Anatomical landmark
48
PRESENTED BY : DR.NISCHAL NIRAULA KUSMS ANATOMICAL LANDMARKS
-
Upload
nischal-chhetri -
Category
Health & Medicine
-
view
116 -
download
2
Transcript of Anatomical landmark

PRESENTED BY :
DR.NISCHAL NIRAULA
KUSMS
ANATOMICAL LANDMARKS

Maxillary and Mandibular landmarks
1.Limiting structures 2. Supporting Structures
Primary stress Secondary stress 3. Relief
bearing areas bearing areas areas


Limiting structures are sites that will guide us in having an optimum extension of denture so as to engage maximum surface area without encroaching upon the muscle action. They are:
Labial frenum
Labial vestibule
Buccal frenum
Buccal vestibule
Hamular notch
Posterior palatal seal
Fovea palatinae
Limiting structures

Labial frenum
a) Single or double fibrous band covered by mucous membrane which extends from labial aspect of residual alveolar ridge to the lip.
b) Absence of muscle fibers.
CLINICAL SIGNIFICANCE
a) Limits labial flange of denture.
b) Relief if not given causes pain and also dislodgement of denture.

Labial vestibule
Boundaries:a) Extent---from buccal frenum on one side to the other,being divided
into right and left by labial frenum.
b) Anteriorly:orbicularis oris muscle
c) Posteriorly:labial aspect of alveolar ridge.
FEATURES
a) Thin mucosa and thick submucosa with large amount of loose areolar tissue and elastic fibers.
CLINICAL SIGNIFICANCE
The labial flange of the denture will be in complete contact with labial vestibule to provide a peripheral seal in the denture.

Buccal frenum
Band of fibrous tissue overlying the levator anguli oris,that divides labial vestibule from buccal vestibule.
The orbicularis oris pulls frenum forward and the buccinator pulls it backward
CLINICAL SIGNIFICANCE
Since it has muscular attachments adequate relief must be provided to
prevent the dislodgment of denture.(that is,it can move posteriorly as a
result of the buccinator muscle and anteriorly as a result of the orbicularis oris.)

Buccal vestibule
Buccal vestibule extends from the buccal frenum to the hamular notch.
Bounded externally by cheeks and internally by residual alveolar ridge.
CLINICAL SIGNIFICANCE The patient’s mouth must be half open during impression
taking,because opening of mouth during final impression results the coronoid process to come front narrowing buccal vestibule.

