An in vivo investigation of associations between saliva properties, caries prevalence and potential...
6
An in vivo investigation of associations between saliva properties, caries prevalence and potential lesion activity in an adult UK population Sachin Varma, Avijit Banerjee *, David Bartlett Department of Conservative Dentistry and Prosthodontics, King’s College London Dental Institute at Guy’s, King’s College & St. Thomas’ Hospitals, Guy’s Dental Hospital, London Bridge, London SE1 9RT, UK 1. Introduction There have been few reports on the prevalence of incipient, pre-cavitated lesions. Pitts 1,2 described an epidemiological ‘‘iceberg’’ to explain caries progression with a D4 lesion extending into the pulp and D1 representing pre-cavitated, incipient enamel lesions. Lesions recorded at the D3 threshold are defined as those lesions involving dentine, cavitated or not. Pitts 2 stated that the D3 threshold was most commonly reported by classical epidemiological studies surveying caries incidence, prevalence and aetiolo- gical relationships. The most common method of recording caries for epidemiological studies is the DMFT index (decayed, missing, filled teeth) and DMFS (decayed, missing, filled surfaces). 3 The problems with this index include the missing and filled journal of dentistry 36 (2008) 294–299 article info Article history: Received 2 October 2007 Received in revised form 9 January 2008 Accepted 15 January 2008 Keywords: Caries prevalence Lesion activity Caries detection DMFT Epidemiology ICDAS Saliva abstract Objective: To investigate associations between prevalence and activity of intra-oral incipi- ent, carious lesions and salivary properties tested using the Saliva Check kit (GC Corp., Belgium). Methods: With ethical approval, 58 subjects with >16 teeth underwent clinical/radiographic examination. Conventional decayed, missing, filled teeth/decayed, missing, filled surfaces (DMFT/DMFS) indices and a more recently developed visual index described by International Caries Detection and Assessment System (ICDAS) were used to ascertain caries prevalence. Potential lesion activity was scored using an Ekstrand visual index. Saliva properties tested included hydration, resting pH, stimulated flow and buffering capacity. Spearman’s rank correlation was used to analyse data. Results: No saliva parameters correlated significantly with DMFT/DMFS caries prevalence scores (D3 threshold). The resting pH correlated negatively and significantly with the total number of lesions (r = À0.267, p = 0.043), with ICDAS scores >1(r = À0.333, p = 0.011) and with mild lesions (r = À0.263, p = 0.046). A negative correlation was found between saliva buffer- ing capacity and the potential activity of moderate lesions (ICDAS 3 and 4; r = À0.227, p = 0.035). Conclusions: There appeared to be a correlation between the resting pH of saliva and the prevalence of early lesions as well as the saliva buffering capacity and the potential lesion activity of moderate lesions. A difference was shown between lesion prevalence calculated using traditional DMFT(S) D3 versus the ICDAS D1 thresholding. # 2008 Elsevier Ltd. All rights reserved. * Corresponding author at: Floor 26, Guy’s Dental Hospital, London Bridge, London SE1 9RT, UK. Tel.: +44 207 188 1577; fax: +44 207 188 7486. E-mail address: [email protected] (A. Banerjee). available at www.sciencedirect.com journal homepage: www.intl.elsevierhealth.com/journals/jden 0300-5712/$ – see front matter # 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.jdent.2008.01.009
-
Upload
sachin-varma -
Category
Documents
-
view
214 -
download
1
Transcript of An in vivo investigation of associations between saliva properties, caries prevalence and potential...

j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9
avai lable at www.sc iencedi rec t .com
journal homepage: www. int l .e lsev ierhea l th .com/ journals / jden
An in vivo investigation of associations between salivaproperties, caries prevalence and potential lesionactivity in an adult UK population
Sachin Varma, Avijit Banerjee *, David Bartlett
Department of Conservative Dentistry and Prosthodontics, King’s College London Dental Institute at Guy’s,
King’s College & St. Thomas’ Hospitals, Guy’s Dental Hospital, London Bridge, London SE1 9RT, UK
a r t i c l e i n f o
Article history:
Received 2 October 2007
Received in revised form
9 January 2008
Accepted 15 January 2008
Keywords:
Caries prevalence
Lesion activity
Caries detection
DMFT
Epidemiology
ICDAS
Saliva
a b s t r a c t
Objective: To investigate associations between prevalence and activity of intra-oral incipi-
ent, carious lesions and salivary properties tested using the Saliva Check kit (GC Corp.,
Belgium).
