
An update on core needle biopsy for radiologically detected breast lesions
6
2340 An Update on Core Needle Biopsy for Radiologically Detected Breast Lesions Mai Nguyen, M.D.' Marie M. McCornbs, M.D? Sara Ghandehari' Andrea Kim, 8.s.l Hejing Wang, Ph.o.3 Sanford H. Barsky, M.D; Susan Love, M.D.~ Lawrence W. Bassett, M.D* ' Department of Surgery, UCLA, Los Angeles, California. Department of Radiology, UCLA, Los Angeles, Department of Mathematics, UCLA, Los Department of Pathology, UCLA, Los Angeles, California. Angeles, California. California. A portion of the manuscript was previously pre- sented by Dr. McCombs. Dr. Nguyen is a recipient of the American Cancer Society Junior Faculty Research Award. This work is also supported by the ACS Institutional Grant No. IRG-l31N, the UCLA Jonsson Com- prehensive Cancer Center, and the Stein-Oppen- heim Foundation. Address for reprints: Mai Nguyen, M.D., UCLA Surgery/Oncology, CHS 54-140, Box 951782, Los Angeles, CA 90095-1782. Received May 22, 1996; revision received Au- gust 21, 1996; accepted August 21, 1996. BACKGROUND. Traditionally, radiologically detected lesions of the breast have been evaluated by open surgical biopsy with wire localization. Recently, core needle biopsy has been introduced as an alternative to open surgical biopsy. The authors evaluated their own results with long term follow-up after core needle biopsy and reviewed the experience of other physicians with this new technique. METHODS. Four hundred thirty-one core needle biopsies performed at UCLA were analyzed. The outcome of these cases was determined by either surgery or long term follow-up. Statistical analysis was performed to determine the accuracy of the method. RESULTS. Definitive outcome was obtained in 96% of the core needle biopsy cases, with a median follow-up time of 18 months (range, 6-38 months). The authors achieved a sensitivity of 99% and a specificity of 100%. The false-negative rate was 1.7%. There were no complications in this series. CONCLUSIONS. Core needle biopsy is a highly accurate and safe method for the diagnosis of radiologically detected lesions of the breast. Cancer 1996; 78:2340-5. 0 1996 American Cancer Society. KEYWORDS: core needle biopsy, breast carcinoma, mammogram, cancer diagnosis. reast carcinoma is the most common malignancy among women B in North America. Multiple randomized clinical trials have dem- onstrated that screening mammography reduces breast carcinoma mortality by approximately 25%.' However, the vast majority of the biopsies of these lesions generated by screening mammography show only benign processes in the breast.' Traditionally, these biopsies are performed in the operating room by a surgeon after wire localization in the radiology suite. The surgical procedure leaves the woman scarred physically and sometimes radiologically, and may deter some women from obtaining screening mammograms. In addition, the cost of benign surgical biopsies puts a great economic burden on screening programs. Recently, core needle biopsy of radiologically detected lesions offers an attractive alternative to surgical biopsy because it leaves no scar, causes less morbidity, and is less expen~ive.~ Several series using core needle biopsy have been published over the last few years, show- ing high percentages of sensitivity and ~pecificity."'~ Critics of the technique point out that many of these series were affected by selec- tion bias andlor poor follow-~p.'~ As a result, there are many physi- cians who are not convinced that anything less than a complete exci- sion of the lesion is acceptable, and thousands of women continue to undergo open surgical biopsies for benign lesions of the breast. Therefore, we began a program at the UCLA Medical Center of routine core needle biopsies for radiologically detected lesions of the 0 1996 American Cancer Society
-
Upload
mai-nguyen -
Category
Documents
-
view
214 -
download
2
Transcript of An update on core needle biopsy for radiologically detected breast lesions
2340
An Update on Core Needle Biopsy for Radiologically Detected Breast Lesions
Mai Nguyen, M.D.'
Marie M. McCornbs, M.D?
Sara Ghandehari' Andrea Kim, 8.s.l Hejing Wang, Ph.o.3
Sanford H. Barsky, M.D;
Susan Love, M.D.~
Lawrence W. Bassett, M.D*
' Department of Surgery, UCLA, Los Angeles, California.
Department of Radiology, UCLA, Los Angeles,
Department of Mathematics, UCLA, Los
Department of Pathology, UCLA, Los Angeles,
California.
Angeles, California.
