Anaemia
24
LABORATORY INVESTIGATION OF ANAEMIA BY PROF.YETUNDE. A. AKEN’OVA
-
Upload
femi-austin -
Category
Documents
-
view
214 -
download
1
description
anaemic mgt
Transcript of Anaemia

LABORATORY INVESTIGATION OF ANAEMIA
BY
PROF.YETUNDE. A. AKEN’OVA

Anaemia is an erythrocyte disorder characterized
by a haemoglobin concentration below normal for
the age and sex.
Anaemia can be categorized
1. A failure of production or shortened red cells survival- Intrinsic or extrinsic defect.
2. Anaemia of chronic disease consequent on chronic infection or inflammation or malignancy.

Haematocrit variation throughout life.Term newborn (cord blood) 44 %Term newborn (Capillary blood) 53 – 68Infant (3 months) 30 – 38Child (10 years) 37 – 44Pregnancy (30 wks gestation) 26 – 34 Adult female 37 – 47Adult male 42 – 54

Hct swings as high as 6-8% may occur with correction of dehydration of volume overload.
How was the blood specimen obtain Hgb/Hct values are frequently higher from a finger
stick than from a venous sample, unless excessive pressure is applied to facilitate blood flow.
Prolonged stasis from a tourniquet increases the haematocrit as do muscular activity and cold.

