
NTP Network Time Protocol Nóirín Plunkett Network Time Protocol Nóirín Plunkett.

Analgesic Ladder in TBI Analgesic Ladder in TBI Pain ManagementPain Management
Jim Plunkett, M.D.Jim Plunkett, M.D.
VA Medical Center/UC Dept of VA Medical Center/UC Dept of PM&RPM&R
2013 NKY TBI Conference2013 NKY TBI Conference
March 22, 2013March 22, 2013

Chronic PainChronic Pain
IASP definitionIASP definition ““an unpleasant sensory or emotional an unpleasant sensory or emotional
response to a stimulus associated with actual response to a stimulus associated with actual or potential tissue damage”or potential tissue damage”
Pain “lasting longer than the anticipated Pain “lasting longer than the anticipated course of recovery” – often 3-6 monthscourse of recovery” – often 3-6 months
Neurologic, physiologic, and emotional Neurologic, physiologic, and emotional components ( suffering) components ( suffering)

Nociceptive PainNociceptive Pain
Noxious stimuli activating peripheral Noxious stimuli activating peripheral receptors producing typical acute pain receptors producing typical acute pain along a-delta and C fibersalong a-delta and C fibers
Pin-prick or stab wound or stubbed toePin-prick or stab wound or stubbed toe Burn injuryBurn injury FracturesFractures

Neuropathic PainNeuropathic Pain
Pain associated with injury or disease of Pain associated with injury or disease of peripheral nervesperipheral nerves DM peripheral neuropathyDM peripheral neuropathy Shingles ( PHN)Shingles ( PHN) RadiculopathyRadiculopathy
Burning, shooting, lancinating painBurning, shooting, lancinating pain
Allodynia, hyperpathia, central sensitizationAllodynia, hyperpathia, central sensitization


Beginning to End: The Chronic Pain CycleBeginning to End: The Chronic Pain Cycle Pathology:-Muscle atrophy, weakness;-Bone loss;-Immunocomprimise-Depression / Suicide
Less activeKinesophobiaDecreased motivationIncreased isolationRole loss
Disability
Pathophysiology of Maintenance:-Radiculopathy-Neuroma traction-Myofascial sensitization-Brain, SC pathology (atrophy, reorganization)
Psychopathologyof maintenance:-Encoded anxiety dysregulation - PTSD-Emotional allodynia-Mood disorder
NeurogenicInflammation:- Glial activation- Pro-inflammatory cytokines- blood-nerve barrier dysruption
Acute injuryand pain
PeripheralSensitization:New Na+ channelscause lower threshold
Central Sensitization-Neuroplastic changes
Gallagher RM, in Ebert & Kerns, 2010)

PTSD N=23268.2% 2.9%
16.5%
42.1%
6.8%
5.3%
10.3%
12.6%
TBI N=22766.8%
Chronic Pain N=27781.5%
Prevalence of Chronic Pain, PTSD and TBI in a sample of 340 OEF/OIF veterans
Lew, Otis, Tun et al., (in Press). Prevalence of Chronic Pain, Posttraumatic Stress Disorder and Post-concussive Symptoms in OEF/OIF Veterans: The Polytrauma Clinical Triad. JRRD

WHO Analgesic Ladder WHO Analgesic Ladder 19861986
Step 1: Non-opioids (tylenol +/- NSAID)Step 1: Non-opioids (tylenol +/- NSAID) +/- adjuvants+/- adjuvants
Step 2: “Weak opioids” Step 2: “Weak opioids” + non-opioids +/- adjuvants+ non-opioids +/- adjuvants
Step 3: “ Strong opioids”Step 3: “ Strong opioids” + non-opioids +/- adjuvants+ non-opioids +/- adjuvants

Expanded Analgesic LadderExpanded Analgesic Ladder Activity modificationActivity modification Thermal modalitiesThermal modalities Electrical topical modalitiesElectrical topical modalities Topical medical analgesicsTopical medical analgesics Gait and mobility aidesGait and mobility aides BracingBracing Stretching/ROM/massageStretching/ROM/massage StrengtheningStrengthening Aerobic reconditioningAerobic reconditioning Basic self-care health habitsBasic self-care health habits

Ladder ( con’t)Ladder ( con’t)
Non-opioidsNon-opioids AcetaminophenAcetaminophen AspirinAspirin
NSAIDSNSAIDS

AdjuvantsAdjuvants
Muscle relaxantsMuscle relaxants Anti-epileptic drugs ( AEDs)Anti-epileptic drugs ( AEDs) Anti-depressantsAnti-depressants CorticosteroidsCorticosteroids

NarcoticsNarcotics
Pseudo-narcotics ( tramadol)Pseudo-narcotics ( tramadol) Weak potency vs. Strong potencyWeak potency vs. Strong potency Short-acting vs. Long- actingShort-acting vs. Long- acting Oral vs. topical vs. transmucosal vs. IVOral vs. topical vs. transmucosal vs. IV Combination Combination