California.
A portion of the manuscript was previously pre- sented by Dr. McCombs.
Dr. Nguyen is a recipient of the American Cancer Society Junior Faculty Research Award. This work is also supported by the ACS Institutional Grant No. IRG-l31N, the UCLA Jonsson Com- prehensive Cancer Center, and the Stein-Oppen- heim Foundation.
Address for reprints: Mai Nguyen, M.D., UCLA Surgery/Oncology, CHS 54-140, Box 951782, Los Angeles, CA 90095-1782.
Received May 22, 1996; revision received Au- gust 21, 1996; accepted August 21, 1996.
BACKGROUND. Traditionally, radiologically detected lesions of the breast have been evaluated by open surgical biopsy with wire localization. Recently, core needle biopsy has been introduced as an alternative to open surgical biopsy. The authors evaluated their own results with long term follow-up after core needle biopsy and reviewed the experience of other physicians with this new technique. METHODS. Four hundred thirty-one core needle biopsies performed at UCLA were analyzed. The outcome of these cases was determined by either surgery or long term follow-up. Statistical analysis was performed to determine the accuracy of the method. RESULTS. Definitive outcome was obtained in 96% of the core needle biopsy cases, with a median follow-up time of 18 months (range, 6-38 months). The authors achieved a sensitivity of 99% and a specificity of 100%. The false-negative rate was 1.7%. There were no complications in this series. CONCLUSIONS. Core needle biopsy is a highly accurate and safe method for the diagnosis of radiologically detected lesions of the breast. Cancer 1996; 78:2340-5. 0 1996 American Cancer Society.
KEYWORDS: core needle biopsy, breast carcinoma, mammogram, cancer diagnosis.
reast carcinoma is the most common malignancy among women B in North America. Multiple randomized clinical trials have dem- onstrated that screening mammography reduces breast carcinoma mortality by approximately 25%.' However, the vast majority of the biopsies of these lesions generated by screening mammography show only benign processes in the breast.' Traditionally, these biopsies are performed in the operating room by a surgeon after wire localization in the radiology suite. The surgical procedure leaves the woman scarred physically and sometimes radiologically, and may deter some women from obtaining screening mammograms. In addition, the cost of benign surgical biopsies puts a great economic burden on screening programs.
Recently, core needle biopsy of radiologically detected lesions offers an attractive alternative to surgical biopsy because it leaves no scar, causes less morbidity, and is less expen~ive.~ Several series using core needle biopsy have been published over the last few years, show- ing high percentages of sensitivity and ~pecificity."'~ Critics of the technique point out that many of these series were affected by selec- tion bias andlor poor follow-~p. '~ As a result, there are many physi- cians who are not convinced that anything less than a complete exci- sion of the lesion is acceptable, and thousands of women continue to undergo open surgical biopsies for benign lesions of the breast.
Therefore, we began a program at the UCLA Medical Center of routine core needle biopsies for radiologically detected lesions of the
0 1996 American Cancer Society

Core Needle Biopsy for Breast LesionsINguyen et al. 2341
TABLE 1 Final Assessment Categories of the American College of Radiology Breast Imaging Reporting and Data System
Category Assessment Description of finding
1 Negative There is nothing on which
2 Benign finding A definitely benign finding
3 Probably benign Very high prcibabiiity of
to comment.
is described.
finding being benign; short term follow-up is recommend to establish stability.
4 Suspicious Not characteristic, but has abnormaliv a reasonable
probability of being malignant; biopsy
5 should be urged.
Highly suggestive High probability of being
action should be taken. of malignancy cancer: appropriate
breast, with long term follow-up. This article reports the results of our review of 431 core needle biopsies and also presents a review of the recent literature on this subject.
METHODS Patient Population At the UCLA Medical Center, we routinely grouped mammographic abnormalities into one of the five final assessment categories of the American College of Ra- diology Breast Imaging Reporting and Data System (Table l).”’ Cases with findings that were “highly sug- gestive of malignancy” or “suspicious” for malignancy were considered appropriate candidates for core nee- dle biopsy. Women with abnormalities categorized as “probably benign” were usually managed by a follow- up mammogram after six months, with core needle biopsy limited to those cases in which the woman was extremely anxious. There were no other selection criteria used. From December 1992 to June 1995, we performed 431 core biopsies on 408 patients at the UCLA Medical Center. Twenty-one patients had two biopsies for two separate lesions, and one patient had three biopsies for three separate lesions. Three hun- dred seventy-eight were performed under stereotactic mammographic guidance and 53 under ultrasound guidance.