MCV = Hct RBC (Femtolitres)
MCH = Hgb RBC (Picograms)
MCHC = HgbHct ( g/dl RBC)
MCV – is a measure of cell size
MCH – is a measure of the average amount
of haemoglobin in each individual
cell.
MCHC – Is a measure of the concentration of
haemoglobin in each cell.
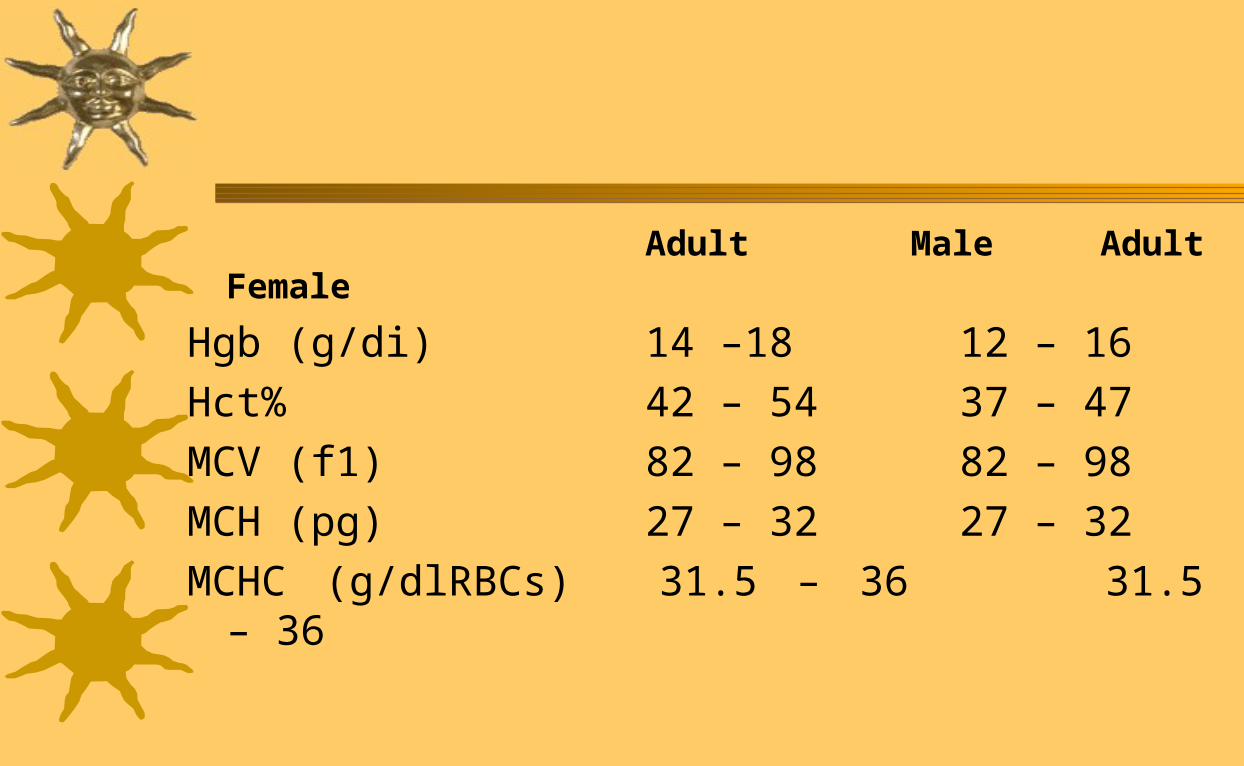
Adult Male Adult Female
Hgb (g/di) 14 –18 12 – 16
Hct% 42 – 54 37 – 47
MCV (f1) 82 – 98 82 – 98
MCH (pg) 27 – 32 27 – 32
MCHC (g/dlRBCs) 31.5 – 36 31.5 – 36
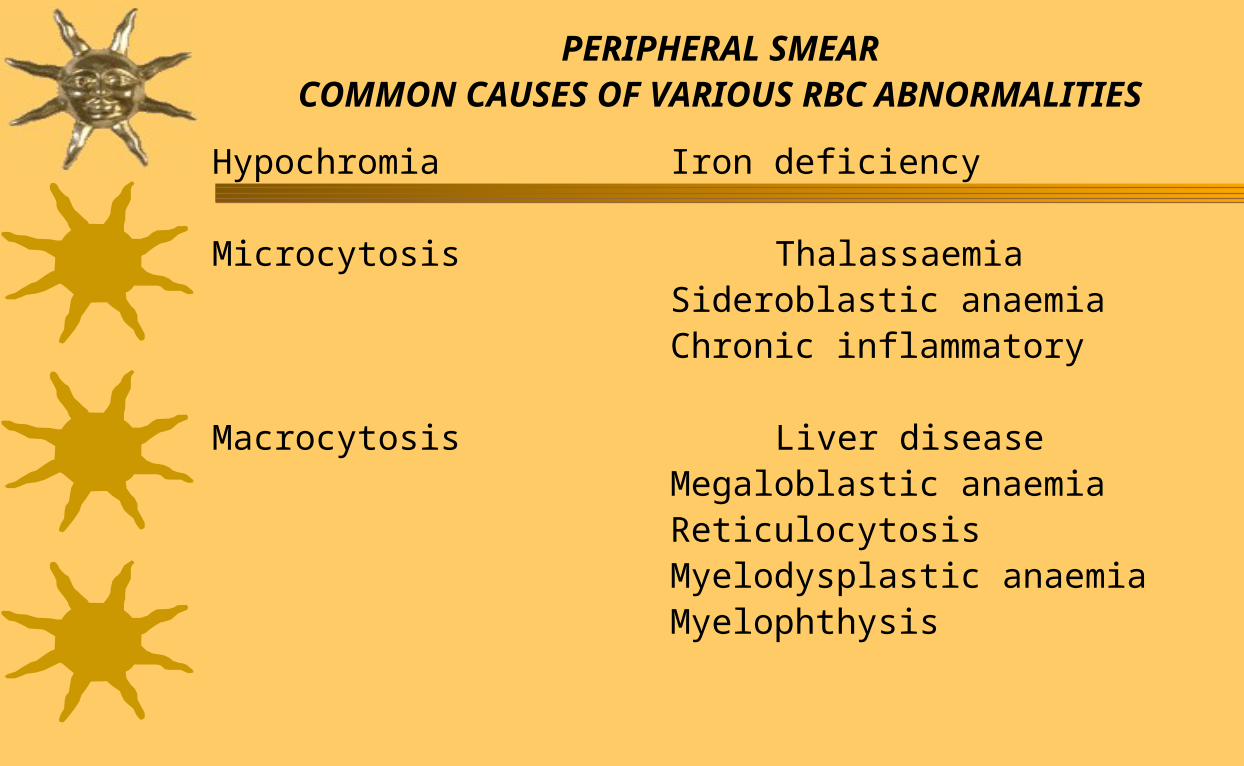
PERIPHERAL SMEARCOMMON CAUSES OF VARIOUS RBC ABNORMALITIES
Hypochromia Iron deficiency Microcytosis Thalassaemia
Sideroblastic anaemiaChronic inflammatory
Macrocytosis Liver diseaseMegaloblastic anaemiaReticulocytosisMyelodysplastic anaemiaMyelophthysis

Marked Amsocytosis Marked iron deficiencyAnd Poikilocytosis megaloblastic
MicroanglopathicHaemolysisLeukoerythroblastosisHaemoglobinopathies
Target cells Liver diseaseHaemoglobinC,AC, SS, SCPost SplenectomyThalassaemia

Spiculated RBCs Hereditary AcanthocytosisLiver diseaseRenal disease
Post SplenectomyHypothyroidismMicroangiopathicHaemolysis
Tear drop cells LeukoerythroblastosisMegaloblastic anaemiaThalassaemiaErythroleukaemia

Howell – Jolly bodies Post Splenectomy
Megaloblastic Anaemia
Erythroleukemia
Spherocytes Hereditary Sphenocytosis
Auto immune haemolysis
Haemoglobin C disorders CC, SC.
Ovalocytes Hereditary ovalocytosis
Megaloblastic anaemia
Iron deficiency
Thalassaemia.

