AN INVESTIGATION INTO THE ROLE OF THE GHRELIN AXIS IN...
62
AN INVESTIGATION INTO THE ROLE OF THE GHRELIN AXIS IN HORMONE-DEPENDENT CANCER AND CHARACTERISATION OF A NOVEL EXON 3-DELETED PREPROGHRELIN ISOFORM AND ITS MURINE HOMOLOGUE Penelope Lorrelle Jeffery BAppSc (Hons) Science Research Centre School of Life Sciences Queensland University of Technology A thesis submitted for the degree of Doctor of Philosophy of the Queensland University of Technology 2005
Transcript of AN INVESTIGATION INTO THE ROLE OF THE GHRELIN AXIS IN...

AN INVESTIGATION INTO THE ROLE OF THE GHRELIN
AXIS IN HORMONE-DEPENDENT CANCER AND
CHARACTERISATION OF A NOVEL EXON 3-DELETED
PREPROGHRELIN ISOFORM AND ITS MURINE
HOMOLOGUE
Penelope Lorrelle Jeffery BAppSc (Hons)
Science Research Centre
School of Life Sciences
Queensland University of Technology
A thesis submitted for the degree of Doctor of Philosophy of the
Queensland University of Technology
2005

ii

iii
Abstract
Ghrelin is a 28 amino acid peptide hormone with a unique octanoic acid
modification that has an extensive range of physiological effects, including
stimulation of growth hormone (GH) release, appetite regulation, and modulation of
reproductive functions. The cognate receptor for ghrelin is the growth hormone
secretagogue receptor (GHS-R), a G protein-coupled receptor with two documented
isoforms, the functional GHS-R type 1a and the C-terminally truncated GHS-R type
1b. Several ghrelin variants have also been identified in addition to the n-
octanoylated form of ghrelin. In our laboratory, we have identified a novel exon 3-
deleted preproghrelin variant that retains sequence for the mature ghrelin hormone
and also encodes a novel C-terminal peptide (designated as C-terminal 3 peptide).
There is emerging evidence to suggest that the ghrelin axis, encompassing ghrelin,
several ghrelin variants and both forms of the GHS-R, is implicated in tumour
growth. The objective of this project is to investigate the role of the ghrelin axis in
hormone-dependent cancer and to further characterise the expression and function of
the novel exon 3-deleted preproghrelin isoform.
Hormone-dependent cancers, including prostate and breast cancers, are
significant causes of morbidity and mortality in the Western world. Improved
diagnoses and treatments earlier in the progression of the disease are urgently
required to improve patient outcomes. Growth factors play an integral role in
prostate and breast cancer, particularly in the emergence of aggressive, hormone-
refractory disease that is resistant to standard therapies. We have previously
identified ghrelin as being a novel growth factor for prostate cancer cells in vitro and
have hypothesised that this may be extended to other hormone-dependent cancer
types including breast cancer.
In the current study, techniques including real-time quantitative RT-PCR,
Western blot analysis and immunohistochemistry have been used to determine and
quantitate ghrelin, exon 3-deleted preproghrelin and GHS-R expression in prostate
and breast cancer. Ghrelin and exon 3-deleted preproghrelin are highly expressed in
prostate cancer tissues compared to expression levels in normal prostate glands.
Similarly, breast carcinoma specimens display greater immunoreactivity for ghrelin

iv
and exon 3-deleted preproghrelin than normal breast tissues. Expression of the exon
3-deleted preproghrelin mRNA isoform is upregulated in the oestrogen-independent,
highly malignant MDA-MB-435 breast cancer cell line compared to the non-
tumourigenic MCF-10A breast epithelial cell line, suggesting that augmented
transcription of the isoform is associated with an increased malignant potential in
breast cancer. The functional GHS-R type 1a is expressed in normal breast tissue and
breast cancer specimens and cell lines. In contrast, the truncated GHS-R type 1b
isoform is exclusively expressed in breast carcinoma. These data suggest that GHS-R
type 1b, ghrelin and exon 3-deleted preproghrelin display potential as novel
diagnostic markers for prostate and breast cancer.
These studies have been the first to demonstrate that ghrelin may have an
important role in cell proliferation in breast and prostate cancer. Functional assays
demonstrated that (10nM) ghrelin stimulated proliferation in the LNCaP prostate
cancer cell lines (45.0 ± 1.7% above control, P <0.01) and rapidly activated the ERK
1/2 mitogen-activated kinase (MAPK) pathway in both PC3 and LNCaP cell lines. It
does not, however, protect these cells from chemically-induced apoptosis. The
MAPK inhibitors PD98059 and U0126 blocked ghrelin-induced MAPK activation,
as well as cell proliferation, in both cell lines. Prostate cancer cells secrete mature
ghrelin in vitro, and may therefore stimulate MAPK pathways in an autocrine
manner. Ghrelin also appears to act as a growth factor in breast cancer cell
proliferation, as the growth of MDA-MB-435 and MDA-MB-231 breast cancer cell
lines is significantly increased by ghrelin treatment. Our findings suggest that the
ghrelin axis could provide an important new target for adjunctive therapies for both
breast and prostate cancer.
The C-terminal 3 peptide derived from exon 3-deleted preproghrelin
may be an important new component of the ghrelin axis and studies into its function
are currently in progress. Although it did not induce MAPK cascades or stimulate
proliferation in prostate or breast cancer cell lines, the discovery of a murine
counterpart, exon 4-deleted preproghrelin, indicates that it is highly conserved. Exon
4-deleted preproghrelin is expressed in all mouse tissues examined, with stomach
being the predominant site of synthesis. Other components of the ghrelin axis were
also found to be present in a wide-range of mouse tissues including brain, ovary and

v
prostate. This comprehensive report has paved the way for future work with in vivo
mouse models of cancer.
This study has provided a substantial basis for the further evaluation of
ghrelin, exon 3-deleted preproghrelin and the GHS-R type 1b as novel
diagnostic/prognostic markers for prostate and breast cancer and supports the
rationale for targeting the ghrelin axis for treatment of these tumours.
Keywords: Ghrelin, exon 3-deleted preproghrelin, GHS-R, growth factors, MAPK,
ERK 1/2, hormone-dependent cancer, prostate, breast, diagnostic/prognostic marker,
therapeutic targets.

vi
List of publications, conference abstracts and patents The following is a list of publications and submitted manuscripts, conference
abstracts and patents that have been derived from the work performed for this thesis:
Jeffery PL, Herington AC, Chopin LK (2003) The potential autocrine/paracrine
roles of ghrelin and its receptor in hormone-dependent cancer. Cytokine and Growth
Factor Reviews 14: 113-122.
Jeffery PL, Duncan RP, Yeh AH, Jaskolski RJ, Hammond DS, Herington AC,
Chopin LK (2005) Expression of the ghrelin/GHS-R axis in the mouse: an exon 4-
deleted proghrelin variant encondes a novel C-terminal peptide. Endocrinology 146:
432-440.
Jeffery PL, Murray RE, Yeh AH, McNamara JF, Duncan RP, Francis G, Herington
AC, Chopin LK (2005) Expression and function of the ghrelin axis, including a novel
preproghrelin isoform, in human breast cancer tissues and cell lines. Endocrine
Related Cancer, in press.
Yeh AH*, Jeffery PL*, Duncan RP, Herington AC, Chopin LK (2005) Ghrelin and
a novel preproghrelin isoform are highly expressed in prostate cancer compared to
normal prostate tissue and ghrelin-mediated prostate cancer cell line proliferation
involves the MAPK pathway. Clinical Cancer Research, in press.
* These two authors contributed equally to the work as first authors
Other related publications:
Jeffery PL, Herington AC, Chopin LK (2002) Expression and action of the growth
hormone releasing peptide ghrelin and its receptor in prostate cancer cells lines.
Journal of Endocrinology 172: 7-11.

vii
Gaytan F, Morales C, Barreiro ML, Jeffery PL, Chopin LK, Herington AC,
Casanueva FF, Aguilar E, Dieguez C, Tena-Sempere M (2005) Expression of
Growth Hormone Secretagogue Receptor Type 1a, the Functional Ghrelin Receptor,
in Human Ovarian Surface Epithelium, Mullerian Duct Derivatives and Ovarian
Tumors. Endocrinology 90: 1798-1803.
Conference Abstracts
PL Jeffery, RP Duncan, AH Yeh, RA Jaskolski, DS Hammond, AC Herington, LK
Chopin (2004) Expression of the ghrelin axis in the mouse: an exon 4-deleted
proghrelin variant encodes a novel C terminal peptide. Second International GH-IGF
Symposium, Cairns, Queensland, April 2004.
LK Chopin, AH Yeh, PL Jeffery, AC Herington (2004) Ghrelin promotes cellular
proliferation in the PC3 and LNCaP prostate cancer cell lines through the activation
of mitogen activated protein kinase pathway. Second International GH-IGF
Symposium, Cairns, Queensland, April 2004.
PL Jeffery, AH Yeh, JF McNamara, AC Herington and LK Chopin (2003) The roles
of ghrelin, its cognate receptor and a novel proghrelin isoform in hormone-dependent
cancer and reproduction. Annual meeting of the Society for Endocrinology, Royal
College of Physicians, London, November 2003.
R Jaskolski, RP Duncan, PL Jeffery, C Craven, AC Herington and LK Chopin
(2003) The expression of ghrelin, an exon 4 deleted proghrelin isoform and the
ghrelin receptor in the mouse embryo. ASMR annual meeting, Adelaide, November
2003.
PL Jeffery, AH Yeh, AC Herington and LK Chopin (2003) The autocrine/paracrine
roles of ghrelin and the GHS-R in hormone-dependent cancer. Endocrine Society of
Australia, Novartis junior investigator finalist presentation, Melbourne, September
2003.

