![Calotropisprocera LatexExtractAffordsProtection ...downloads.hindawi.com/journals/mi/2007/047523.pdf · inflammatory, analgesic, and weak antipyretic effects in var- iousanimalmodels[14–16].Bothlatexanditsmethanolex-](https://static.fdocuments.us/doc/165x107/5d5e0cee88c99328118b864b/calotropisprocera-latexextractaffordsprotection-inammatory-analgesic.jpg)
Analgesic, Anitpyretic, Anit ... - PHARMACEUTICAL REVIEW · PDF file03.05.2013 ·...
10
3 rd PART: Unit VIII: ANTI-INFLAMMATORY, ANALGESIC AND ANTIPYRETIC DRUGS Chapter 26: ANTIPYRETIC, ANTI-INFLAMMATORY AND ANALGESIC DRUGS. (Non-narcotic or non-opioid (NSAID,s) and Aspirin like analgesics.) Introduction & chemistry: Drugs grouped in this class having analgesic, antipyretic & anti-inflammatory effect of different measures Having less analgesic effect when compared to narcotics Having no CNS , dependence & abusing liability. Bitter glycosides of willow bark (Salix alba) hydrolyzed to synthesis salicylic acid – used for many centuries. Na Salicylate introduced in 1875 for fever & pain. Acetyl salicylic acid introduced in 1899. 1 st NSAID,s phenylbutazone discovered in 1949 and Indomethacin in 1963. COX inhibitors – ibuprofen and COX-2 inhibitors added recently. These are chemically diverse but mostly organic acid. Inflammation: A normal protective response of tissues injured by physical trauma, noxious chemicals or microbial agents. It is the body effort to destroy organism, remove irritation and restore the tissue reparation. It may be triggered by innocuous agent (pollens) or autoimmune response (asthma, rheumatoid arthritis). Chemical inflammatory mediators are histamine, 5-HT, PG,s, bradykinins, interleukines etc. It’s not possible to control all involved mediators.
Transcript of Analgesic, Anitpyretic, Anit ... - PHARMACEUTICAL REVIEW · PDF file03.05.2013 ·...
3rd PART:
Unit VIII:
ANTI-INFLAMMATORY, ANALGESIC AND ANTIPYRETIC DRUGS
Chapter 26:
ANTIPYRETIC, ANTI-INFLAMMATORY AND ANALGESIC DRUGS. (Non-narcotic or non-opioid (NSAID,s) and
Aspirin like analgesics.)
Introduction & chemistry:
Drugs grouped in this class having analgesic, antipyretic & anti-inflammatory effect of different measures
Having less analgesic effect when compared to narcotics
Having no CNS , dependence & abusing liability.
Bitter glycosides of willow bark (Salix alba) hydrolyzed to synthesis salicylic acid – used for many centuries.
Na Salicylate introduced in 1875 for fever & pain.
Acetyl salicylic acid introduced in 1899.
1st NSAID,s phenylbutazone discovered in 1949 and Indomethacin in 1963.
COX inhibitors – ibuprofen and COX-2 inhibitors added recently.
These are chemically diverse but mostly organic acid. Inflammation: A normal protective response of tissues injured by physical trauma, noxious chemicals or microbial agents. It is the body effort to destroy organism, remove irritation and restore the tissue reparation. It may be triggered by innocuous agent (pollens) or autoimmune response (asthma, rheumatoid arthritis). Chemical inflammatory mediators are histamine, 5-HT, PG,s, bradykinins, interleukines etc. It’s not possible to control all involved mediators.
