ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN ......i ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN...
55
i ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN KENYA: 2008-2011 By KIBE NICHOLAS IRUNGU Reg. No. X50/65535/2010 A Research Paper Submitted in Partial Fulfilment of the Requirements for the Award of the Degree of Master of Arts in Economics, University of Nairobi. NOVEMBER 2012
Transcript of ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN ......i ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN...

i
ANALYSIS OF EFFICIENCY OF PUBLIC HOSPITALS IN KENYA: 2008-2011
By
KIBE NICHOLAS IRUNGU
Reg. No. X50/65535/2010
A Research Paper Submitted in Partial Fulfilment of the Requirements for the Award of the
Degree of Master of Arts in Economics, University of Nairobi.
NOVEMBER 2012
DECLARATION

ii
DECLARATION
I hereby declare that this is my original work and that to the best of my knowledge it has not
been presented for the award of a degree at any other university.
Signed ………………………………………. Date: ………………...........…………
Kibe Nicholas Irungu
X50/65535/2010
Approval
This research paper has been submitted for examination with our approval as university
supervisors.
Signed: ……………………………………….. Date: ……………………………………
Dr. Urbanus Kioko
Signed: …………………………………………Date: ……………………………………
Dr. Mercy Mugo

iii
ABSTRACT
Efficiency of health facilities in Kenya is crucial especially in the face of the increased
budgetary allocations and recent health care reforms. Provision of health services remains sub-
optimal and efficiency use remains a challenge to policy makers and health managers. It is
therefore imperative to estimate efficiency levels, factor productivity growth and determinants
of (in)efficiency to alert the policy makers and health managers of any potential gains towards
provision of quality healthcare.
Level 5 (provincial and regional) public general hospitals and Level 4 (district and sub-district)
public hospitals were studied. Malmquist data envelopment analysis was used to estimate
technical efficiency scores and total factor productivity, stochastic frontier analysis estimated
cost efficiency scores while tobit regression analysis was used to identify the determinants of
(in)efficiency. Data for 2008 to 2011 was used in the analysis.
Data envelopment analysis revealed an average technical efficiency score of 95.75% for level 5
hospitals and 97.72% for level 4 hospitals. Stochastic frontier analysis revealed an average cost
efficiency score of 77.49% for level 5 hospitals and 66.78% for level 4 hospitals. A negative
technological change for level 4 and 5 public hospitals was found to impact negatively on the
total factor productivity for the two levels of public hospitals. An increase in recurrent
expenditure was found to reduce cost efficiency in both level 4 and level 5 public hospitals.
Increases in number of nurses was found to increase cost efficiency in level 5 public general
hospitals while increases of doctors increased cost efficiency in level 4 public hospitals.
Conclusively, the study shows that there is potentiality for productivity growth in health sector
in Kenya by considering efficiency use and increased investments in technological innovations.
Further research study is recommended to seek why increases in recurrent expenditure results
into a decline in cost efficiency in level 4 and 5 public hospitals.

iv
DEDICATION
To my wife; Leah and sons; Linus, Collins and Ryan.

v
ACKNOWLEDGEMENT
I wish to thank my Almighty God for giving me the strength and good state of health to pursue my education. He has continued to give me victory in all my educational life and He has enabled me reach this far.
I also wish to express my deepest gratitude to the School of economics, University of Nairobi for offering me an admission to further my studies.
I am highly indebted to Ministry of State for Planning, National Development and Vision 2030 for the financial support which enabled me pursue my postgraduate studies.
I am also sincerely and heartily grateful to my supervisors, Dr. Urbanus Kioko and Dr. Mercy Mugo for their continued support, encouragement and guidance they gave me throughout my research which has been invaluable both in my academic and professional life. I am also thankful to all other lecturers in the School of Economics who sharpened my understanding and critical thinking on real life experiences.
I salute my classmates who boosted me morally and provided much information through discussions. I also offer my regards and blessings to Mr. Cheburet and Mr. David Njuguna from Ministry of Medical Services for providing me with data necessary for my research.
I would also sincerely like to thank my parents who gave me the opportunity of an education, care and support throughout my life.
May Almighty God bless you all.

vi
Table of Contents
DECLARATION ............................................................................................................................................... ii
ABSTRACT ..................................................................................................................................................... iii
DEDICATION ................................................................................................................................................. iv
ACKNOWLEDGEMENT ................................................................................................................................... v
List of Tables .............................................................................................................................................. viii
List of Figures ............................................................................................................................................... ix
List of Abbreviations ..................................................................................................................................... x
CHAPTER ONE ............................................................................................................................................... 1
1.0 Background ................................................................................................................................... 1
1.1 Kenya’s Health System .................................................................................................................. 4
1.2 Statement of the Problem ............................................................................................................ 5
1.3 Objectives...................................................................................................................................... 6
1.4 Specific Objectives ........................................................................................................................ 6
1.6 Justification of the Study............................................................................................................... 6
CHAPTER TWO .............................................................................................................................................. 8
LITERATURE REVIEW ..................................................................................................................................... 8
2.1 Theoretical review of literature .................................................................................................... 8
2.1.1 Production Economics Theory .............................................................................................. 8
2.1.2 Seminal Works by Farrell (1957) ........................................................................................... 9
2.2 Empirical review of literature ..................................................................................................... 11
2.3 Overview of Literature ................................................................................................................ 15
CHAPTER THREE .......................................................................................................................................... 16
METHODOLOGY .......................................................................................................................................... 16
3.1 Data Envelopment Analysis (DEA) .............................................................................................. 16
3.2 Stochastic Frontier Analysis (SFA) ............................................................................................... 19
3.3 Malmquist Productivity Index ..................................................................................................... 20
3.4 Tobit Regression Analysis ............................................................................................................ 21
3.5 Data and Variables ...................................................................................................................... 23
CHAPTER FOUR ........................................................................................................................................... 25
EMPIRICAL RESULTS .................................................................................................................................... 25

vii
4.1 Introduction ................................................................................................................................ 25
4.2 Descriptive Statistics and Correlation Matrix of variables-Level 5 public hospitals ................... 25
4.3 Technical Efficiency Analysis (Data Envelopment Analysis) of Level 5 (provincial and regional)
hospitals in Kenya ................................................................................................................................... 26
4.4 Cost Efficiency Analysis (Stochastic Frontier Analysis) of Level 5 (provincial) hospitals in Kenya
27
4.5 Determinants of Efficiency in Level 5 (provincial and regional) public hospitals in Kenya ......... 29
4.6 Analysis of Efficiencies of Level 4 public hospitals in Kenya ....................................................... 30
4.7 Cost Efficiency Analysis (Stochastic Frontier Analysis) of level 4 public hospitals ...................... 33
4.8 Determinants of Efficiency in Level 4 public hospitals................................................................ 35
4.9 Conclusion ................................................................................................................................... 36
CHAPTER FIVE ............................................................................................................................................. 37
SUMMARY, POLICY RECOMMENDATIONS AND CONCLUSIONS ................................................................. 37
5.1 Summary ..................................................................................................................................... 37
5.2 Policy Recommendations ............................................................................................................ 38
5.3 Conclusion ................................................................................................................................... 38
5.4 Limitations of the Study .............................................................................................................. 38
References .................................................................................................................................................. 40
Appendices .................................................................................................................................................. 44

viii
List of Tables
Table 1: Descriptive Statistics of variables-Level 5 public hospitals.............................................25
Table 2: Correlation Matrix of variables- Level 5 public hospitals...............................................25
Table 3: Technical Efficiency Scores of Provincial (Level 5) Public Hospitals in Kenya..............26
Table 4: Malmquist Index Summary of Level 5 Hospitals in Kenya..............................................27
Table 5: Estimated Coefficients of the Cobb Douglas Cost Function for level 5 public
Hospitals...................................................................................................................................28
Table 6: Cost Efficiency Scores (Stochastic Frontier Analysis) for Level 5 (provincial and
regional) hospitals in Kenya.....................................................................................................28
Table 7: Results from Tobit Regression using DEA Technical Efficiency Scores........................30
Table 8: Results of Tobit regression using SFA Cost Efficiency Scores.......................................30
Table 9: Descriptive statistics of variables (DEA) for Level 4 public hospitals...........................31
Table 10: Correlation matrix of variables (DEA) for Level 4 public hospitals...........................31
Table 11: Technical Efficiency Scores of Level 4 public hospitals estimated using DEA...........32
Table 12: Malmquist Index Summary of level 4 public hospitals provincial means.................32
Table 13: The estimated parameters of the Cobb Douglas Cost Function for level 4 public
hospitals...................................................................................................................................33
Table 14: Level 4 public hospitals cost efficiency scores (SFA).................................................34
Table 15: Tobit Regression using DEA Technical Efficiency Scores-level 4 public hospitals.....35
Table 16: Results from Tobit regression SFA Analysis-level 4 public hospitals..........................36
Table 17: Number of health facilities by type............................................................................45
Table 18: Number of health facilities by ownership.................................................................45

ix
List of Figures
Figure 1.1: Input-oriented measure of efficiency......................................................................11

x
List of Abbreviations
AIDS Acquired Immune Deficiency Syndrome
ALOS Average Length of Stay
ANC Antenatal Clinic
CBHW Community Based Health Workers
CHCs Community Health Centres
CHPs Community Health Posts
CRS Constant returns to Scale
DALYs Disability Adjusted Life Years
DEA Data Envelopment Analysis
DEAP Data Envelopment Analysis Program
FBO Faith Based Organisations
GDP Gross Domestic Product
HLYs Healthy Life Years
HIV Human Immuno-deficiency Virus
MCHPs Maternal and Child Health Posts
MPI Malmquist Productivity Index
MTEF Medium Term Expenditure Framework
NGO Non-Governmental Organisations
NHSSP National Health Sector Strategic Plan
PGH Provincial General Hospital
QALYs Quality of Life Adjusted Life Years
SE Scale Efficiency
SECHN State Enrolled Community Health Nurses

xi
SFA Stochastic Frontier Analysis
TE Technical Efficiency
TFP Total Factor Productivity
UNICEF United Nations Children’s Fund
WHO World Health Organisation