Technique of Core Needle Biopsy Mammographic guidance was performed with a dedi- cated stereotactic prone biopsy unit (Stereo Guide DSM, LORAD, Danbury, CT). The core biopsies were
accomplished using either a Manan 14-gauge needle (Manan Medical Products, Northbrook, IL) or a Bard 14-gauge needle (Bard Radiology, Covington, GA). If the mammographic lesion had calcifications, a speci- men radiograph was taken to verify that there were calcifications within the specimen. Ultrasound-guided core biopsies were performed on a Diasonics VST (Di- asonics, Milpitas, CA) using one of the following 14- gauge needles: Bard monopty, ASAP (Medi-Tech, Wa- tertown, MA) with Hawkins Blunt needle introducer (Medical Device Technologies, Gainesville, FL), or Ma- nan. Five specimens were obtained routinely for de- tection of masses, asymmetric densities, or architec- tural distortions. Between 5 and 10 biopsy specimens were obtained for detection of calcifications.
Patient Management Imaging and histologic findings for each patient were reviewed at a weekly conference so that any dis- cordances could be identified. If the core biopsy showed malignant cells, definitive treatments, includ- ing surgery, were carried out. If the core biopsy showed atypical ductal hyperplasia (ADHI, an open excisional biopsy was recommended to the patient. If the ini- aging and histologic findings were discordant, e.g., if the radiologic appearance was highly suspicious and the pathology result showed benign cells, an open ex- cisional biopsy was also recommended. Finally, if the imaging and histologic findings were concordant and benign, radiologic surveillance, beginning with a six month follow-up, was recommended and performed for all except the 18 patients who were lost to follow- up (these patients presumably moved without notify- ing us of their new addresses or phone numbers). For patients who did not have surgery, follow-up data was obtained by review of UCLA medical records and by telephone or mail contact with the patients.
Data Analysis A true-positive core needle biopsy showed malignant cells and was later interpreted during surgery as intra- ductal or invasive carcinoma. A false-positive core needle biopsy did not show malignancy during subse- quent surgery. A core needle biopsy diagnosis was considered to be a false-negative when it was originally interpreted as benign by the pathologist and subse- quent excisional biopsy showed malignancy. A true- negative core needle biopsy diagnosis was indeed be- nign at surgery or unchanged on a follow-up mammo- gram. The core needle biopsies that revealed ADH were analyzed separately. Sensitivity was calculated by dividing the number of true-positives by all cases of malignancies detected during surgical excision. Speci- ficity was calculated by dividing the number of true-

2342 CANCER December 1, 1996 / Volume 78 / Number 11
TABLE 2 Follow-Up Outcome of All Core Biopsies
Surgery after Core biopsies Core diagnosis Initial surgery FOIIOW-UP follow-up
431+ Malignant: 1791 Malignant: 178 No residual tumor: 1
Atypical: 1 Benign: 8
Benign: 22 Change: 1+ Malignant: 1
Atypical: 13+ Malignant: 4
Benign: 239- Malignant: 3+ Benign: 195
No flu: 18
Total 431 217 214 1
negatives by all cases of benign lesions confirmed by surgical excision or follow-up.
For diagnosis of malignancy, kappa statistics were used to assess the degree of agreement between core needle biopsy and information from surgery or follow- up. A chi-square test was used to evaluate the association among several categorical variables. The continuity cor- rected score method was used to compute the 95% bino- mial confidence interval for the estimated rates. Logistic regression was used to examine the association of radio- logic score and type with cancer diagnosis.
RESULTS Confirmation of core needle biopsy results, by either surgery or follow-up, was achieved for 96% of the pa- tient population. Of those patients who did not have surgery and entered a surveillance program, the me- dian follow-up time was 18 months. The minimum follow-up time was 6 months, and the maximum was 38 months.