Methods: With ethical approval, 58 subjects with >16 teeth underwent clinical/radiographic
examination. Conventional decayed, missing, filled teeth/decayed, missing, filled surfaces
(DMFT/DMFS) indices and a more recently developed visual index described by International
Caries Detection and Assessment System (ICDAS) were used to ascertain caries prevalence.
Potential lesion activity was scored using an Ekstrand visual index. Saliva properties tested
included hydration, resting pH, stimulated flow and buffering capacity. Spearman’s rank
correlation was used to analyse data.
Results: No saliva parameters correlated significantly with DMFT/DMFS caries prevalence
scores (D3 threshold). The resting pH correlated negatively and significantly with the total
number of lesions (r = �0.267, p = 0.043), with ICDAS scores>1 (r = �0.333, p = 0.011) and with
mild lesions (r = �0.263, p = 0.046). A negative correlation was found between saliva buffer-
ing capacity and the potential activity of moderate lesions (ICDAS 3 and 4; r = �0.227,
p = 0.035).
Conclusions: There appeared to be a correlation between the resting pH of saliva and the
prevalence of early lesions as well as the saliva buffering capacity and the potential lesion
activity of moderate lesions. A difference was shown between lesion prevalence calculated
T(S) D3 versus the ICDAS D1 thresholding.
# 2008 Elsevier Ltd. All rights reserved.
using traditional DMF
1. Introduction
There have been few reports on the prevalence of incipient,
pre-cavitated lesions. Pitts1,2 described an epidemiological
‘‘iceberg’’ to explain caries progression with a D4 lesion
extending into the pulp and D1 representing pre-cavitated,
incipient enamel lesions. Lesions recorded at the D3
threshold are defined as those lesions involving dentine,
* Corresponding author at: Floor 26, Guy’s Dental Hospital, London BridgE-mail address: [email protected] (A. Banerjee).
0300-5712/$ – see front matter # 2008 Elsevier Ltd. All rights reservedoi:10.1016/j.jdent.2008.01.009
cavitated or not. Pitts2 stated that the D3 threshold was
most commonly reported by classical epidemiological
studies surveying caries incidence, prevalence and aetiolo-
gical relationships.
The most common method of recording caries for
epidemiological studies is the DMFT index (decayed, missing,
filled teeth) and DMFS (decayed, missing, filled surfaces).3 The
problems with this index include the missing and filled
e, London SE1 9RT, UK. Tel.: +44 207 188 1577; fax: +44 207 188 7486.
d.
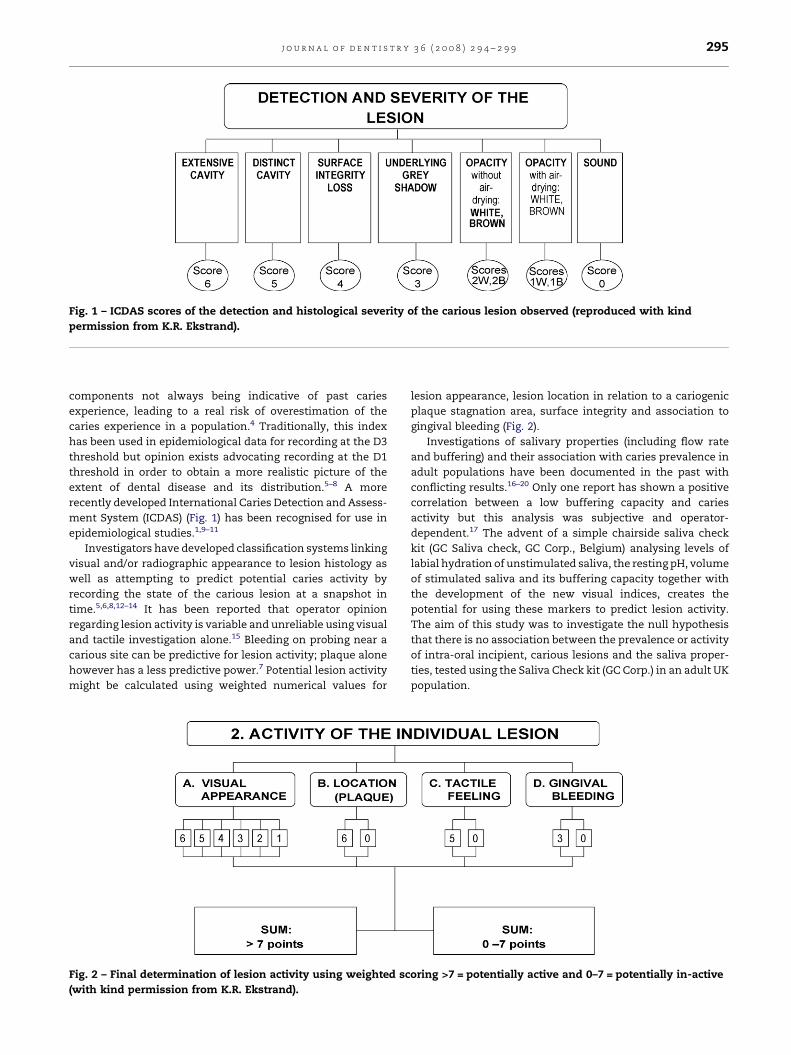
Fig. 1 – ICDAS scores of the detection and histological severity of the carious lesion observed (reproduced with kind
permission from K.R. Ekstrand).