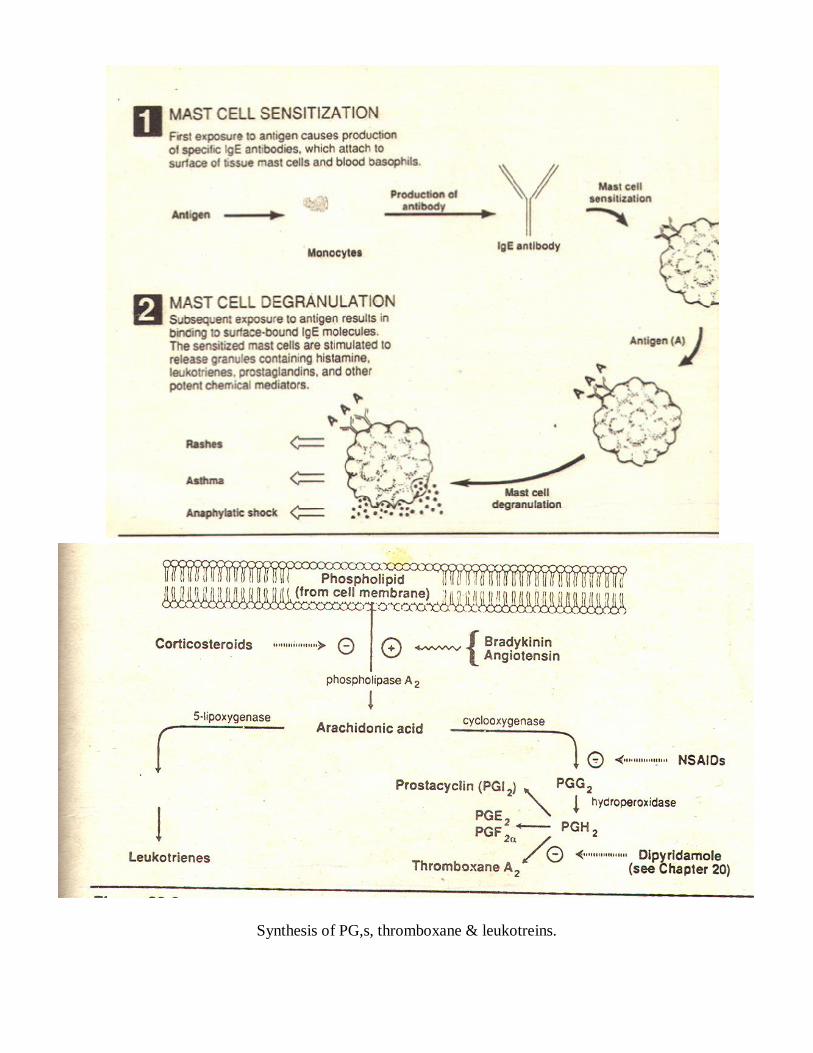
Illustration of asthma/ anaphylactic shock.
Synthesis of PG,s, thromboxane & leukotreins.
CLASSIFICATION: A NSAID,s: (Non- selective COX inhibitors) 1 Salicylate - Aspirin 2 Pyrazolon derivative - Phenylbutazone 3 Indole derivative – Indomethacine, sulindac 4 Propionic acid - Ibuprofen, flurbeprofen, naproxen 5 Anthranilic acid derivative - Mefnamic acid (Fenamates) 6 Aryl acetic acid derivative – Diclofenac, Ketorolac 7 Oxicame derivative – Piroxicam, meloxicam B preferential COX-2 inhibitors Nimsulide C Selective COX-2 inhibitors Celecoxib, rofecoxib. D Analgesic, antipyretic with poor anti-inflammatory effects.
1 Para-aminophenol derivative Paracetamol (Acetaminophene) 2 Pyrazolone derivative - Metamizole (dypron)
E Drugs for Arthritis:
Gold salts, chloroquine, D-Penicilline, immunosuppressants -methotrexate, cyclosprorin.
F Drugs for Gout; 1 For acute gout;
NSAID,s, colchicines, carticosteroids. 2 For chronic gout/ hyperuricaemia;
Uricosurics, probenecid, sulfinpyrazone.
26.1 Salicylates (aspirin)
Aspirin is prototype of Salicylates Most common, less toxic & comparatively cheap. No sedation, dependence & tolerance (like morphine). Treatment coupled with H+ Pump or H2 blockers. Mostly weak organic acid. Dosage: 160- 325mg/ day MI, Post MI & coronary diseases. 300mg tablet four time a day for analgesic effect. 300mg 12-20 tablets/ dayfor pain & inflammation.