Invasive proceduresInvasive procedures
BasicBasic Myofascial trigger point injectionsMyofascial trigger point injections Intra-articular injectionsIntra-articular injections Botox – headache and spasticityBotox – headache and spasticity AcupunctureAcupuncture Nerve blocksNerve blocks

Invasive proceduresInvasive procedures
Advanced: ( Fluoro-guided)Advanced: ( Fluoro-guided) Cervical, thoracic, and lumbosacral ESICervical, thoracic, and lumbosacral ESI Facet injectionsFacet injections Medial branch blocksMedial branch blocks Sacro-iliac joint injectionsSacro-iliac joint injections RF nerve ablationRF nerve ablation IDETIDET Stellate ganglion and LS sympathetic blocksStellate ganglion and LS sympathetic blocks Celiac plexus block, Bier blockCeliac plexus block, Bier block

Quaternary InterventionsQuaternary Interventions
Spinal Cord ( or Dorsal column) stimulatorSpinal Cord ( or Dorsal column) stimulator Intrathecal Pain pumpIntrathecal Pain pump Rhizotomy or myelotomyRhizotomy or myelotomy Deep Brain stimulationDeep Brain stimulation ThalatomyThalatomy

Cognitive/Behavioral therapiesCognitive/Behavioral therapies
Progressive relaxationProgressive relaxation Guided imageryGuided imagery Individual and Group therapyIndividual and Group therapy Cognitive/behavioral therapyCognitive/behavioral therapy BiofeedbackBiofeedback

Pain CategoriesPain Categories
““Orthopedic”Orthopedic” OA/DJDOA/DJD Muscles, tendons, ligamentsMuscles, tendons, ligaments
““Neuropathic”Neuropathic” Myelopathy, radiculopathyMyelopathy, radiculopathy Peripheral neuropathyPeripheral neuropathy
Complex/Central PainComplex/Central Pain

CategoriesCategories
Above + Chronicity help guide treatmentAbove + Chronicity help guide treatment Other factors – Secondary GainOther factors – Secondary Gain
Workmen’s Comp, Tort claim, SSDIWorkmen’s Comp, Tort claim, SSDI
Medical co-morbiditiesMedical co-morbidities Traumatic Brain InjuryTraumatic Brain Injury
AgeAge

HeadacheHeadache
Episodic Headache•Characterize type•Abortive therapy
•Maximum 6 doses/week
Chronic Daily Headache•> 15 HA days per month•Analgesic rebound•Prophylaxis is key
Abortive
NSAIDs•GI side effects
IbuprofenNaproxen SodiumAspirin
Triptans•Contraindicated in patients with CAD
CombinationMedications•Cognitive side effects•Risk of W/D
FioricetFiorinalMidrin
ProphylaxisOnset of action ~ 4 wks
Beta-blockers•Non-selective may have benefit on autonomic effects of PTSD
Propranolol
Anti-depressants•May improve mood•Improves sleep
NortriptyllineAmitryptillineParoxetineFluoxetine
AEDS
•Neuropathic pain
gabapentin•Mood lability valproic acid topirimate
AlternativesPromethazineMetoclopramideProchloroperazineTizanidineNon-medicationTrigger point injectionOccipital nerve blockPhysical therapy
Avoid narcotics& Benzos

Drug InteractionsDrug InteractionsHeadache Drug
PTSD Drug Interaction
Tricyclic Antidepressants
SSRIs1) Inc TCA levels
2) Serotonin syndrome
Triptans SSRIsSerotonin Syndrome*
Propranolol PrazosinAdditive lowering of BP, orthostasis
Tricyclic
AntidepressantsBenzodiazepine
Additive increase in sedation

Back to Ladder detailsBack to Ladder details
Activity modificationsActivity modifications ““RICE” + Lifting and positional limitationsRICE” + Lifting and positional limitations Work hours and work pacingWork hours and work pacing Rotation of repetitive tasksRotation of repetitive tasks Ergonomic adjustmentsErgonomic adjustments Biomechanical optimizationBiomechanical optimization Graduated return to workGraduated return to work
Topical modalitiesTopical modalities
IceIce HeatHeat Topical analgesicsTopical analgesics
CapsaicinCapsaicin LidodermLidoderm Camphor, menthol and salicylates ( Ben-gay)Camphor, menthol and salicylates ( Ben-gay)
Ultrasound or Iontophoresis ( steroids/NSAIDs)Ultrasound or Iontophoresis ( steroids/NSAIDs) TENS unitTENS unit E-stim, Biovest, Alpha stimE-stim, Biovest, Alpha stim Cold laserCold laser
Gait and mobility aidesGait and mobility aides
CaneCane Walker incl. Rolling walker w/ fold-down Walker incl. Rolling walker w/ fold-down
seatseat Wheelchair ( manual vs. electric)Wheelchair ( manual vs. electric)
ScooterScooter

