Anatomie et biomécanique du LCA: natif - sofarthro.com LCA.pdf · Anatomie et biomécanique du...
53
Anatomie et biomécanique du LCA : natif Hulet Ch, et la SFA Département d’Orthopédie, CHU de Caen Unité INSERM COMETE DIU ARTHROSCOPIE 2018 VERSAILLES
Transcript of Anatomie et biomécanique du LCA: natif - sofarthro.com LCA.pdf · Anatomie et biomécanique du...

AnatomieetbiomécaniqueduLCA :natifHuletCh,etlaSFA
Département d’Orthopédie, CHUdeCaenUnitéINSERMCOMETE
DIUARTHROSCOPIE2018VERSAILLES

LésionduPivotcentral
Labiomécanique:Système4barres(PChambat) 30°0° 90°
LCA
LCPLCPLCA
GenoudroitGenoudroit
Introduction

J M Rogez, CD Esska anatomyH.K.Uhthoff Ottawa Ontario CanadaThe Embryology of the Human Locomotor System,Springer-Verlag
Almost 7 monthsof gestation
6weeks ofgestationEmbryo 6 mmlongBourgeonsdesmembres
Ontogénie Méniscale

Lateral compartmentVascularisation of the meniscus
J M Rogez, CD Esska anatomyH.K.Uhthoff Ottawa Ontario CanadaThe Embryology of the Human Locomotor System, Springer-Verlag
Fetus 135 mm : 16 weeks

LCA : Anatomie fonctionnelle avec 2 faisceauxCylindre ou ruban
Anatomie revisitée 2010-2017
Pineau V, C Hulet, D Belot, B Lebel, B Geffard, B Galaud, G Burdin, E Salamé. Proprioception du LCAModifications de la vascularisation méniscale pendant la vie intra-utérine. SFA 07, ESSKA 08, SOFCOT 08, Isakos 09.
16 menisci et 14LCA
24 to 35 weeks old
Meniscusvascularization
Hulet
Hulet
Fœtus4monthsFoetus 7 months

MLMM
Pineau V, C Hulet, D Belot, B Lebel, B Geffard, B Galaud, G Burdin, E Salamé. Modifications de la vascularisation méniscale pendant la vie intra-utérine. SFA 07, ESSKA 08, SOFCOT 08, Isakos 09.
F
T
HES
LCA : Anatomie fonctionnelle avec 2 faisceauxCylindre ou ruban
Anatomie revisitée
• Rich vasculariszationML=MM

Anatomie revisitéeWebster 1870Rouviere 1932

Anatomie revisitée
Largeur : 7– 12mmLongueur :22– 41mmMoyenne:32mm
L’Arthroscopie Menetrey DuthonAmis AA, Dawkins GP.Functional anatomy of the ACL: Fiber bundle actions related to ligament replacements and injuries. JBJS Br 1991;73:260–267
PL17.8mm

Courtesy of J.Menetrey,Genève(ESSKADVDanatomie dugenou)
PostérolateralLooseinflexion
AntéromedialTightinflexion
PL
Am
LCA:Anatomiefonctionnelleavec2faisceauxCylindreouruban
Anatomie revisitée2010-2017
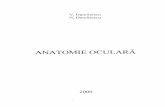
Orientation- conventionsSupérieur / roof (antérieur)
Inférieur / flor (postérieur)
Superficiel / shallow(distal)
Profond / deep(proximal)
Arthroscopie Nomenclature
anatomique

Nouvelleapprochedel’anatomie« Ribbonlike ACL »
• TravauxanatomiquesdeSmigielski etcoll.
• Sieboldetcoll.• Noailles(2014)
• LCAproched’un« ruban »
• Latorsiondurubandonnel’effetdefaisceaux:unrubanestuncylindre« écrasé »
Twist:« bundleeffect »« Ribbon aspect »

Le RUBAN de R. SmigielskySmigielski,R.,etal.,Theanatomyoftheanteriorcruciateligamentanditsrelevancetothetechniqueofreconstruction.BoneJointJ,2016.98-B(8):p.1020-6.
Siebold,R.,etal.,Flatmidsubstance oftheanteriorcruciateligamentwithtibial"C"-shapedinsertionsite. KneeSurgSportsTraumatol Arthrosc,2015.23(11):p.3136-42.