viii
LK Chopin, PL Jeffery, JF McNamara, AC Herington (2002) Expression of
components of the ghrelin/Growth hormone secretagogue receptor axis in breast
cancer cell lines and in breast cancer histopathological specimens. US Endocrine
Society 84th Annual meeting, San Francisco, June 2002.
Lisa K Chopin, Penny L. Jeffery, John F. McNamara, Carolyn S. Chan, Ying Dong,
Judith A Clements, Adrian C Herington (2002) Ghrelin and growth hormone
secretagogue receptor (GHS-R) expression in ovarian and endometrial cell lines and
tumours. US Endocrine Society 84th Annual meeting, San Francisco, June 2002.
PL Jeffery, John F. McNamara, Adrian C Herington and LK Chopin (2002) The
identification and expression pattern of a ghrelin variant that encodes a novel peptide
in the human and mouse. Endocrine Society of Australia, annual scientific meeting,
Adelaide, September 2002.
LK Chopin, PL Jeffery, JF McNamara, AC Herington (2002) Expression of the
ghrelin/ growth hormone secretagogue receptor axis in the mouse. GH and IGF
Society Joint Symposium, Boston, October 2002.
LK Chopin, PL Jeffery, JF McNamara, AC Herington (2002) The identification and
expression pattern of a ghrelin mRNA variant encoding a novel peptide in the
human. GH and IGF Society joint Symposium, Boston, October 2002.
Patents
International Patent PCT/AU02/00582
‘Reproductive cancer diagnosis and therapy’
Chopin LK, Jeffery PL, Herington AC (14/11/2002)

ix
Table of Contents pg
Title page i
Abstract and keywords iii
List of publications, conference abstracts and patents vi
Table of Contents ix
Declaration xi
Acknowledgements and dedication xii
List of abbreviations xiii
Chapter 1 – Introduction 1
Chapter 2 – Literature Review 11
Statement of joint authorship 12
Abstract 13
2.1 Introduction 14
2.1.1 The growth hormone secretagogues (GHS) 14
2.1.2 The growth hormone secretagogue receptor (GHS-R) 15
2.1.3 Splice variants of the GHS-R 15
2.1.4 Ghrelin 17
2.1.5 Ghrelin variants 18
2.1.6 Tissue distribution of ghrelin and the GHS-R 21
2.2 The GHRH/GH/IGF axis in cancer 24
2.2.1 GH and insulin-like growth factors (IGFs) 24
2.2.2 GH releasing hormone (GHRH) 26
2.2.3 Ghrelin and the GHS-R in cancer 27
2.3 References 34
Chapter 2B – Literature Review Update 47
2B.1 Ghrelin/GHS-R expression in Cancer 48
2B.2 Interaction of the ghrelin axis with sex steroid hormones 48
2B.3 Functional studies of the role of ghrelin/GHS-R in cancer 50
2B.4 References 52

x
Chapter 3 - Ghrelin and a novel preproghrelin isoform are highly expressed in
prostate cancer compared to normal prostate tissue and ghrelin-mediated
prostate cancer cell line proliferation involves the MAPK pathway 59
Statement of joint authorship 60
Abstract 62
Introduction 63
Materials and methods 64
Results 69
Discussion 79
References 88
Chapter 4 - Expression and function of the ghrelin axis, including a novel
preproghrelin isoform, in human breast cancer tissues and cell lines 95
Statement of joint authorship 96
Abstract 98
Introduction 99
Materials and methods 100
Results 105
Discussion 116
References 120
Chapter 5 - Expression of the ghrelin axis in the mouse: an exon 4-deleted
proghrelin variant encodes a novel C terminal peptide 127
Statement of joint authorship 128
Abstract 130
Introduction 131
Materials and methods 132
Results 136
Discussion 153
References 158
Chapter 6 – General Discussion 163

xi
Declaration
The work contained in this thesis has not been previously submitted for a
degree or diploma at any other higher education institution. To the best of my
knowledge and belief, the thesis contains no material previously published or written
by another person except where due references are made.
Signed:…………………………
Penelope Jeffery
Date:……………………………

xii
Acknowledgements and Dedication
I would like to thank my supervisors, Dr Lisa Chopin and Professor
Adrian Herington for their invaluable support, encouragement and friendship during
my candidature. Many thanks also go to all of my colleagues in the Hormone-
dependent cancer program for their advice and friendship. I would like to
acknowledge the financial support I have received from the Australian Postgraduate
Award PhD scholarship scheme and from the QUT Dean of Science top-up
scholarship.
Many thanks and love to my parents, Adrienne and Ross, and to my
partner John, for their boundless patience, support and babysitting and to my
daughter Cordelia, my greatest achievement of all.
This thesis is dedicated to my brother, Randall.

xiii
List of Abbreviations
aa Amino acid
AEBSF 4-(2-aminoethyl)-benzenesulfonyl fluoride hydrochoride
AGRF Australian Genome Research Facility
AMV Avian myeloblastosis virus
ANOVA Analysis of variance
ATCC American type culture collection
bp Base pairs
BSA Bovine serum albumin
cDNA Complementary deoxyribose nucleic acid
DAPI 4,6-Diamidino-2-phenylindole
DMEM Dulbecco’s modified eagle medium
DMSO Dimethyl Sulfoxide
DNA Deoxyribose nucleic acid
dNTP Deoxy-nucleotide triphosphate
DTT Dithiothreitol
EDTA Ethylenediamine tetra acetic acid di-sodium salt
EGF Epidermal growth factor
ERK Extracellular-signal regulated kinase
EST Expressed sequenced tag
FBS Foetal bovine serum
FCS Foetal calf serum
g Grams
GGDT Ghrelin gene-derived transcript
GH Growth hormone
GH-R Growth hormone receptor
GHS Growth hormone secretagogue
GHS-R Growth hormone secretagogue receptor
h Hour
HRP Horse radish peroxidase
IGF Insulin-like growth factor
kDa Kilodaltons

xiv
M Molarity (when refering to concentration)
MAPK Mitogen activated protein kinase
mg/ml Milligrams per millilitres
min Minute
ml Millilitre
mM Millimolar
mmol/L Millimoles per litre
mRNA Messenger ribose nucleic acid
MTT 3,[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide
mV Millivolts
MW Molecular weight marker
NCBI National centre for biotechnology information
PAGE Polyacrylamide gel electrophoresis
PBS Phosphate buffered saline
PCR Polymerase chain reaction
PKC Protein kinase C
PLC Phospholipase C
pmol Picomole
PSA Prostate specific antigen
RNA Ribose nucleic acid
RPM Revolutions per minute
RPMI Roswell park memorial institute
RT-PCR Reverse transcriptase polymerase chain reaction
s Seconds
SDS Sodium dodecyl sulphate
SEM Standard error of the mean
Ser-3 3rd residue (serine)
SSC Tri-sodium citrate
Ta Annealing temperature
TBS Tris buffered saline
TBST Tris buffered saline/tween
TMD Transmembrane domain
U/ml Units per millilitre

xv
WST-1 2-(4-Iodophenyl)-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-
tetrazolium monosodium salt
w/v Weight per volume
μg Micrograms
μg/ml Micrograms per millilitre
μl Microlitre
μm Micrometre
μM Micromolar

1
CHAPTER ONE
INTRODUCTION
Description of scientific problem investigated
Hormone-dependent cancer has a significant impact upon morbidity and
mortality rates in the Western world. Extensive research is underway to identify new
therapeutic targets and markers to treat and more effectively diagnose the wide-
ranging spectrum of these cancers that include prostate, breast, endometrial and
ovarian cancers. The most prevalent forms of hormone-dependent cancer, prostate
and breast cancer, account for over 30% of newly diagnosed cancers in Western men
and women respectively (Jemal et al. 2005). Prostate cancer is the second-leading
cause of cancer mortality in men, with males from developed countries facing a
lifetime risk of 1 in 6 of developing prostate cancer (Jemal et al. 2005). Prostate
tumourigenesis is driven largely by steroid androgens and anti-androgen therapy is
the mainstay of prostate cancer treatment (So et al. 2003, Van der Poel, 2004). There
is now considerable evidence that up-regulated growth factor activity promotes an
aggressive, androgen-independent prostate cancer phenotype that is resistant to
traditional hormonal therapies and is associated with a poor prognosis (Feldman and
Feldman, 2001). This highlights the need for adjunctive therapies that can prevent, or
overcome, hormone-refractory disease. The activation of mitogen-activated protein
kinase (MAPK) cascades by growth factors can enhance prostate cancer cell
proliferation and survival (Maroni et al. 2004). Manipulation of MAPK signal
transduction pathways is therefore a novel therapeutic strategy that has been
proposed for the treatment of advanced prostate cancer (Sebolt-Leopold and Herrera,
2004). Diagnosis of prostate cancer has proven problematic due to the non-
specificity of the most widely used tumour marker, serum prostate specific antigen
(PSA) (Thompson et al. 2004). The PSA detection test is also unable to accurately
predict pathological stage and new prognostic markers are clearly required to give a
better profile of prostate tumour grade and severity (Watson and Schalken, 2004).

2
Breast cancer in women and prostate cancer in men share many common
features including epidemiology, mortality rates and hormonal-dependence (Lopez-
Otin and Diamandis, 1998). The effectiveness of selective oestrogen receptor
modulators (SERMs) attests to the importance of oestrogen-withdrawal in the
treatment of breast cancer. As is the case for prostate cancer, however, elevated
growth factor signalling may allow for the emergence of hormone-refractory breast
cancer which is associated with higher mortality rates, particularly in premenopausal
women (Nicholson et al. 2004). Pharmacological molecules designed to block
various growth factors and their receptors have displayed some success in the
laboratory and the clinic, and this field of cancer treatment, including small molecule
therapy, remains promising (Guillemard and Saragovi, 2004). The identification of
new therapeutic targets as well as novel diagnostic and prognostic markers,
particularly in hormone-refractory cancer, is imperative. Growth factors have the
potential to fulfil these roles in the future.
Growth hormone (GH) and its downstream mediators, the insulin-like growth
factors (IGFs), have been implicated in both direct and indirect modulation of
prostate and breast cancer cell function (Chopin and Herington, 1999, Laban et al.
2003). Components of the GH axis have therefore been presented as potential targets
for anti-tumour therapy. In 1999, a 28 amino acid peptide hormone capable of
potently stimulating GH release was purified from stomach tissue (Kojima et al.
1999). This hormone, named ghrelin (ghre: grow), was identified several years after
its endogenous receptor, the growth hormone secretagogue receptor (GHS-R)
(Howard et al. 1996). It is now widely accepted that ghrelin and its receptor are
important new components of the GH axis. Ghrelin action is not restricted to GH
release, however, and it possesses many potentially important physiological
functions including appetite stimulation and energy homeostasis (Nakazato et al.
2001, Shintani et al. 2001), embryo implantation (Tanaka et al. 2003, Duncan et al.
2005) and cardiovascular actions (Benso et al. 2004). Several ghrelin isoforms have
also been identified, including a novel exon 3-deleted preproghrelin variant
discovered in our laboratory (Jeffery et al. 2002). Expression and function of this
variant, along with that of its murine homologue, exon 4-deleted preproghrelin, was
investigated over the course of this project. Ghrelin has also been shown to be a
mitogen for cancer cell lines and our study of the proliferative effect of ghrelin on

3
prostate cancer cells was one of the first published in this field (Jeffery et al. 2002).
The physiological role of ghrelin as a growth factor in hormone-dependent cancer
requires further elucidation.
Overall objectives of the study
Preliminary data from our laboratory suggested that components of the
ghrelin axis display potential as novel therapeutic targets and diagnostic markers for
prostate cancer (Jeffery et al. 2002). The overall objective of this study was to
investigate the role that the ghrelin axis, including the novel exon 3-deleted
preproghrelin isoform, may play in prostate cancer, and to extend these studies to
encompass breast cancer. This study also aimed to provide a better understanding of
the physiology of the human ghrelin axis in general. Expression of the murine
ghrelin axis was also investigated to prepare for the development of future mouse
models.
Specific aims of the study were:
• To investigate the expression of mRNA and protein for ghrelin,
preproghrelin isoforms and the GHS-R in prostate and breast cancer cell
lines and tissues, as well as in normal tissues, using RT-PCR, real time
quantitative RT-PCR, immunohistochemistry and Western blot analysis
• To perform functional assays on prostate and breast cancer cell lines in
vitro treated with synthetic ghrelin
Proliferation, migration and apoptosis assays were performed and the
concentration of GH secreted into the conditioned media measured. The
signalling mechanisms underlying ghrelin action in prostate cancer cells were
also investigated in the laboratory, by studying the involvement of the
mitogen-activated protein kinase (MAPK) pathways.
• To investigate the expression of a mouse homologue of ghrelin and
preproghrelin isoforms in a wide range of mouse tissues using RT-PCR,
real time quantitative RT-PCR and immunohistochemistry