j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9 295
components not always being indicative of past caries
experience, leading to a real risk of overestimation of the
caries experience in a population.4 Traditionally, this index
has been used in epidemiological data for recording at the D3
threshold but opinion exists advocating recording at the D1
threshold in order to obtain a more realistic picture of the
extent of dental disease and its distribution.5–8 A more
recently developed International Caries Detection and Assess-
ment System (ICDAS) (Fig. 1) has been recognised for use in
epidemiological studies.1,9–11
Investigators have developed classification systems linking
visual and/or radiographic appearance to lesion histology as
well as attempting to predict potential caries activity by
recording the state of the carious lesion at a snapshot in
time.5,6,8,12–14 It has been reported that operator opinion
regarding lesion activity is variable and unreliable using visual
and tactile investigation alone.15 Bleeding on probing near a
carious site can be predictive for lesion activity; plaque alone
however has a less predictive power.7 Potential lesion activity
might be calculated using weighted numerical values for
Fig. 2 – Final determination of lesion activity using weighted sc
(with kind permission from K.R. Ekstrand).
lesion appearance, lesion location in relation to a cariogenic
plaque stagnation area, surface integrity and association to
gingival bleeding (Fig. 2).
Investigations of salivary properties (including flow rate
and buffering) and their association with caries prevalence in
adult populations have been documented in the past with
conflicting results.16–20 Only one report has shown a positive
correlation between a low buffering capacity and caries
activity but this analysis was subjective and operator-
dependent.17 The advent of a simple chairside saliva check
kit (GC Saliva check, GC Corp., Belgium) analysing levels of
labial hydration of unstimulated saliva, the resting pH, volume
of stimulated saliva and its buffering capacity together with
the development of the new visual indices, creates the
potential for using these markers to predict lesion activity.
The aim of this study was to investigate the null hypothesis
that there is no association between the prevalence or activity
of intra-oral incipient, carious lesions and the saliva proper-
ties, tested using the Saliva Check kit (GC Corp.) in an adult UK
population.
oring >7 = potentially active and 0–7 = potentially in-active

Table 1 – Mean and S.D. for caries prevalence usingconventional DMFT(S) (D3 threshold) and ICDAS scoring
Mean per patient S.D.
DMFT (D3 cut-off) 18.02 6.94
DFT (D3 cut-off) 12.21 5.40
DMFS (D3 cut-off) 58.78 28.16
DFS (D3 cut-off) 30.88 18.90
No. of lesions recorded at D1 4.33 3.23
ICDAS scores above 1 3.64 3.04
ICDAS scores above 2 1.28 1.61
ICDAS scores above 3 0.67 1.05
ICDAS scores above 4 0.43 0.75
ICDAS scores above 5 0.17 0.17
Score 1 + 2 (pre-cavitated lesion) 1.12 1.11
Score 3 + 4 (moderate lesion) 0.37 0.71
Score 5 + 6 (severe lesion) 0.13 0.29
No. of active lesions 1.55 2.35
j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9296
2. Materials and methods
Fifty-eight patients presenting to the Restorative Assessment
Clinic at King’s College London Dental Institute at Guy’s
Hospital for routine care by undergraduate students were
recruited with ethical approval from the Guy’s and St.