1
CHAPTER ONE
INTRODUCTION
1.0 Background
Achieving a high level of efficiency in the health sector in Kenya is an important task in the
face of significant budgetary allocations in the public health sector. The public expenditure on
health has been increasing significantly from Ksh. 26 billion in 2007/08 to Ksh. 32.94billion
in 2008/09, Ksh. 43.33 billion in 2009/10 and to Ksh. 50.37 billion in 2010/11 (Luoma, et
al., 2010, Health Sector Working Group, 2012). However, according to Sealy and Rosbach
(2010), Government health expenditure as a percent of total government budget was 6.5% for
the financial year 2010/2011 which falls below the target of 15% recommended by the Abuja
Declaration.
UNICEF (2007) noted that the Kenyan government allocates 1.5% of GDP to health, most of
which is expended to curative health interventions instead of spearheading preventive health
interventions which is the policy goal. Consequently, diseases which could have been
prevented at lower costs are treated later at much higher costs leading to large scale
inefficiencies.
The Kenyan health budget has been growing over time, but there has not been a corresponding
significant change in key health indicators. Comparisons from the Kenya Demographic and
Health Survey conducted in 2003 and Kenya Demographic and Health Survey conducted in
financial year 2008/09 reveals that maternal mortality ratio remains high at 488 maternal
deaths per 100000 live births in 2008/09 from 414 per 100000 in 2003. Also, proportion of
women attending antenatal care visits of four times and above has been declining from 64
percent in 1993 to 52 percent in 2003 and to 47 percent in 2008/09. However, infant
mortality rate improved to 52 in 2008/09 from 77 per 1000 live births in 2003. In addition,

2
under 5 mortality rate also improved to 74 in 2008/09 from 115 per 1000 live births in
2003.
Efficient allocation of the health care resources remains a serious challenge in health policies.
The failure to achieve the required improvements in health indicators despite increased budget
allocation implies that the available resources may not have been utilized efficiently. It is
imperative to note that inefficiency slows down productivity1 of the health facilities and this is
viewed as a major cause of increasing health care cost.
According to UNICEF (2007), the provision of health services in Kenya remains generally sub-
optimal because majority of the health facilities have staffing imbalances of qualified personnel
resulting from weak deployment procedures. Additionally, insufficient skilled human resources
(medical officers, dentists, nurses, midwives and other specialists) are also a major constraint
to improving service delivery. For example, the doctor-patient ratio is about 17:100,000 (GoK,
2009c) against the recommended 1:600 by the World Health Organization (WHO) while the
nurse-patient ratio is 121:100,000 (GoK, 2009c) against the recommended 200:100,000 by
WHO.
In addition, upsurge in non-communicable diseases (for example cancer and diabetes),
excessive dependence on donors, HIV/AIDS pandemic, poverty and weak management systems
are a challenge in the health sector. UNICEF (2007) noted that the weak management capacity
of the health sector allows in particular the leakage of development funding from reaching the
destined projects/programmes due to an inefficient financial management systems. UNICEF
further noted that there has been limited access to health services particularly in rural areas
and usually characterized by poor quality service.
1 Productivity is output produced per unit of input. It involves technical efficiency with which inputs are turned into
outputs.

3
Several economic development policies and plans like the Kenya Vision 2030, the National
Health Sector Strategic Plan (NHSSP) II 2005-2010 and the National Health Accounts
2009/10 place emphasis on improving efficiency in health sector service delivery. Efficiency
improvement in hospitals is a key strategy to mobilize more resources domestically for the
decentralized health facilities. In addition to lobbying for more domestic and external
resources, health managers and policy makers should ensure optimal use of available
resources. According to Sealy and Rosbach (2010), hospitals in Kenya account for 75% of the
health sector recurrent budget and employ 80% of the key professional health staff. However,
despite the increased health sector allocations, the sector according to Owino and Korir (1997)
faces shortages of drugs and medical supplies, dilapidated facilities (malfunctioning operating
theatres), poor servicing of equipments and shortage of professional staff, which points to
insufficient or inefficient use of the available resources.
Kirigia, et al., (2004) highlighted some of the major reforms initiated in Kenya to eliminate
inefficiencies in healthcare. These included harmonization and decentralization of health care
interventions, expansion of preventive health services including family planning services, use
of health insurance schemes, integration of traditional medicine with western medicine, and
use of user fees in government health facilities. Efficiency determination is crucial especially in
the face of the increased budgetary allocations coupled with the recent reforms by the NHIF of
financing health facilities through the capitation method2.
2 Capitation method refers to a fixed per capita amount paid periodically to a hospital for each enrolled patient
served.

4
1.1 Kenya’s Health System
The Kenyan health sector comprises the public sector and the private sector. The public sector
consists of Ministry of Public Health and Sanitation, Ministry of Medical Services and
parastatal organizations while the private sector consist of private for profit and private not for
profit NGO and FBO facilities. The ministries of health are responsible for policy formulation
for all service providers (both public and private). The Ministry of Public Health and Sanitation
plays an oversight role in service delivery of primary healthcare facilities which mainly deal in
preventive services with limited curative care (levels 1-3) while the Ministry of Medical
Services is responsible for curative care (levels 4-6).
The public health care system is organized around six levels (Level 1-6). Level 1 consists of
community based health care offered by Community Based Health Workers (CBHW). They
offer promotive and preventive primary health service thus, improving efficiency and timely
referral to the next level of facility. Level 2 comprise dispensaries and clinics. They are a link
between community based healthcare and health facilities providing ambulatory services
including maternal services. Level 3 are health centres, nursing homes and maternity homes
comprising first in-patient services including maternal delivery. Level 4 are the sub-district
and district hospitals which forms the beginning of a well established curative primary referral
health care system offering in-patient services with specialized medical attention. Level 5 are
the provincial or regional referral hospitals constituting a secondary specialized curative
health care intervention. Level 6 are the national teaching and referral hospitals which are the
highly specialized tertiary health care facilities.
This study intends to concentrate on level 4 and 5 hospitals being the first defined referral
health care providers, decentralized to deal with the grassroot health problems but often faced
with limited accessibility to affordable and quality healthcare. According to National Economic

5
and Social Council (2010), they suffer from weak financial management systems, inadequate
policy and supporting regulations, inefficient procurement systems and inadequate or
unevenly distributed human resources.
1.2 Statement of the Problem
Efficiency improvement should be seen as a strategy for mobilizing domestic resources and
utilizing the available resources without waste to achieve the desired health sector goals.
Moreover, the estimation of efficiency ought to be done more often so as to maximize health
gains from available health sector resources, however it is not usually the case especially in
low income countries like Kenya.
Practically, there is not much consideration to efficiency by health care administrators in
contrast to it being mentioned in health policies. Policy makers and health managers in Kenya’s
health sector use programme based budgeting where they use cost estimates in determining
their budget requirements without considering savings from efficiency gains. Secondly, the
MTEF budgeting process considers mainly the previous absorption capacity in the allocation of
resources and not the efficiency with which the ministry utilizes its resources.
From the foregoing, it is evident that the policy makers and health managers are largely
concerned with mobilizing additional funding without paying much attention to efficiency
savings. However, despite the increased funding in the health sector, the sector continues to
face many serious challenges such as poor working conditions, inadequate medical staff,
inadequate medical supplies, frequent drug stock-outs and patient congestion. Most of these
challenges can be addressed by improving efficiency in the use of available resources thereby
avoiding wastage.