4
Summary of scientific progress linking the journal manuscripts
This thesis is being presented “By Publication” based on Queensland
University of Technology guidelines. Accordingly, each chapter represents a
manuscript that has been published, or has been submitted for publication, in an
international refereed journal.
Chapter 2: Literature Review: The potential autocrine/paracrine roles of ghrelin and
its receptor in hormone-dependent cancer
This literature review was the first to be published regarding the role of
the ghrelin axis in hormone-dependent cancer. This paper reviews the literature
describing the expression, regulation and function of ghrelin and the GHS-R in
cancer, as well as providing an updated assessment of studies exploring the role of
GH and IGF-1 in cancer. The exon 3-deleted preproghrelin isoform was first
discovered in prostate cancer cell lines (Jeffery et al. 2002), and this review contains
a further analysis and schematic depiction of the exon deletion and putative protein
sequence of this isoform. This paper was published in Cytokine and Growth Factor
Reviews (2003) 14: 113-22. A brief literature update, encompassing recent studies on
the ghrelin axis in cancer (2002-2005), is also included at the end of this chapter
(Chapter 2, part B).
Chapter 3: Research article: Ghrelin and a novel preproghrelin isoform are highly
expressed in prostate cancer compared to normal prostate tissue and ghrelin-
mediated prostate cancer cell proliferation involves the MAPK pathway
As a natural progression following our studies in prostate cancer cell lines
(Jeffery et al. 2002) we investigated the signalling pathways underlying ghrelin-
stimulated prostate cancer cell proliferation. This paper contains novel data, derived
from studies performed with the co-author Anthony Yeh, demonstrating that ghrelin
increases prostate cancer cell proliferation via the MAPK pathway. The expression
and function of the exon 3-deleted preproghrelin isoform discovered in our
laboratory (Jeffery et al. 2002), and wild-type ghrelin, are more fully characterised in

5
prostate histopathological specimens and cell lines. This manuscript has been
accepted for publication in Clinical Cancer Research (2005) and is currently in press.
Chapter 4: Research article: Expression and function of the ghrelin axis, including a
novel preproghrelin isoform, in human breast cancer tissues and cell lines
Breast cancer is the most commonly diagnosed malignancy in women in
the Western world (Jemal et al. 2005), and like prostate cancer in men, is highly
sensitive to the effects of growth factors. We therefore decided to investigate the
role of the ghrelin axis in this hormone-dependent cancer. Ghrelin, exon 3-deleted
preproghrelin, and GHS-R expression was demonstrated at the mRNA and protein
level in breast cancer cell lines and tissues. Negligible expression of the GHS-R type
1b in normal breast tissue compared to expression in breast cancer tissues indicates
that this receptor isoform may possess a unique role in breast cancer and has
potential as a diagnostic marker. Ghrelin treatment elicited proliferation in breast
cancer cell lines, as was previously observed in prostate cancer cell lines. Expression
of the exon 3-deleted preproghrelin mRNA isoform was observed to be upregulated
in breast cancer cell lines compared to expression in a non-tumourigenic breast
epithelial cell line. This manuscript has been accepted for publication in Endocrine
Related Cancer (2005) and is currently in press.
Chapter 5: Research article: Expression of the ghrelin axis in the mouse: an exon 4-
deleted proghrelin mouse variant encodes a novel C-terminal peptide
The data generated from the in vitro studies described in Chapters 3 and 4
has provided a substantial base for future work examining the role of the ghrelin axis
in prostate and breast cancer in vivo. Mouse models will be important tools for this
work, therefore, characterisation of the murine ghrelin axis was undertaken and the
data derived from these studies are presented in Chapter 5. This paper also describes
the expression of a murine homologue of exon 3-deleted preproghrelin and
demonstrates that the novel isoform is conserved across species, implying
physiological significance. The murine ghrelin isoform was shown to be expressed at
the mRNA and protein levels by quantitative RT-PCR, Western blot and
immunohistochemical analysis. This research article was the first comprehensive

6
report on the expression of the ghrelin axis and the ghrelin isoform in the mouse
(Jeffery et al. 2005) and has been published in Endocrinology (2005, 146: 432-40).

7
REFERENCES
Benso A, Broglio F, Marafetti L, Lucatello B, Seardo MA, Granata R, Martina V,
Papotti M, Muccioli G, Ghigo E (2004) Ghrelin and synthetic growth hormone
secretagogues are cardioactive molecules with identities and differences. Seminars
in Vascular Medicine 4: 107-114.
Chopin L, Herington A (1999) The growth hormone insulin-like growth factor axis
and prostate cancer. Clinical Biochemists Reviews 20: 3-16.
Duncan RP, Jaskolski RA, Jeffery PL, Herington AC, Chopin LK (2005) A potential
role for ghrelin in embryo implantation. In preparation.
Feldman BJ, Feldman D (2001) The development of androgen-independent prostate
cancer. Nature Reviews Cancer 1: 34-45.
Guillemard V, Saragovi HU (2004) Novel approaches for targeted cancer therapy.
Current Cancer Drug Targets 4: 313-326.
Howard A, Feighner S, Cully D, Arena J, Liberator P, Rosenblum C, Hamelin M,
Hreniuk D, Palyha O, Anderson J, Paress P, Diaz C, Chou M, Liu K, McKee KK,
Pong S, Chuang L, Elbrecht A, Dashkevicz M, Heavens R, Rigby M, Sirinathsinghji
D, Dean D, Melillo D, Patchett AA, Nargund R, Grifin P, DeMartino J, Gupta S,
Schaefer JA, Smith R, Van der Ploeg L (1996) A receptor in pituitary and
hypothalamus that functions in growth hormone release. Science 12: 137-145.
Jeffery PL, Herington AC, Chopin LK (2002) Expression and action of the growth
hormone releasing peptide ghrelin and its receptor in prostate cancer cells lines.
Journal of Endocrinology 172: 7-11.
Jeffery PL, Duncan RP, Yeh AH, Jaskolski RJ, Hammond DS, Herington AC,
Chopin LK (2005) Expression of the ghrelin/GHS-R axis in the mouse: an exon 4-
deleted proghrelin variant encodes a novel C-terminal peptide. Endocrinology 146:
432-440.

8
Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ
(2005) Cancer Statistics, 2005. CA: A cancer journal for clinicians 55: 10-30.
Kojima M, Hosodo H, Date Y, Nakazato M, Matsuo H, Kanagawa K (1999) Ghrelin
is a growth hormone releasing acylated peptide from stomach. Nature 402: 656-660.
Laban C, Bustin SA, Jenkins PJ (2003) The GH-IGF-I axis and breast cancer. Trends
in Endocrinology and Metabolism 14: 28-34.
Lopez-Otin C, Diamandis EP (1998) Breast and prostate cancer: an analysis of
common epidemiological, genetic and biochemical features. Endocrine reviews 19:
365-396.
Maroni PD, Koul S, Meacham RB, Koul H. (2004) Mitogen activated protein kinase
signal transduction pathways in the prostate. Cell Communication and Signaling 2:5-
18.
Nakazato M, Murakami N, Date Y, Kojima M, Matsuo H, Kengawa K, Matsukura S
(2001) A role for ghrelin in the central regulation of feeding. Nature 409: 194-198.
Nicholson RI, Staka C, Boyns F, Hutcheson IR, Gee JMW (2004) Growth factor-
driven mechanisms associated with resistance to estrogen deprivation in breast
cancer: new opportunities for therapy. Endocrine-Related Cancer 11: 623-641.
Sebolt-Leopold JS, Herrera R (2004) Targeting the mitogen-activated protein kinase
cascade to treat cancer. Nature Reviews Cancer 4: 937-947.
Shintani M, Ogawa Y, Ebihara K, Aizawa-Abe M, Miyanaga F, Takaya K, Hayashi
T, Inoue G, Hosoda K, Kojima M, Kangawa K, Nakao K (2001) Ghrelin, an
endogenous growth hormone secretagogue, is a novel orexigenic peptide that
antagonizes leptin action through the activation of hypothalamic neuropeptide Y/Y1
receptor pathway. Diabetes 50: 227-232.

9
So AI, Hurtado-Coll A, Gleave ME (2003) Androgens and prostate cancer. Journal
of Urology 21: 325-337.
Tanaka K, Minoura H, Isobe T, Yonaha H, Kawato H, Wang DF, Yoshida T, Kojima
M, Kangawa K, Toyoda N (2003) Ghrelin is involved in the decidualization of
human endometrial stromal cells. Journal of Clinical Endocrinology and Metabolism
88: 2335-2340.
Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL,
Minasian LM, Ford LG, Lippman SM, Crawford ED, Crowley JJ, Coltman CA
(2004) New England Journal of Medicine 350: 2239-2246.
Van de Poel HG (2004) Smart drugs in prostate cancer. European Urology 45: 1-7.
Watson RWG, Schalken JA (2004) Future opportunities for the diagnosis and
treatment of prostate cancer. Prostate Cancer and Prostatic Diseases. 7 (Suppl 1): 8-
13.

10

11
CHAPTER TWO
LITERATURE REVIEW
THE POTENTIAL AUTOCRINE/PARACRINE ROLES
OF GHRELIN AND ITS RECEPTOR IN
HORMONE-DEPENDENT CANCER
Penny L Jeffery, Adrian C Herington and Lisa K Chopin
Cytokine and Growth Factor Reviews (2003) 14: 113-22.
halla
This article is not available online. Please consult the hardcopy thesis available from the QUT Library

47
CHAPTER TWO (PART B)
LITERATURE REVIEW UPDATE

48
Literature Review Update
From the time that our review was published in early 2003, the body of
research concerning the role of the ghrelin axis in cancer has expanded considerably;
hence a brief update of the literature is required. This chapter contains a review of
recent articles pertaining to ghrelin and the GHS-R in cancer, as this is the focus of
subsequent chapters in this thesis.
2B.1 Ghrelin/GHS-R expression in cancer
The number of tumour types that have been demonstrated to express
ghrelin and the GHS-R has increased in recent years. Endocrine tumours that
produce and secrete high quantities of ghrelin into the circulation (named
ghrelinomas), have been identified. A grossly elevated serum ghrelin concentration
was measured in a patient with a highly malignant gastric ghrelinoma (Tsolakis et al.
2004) and the occurance of a rare pancreatic ghrelinoma has been reported (Corbetta
et al. 2003). A subset of pancreatic islet cell tumours associated with multiple
endocrine neoplasia-1 (MEN-1) show ghrelin immunoreactivity (Iwakura et al.
2002). Ghrelin and both isoforms of the GHS-R are expressed in a bronchial
neuroendocrine tumor, but not in adjacent normal lung tissue, suggesting a
modulatory role for the ghrelin axis in this tumour type (Arnaldi et al. 2003).
Ghrelin and the functional GHS-R type 1a are also expressed in reproductive system
malignancies including highly differentiated testicular tumours (Gaytan et al. 2004)
and ovarian tumours (Gaytan et al. 2005).
2B.2 Interaction of the ghrelin axis with sex steroid hormones
A plethora of experimental and epidemiological studies has demonstrated
that sex steroids, including oestrogens and androgens, are the prime modulators of
hormone-dependent cancers, particularly those of the breast and prostate (Haslam
and Woodward, 2003, So et al. 2003). Recent research has indicated that ghrelin and
its cognate receptor (GHSR 1a) may interact with sex steroid hormones including
androgens, oestrogens and progesterone. Ovarian thecal and granulosa cells are
prime sites of oestrogen biosynthesis in the pre-menopausal female (Ryan and Petro,

