An Evaluation of Three Demonstration Child Abuse and Neglect Treatment Programs
9
An Evaluation of Three Demonstration Child Abuse and Neglect Treatment Programs Anne Harris Cohn, Dr.P.H. Abstract. This paper reviews findings about treating the abused or neglected child from the first national evaluation of child abuse and neglect programs. Very few children were treated by these programs. Seventy children who did receive therapeutic intervention exhi- bited a variety of psychosocial, emotional, and developmental problems, not unlike those possessed by abusive parents, at the time they entered treatment. Many of these prob- lems were resolved by the end of treatment. Success with 1,724 parents served by the projects, however, was not the rule. Better ways of working with these families in crisis are required. With the increasing knowledge base about the etiology of child abuse and neglect in the past decade has come a number of ef- forts to determine the mose effective means of assisting the mem- bers of families in which abuse or neglect has occurred. This paper presents select findings from one such effort, a multiyear evaluation of a national demonstration treatment program in child abuse and neglect. In May 1974 II 3-year demonstration child abuse and neglect service projects were established in order to develop and test al- ternative strategies for treating abusive and neglectful parents and their children. The projects, spread throughout the country and in Puerto Rico, differed in size, the types of agencies in which they were housed, the kinds of staff they employed, and the vari- ety of services they offered. Concomitantly, a 3-year evaluation Dr. Cohn, until recently a lecturer at the University of California (Berkeley) School of Public Health and an Associate at Berkeley Planning Associates, is currently a Congressional Science Fellow in Child Policy sponsored by the American Associationfor the Advancement of Science. This work was conducted under contracts HRA 106-74-120 and HRA 230-76"'()075 with Mary Kay Miller at Berkeley Planning Associates. Reprints may be requestedfrom Dr. Cohn at 1406-A Hawthorne Terrace, Berkeley, CA 94708. 0002-7138/79/1802--0283 $00.8& e American Academy of Child Psychiatry. 283
-
Upload
anne-harris -
Category
Documents
-
view
212 -
download
0
Transcript of An Evaluation of Three Demonstration Child Abuse and Neglect Treatment Programs
An Evaluation of Three DemonstrationChild Abuse and Neglect TreatmentPrograms
Anne Harris Cohn, Dr.P.H.
Abstract. This paper reviews findings about treating the abused or neglected child from thefirst national evaluation of child abuse and neglect programs. Very few children weretreated by these programs. Seventy children who did receive therapeutic intervention exhibited a variety of psychosocial, emotional, and developmental problems, not unlike thosepossessed by abusive parents, at the time they entered treatment. Many of these problems were resolved by the end of treatment. Success with 1,724 parents served by theprojects, however, was not the rule. Better ways of working with these families in crisis arerequired.
With the increasing knowledge base about the etiology of childabuse and neglect in the past decade has come a number of efforts to determine the mose effective means of assisting the members of families in which abuse or neglect has occurred. Thispaper presents select findings from one such effort, a multiyearevaluation of a national demonstration treatment program inchild abuse and neglect.
In May 1974 II 3-year demonstration child abuse and neglectservice projects were established in order to develop and test alternative strategies for treating abusive and neglectful parents andtheir children. The projects, spread throughout the country andin Puerto Rico, differed in size, the types of agencies in whichthey were housed, the kinds of staff they employed, and the variety of services they offered. Concomitantly, a 3-year evaluation
Dr. Cohn, until recently a lecturer at the University of California (Berkeley) School of Public Healthand an Associate at Berkeley Planning Associates, is currently a Congressional Science Fellow in ChildPolicy sponsored by the American Association for the Advancement of Science.
This work was conducted under contracts HRA 106-74-120 and HRA 230-76"'()075 with Mary KayMiller at Berkeley Planning Associates.
Reprints may be requestedfrom Dr. Cohn at 1406-A Hawthorne Terrace, Berkeley, CA 94708.0002-7138/79/1802--0283 $00.8& e American Academy of Child Psychiatry.
283
284 Anne Harris Cohn
research effort was begun . The overall purpose of this evaluationwas to document the experiences of the demonstration projects.
While the impetus for concern in the child abuse area has certainly been for the victim-the child-almost all resources devotedto the problem have been directed to the parent, on behalf of thechild . With the exceptions of medical care for the injured childand foster home placement (which many argue is not a "service tothe child"), public and private agencies working with abuse orneglect rarely provide direct treatment to the child. Indeed, of the11 demonstration projects studied, only 3 developed and operatedtreatment programs for the abused or neglected child. And ofthese 3, very small numbers of children (8 to 15) were served atanyone time (Miller, 1977).