Hamular notch
Hamular notch forms the distal limit of the buccal vestibule ,located between the tuberosity and the hamulus of the medial pterygoid plate.
Pterygomandibular raphe is attached to the hamular notch.
It has thick submucosa made up of loose areolar tissue.
CLINICAL SIGNIFICANCE If denture border is short of the hamular notch The denture will not
have a posterior seal resulting in loss of retention of the denture.
If denture extend beyond hamular notch The pterygomandibular raphe is pulled forward when patient opens mouth causing dislodgement of denture.
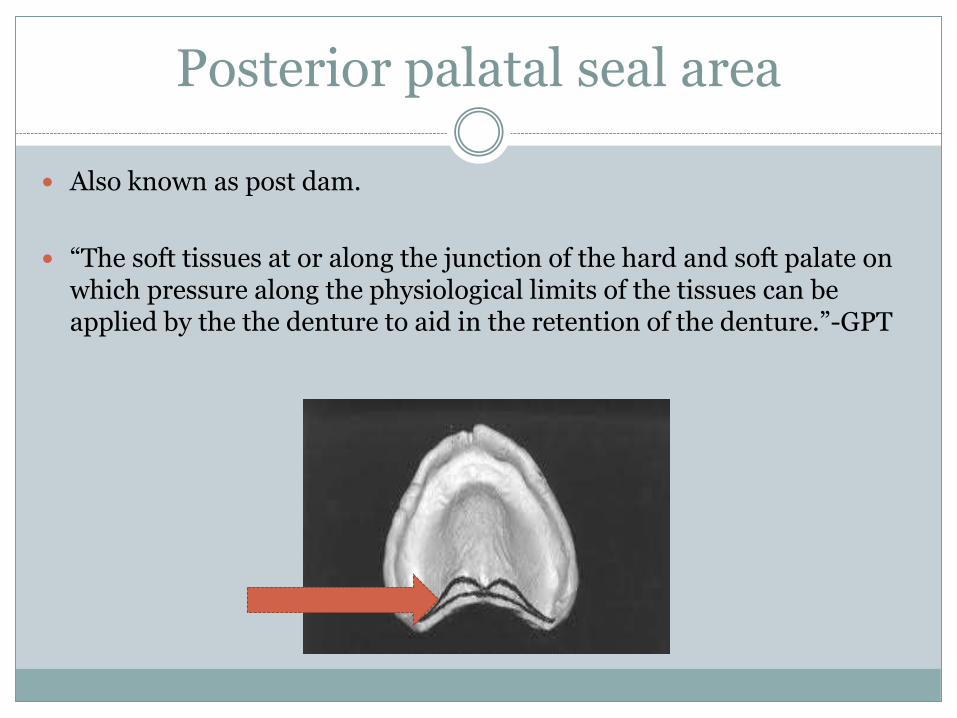
Posterior palatal seal area
Also known as post dam.
“The soft tissues at or along the junction of the hard and soft palate on which pressure along the physiological limits of the tissues can be applied by the the denture to aid in the retention of the denture.”-GPT

…..
Functions:
a) Aids in retention by maintaining contact with the soft palate during functional movements like speech,mastication and deglutition.
b) Reduces the tendency for gag reflex as it prevents the formation of the gap between the denture base and the soft palate during duringfunctional movements.
c) Prevents food accumulation between the posterior border of the denture and the soft palate.

…continued
The posterior palatal seal can be divided into:
a) Pterygomaxilary seal
b) Postpalatal seal

Pterygomaxillary seal Posterior palatal seal
It is the part of the posterior palatal seal that extends across the hamular notch and extends 3 to 4 mm anterolaterally to end in the mucogingival junction on the posterior part of the maxillary ridge.
It is the part of the posterior palatal seal area that extends between the two maxillary tuberosities.
Vs


Fig:posteriorpalatal seal

Vibrating line
“The imaginary line across the posterior part of the palate marking the division between the movable and immovable tissues of the soft palate which can be identified when the movable tissue is moving’’-GPT
Denture should extend 1-2mm posterior to this vibrating lines.
Types:
1. Anterior vibrating line
2. Posterior vibrating line
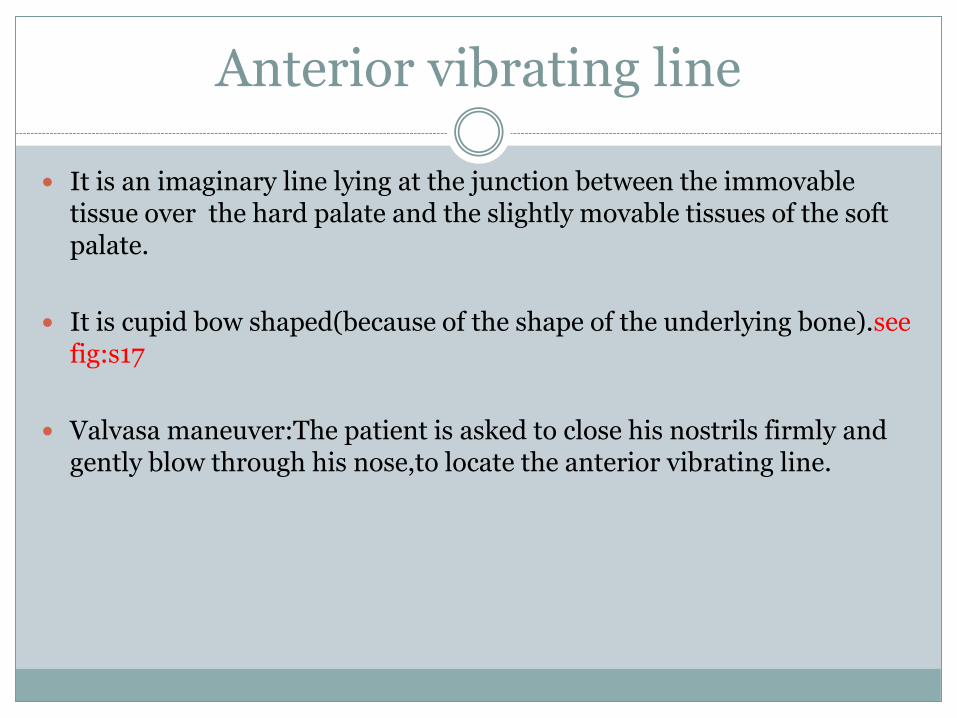
Anterior vibrating line
It is an imaginary line lying at the junction between the immovable tissue over the hard palate and the slightly movable tissues of the soft palate.
It is cupid bow shaped(because of the shape of the underlying bone).see fig:s17
Valvasa maneuver:The patient is asked to close his nostrils firmly and gently blow through his nose,to locate the anterior vibrating line.