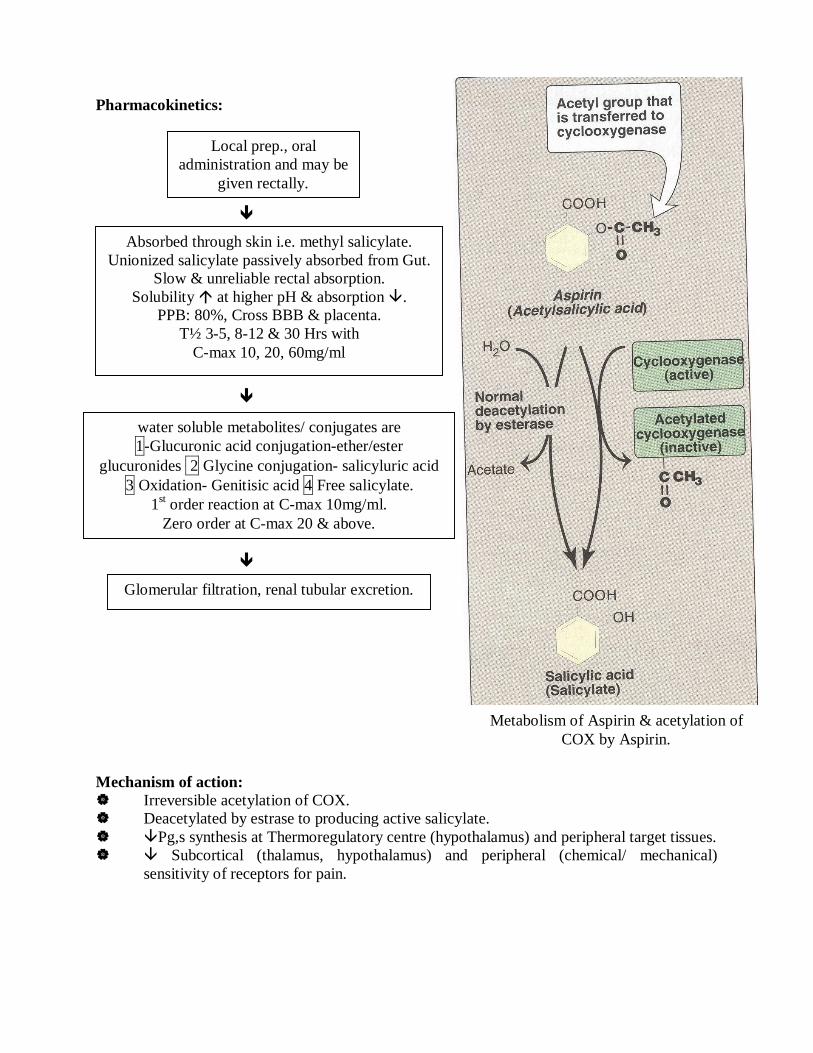
Pharmacokinetics:
Mechanism of action: Irreversible acetylation of COX. Deacetylated by estrase to producing active salicylate. Pg,s synthesis at Thermoregulatory centre (hypothalamus) and peripheral target tissues. Subcortical (thalamus, hypothalamus) and peripheral (chemical/ mechanical)
sensitivity of receptors for pain.
Local prep., oral administration and may be
given rectally.
Absorbed through skin i.e. methyl salicylate. Unionized salicylate passively absorbed from Gut.
Slow & unreliable rectal absorption. Solubility at higher pH & absorption .
PPB: 80%, Cross BBB & placenta. T½ 3-5, 8-12 & 30 Hrs with
C-max 10, 20, 60mg/ml
Glomerular filtration, renal tubular excretion.
water soluble metabolites/ conjugates are 1-Glucuronic acid conjugation-ether/ester
glucuronides 2 Glycine conjugation- salicyluric acid 3 Oxidation- Genitisic acid 4 Free salicylate.
1st order reaction at C-max 10mg/ml. Zero order at C-max 20 & above.
Metabolism of Aspirin & acetylation of COX by Aspirin.
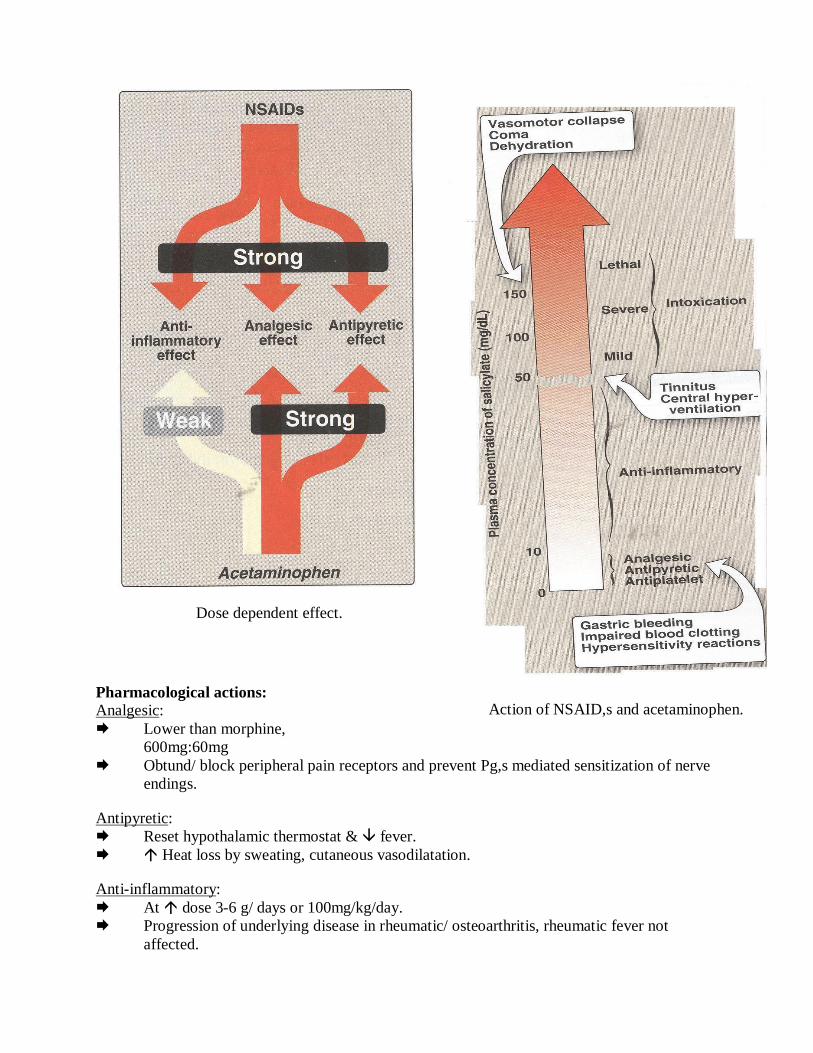
Pharmacological actions: Analgesic: Lower than morphine,
600mg:60mg Obtund/ block peripheral pain receptors and prevent Pg,s mediated sensitization of nerve
endings.