OrthoticsOrthotics
Lumbar supportLumbar support Wrist splint +/- thumb spicaWrist splint +/- thumb spica Elbow pads, arm slingElbow pads, arm sling Soft cervical collarSoft cervical collar Knee brace – hinged/unhingedKnee brace – hinged/unhinged Ankle brace or AFOAnkle brace or AFO PTB AFOPTB AFO Shoe orthotic inserts, sole modificationsShoe orthotic inserts, sole modifications

PT + HEPPT + HEP
Stretching/ROM/soft tissue mobilizationStretching/ROM/soft tissue mobilization Strengthening – Isometric -> IsotonicStrengthening – Isometric -> Isotonic Work or activity - specific trainingWork or activity - specific training PlyometricsPlyometrics Basic or modified aerobic reconditioningBasic or modified aerobic reconditioning
Walking/treadmill - graduatedWalking/treadmill - graduated Bike riding – upright/recumbentBike riding – upright/recumbent Aquatic – basedAquatic – based Cardiopulmonary parametersCardiopulmonary parameters

Massage TherapyMassage Therapy
Craniosacral techniques for TBICraniosacral techniques for TBI

ChiropracticChiropractic
ManipulationManipulation ModalitiesModalities

Basic Selfcare – Health habitsBasic Selfcare – Health habits
Obesity – dietObesity – diet SmokingSmoking AlcoholAlcohol Drug abuseDrug abuse Sleep hygieneSleep hygiene Stress managementStress management

Basic analgesicsBasic analgesics
Acetaminophen ( NTE 4000 mg/day)Acetaminophen ( NTE 4000 mg/day) Hepatic caveatsHepatic caveats
ASA ASA GI monitoringGI monitoring

NSAIDsNSAIDs SalicylatesSalicylates
Non-acetylated ( Salsalate, Disalcid, Trilisate)Non-acetylated ( Salsalate, Disalcid, Trilisate) Propionic acidsPropionic acids
Ibuprofen, Naproxen, ketoprofen, OxaprasinIbuprofen, Naproxen, ketoprofen, Oxaprasin Acetic acidsAcetic acids
Indomethacin, diclofenac, sulindac, toradolIndomethacin, diclofenac, sulindac, toradol OxicamsOxicams
PiroxicamPiroxicam Cox-2 InhibitorsCox-2 Inhibitors
CelebrexCelebrex Xyflamend – herbal - OTCXyflamend – herbal - OTC
Muscle relaxantsMuscle relaxants
Cyclobenzaprine ( TCA)Cyclobenzaprine ( TCA) Parafon forte, methocarbamol, carisoprodolParafon forte, methocarbamol, carisoprodol DantriumDantrium BaclofenBaclofen TizandineTizandine DiazepamDiazepam
Caveat re sedation and liver functionCaveat re sedation and liver function Soma – ( and valium) dependency Soma – ( and valium) dependency

Neuropathic agentsNeuropathic agents
AntidepressantsAntidepressants TCA – ami/nortriptyline, trazodone, TCA – ami/nortriptyline, trazodone,
desipraminedesipramine SSRI’s:SSRI’s: SNRI’s: venlafaxine, duloxetineSNRI’s: venlafaxine, duloxetine

Neuropathic agentsNeuropathic agents
Anti-epileptic drugs:Anti-epileptic drugs: Carbamazepine, oxcarbazepineCarbamazepine, oxcarbazepine Topiramate, KeppraTopiramate, Keppra Gabapentin ( Neurontin)Gabapentin ( Neurontin) Pregabalin ( Lyrica)Pregabalin ( Lyrica)
Watch for CNS SE, drug interactions esp Watch for CNS SE, drug interactions esp tegretoltegretol
LFT and WBC monitoring LFT and WBC monitoring

Oral steroidsOral steroids
Medrol dospak ( Methylprednisolone)Medrol dospak ( Methylprednisolone)
Prednisone taper ( 40 mg -> 0 over 12 d)Prednisone taper ( 40 mg -> 0 over 12 d)
GI, DM, cataract, osteoporosisGI, DM, cataract, osteoporosis
But also watch out for Bipolar d/o But also watch out for Bipolar d/o

NarcoticsNarcotics
Pseudo-narcoticPseudo-narcotic Tramadol – mu agonist activityTramadol – mu agonist activity
Mild analgesiaMild analgesia
Watch for serotonin syndrome w/ SSRI’sWatch for serotonin syndrome w/ SSRI’s Habit-formingHabit-forming