49
1966), and these cell types express ghrelin and the GHSR 1a in a variable pattern
across the normal menstrual cycle, suggesting that ghrelin may modulate oestrogen
function (Gaytan et al. 2003). This may only be relevant to autocrine/paracrine
oestrogen physiology, as ghrelin administration in rats did not perturb serum
estradiol levels (Fernandez-Fernandez et al. 2005), and surprisingly, there are no
available data regarding the impact of ghrelin treatment on oestrogen levels in
humans.
Conversely, oestrogen may regulate ghrelin expression, as in rats
oophorectomy significantly increases plasma ghrelin levels and the number of
ghrelin-immunoreactive cells in the stomach (Matsubara et al. 2004). This effect is
reversed upon administration of 17-β-estradiol indicating that oestrogen negatively
regulates ghrelin production in the rat (Matsubara et al. 2004). In humans studies
however, oestrogen supplementation increased plasma ghrelin concentrations in
severely-undernourished female patients (Grinspoon et al. 2004) and in
postmenopausal women receiving HRT (hormone replacement therapy), although the
mechanisms behind these effects are unknown (Kellokoski et al. 2005). Post-
menopausal HRT use has been associated with an increased risk of developing breast
cancer (Chlebowski et al. 2003), although studies in this field are contradictory
(Creasman, 2005). Oestrogen also potentiates ghrelin-induced pulsatile GH secretion
(Veldhuis and Bowers, 2003), and is an important modulator of GH function (Leung
et al. 2004). GH is emerging as an important oncogenic hormone in breast cancer
(Waters and Conway-Campbell, 2004). No research has been published to date
regarding the potential interaction of ghrelin with oestrogen in the context of breast
cancer.
Other sex hormones appear to influence ghrelin secretion. Androgen
levels in women with polycystic ovary disease are elevated and may inhibit ghrelin
secretion, resulting in lower circulating ghrelin levels compared to normal controls
(Pagotto et al. 2002, Panidis et al. 2005). Ghrelin levels increase to normal
concentrations in these patients after androgen-blockade (Gambineri et al. 2003).
Ghrelin and GHSR 1a co-immunoreactivity is present in ovarian hilus interstitial
cells which are capable of testosterone secretion, under the control of luteinising
hormone (Gaytan et al. 2003, Erickson et al. 1985). This research indicates that

50
ghrelin may regulate androgen secretion and/or function in the ovary (Gaytan et al.
2003). Ghrelin and the GHSR 1a are also co-expressed in the steroidogenic Leydig
cells of the testis and ghrelin inhibits testosterone secretion from testicular tissue in
vitro, potentially by downregulating the expression of key enzymes in the
steroidogenic pathway (Gaytan et al. 2004).
The synthetic progestin molecule, cyproterone acetate, is the most
frequently used steroidal anti-androgen in prostate cancer therapy (Culig et al. 2004).
The recent finding that cyproterone acetate significantly elevates total ghrelin levels
in healthy men (Gambineri et al. 2005) may hold significance for the treatment of
men with advanced prostate cancer, as cell lines derived from metastatic prostate
tumours proliferate in response to ghrelin treatment (Jeffery et al. 2002).
2B.3 Functional studies on the role of ghrelin/GHS-R in cancer
Enhanced proliferation in response to ghrelin treatment has now been
demonstrated in numerous cell lines and many studies have investigated the signal
transduction pathways underlying this response. Exogenous ghrelin increases the
proliferative, invasive and migratory potential of pancreatic adenocarcinoma cells in
vitro, via augmented Akt phosphorylation (Duxbury et al. 2003). Ghrelin activates
the ERK1/2 MAPK pathway and thereby stimulates growth in adrenocortical cells
(Andreis et al. 2003, Mazzocchi et al. 2004), 3T3-L1 adipocytes (Kim et al. 2004)
and the rodent somatotroph pituitary tumour cell line GH3 (Nanzer et al. 2004).
Proliferation of primary cultures of rodent osteoblasts also increases after treatment
with physiological concentrations of ghrelin (Maccarinelli et al. 2005), whilst rodent
neuronal proliferation is stimulated by ghrelin both in vivo and in vitro (Zhang et al.
2004). Endogenous ghrelin may be part of an autocrine loop sustaining growth of
human erythroleukemic (HEL) cells, as blocking antibodies inhibit proliferation of
this cell line in vitro (De Vriese et al. 2005). The growth-promoting role of ghrelin
may also be attributed to its anti-apoptotic actions in many cell lines (Baldanzi et al.
2002, Kim et al. 2004, Mazzocchi et al. 2004, Kim et al. 2005). Apoptosis plays an
integral role in tumour growth; therefore ghrelin may contribute to tumourigenesis by
enhancing tumour cell survival. Some conflicting studies, however, have reported an
inhibitory role for ghrelin in tumour biology. For example, apoptosis is increased in

51
aldosteronoma cell lines after exposure to exogenous ghrelin (Belloni et al. 2004). In
agreement with their previous work in breast cancer cells (Cassoni et al. 2001),
Volante and co-workers have demonstrated that ghrelin inhibits proliferation of
thyroid carcinoma cell lines in vitro, an effect that may be mediated by a receptor
other than the GHS-R (Volante et al. 2003). This research group has also recently
published data that agreed with our own studies (Jeffery et al. 2002) regarding the
mitogenic effect of ghrelin in the PC3 prostate cancer cell line (Cassoni et al. 2004).
The non-acylated form of ghrelin may have a negative impact upon cell growth, as
the des-acyl ghrelin overexpressing transgenic mouse displays a small phenotype and
lowered GH/IGF-I levels (Ariyasu et al. 2005). The physiological effect of ghrelin
on cultured cells in vitro is clearly cell type-specific and may be reliant upon GHS-R
isoform expression, intracellular signalling crosstalk, and ghrelin acylation status;
however, this phenomenon is yet to be fully explored.

52
REFERENCES
Andreis PG, Malendowicz LK, Trejter M, Neri G, Spinazzi R, Rossi GP, Nussdorfer
GG (2003) Ghrelin and growth hormone secretagogue receptor are expressed in the
rat adrenal cortex: Evidence that ghrelin stimulates the growth, but not secretory
activity of adrenal cells. FEBS Letters 536: 173-179.
Ariyasu H, Takaya K, Iwakura H, Hosoda H, Akamizu T, Arai Y, Kangawa K &
Nakao K (2005) Transgenic mice overexpressing des-acyl ghrelin show small
phenotype. Endocrinology 146: 355-364.
Arnaldi G, Mancini T, Kola B, Appolloni G, Freddi S, Concettoni C, Bearzi I,
Masini A, Boscaro M & Mantero F (2003) Cyclical Cushing's syndrome in a patient
with a bronchial neuroendocrine tumour (typical carcinoid) expressing ghrelin and
growth hormone secretagogue receptors. Journal of Clinical Endocrinology and
Metabolism 88: 5834-5840.
Baldanzi G, Filigheddu N, Cutrupi S, Catapano F, Bonissoni S, Fubini A, Malan D,
Baj G, Granata R, Broglio F, Papotti M, Surico N, Bussolino F, Isgaard J, Deghenghi
R, Sinigaglia F, Prat M, Muccioli G, Ghigo E, Graziani A (2002) Ghrelin and des-
acyl ghrelin inhibit cell death in cardiomyocytes and endothelial cells through
ERK1/2 and PI 3-kinase/AKT. Journal of Cell Biology 159: 1029-1037.
Belloni AS, Macchi C, Rebuffat P, Conconi MT, Malendowicz LK, Parnigotto PP,
Nussdorfer GG (2004) Effect of ghrelin on the apoptotic deletion rate of different
types of cells cultured in vitro. International Journal of Molecular Medicine 14:165-
167.
Cassoni P, Papotti M, Ghe C, Catapano F, Sapino A, Graziani A, Deghenghi R,
Reissmann T, Ghigo E & Muccioli G (2001) Identification, characterisation and
biological activity of specific receptors for natural (ghrelin) and synthetic growth
hormone secretagogues and analogs in human breast carcinoma and cell lines.
Journal of Clinical Endocrinology and Metabolism 86: 1738-1745.

53
Cassoni P, Ghe C, Marrocco T, Tarabra E, Allia E, Catapano F, Deghenghi R, Ghigo
E, Papotti M, Muccioli G (2004) Expression of ghrelin and biological activity of
specific receptors for ghrelin and des-acyl ghrelin in human prostate neoplasms and
related cell lines. European Journal of Endocrinology 150: 173-84.
Chlebowski RT, Hendrix SL, Langer RD, Stefanick ML, Gass M, Lane D,
Rodabough RJ, Gilligan MA, Cyr MG, Thomson CA, Khandekar J, Petrovitch H,
McTiernan A (2003) Influence of estrogen plus progestin on breast cancer and
mammography in healthy postmenopausal women: the Women's Health Initiative
Randomized Trial. Journal of the American Medical Association 289: 3243-3253.
Corbetta S, Peracchi M, Cappiello V, Lania A, Lauri E, Vago L, Beck-Peccoz P,
Spada A (2003) Circulating ghrelin levels in patients with pancreatic and
gastrointestinal neuroendocrine tumours: identification of one pancreatic ghrelinoma.
Journal of Clinical Endocrinology and Metabolism 88: 3117-3120.
Creasman WT (2005) Breast cancer: the role of hormone therapy. Seminars in
Reproductive Medicine 23: 167-171.
Culig Z, Bartsch G, Hobisch A (2004) Antiandrogens in prostate cancer endocrine
therapy. Current Cancer Drug Targets 4:455-461.
De Vriese C, Gregoire F, DE Neef P, Robberecht P, Delporte C (2005) Ghrelin is
produced by the human erythroleukemic HEL cell line and involved in an autocrine
pathway leading to cell proliferation. Endocrinology 146: 1514-1522.
Duxbury MS, Waseem T, Ito H, Robinson MK, Zinner MJ, Ashley SW, Whang EE
(2003) Ghrelin promotes pancreatic adenocarcinoma cellular proliferation and
invasiveness. Biochemical and Biophysical Research Communications 309: 464-468.
Erickson GF, Magoffin DA, Dyer CA, Hofeditz C (1985) The ovarian androgen
producing cells: a review of structure/function relationships. Endocrine Reviews 6:
371–339.