Thomas’ Hospital Ethics Committee (04/Q0704/117). Subjects
were included if they had no removable dental prostheses, a
minimum of 16 teeth and had not eaten for 2 h prior to the
appointment. Subjects were at least 18 years of age but with no
upper age limit. The medical history of the patients was
assessed and those patients requiring antibiotic prophylaxis
and/or receiving medications that can cause hyposalivation
including antidepressants, diuretics, antihistamines, narco-
tics and b-adrenoreceptor agonists were excluded from the
study.21
2.1. Caries detection and diagnosis
The smooth and occlusal surfaces of teeth were cleaned with a
rotating bristle brush, dried and examined using magnifica-
tion (2�). As the subjects were due further treatment by
undergraduates, bite-wing radiographs were taken using film
holders to aid lesion detection on approximal tooth surfaces.
The radiographs were used to detect lesions at the D1 and D3
level. DMFT, DFT, DMFS and DFS scores at the D3 level were
recorded. International Caries Detection and Assessment
System scoring was used to detect caries on all tooth surfaces
in order to record both cavitated and pre-cavitated lesions
(Fig. 1). Expert training was given for the ICDAS9 visual and
Ekstrand activity indices and practised in a clinical pilot study
prior to definitive data collection.
2.2. Caries activity
An activity score for each lesion was calculated from the visual
appearance, in association with a plaque stagnation area,
lesion surface integrity (using a ball-ended CPITN probe) and
associated gingival bleeding for lesions located at the gingival
third of the crown. A final, weighted activity score was then
calculated, as per Fig. 2, where lesions scoring>7 were classed
as potentially active. All caries detection and scoring was
performed independently by two examiners with final agree-
ment decided at the time of examination.
2.3. Saliva analysis
Samples were taken between 9 a.m. and 12 noon. Using the GC
Saliva Check Kit (GC Corp., Belgium) the unstimulated flow
rate was measured visually, noting the time taken for a
salivary droplet to form on the lower lip. A time greater than
60 s was considered as an abnormally low (according to the
manufacturer’s instructions). Subjects were then asked to
pool their saliva in the floor of the mouth and then expectorate
over 30 s. A pH strip was dipped in the saliva and the colour
used to estimate the pH. To stimulate saliva subjects were
given paraffin wax to chew and saliva was collected for 5 min
in a measuring cup and the volume was calculated. From the
collected saliva a drop was placed on a buffering strip, left for
5 min and then measured on the pH scale provided.
2.4. Reproducibility
Intra-examiner reproducibility was confirmed by randomly re-
examining seven patients (12% of the total) and re-recording
the visual indices for caries detection, activity and saliva
properties. Re-examination was carried out on the same day at
different times.
2.5. Statistical analysis
The highest score was recorded for teeth with multiple lesions
on multiple surfaces. The scores were classified by recording
the total number of lesions per patient and dividing this by the
number of teeth per patient to give a proportionate score. The
scores were grouped into mild or pre-cavitated enamel lesions
(ICDAS 1 and 2), moderate open or closed dentine lesions
(ICDAS 3 and 4), and severe cavitated lesions with possible
pulpal involvement (ICDAS 5 and 6). Statistical analysis was
carried out using Stata 8 statistical software (Stata Co., TX,
USA). The sample size permitted the use of the arithmetic
mean as an average and standard deviation as an indication of
spread. Correlations between salivary properties and caries
prevalence and activity were analysed with Spearman’s rank
correlations. Statistical significance was set at p < 0.05, r-
values were calculated to show positive or negative correla-
tions. Reproducibility was determined by using the Kappa
statistic.
3. Results
All 58 subjects with a mean age of 52.7 years (standard
deviation (S.D.) 15.6; age range 22–79 years) comprising 26
males (44.8%) and 32 females (55.2%) successfully completed
the study. The average number of teeth per patient was
26.1(3.2). Of these 13(22.4%) reported smoking.