Courtesy Dr.Noailles
Courtesy Dr.Smigielski
ifthecylinderisflattened, itsbecomesaribbon?
Smigielski
Noailles,Boisrenoult


The Ribbon Concept Robert Smigielsky Warsaw PolandJackson Hole ACLSG wy usa 2012Il décrit des
Fibres Antero Médiale et Fibres Postero LatéralesFibres directes et fibres indirectes
Fibresindirectes
Fibresdirectes
CourtesyRSmigielsky

• Dans le prolongement du cortex fémoral postérieur

Insertionfémorale
•Surfacesemicirculaire
•Faceaxialeducondyleexterne
•Enarrièredelacorticalepost
Vuespostérieures

AM
PL« Lateral
Intercondylarridge »
« Lateralbifurcateridge »
Fémur: Inscritedanslaconcavitédupourtourcartilagineux.Limitéenavantpar« thelateralintercondylar ridge ».Faisceauxséparéspar« thelateralbifurcateridge ».
T Mochizuki 2006, A Ferretti 2007 – 2008, F Giron 2007, W Petersen 2007,R Siebold 2008, A Edward 2008.
AnatomieinsertionfémoraleduLCA

Medial meniscus
Lateralmeniscus
RapportaveclacorneAnt duME
3typesd’insertion

• Tibia ++++KissfromtheAcltotheLM
Plus antérieure que l’on croit, Forme de « C »
ML

Insertion tibiale
Surface pré spinale (18 sur 11mm)En arrière du toit en extensionContinuité avec la glène interneGouttière condylienne en extensionÉlargissement distal de l’échancrure
11mm
18mm
Vuesantérieures

Anatomieduligament croisé antérieur
PL
PL
En extension:AM et PL sont presque parallèlesPL : tenduAM : moderément détendu
En flexion : AM : tenduPL : détendu

AM tendu
PL tendu
Extension
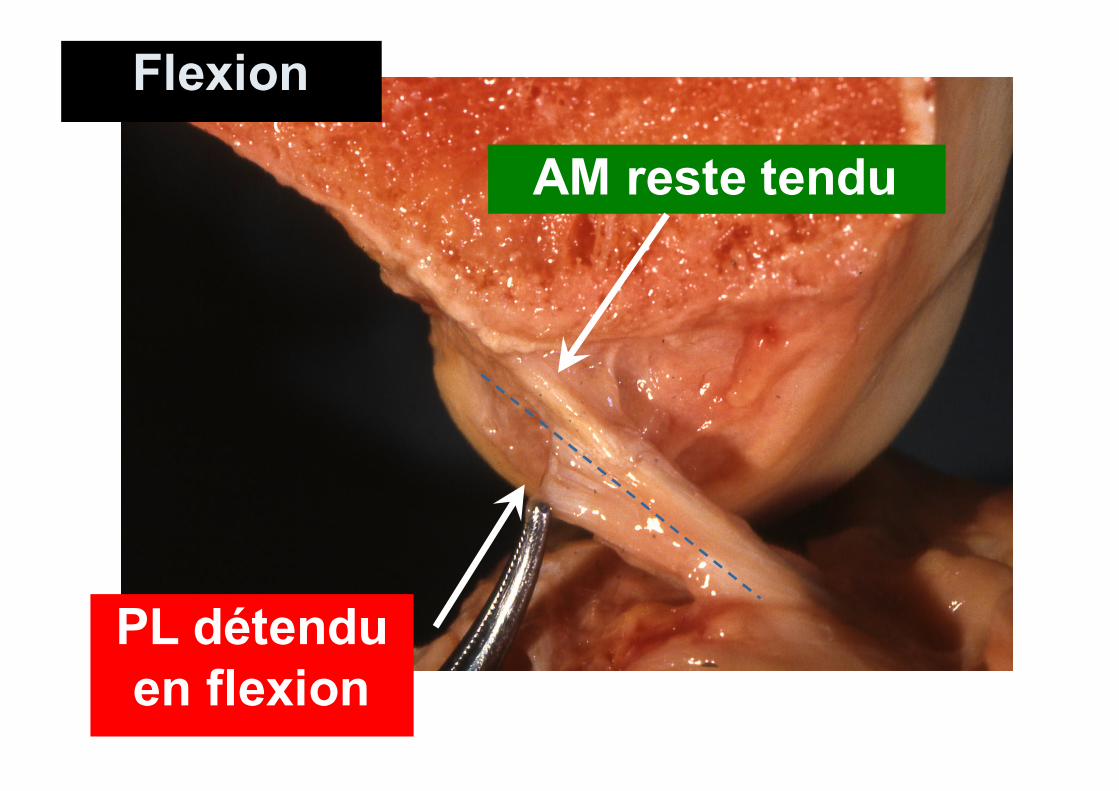
AM reste tendu
PL détenduen flexion
Flexion