54
Fernandez-Fernandez R, Navarro VM, Barreiro ML, Vigo EM, Tovar S, Sirotkin
AV, Casanueva FF, Aguilar E, Dieguez C, Pinilla L, Tena-Sempere M (2005) Effects
of chronic hyperghrelinemia on puberty onset and pregnancy outcome in the rat.
Endocrinology 146: 3018-3025.
Gambineri A, Pagotto U, Tschop M, Vicennati V, Manicardi E, Carcello A, Cacciari
M, De Iasio R, Pasquali R (2003) Anti-androgen treatment increases circulating
ghrelin levels in obese women with polycystic ovary syndrome. Journal of
Endocrinological Investigations 26: 629-634.
Gambineri A, Pagotto U, De Lasio R, Meriggiola MC, Costantino A, Patton L, Pelusi
C, Pelusi G, Pasquali R (2005) Short-term modification of sex hormones is
associated with changes in ghrelin circulating levels in healthy normal-weight men.
Journal of Endocrinological Investigations. 28: 241-246.
Gaytan F, Barreiro ML, Chopin LK, Herington AC, Morales C, Pinilla L, Casanueva
FF, Aguilar E, Diéguez C, Tena-Sempere M (2003) Immunolocalization of Ghrelin
and Its Functional Receptor, the Type 1a Growth Hormone Secretagogue Receptor,
in the Cyclic Human Ovary. Journal of Clinical Endocrinology and Metabolism 88:
879-887.
Gaytan F, Barreiro ML, Caminos JE, Chopin LK, Herington AC, Morales C, Pinilla
L, Paniagua R, Nistal M, Casanueva FF, Aguilar E, Dieguez C, Tena-Sempere M
(2004) Expression of ghrelin and its functional receptor, the type 1a growth hormone
secretagogue receptor, in normal human testis and testicular tumors. Journal of
Clinical Endocrinology and Metabolism 89: 400-409.
Gaytan F, Morales C, Barreiro ML, Jeffery P, Chopin LK, Herington AC, Casanueva
FF, Aguilar E, Dieguez C, Tena-Sempere M (2005) Expression of growth hormone
secretagogue receptor type 1a, the functional ghrelin receptor, in human ovarian
surface epithelium, mullerian duct derivatives and ovarian tumors. Endocrinology
90: 1798-1804.

55
Grinspoon S, Miller KK, Herzog DB, Grieco KA, Klibanski A (2004) Effects of
estrogen and recombinant human insulin-like growth factor-I on ghrelin secretion in
severe undernutrition. Journal of Clinical Endocrinology and Metabolism 89: 3988-
3993.
Haslam SZ, Woodward TL (2003) Host microenvironment in breast cancer
development: epithelial-cell-stromal-cell interactions and steroid hormone action in
normal and cancerous mammary gland. Breast Cancer Research 5: 208-215.
Iwakura H, Hosoda K, Doi R, Komoto I, Nishimura H, Son C, Fujikura J, Tomita T,
Takaya K, Ogawa Y, Hayashi T, Inoue G, Akamizu T, Hosoda H, Kojima M,
Kangawa K, Imamura M, Nakao K (2002) Ghrelin expression in islet cell tumours:
augmented expression of ghrelin in a case of glucagonoma with multiple endocrine
neoplasm type I. Journal of Clinical Endocrinology and Metabolism 87: 4885-4888.
Jeffery P, Herington A, Chopin L (2002) Expression and action of the growth
hormone releasing peptide ghrelin and its receptor in prostate cancer cell lines.
Journal of Endocrinology 172: 7-11.
Kellokoski E, Poykko SM, Karjalainen AH, Ukkola O, Heikkinen J, Kesaniemi YA,
Horkko S (2005) Estrogen replacement therapy increases plasma ghrelin levels.
Journal of Clinical Endocrinology and Metabolism 90: 2954-2963.
Kim MS, Yoon CY, Jang PG, Park YJ, Shin CS, Park HS, Ryu JW, Pak YK, Park
JY, Lee KU, Kim SY, Lee HK, Kim YB, Park KS (2004) The mitogenic and
antiapoptotic actions of ghrelin in 3T3-L1 adipocytes. Molecular Endocrinology 18:
2291-2301.
Kim SW, Her SJ, Park SJ, Kim D, Park KS, Lee HK, Han BH, Kim MS, Shin CS,
Kim SY (2005) Ghrelin stimulates proliferation and differentiation and inhibits
apoptosis in osteoblastic MC3T3-E1 cells. Bone 37: 359-369.
Leung KC, Johannsson G, Leong GM, Ho KK (2004) Estrogen regulation of growth
hormone action. Endocrine Reviews 25: 693-721.

56
Maccarinelli G, Sibilia V, Torsello A, Raimondo F, Pitto M, Giustina A, Netti C,
Cocchi D (2005) Ghrelin regulates proliferation and differentiation of osteoblastic
cells. Journal of Endocrinology 184: 249-256.
Matsubara M, Sakata I, Wada R, Yamazaki M, Inoue K, Sakai T (2004) Estrogen
modulates ghrelin expression in the female rat stomach. Peptides 25: 289-297.
Mazzocchi G, Neri G, Rucinski M, Rebuffat P, Spinazzi R, Malendowicz LK,
Nussdorfer GG (2004) Ghrelin enhances the growth of cultured human adrenal zona
glomerulosa cells by exerting MAPK-mediated proliferogenic and antiapoptotic
effects. Peptides 25: 1269-1277.
Nanzer AM, Khalaf S, Mozid AM, Fowkes RC, Patel MV, Burrin JM, Grossman A,
Korbonits M (2004) Ghrelin exerts a proliferative effect on a rat pituitary
somatotroph cell line via the mitogen-activated protein kinase pathway. European
Journal of Endocrinology 151: 223-240.
Pagotto U, Gambineri A, Vicennati V, Heiman ML, Tschop M, Pasquali R (2002)
Plasma ghrelin, obesity, and the polycystic ovary syndrome: correlation with insulin
resistance and androgen levels. Journal of Clinical Endocrinology and Metabolism
87: 5625-5629.
Panidis D, Farmakiotis D, Koliakos G, Rousso D, Kourtis A, Katsikis I, Asteriadis C,
Karayannis V, Diamanti-Kandarakis E (2005) Comparative study of plasma ghrelin
levels in women with polycystic ovary syndrome, in hyperandrogenic women and in
normal controls. Human Reproduction 20: 2127-2132.
Ryan KJ, Petro Z (1966) Steroid biosynthesis by human ovarian granulosa and thecal
cells. Journal of Clinical Endocrinology and Metabolism 26: 46-52.
So AI, Hurtado-Coll A, Gleave ME (2003) Androgens and prostate cancer. Journal
of Urology 21: 325-337.

57
Tsolakis AV, Portela-Gomes GM, Stridsberg M, Grimelius L, Sundin A, Eriksson
BK, Oberg KE, Janson ET (2004) Malignant gastric ghrelinoma with
hyperghrelinemia. Journal of Clinical Endocrinology and Metabolism 89: 3739-
3744.
Veldhuis JD, Bowers CY (2003) Sex steroid modulation of growth hormone (GH)
secretory control: three-peptide ensemble regulation under dual feedback restraint by
GH and IGF-1. Endocrine 22: 25-40.
Volante M, Allia E, Fulcheri E, Cassoni P, Ghigo E, Muccioli G, Papotti M (2003)
Ghrelin in fetal thyroid and follicular tumors and cell lines: expression and effects on
tumor growth. American Journal of Pathology 162: 645-654.
Waters MJ, Conway-Campbell BL (2004) The oncogenic potential of autocrine
human growth hormone in breast cancer. Proceedings of the National Academy of
Sciences of the United States of America 101:14992-14993.
Zhang W, Lin TR, Hu Y, Fan Y, Zhao L, Stuenkel EL, Mulholland MW (2004)
Ghrelin stimulates neurogenesis in the dorsal motor nucleus of the vagus. Journal of
Physiology 559: 729-737.

58

59
CHAPTER THREE
GHRELIN AND A NOVEL PREPROGHRELIN ISOFORM ARE
HIGHLY EXPRESSED IN PROSTATE CANCER COMPARED
TO NORMAL PROSTATE TISSUE AND GHRELIN-MEDIATED
PROSTATE CANCER CELL LINE PROLIFERATION
INVOLVES THE MAPK PATHWAY
Anthony H. Yeh*, Penelope L. Jeffery*, Russell P. Duncan, Adrian C. Herington and
Lisa K. Chopin
* These two authors contributed equally to the work as first authors.
Clinical Cancer Research (2005), in press
halla
This article is not available online. Please consult the hardcopy thesis available from the QUT Library

95
CHAPTER FOUR
EXPRESSION AND FUNCTION OF THE GHRELIN AXIS,
INCLUDING A NOVEL PREPROGHRELIN ISOFORM, IN
HUMAN BREAST CANCER TISSUES AND CELL LINES
Jeffery PL, Murray RE, Yeh AH, McNamara JF, Duncan RP, Francis G,
Herington AC and Chopin LK.
Endocrine-Related Cancer (2005), in press
halla
This article is not available online. Please consult the hardcopy thesis available from the QUT Library

127
CHAPTER FIVE
EXPRESSION OF THE GHRELIN AXIS IN THE MOUSE: AN
EXON 4-DELETED MOUSE PROGHRELIN VARIANT
ENCODES A NOVEL C-TERMINAL PEPTIDE
PL Jeffery, RP Duncan, AH Yeh, RA Jaskolski, DS Hammond, AC Herington and
LK Chopin.
Endocrinology (2005) 146: 432-440.
halla
This article is not available online. Please consult the hardcopy thesis available from the QUT Library

163
CHAPTER SIX
GENERAL DISCUSSION
The discovery of the peptide hormone ghrelin in 1999, several years after
its endogenous receptor, the growth hormone secretagogue receptor (GHS-R) was
identified, has had a substantial impact upon the field of endocrinology. The
ubiquitous expression of ghrelin in the body, as well as its significant concentration
in serum (Kojima et al. 1999), suggests a wide range of physiological roles for this
unique hormone, in addition to growth hormone (GH) release. There is an expanding
body of research supporting a role for ghrelin and its receptor in cancer. Our previous
work published in 2002, was the first to report the expression of ghrelin, an exon 3-
deleted preproghrelin mRNA variant, and the GHS-R in prostate cancer cell lines and
also reported the growth-promoting effect of ghrelin on PC3 prostate cancer cells in
vitro (Jeffery et al. 2002). This work led to our hypothesis that ghrelin is a growth
factor in prostate cancer and, potentially, other cancers. Prostate and breast cancer
are hormone-dependent cancers that are significant causes of cancer mortality in
Western men and women respectively (Jemal et al. 2005) and are sensitive to the
effects of growth factors and cytokines. Therefore, a logical extension of my initial
studies in prostate cancer cell lines (Jeffery et al. 2002) was to investigate the role of
the ghrelin axis in breast cancer.
Our hypothesis that ghrelin is a growth factor for cancer required further
elucidation and therefore the objectives of this thesis were to investigate the
expression and function of the ghrelin axis in human hormone-dependent cancers,
specifically prostate and breast cancer. These studies include the description of a
novel ghrelin isoform, exon 3-deleted preproghrelin. The salient findings of this
project include the full description of exon 3-deleted preproghrelin expression in
prostate and breast cancer, the identification of ghrelin and exon 3-deleted
preproghrelin as potential diagnostic markers for cancer and the identification of the
ghrelin axis as a novel target for therapeutics. A full characterisation of the murine
ghrelin axis, as a prelude to future in vivo studies using mouse models, has also been
performed.