6
This study therefore seeks to determine the technical and cost efficiency of the public hospitals
in Kenya and identify factors responsible for contributing to (in) efficiency in service delivery.
The study is guided by the following policy questions: i) which level 4-5 public hospitals are
the most efficient? ii) Which are some of the factors associated with inefficiency? iii) How did
the productivity change between 2008 and 2011 in the level 4-5 public hospitals? iv) What
are some of the policy implications which can be drawn from the study?
1.3 Objectives
The broad objective of this study is to estimate the relative technical and cost efficiency of level
4-5 public hospitals in Kenya; and derive policy implications.
1.4 Specific Objectives
The specific objectives of the study include;
1. To estimate the relative technical efficiency and cost efficiency of level 4 and 5 public
hospitals in Kenya.
2. To measure the productivity change of the public hospitals between 2008 and 2011.
3. To identify the determinants of (in) efficiency in levels 4 and 5 public hospitals in
Kenya.
4. To draw policy implications and recommendations based on study findings.
1.6 Justification of the Study
There is limited literature on efficiency studies of public hospitals in Kenya. The study by
Kirigia et al., (2002) in Kenya on technical efficiency of public hospitals looked only at the
efficiency levels and the magnitudes of the performance targets without determining the
causes of inefficiency and productivity changes. The study by Owino and Korir (1997) in

7
Kenya, also failed to determine the productivity change. There is also need to re-estimate the
technical efficiency of the public hospitals given the reforms that have taken place within the
public health sector.
Efficiency estimation over a period of time will provide direction to hospital managers, policy
makers and other stakeholders on issues of (in)efficiency and productivity growth of the
hospitals. This will guide them in the development of strategies to reduce inefficiency and
increase productivity. This will also guide in the distribution of resources especially from
facilities where there is excess (wastage) to areas where they will increase output. The analysis
of productivity growth decomposed into technical efficiency changes, technological changes
and scale changes ensures that the hospitals are aware of the sources of their productivity. This
will make hospitals increase productivity in both technical progress and efficiency
improvement and be able to decide on their scale of operations.
This study estimates efficiency of public hospitals by use of both DEA and SFA as a crosscheck
with each other. Each of these methods has its weaknesses and strengths such that a trade off
exists on the use of either one of them.

8
CHAPTER TWO
LITERATURE REVIEW
2.1 Theoretical review of literature
According to Zere, et al., (2006), technical efficiency of a hospital can be decomposed into
scale efficiency and pure technical efficiency. The pure technical efficiency refers to the ability
by the management to organize inputs in the process of production while the scale efficiency
refers to the managerial ability to choose the optimum size of the hospital. Inappropriate
hospital size may cause scale inefficiency. Scale inefficiency can be either due to decreasing
returns to scale as a result of a hospital being too large for the volume of activities it conducts
or increasing returns to scale as a result of it being too small for its volume of activities.
Measurement of technical efficiency is founded on microeconomic theory. It has its basis on
the theory of the firm. The seminal work by Farrell (1957), gives a theoretical background to
the measurement of the technical efficiency.
2.1.1 Production Economics Theory
According to Maddala and Ellen (1989), production economics is part of microeconomic
theory concerned with production of output from a given set of inputs usually expressed in
terms of a production function. A production function is a functional relationship between
outputs and inputs showing the maximum output to be obtained from a given set of inputs. It
defines a technological relationship between inputs and output of a product. It is usually
specified as:
Q =f (x1, x2, ........., xn)
Where Q=maximum amount of output
x1, x2, ........., xn = are amounts of various inputs;

9
Maddala and Ellen (1989) stated further that a firm is technically efficient if it obtains
maximum level of output from any given set of inputs. A production function therefore defines
a technically efficient method of production such that a producer cannot decrease one input
and maintain the same output level at the same time without increasing one or more inputs.
A production plan is therefore efficient if more output cannot be produced with the same
inputs or the same output cannot be obtained with less input. Hospitals combine multiple
inputs (human, financial, informational resources) to produce multiple outputs (services or
interventions) intended to ultimately improve health or quality of life outcomes.
2.1.2 Seminal Works by Farrell (1957)
Farrell (1957) pioneered measurement of efficiency in his seminal work, “the measurement of
productive efficiency”. He considered a firm using two factors of production X1(medical staff)
and X2 (number of beds) to produce a single output, Y (outpatient visit) under constant returns
to scale. He also assumed an efficient production function. These assumptions helped explain
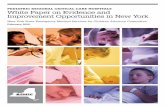
the production function by using an isoquant SS’ as shown in the figure 1.1.
In Farrell’s seminal work, efficiency of an individual firm is measured in comparison to the
efficiency of other firms in the industry given that the firms are on or below the frontier. A
firm is considered to be technically efficient if it operates on the best practice production
frontier in the industry. The basic ideas underlying Farrell’s concepts of technical and
allocative efficiencies are explained in figure 1.1.
A hospital produces its output (outpatient visit) using a combination of two inputs (medical
staff and number of beds). A technically efficient hospital is the one located on the isoquant SS’.
Therefore, hospitals at points B, Q and Q’ are technically efficient while at points P and T are
technically inefficient. The technical efficiency for a hospital at point P is given as, .

10
This defines the ratio of the required minimum input to the actual input used, given the input
combination used by P. The ratio defines the percentage by which all inputs could be
decreased without a decrease in output. The hospital producing at point P has to relocate to
point Q for it to be efficient.
When input prices are given, the isocost line AA’ gives the minimum cost of producing a unit
of output. Allocative efficiency requires production to take place where the isoquant is tangent
to isocost line. Therefore, the hospitals at point B and Q are allocatively inefficient but
technically efficient. The hospital at point Q’ is both allocatively and technically efficient. The
allocative efficiency of hospital P is given as, . The ratio defines the percentage
decrease in costs of production if production were to take place in the allocative efficient point,
Q’.
Farrell proposed overall (economic efficiency) to be measured as, , meaning that the
overall efficiency is a product of technical efficiency and allocative efficiency.
According to Moshiri et al., (2010), a hospital is termed to be technically efficient if an output
increase leads to a reduction in another output or an increase in another input. Consequently,
a decrease in any input leads to an increase in another input or a reduction in another output.

11
Figure 1.1: Input-oriented measure of efficiency
2.2 Empirical review of literature
This section analyses some of the empirical studies conducted in Africa. Among the studies
reviewed, two articles are from Kenya on technical efficiency measurements of public hospitals
conducted in 2002 and 1997.
A study in Ghana by Akazili, et al., (2008) demonstrated that public health facilities are not
maximizing healthcare outcomes from available resource endowments. The input variables
used were number of non-clinical staff, number of clinical staff, number of beds and cots, and
cost of drugs and supplies while the outputs were number of general outpatient visits, visits to
antenatal care clinic, number of deliveries, number of immunizations to children, and visits to
family planning clinic. Results from 89 randomly selected health centres using DEA analysis
showed that 58 (65%) were technically inefficient with average technical efficiency score of
X2/Y .S
.B .P
.Q .T
A . R
.Q’ .S’
.A’
0 X1/Y
Source: Farrell (1957) Coelli et al. (2005)

12
57% while 70 (79%) were scale inefficient with average scale efficiency score of 86%. The
study recommended performance targets for the inefficient facilities.
High inefficiencies in hospitals impedes government’s initiatives to improve access to quality
healthcare according to a study by Zere, et al., (2006) in Namibia based on all 30 public sector
hospitals. The study used DEA technique to analyze data for 1997/98 to 2000/01 but did not
estimate change in productivity because of incomplete data. The inputs were total recurrent
expenditure, number of beds, and number of the nursing workforce while outputs were total
outpatient visits, and number of inpatient days. The average technical efficiency level for the
given period ranged from 62.7% to 74.3%. Increasing returns to scale was the most form of
scale inefficiency. Output expansion in presence of increasing returns to scale decreases unit
costs, which would necessitate an increase in demand for healthcare which was found to be
beyond the control of the hospital management and as a result merger of hospitals in close
proximity was viewed to be an option.
In South Africa, a study by Zere (2000) showed that inefficiency was a major problem
affecting hospitals. Among three levels of public hospitals: community hospitals with
emergency services only (level one), community hospitals with outpatient services (level two)
and non-academic secondary and tertiary hospitals (level three), the average technical
efficiency from DEA analysis was 0.74, 0.68 and 0.70 for level one, level two, and level three
hospitals respectively. The tobit regression showed that occupancy rate affected technical
efficiency positively in all three levels while average length of stay adversely affected only level
three hospitals. The number of outpatient visits as a proportion of inpatient days affected
technical efficiency positively and this could indicate presence of economies of scope between
the two inputs. Recurrent expenditure and bed size were used as inputs and inpatient days and
outpatient days were used as outputs.