Fig:S17-arrow showing the bone that gives bow shape to anterior vibrating line in edentulous patients.

Posterior vibrating line
It is an imaginary line located at the junction of the soft palate that shows limited movement and the soft palate that shows marked movement.
This line is usually straight.
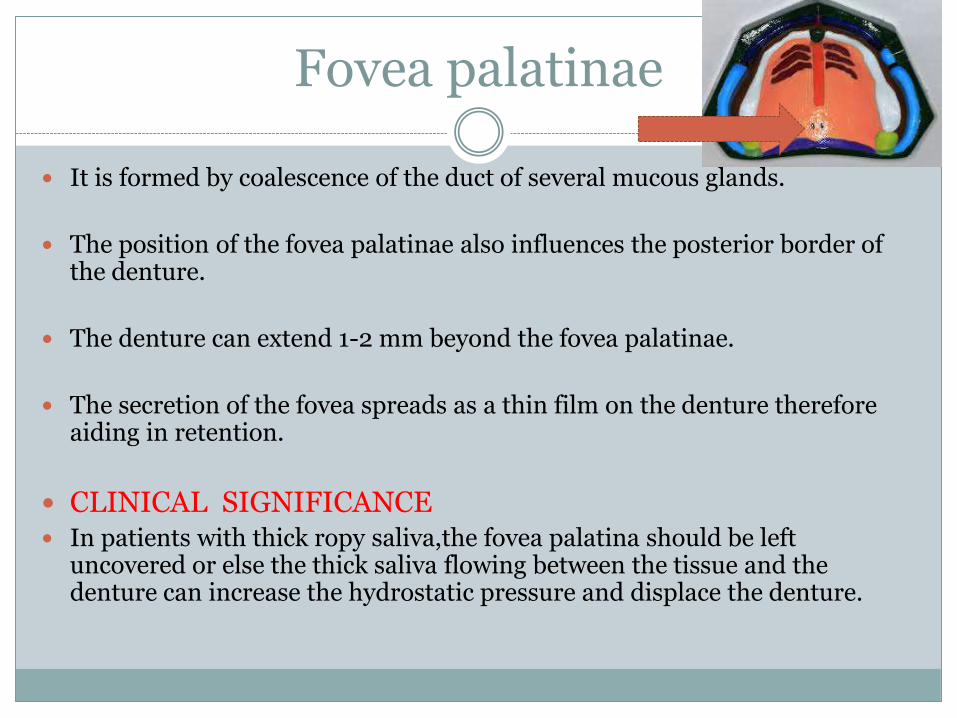
Fovea palatinae
It is formed by coalescence of the duct of several mucous glands.
The position of the fovea palatinae also influences the posterior border of the denture.
The denture can extend 1-2 mm beyond the fovea palatinae.
The secretion of the fovea spreads as a thin film on the denture therefore aiding in retention.
CLINICAL SIGNIFICANCE In patients with thick ropy saliva,the fovea palatina should be left
uncovered or else the thick saliva flowing between the tissue and the denture can increase the hydrostatic pressure and displace the denture.