NarcoticsNarcotics
MildMild
Propoxyphene ( Darvocet/Darvon)Propoxyphene ( Darvocet/Darvon) No efficacy > tylenol – removed from marketNo efficacy > tylenol – removed from market
Codeine Codeine Poor GI tolerancePoor GI tolerance 2-10 % transformation to morphine2-10 % transformation to morphine

NarcoticsNarcotics
Short-actingShort-acting Oxycodone – schedule IIOxycodone – schedule II Hydrocodone – schedule III-> IIHydrocodone – schedule III-> II Meperidine ( Demerol)Meperidine ( Demerol) Hydromorphone ( Dilaudid)Hydromorphone ( Dilaudid)
• Avoid for chronic pain – rapid accommodationAvoid for chronic pain – rapid accommodation Morphine IRMorphine IR

NarcoticsNarcotics
Long-actingLong-acting OxyContinOxyContin Morphine SR, MS ContinMorphine SR, MS Contin Avinza, OpanaAvinza, Opana MethadoneMethadone Fentanyl patch or lollipopFentanyl patch or lollipop Tapentadol (Nucynta)Tapentadol (Nucynta)

Narcotic SENarcotic SE
CommonCommon N/VN/V Constipation – proactive bowel regimenConstipation – proactive bowel regimen Sedation *** Key to avoid in TBI**Sedation *** Key to avoid in TBI** ItchingItching Physiologic/psychological dependencePhysiologic/psychological dependence SweatingSweating AnorexiaAnorexia MyoclonusMyoclonus

Narcotic SENarcotic SE
MyoclonusMyoclonus Dizziness/orthostasisDizziness/orthostasis AccommodationAccommodation Respiratory suppressionRespiratory suppression Cardiac dysrhythmia – methadoneCardiac dysrhythmia – methadone
Methadone also difficult to achieve Methadone also difficult to achieve equianalgesic dosing + occ idiosyncratic buildup equianalgesic dosing + occ idiosyncratic buildup w/ long ½ life > analgesic effectw/ long ½ life > analgesic effect

Narcotic IssuesNarcotic Issues
Avoid as unimodal pharmacologic approach – Avoid as unimodal pharmacologic approach – opioid sparing conceptopioid sparing concept
Possible opioid hyperalgesiaPossible opioid hyperalgesia May need to rotate type of narcotic if May need to rotate type of narcotic if
accommodatedaccommodated Addiction vs Pseudo-addiction ( UDS)Addiction vs Pseudo-addiction ( UDS) Dependency – physiologic/psychologicDependency – physiologic/psychologic Taper ( 50 %/week) vs. DetoxTaper ( 50 %/week) vs. Detox Buprenex vs. methadone maintenanceBuprenex vs. methadone maintenance
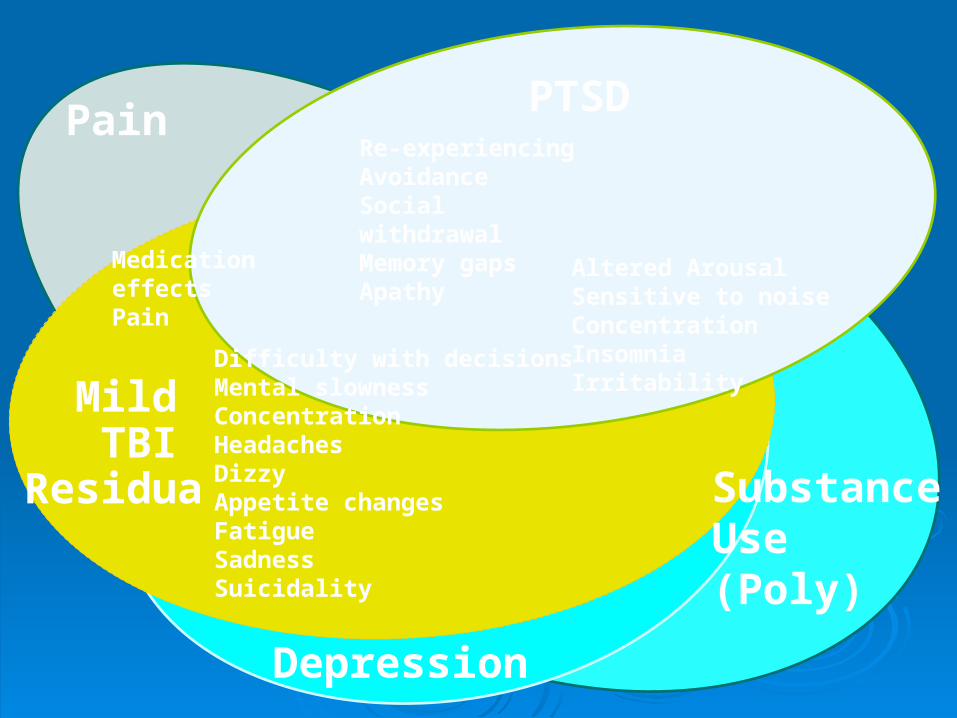
PTSD Re-experiencingAvoidance Social withdrawal Memory gapsApathy
Mild TBIResidua
Difficulty with decisionsMental slownessConcentrationHeadachesDizzyAppetite changesFatigueSadnessSuicidality
Altered Arousal Sensitive to noise Concentration Insomnia Irritability
Depression
Substance Use (Poly)
Pain
Medication effectsPain