13
Similar results were reported in Botswana like those for South Africa, Namibia and Ghana. The
study by Tlotlego, et al., (2010) based on 21 non-teaching hospitals showed that hospitals had
significant inefficiencies and failed to make best use of health inputs and existing technology.
DEA analysis was used with number of clinical staff and number of hospital beds used as
inputs and number of outpatient visits and number of inpatient days used as outputs. The
technical efficiency scores were 70.4%, 74.2% and 76.3% for the years 2006, 2007 and 2008
respectively. On average Malmquist total factor productivity decreased by 1.5%. Whilst
hospital efficiency increased by 3.1%, technical change (innovation) regressed by 4.5%.
Efficiency change was due to a pure efficiency improvement of 4.2% and a reduction in scale
efficiency by 1%.
Evidence from Sierra Leone also showed technical and scale inefficiencies. A study by Kirigia,
et al., (2011) attempted to demonstrate how savings from efficiency use can augment
government plans to funding increased health care for the population. The study singled out
input decreases and output increases necessary to make inefficient public health units efficient.
DEA analysis used outpatient visits, visits to maternal clinic, visits to child health and family
planning clinics, number of activities on vector control, and health education sessions held as
outputs while numbers of the community health officers, community health nurses and
support staff were used as inputs. Results from 36 maternal and child health posts (MCHPs),
22 community health centres (CHCs) and 21 community health posts (CHPs) revealed an
average technical efficiency levels of 68.2%, 69.2% and 59% respectively and 52.8%, 88.8%
and 95.5% average scale efficiency scores respectively.
In Kenya a study by Kirigia, et al., (2002) revealed inefficiencies in public hospitals. Among the
54 public hospitals analysed using DEA approach, 14 (26%) were technically inefficient with
an average technical efficiency score of 84% and standard deviation of 15.5% and 16 (29.6%)

14
of the hospitals were found to be scale inefficient scoring a 90% average scale efficiency. The
study provided magnitudes by which input could be reduced or output increased so as to make
inefficient hospitals attain technical efficiency. The input variables used were medical
officers/pharmacists/dentists, clinical officers, nurses, administrative staff,
technicians/technologists, subordinate staff, pharmaceuticals, non-pharmaceutical supplies,
maintenance of equipments, vehicles and buildings, and food and rations. The intermediate
outputs used were outpatient casualty visits, special clinic visits, MCH/family planning visits,
dental care visits, general medical admissions, paediatric admissions, maternity admissions,
and amenity ward admissions.
Another study in Kenya by Owino and Korir (1997) using stochastic frontier analysis estimated
an average inefficiency level of 30% in the public health sector. The inefficiency emanated
from inadequate professional staff, poor input combinations, malfunctioning operating
theatres, poor distribution of drugs and poor servicing of machines and equipments. The study
indicated that public hospitals operated at higher than their minimum average costs. This
study used recurrent expenditure as the dependent variable while average wage, admissions,
outpatients, number of surgical operations and number of beds were used as explanatory
variables.

15
2.3 Overview of Literature
The common characteristics from the studies reviewed above are: Firstly, all the studies
attempted to analyze technical efficiency of health facilities using process approach as proxies
to improved health status. Secondly, majority of the studies used data envelopment analysis to
estimate efficiency using different input and output variables. Thirdly, all the studies showed
presence of inefficiencies indicating potentials to reduce inputs or alternatively increase
outputs in-order to improve efficiency. Lastly, the inputs used in the studies included staff
members categorized into various cadres to represent labour component and number of beds
and cots were used as a proxy to capital. The outputs included outpatient visits categorized into
various visits (for example, maternal visits, antenatal visits, family planning visits and general
outpatient visits) and either inpatient days or number of inpatients.
It is also evident that there are studies on efficiency of health facilities in Kenya but these
studies have not attempted to analyze productivity change arising from technical efficiency
and technical changes. The Kenyan study by Kirigia, et al. (2002) considered one year period
and thus failed to calculate total factor productivity change. The study also failed to determine
the causes of (in)efficiency. The study by Owino and Korir (1997), also failed to determine the
total factor productivity change.

16
CHAPTER THREE
METHODOLOGY
This chapter describes analyses on data envelopment (DEA), stochastic frontier (SFA),
malmquist productivity index, the tobit regression, and data and variables to be used. This
study will use both DEA and SFA as measures of technical efficiency.
3.1 Data Envelopment Analysis (DEA)
Coelli (1994) defined Data Envelopment Analysis (DEA) as a non-parametric mathematical
programming approach to frontier estimation which uses linear programming to sketch a
boundary function (efficient frontier) to observed data for relatively homogenous firms. It
evaluates the efficiency of an individual hospital in comparison to other hospitals in the same
hospital industry. The hospitals on the frontier have an efficiency score of one and are
considered to be technically efficient relative to their peers. The efficiencies of the hospitals
below the efficiency frontier are measured by their distance to the frontier.
As stated by Kengil, et al., (2010), Tlotlego, et al., (2010), and Osei, et al., (2005), DEA is
mostly used when measurement error is most unlikely. It does not require a specified
functional form and therefore problem of model misspecification does not arise. It also uses
multiple inputs and multiple outputs in measurement of efficiency as opposed to the SFA which
typically can only use a single output with multiple inputs. Additionally, it gives targets on
specific input and output which makes an inefficient hospital attain technical efficiency. Lastly,
it fits to models where prices of resources and products are unknown.
However, according to Kengil, et al., (2010), Tlotlego, et al., (2010) and Osei, et al., (2005,
DEA being a non-parametric technique makes statistical hypothesis testing difficult to do.
Secondly, it estimates efficiency in comparison to best performing hospitals within a

17
homogeneous group and therefore, makes it is impossible to compare how public hospitals in
Kenya fare relative to other countries with respect to technical efficiency.
The technical efficiency of an individual hospital from the basic ideas of Charnes, et al.,
(1978), can be obtained by solving the linear programming model below and assuming
constant returns to scale (CRS);
(1.1)
Where:
amount of output from hospital ,
amount of input to hospital ,
weight given to output ,
weight given to input ,
number of hospitals,
number of outputs,
number of inputs
The first constraint means that the weighted sum of inputs for an individual hospital equals to
one. The second constraint means that all hospitals are on or below the frontier, that is,
efficiencies of all hospitals have an upper bound of one. The weights and are unknowns
obtained by solving the linear programming problem. Based on the production theory, a

18
hospital operating below the frontier could operate on the frontier by either increasing output
with the same input combination or produce the same output with less input.
The assumption of constant returns to scale becomes appropriate only if all hospitals operate at
an optimal scale which is not usually the case. Technical efficiency is decomposed into pure
technical efficiency3 and scale efficiency4 if hospitals are not operating at optimal scale. To
capture the effects of scale efficiency, Banker, et al., (1984) proposed an extension of the
original CRS DEA model to account for the variations in returns to scale. The problem now to
be solved becomes;
is either (1.2)
Notations remain the same as in equation 1.1. is an unconstrained in sign intercept
determining the returns to scale. If it indicates increasing returns to scale5, if it
indicate constant returns to scale and if it indicates decreasing returns to scale6.
3 Pure technical efficiency is a situation whereby with a given level of technology, a hospital cannot produce more
output from the same inputs.
4 Scale efficiency refers to the appropriate (optimum) size of a hospital. If a hospital is small for its volume of
activities, it depicts economies of scale (corresponding to increasing returns to scale in production) while if it is too
large for its scale of operation it depicts diseconomies of scale (corresponding to decreasing returns to scale in
production).
5 Increasing returns to scale in production occurs if a proportionate increase in all inputs under the control of a
hospital results in a greater than proportionate increase in output. Increasing returns to scale usually emerge for
relatively small levels of production (hospital size being too small for its scale of operation)

19
Masiye (2007) stated that Scale efficiency (SE) is obtained by dividing a hospital’s technical
efficiency (TE) score assuming constant returns to scale (CRS) by the corresponding technical
efficiency score under variable returns to scale (VRS).
(1.3)
3.2 Stochastic Frontier Analysis (SFA)
Stochastic Frontier Analysis (SFA) was proposed by Aigner, Lovell and Schmidt (1977). SFA
considers the measurement errors and a functional form which reflects the properties
underlying a production technology. According to Heidenberger (2002), SFA is a statistical
technique which generates a stochastic error term and an inefficiency term using residuals
from an estimated production or cost frontier. SFA may be estimated by maximum likelihood
where a panel model with fixed effects is estimated. From the ideas of Owino and Korir
(1997), a Cobb Douglas functional form of a cost function will be assumed in this study. The
choice of the use of a cost function was dictated by the fact that use of a production function
would require estimation for the production function for each output and also because of the
multi-product nature of hospital output.
The model to be estimated is expressed as;
The stochastic cost frontier is expressed as;
6 Decreasing returns to scale in production occurs if a proportionate increase in all inputs under the control of a
hospital results in a less than the proportionate increase in output. Decreasing returns to scale usually emerge for
relatively high levels of production (Maddala and Ellen, 1989).

20
Where natural logarithm of annual recurrent expenditure of the ith hospital
=constant
=parameters to be estimated
=random (stochastic) variables assumed to be iid and independent of
= random variable which is non-negative accounting for inefficiency in production
and assumed to be iid . According to Coelli (1996), this is the distance from the cost
frontier or the degree of inefficiency. The common assumption is that is normally distributed
while is represented by a half normal distribution. When allocative efficiency is assumed
then defines the cost of technical inefficiency.
3.3 Malmquist Productivity Index
Malmquist Total Factor Productivity7 (TFP) is used to measure productivity change and to
decompose this productivity into technical change and technical efficiency change (Coelli,
1994). Fare, et al. (1992), using period t benchmark technology, specified output oriented
malmquist productivity index for period t as;
(1.5)
Where D represents the output distance function; the Mo is the output oriented malmquist
productivity index; and y and x are outputs and inputs respectively.
Fare, et al. (1992), used the period t+1 technology to specify the output oriented malmquist
productivity index for period t+1 as;
7 Total Factor Productivity is the ratio of actual output to the optimal value as specified by a production function.