3.1. Caries detection
Table 1 summarises the mean (S.D.) for caries prevalence in
the sample population using DMFT(S) and ICDAS. The mean
j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9 297
DMFT score per patient was 18.02 (S.D. 6.94) and the mean
DMFS score was 58.78 (S.D. 5.40) using a D3 threshold. The
mean total number of lesions detected using the ICDAS
scoring at D1 threshold was 4.33 (S.D. 3.23). The mean number
of pre-cavitated lesions was 1.12 (S.D. 1.11). The mean for
moderate lesions was 0.37 (S.D. 0.71) and the mean for severe
lesions was 0.13 (S.D. 0.29). The mean number of active lesions
diagnosed was 1.55 (S.D. 2.35).
3.2. Saliva examination
The saliva hydration scores had a mean of 32.5 s per patient
(S.D. 19.5). The mean pH was calculated as 6.8 (S.D. 0.4).
Stimulated volume was recorded over 5 min and a mean was
5.9 ml (S.D. 2.8), calculated as millilitre/minute the mean was
1.18 ml/min. The mean buffer score was 9.7 (S.D. 2.5).
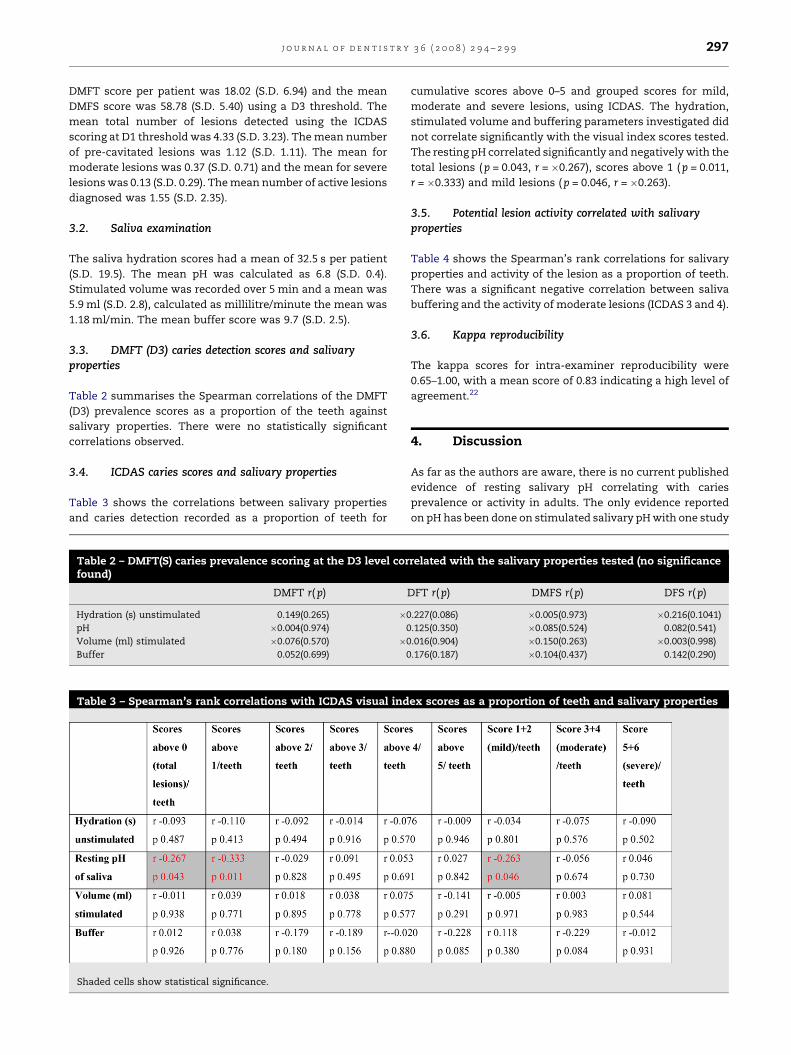
3.3. DMFT (D3) caries detection scores and salivaryproperties
Table 2 summarises the Spearman correlations of the DMFT
(D3) prevalence scores as a proportion of the teeth against
salivary properties. There were no statistically significant
correlations observed.
3.4. ICDAS caries scores and salivary properties
Table 3 shows the correlations between salivary properties
and caries detection recorded as a proportion of teeth for
Table 2 – DMFT(S) caries prevalence scoring at the D3 level corfound)
DMFT r( p)
Hydration (s) unstimulated 0.149(0.265) �0
pH �0.004(0.974) 0
Volume (ml) stimulated �0.076(0.570) �0
Buffer 0.052(0.699) 0
Table 3 – Spearman’s rank correlations with ICDAS visual ind
Shaded cells show statistical significance.
cumulative scores above 0–5 and grouped scores for mild,
moderate and severe lesions, using ICDAS. The hydration,
stimulated volume and buffering parameters investigated did
not correlate significantly with the visual index scores tested.