Conservative Conservative management of pain management of pain
after TBIafter TBI
Rachel Heberling, MDRachel Heberling, MD
Cincinnati VA Medical CenterCincinnati VA Medical Center
University of CincinnatiUniversity of Cincinnati

Why Conservative Pain Why Conservative Pain Management in TBI?Management in TBI?
Increased sensitivity to medicationsIncreased sensitivity to medications Increased difficulty managing medications, Increased difficulty managing medications,
especially prn’sespecially prn’s Increased self-efficacy via self-Increased self-efficacy via self-
managementmanagement Potentially decreased number of office Potentially decreased number of office
visitsvisits Cost-effectiveCost-effective

HeatHeat
Superficial heat: heating pad, hot shower, Superficial heat: heating pad, hot shower, hot bathhot bath
Deep heat: ultrasoundDeep heat: ultrasound
Effective for pain relief, increased muscle Effective for pain relief, increased muscle flexibilityflexibility
Not much evidence, but obviously effective Not much evidence, but obviously effective brieflybriefly

ColdCold
Superficial: Ice packsSuperficial: Ice packs Deep: cold laserDeep: cold laser
Cold effective for pain relief and reducing Cold effective for pain relief and reducing inflammation, but contracts musclesinflammation, but contracts muscles
Unclear mechanism and efficacy of cold Unclear mechanism and efficacy of cold laserlaser

STRETCHING!STRETCHING!
Muscle has viscoelastic propertiesMuscle has viscoelastic properties Slow, deep stretch paired with deep Slow, deep stretch paired with deep
breathing necessarybreathing necessary Muscle properties change for ~10 hrs after Muscle properties change for ~10 hrs after
deep stretchdeep stretch
Evidence not compelling, but pain-relief Evidence not compelling, but pain-relief effect of stretching is very obvious clinicallyeffect of stretching is very obvious clinically

Stretching!Stretching!

Other types of ExerciseOther types of Exercise
Aerobic exercise – has huge role in Aerobic exercise – has huge role in decreasing muscle tension and decreasing muscle tension and consequent pain.consequent pain.
Strength training – some role in Strength training – some role in decreasing pain (e.g. core strengthening), decreasing pain (e.g. core strengthening), but generally minimized until pain but generally minimized until pain beginning to improve.beginning to improve.

MeditationMeditation
Increasing base of evidence for the pain Increasing base of evidence for the pain relief effects of meditationrelief effects of meditation
Decreases stressDecreases stress Improved emotional acceptance of painImproved emotional acceptance of pain

YogaYoga
EXCELLENT choice for exercise EXCELLENT choice for exercise maintenancemaintenance
Has role in decreasing active pain issues Has role in decreasing active pain issues as well.as well.
Must start in beginner class! Must start in beginner class!

Advanced Yoga ClassAdvanced Yoga Class

Tai ChiTai Chi
Becoming more popular topic of researchBecoming more popular topic of research Have found that Tai Chi practice Have found that Tai Chi practice
decreases falls in the elderlydecreases falls in the elderly Somewhat similar to yoga, but more Somewhat similar to yoga, but more
focused on gentle fluid movement, as focused on gentle fluid movement, as opposed to deep prolonged stretchopposed to deep prolonged stretch

Physical TherapyPhysical Therapy
Many treatment modalities availableMany treatment modalities available StretchingStretching StrengtheningStrengthening UltrasoundUltrasound TENSTENS TractionTraction

Bracing & Assistive DevicesBracing & Assistive Devices
Lumbar supportLumbar support Knee bracesKnee braces CaneCane WalkerWalker