Table 2 summarizes the results of the 431 core needle biopsies. One hundred seventy-nine cases showed malignant cells. All of these patients pro- ceeded to surgical excision, where it was confirmed that 178 specimens contained cancer. One patient had a mastectomy without localization, and routine exami- nation of the surgical specimen did not reveal any residual tumor. Two hundred thirty-nine core needle biopsy patients showed benign cells. Of these, 25 un- derwent immediate surgery because of either radio- logic discordance or patient anxiety. For 3 of these 25 patients, cancer was found in the surgical specimens. All three of them presented with calcification as the abnormality found on mammograms. It was recom- mended that they undergo surgery because the core needle biopsy specimens did not contain calcification on histologic exam. During surgery, two were found to have comedo-type ductal carcinoma in situ (DCIS),
and one had infiltrating ductal carcinoma. The rest of the patients with benign core needle biopsies were advised to enter a surveillance program that included follow-up mammograms. Of these 214 patients, 195 did not show any changes in the follow-up mammo- grams that suggested malignancy. Eighteen patients were lost to follow-up. One patient had a suspicious mammogram 9 months after her core needle biopsy. She then underwent surgery, where DCIS was discov- ered. Overall, there were four false-negatives.
There were 13 patients whose core biopsies showed ADH. All of them had subsequent surgery, where histologic examination revealed cancer in 4 pa- tients (31%), benign lesions in 8, and ADH in l . Four of 26 patients (15%) had DCIS on their core needle biopsies and then had infiltrating carcinoma at the time of surgery. Two of these four patients had mostly DCIS with microscopic foci of microinvasion on the surgical specimens. The other two patients had infil- trating carcinoma with extensive intraductal compo- nents. All of these patients had calcification as the presenting abnormality. All who had infiltrating carci- noma on their core needle biopsies indeed had the same type on their surgical specimens, except for the one patient with no residual tumor discussed earlier.
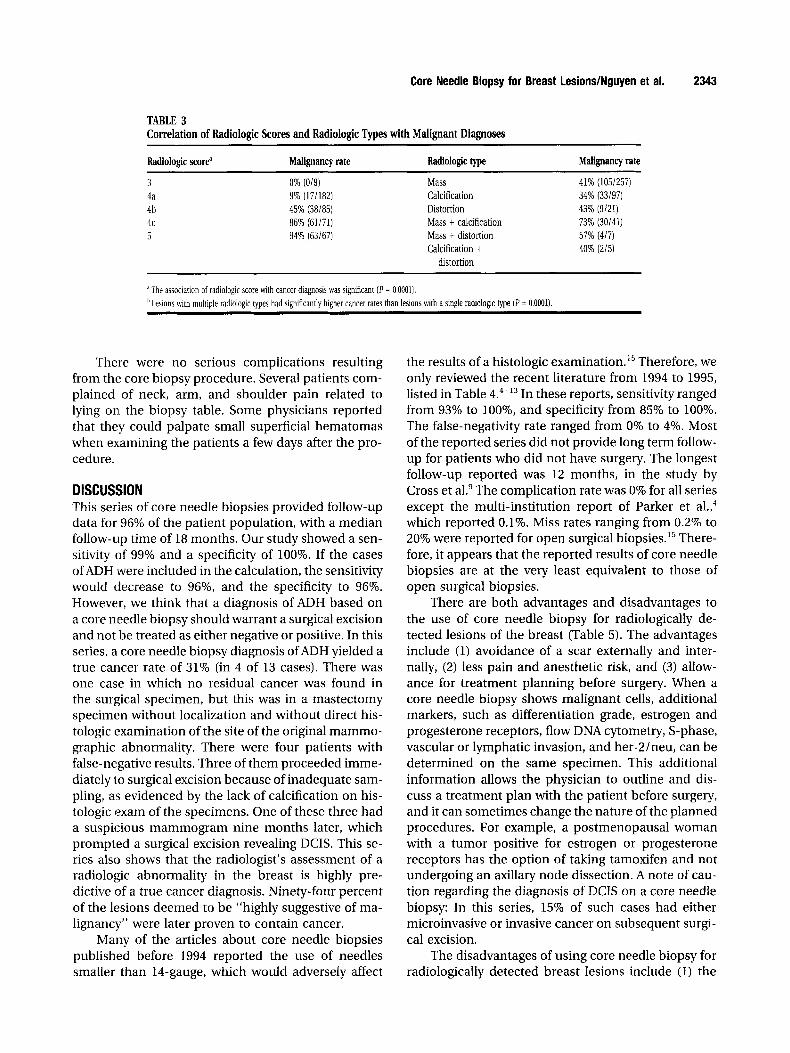
Table 3 shows that higher radiologic scores corre- lated with a diagnosis of malignancy. This correlation was statistically significant, with P = 0.0001. In addi- tion, analysis of radiologic types showed that tumors with multiple radiologic manifestations had higher cancer rates than those with single radiologic manifes- tations ( P = 0.0001). The combination of a mass with calcification was the most likely to be malignant (73%). However, logistic regression analysis showed that after adjustment for radiologic scores, there was no signifi- cant association between radiologic type and a cancer diagnosis. In this series, the radiologists seem to have been very accurate in their predictions of malignancy.