The resting pH correlated significantly and negatively with the
total lesions (p = 0.043, r = �0.267), scores above 1 ( p = 0.011,
r = �0.333) and mild lesions (p = 0.046, r = �0.263).
3.5. Potential lesion activity correlated with salivaryproperties
Table 4 shows the Spearman’s rank correlations for salivary
properties and activity of the lesion as a proportion of teeth.
There was a significant negative correlation between saliva
buffering and the activity of moderate lesions (ICDAS 3 and 4).
3.6. Kappa reproducibility
The kappa scores for intra-examiner reproducibility were
0.65–1.00, with a mean score of 0.83 indicating a high level of
agreement.22
4. Discussion
As far as the authors are aware, there is no current published
evidence of resting salivary pH correlating with caries
prevalence or activity in adults. The only evidence reported
on pH has been done on stimulated salivary pH with one study
related with the salivary properties tested (no significance
DFT r(p) DMFS r(p) DFS r(p)
.227(0.086) �0.005(0.973) �0.216(0.1041)
.125(0.350) �0.085(0.524) 0.082(0.541)
.016(0.904) �0.150(0.263) �0.003(0.998)
.176(0.187) �0.104(0.437) 0.142(0.290)
ex scores as a proportion of teeth and salivary properties

Table 4 – Spearman’s rank correlations with active lesions’ ICDAS scores as a proportion of teeth and the salivaryproperties
Shaded cell shows statistical significance.
j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9298
showing a negative correlation between stimulated salivary
pH and caries prevalence23 and another showing a positive
correlation, caries prevalence both detected at the D3 thresh-
old.24 In the latter study those patients with a low resting pH
had a larger number of pre-cavitated lesions and may reflect
that this population was more likely to develop early lesions.
Pre-cavitated lesions are in a constant state of dissolution and
repair depending on a critical pH and pH fluctuations can
cause a loss of mineral from the tooth when the pH drops and a
gain in mineral when the pH rises.25
Plaque pH and caries activity have been previously
investigated26 and there is evidence to suggest a fall in plaque
pH below a critical point will cause caries on certain prone
individuals.27 Whether the plaque pH was a factor in
influencing the resting salivary pH is not known and requires
further investigation. Moderate or severe lesions had no
significant correlation with caries prevalence. For moderate
and severe lesions other aetiological factors may override any
saliva effects, as caries is a multifactorial disease.28
Previous methods to measure unstimulated saliva were
described by Navazesh and Christensen29 but they did not
include using the lower labile minor salivary gland hydration
time. The estimation of buffering capacity has been investi-
gated using similar methods using the Dentobuff (Orion
Diagnostics, Helsinki).30 Widodo et al. reported the results of a
study on a group of patients with dental erosion using the GC
Saliva Check Kit (GC Corp., Belgium).31 Although, the methods
used to record the saliva properties are unique to this product
the data recorded in this study appear to correlate with
previously published literature.15,31–35
Results from this study showed no correlations with
hydration, stimulated volume and stimulated buffering with
the caries scores using the modified visual indices and
supports the findings from studies.19,36,37 There has been only
one study in the literature and that was on a child population
which found a low unstimulated flow rate associated with an
increase in DFS.34 This is contrary to the correlations found
between hydration and caries detection in this study and may
reflect the age difference between the sample populations.
The resting pH was found to be negatively and significantly
correlated to the total lesions recorded at the D1 threshold,
scores above 1 and the pre-cavitated scores using the ICDAS
visual index (Table 3). However, there were no correlations
with pH and caries scores recorded with DMFT/DMFS indices
detecting caries at the D3 level (Table 2). This finding was
possibly due to the lack of sensitivity of the DMFT/DMFS
indices used conventionally at the D3 thresholding.1,38
Potential activity of the ICDAS 3 and 4 lesions did show a
negative correlation with saliva buffering capacity. Wiktorsson
et al. reported that lesion activity was correlated to saliva but
used an operator-based, subjective opinion to determine the
activity of the lesion.17 The results presented require further
development to validate the scoring system and to investigate
these potentially clinically useful associations, especiallyuseful
when performing clinical caries risk assessments. The follow-
ing conclusions from this study were deduced:
1. S
alivary parameters (hydration, resting pH, stimulated flowand stimulated buffering) as tested by the Saliva Check kit
(GC Corp.) showed no correlations with caries prevalence
scored using DMFS/DMFT at the D3 threshold.