Why has this been so? Certainly, many professionals have maintained a belief that since the parent is the perpetrator of the abusive or neglectful episode, if the parent can be helped, the behavior, and thus the problem will cease. Or, it is believed that byhelping the parent one is helping the family and thus the child.The assumption here is that the child suffers only from poor family functioning, and if that can be rectified, the child will be infine shape. Apart from theories and assumptions about treatmentand effect, working with the parent is often easier. Parents aremore accessible, generally more verbal, and certainly more mobile.Working with parents is also less expensive and less timeconsuming (e.g., the annual cost of a basic treatment package fora parent is about $1,800 as contrasted with $3,500 a year or morefor one common mode of treatment, therapeutic day care for achild). In addition, the anger, and subsequently the compassion,directed toward the needy par'ent who has maltreated the childhas resulted in a surge of concern for the parent, leaving littletime to ask if the child too needs help.
Studies of the abused child himself suggest that these childrensustain a number of developmental and physical problems as aresult of the abuse or neglect (Elmer and Gregg, 1967; Green,1978b, Martin, 1976). Some researchers suggest that certain problems or behaviors of the child may help cause or contribute to theabusive or neglectful episodes. They theorize that the problems ofthe abused or neglected child may lead to later social deviancy,including abusive or neglectful behavior in adulthood. This is anunfortunate burden for the child to bear; it is also costly to society.
In the evaluation of the demonstration programs, it was of in-
An Evaluation of Child Abuse Treatment Programs 285
terest to look more closely at the abused and neglected child inorder: (1) to document the characteristics and types of developmental, emotional, and psychosocial problems which these childrenhave; and (2) .to ascertain the effects of therapeutic interventions inameliorating these problems. Such information is valuable in determining the essential elements of a comprehensive and effectivechild abuse and neglect program. The policy concern was whethertreatment should be extended to the child rather than be limited tothe parent.
SETTINGS
Seventy abused or neglected children recelvmg direct treatmentservices at 3 demonstration projects were followed from intakethrough termination. The projects included: the Family Center inAdams County, Colorado; the Family Care Center in Los Angeles,California; and the Family Resource Center in St. Louis, Missouri.Problem-oriented records were maintained by clinicians on thechildren served by these projects.
Each of the projects provided a variety of services to the children: play therapy, individual and group therapy, residential care,therapeutic day care, crisis nursery services, and medical care. Services were generally provided by professionally trained socialworkers and clinical psychologists on the projects' staffs, and backup support was available from psychiatrists and physicians consulting with the projects.
The majority of the children served were Caucasian (67%). Although the children ranged in age from birth to 12 years, 44%were 3 to 5 years old, while almost three-quarters were between theages of 2 and 7. Most of the children were victims of emotionalabuse or neglect, although 16% had sustained a severe injury.
METHOD
The data set for the evaluation included basic demographic andcase history information, information on the amount and types ofservices received, and descriptions of the range and severity ofproblems children possessed and the degree to which these problems appeared to be resolved during treatment. The data set alsocontained scores on selected standardized tests, including the Denver Developmental Screening Test, the McCarthy Scales of Chil-

286 AmU' Harris Cohn
dren's Abilities, and the Bayley Scales of Infant Development. Datawere available on the families of 44 of the 70 children. Thesefamilies were similar on key demographic characteristics to otherabusive or neglectful families served by the demonstration projects.It is not known if the children served were similar to children notserved.
Another focus of the evaluation of the national child abuse andneglect program was that of determining the effectiveness of theprojects in working with abusive and neglectful parents. Was abusive or neglectful behavior arrested during treatment? Were parents less likely to maltreat their children by the end of treatment?An additional concern was that of determining the relative effectiveness of different treatment strategies for the parent. In order tostudy treatment effects, all adults receiving treatment services fromall the demonstration projects were studied. Data on 1,724 clients,recorded by case managers, included case history informationabout the nature and severity of the maltreatment, the servicesreceived by the parent, and outcome information.
A number of constraints imposed on the study limit the conclusivcncss of thc findings to be reported. Although the study population is similar to the kinds of cases routinely handled by publicprotective service departments, the projects studied, selected because of the different treatment strategies they proposed to demonstrate, are not necessarily representative of child abuse andneglect treatment programs in general. The study included no control or nontreatment groups. All data were collected from casemanagers rather then directly from the clients themselves. And nofollow-up data were collected.
FINDINGS
Children's Problems
At the time they entered treatment, the children as a group exhibited a variety of psychosocial, emotional, and developmental problems. There was no single area of functioning in which they wereall deficient, nor did any specific behaviors stand out as universallyproblematic. Thus, while all children exhibited some dysfunctionalbehavior, there was, for this study group, no composite picture ofthe maltreated child; rather, a number of different behaviors andproblems emerged for different children .