Antipyretic: Reset hypothalamic thermostat & fever. Heat loss by sweating, cutaneous vasodilatation.
Anti-inflammatory: At dose 3-6 g/ days or 100mg/kg/day. Progression of underlying disease in rheumatic/ osteoarthritis, rheumatic fever not
affected.
Action of NSAID,s and acetaminophen.
Dose dependent effect.
Metabolic effects: Cellular metabolism (in skeletal M.) at higher dose. Glucose utilization (diabetes) & liver glycogen depletion. Large chronic use plasma Free FA & cholesterol level by conversion of proteins
into carbohydrates. / oidation of ketone bodies is also Respiration: At higher dose respiration rate , because of CO2 level that stimulate central
(medulla) & peripheral receptors. Salicylate poisoning Hyperventilation. Salicylate level Resp. depression Resp. failure Death Respiratory alkalosis compensated by kidney. GIT: Prostacyclin gastric acid secretion, PgE2 & PgE2α protective mucous secretion. acid, mucous synthesis, Epigastric distress, ulceration & hemorrhage, erosive
gastritis Platelets: TXA2 synthesis that platelet aggregation. endothelial TXA2 synthesis remained
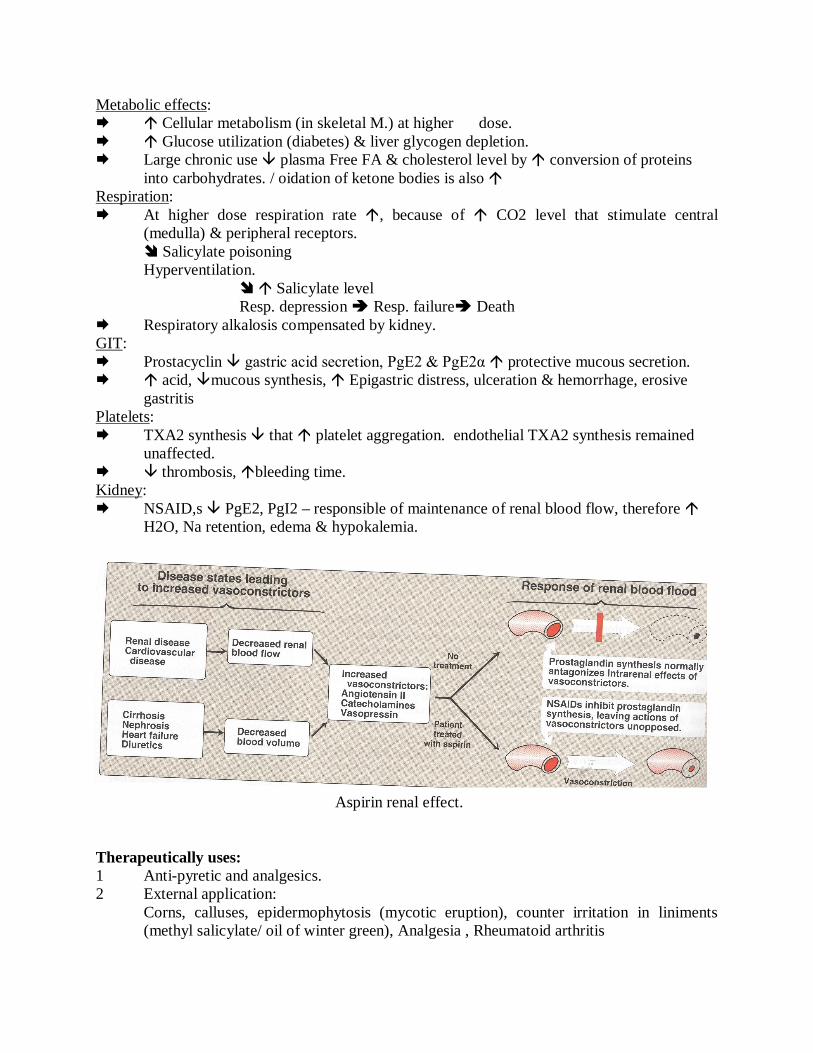
unaffected. thrombosis, bleeding time. Kidney: NSAID,s PgE2, PgI2 – responsible of maintenance of renal blood flow, therefore
H2O, Na retention, edema & hypokalemia.