164
Characterisation of the exon 3-deleted preproghrelin isoform
The expression of the human exon 3-deleted preproghrelin mRNA variant
was first identified in prostate cancer cell lines (Jeffery et al. 2002) and in this thesis
I have characterised its expression and explored the potential functions of this novel
isoform in prostate cancer and breast cancer tissues and cell lines. Translation of the
full-length human preproghrelin transcript results in a 117 amino acid peptide that is
processed to produce the 28 amino acid mature ghrelin hormone (Kojima et al.
1999). Low molecular weight peptides derived from the carboxy terminus of
proghrelin, which may possess cardiovascular activity, are also present in human
serum (Pemberton et al. 2003). Exclusion of exon 3 from the preproghrelin
transcript results in a truncated preproghrelin peptide of 91 amino acids, with a
unique 16 amino acid C-terminal peptide sequence (C terminal 3 peptide). The C-
terminal peptide begins with a pair of arginine residues, known to be a classic
protease cleavage signal for prohormones (Docherty and Steiner, 1982, Seidah and
Chretien, 1997). Bioinformatic analysis of the dibasic sequence demonstrates that it
is a trypsin cleavage site (Expasy Proteomics Server, Swiss Institute of
Bioinformatics), indicating that C- terminal 3 peptide may be cleaved and exist
independently from the rest of exon 3-deleted preproghrelin. Using Western blot
analysis, we were able to determine that cleavage of C terminal 3 peptide from the
rest of the exon 3-deleted preproghrelin peptide does occur in human stomach tissue
and in LNCaP prostate cancer cell lysate (Chapter 3). Importantly, the exon 3-
deleted preproghrelin isoform retains sequence coding for the mature ghrelin peptide
(Figure 1). Using primers specific for the exon 3-deleted preproghrelin transcript, I
have now demonstrated the expression of the isoform in prostate (Chapter 3) and
breast cancer specimens and cell lines (Chapter 4), and in a range of other human
tissues including anterior pituitary and placenta (Jeffery et al. in preparation). The
antibody used to detect protein expression of the exon 3-deleted preproghrelin was
raised against the C-terminal peptide and displayed specificity for the isoform. This
is the only antibody currently available that can distinguish the unique isoform from
full-length preproghrelin protein and has enabled detection of exon 3-deleted
preproghrelin expression in prostate and breast tissue specimens by
immunohistochemistry. Measurement of C-ghrelin peptide concentrations in human
blood has recently been successfully performed (Pemberton et al. 2003) and a similar

165
approach using HPLC coupled with RIA could be used in the future to quantitate C-
terminal 3 peptide immunoreactivity in serum taken from prostate and breast
cancer patients.
A comparison of the exon 3-deleted preproghrelin sequence with those in
EST databases (Blast, NCBI) unearthed an homologous preproghrelin sequence in a
mixed mouse pancreas library (GenBank accession # BM054332), leading to the
discovery and characterisation of the murine homologue (Chapter 5). This isoform
was named exon 4-deleted preproghrelin because the mouse ghrelin gene was known
to consist of 5 exons (Tanaka et al. 2001). It has since been demonstrated that human
ghrelin gene also consists of five exons (Kanamoto et al. 2004), although the human
exon 3-deleted preproghrelin has been named according to coding exons only.
Along with murine GHS-R and ghrelin, exon 4-deleted preproghrelin was detected in
a wide-range of mouse tissues, with stomach being the predominant site of exon 4-
deleted preproghrelin synthesis (Jeffery et al. 2005; Chapter 5). The unique C-
terminal peptide of mouse exon 4-deleted preproghrelin exhibits significant
homology (approximately 60%) with its human counterpart. This peptide sequence
conservation suggests a functional role for the novel isoform.
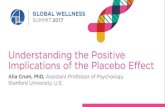
Exon 3-deleted preproghrelin
Full-length preproghrelin
Signal peptide Ghrelin C-peptide
Amino acids 23 51 117
Signal peptide Ghrelin
RPQPTSDRPQALLTSL (C-terminal 3 peptide)
C-peptideProteolytic cleavage site
Amino acids 23 51 91
Figure 1. Schematic depiction of full-length and exon 3-deleted preproghrelin proteins.
Full-length preproghrelin is a 117 amino acid prohormone which is processed to produce the
mature ghrelin hormone. Deletion of exon 3 from the preproghrelin transcript generates a
premature stop codon and therefore a truncated C-peptide with a novel pro-fragment (C-
terminal 3 peptide). The introduction of a dibasic cleavage site (RR) may allow cleavage of this
C-terminal pro-fragment in vivo.

166
The identification of ghrelin and exon 3-deleted preproghrelin as potential
diagnostic markers for hormone-dependent cancer
Better indicators of prostatic disease and tumour progression are urgently
required. The widely used serum prostate-specific antigen (PSA) test for prostate
malignancy is limited by poor specificity (Thompson et al. 2004), and there are
currently no reliable prognostic markers for prostate cancer (Watson and Schalken,
2004). Similarly, there are few validated prognostic markers for breast cancer,
although expression of growth factors and their receptors (for example HER-2/neu)
are often included in diagnostic profiles of breast disease (Coradini and Daidone,
2004). Immunohistochemistry is commonly employed for detection and localization
of protein expression in histological sections; however, it is also emerging as an
important tool in the diagnosis of malignant changes in tissue, as well as for grading
tumour severity. Prognostication aided by immunohistochemical markers has the
potential to better predict prostate cancer behaviour than traditional histological
grading alone (Sivridis et al. 2002, Epstein, 2004). The immunohistochemical studies
performed in this project revealed that both ghrelin and the novel preproghrelin
isoform are more abundantly expressed in malignant tissues when compared to levels
of expression in normal tissues. At the protein level, greater immunoreactivity for
ghrelin and exon 3-deleted preproghrelin was found in human prostatectomy tumour
specimens than normal prostate tissue by immunohistochemistry (Chapter 3). This
was also found to be the case in breast cancer specimens when compared to normal
breast tissue (Chapter 4) and this suggests that ghrelin and exon 3-deleted
preproghrelin may represent novel diagnostic or prognostic immunohistochemical
markers for prostate and breast cancer.
Real-time RT-PCR is an effective, sensitive technique for the detection and
quantitation of low levels of mRNA expression (Pfaffl et al. 2002). Ghrelin mRNA is
known to be a low abundance mRNA species, therefore, we utilised this technique to
quantitate full-length preproghrelin and exon 3-deleted preproghrelin transcripts in
breast cancer cell lines of varying oncogenic phenotypes. Two methods of
quantitation are possible: absolute and relative quantitation. In this project, the
relative quantitation strategy was employed. This method is based on the expression
ratio of a target transcript versus a reference transcript (in this case 18S ribosomal

167
RNA). This technique is effective for detecting changes in the mRNA levels between
different samples and has been used successfully to investigate potential prognostic
markers in breast cancer (Peirce and Chen, 2001). Importantly, real time RT-PCR
demonstrated that exon 3-deleted preproghrelin transcript expression is significantly
up-regulated in highly malignant breast cancer cell lines (MDA-MB-231 and MDA-
MB-435) when compared to a benign breast epithelial cell line (MCF-10A). This
reflects our data generated from immunohistochemical studies on breast tissues and
provides more evidence for a role for the unique isoform in breast cancer, including
its potential as a novel diagnostic marker (Chapter 4).
Current mathematical models used to analyse data generated with the relative
quantitation strategy allow for only one transcript to be quantitated at a time – that is,
relative expression levels of a single transcript can be compared between samples,
however, multiple transcripts cannot. Software that can compare the relative
expression levels of up to four target genes in a sample has been developed to
circumvent this problem (Pfaffl et al. 2002) and could be useful for future studies.
This would allow the direct comparison of full-length and exon 3-deleted
preproghrelin transcript levels in one tissue and would allow us to determine if
transcription of the exon 3-deleted preproghrelin isoform is favoured over full-length
preproghrelin, as is the case for many alternatively-spliced transcripts in tumour
tissues (Venables, 2004). During the course of this project, real time RT-PCR
analysis of prostate cancer specimens for ghrelin and exon 3-deleted preproghrelin
expression was commenced; however, difficulty in obtaining prostate tumour
samples did not allow completion of this task. Full evaluation and validation of
ghrelin and exon 3-deleted preproghrelin as novel prognostic markers for prostate
and breast cancer requires further experiments with a larger number of
histopathological specimens. This work is clearly warranted given the data presented
in this thesis.
Identification of the ghrelin axis as a potential target for therapeutics in prostate and
breast cancer
The mechanism behind the proliferative effect of ghrelin in the LNCaP and
PC3 prostate cancer cell lines (Jeffery et al. 2002) was further explored in this study.

168
Ghrelin is the endogenous ligand for the GHS-R; a G protein-coupled receptor
(GPCR) (Kojima et al. 1999, Sun et al. 2004) that is expressed in prostate cancer cell
lines and tissues (Jeffery et al. 2002, Chapter 3) and may be involved in an
autocrine/paracrine loop in ghrelin-mediated prostate cancer cell proliferation
(Jeffery et al. 2002). GPCR signalling by various ligands can generate a mitogenic
response in prostate cell lines, often via crosstalk with mitogen activated protein
kinase (MAPK) pathways (Daaka, 2004). Phosphorylated (activated) MAPKs,
specifically the extracellular-signal regulated kinases (ERK 1 and 2), have been
implicated in prostate tumourigenesis, and growth factor-induced activation of
MAPK pathways results in increased cell proliferation and metastasis (Maroni et al.
2004). Murata and co-workers reported that ghrelin upregulates MAPK activity and
cell proliferation in the hepatoma cell line HepG2 (Murata et al. 2002) and therefore,
we speculated that this might also occur in prostate cancer cell lines (Figure 2). In
studies carried out primarily by an Honours student in our laboratory (Anthony Yeh),
it was shown that ghrelin did indeed rapidly activate the extracellular-signal
regulated kinases (ERKs) in the LNCaP and PC3 prostate cancer cell lines, an effect
that was completely abolished with specific MAPK inhibitors (Chapter 3, Yeh et al,
in press). The alternative MAPK pathway, the p38 kinase pathway, was also
activated (phosphorylated) in the LNCaP cell line after ghrelin treatment (Chapter 3).
Phosphorylated p38 MAPK activates transcription factors and cell-cycle regulators
which in turn influence cell proliferation, apoptosis and splicing events (Olson and
Hallahan, 2004). In the MCF-10A breast epithelial cell line, the p38 MAPK pathway
also interacts with the ERK 1/2 cascade resulting in increased cell migration and
invasion (Kim et al. 2003). Phospho-p38 MAPK can also activate the pro-survival
PI3K/AKT pathway (Horowitz et al. 2004) and ghrelin has also been shown to signal
through the PI3/AKT pathway in some cell types (Duxbury et al. 2003); therefore,
further work focusing on the downstream effects ghrelin-induced p38 activation in
prostate cancer is required.
Although ghrelin did not appear to protect prostate cancer cells from
chemically-induced apoptosis, the potential effect of ghrelin on apoptosis and cell
survival could be more accurately quantified using a Cell Death ELISAPLUS (Roche)
to measure DNA fragmentation and a Caspase 3 Activity Assay (Roche), both using
a fluorescence microplate reader (PolarSTAR, BMG). Direct observation of DNA

169
fragmentation could also be achieved by fluorescent microscopy using a TUNEL
assay (In situ cell death detection kit, Roche) on cells grown on coverslips. The
influence of ghrelin treatment on the regulation of genes that are anti-apoptotic (Bcl-
2/BclXL, NF-κB, IGF-I, caveolin and Akt) or pro-apoptotic (PTEN, p53, Bin1,
TGF-beta, and Par-4) in prostate cancer (Gurumurthy et al. 2001) could be
determined using real-time PCR, although not all of these genes are present in all of
the cell lines used in this study.
A number of studies have since been published demonstrating that ghrelin
augments cell proliferation via MAPK activation in a range of cell lines (Andreis et
al. 2003, Kim et al. 2004, Mazzocchi et al. 2004, Nanzer et al. 2004, Zhang et al.
2004). The finding that the proliferative effect of ghrelin in prostate cancer cells is
primarily a result of ghrelin-induced MAPK pathways is extremely significant given
that new treatments for hormone-refractory prostate cancer are urgently required,
with MAPK cascades being a promising new target for anti-cancer therapy (Maroni
et al. 2004) (Figure 2).