Supporting structures
A)Primary stress bearing areas
1. Hard palate
2. The postero-lateral slopes of the residual alveolar ridge.
B)Secondary stress bearing areas
1. Rugae
2. Maxillary tuberosity

Hard palate
It is formed by palatine shelves of the maxillary bone and the premaxilla.
Lined by keratinised epithelium.
CLINICAL SIGNIFICANCE
a) The trabecular pattern in the bone is perpendicular to the direction of force,making it capable of withstanding any amount of force without marked resorption.

Posterolateral slopes of residual ridge
“The portion of the alveolar ridge and its soft tissue covering which remains following removal of the teeth.”-GPT
Lined by thick stratified squamous epithelium.
Even though the submucosa is thin it sufficiently provide adequate resiliency to support the denture.
CLINICAL SIGNIFICANCE
a) The vertical forces during physiological activities like mastication falls on denture and is transmitted posteriorly.The posterolateral slopes of the ridge bears the force and hence is the primary supporting structure.

Rugae
These are the mucosal folds located in the anterior region of the palatal mucosa.
In the area of rugae,the palate is set at an angle to the residual alveolar ridge and is thinly covered by soft tissue which contributes to the secondary stress bearing area.

Maxillary tuberosity
It is the bulbous extension of the residual alveolar ridge in the 2nd and 3rd molar region,terminating in the hamular notch.
CLINICAL SIGNIFICANCE
a) The area is less likely to resorb.
b) Artficial teeth are not set on tuberosity region

Relief Area
1. Incisive papillae
2. Midpalatine raphe
Incisive papillae
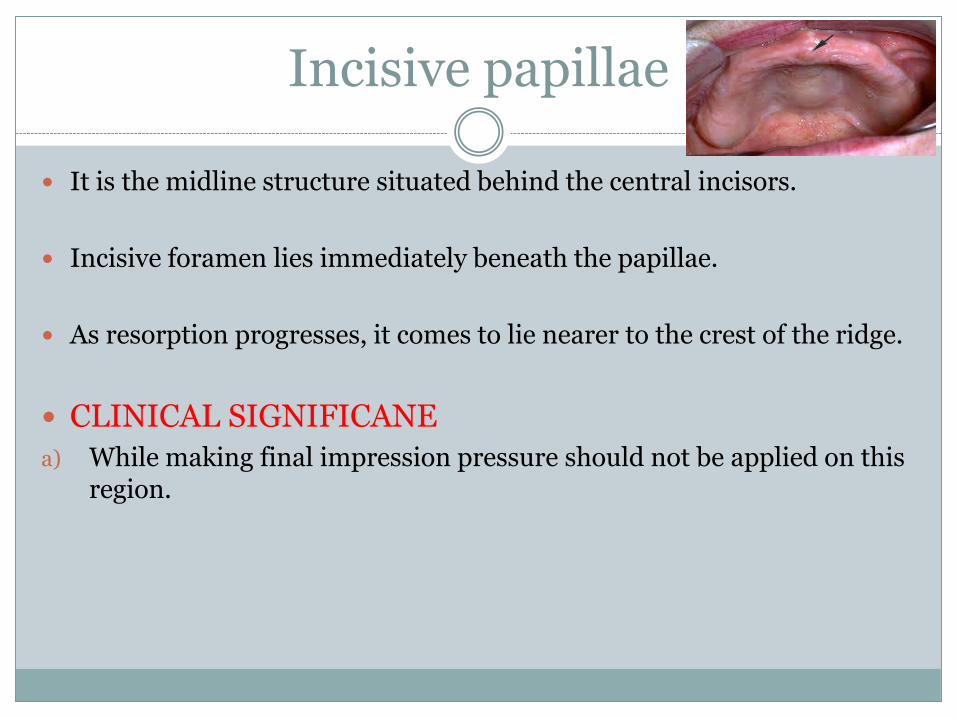
It is the midline structure situated behind the central incisors.
Incisive foramen lies immediately beneath the papillae.
As resorption progresses, it comes to lie nearer to the crest of the ridge.
CLINICAL SIGNIFICANE
a) While making final impression pressure should not be applied on this region.