Anatomieduligament croisé antérieur
AnalyseIRM(3T)
SteckelH,KSSTA2006&2007
AM
PL
AM
Coupes paracoronales obliques
PL
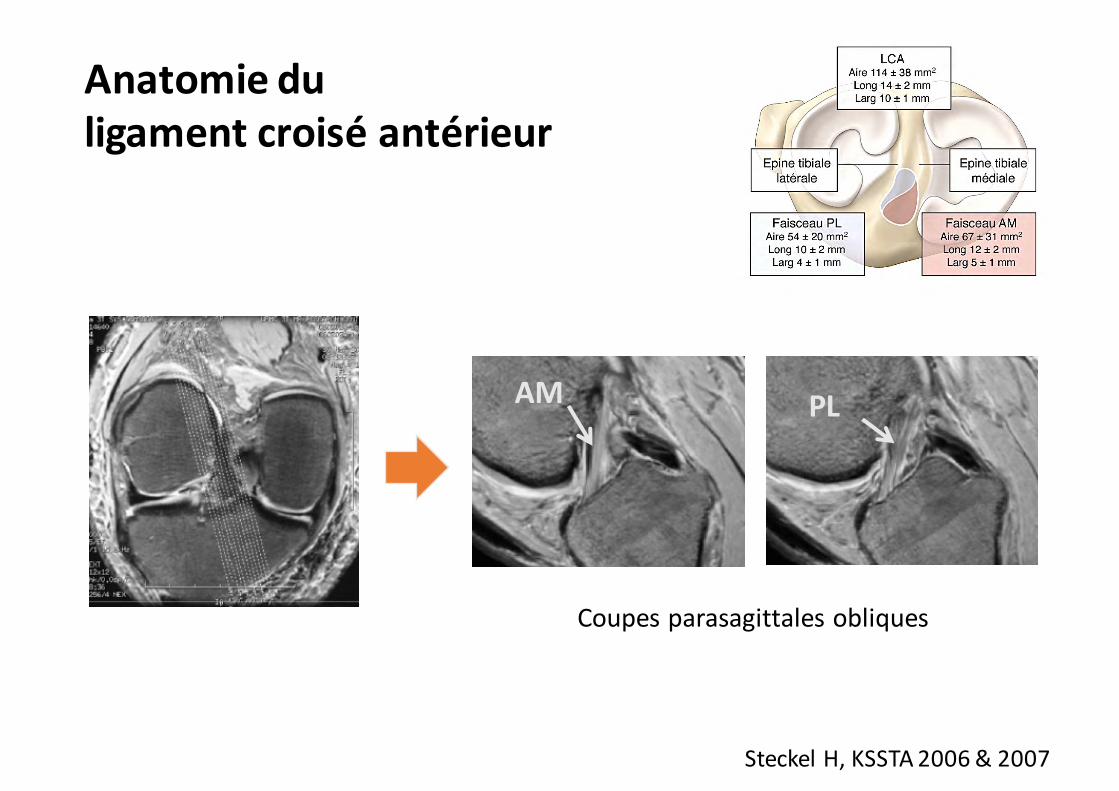
Anatomieduligament croisé antérieur
SteckelH,KSSTA2006&2007
AM PL
Coupes parasagittalesobliques
AnalyseIRM(3T)

• 1 Contrôle de la translation tibiale antérieure (Lachman-Trillat)
Buts principaux
ESSKA2000
LCA
• 3Déterminationdel’axederotationdugenou
• 2Synchronisationducondylelatéral/tibia(Jerk-test)
LELCA

Le faisceau AM tend àmaintenir une longueur(tension) constante lorsde la flexion
Le faisceau PL se détend en flexion
Le faisceau PL se tend rapidement en extension
Amis & Dawkins,JBJS 73 Br: 260-7, 1991
AM
PL
Variationdelongueurdesdeuxfaisceaux

(Amis & Dawkins, JBJS 73 Br: 260-7, 1991)
Le faisceau PL est celui quirésiste le plus à la translation tibiale antérieure près de l’extension
Le faisceau AM devient le frein pricipal quand le genou est fléchi
Cela reflète le mode de variation de longeur des faisceaux
Contribution des faisceaux du LCA à la résistance au tiroir antérieur
PLB AMB

Orientation de la chargedans chaque faisceau pour un tiroir de 110 N
0
20
40
60
0° 15° 30° 60° 90°AM PL
-5
0
5
10
0° 15° 30° 60° 90°
AM PL
β
α
α
β
°
°
Le faisceau PL est le plus chargé entre 0° et 45° de flexionA 90° de flexion il supporte encore 35 % de la charge

15°110 N
•Il contrôle uniquement latranslation tibiale antérieure•Il ne peut pas contrôler la laxité rotatoire car, il se confond avec le centrede rotation du genou
Conséquences
•A 15 ° de flexion le faisceau AM est chargé de Manière quasi sagittale

15°110 N
•Il contrôle la translation
tibiale antérieure etla rotation interne
Conséquences
•A 15 ° de flexion le faisceau PL est chargé de manière oblique (6°)
=Problèmetridimensionnel3D

0 à 30°: 1er frein: LCA
Après 30°:1er frein: LCA
1.LCA
2ème frein: Sgt post du MM 2.MM
3ème frein: Pente tibiale
3.PenteTibiale
Burdin