Core Needle Biopsy for Breast LesionslNguyen et al. 2343
TABLE 3 Correlation of Radiologic Scores and Radiologic Types with Malignant Diagnoses
Radiologic scorea Malignancy rate Radiologic type Malignancy rate
3 4a 4b 4c 5
0% (019) 9% (171182) 45% (38185) 86% 61/71) 94% (63/67)
Mass 41% (105/257) Calcification 34% (33/97) Distortion 43% (9/21) Mass t calcification 73% (30/41) Mass t distortion 57% (4/7) Calcification t 40% (U5)
distortion
The association of radiologic score with cancer diagnosis was significant ( P = 0.0001). ‘I Lesions with multiple radiologic types had significantly higher cancer rates than lesions with a single radiologic type ( P = 0.0001).
There were no serious complications resulting from the core biopsy procedure. Several patients com- plained of neck, arm, and shoulder pain related to lying on the biopsy table. Some physicians reported that they could palpate small superficial hematomas when examining the patients a few days after the pro- cedure.
DISCUSSION This series of core needle biopsies provided follow-up data for 96% of the patient population, with a median follow-up time of 18 months. Our study showed a sen- sitivity of 99% and a specificity of 100%. If the cases of ADH .were included in the calculation, the sensitivity would decrease to 96%, and the specificity to 96%. However, we think that a diagnosis of ADH based on a core needle biopsy should warrant a surgical excision and not be treated as either negative or positive. In this series, a core needle biopsy diagnosis of ADH yielded a true cancer rate of 31% (in 4 of 13 cases). There was one case in which no residual cancer was found in the surgical specimen, but this was in a mastectomy specimen without localization and without direct his- tologic examination of the site of the original mammo- graphic abnormality. There were four patients with false-negative results. Three of them proceeded imme- diately to surgical excision because of inadequate sam- pling, as evidenced by the lack of calcification on his- tologic exam of the specimens. One of these three had a suspicious mammogram nine months later, which prompted a surgical excision revealing DCIS. This se- ries also shows that the radiologist’s assessment of a radiologic abnormality in the breast is highly pre- dictive of a true cancer diagnosis. Ninety-four percent of the lesions deemed to be “highly suggestive of ma- lignancy” were later proven to contain cancer.
Many of the articles about core needle biopsies published before 1994 reported the use of needles smaller than 14-gauge, which would adversely affect
