeal artery

VENOUS DRAINGE• Upper Larynx• Superior laryngeal vein• Superior thyroid vein• Internal jugular vein
• Lower Larynx• Inferior laryngeal vein• Inferior thyroid vein• subclavian vein

LYMPHATIC DRAINGE• SUPRA GLOTTIC AREA superior lymphatics drain to the upper deep cervical nodes, located at the level of the carotid bifurcation.• Some drainage passes to
prelaryngeal nodes.• INFRA GLOTTIC AREA drain to the pretracheal lymph nodes of the proximal trachea anteriorly paratracheal nodes laterally and then to the deep cervical and superior mediastinal nodes.

NERVE SUPPLY

SUPERIOR LARYNGEAL NERVE
• Sup. Laryngeal N- • Inf ganglion vagus & superior
cervical sympathetic. Descend behind ICA
• At greater horn- Divide small external & larger internal branch
• External branch – • Motor to Cricothyroid

SUPERIOR LARYNGEAL NERVE• INTERNAL BRANCH • Pierce thyrohyoid membrane.• Divide-Two sensory & secretomotor• Upper-
pharynx,epiglottis,valeculla,vestibule • Lower- Aryepiglottic fold, mucous
membrane up to vocal cords• Internal branch- caries Afferent
fibers from neuromuscular & stretch receptor
• Sup. Laryngeal nerve end by anastomoses with RLN (Galens anastomoses)

RECURRENT LARYNGEAL NERVE• Rt RLN leaves vagus
loops Rt Subclavian A• Ascends in
tracheo-eosophageal groove to reached larynx.
• Lt RNL-Passes under aortic arch and Ligamentum arteriosum to reach tracheoesophageal groove.

RECURRENT LARYNGEAL NERVE
• Pass upwards with Laryngeal branch of Inferior Thyroid Artery.
• Deep to lower border of inferior constrictor muscle
• Enters larynx behind Cricothyroid joint
• Divide: Motor & sensory• Motor- All intrinsic muscle except
Cricothyroid ( Ext branch SLN)• Sensory-Laryngeal mucosa below
vocal folds

INFANT LARYNX• Positioned high in the neck- this allows the
epiglottis to meet soft palate and makes nasopharyngeal channel for nasal breathing during sucking.
• Laryngeal cartilage are softer ,easily displaced, easily irritable
• Epoigloittis- longer, narrower, tubular; hence mentioned as omega shaped.
• Thyroid cartilage is flat, cricoid cartilage is smaller then size of glottis making subglottis the narrowest part.

INFANT LARYNX• Aryepiglottic folds are
disproportionately large.• Arytenoids are more prominent• Mucous membrane and connective tissue
are loosely attached and easily undergo oedematous changes.

DIFFERENCE BETWEEN ADULT&INFANT

INFANT LARYNX

INFANT LARYNX

INFANT LARYNX

DIFERENCE BETWEEN ADULT&INFANT

Laryngoscopic Anatomy

Laryngoscopic Anatomy
Modified Cormack and Lehane grading system.
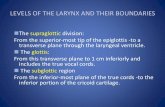
Grade 1 – Full view of glottis.
Grade 2a – Partial view of glottis.
Grade 2b – Only Posterior part of glottis is visible or only arytenoid is visible.
Grade 3 – Only Epiglottis is visible.
Grade 4 – Epiglottis not visible.

CORD PALSIES• Description of normal and abnormal
movements of cord is done with help of direct laryngosocpe
• Intubation & extubation should done at end of deep inspiration.

NORMAL MOVEMENTS OF CORDS


Cord Palsies• 1.Unilateral Pure Abductor Palsy• a)On Phonation: Cords meet in midline because
adductor fibers on damaged side are still active
• b)On Inspiration: Injured side cord remains in same position
• Normal side cord moves into full abduction

2)Unilateral abductor and adductor palsy: Damaged cord lies slightly in abduction
a)On Phonation:• Normal side cord crosses the midline in an
attempt to meet its opposite cord

b)On Inspiration:• Normal side cord moves into full
abduction

3)BiLateral damage to Recurrent Laryngeal.N a)Mild trauma on both sides• Bilateral Abductor Paralysis• Adductor fibres are still functioning• So vocal cords lie near midline• Airway is greatly reduced • Patient shows severe respiratory obstruction

b)Severe trauma on both sides:• Loss of both abductors and adductors• Both vocal cords lie in midposition• Fair sized lumen between them• Airway is fairly adequate with
Marked Respiratory effort• Cords sucked in with each inspiration

4)Bilateral Palsy of recurrent laryngeal.N with
palsy of external branch of superior laryngeal.N
• Paralysis of crico thyroid muscles leads to loss
of tension of the cords and reduced
antero-posterior diameter of glottis

Superior Laryngeal Nerve Block
Tracheal Injection
Pharyngeal Gargle

SUPERIOR LARYNGEAL N BLOCK• Locate the hyoid bone
• 1cm below each greater cornu (where the
internal branch of the superior laryngeal
nerve penetrates the thyrohyoid
membrane)
• Infiltrate 3ml 2% lignocaine
• Feel a ‘pop’ as the needle penetrates the
membrane

TRANSTRACHEAL BLOCK
• Extend the neck.
• Identify the cricothyroid membrane.• Inject 4ml 4% lignocaine at the end of
inspiration.• A resultant cough will distribute the
anaesthetic.
•••
•

THANK YOU