21
(1.6)
Consequently, Fare, et al., (1992) conventionally defined the malmquist productivity index as a
geometric mean of the two as;
(1.7)
(1.8)
Fare, et al., (1992) decomposed equation 1.8 by extracting the term from the
right side to yield;
(1.9)
The first term on the right hand side of equation 1.9 defines the productivity change8 due to
technical efficiency while the second term defines the productivity change due to technical
change (measures shift due to technological difference between period t and t+1).
3.4 Tobit Regression Analysis
The tobit regression analysis will be used to identify factors affecting hospital efficiency. The
tobit regression will relate the efficiency scores (dependent variable) to a number of
explanatory variables. Explanatory variables will include medical staff, other staff, number of
beds and cots, outpatient visits, inpatient visits and MCH/family planning visits.
8Productivity Change is defined as a ratio of output growth to input growth, (yt+1/yt)/(xt+1/xt). It can
be as a result of efficiency change, technical change, scale economies and environmental factors
which may affect production.

22
The tobit regression (censored normal regression) estimates a linear relationship in case of a
censoring in the dependent variable. Zere (2000) proposed a censoring point at zero for
computational convenience and transformed DEA efficiency scores into inefficiency scores,
left-censored at zero using the formula below;
(2.0)
According to Woodridge (2002), the tobit structural equation is specified as:
where . is an observable latent variable for values greater than 0
but censored otherwise.
(2.1)
is observed inefficiency score, is a K X 1 vector of explanatory variables and is a vector
of parameters. is a column vector of disturbances.
The empirical models will take the following forms;
Where ineff=inefficiency, ALOS=average length of stay, Deliveries=births attended by skilled
health staff, ANC=antenatal clinic visits, malaria=number of under 5 years treated from
malaria, beds=number of beds and cots, doctors=number of doctors, nurses=number of nurses
and reccexp=recurrent expenditure.
Equation 2.2 will be estimated using DEA technical efficiency scores while equation 2.3 will be
estimated using SFA cost efficiency scores. The choice of tobit regression was based on the
assumption that the dependent variable (inefficiency) clusters towards the left limit, that is,

23
zero (left-censored at zero). Tobit regression provides consistent estimates and uses all
information including information on censoring as opposed to logit and probit analysis.
STATA will be used to do the tobit regression analysis to determine the statistical significance of
the coefficients of the explanatory variables.
3.5 Data and Variables
The study intends to use secondary data from the Ministry of Medical Services for the years
2008 to 2011. This period of time was chosen because it had a significant budgetary allocation
increment. The data to be used was collected by the above Ministry for their administrative
use. The study will use process approach as opposed to outcomes approach in measurements of
output. Health care delivery points in Kenya rarely collect information on health outcomes, for
example, the DALYs, QALYs, HLYs, and life expectancy at birth.
In this study, an input oriented technical efficiency will be used. According to Kengil, et al.
(2010), input-orientation focuses on reducing amounts of input used for a given output.
The inputs in this study will be classified as number of doctors, number of nurses and number
of beds and cots. Number of doctors and nurses constitute the labour component while capital
is proxied by the number of beds and cots.
Outputs will be classified as number of antenatal clinic visits, average length of stay, number
of births attended by skilled health staff and the number of under 5 years treated from malaria.
The selection of inputs and outputs for this study was prompted by previous efficiency
measurement studies done in the African region and conceptual model of healthcare
production.
The analysis of hospitals will be in two categories grouped into level 5 (provincial) hospitals to
be analyzed distinctively and level 4 (district and sub-district) hospitals to be analyzed as per
province. The study will use DEAP Version 2.1 computer program developed by Professor Tim
Coelli (1994) to calculate efficiencies and Malmquist Factor Productivity. The study will also

24
use Stochastic Frontier Version 4.1 computer program to obtain maximum likelihood estimates
of the stochastic cost function also developed by Professor Tim Coelli.

25
CHAPTER FOUR
EMPIRICAL RESULTS
4.1 Introduction
This chapter presents the empirical results and data analyses from malmquist data
envelopment analysis, stochastic frontier analysis and tobit regression. The analysis comprises
Level 5 provincial public general hospitals and provincial analysis of level 4 public hospitals
respectively.
4.2 Descriptive Statistics and Correlation Matrix of variables-Level 5 public hospitals
Table 1 and 2 presents the summary statistics and correlation matrix respectively for the
outputs and inputs used in the seven (7) provincial (level 5) public general hospitals.
Table 1: Descriptive Statistics of variables-Level 5 public hospitals.
Variable Mean Std. Dev. Min. Max.
Average Length of Stay 6.892857 2.02465 4 12
No. of deliveries attended by skilled health staff
11713.82 7714.008 1189 32105
Antenatal Clinic Visits 8745.893 4703.494 1635 21981
Under 5 yrs treated for malaria 128106.4 196024.1 8705 959194
No. of beds 431.0357 137.8269 162 715
No. of doctors 31.92857 18.6089 7 86
No. of nurses 268.2857 104.0715 93 486
Source: Author’s computation
Table 2: Correlation Matrix of variables- Level 5 public hospitals.
Variable Average Length of Stay
No. of Deliveries attended by skilled health staff
ANC Under 5 yrs malaria treated
beds doctors nurses
Average Length of Stay
1
No. of Deliveries attended by skilled health staff
0.0218 1
ANC 0.1269 0.6517 1

26
Under 5 yrs malaria treated
0.3562 0.1959 0.0925 1
beds 0.1042 0.5409 0.5579 0.1283 1
doctors 0.3999 0.5201 0.5675 0.0207 0.6048 1
nurses 0.4649 0.4841 0.5585 0.0918 0.7106 0.7787 1
Source: Author’s computation
4.3 Technical Efficiency Analysis (Data Envelopment Analysis) of Level 5 (provincial and regional) hospitals in Kenya
The estimation of the technical efficiency scores assumed Variable Returns to Scale (VRS) using
data envelopment analysis. The average annual technical efficiency score of the Level 5
(provincial) public hospitals in Kenya was 95.75% between 2008 and 2011as shown in Table
3. The results indicate that, out of a population of seven public general hospitals, only two
(Embu PGH and Nakuru PGH) were found to operate below the average technical efficiency
score. Only two provincial hospitals (Garissa PGH and Nyeri PGH) were technically efficient
between 2008 and 2011. Results further showed that all the provincial general hospitals were
technically efficient in 2010. To measure technical efficiency change, a Malmquist DEA was
estimated whose results are presented in Table 4.
Table 3: Technical Efficiency Scores of Provincial (Level 5) Public Hospitals in Kenya.
Year Coast PGH Embu PGH Nakuru PGH Garissa PGH Nyeri PGH Nyanza PGH Kakamega PGH All Hospitals
2008 1 1 1 1 1 1 0.917 0.988
2009 1 1 1 1 1 0.828 1 0.975
2010 1 1 1 1 1 1 1 1
2011 0.864 0.433 0.774 1 1 1 1 0.867
Average 0.966 0.85825 0.9435
1
1 0.957 0.97925 0.9575
Source: Author’s computation

27
Table 4: Malmquist Index Summary of Level 5 Hospitals in Kenya.
Source: Author’s computation
It is evident that the total technical efficiency decreased by 5.2%. The decline was due to the
fact that the 0.01% increase in scale efficiency was very minimal to absorb the 5.3% decline in
pure technical efficiency. Total factor productivity declined by 13.3% probably as a result of
the 8.5% decline in technological change and 5.2% decline in total technical efficiency change.
The results reflects that technological innovations were very minimal if any and that the
managerial ability to order inputs in the production process is very poor as reflected by the
decline in the technical efficiency.
4.4 Cost Efficiency Analysis (Stochastic Frontier Analysis) of Level 5 (provincial) hospitals in Kenya
The cost efficiency of the provincial general hospitals in Kenya was estimated using the
Stochastic Frontier Analysis. The Cobb-Douglas cost function was estimated using Frontier 4.1
computer program for stochastic frontier cost function estimation. The estimated coefficients of
the Cobb-Douglas cost function are presented in Table 5 below;
Hospital Total Technical
Efficiency
Change
Technological
Change
Pure Technical
Efficiency Change
Scale Efficiency
Change
Total Factor
Productivity
Change
Coast PGH 0.949 0.887 0.952 0.996 0.842
Embu PGH 0.757 0.811 0.757 1 0.613
Nakuru PGH 0.911 1.019 0.918 0.992 0.928
Garissa PGH 1 0.793 1 1 0.793
Nyeri PGH 1 0.001 1 1 1.001
Nyanza PGH 1 0.755 1 1 0.755
Kakamega PGH 1.05 1.22 1.029 1.02 1.281
Mean 0.948 0.915 0.947 1.001 0.867