Aspirin renal effect. Therapeutically uses: 1 Anti-pyretic and analgesics. 2 External application:
Corns, calluses, epidermophytosis (mycotic eruption), counter irritation in liniments (methyl salicylate/ oil of winter green), Analgesia , Rheumatoid arthritis
3 Cardiovascular application: Platelet aggregation, transient ischemia, angina,
coronary artery diseases/ thrombosis & closure of patent ductus arteriosus. 4 Colorectal cancer Adverse effects: 1 GIT: Epigastric distress, nausea, vomiting. 2 CVS: Bleeding time 3 Respiratory effect: Respiration. 4 Metabolism:
Uncouple oxidative phosphorylation, ATP synthesis , pyretic effect at toxic dose.
5 Hypersensitivity: Urticaria, bronchoconstriction, angioneurotic edema, anaphylactic shock.
6 Reye syndromes: Salicylism: Mild: Tinnitus, headache, mental confusion.
Sweating, thirst, Dimness of vision, dizziness, lassitude.
Sever: Restlessness, delirium, hallucination, respiratory/ metabolic acidosis, convulsions skin eruptions, coma and death.
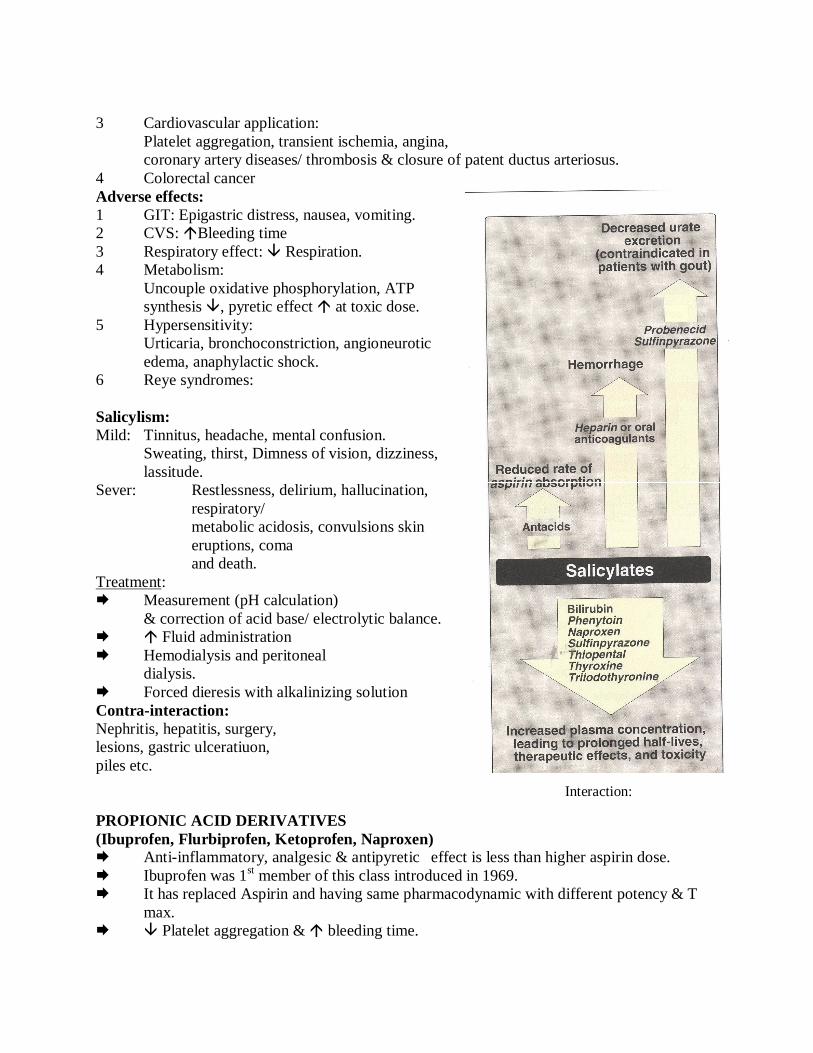
Treatment: Measurement (pH calculation)
& correction of acid base/ electrolytic balance. Fluid administration Hemodialysis and peritoneal
dialysis. Forced dieresis with alkalinizing solution Contra-interaction: Nephritis, hepatitis, surgery, lesions, gastric ulceratiuon, piles etc.
