An Unusual Case Of Recurrent Atrial Fibrillation
15
An Unusual Case Of Recurrent Atrial Fibrillation Mark Linzer MD Section of GIM Scholars GIM Conference 4-16-08
-
Upload
samson-allison -
Category
Documents
-
view
26 -
download
0
description
An Unusual Case Of Recurrent Atrial Fibrillation. Mark Linzer MD Section of GIM Scholars GIM Conference 4-16-08. Financial Disclosure. No support for this talk. Learning Objectives. To learn an uncommon cause of recurrent atrial fibrillation More objectives after the case report. - PowerPoint PPT Presentation
Transcript of An Unusual Case Of Recurrent Atrial Fibrillation

An Unusual Case Of Recurrent Atrial Fibrillation
Mark Linzer MDSection of GIM Scholars
GIM Conference 4-16-08

Financial Disclosure
No support for this talk

Learning Objectives
To learn an uncommon cause of recurrent atrial fibrillation
More objectives after the case report
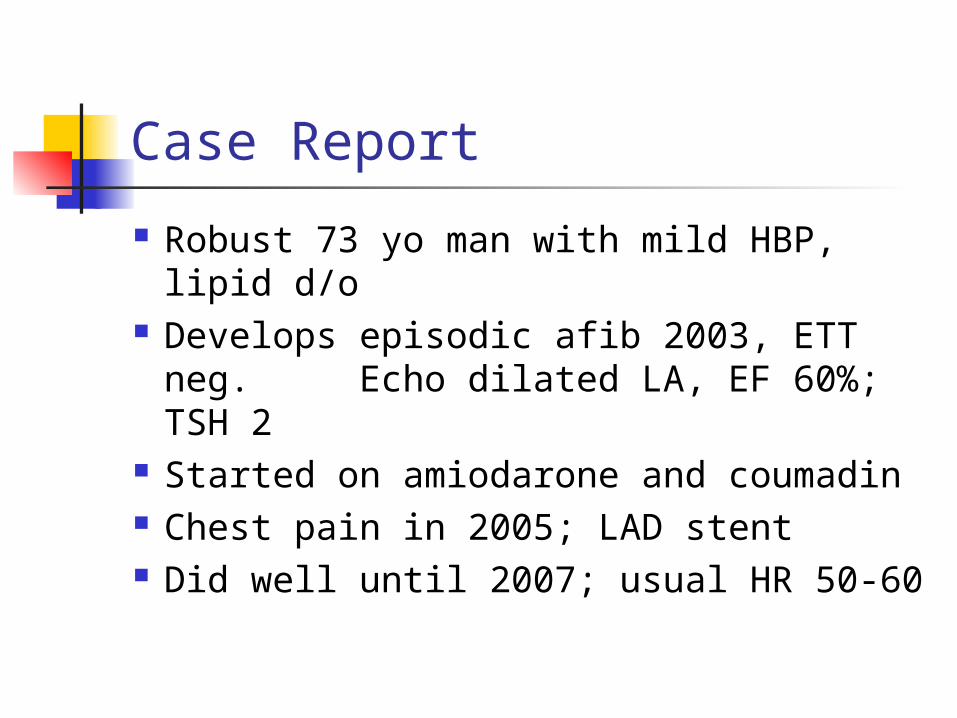
Case Report
Robust 73 yo man with mild HBP, lipid d/o
Develops episodic afib 2003, ETT neg. Echo dilated LA, EF 60%; TSH 2
Started on amiodarone and coumadin Chest pain in 2005; LAD stent Did well until 2007; usual HR 50-60

2007: Abnormal Liver Function Tests
7/07 ALT 160, AST 80; amio discontinued.
10/07 frequent afib, SOB, anxiety. PMH: CAD, BPH, GERD, lipids, OA Meds: ASA, lipitor, doxazosin,
lisinopril, metoprolol, PPI, warfarin PE: BP 130/70, pulse 60-80, o/w neg

Next steps? (Don’t turn page)

Objectives:
Know two types of amiodarone-induced thyrotoxocosis (AIT)
Know how to attempt to distinguish them
Know the treatments

Work Up TSH 0, FT4 high; LFTs near nl; amio zero Paged Endocrine, bumped beta blockers Scan arranged for Txgiving wkend Uptake 1% (very low) Dx: amiodarone induced thyroiditis
(likely) Rx: high doses steroids, beta blockers

Amio-induced thyrotoxicosis (AIT) Prevalence 3% (2-3 yrs after Rx onset) Type 1: exacerbation of latent Graves Type 2: drug-induced thyroiditis (majority) Some patients have mixed picture Amio half life 100 days Note amio and hyperthyroidism can
increase sensitivity to warfarin* Kurnik et al. Medicine. 2004;83:107-113.