28
Table 5: Estimated Coefficients of the Cobb Douglas Cost Function for level 5 public hospitals.
Variable Coefficient Standard Error t-ratio
Constant 13.51073 1.70578 7.92055
Average length of stay -0.00856297 0.273024 0.0313629
Deliveries attended by skilled
health staff
-0.0629646 0.113301 -0.55572409
Ante Natal Clinic Visits -0.04051847 0.2300692 -0.17611422
Under 5yr treated from malaria -0.04428995 0.0732567 -0.6045849
Beds + cots 0.30908912 0.4823801 0.64075383
Doctors 0.07414333 0.16454345 0.45060028
Nurses 0.37524638 0.36094199 1.0396307
Sigma squared 0.7210097 0.97035431 0.74303756
Gamma 0.89692037 0.14878274 6.02839
MU 0.42670147 1.1466786 0.3721195
Eta -1.0036324 0.31622142 -3.1738279
Number of observations 28
LR test of the one sided error 14.596465
Source: Author’s computation
Results from table 5 shows that none of the coefficients is significant.
Table 6: Cost Efficiency Scores (Stochastic Frontier Analysis) for Level 5 (provincial and
regional) hospitals in Kenya.
PGH 2008 2009 2010 2011 Average
Coast 0.99075 0.97485 0.93203 0.8195629 0.929298
Embu 0.92986 0.819772 0.5800458 0.2221377 0.637954
Nakuru 0.9352 0.832684 0.6053058 0.24953893 0.655682
Garissa 0.98822 0.9680387 0.914083 0.77532746 0.911417
Nyeri 0.98345 0.95528 0.881145 0.6988103 0.879671
Nyanza 0.958 0.8892479 0.7241789 0.407002 0.744607

29
Kakamega 0.938123 0.83979859 0.61951938 0.26585107 0.665823
Average 0.96051471 0.897095884 0.750901126 0.491175766 0.77492187
Source: Author’s computation
From Table 6 above, the average cost efficiency of Level 5 (provincial and regional) public
hospitals in Kenya is 77.49%. The highest average cost efficiency score is 92.9% (Coast PGH)
while the lowest is 63.79% (Embu PGH). Four (4) provincial general hospitals (Embu, Nakuru,
Kakamega and Nyanza) have cost efficiency scores below the average cost efficiency score. It is
also evident that the annual average cost efficiency scores continues to decline from year 2008
(96.05%) to 2011 (49.11%). The annual cost efficiency scores for individual provincial
general hospitals continue to decline from 2008 to 2011. This decline calls for remedial
measures by looking at some the possible determinants of inefficiency.
4.5 Determinants of Efficiency in Level 5 (provincial and regional) public hospitals in Kenya
Firstly, a tobit regression is run using the DEA technical efficiency scores as the dependent
variable. This helps to determine the statistical significance of the coefficients of the
explanatory variables likely to influence efficiency.
Table 7: Results from Tobit Regression using DEA Technical Efficiency Scores.
0 right-censored observations 27 uncensored observations Obs. summary: 1 left-censored observation at efficiency<=.2221377 /sigma .1654528 .0228278 .1179798 .2129259 _cons 1.380888 .166073 8.31 0.000 1.03552 1.726256 nurses .000643 .0006247 1.03 0.315 -.0006562 .0019421 doctors -.0007664 .0029819 -0.26 0.800 -.0069675 .0054348 beds -.000878 .0003806 -2.31 0.031 -.0016695 -.0000864 yrsmalaria 1.87e-07 1.92e-07 0.97 0.341 -2.12e-07 5.86e-07 anc -.0000235 9.81e-06 -2.40 0.026 -.0000439 -3.14e-06 deliveries 7.75e-07 6.08e-06 0.13 0.900 -.0000119 .0000134 alos -.0296863 .0224827 -1.32 0.201 -.0764416 .017069 efficiency Coef. Std. Err. t P>|t| [95% Conf. Interval]
Log likelihood = 8.7258617 Pseudo R2 = 7.8129 Prob > chi2 = 0.0055 LR chi2(7) = 20.01Tobit regression Number of obs = 28

30
From Table 7, antenatal clinic visits and number of beds are the only variables with significant
coefficients at 5% level of significance. The results indicate that increases in antenatal clinic
visits and number of beds will lead to a decline in technical efficiency in the provincial general
public hospitals in Kenya.
By use of cost efficiencies from the Stochastic Frontier Analysis, the tobit regression results are
presented in table 8 below:
Table 8: Results of Tobit regression using SFA Cost Efficiency Scores.
0 right-censored observations 27 uncensored observations Obs. summary: 1 left-censored observation at efficiency<=.2221377 /sigma .086377 .011717 .0619357 .1108184 _cons 1.145307 .0910432 12.58 0.000 .955394 1.33522 nurses .000656 .0003295 1.99 0.060 -.0000313 .0013433 doctors -.0009017 .001582 -0.57 0.575 -.0042017 .0023983 beds .0000294 .0002266 0.13 0.898 -.0004433 .0005022 yrsmalaria 1.04e-07 1.01e-07 1.03 0.315 -1.06e-07 3.15e-07 anc -.0000135 5.82e-06 -2.32 0.031 -.0000256 -1.35e-06 deliveries -2.23e-06 3.23e-06 -0.69 0.497 -8.96e-06 4.50e-06 alos -.0220516 .0119228 -1.85 0.079 -.0469221 .0028189recurrentexp -1.25e-08 1.84e-09 -6.80 0.000 -1.64e-08 -8.68e-09 efficiency Coef. Std. Err. t P>|t| [95% Conf. Interval]
Log likelihood = 27.679109 Pseudo R2 = 22.6112 Prob > chi2 = 0.0000 LR chi2(8) = 57.92Tobit regression Number of obs = 28
From Table 8, the coefficients on recurrent expenditure, average length of stay, antenatal clinic
visits and number of nurses are statistically significant at 10% level of significance. The results
indicate that increases in recurrent expenditure, average length of stay and antenatal clinic
visits are found to reduce cost efficiency while increases in number of nurses is found to
increase cost efficiency in the provincial general public hospitals in Kenya.
4.6 Analysis of Efficiencies of Level 4 public hospitals in Kenya
The technical and cost efficiencies of level 4 public hospitals were analyzed per province using
DEA and SFA respectively. Tables 12 and 13 present the descriptive statistics and the
correlation matrix of variables respectively.

31
Table 9: Descriptive statistics of variables (DEA) for Level 4 public hospitals.
Variable Mean Std. Dev. Min Max
Alos 6.71875 2.642511 2 13
Deliveries attended by skilled health staff
63944.88 32075.85 11511 145667
Anc 83333.88 50864.91 10092 215678
Malaria 464435 302989..9 17263 1040448
Beds 3162.375 2552.772 380 11904
Doctors 155.1875 118.3389 19 422
Nurses 1801.5 1196.028 223 4159
Source: Author’s computation
Table 10: Correlation matrix of variables (DEA) for Level 4 public hospitals.
nurses 0.3443 0.7697 0.4948 0.3786 0.7239 0.7082 1.0000 doctors 0.1801 0.5934 0.2414 0.1963 0.4010 1.0000 beds 0.3860 0.5957 0.2105 0.4128 1.0000 malaria 0.1505 0.4567 0.3493 1.0000 anc 0.0542 0.6285 1.0000 deliveries 0.1457 1.0000 alos 1.0000 alos delive~s anc malaria beds doctors nurses
The technical efficiency scores of Level 4 public hospitals per province from data envelopment
analysis are as presented in table 11 below:
Table 11: Technical Efficiency Scores of Level 4 public hospitals estimated using DEA.
Year Central
Province
Rift Valley
Province
Nyanza
Province
Eastern
Province
Coast
Province
North
Eastern
Province
Nairobi
Province
Western
Province
All Provinces
2008 0.833 1 1 1 0.86 1 1 1 0.962
2009 0.806 1 1 1 1 1 1 1 0.976
2010 1 1 1 1 1 1 1 1 1
2011 1 1 1 0.92 0.849 1 1 1 0.971
Average 0.90975 1 1 0.98 0.92725 1 1 1 0.97725
Source: Author’s computation
Results from Table 11 shows that five provinces out of eight were technically efficient. The
average technical efficiency score for the period 2008-2011 was 97.72%. In the year 2010, all

32
the provinces were technically efficient. The lowest technical efficiency score was 90.97%. The
technically inefficient provinces had a technical efficiency score of 93.9%. This was an
improvement from the study by Kirigia et. al (2002) in Kenya which showed that out of the 54
public hospitals which had been analyzed the inefficient public hospitals had a technical
efficiency score of 84%.
To estimate the technical efficiency change, a Malmquist DEA was conducted and the results
are presented in Table 12 below:
Table 12: Malmquist Index Summary of level 4 public hospitals provincial means.
Province Total
Efficiency
Change
Technological
Change
Pure Technical
Efficiency
Change
Scale Efficiency
Change
Total Factor
Productivity
Change
Central 1.221 0.602 1.063 1.149 0.736
Rift Valley 1.173 0.656 1 1.173 0.77
Nyanza 0.985 0.745 1 0.985 0.734
Eastern 0.911 0.626 0.973 0.936 0.57
Coast 0.996 0.68 0.996 1 0.677
North Eastern 1 0.833 1 1 0.833
Nairobi 1 0.596 1 1 0.596
Western 1 0.648 1 1 0.648
Average 1.031 0.669 1.004 1.028 0.69
Source: Author’s computation
Results from Table 12 shows that total efficiency change increased by 3.1% as a result of a
0.4% increase in pure technical efficiency and 2.8% increase in scale efficiency. However, the
total factor productivity declined by 31% which was as a result of a decline in technological
changes by 33.1%. This means that investment in technological innovations have been very
low if any impacting negatively on the total factor productivity.