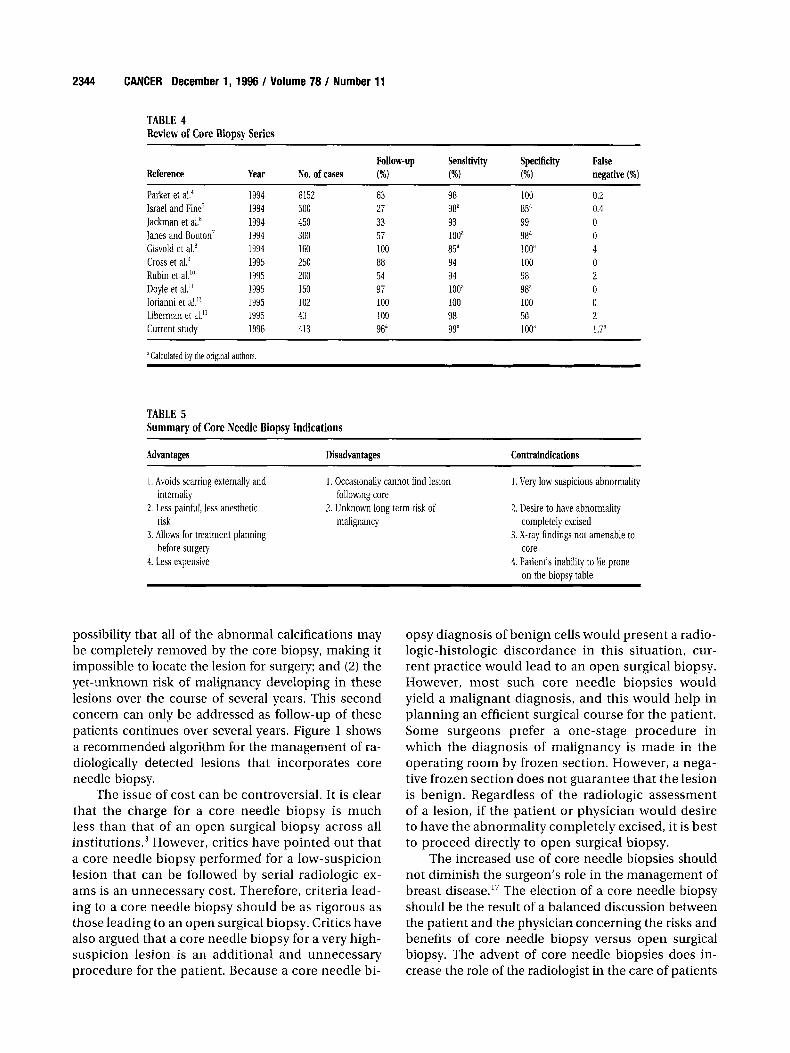
the results of a histologic e~amination.’~ Therefore, we only reviewed the recent literature from 1994 to 1995, listed in Table 4.4-13 In these reports, sensitivity ranged from 93% to loo%, and specificity from 85% to 100%. The false-negativity rate ranged from 0% to 4%. Most of the reported series did not provide long term follow- up for patients who did not have surgery. The longest follow-up reported was 12 months, in the study by Cross et al.’ The complication rate was 0% for all series except the multi-institution report of Parker et al.,4 which reported 0.1%. Miss rates ranging from 0.2% to 20% were reported for open surgical biopsies. l5 There- fore, it appears that the reported results of core needle biopsies are at the very least equivalent to those of open surgical biopsies.
There are both advantages and disadvantages to the use of core needle biopsy for radiologically de- tected lesions of the breast (Table 5 ) . The advantages include (1) avoidance of a scar externally and inter- nally, (2) less pain and anesthetic risk, and (3) allow- ance for treatment planning before surgery. When a core needle biopsy shows malignant cells, additional markers, such as differentiation grade, estrogen and progesterone receptors, flow DNA cytometry, S-phase, vascular or lymphatic invasion, and her-2/neu, can be determined on the same specimen. This additional information allows the physician to outline and dis- cuss a treatment plan with the patient before surgery, and it can sometimes change the nature of the planned procedures. For example, a postmenopausal woman with a tumor positive for estrogen or progesterone receptors has the option of taking tamoxifen and not undergoing an axillary node dissection. A note of cau- tion regarding the diagnosis of DCIS on a core needle biopsy: In this series, 15% of such cases had either microinvasive or invasive cancer on subsequent surgi- cal excision.
The disadvantages of using core needle biopsy for radiologically detected breast lesions include (1) the
2344 CANCER December 1, 1996 I Volume 78 I Number 11
TABLE 4 Review of Core Biopsy Series
FOUOW-UP Sensitivity Specificity False Reference Year No. of cases (%I (%I (%I negative (%I Parker et al." Israel and Fine' I a c h a n et lanes and Bouton' Gisvold et al! Cross et al! Rubin et al."' Doyle et al." lorianni et d.'' Liberman et at" Current study
1994 6152 1994 500 1994 450 1994 300 1994 160 1995 250 1995 200 1995 150 1995 102 1995 43 1996 413