1.Cell size – Microcytic Macrocytic Normocytic
2. What is the basic Mechanism of the anaemia.a. Decreased affective marrow productionb. Bleedingc. Haemolysis
- Reticulocyte index – used to assess the appropriateness of the bone marrow
response to the anaemia.- The rate of Hct fall
Anaemia with appropriate reticulocyte response in the absence of bleeding means haemolysis.
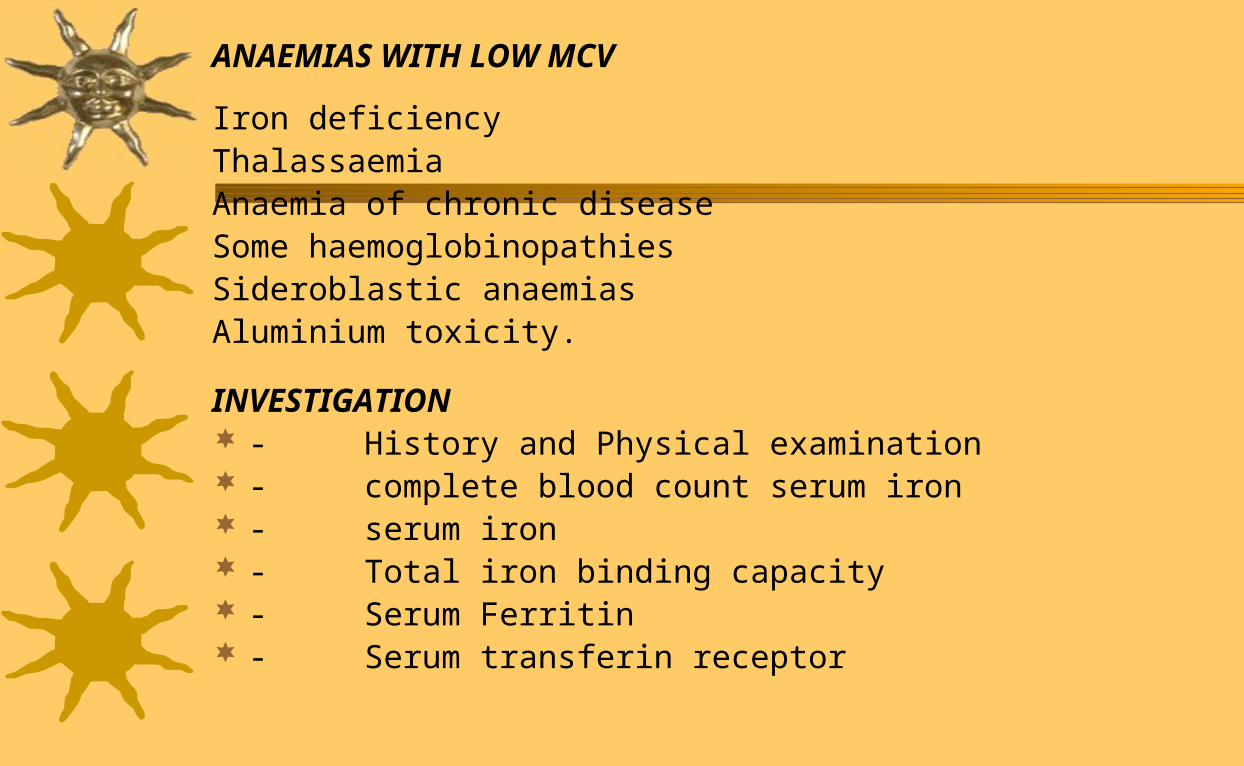
ANAEMIAS WITH LOW MCV
Iron deficiencyThalassaemiaAnaemia of chronic diseaseSome haemoglobinopathiesSideroblastic anaemiasAluminium toxicity.
INVESTIGATION - History and Physical examination - complete blood count serum iron - serum iron - Total iron binding capacity - Serum Ferritin - Serum transferin receptor