33
4.7 Cost Efficiency Analysis (Stochastic Frontier Analysis) of level 4 public hospitals
The parameters of the Cobb-Douglas cost function were estimated together with the cost
efficiencies using the Frontier 4.1 computer program and the results are presented in Tables 13
and 14 respectively.
Table 13: The estimated parameters of the Cobb Douglas Cost Function for level 4 public
hospitals.
Variable Coefficient Standard Error t-ratio
Constant 11.90767 1.083327 10.99176
Average length of stay -0.30325 0.168213 -1.8028
Deliveries attended by skilled
health staff
-0.39754 0.195741 -2.03096
Ante Natal Clinic Visits 0.475149 0.147566 3.219909
Under 5yr treated from malaria 0.519417 0.09358 5.550536
Beds + cots -0.16794 0.130886 -1.28313
Doctors 0.256994 0.135594 1.895324
Nurses -0.05919 0.159349 -0.37144
Sigma squared 0.091892 0.027259 3.371059
Gamma 0.097286 0.084856 1.146481
MU 0.189101 0.094697 1.996905
Eta 0.395965 0.145664 2.718353
Number of observations 32
LR test of the one sided error 10.41215
Source: Author’s computation

34
Table 14: Level 4 public hospitals cost efficiency scores (SFA).
Province 2008 2009 2010 2011 Average
Central 0.44113 0.5784948 0.6929587 0.78181217 0.623599
R. Valley 0.3592258 0.50380869 0.631397 0.7343599 0.557198
Nyanza 0.4142309 0.55441988 0.673415 0.766902 0.602242
Eastern 0.44448517 0.58177475 0.6956 0.7838168 0.626419
Coast 0.42693 0.5658949 0.6827641 0.774052 0.61241
N. Eastern 0.533652 0.65768139 0.7553695 0.8285291 0.693808
Nairobi 0.6736447 0.76899066 0.8391676 0.8892645 0.792767
Western 0.6391855 0.8594635 0.90398046 0.934727 0.834339
Average 0.491561 0.633816 0.734332 0.811683 0.667848
Source: Author’s computation
The results from table 13 show that the coefficients on deliveries attended by skilled health
staff, antenatal clinic visits and under 5 years treated from malaria were significant. The
average cost efficiency of level 4 public hospitals in Kenya is 66.78% as presented in table 14.
Rift Valley province had the least cost efficiency of 55.71% compared to Western province
which had the highest cost efficiency score of 83.43%.
Five (5) provinces out of a population of eight (8) have their cost efficiencies below the average
cost efficiency score. These are Central (62.35%), Rift Valley (55.71%), Nyanza (60.22%),
Eastern (62.64%) and Coast (61.24%). The results indicate that the annual average cost
efficiencies of level 4 public hospitals continues to rise from 2008 (49.15%) to 2011 (81.16%).
This has a reverse trend as compared to the level 5 public general hospitals. Health managers
should be aware of the factors that are behind the efficiency improvement.

35
4.8 Determinants of Efficiency in Level 4 public hospitals
Firstly, the tobit regression analysis was run using the DEA technical efficiency scores and the
results are as presented in table 15.
Table 15: Tobit Regression using DEA Technical Efficiency Scores-level 4 public hospitals.
0 right-censored observations 31 uncensored observations Obs. summary: 1 left-censored observation at technicale~y<=.80599999 /sigma .0472515 .006062 .0347665 .0597365 _cons .9525392 .0295527 32.23 0.000 .8916744 1.013404 nurses -.0000144 .0000168 -0.85 0.402 -.000049 .0000203 doctors -.0002694 .0001131 -2.38 0.025 -.0005024 -.0000364 beds 3.49e-06 5.72e-06 0.61 0.547 -8.29e-06 .0000153 malaria 6.99e-09 3.27e-08 0.21 0.832 -6.03e-08 7.43e-08 anc 9.93e-08 2.45e-07 0.41 0.689 -4.05e-07 6.04e-07 deliveries 6.57e-07 5.17e-07 1.27 0.215 -4.07e-07 1.72e-06 alos .0040312 .0035975 1.12 0.273 -.0033779 .0114404 technicale~y Coef. Std. Err. t P>|t| [95% Conf. Interval]
Log likelihood = 49.305159 Pseudo R2 = -0.1415 Prob > chi2 = 0.0935 LR chi2(7) = 12.22Tobit regression Number of obs = 32
. tobit technicalefficiency alos deliveries anc malaria beds doctors nurses, ll
Results from table 15 shows that the only coefficient which is significant is for doctors,
however it exhibits a negative sign.
The tobit regression analysis using SFA cost efficiency scores is as presented in table 16. The
results show that the coefficients on recurrent expenditure, deliveries attended by skilled
health staff, antenatal clinic visits, number of under 5 years treated from malaria and number
of doctors are significant at 5% level of significance. The results indicate that increases in
antenatal clinic visits, number of under 5 years treated from malaria and number of doctors
will raise the cost efficiency while increases in recurrent expenditure and number of deliveries
will decrease the cost efficiency.

36
Table 16: Results from Tobit regression SFA Analysis-level 4 public hospitals.
.
0 right-censored observations 31 uncensored observations Obs. summary: 1 left-censored observation at costeffici~y<=.35922581 /sigma .0777312 .0099369 .0572225 .09824 _cons .8038417 .0511834 15.71 0.000 .6982043 .9094791 nurses .0000303 .0000283 1.07 0.295 -.0000281 .0000888 doctors .0004407 .0001927 2.29 0.031 .0000429 .0008385 beds -8.56e-06 .0000104 -0.82 0.419 -.0000301 .0000129 malaria 2.76e-07 6.73e-08 4.10 0.000 1.37e-07 4.15e-07 anc 2.64e-06 5.76e-07 4.59 0.000 1.46e-06 3.83e-06 deliveries -2.80e-06 9.03e-07 -3.10 0.005 -4.67e-06 -9.37e-07 alos -.0084186 .0062202 -1.35 0.189 -.0212566 .0044193 recurrent -1.81e-09 2.21e-10 -8.17 0.000 -2.26e-09 -1.35e-09 costeffici~y Coef. Std. Err. t P>|t| [95% Conf. Interval]
Log likelihood = 34.157047 Pseudo R2 = -1.8354 Prob > chi2 = 0.0000 LR chi2(8) = 44.22Tobit regression Number of obs = 32
4.9 Conclusion
The empirical results obtained from DEA on technical efficiency ranged from 85.82% to 100%
for level 5 public general hospitals and from 90.97% to 100% provincial analysis for the level
4 public hospitals. In addition, the empirical results obtained from SFA on cost efficiency
ranged from 63.79% to 92.92% for level 5 public general hospitals and from 55.71% to
83.83% provincial analysis for the level 4 public hospitals.
Malmquist DEA analysis confirmed that technological innovations are very minimal if any.
This was mostly the cause of the decline in the total factor productivity. Determinants of
efficiency were determined from the tobit regression analysis. Increases in antenatal clinic
visits were found to reduce technical efficiency and cost efficiency for level 5 public general
hospitals while they increased cost efficiency in level 4 public hospitals. Increases in recurrent
expenditure were found to reduce cost efficiency in both level 4 and level 5 public hospitals.
Increases in number of nurses was found to increase cost efficiency in level 5 public general
hospitals while increases of doctors increased cost efficiency in level 4 public hospitals.

37
CHAPTER FIVE
SUMMARY, POLICY RECOMMENDATIONS AND CONCLUSIONS
5.1 Summary
Estimation of efficiency is vital in provision of healthcare. It is one of the measures to
supplement the domestic resources in health financing through efficiency savings. Efficiency
use of health resources should be a key concern in the budgeting process in Kenya. This study
estimated the technical and cost efficiencies of level 4 and 5 public hospitals in Kenya from
2008 to 2011 and tried to identify some of the determinants of (in)efficiency.
It is evident from literature reviewed that inefficiency is a major challenge in all African
countries as it affects productivity and slows the health sector from attaining the Millenium
Development Goals. Various studies showed that inefficiencies compromises access to quality
health care. Emphasis has been put to the policy makers and health managers to take
cognizance of the optimal health input mix and technological advancement.
This study analyzed technical efficiency by use of data envelopment analysis while stochastic
frontier analysis was used to measure cost efficiency. Tobit regression analysis was used to
identify factors causing (in)efficiency. Level 5 public general hospitals had an average
technical efficiency score of 95.75% and an average cost efficiency score of 77.49% while
Level 4 public hospitals’ provincial analysis revealed an average technical efficiency score of
97.72% and an average cost efficiency score of 66.78%.
The total factor productivity for level 4 and 5 public hospitals in Kenya seemed to be negatively
affected by low levels of technological innovations. An increase in recurrent expenditure was
found to reduce cost efficiency which calls for further research.