Midpalatine raphe
This is the median suture area covered by a thin submucosa.
This area is sensitive to pressure application
CLINICAL SIGNIFICANCE
a) If pressure is applied during impression making,the denture base will cause soreness over the midpalatine raphe area.

Mandibular landmarks
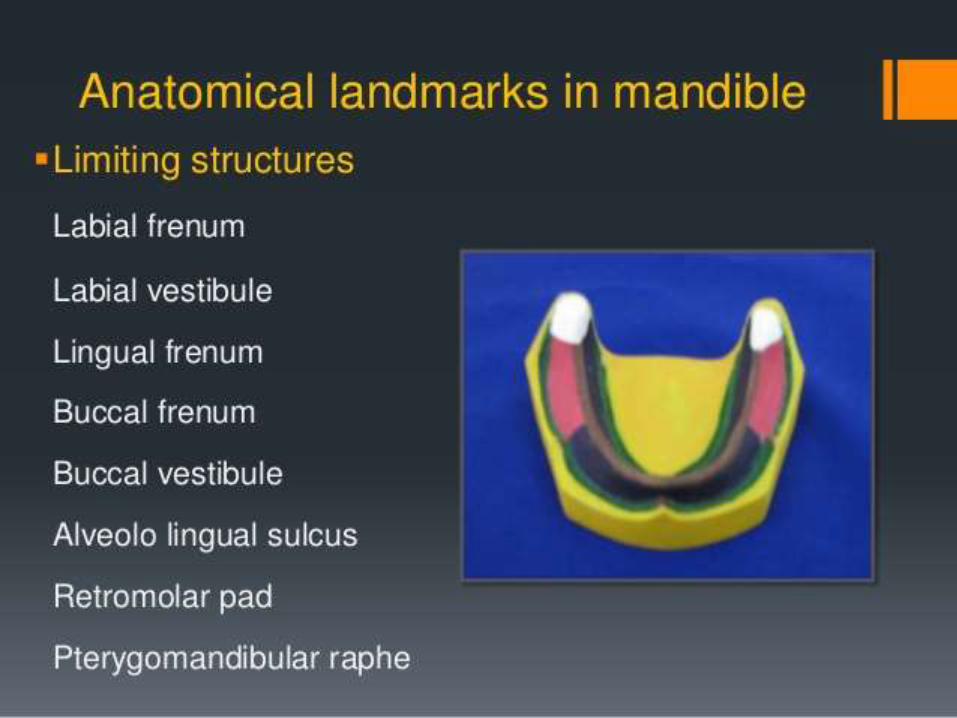
Limiting structures
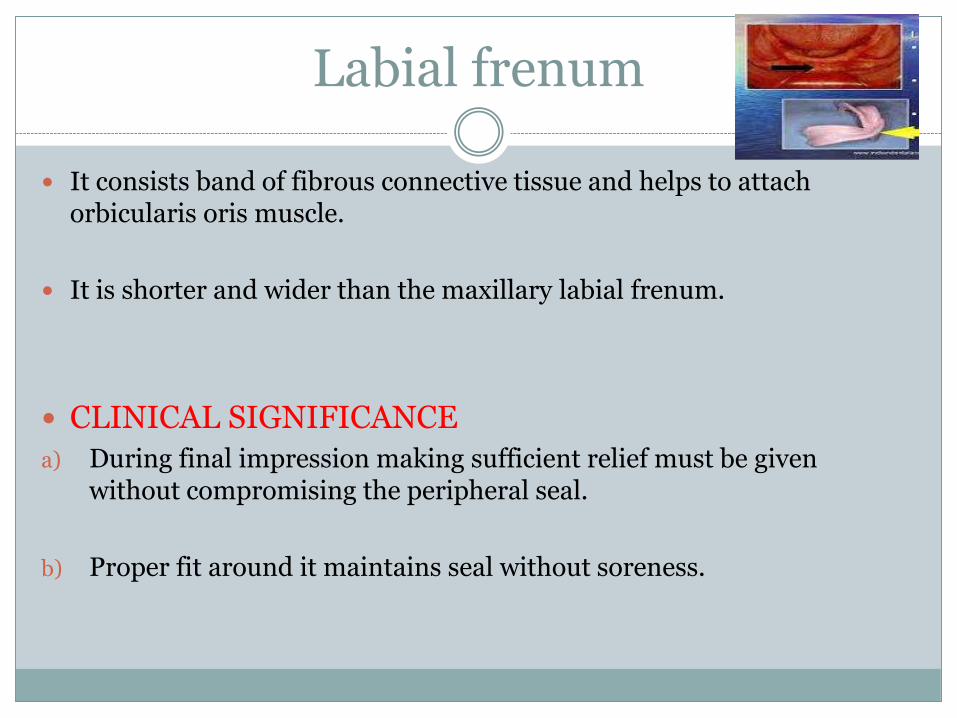
Labial frenum
It consists band of fibrous connective tissue and helps to attach orbicularis oris muscle.
It is shorter and wider than the maxillary labial frenum.
CLINICAL SIGNIFICANCE
a) During final impression making sufficient relief must be given without compromising the peripheral seal.
b) Proper fit around it maintains seal without soreness.