SPECIAL INVESTIGATIONGIT –Radioraphic studies, Endoscopy, Gastroscopy, Esophagoscopy,Exploratory laparotomy
Blood film
Anaemia with high MCV >100flDifferential diagnosis1. Liver disease2. Alcoholism3. No associated disease4. Myelodysplastic syndromes5. Drugs6. Megaloblastic anaemias

Serum Vit B12
RBC folic acid Assay Bone marrow Aspiration
CAUSES OF VIT B12 DEFICIENCY IRON STAINDietary, Gastric, Terminal Ileum disease, fish tape worm.Pancreatic insufficiencyDrugsCongenital (transcobalamin 11 deficiency)
HAEMOLYSIS AND BLEEDINGAnaemia with a Normal or slightly elevated MCV and an appropriate Reticulocyte index.
Haemolysis would lead to Reticulocytosis Appropriate bone marrow response

An anaemia with an appropriate reticulocyte response in the absence of alert bleeding suggests haemolysis.
Retic count in a Normal Hct – 1%.
If haemolysis is chronic (months to years) the marrow production may reach a level of production greater than 10 times normal.Reticulocyte = Reticulocyte X Pt hct
Normal hct

ALLOANTIBODY VERSUS AUTOANTIBODY ALLOANTIBODY AUTOANTIBODY
Direct coombs’ Frequently negative. Positive
May be positive if
sensitized foreign
red cells are still
circulating.
Indirect Coombs’ Positive Positive or Negative
Antibody Screen
(Panel) specificity is seen Panagglutination no
specificity.

ANAEMIA WITH A NORMAL MCV AND LOW RETICULOCYTE INDEX
DIFFERENTIAL DIAGNOSIS
Renal failureAnaemia of inflammatory disease (Anaemia of Malignancy.etc)Mild (early) iron deficiencyCombined iron deficiency and megaloblastic anaemia Sideroblastic anaemiaAplastic anaemiaBone marrow infiltration (myelophthisis)Bleeding or hemolysis plus one of the above

Intravascular Haemolysis
When RBC destruction is rapid and occurs primarily Within
the vascular space, diagnosis is relatively easy.one sees the
following.
1. Haemoglobinaemia
2. Haemoglobinuria
3. Haptoglobin saturation
4. Haemosiderinuria

Extravascular haemolysis1. Autoimmune haemolysis2. Delayed haemolytic transfusion reactions3. Haemoglobinopathies4. Hereditary spherocytosis5. Hypersplenism6. Haemolysis with liver disease
The following cell types are seen1. Spherocytes2. Schistocytes3. Spiculated cells4. Bite cells