AcupunctureAcupuncture

AcupunctureAcupuncture

WHO, NIH Consensus StudyWHO, NIH Consensus Study
Classified disease Classified disease processes according to processes according to evidence for evidence for acupuncture efficacyacupuncture efficacy
20032003
ProvenProven Needs further researchNeeds further research Worth tryingWorth trying
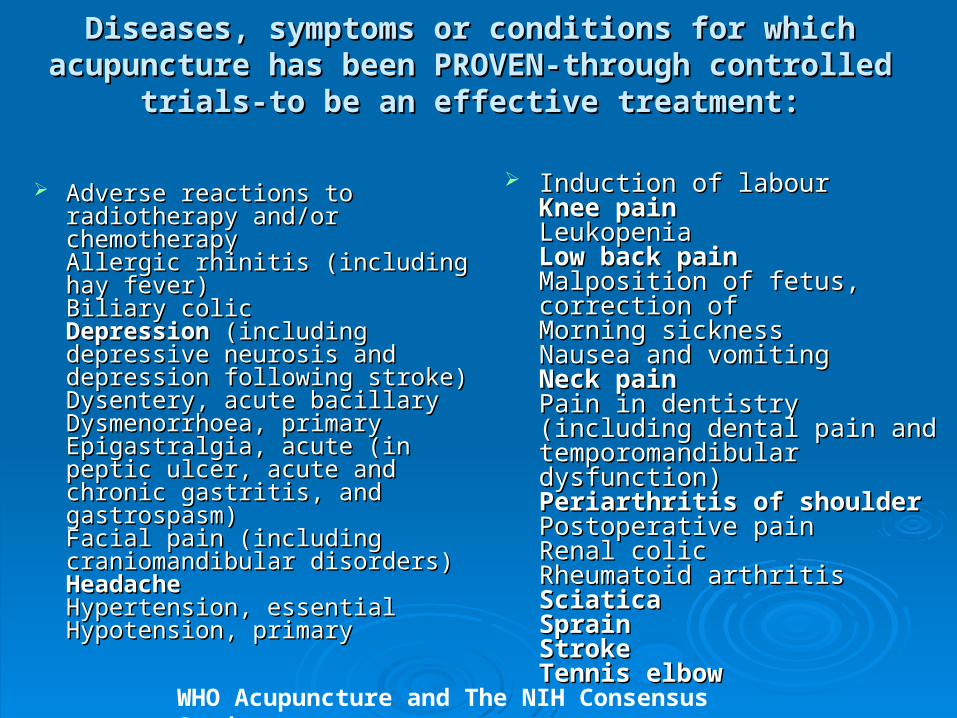
Diseases, symptoms or conditions for which acupuncture Diseases, symptoms or conditions for which acupuncture has been PROVEN-through controlled trials-to be an has been PROVEN-through controlled trials-to be an
effective treatment:effective treatment:
Adverse reactions to radiotherapy Adverse reactions to radiotherapy and/or chemotherapyand/or chemotherapyAllergic rhinitis (including hay Allergic rhinitis (including hay fever)fever)Biliary colicBiliary colicDepression Depression (including (including depressive neurosis and depressive neurosis and depression following stroke)depression following stroke)Dysentery, acute bacillaryDysentery, acute bacillaryDysmenorrhoea, primaryDysmenorrhoea, primaryEpigastralgia, acute (in peptic Epigastralgia, acute (in peptic ulcer, acute and chronic gastritis, ulcer, acute and chronic gastritis, and gastrospasm)and gastrospasm)Facial pain (including Facial pain (including craniomandibular disorders)craniomandibular disorders)HeadacheHeadacheHypertension, essentialHypertension, essentialHypotension, primaryHypotension, primary
Induction of labourInduction of labourKnee painKnee painLeukopeniaLeukopeniaLow back painLow back painMalposition of fetus, correction ofMalposition of fetus, correction ofMorning sicknessMorning sicknessNausea and vomitingNausea and vomitingNeck painNeck painPain in dentistry (including dental Pain in dentistry (including dental pain and temporomandibular pain and temporomandibular dysfunction)dysfunction)Periarthritis of shoulderPeriarthritis of shoulderPostoperative painPostoperative painRenal colicRenal colicRheumatoid arthritisRheumatoid arthritisSciaticaSciaticaSprainSprainStrokeStrokeTennis elbowTennis elbow
WHO Acupuncture and The NIH Consensus Study