Labial vestibule
It runs from the labial frenum to buccal frenum.
Fibers of orbicularis oris,incisivus and mentalis are inserted near the crest of the ridge. Mentalis muscle is an active muscle.
CLINICAL SIGNIFICANCE.
a) Extent of the denture flange in this region is often limited because of muscle that are inserted close to the crest of the ridge.
b) Thick denture flanges may cause dislodgement of dentures when patient opens the mouth wide open.

Buccal frenum
It is a mucous membrane extending from buccal mucous membrane reflection toward the slope or crest of the residual ridge in the region just distal to the cuspid eminence.
May be single or double.
It overlies depressor anguli oris muscle.
CLINICAL SIGNIFICANCE.
a) Relief for buccal frenum is given in denture to avoid displacement of the denture.
Buccal vestibule
Extends from buccal frenum to the outside back corner of the retromolarpad.
It is nearly at right angles to biting forces.
Extent of the buccal vestibule is influenced by buccinators muscle,whichextends from modiolous anteriorly to pterygomandibular raphe.
The masseter muscle contracts under heavy closing force and pushes inward against the buccinators muscle to produce a massetric notch in the distobuccal border of the lower denture.
CLINICAL SIGNIFICANCE
The distobuccal border of the lower denture should accommodate the contracting masseter muscle so that the denture does not dislodge during heavy closing force.

Lingual frenum
It is a fold of mucous membrane existing when the tip of the tongue is elevated.
It overlies the genioglossus muscle which takes origin from the superior genial tubercle.
CLINICAL SIGNIFICANCE
The relief for the lingual frenum should be registered during function.