2. T
here was a negative correlation with resting pH and totalcarious lesions detected at the pre-cavitated threshold. Pre-
cavitated lesions alone correlated negatively with resting pH.
3. T
he potential activity of moderate (ICDAS 3 and 4) lesionsdid negatively correlate with salivary buffering.
The null hypothesis was therefore rejected. The clinical
implications of the findings of this study indicate that the
resting saliva pH may be a predictor in patients developing
pre-cavitated lesions. In terms of lesion activity, the buffering
capacity might help to predict the potential activity of dentine
lesions present but further experimentation and validation is
required.

j o u r n a l o f d e n t i s t r y 3 6 ( 2 0 0 8 ) 2 9 4 – 2 9 9 299
Acknowledgement
The authors would like to acknowledge the assistance
provided by Dr. Ron Wilson with the statistical analysis
completed in this study.
r e f e r e n c e s
1. Pitts NB. Modern concepts of caries measurement. Journal ofDental Research 2004;83:C43–7.
2. Pitts NB. Clinical diagnosis of dental caries: a Europeanperspective. Journal of Dental Education 2001;65:972–8.
3. World Health Organisation. A guide to oral healthepidemiological investigations. Geneva: Oral Health Unit;1997.
4. Broadbent JM, Thompson WM. For debate: problems withthe DMF index pertinent to dental caries data analysis.Community Dental and Oral Epidemiology 2005;33:400–9.
5. Ekstrand KR, Ricketts DNJ, Kidd EAM. Reproducibility andaccuracy of three methods for assessment ofdemineralisation depth on the occlusal surface: an in vitroexamination. Caries Research 1997;31:224–31.
6. Ekstrand KR, Ricketts DNJ, Kidd EAM, Qvist V, Schou S.Detection, diagnosing, monitoring and logical treatment ofocclusal caries in relation to lesion activity and severity: anin vivo examination with histological validation. CariesResearch 1998;32:247–54.
7. Ekstrand KR, Bruun G, Bruun M.. Plaque and gingival statusas indicators for caries progression on approximal surfaces.Caries Research 1998;32:41–5.
8. Nyvad B, Machiulskiene V, Baelum V. Reliability of a newcaries diagnostic system differentiating between active andinactive caries lesions. Caries Research 1999;33:252–60.
9. International Caries Detection and Assessment SystemCoordinating Committee. International Caries Detectionand Assessment System (ICDAS II) Workshop held inBaltimore, MD, March 12–14, 2005. Available http://www.dundee.ac.uk/dhsru/docs/ICDAS%20II%20criteria%20document%20September%2010.doc [accessed 25/1/06].
10. Burt BA, Kolker JL, Sandretto AM, Yuan Y, Sohn W, Ismail AI.Dietary patterns related to caries in a low-income adultpopulation. Caries Research 2006;40:473–80.
11. Sohn W, Ismail A, Amaya A, Lepkowski J. Determinants ofdental care visits among low-income African-Americanchildren. Journal of the American Dental Association2007;138:309–18.
12. Ekstrand KR, Ricketts DNJ, Kidd EAM. Occlusal caries:pathology, diagnosis and logical management. Dental Update2001;28:380–7.
13. Ricketts DNJ, Ekstrand KR, Kidd EAM, Larsen T. Relatingvisual and radiographic ranked scoring systems for occlusalcaries detection to histological and microbiologicalevidence. Operative Dentistry 2002;27:231–7.
14. Kidd EAM, Banerjee A, Ferrier S, Longbottom C, Nugent Z.Relationships between a clinical-visual scoring system andtwo histological techniques: a laboratory study on occlusaland approximal carious lesions. Caries Research 2003;37:125–9.
15. Ekstrand KR, Ricketts DNJ, Longbottom C, Pitts NB.Visual and tactile assessment of arrested initial enamelcarious lesions: an in vivo pilot study. Caries Research2005;39:173–7.