63 27 33 57 100 88 54 97 100 100 96a
98 9Ba 93 looa
94 94 looa 100 98 9ga
100 8 Y 99 98" 100" 100 98 98a 100 50 looa
0.2 0.4 0 0 4 0 2 0 0 2 1.7a
'Calculated bv the orieinal authors
TABLE 5 Summary of Core Needle Biopsy Indications
Advantages Disadvantages Contraindications
I . Avoids scarring externally and
2. Less painful, less anesthetic
3. Allows for treatment planning
1. Less expensive
1. Occasionally cannot find lesion
2. Unknown long term risk of
1. Very low suspicious abnormality
2. Desire to have abnormality
3. X-ray findings not amenable to
4. Patient's inability to lie prone
internally following core
risk malignancy completely excised
before surgery core
on the biousv table
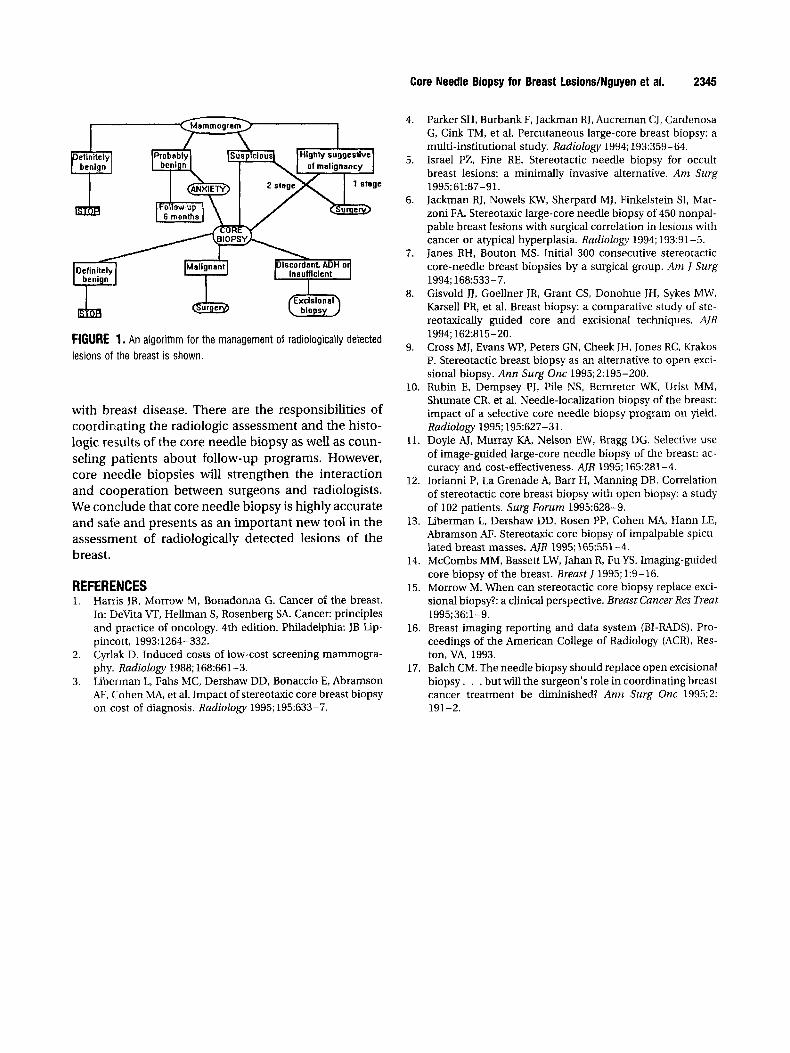
possibility that all of the abnormal calcifications may be completely removed by the core biopsy, making it impossible to locate the lesion for surgery; and (2) the yet-unknown risk of malignancy developing in these lesions over the course of several years. This second concern can only be addressed as follow-up of these patients continues over several years. Figure 1 shows a recommended algorithm for the management of ra- diologically detected lesions that incorporates core needle biopsy.
The issue of cost can be controversial. It is clear that the charge for a core needle biopsy is much less than that of an open surgical biopsy across all institution^.^ However, critics have pointed out that a core needle biopsy performed for a low-suspicion lesion that can be followed by serial radiologic ex- ams is an unnecessary cost. Therefore, criteria lead- ing to a core needle biopsy should be as rigorous as those leading to an open surgical biopsy. Critics have also argued that a core needle biopsy for a very high- suspicion lesion is an additional and unnecessary procedure for the patient. Because a core needle bi-
opsy diagnosis of benign cells would present a radio- logic-histologic discordance in this situation, cur- rent practice would lead to an open surgical biopsy. However, most such core needle biopsies would yield a malignant diagnosis, and this would help in planning an efficient surgical course for the patient. Some surgeons prefer a one-stage procedure in which the diagnosis of malignancy is made in the operating room by frozen section. However, a nega- tive frozen section does not guarantee that the lesion is benign. Regardless of the radiologic assessment of a lesion, if the patient or physician would desire to have the abnormality completely excised, it is best to proceed directly to open surgical biopsy.