PROPIONIC ACID DERIVATIVES (Ibuprofen, Flurbiprofen, Ketoprofen, Naproxen) Anti-inflammatory, analgesic & antipyretic effect is less than higher aspirin dose. Ibuprofen was 1st member of this class introduced in 1969. It has replaced Aspirin and having same pharmacodynamic with different potency & T
max. Platelet aggregation & bleeding time.
Interaction:
Pharmacokinetics: Mechanism of action:
Reversible inhibit COX and Pg synthesis. Therapeutical uses:
Osteo-arthritis, rheumatic arthritis, analgesic, anti-inflammatory. Adverse effects:
G.I. disturbance (nausea, vomiting), dyspepsia, bleeding, CNS effects, headache, tinnitus, dizziness, thrombocytopenia, skin rashes, blurred vision.
Contraindications: Pregnancy, lactation. Drug Interactions:
Antagonize the natriuretic and antihypertensive effects of furosemide, thiazides diuretics, antihypertensive effect of -adrenergic blocking agents, inhibitors of ACE.
INDOL DERIVATIVE/ ACETIC ACID DERIVATIVE (Indomethacin, Sulindac) Introduced in 1963. Analgesic, anti-inflammatory and not recommended for fever. Neutrophil motility, T cell & B cell proliferation. Phospholipase A & C. Pharmacokinetics: Oral administration, 50-70 mg tid, T½ 4.5-8 average about 2.5 hrs. Indomethacin - 90% PPB, liver metabolism and renal excretion.
Mechanism of action:
Reversible non-selective COX . Pg, Neutrophil motility. At toxic dose uncouple oxidative phosphorylation and depreses the biosynthesis
of mucopolysacchrides.
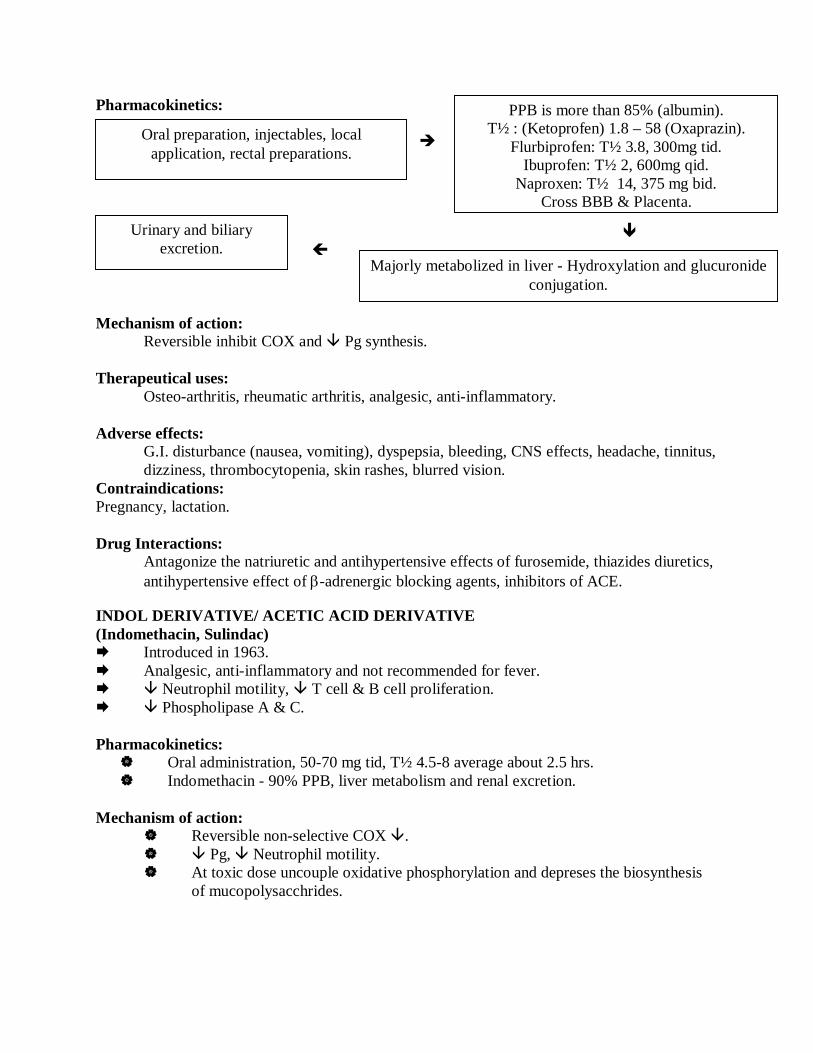
Oral preparation, injectables, local application, rectal preparations.