16. Rask PI, Emilson CG, Krasse B, Sundgerg H. Dental cariesand salivary and microbial conditions in 50–60-year-oldpersons. Community Dental Oral Epidemiology 1991;19:93–7.
17. Wiktorsson A-M, Martinsson T, Zimmerman M. Salivarylevels of lactobacilli, buffer capacity and salivary flow raterelated to caries activity among adults in communities withoptimal and low water fluoride concentrations. SwedishDental Journal 1992;16:231–7.
18. Mazengo MC, Soderling E, Alakuijala P, Tiekso J, Tenovuo J,Simell O, Hausen H. Flow rate and composition of wholesaliva in rural and urban Tanzania with special reference todiet, age, and gender. Caries Research 1994;28:468–76.
19. Mazengo MC, Tenovuo J, Hausen H. Dental caries in relationto diet, saliva and cariogenic microorganisms in Tanzaniansof selected age groups. Community Dental Oral Epidemiology1996;24:169–74.
20. Powell LV, Leroux BG, Persson RE, Kiyak HA. Factorsassociated with caries incidence in an elderly population.Community Dental Oral Epidemiology 1998;26:170–6.
21. Tenovuo J.. Human saliva clinical chemistry and microbiology,vol. 1. Florida: CRC Press; 1989. p 26–73.
22. Landis JR, Koch GG. The measurement of observeragreement for categorical data. Biometrics 1977;33:159–74.
23. Johansson I, Saellstrom AK, Rajan BP, Parameswaran A.Salivary flow and dental caries in Indian children sufferingfrom chronic malnutrition. Caries Research 1992;26:38–43.
24. Crossner C-G, Holm A-K. Saliva tests in the prognosis ofcaries in children. Acta Odontologica Scandinavia 1976;35:135–9.
25. Manji F, Fejerskov O, Nagelkerke NJD, Baelum V. A randomeffects model for some epidemiological features of dentalcaries. Community Dental Oral Epidemiology 1991;19:324–8.
26. Fejerskov O, Scheie AA, Manji F. The effect of sucrose onplaque pH in the primary and permanent dentition ofcaries-inactive and -active Kenyan children. Journal of DentalResearch 1992;71:25–31.
27. Stephan RM. Intra-oral hydrogen-ion concentrationsassociated with dental caries activity. Journal of DentalResearch 1944;23:256–7.
28. Fejerskov O, Kidd E. Dental caries. The disease and its clinicalmanagement. Oxford/Blackwell Munksgaard; 2003.
29. Navazesh M, Christensen CM. A comparison of wholemouth resting and stimulated salivary measurementprocedures. Journal of Dental Research 1982;61:1158–62.
30. Ericson D, Bratthall D. Simplified method to estimatesalivary buffer capacity. Scandinavian Journal of DentalResearch 1989;97:405–7.
31. Widodo G, Wilson R, Bartlett D. Oral clearance of an acidicdrink in patients with erosive tooth wear compared withthat in control subjects. International Journal of Prosthodontics2005;18:323–7.
32. Ericsson Y, Hardwick L. Individual diagnosis, prognosis andcounselling for caries prevention. Caries Research 1978;12:94–103.
33. Edgar WM. Saliva: its secretion, composition and functions.British Dental Journal 1992;172:305–12.
34. Vehkalahti M, Nikula-Sarakorpi E, Paunio I. Evaluation ofsalivary tests and dental status in the prediction of cariesincrement in caries-susceptible teenagers. Caries Research1996;30:22–8.
35. Dawes C. Factors influencing salivary flow rate andcomposition. In: Edgar M, Dawes C, O’Mullane D, editors.Saliva and oral health. 3rd ed. London: BDJ Books; 2004. p. 32–49.
36. Lundgren M, Emilson CG, Osterberg T. Root caries and somerelated factors in 88-year-old carriers and non-carriers ofStreptococcus sobrinus in saliva. Caries Research 1998;32:93–9.
37. Gabris K, Nagy G, Madlena M, Denes Z, Marton S, KeszthelyiG, Banoczy J. Associations between microbiological andsalivary caries activity tests and caries experience inHungarian adolescents. Caries Research 1999;33:191–5.
38. Nyvad B. Diagnosis versus detection of caries. CariesResearch 2004;38:192–8.