The increased use of core needle biopsies should not diminish the surgeon's role in the management of breast di~ease. '~ The election of a core needle biopsy should be the result of a balanced discussion between the patient and the physician concerning the risks and benefits of core needle biopsy versus open surgical biopsy. The advent of core needle biopsies does in- crease the role of the radiologist in the care of patients
Core Needle Biopsy for Breast Lesions/Nguyen et al. 2345
FIGURE 1. An algorithm for the management of radiologically detected lesions of the breast is shown.
with breast disease. There are the responsibilities of coordinating the radiologic assessment and the histo- logic results of the core needle biopsy as well as coun- seling patients about follow-up programs. However, core needle biopsies will strengthen the interaction and cooperation between surgeons and radiologists. We conclude that core needle biopsy is highly accurate and safe and presents as an important new tool in the assessment of radiologically detected lesions of the breast.
REFERENCES 1. Harris JR, Morrow M, Bonadonna G. Cancer of the breast.
In: DeVita VT, Hellman S, Rosenberg SA. Cancer: principles and practice of oncology. 4th edition. Philadelphia: JB Lip- pincott, 1993:1264-332. Cyrlak D. Induced costs of low-cost screening mammogra- phy. Radiology 1988; 168:661-3. Liberman L, Fahs MC, Dershaw DD, Bonaccio E, Abramson AF, C:ohen MA, et al. Impact of stereotaxic core breast biopsy on cost of diagnosis. Radiology 1995; 195:633-7.
2.
3.
4. Parker SH, Burbank F, Jackman RJ, Aucreman CJ, Cardenosa G, Cink TM, et al. Percutaneous large-core breast biopsy: a multi-institutional study. Radiology 1994; 193:359-64. Israel PZ, Fine RE. Stereotactic needle biopsy for occult breast lesions: a minimally invasive alternative. Am Surg 1995; 61:87-91. Jackman RJ, Nowels KW, Sherpard MJ, Finkelstein SI, Mar- zoni FA. Stereotaxic large-core needle biopsy of 450 nonpal- pable breast lesions with surgical correlation in lesions with cancer or atypical hyperplasia. Radiology 1994; 193:91-5. Janes RH, Bouton MS. Initial 300 consecutive stereotactic core-needle breast biopsies by a surgical group. Am J Surg
Gisvold JJ, Goellner JR, Grant CS, Donohue JH, Sykes MW, Karsell PR, et al. Breast biopsy: a comparative study of ste- reotaxically guided core and excisional techniques. AJR
Cross MJ, Evans WP, Peters GN, Cheek JH, Jones RC, Krakos P. Stereotactic breast biopsy as an alternative to open exci- sional biopsy. Ann Surg Onc 1995;2:195-200.
10. Rubin E, Dempsey PJ, Pile NS, Bernreter WK, Urist MM, Shumate CR, et al. Needle-localization biopsy of the breast: impact of a selective core needle biopsy program on yield. Radiology 1995; 195:627-31.
11. Doyle AJ, Murray KA, Nelson EW, Bragg DG. Selective use of image-guided large-core needle biopsy of the breast: ac- curacy and cost-effectiveness. AJR 1995; 165281-4.
12. Iorianni P, La Grenade A, Barr H, Manning DB. Correlation of stereotactic core breast biopsy with open biopsy: a study of 102 patients. Surg Forum 1995:628-9.
13. Liberman L, Dershaw DD, Rosen PP, Cohen MA, Hann LE, Abramson AF. Stereotaxic core biopsy of impalpable spicu- lated breast masses. AIR 1995; 1651551-4.
14. McCombs MM, Bassett LW, Jahan R, Fu YS. Imaging-guided core biopsy of the breast. Breast f 1995; 1:9-16.
15. Morrow M. When can stereotactic core biopsy replace exci- sional biopsy?: a clinical perspective. Breast Cancer Res Treat
16. Breast imaging reporting and data system (BI-RADS). Pro- ceedings of the American College of Radiology (ACR), Res- ton, VA, 1993.
17. Balch CM. The needle biopsy should replace open excisional biopsy. . . but will the surgeon’s role in coordinating breast cancer treatment be diminished? Ann Surg Onc 1995;2: 191-2.
5.
6.
7.
1994; 168:533-7. 8.
1994; 1622315-20. 9.
1995; 36: 1-9.


