Low Haematocrit (Haemoglobin)
*Corrected Reticulocyte Count (Reticulocyte Index)
Normal value 0.5 – 2.5%
INVESTIGATE FOR:-Haemolytic Anaemias
(See Chart II)
INVESTIGATE FOR:-
Acute Blood LossEarly Iron DeficiencyInfectionInflammationNeoplasiaRenal Disease(Iron Folic Acid/B12)Sideroblastic AnaemiaRed cell AplasiaAplastic Anaemia
INVESTIGATE FOR:-
Folic Acid DeficiencyVitamin B12 DeficiencyLiver DiseaseBone Marrow FailureSideroblastic AnaemiaHypothyroidismChronic AlcoholismDrugs
Elevated
Low / Normal
Peripheral Blood FilmNormocytesMacrocytes
INVESTIGATE FOR:-Iron DeficiencyThalassaemiaSideroblastic AnaemiaAnaemia of Chronic Disease
Microcytes
Reticulocyte Index = (Reti culocyte Count (%) x Pt. Haemoglobin (g/dl)Expected Normal Haemoglobin (g/dl)
+ Correction Factor for Premature Release
+ Haemoglobin (g/dl)10 – 117 – 9<7
Correction Factor1.52.02.5
FLOW CHART FOR INVESTIGATING ANAEMIA
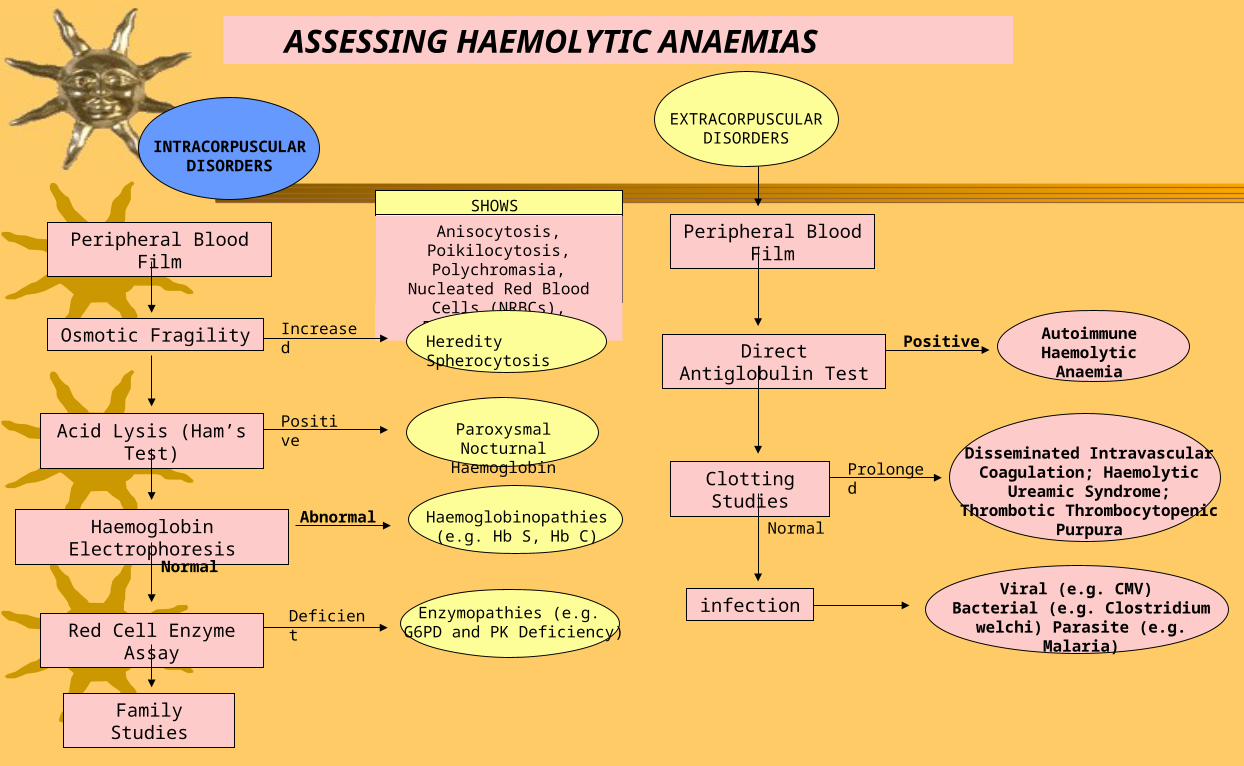
INTRACORPUSCULAR DISORDERS
Peripheral Blood Film
Osmotic Fragility
Acid Lysis (Ham’s Test)
Haemoglobin Electrophoresis
Red Cell Enzyme Assay
Family Studies
Normal
Anisocytosis, Poikilocytosis, Polychromasia, Nucleated Red
Blood Cells (NRBCs), Fragmented Cells
SHOWS
Heredity Spherocytosis
Paroxysmal Nocturnal Haemoglobin
Haemoglobinopathies (e.g. Hb S, Hb C)
Enzymopathies (e.g. G6PD and PK Deficiency)
Increased
Positive
Abnormal
Deficient
EXTRACORPUSCULAR DISORDERS
Peripheral Blood Film
Direct Antiglobulin Test
Clotting Studies
infection
Autoimmune Haemolytic Anaemia
Disseminated Intravascular Coagulation; Haemolytic Ureamic
Syndrome; Thrombotic Thrombocytopenic Purpura
Viral (e.g. CMV) Bacterial (e.g. Clostridium welchi)
Parasite (e.g. Malaria)
Positive
Prolonged
Normal
ASSESSING HAEMOLYTIC ANAEMIAS

Anaemia of chronic disease is characterized by1. Low serum iron concentration and defective
incorporation into haemoglobin despite adequate bone marrow stores of iron
2. A blunted erythropoietin response to anaemia. When mild it is normocytic normochromic but it can become severe and become hypochromic microcytic
3. Absoulte reticulocyte count is reduced, also ass.features indicative of chronic inflammation may be present.e.g. Neutrophilia, thrombocytosis, increased rouleaux formation.

Serum iron, serum transferin, are reduced while total iron binding capacity is increased.
Serum ferritin is increased, increase ESR,
plasma viscosity, reduced albumin and increased
fibrinogen 2 macroglobulin and - globulins are
increased