170

171
Ghrelin gene
Autocrine ghrelin
Paracrine ghrelin
Increased cell proliferation
Exon 3-deleted preproghrelin
Figure 2. A proposed model of ghrelin-mediated cell proliferation in prostate cancer
cells.
Ghrelin is produced by prostate cancer cells and is secreted into culture medium.
Secreted ghrelin may then act in an autocrine/paracrine fashion to stimulate MAPK
cascades via the GHS-R, which is also expressed in prostate cancer. Phosphorylation
of ERK 1 and 2 by exogenous ghrelin treatment stimulates prostate cancer cell
proliferation. Activated ERK 1 and 2 may also bind transcription factors (TF)
including ELK-1. Binding sites for ELK-1 exist on the ghrelin promoter (Kanamoto et
al. 2004); hence, autocrine/paracrine ghrelin action may also augment ghrelin
production, further driving cell proliferation. The novel exon 3-deleted preproghrelin
isoform is also expressed by prostate cancer cells, although its precise function is as
yet unknown. MAPK inhibitors decrease cancer cell proliferation (blue arrows) and
blocking of ghrelin production, secretion or signalling (red arrows) may also
antagonize MAPK cascades, thereby representing a novel therapeutic approach for
cancer in the future. This model may also be applicable to breast cancer cells and
other hormone-dependent cancer cell types.
GHS-RERK /MAPK
P
preproghrelin
inter-cascade cross-talk
TF
Inhibition of cell proliferation ?
MAPK inhibition

172

173
Ghrelin stimulates cultured pituitary cells to secrete growth hormone (GH)
(Kojima et al. 1999). GH is a potent mitogen for prostate cancer cells in vitro
(Untergasser et al. 1999), and has been identified as being an important oncogene in
breast cancer (Zhu et al. 2005). As prostate cancer cells have been shown to express
the GH axis (Chopin et al. 2002a), a commercial GH ELISA (Roche) was used to
determine if the addition of ghrelin to prostate cancer cells induced the secretion of
prostatic GH in vitro. Neither ghrelin nor C-terminal 3 peptide induced measurable
GH release from LNCaP or PC3 prostate cancer cell lines (data not shown).
However, investigating the effect of ghrelin treatment on expression of GH, and its
downstream mediator insulin-like growth factor I (IGF-I), in the prostate in vivo is an
important area of future study.
Functional assays demonstrating that ghrelin promotes proliferation in breast
cancer cell lines also supports previous work performed in prostate cancer cell lines
(Jeffery et al. 2002, Chapter 3). However, this contrasts with reports published by
other groups. In particular, ghrelin has been shown to inhibit cell proliferation of
breast and thyroid carcinoma cell lines in vitro (Cassoni et al. 2001, Volante et al.
2003). The proliferative actions of ghrelin appear to be cell-specific, possibly due to
GHS-R subtype expression and crosstalk between signalling pathways (Duxbury et
al. 2003, Maroni et al. 2004). The acylation status of ghrelin also clearly influences
the function of the peptide (Ariyasu et al. 2004) and the octanoic acid modification
of ghrelin is lost rapidly with non-optimum storage conditions (Hosoda et al. 2004).
Des-acyl ghrelin has recently been shown to have a negative impact on tissue growth
in an over-expressing mouse model, potentially via the modulation of octanoylated
ghrelin-induced GH secretion (Ariyasu et al. 2005). Evidence to support a clear role
for ghrelin in the mitogenesis of a range of cell lines in vitro now exists (see
Literature update, Chapter 2). The moderate yet significant increase in cell growth
post-ghrelin treatment may be due to the fact that autocrine production of
endogenous ghrelin (Figure 2) is sufficient to stimulate proliferation, as is postulated
to be the case with the human erythroleukemic cell line HEL (DeVriese et al. 2005).
The use of anti-sense technology to downregulate ghrelin expression could help to
clarify this issue in the future. Indeed, inhibition of ghrelin signalling may have
therapeutic potential in prostate and breast (Chopin et al. 2002b); however, effective
ghrelin/GHS-R antagonists were not available during the course of this project.

174
Potent and selective ghrelin analogues that bind to the GHS-R and inhibit ghrelin
signalling have recently been developed (Halem et al. 2004, Liu et al. 2004) and may
prove useful for inhibition of the ghrelin axis in prostate and breast cancer.
Treatment of prostate and breast cancer cell lines with the C-terminal peptide
of exon 3-deleted preproghrelin (C-terminal 3 peptide) had no effect on
proliferation or MAPK phosphorylation, and the primary role of the isoform may
only be to produce the mature ghrelin peptide (Figure 1). I have established a
continuous cell line derived from normal epithelial prostate cells (RWPE-1, Bello et
al. 1997) and the PC3 prostate cancer cell lines, transfected with exon 3-deleted
preproghrelin mRNA using a tetracycline-regulated expression system for
mammalian cells (T-Rex, Invitrogen). The phenotype of these cell lines is currently
being investigated and will allow a more thorough functional analysis of the novel
isoform in the future. Prostate cancer cell lines overexpressing full-length
preproghrelin have also been generated in our laboratory, although due to time
constraints, their phenotypes have yet to be examined. Migration of RWPE-1 cells
towards a chemoattractant (bovine calf serum) is increased in the presence of
exogenous ghrelin (data not shown) and therefore it would be interesting to examine
the migratory properties of these overexpressing cell lines and the behaviour of
breast cancer cell lines transfected with these constructs. Future studies involving the
subcutaneous or subcapsular renal injection of the transfected cells into nude or
SCID mice would also be valuable in assessing the metastatic potential of prostate or
breast cancer cells overexpressing ghrelin and or exon 3-deleted preproghrelin in an
in vivo model.
This project has relied heavily on the use of experimentally immortalized cell
lines for in vitro functional assays and for extraction of RNA and protein. It is a
regular criticism that cell-based assays are not physiologically relevant and that cell
line models are not valid representations of disease in vivo. The immortalization of
cells, essential to circumvent natural cell senescence, often results in karyotypic
change, a transformed phenotype, and selection of non-representative cell
populations (Navone et al. 1999, Gudjonsson et al. 2004). However, transformed cell
lines are relatively inexpensive to maintain, safe to manipulate and provide valuable
preliminary in vitro data, often providing the justification for more expensive and

175
difficult in vivo investigations. Although the availability of human tumour tissue
samples has been limited over the course of this project, data generated from cell
lines and in vitro cell assays have allowed us to establish excellent collaborations
with the medical fraternity, thereby providing substantial resources of clinical
samples for future work. In addition, the future use of primary cell cultures,
multicellular spheroids (three-dimensional aggregates of cells) and anchorage-
independent cell culture (via soft agar assays) may also provide a better model of in
vivo tumour behaviour than traditional monolayer cell culture. For example, spheroid
cell culture has been shown to more accurately reflect tumour microenvironment and
stromal-epithelial interactions (Hamilton, 1998, Bates et al. 2000). A more accurate
depiction of the role of the ghrelin axis in hormone-dependent cancer is likely to be
generated, however, through the future use of in vivo mouse models.
The characterisation of the ghrelin axis in the mouse for the future development of
mouse models of cancer.
Mouse models of prostate and breast cancer are important tools for studying
the mechanisms behind early and late carcinogenesis (Abate-Shen and Shen, 2002,
Cardiff et al. 2003), particularly when there are difficulties in accessing human tissue
specimens. They also allow in vivo investigations into the physiological effects of
administration of compounds, as well as chemoprevention studies, which would be
otherwise unfeasible. In the TRAMP (Transgenic Adenocarcinoma Mouse Prostate)
mouse model, specific expression of the oncogene SV40 T antigen in prostate
epithelia is driven by the prostate-specific probasin promoter and results in the
development of prostate cancer and subsequent distant site metastases (Greenberg et
al. 1995). Interrogation of signalling pathways in TRAMP mice has demonstrated
the importance of growth factors including IGF-I in prostate cancer progression
(Foster et al. 1999) and it would be interesting to investigate in vivo ghrelin/GHS-R
expression and signalling in this manner. To ensure that future studies of the ghrelin
axis in this and other mouse models of cancer are warranted, we examined the
expression of the axis in a wide range of mouse tissues (Chapter 5, Jeffery et al.
2005). This report is the first to fully characterise the expression of ghrelin, a murine
homologue of exon 3-deleted preproghrelin, and the GHS-R type 1a in the mouse.
This will serve as an important reference for the examination of the role of the

176
ghrelin axis in development/progression of prostate cancer and other hormone-
dependent cancers, including breast cancer. This work has also generated important
collaborations with international research groups. Ongoing work includes in vivo
mouse studies to investigate the potential function of the exon 3-deleted
preproghrelin variant via injection of the novel isoform into mice and binding assays
investigating its affinity for orphan G protein-coupled receptors.
In summary, this study has provided new and compelling evidence that
supports a role for the ghrelin axis in hormone-dependent cancer and specifically in
prostate and breast cancer. We have identified several potential diagnostic markers
for prostate and breast cancer within the ghrelin axis. Ghrelin stimulates proliferation
of hormone-dependent cancer cells and therefore the ghrelin axis represents a novel
target for the treatment of such cancers (Figure 2). This project has also provided a
basis for future in vivo work in mouse models, which will potentially aid in the
development of new adjunctive therapies for prostate and breast cancer.

177
REFERENCES
Abate-Shen C, Shen MM (2002) Mouse models of prostate carcinogenesis. Trends in
Genetics 18: 1-5.
Andreis PG, Malendowicz LK, Trejter M, Neri G, Spinazzi R, Rossi GP, Nussdorfer
GG (2003) Ghrelin and growth hormone secretagogue receptor are expressed in the
rat adrenal cortex: Evidence that ghrelin stimulates the growth, but not secretory
activity of adrenal cells. FEBS Letters 536: 173-179.
Ariyasu H, Takaya K, Iwakura H, Hosoda H, Akamizu T, Arai Y, Kangawa K &
Nakao K (2005) Transgenic mice overexpressing des-acyl ghrelin show small
phenotype. Endocrinology 146: 355-364.
Bates RC, Edwards NS, Yates JD (2000) Spheroids and cell survival. Critical
Reviews in Oncology/Hematology 36: 61-74.
Bello D, Webber MM, Kleinman HK, Wartinger DD, Rhim JS (1997). Androgen
responsive adult human prostatic epithelial cell lines immortalized by human
papillomavirus 18. Carcinogenesis 18: 1215-1223.
Cardiff RD (2003) Mouse models of human breast cancer. Comparative Medicine
53: 250-253.
Cassoni P, Papotti M, Ghe C, Catapano F, Sapino A, Graziani A, Deghenghi R,
Reissmann T, Ghigo E, Muccioli G (2001). Identification, characterisation and
biological activity of specific receptors for natural (ghrelin) and synthetic growth
hormone secretagogues and analogs in human breast carcinoma and cell lines.
Journal of Clinical Endocrinology and Metabolism 86: 1738-45.
Chopin LK, Veveris-Lowe TL, Philipps AF, Herington AC (2002a) Co-expression of
GH and GHR isoforms in prostate cancer cell lines. Growth Hormone and IGF
Research 12: 126-136.