PPB is more than 85% (albumin). T½ : (Ketoprofen) 1.8 – 58 (Oxaprazin).
Flurbiprofen: T½ 3.8, 300mg tid. Ibuprofen: T½ 2, 600mg qid.
Naproxen: T½ 14, 375 mg bid. Cross BBB & Placenta.
Urinary and biliary excretion.
Majorly metabolized in liver - Hydroxylation and glucuronide conjugation.
Therapeutical uses: Gouty arthritis, ankylosing spondylitis, osteo-arthritis of hip, rheumatic arthritis, sweet syndrome, juvenile rheumatoid arthritis, pleurisy, nephrotic syndrome, diabetes insipidus, Urticaria vasculitis, post-episiotomy pain, heterotropic ossification in arthroplasty. Adverse effects:
Abdominal pain, diarrhea, G.I. hemorrhage, pancreatitis, thrombocytopenia, aplastic anemia, hyperkalemia, hepatitis, jaundice, neutropenia.
Contraindications:
Pregnancy, lactation, person operating machinery patients with psychiatric disorders, epilepsy or parkinsonism, renal disease, ulcerative lesions of stomach and intestine.
PYRAZOLONE DERIVATIVE (Phenylbutazone, Oxyphenbutazone, Propiphenazone) Phenazone and amidopyrin introduced in 1884 as antipyretic & analgesic but banned