Retromolar pad
It is a non-keratinised triangular pear-shaped pad of tissue at the distal end of the lower ridge.
Submucosa contains glandular tissue, fibers of buccinators and superior constrictor muscle, pterygomandibular raphe and terminal part of the tendon of the temporalis.
CLINICAL SIGNIFICANCE.
a) The distal end of the denture pad should cover 2/3rd of the retromolarpad.
b) The retromolar pad provides the peripheral posterior seal for the lower denture.

Pterygomandibular raphe
Raphe=tendinous insertion of two muscles.
Arises from the hamular process of the medial pterygoid and gets attached to the mylohyoid ridge.
Muscular attachments present here are:
a) superior constrictor---postreolaterally
b) Buccinator-------------anterolaterally
CLINICAL SIGNIFICANCE
a) Since it is very prominent in some patients a notch like relief must be provided on the denture.

Alveolingual Sulcus
It is the space between residual ridge and tongue
CLINICAL SIGNIFICANCE
The lingual flange of the lower denture will be short anteriorly than posteriorly
The lingual flange in the middle region slopes medially towards the tongue


Buccal shelf area
It is the area between buccal frenum and anterior border of masseter muscle.
BOUNDARIES:
a) Medially-the crest of the ridge.
b) Distally-the retromolar pad
c) Laterally-the external oblique ridge.
It has a thick submucosa overlying a cortical plate.
CLINICAL SIGNIFICANCE
a) It lies at right angles to the vertical occlusal force;makes it suitable as primary stress bearing area for lower denture.
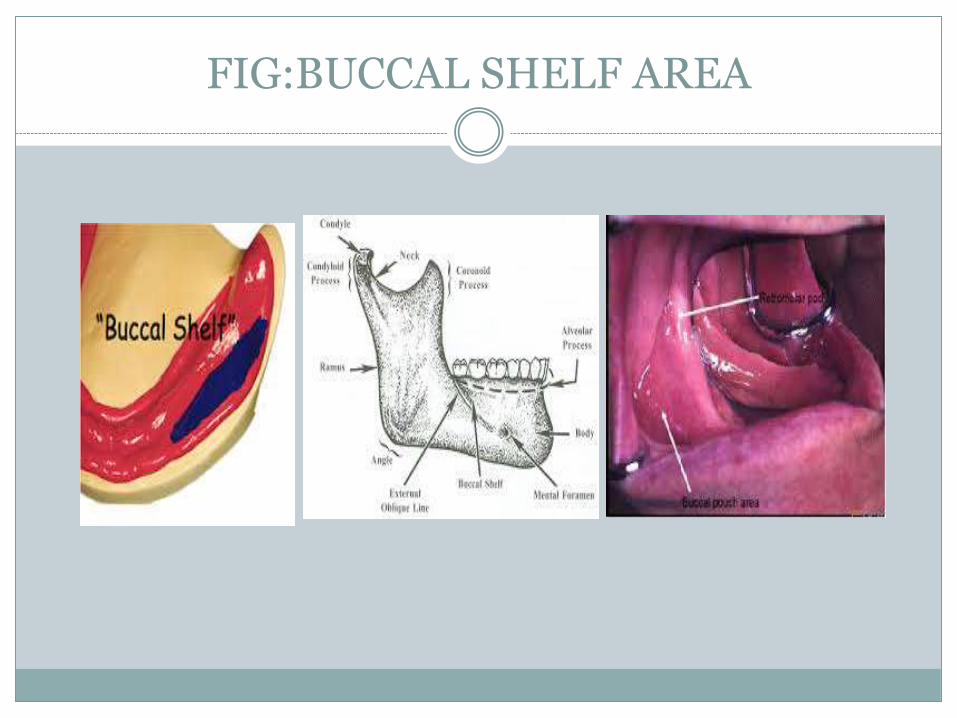
FIG:BUCCAL SHELF AREA

Residual alveolar ridge
The endentulous mandible may become flat, due to resorption; which results into outward inclination and progressively widening of mandible.
Similarly maxilla resorbs upward and inward making it smaller.
It is the reason for edentulous patients to have prognathic apperance.