Diseases, symptoms or conditions for which the Diseases, symptoms or conditions for which the therapeutic effect of acupuncture has been shown but therapeutic effect of acupuncture has been shown but
for which FURTHER PROOF IS NEEDED:for which FURTHER PROOF IS NEEDED: Abdominal pain (in acute Abdominal pain (in acute
gastroenteritis or due to gastroenteritis or due to gastrointestinal spasm)gastrointestinal spasm)Acne vulgarisAcne vulgarisAlcohol dependence and Alcohol dependence and detoxificationdetoxificationBell’s palsyBell’s palsyBronchial asthmaBronchial asthmaCancer painCancer painCardiac neurosisCardiac neurosisCholecystitis, chronic, with acute Cholecystitis, chronic, with acute exacerbationexacerbationCholelithiasisCholelithiasisCompetition stress syndromeCompetition stress syndromeCraniocerebral injury, closedCraniocerebral injury, closedDiabetes mellitus, non-insulin-Diabetes mellitus, non-insulin-dependentdependentEaracheEaracheEpidemic haemorrhagic feverEpidemic haemorrhagic feverEpistaxis, simple (without Epistaxis, simple (without generalized or local disease)generalized or local disease)
Eye pain due to subconjunctival Eye pain due to subconjunctival injectioninjectionFemale infertilityFemale infertilityFacial spasmFacial spasmFemale urethral syndromeFemale urethral syndromeFibromyalgia and fasciitisFibromyalgia and fasciitisGastrokinetic disturbanceGastrokinetic disturbanceGouty arthritisGouty arthritisHepatitis B virus carrier statusHepatitis B virus carrier statusHerpes zoster (human (alpha) Herpes zoster (human (alpha) herpesvirus 3)herpesvirus 3)HyperlipaemiaHyperlipaemiaHypo-ovarianismHypo-ovarianismInsomniaInsomniaLabour painLabour painLactation, deficiencyLactation, deficiencyMale sexual dysfunction, non-Male sexual dysfunction, non-organic Ménière diseaseorganic Ménière diseaseNeuralgia, post-herpeticNeuralgia, post-herpetic
WHO Acupuncture and The NIH Consensus Study

Diseases, symptoms or conditions for which the Diseases, symptoms or conditions for which the therapeutic effect of acupuncture has been shown but therapeutic effect of acupuncture has been shown but
for which FURTHER PROOF IS NEEDED:for which FURTHER PROOF IS NEEDED:
NeurodermatitisNeurodermatitisObesityObesityOpium, cocaine and heroin Opium, cocaine and heroin dependencedependenceOsteoarthritisOsteoarthritisPain due to endoscopic Pain due to endoscopic examinationexaminationPain in thromboangiitis obliteransPain in thromboangiitis obliteransPolycystic ovary syndrome (Stein-Polycystic ovary syndrome (Stein-Leventhal syndrome)Leventhal syndrome)Postextubation in childrenPostextubation in childrenPostoperative convalescencePostoperative convalescencePremenstrual syndromePremenstrual syndromeProstatitis, chronicProstatitis, chronicPruritusPruritusRadicular and pseudoradicular Radicular and pseudoradicular pain syndromepain syndromeRaynaud syndrome, primaryRaynaud syndrome, primary
Recurrent lower urinary-tract Recurrent lower urinary-tract infectioninfectionReflex sympathetic dystrophyReflex sympathetic dystrophyRetention of urine, traumaticRetention of urine, traumaticSchizophreniaSchizophreniaSialism, drug-inducedSialism, drug-inducedSjögren syndromeSjögren syndromeSore throat (including tonsillitis)Sore throat (including tonsillitis)Spine pain, acuteSpine pain, acuteStiff neckStiff neckTemporomandibular joint Temporomandibular joint dysfunctiondysfunctionTietze syndromeTietze syndromeTobacco dependenceTobacco dependenceTourette syndromeTourette syndromeUlcerative colitis, chronicUlcerative colitis, chronicUrolithiasisUrolithiasisVascular dementiaVascular dementiaWhooping cough (pertussis)Whooping cough (pertussis)
WHO Acupuncture and The NIH Consensus Study

Diseases, symptoms or conditions for which there are Diseases, symptoms or conditions for which there are only individual controlled trials reporting some only individual controlled trials reporting some
therapeutic effects, but for which acupuncture is WORTH therapeutic effects, but for which acupuncture is WORTH TRYING because treatment by conventional and other TRYING because treatment by conventional and other
therapies is difficult:therapies is difficult:
ChloasmaChloasma
Choroidopathy, central Choroidopathy, central serousserous
Colour blindnessColour blindness
DeafnessDeafness
HypophreniaHypophrenia
Neuropathic bladder in Neuropathic bladder in spinal cord injuryspinal cord injury
Pulmonary heart disease, Pulmonary heart disease, chronicchronic
Small airway obstruction Small airway obstruction
Irritable colon syndromeIrritable colon syndrome

GERAC – DesignGERAC – Design Journal of Alternative and Complementary MedicineJournal of Alternative and Complementary Medicine. Volume 12, Number . Volume 12, Number
8, 2006. pp 733-428, 2006. pp 733-42
German Acupuncture Trials for Low Back PainGerman Acupuncture Trials for Low Back Pain 1162 patients in Germany at 340 centers1162 patients in Germany at 340 centers Chronic non-specific low back pain >6 monthsChronic non-specific low back pain >6 months Compared verde vs sham vs conventional Compared verde vs sham vs conventional
guideline-based treatmentguideline-based treatment Semi-standardized verde acupuncture Semi-standardized verde acupuncture
treatment protocoltreatment protocol

GERAC – DesignGERAC – Design
10 sessions over 10 weeks regardless of 10 sessions over 10 weeks regardless of groupgroup
5 additional sessions for partial 5 additional sessions for partial responders (>10%, <50% improvement)responders (>10%, <50% improvement)
Limited communication with acupuncturist Limited communication with acupuncturist to avoid unblindingto avoid unblinding
Allowed NSAID for rescue, max twice Allowed NSAID for rescue, max twice weekly.weekly.