38
5.2 Policy Recommendations
This study has demonstrated that technical change through technological innovations is
impacting negatively to the total factor productivity of level 4 and 5 public hospitals in Kenya.
The malmquist total factor productivity for level 4 and 5 public hospitals in Kenya for the
period 2008 to 2011 was less than 100% which was mostly due to a decline in technological
advancement. Investment in technological innovations is therefore a key recommendation to
policy makers and health managers.
This study recommends further research on why increases in recurrent expenditure results in
decreasing cost efficiency in level 4 and 5 public hospitals. It is therefore imperative for the
policy makers and health managers to consider efficiency use of the recurrent budget.
5.3 Conclusion
This study confirms that inefficiency remains a major challenge in the health sector in Kenya
despite the recent reforms in the health sector. This study revealed an average inefficiency level
of 22.51% for level 5 public general hospitals and 33.22% for level 4 public hospitals. These
results do not differ much from the study results by Owino and Korir (1997) in Kenya which
found an average inefficiency level of 30% in the public health sector. This study shows that
there is potentiality for productivity growth in health sector in Kenya by considering efficiency
and investments in technological innovations.
5.4 Limitations of the Study
Firstly, this study estimated efficiency of public hospitals in Kenya by considering four output
variables and three input variables due to accessibility and availability of data. These variables
do not include all the variables in the health sector.

39
Secondly, the study did not consider cultural, social and behavioral characteristics of the health
personnel which can affect productivity. Thirdly, the study relied on secondary data whose
correctness could not be verified and authenticated. Lastly, the study used process approach as
opposed to outcomes approach in measurements of output due to the fact that health care
delivery points in Kenya rarely collect information on health outcomes.

40
References
Aigner, D. J., Lovell, C. A. K., and Schimdt, P., 1977. Formulation and Estimation of Stochastic
Frontier Production Function Models. Journal of Econometrics, 6, 21-37.
Akazili, J., Adjuik, M., Jehu-Appiah, C., and Zere, E., 2008. Using data envelopment analysis to
measure the extent of technical efficiency of public health centres in Ghana. BMC
international health and human rights, 8, 11.
Banker, R. D., Charnes, A., and Cooper, W. W., 1984. Some models for estimating technical
and scale inefficiencies in data envelopment analysis. Management Science, 30(9), 1078-
1092.
Central Bureau of Statistics, Ministry of Health [Kenya] and ORC Macro (2004). Kenya
Demographic and Health Survey 2003. Calverton, Maryland: CBS, MOH, and ORC Macro.
Charnes, A., Cooper, W. W. and Rhodes, E., 1978. Measuring the efficiency of decision making
units. European Journal of Operational Research, 2, 429-444.
Coelli, T., 1994. A Guide to DEAP Version 2. 1: A Data Envelopment Analysis (Computer)
Program. Frontiers: A Journal of Women Studies, 1-49.
Coelli, T. J., 1996. A Guide to Frontier Version 4. 1: A Computer Program for Stochastic
Frontier Production and Cost Function Estimation. CEPA Working Paper 96/07. University of
New England.
Coelli T. J., Rao, D.S.P., O’Donnell, C. J., and Battesse, G. E., 2005. An Introduction to Efficiency
and Productivity Analysis. 2nd edition. Springer Science and Business Media, inc., Newyork.
Fare, R., Grosskopf, S., Lindgren, B., and Roos, P., 1992. Productivity Changes in Swedish

41
Pharmacies 1980-1989: A non-parametric Malmquist Approach. Journal of productivity
analysis 3:1/2 pp. 85-101.
Farrell, M. J., 1957. The measurement of productive efficiency. Journal of the Royal Statistical
Society. Series A (General), Vol. 120, No. 3 pp. 253-290.
Government of Kenya, 2009a. Annual Health Sector Statistics Report 2008, Division of Health
Management Information Systems.
Government of Kenya, 2009b. Health Sector Strategic Plan for Health Information System
2009-2014
Government of Kenya, 2009c. Kenya National Health Accounts 2009/10.
Health Sector Working Group, 2012. MTEF for 2012/13-2014/15. Ministry of Medical
Services and Ministry of Public Health and Sanitation.
Heindenberger, K., 2002. Alternative Methods to Examine Hospital Efficiency-Data
Envelopment Analysis and Stochastic Frontier Analysis. Stefan Staevski.
Kengİl, B. Ç., Gokmen N., and Tozan, H., 2010. Efficiency measures in the health services with
DEA - An Overview. Journal of Naval Science and Engineering, 6(1), 1-14.
Kenya National Bureau of Statistics (KNBS) and ICF Macro. (2010). Kenya Demographic and
Health Survey 2008-09. Calverton, Maryland: KNBS and ICF Macro.
Kirigia, J. M., Emrouznejad, A., and Sambo, L. G., 2002. Measurement of technical efficiency of
public hospitals in Kenya: using Data Envelopment Analysis. Journal of medical systems, 26(1),
39-45.

42
Kirigia, J. M., Emrouznejad, A., Sambo, L. G., Munguti, N., and Liambila, W., 2004. Using data
envelopment analysis to measure the technical efficiency of public health centers in Kenya.
Journal of medical systems, 28(2), 155-66.
Kirigia, J. M., Sambo, L. G., Renner, A., Alemu, W., Seasa, S., and Bah, Y., 2011. Technical
efficiency of primary health units in Kailahun and Kenema districts of Sierra Leone.
International archives of medicine, 4(i), 15.
Maddala, G. S., and Ellen, M., 1989. Microeconomics: Theory and Applications. McGraw-Hill,
Newyork.
Marc, L., Doherty, J., Muchiri, S., Barasa T., Hofler, K., Maniscalco, L., Ouma, C., Kirika, R. and
Maundu, J., 2010. Kenya Health System Assessment 2010. Bethesda, MD: Health Systems
20/20 project, Abt Associates Inc.
Masiye, F., 2007. Investigating health system performance: An application of data envelopment
analysis to Zambian hospitals. BMC health services research, 7, 58.
Moshiri, H., Aljunid, S. M., and Amin, R. M., 2010. Hospital Efficiency: Concept, measurement
Techniques and Review of Hospital Efficiency Studies. Malaysian Journal of Public Health
Medicine, Vol.10 (2) pp 35-43
National Economic and Social Council of Kenya, 2010. Draft Strategy on Accessible, Affordable
and Quality Healthcare Services in Kenya-Financing Options for Universal Coverage. Vol. 4.
Osei, D., d’ Almeida, S., George, M. O., Kirigia, J. M., Mensah, A. O., and Kainyu, L. H., 2005.
Technical efficiency of public district hospitals and health centres in Ghana: a pilot study. Cost
effectiveness and resource allocation: C/E, 3, 9.

43
Owino, W., and Korir, J., 1997. Public Health Sector Efficiency in Kenya: Estimation and Policy
Implications. Discussion Paper No. DP/007/97. Nairobi. Institute of Policy Analysis and
Research
Rakuom, C., 2010. Nursing Human Resources in Kenya: Case Study. International Centre for
Human Resources in Nursing.
Republic of Kenya, (2007). The Kenya Vision 2030.
Sealy, S., and Rosbach, K., 2010. Kenya Health Sector Budget Analysis. Estimated Government
Spending 2010/11. gtz
Tlotlego, N., Nonvignon, J., Sambo, L. G., Asbu, E. Z., and Kirigia, J. M., 2010. Assessment of
productivity of hospitals in Botswana: A DEA application. International archives of medicine, 3,
27.
UNICEF, 2007. Social Budgeting Investments in Kenya’s Future. Government of Kenya/UNICEF
Programme of Cooperation 2004-2008. Working Paper No.2.
Wooldridge, J. M., 2002. Econometric Analysis of Cross-Section and Panel Data, MIT Press,
Cambridge.
Zere, E., Mbeeli, T., Shangula, K., Mandlhate, C., Mutirua, K., Tjivambi, B., and Kapenambili,
W., 2006. Technical efficiency of district hospitals: Evidence from Namibia using data
envelopment analysis. Cost effectiveness and resource allocation: C/E, 4, 5.
Zere, E., 2000. Hospital Efficiency in Sub-Saharan Africa: Evidence from South Africa. World
Institute for Development Economics Research (WIDER), Working Paper No. 187.

44
Appendices
Table 17: Number of health facilities by type
Province Dispensary Health Centre
Hospital Medical Clinic
Nursing Home
Grand Total
Central 397 67 57 654 24 1199
Coast 253 42 41 368 19 723
Eastern 555 91 61 218 17 942
Nairobi 147 69 43 109 19 387
North Eastern
113 11 21 45 8 198
Nyanza 405 132 86 64 29 716
Rift Valley
1076 210 102 234 26 1648
Western 194 73 35 58 17 377
Grand Total
3140 695 446 1750 159 6190
Source: GoK 2009a
Table 18: Number of health facilities by ownership
Province Community FBO GoK Local
Authority
NGO Private Grand Total
Central 7 146 356 - 7 683 1199
Coast 12 35 231 23 7 415 723
Eastern 3 160 552 - 6 221 942
Nairobi 3 61 69 37 28 189 387
North
Eastern
- 3 137 - 4 54 198
Nyanza 8 104 471 9 16 108 716
Rift Valley 54 238 959 11 26 360 1648
Western 20 55 224 - 3 75 377
Grand Total 107 802 2999 80 97 2105 6190
Source: GoK 2009a