because of association with agranulocytosis. Phenylbutazone introduced in 1949 and usually not recommended now because of bone
marrow depression, agranulocytopenia and reactions. Not suggested more than one week. Strong anti-infalmmatory and poor analgesic & antipyretic. Mechanism of action: COX Pharmacokinetics: Oral absorption, PPB 98%, T½ 60 Hrs. Complete liver metabolism – hydroxylation & glucuronidation. Therapeutical uses:
Rheumatic arthritis, ankylosing spondylitis, acute gout. Adverse effects: (More toxic than aspirin) Nausea, vomiting, peptic ulceration, diarrhea, edema, hypersensitivity, bone marrow suppression, skin rashes, vertigo, insomnia, blurred vision, hematurea, goiter ( iodine absorption).
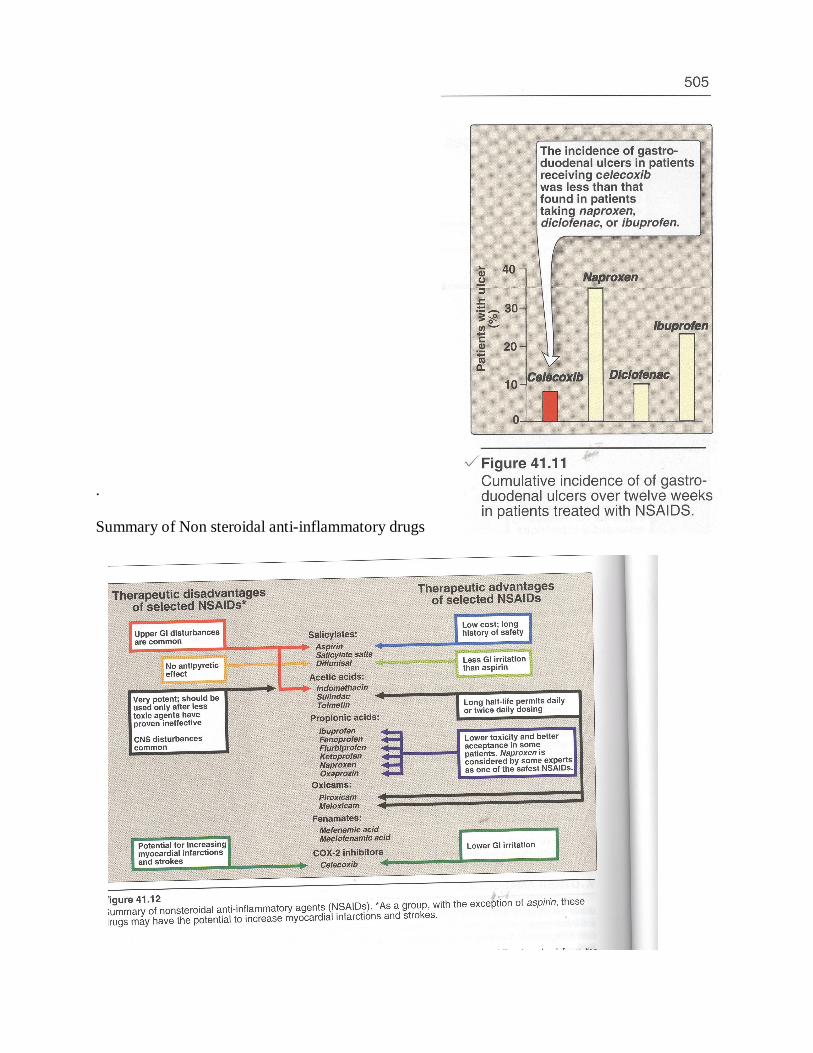
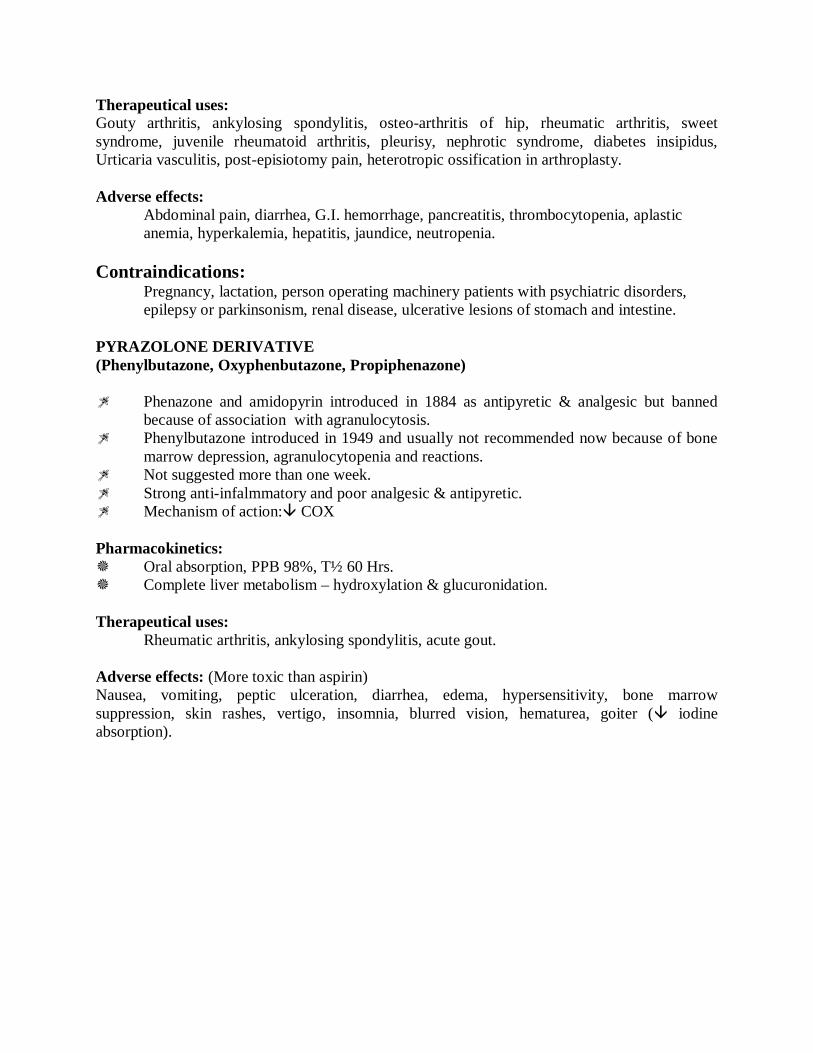
. Summary of Non steroidal anti-inflammatory drugs


















![SM Gr u · allowed paracetamol to become the antipyretic and analgesic of choice in children [1,2] and it is . now the standard antipyretic and analgesic in all age groups. Although](https://static.fdocuments.us/doc/165x107/5e46e07b7d267e4d3734acee/sm-gr-u-allowed-paracetamol-to-become-the-antipyretic-and-analgesic-of-choice-in.jpg)