……continued
The slopes of residual alveolar ridge have thin plate of cortical bone.Theslopes of the ridge are at an acute angle to occlusal forces.
Hence,it is considered as a SECONDARY stress bearing area.
Since crest of the ridge has cancellous bone, it is not favourable as primary stress bearing area.
CLINICAL SIGNIFICANCE.
a) Any movable soft tissue overlying the ridge should not be compressed while making impression.

Relief areas
Mental foramen
Genial tubercle
Torus mandibularis
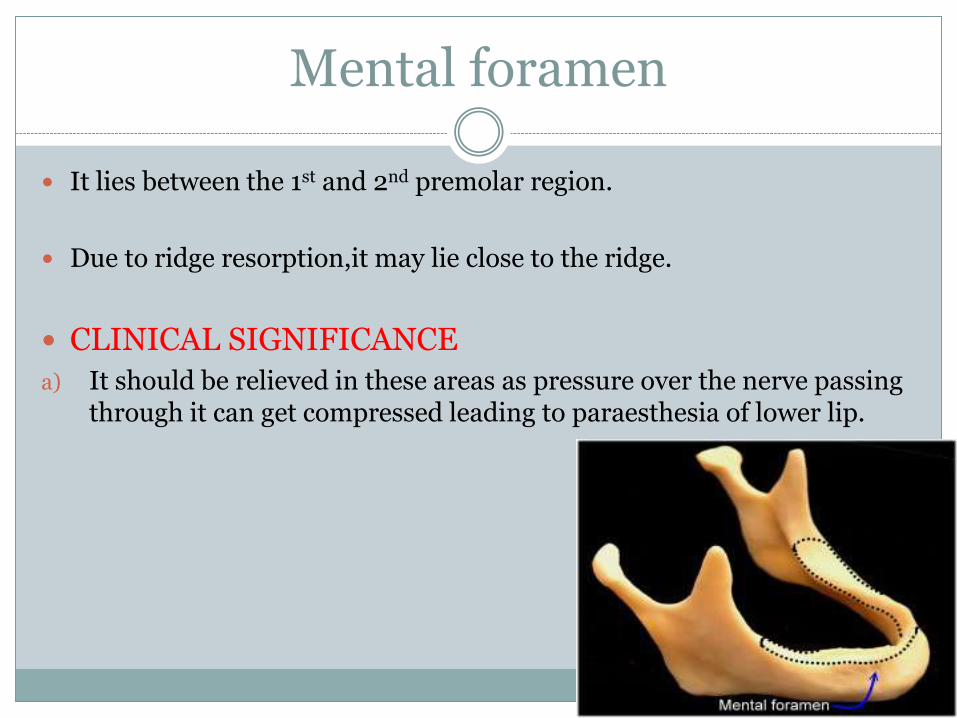
Mental foramen
It lies between the 1st and 2nd premolar region.
Due to ridge resorption,it may lie close to the ridge.
CLINICAL SIGNIFICANCE
a) It should be relieved in these areas as pressure over the nerve passing through it can get compressed leading to paraesthesia of lower lip.

Genial tubercle
These are pair of bony tubercles on lingual side of the body of mandible.
With resorption tubercles become increasingly prominent.
Torus mandibularisa) These are the abnormal bony prominence found bilaterally on the
lingual side, near the premolar region.
b) It is covered by thin mucosa.
c) It has to be relieved or surgically removed,
according to its size and extent.
REFERENCES Prosthodontic treatment for edentulous patient : Zarb Bolender
Preclinical manual of prosthodontics : S Lakshmi
Impressions for complete dentures : Bernard Levin
Textbook of Prosthodontic : Nallasyamy