GERAC - ResultsGERAC - ResultsTable 4. Primary Outcome: Pairwise Comparisonof Treatment Response 6 Months After Randomization
Treatment Response Intergroup Difference P ValueGroup 1 vs group 347.6 (42.4 to 52.6) vs 20.2 (13.4 to 26.7) 0.00127.4 (23.0 to 32.1)
Group 2 vs group 344.2 (39.2 to 49.3) vs 16.8 (10.1 to 23.4) 0.00127.4 (23.0 to 32.1)
Group 1 vs group 2 3.4 (−3.7 to 10.3) 0.3947.6 (42.4 to 52.6) vs 44.2 (39.2 to 49.3)
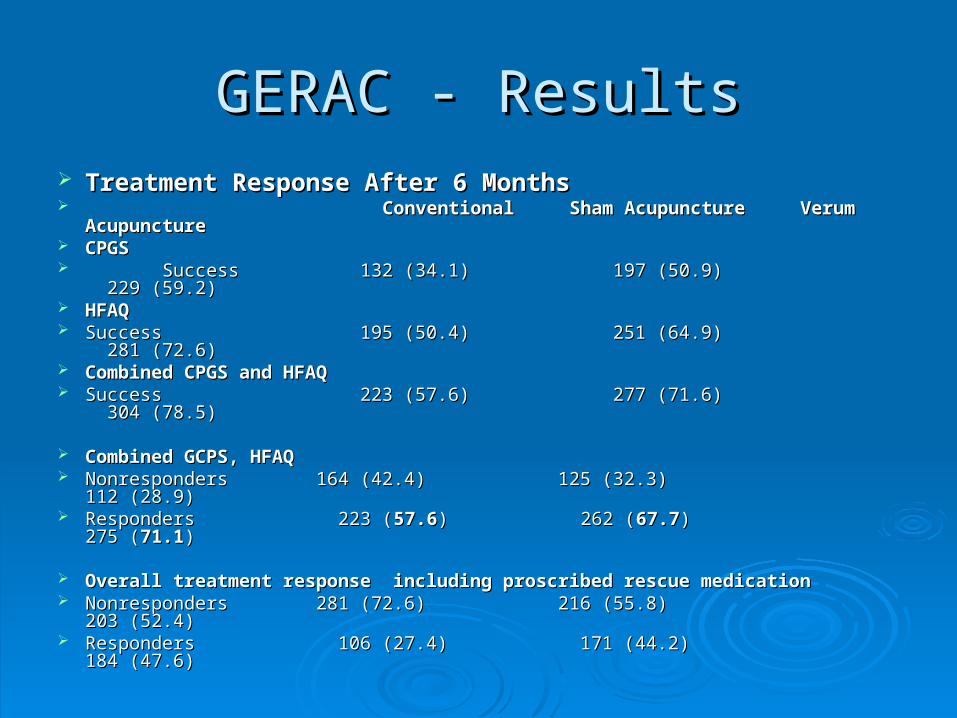
GERAC - ResultsGERAC - Results Treatment Response After 6 MonthsTreatment Response After 6 Months Conventional Sham Acupuncture Verum AcupunctureConventional Sham Acupuncture Verum Acupuncture CPGSCPGS Success 132 (34.1) 197 (50.9) 229 (59.2)Success 132 (34.1) 197 (50.9) 229 (59.2) HFAQHFAQ Success 195 (50.4) 251 (64.9) 281 (72.6)Success 195 (50.4) 251 (64.9) 281 (72.6) Combined CPGS and HFAQCombined CPGS and HFAQ Success 223 (57.6) 277 (71.6) 304 (78.5)Success 223 (57.6) 277 (71.6) 304 (78.5)
Combined GCPS, HFAQCombined GCPS, HFAQ Nonresponders 164 (42.4) 125 (32.3) 112 (28.9)Nonresponders 164 (42.4) 125 (32.3) 112 (28.9) Responders 223 (Responders 223 (57.657.6) 262 () 262 (67.767.7) 275 () 275 (71.171.1))
Overall treatment response including proscribed rescue medicationOverall treatment response including proscribed rescue medication Nonresponders 281 (72.6) 216 (55.8) 203 (52.4)Nonresponders 281 (72.6) 216 (55.8) 203 (52.4) Responders 106 (27.4) 171 (44.2) 184 (47.6)Responders 106 (27.4) 171 (44.2) 184 (47.6)



