• In vitro, Levy (JBJS, 1982)
0
5
10
15
20
25
0° 30° 60° 90°
4,85,45,94,3
NORMAL
13,616,617,4
11,4 LCA
21,8 22,319,7
10,4
LCA + MM
14,718 17
14LCA + ML
AP D
ispl
acem
ent(
mm
)At
100
new
ton
forc
e

Neyret (SFA 99)
In vivo, subluxation active en AMP
Mesure différentielle en RX
Genounormal:3,4+ 2,9mm
LCAisolé:5,6+ 5,8mm
LCA+mén.méd.:7,2+ 4,4mm

Logan,…&FreemanAJSM2004
•Invivo,•IRMdynamique,3D
1.Translationtibialeantérieure
Normal
LCArompuGreffeLCA
Compartimentmédialetlatéral

1.Translationtibialeantérieure
Logan,…&FreemanAJSM2004
Normal
49
022
49
2322
0mm
Médial Latéral
•Invivo,Genounormal•PlusgrandemobilitéduComp.Lat.

LCArompu
1.Translationtibialeantérieure
Logan,…&FreemanAJSM2004
49
017
49
2322
0mm
Médial Latéral
- 8,2
- 14,1
•Invivo,LachmansurLCArompu•Reculdes2condylesetdéplacementCL>CM•SubluxationpostduCLetrotationint.tibialede20°

S’opposeàlatranslationtib ant enampVulnérabilitéFréquencedeslésions
Lerat
MMML
RôledeCale
Burdin

ACLIntact
100%
47%16% 12% 8%
MEDIALMENISCECTOMY SAVETHEMENISCUS
ArthroseLCA/MENISCUS
MM- /ACLtearNeyretRCO88
MM- /ACLreconstructionSofcot201410-20ans
MM- /ACLIntactHuletJBJS2005
MMIntactACLRLebelAmjsm08
MeniscusIntactACLRSofcot201410-20ans
17%
MENISCECTOMYCONSEQUENCES ON ACLSURGERY
ACL
tear ACL
Reconstruction
ACLReconstruction
MMSuture/ACLReconstructionHuletACLSG
OAprevalencewithreferencetopopulation,whereageisgreaterthan45yrsOld,Between5%(Peterson1997)to13.8%(Turkiewicz 2014)

°
Relationdirectepentetibialepost.ettranslationtib.ant.
SiPTde5° LaTTAaugmentede3mm
SiPTde10° LaTTAaugmentede6mm
Bonnin M, Carret JP, Dimnet J, Dejour H.JBJS 93.

Silapentetibialeaugmente :
AgneskirchnerJD,HurschlerC,Stukenborg-ColsmanC,ImhoffAB,LobenhofferP.ArchOrthopTraumaSurg2004;124:575-84.
1.AugmenteTTA(7,2mmà30° flexion)
3.AugmentationcontraintesFT700Nenext.(100Nnormalt)
4.Déplacement pointcontactFTd’arrièreenavant(passede61,4%APà25,4%)
Burdin
2.Elévationantérieurede4,1mmenext.

Déplacementde20°
Hyper-rotationinterne
Contraintesmédiales++++

Ressaut(JerkTest)Sensationd’instabilitéDéplacementdeplusde15mm
ALRMLyon
Disparitioncalepostéro-médiale
Usurepostéromédialeducartilage Défoenvarusetdistensiondesformationpostérolatérales
Burdin
TriplevarusdeNoyesContraintesmédiales+++

n BulletAmis1998TheKnee
Ontmontréquelepivotshiftestunmouvementcomplexe3Dautourd’unaxehélicoïdal
=Problèmetridimensionnel3D
L’instabilitédugenou

• Le ligament croisé antérieur est:le FREIN PRINCIPAL (Primary Restraint):
Ø de la TRANSLATION tibiale antérieureØ de la ROTATION tibiale Interne
• La rupture du LCA est responsabled’une instabilité ROTATOIRE
Reculdes2condyles(CL>CM)SubluxationpostduCLetrotationint.tibialede
20°
RôleduLCA

L’instabilitédugenou
RessautCourtoisieRSeilL’arthroscopie
CourtoisiePColombet

Capo2016 Caterine 2015 Claes2013 Daggett 2016 Dodds2014
Helito 2013 Kennedy2015 Kittl 2016 Kosy 2016 Parsons2015
Rezansoff 2014 Roessler 2016 Ruyz 2016 Saiegh 2015
Schon 2016 Spencer2015 Stijak 2014 Thein 2016 Vincent2011 Zens2015
Lutz2015
Krackow 1983:93
Krackow 1983:93
StructuresannexesdanslabiomécaniqueduGENOULCA,structureslatérales……………LALAKAPLANetc

StructuresannexesdanslabiomécaniqueduGENOULCA,structuresméniscales……

Double reincontrol