Amio and iodine
Very high iodine content (20x usual)* Can cause hypo or hyperthyroidism Has beta blocking properties and
decreases T4 to T3 conversion: can mask hyperthyroidism stopping amio may make sx worse. *UpToDate, Ross DS. Amio and thyroid dysfunction.
2008.
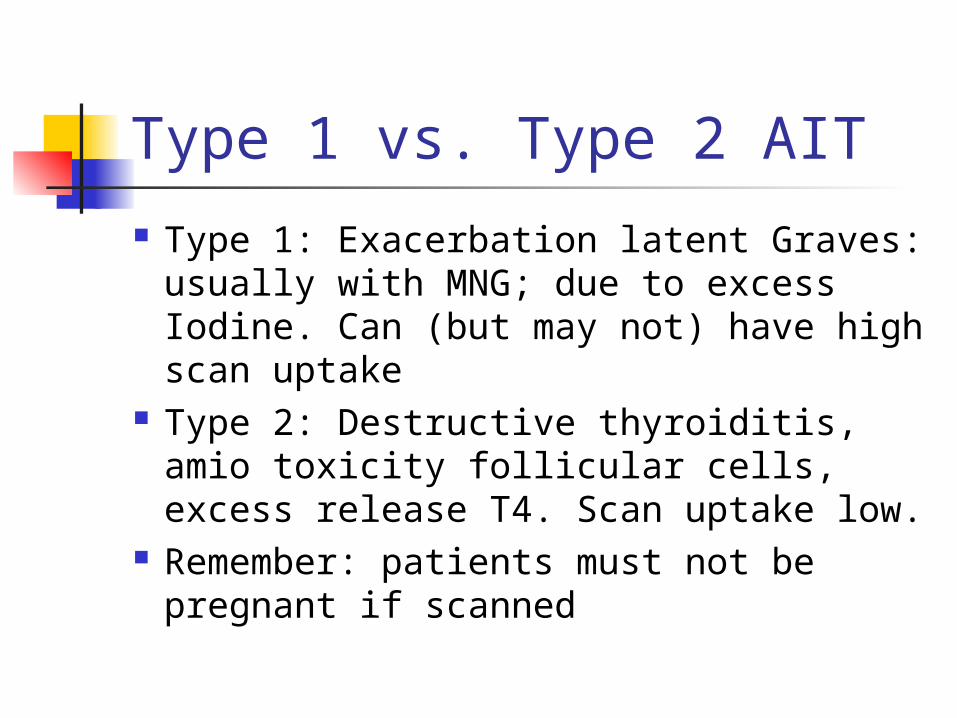
Type 1 vs. Type 2 AIT
Type 1: Exacerbation latent Graves: usually with MNG; due to excess Iodine. Can (but may not) have high scan uptake
Type 2: Destructive thyroiditis, amio toxicity follicular cells, excess release T4. Scan uptake low.
Remember: patients must not be pregnant if scanned

Ways to distinguish Thyroid scan: low uptake Type 2
(thyroiditis); can be low Type 1 (amio competes with tracer)
Other methods*: Color flow doppler: 80% sensitive Type 1 due to
increased vascularity Goiter (type 1) IL-6 elevated in Type 2 Amio duration longer (>2 yrs) in Type 2 Response to prednisone implies Type 2
*Basaria S, Cooper DC. Amiodarone and the thyroid. Am J Med. 2005;118:706-14
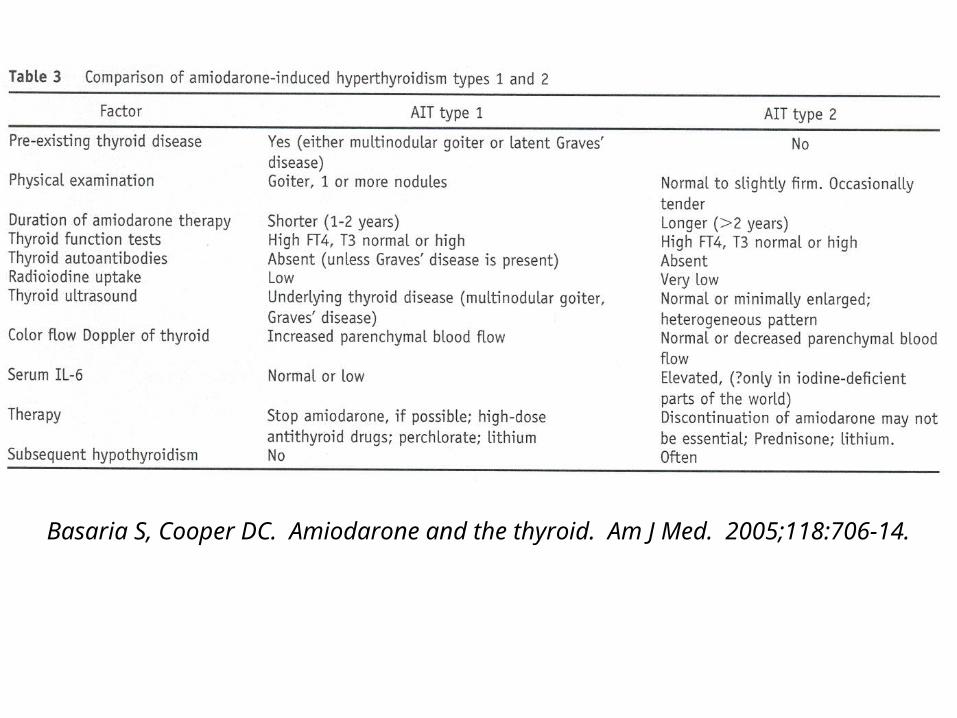
Basaria S, Cooper DC. Amiodarone and the thyroid. Am J Med. 2005;118:706-14.
Treatment “AIT… complex Dx and Rx challenge*.” Type 1: antithyroid meds, beta blockers Type 2: prednisone 40 mg x 1-3
months, slow taper Mixed or uncertain: antithyroid meds
and steroids Other Rx: surgery, plasmapharesis
*Rajeswaran. Swiss Med Wkly 2003;133:579-85

Clinical course for my patient Prednisone 40 mg daily x 2 wks; tapered Free T4 fell, TSH 0 (can lag). Relapsed, with free T4 rising. Refer Endo. Re-Rx with prednisone, longer taper. After 4 weeks, TSH 1, Free T4 normal.
BMD osteopenia Next time: Color flow doppler; IL-6, longer
prednisone Rx, early Endo.