178
Chopin LK, Jeffery PL, Herington AC (2002b) Reproductive cancer diagnosis and
therapy. International Patent PCT/AU02/00582 (14/11/2002).
Coradini D, Daidone MG (2004) Biomolecular prognostic factors in breast cancer.
Current Opinions in Obstetrics and Gynecology. 16: 49-55.
Daaka Y (2004) G proteins in cancer: the prostate cancer paradigm. Science “Signal
Transduction Knowledge Environment” 216: 2.
De Vriese C, Gregoire F, DE Neef P, Robberecht P, Delporte C (2005) Ghrelin is
produced by the human erythroleukemic HEL cell line and involved in an autocrine
pathway leading to cell proliferation. Endocrinology 146: 1514-1522.
Docherty K and Steiner DF (1982) Post-translational proteolysis in polypeptide
hormone biosynthesis. Annual Review of Physiology 44: 625-638.
Duxbury MS, Waseem T, Ito H, Robinson MK, Zinner MJ, Ashley SW, Whang EE
(2003) Ghrelin promotes pancreatic adenocarcinoma cellular proliferation and
invasiveness. Biochemical and Biophysical Research Communications 309: 464-468.
Epstein JL (2004) Diagnosis and reporting of limited adenocarcinoma of the prostate
on needle biopsy. Modern pathology: an official journal of the United States and
Canadian Academy of Pathology, Inc: 307-315.
Foster BA, Kaplan PJ, Greenberg NM (1999) Peptide growth factors and prostate
cancer: new models, new opportunities. Cancer and Metastasis Reviews 17: 317-324.
Greenberg NM, De Mayo F, Finegold MJ, Medina D, Tilley WD, Aspinall JO,
Cunha GR, Donjacour AA, Matusik RJ, Rosen JM (1995) Prostate cancer in a
transgenic mouse. Proceedings of the National Academy of Sciences of the United
States of America 92: 3439-3443.

179
Gudjonsson T, Villadsen R, Ronnov-Jessen L, Petersen OW (2004) Immortalization
protocols used in cell culture models of human breast morphogenesis. Cellular and
Molecular Life Sciences 61: 2523-2534.
Gurumurthy S, Vasudevan KM, Rangnekar VM (2001) Regulation of apoptosis in
prostate cancer. Cancer Metastasis Reviews 20:225-43.
Halem HA, Taylor JE, Dong JZ, Shen Y, Datta R, Abizaid A, Diano S, Horvath T,
Zizzari P, Bluet-Pajot M, Epelbaum J, Culler MD (2004) Novel analogs of ghrelin:
physiological and clinical implications. European Journal of Endocrinology 151:71-
75.
Hamilton G (1998) Multicellular spheroids as an in vitro tumor model. Cancer letters
131: 29-34.
Horowitz JC, Lee DY, Waghray M, Keshamouni VG, Thomas PE, Zhang H, Cui Z,
Thannickal VJ (2004) Activation of the pro-survival phosphatidylinositol 3-
kinase/AKT pathway by transforming growth factor-beta 1 in mesenchymal cells is
mediated by p38 MAPK-dependent induction of an autocrine growth factor. Journal
of Biological Chemistry 279: 1359-1367.
Hosoda H, Doi K, Nagaya N, Okumura H, Nakagawa E, Enomoto M, Ono F,
Kangawa K (2004) Optimum collection and storage conditions for ghrelin
measurements: octanoyl modification of ghrelin is rapidly hydrolyzed to desacyl
ghrelin in blood samples. Clinical Chemistry 50: 1077-1080.
Jeffery PL, Herington AC, Chopin LK (2002) Expression and action of the growth
hormone-releasing peptide ghrelin and the growth hormone secretagogue receptor in
prostate cancer cell lines. Journal of Endocrinology 172: 7-11.
Jeffery PL, Duncan RP, Yeh AH, Jaskolski RJ, Hammond DS, Herington AC,
Chopin LK (2005) Expression of the ghrelin/GHS-R axis in the mouse: an exon 4-
deleted proghrelin variant encondes a novel C-terminal peptide. Endocrinology 146:
432-440.

180
Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ
(2005) Cancer Statistics, 2005. CA: A cancer journal for clinicians 55: 10-30.
Kanamoto N, Akamizu T, Tagami T, Hataya Y, Moriyama K, Takaya K, Hosoda H,
Kojima M, Kangawa K, Nakao K (2004) Genomic structure and characterization of
the 5'-flanking region of the human ghrelin gene. Endocrinology 145: 4144-4153.
Kim MS, Lee EJ, Kim HR, Moon A (2003) p38 kinase is a key signaling molecule
for H-Ras-induced cell motility and invasive phenotype in human breast epithelial
cells. Cancer Research 63: 5454-5461.
Kim MS, Yoon CY, Jang PG, Park YJ, Shin CS, Park HS, Ryu JW, Pak YK, Park JY
Lee KU, Kim SY, Lee HK, Kim YB, Park KS (2004) The mitogenic and
antiapoptotic actions of ghrelin in 3T3-L1 adipocytes. Molecular Endocrinology 18:
2291-2301.
Kojima M, Hosodo H, Date Y, Nakazato M, Matsuo H, Kanagawa, K (1999) Ghrelin
is a growth hormone releasing acylated peptide from stomach. Nature 402: 656-660.
Liu B, Liu G, Xin Z, Serby MD, Zhao H, Schaefer VG, Falls HD, Kaszubska W,
Collins CA, Sham HL (2004) Novel isoxazole carboxamides as growth hormone
secretagogue receptor (GHS-R) antagonists. Bioorganic and Medicinal Chemistry
Letters 14: 5223-5226.
Maroni PD, Koul S, Meacham RB, Koul H (2004) Mitogen activated protein kinase
signal transduction pathways in the prostate. Cell Communication and Signaling 2:5-
18.
Mazzocchi G, Neri G, Rucinski M, Rebuffat P, Spinazzi R, Malendowicz LK,
Nussdorfer GG (2004) Ghrelin enhances the growth of cultured human adrenal zona
glomerulosa cells by exerting MAPK-mediated proliferogenic and antiapoptotic
effects. Peptides 25: 1269-1277.

181
Murata M, Okimura Y, Iida K, Matsumoto M, Sowa H, Kaji H, Kojima M, Kangawa
K, Chihara K (2002) Ghrelin modulates the downstream molecules of insulin
signaling in hepatoma cells. Journal of Biological Chemistry 277: 5667-5674.
Nanzer AM, Khalaf S, Mozid AM, Fowkes RC, Patel MV, Burrin JM, Grossman A,
Korbonits M (2004) Ghrelin exerts a proliferative effect on a rat pituitary
somatotroph cell line via the mitogen-activated protein kinase pathway. European
Journal of Endocrinology 151: 223-240.
Navone NM, Logothetis CJ, von Eschenbach AC, Troncoso P (1999) Model systems
of prostate cancer: Uses and limitations. Cancer and Metastasis Reviews 17: 361-
371.
Olson JM, Hallahan AR (2004) p38 MAP kinase: a convergence point in cancer
therapy. Trends in Molecular Medicine 10: 125-129.
Pemberton C, Wimalasena P, Yandle T, Soule S, Richards M (2003) C-terminal pro-
ghrelin peptides are present in the human circulation. Biochemical and Biophysical
Research Communications. 310: 567-573.
Pfaffl MW, Horgan GW, Dempfle L (2002) Relative expression software tool
(REST©) for group-wise comparison and statistical analysis of relative expression
results in real-time PCR. Nucleic Acids Research 30: 36-46.
Pierce SK, Chen WY (2001) Quantification of prolactin receptor mRNA in multiple
human tissues and cancer cell lines by real time RT-PCR. Journal of Endocrinology
171: 1-4.
Seidah NG, Chretien M (1997) Eukaryotic protein processing: endoproteolysis of
precursor proteins. Current Opinions in Biotechnology 8: 602-607.
Sivridis E, Touloupidis S, Giatromanolaki A (2002) Immunopathological prognostic
and predictive factors in prostate cancer. International Urology and Nephrology 34:
63-71.

182
Sun Y, Wang P, Zheng H, Smith RG (2004) Ghrelin stimulation of growth hormone
release and appetite is mediated through the growth hormone secretagogue receptor.
Proceedings of the National Academy of Sciences of the United States of America
101: 4679-4684.
Tanaka M, Hayashida Y, Iguchi T, Nakao N, Nakai N, Nakashima K (2001)
Organization of the mouse ghrelin gene and promoter: occurrence of a short
noncoding first exon. Endocrinology 142: 3697-3700.
Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL,
Minasian LM, Ford LG, Lippman SM, Crawford ED, Crowley JJ, Coltman CA
(2004) New England Journal of Medicine 350: 2239-2246.
Untergasser G, Rumpold H, Hermann M, Dirnhofer S, Jilg G, Berger P (1999)
Proliferative disorders of the aging human prostate: involvement of protein hormones
and their receptors. Experimental Gerontology 34: 275-287.
Venables JP (2004) Aberrant and alternative splicing in cancer. Cancer Research 64:
7647-7654.
Volante M, Allia E, Fulcheri E, Cassoni P, Ghigo E, Muccioli G, Papotti M (2003)
Ghrelin in fetal thyroid and follicular tumors and cell lines: expression and effects on
tumor growth. American Journal of Pathology 162: 645-654.
Watson RWG, Schalken JA (2004) Future opportunities for the diagnosis and
treatment of prostate cancer. Prostate Cancer and Prostatic Diseases. 7 (Suppl 1): 8-
13.
Yeh AH, Jeffery PL, Duncan RP, Herington AC, Chopin LK (2005) Ghrelin and a
novel preproghrelin isoform are highly expressed in prostate cancer compared to
normal prostate tissue and ghrelin-mediated prostate cancer cell line proliferation
involves the MAPK pathway. Clinical Cancer Research 2005 in press

183
Zhang W, Lin TR, Hu Y, Fan Y, Zhao L, Stuenkel EL, Mulholland MW (2004)
Ghrelin stimulates neurogenesis in the dorsal motor nucleus of the vagus. Journal of
Physiology 559: 729-737.
Zhu T, Starling-Emerald B, Zhang X, Lee KO, Gluckman PD, Mertani HC, Lobie PE
(2005) Oncogenic transformation of human mammary epithelial cells by autocrine
human growth hormone. Cancer Research 65: 317-324.