An Overview of State Medicaid Policies for Mental Health Drugs
12
An Overview of State Medicaid Policies for Mental Health Drugs Kyle E. Hultgren, PharmD Candidate Purdue University School of Pharmacy
description
An Overview of State Medicaid Policies for Mental Health Drugs. Kyle E. Hultgren, PharmD Candidate Purdue University School of Pharmacy. Objective. To provide an accurate overview of current state Medicaid policies regarding mental health drugs. Methods. - PowerPoint PPT Presentation
Transcript of An Overview of State Medicaid Policies for Mental Health Drugs

An Overview of State Medicaid Policies for Mental Health Drugs
Kyle E. Hultgren, PharmD Candidate
Purdue University School of Pharmacy

Objective To provide an accurate overview of
current state Medicaid policies regarding mental health drugs

Methods Identify states with preferred drug lists
(PDLs) Isolate and quantify the use of mental
health drug policies Form clusters of similar policies Associate each state Medicaid
prescription drug benefit structure with a given policy cluster

Identify and Quantify PDL Use
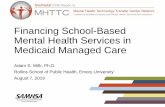
Percent of PDLs That Control a Given Drug Class
44
52 52
72
8084 84
88
0
10
20
30
40
50
60
70
80
90
100
Typicals MAOI TCA Atypicals Non-Stimulant SSRI Misc. Ads Amph. & M-phenidate
Drug Class
Perc
en
t (%
)
74% (37) have a PDL of some form
68% of these 37 states have mental health drug policies in place
Chart displays percentage of policies that address various drug classes

Drug and Policy Clusters Drug classes most
commonly addressed through policies Antipsychotics Antidepressants ADHD medications
Three major arenas of PDL structure and function Brand-Generic
Policies Prior Authorization
Policies Treatment Algorithm
Policies

Brand-Generic Policies All generic medications are preferred over
brand name (mandatory generic substitution and therapeutic substitution)
Brands without generic equivalents may still be preferred
Providers may be able to override preferred status
Brand manufacturers may pay supplemental rebates to become competitive in the class
States: Florida, Alaska, Illinois

Florida Preferred SSRIs
Citalopram Lexapro
Citalopram HBr Paxil CR
Fluoxetine Pexeva
Fluoxetine HCl Zoloft
Table shows mix of both brand name and generic medications

Prior Authorization Policies Requires that specific criteria are met before
a prescription is dispensed May involve “fail-first” edits or time intervals Method of attempting treatment uniformity for
patients with identical diagnoses Moves toward a shared state and provider
responsibility for prescribing behaviors States: Maine, Massachusetts, Missouri

Prior Authorization Policy Example
Condition Submitted ICD-9 Diagnoses
Inferred Diagnosis
History Date Range
Attention Deficit Disorder without
hyperactivity
314.00
------
730 days
Attention Deficit Disorder with hyperactivity
314.01
------
730 days
Narcolepsy (stimulants only)
347 Subject to clinical review
730 days
Table 3: Missouri Prior Authorization for ADHD stimulant medications38
Under 18 years of age Š appropriate diagnosis 18 Š 23 years of age
o Appropriate diagnosis o Goals of therapy Š Current academic/work enrollment
Over 23 years of age with childhood onset and history of treatment o Goals of therapy Š Current academic/work enrollment
Approval and therapy may be subject to supervision by mental health specialist

Treatment Algorithm Policies The most state-centric set of policies Designed to initiate, change, direct, and
terminate patient drug therapy based upon written criteria
Designed using most current evidence in tandem with provider consensus lends credibility to the algorithm
Series of prior authorizations used as guideposts to ensure appropriate use
State: Texas


Summary Few states purely use one method for
creating mental health drug policies










![[ALCOHOL, TOBACCO, DRUGS AND MENTAL …ALCOHOL, TOBACCO, DRUGS AND MENTAL HEALTH] HUG (Action for Mental Health) ... Cromwell Villa, ... DRUGS AND ALCOHOL IN NEW CRAIGS A GOOD IDEA?](https://static.fdocuments.us/doc/165x107/5abdcaff7f8b9ab02d8c11c6/alcohol-tobacco-drugs-and-mental-alcohol-tobacco-drugs-and-mental-health.jpg)