An Evaluation ofChild Abuse Treatment Programs 287
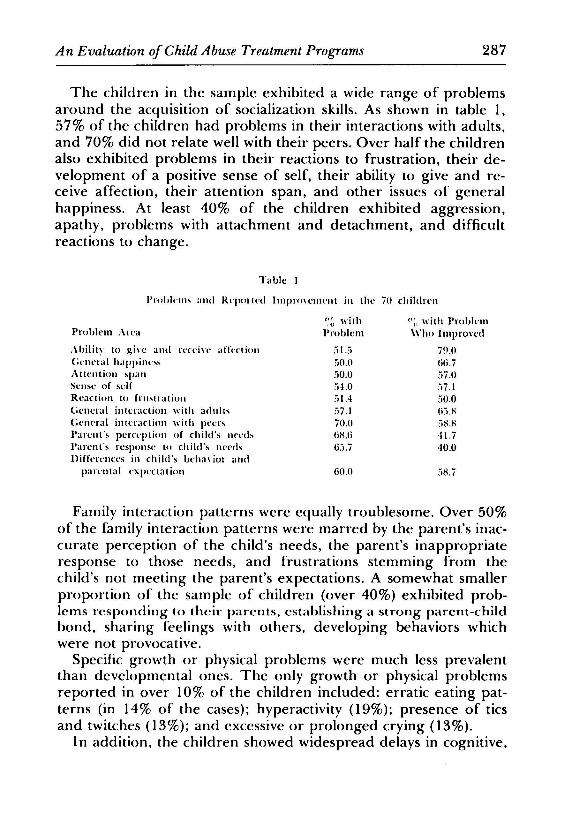
The children in the sample exhibited a wide range of problemsaround the acquisition of socialization skills. As shown in table 1,57% of the children had problems in their interactions with adults,and 70% did not relate well with their peers. Over half the childrenalso exhibited problems in their reactions to frustration, their development of a positive sense of self, their ability to give and receive affection, their attention span, and other issues of generalhappiness. At least 40% of the children exhibited aggression,apathy, problems with attachment and detachment, and difficultreactions to change.
Table I
l'rohh-ms and Reported Improvcuu-ni in the 70 childrcu
Problem .\rca
Ahilitv to g ivc and receive afkctionC;encral happinl"sAttention spanSense of selfReaction to frustrationGcncral interaction with adultsGeneral interaction with peersParent's perception of child's needsParent's rcsponse to child's needsDifferences in child's bcha vior and
parental expcctarion
(",~ withProblem
"J.:j,,0,050.0",1.0,i1.4,,7.170.0mUj(j,i,7
GO,O
p;, with Proble-m\\'ho Improved
7!I.O(j(j,7
,,7.0:"'7.1,,0.0li,i,H:"')~.~
H.740.0
Family interaction patterns were equally troublesome. Over 50%of the family interaction patterns were marred by the parent's inaccurate perception of the child's needs, the parent's inappropriateresponse to those needs, and frustrations stemming from thechild's not meeting the parent's expectations. A somewhat smallerproportion of the sample of children (over 40%) exhibited problems responding to their parents, establishing a strong parent-childbond, sharing feelings with others, developing behaviors whichwere not provocative.
Specific growth or physical problems were much less prevalentthan developmental ones. The only growth or physical problemsreported in over 10% of the children included: erratic eating patterns (in 14% of the cases); hyperactivity (19%); presence of ticsand twitches (13%); and excessive or prolonged crying (13%).
In addition, the children showed widespread delays in cognitive,
288 Anne Harris Cohn
language, and motor skills, but not always severe delays accordingto the results of several standardized tests. For example, on thestandardized tests with IQ scores, the children generally scored ator one standard deviation below the mean, indicating generallypoor functioning but not serious delays. When subtest scores werecalculable, they were all relatively depressed; no one area reflectedsignificantly more deficiency than others, although verbal and language delays, often thought to be particular problems for thesechildren, showed the lowest mean scores.
These findings point to the existence of varied, but pervasive,problems for these sample children who were abused and neglected. The problems were not only in the more developmentallybased areas of cognitive, language, and motor-skill abilities, but alsoin the more behaviorally related areas of interaction patterns andsocialization skills. The problems parallel many of the same behaviors one sees in the abusive and neglectful parent, lending eredeuce to the argument that maltreated children stand a goodchance of growing up to be abusive and neglectful parents themselves.
While it is not known how comparable the study sample is toabused and neglected children generally, the fmdings do suggestthat at least some maltreated children suffer from problems requiring remediation. They further suggest a need for all child abuseand neglect treatment programs to devote some portion of theirresources to the direct treatment of the child, both to help remedyconditions that aggravate poor parent-child interactions and as along-run prevention strategy.
Remediation of Children's Problems During Treatment. Analysis ofclinician-reported gains made by the sample children in problemareas during treatment indicates uneven progress, with childrenexhibiting very different patterns of improvement; some childrenimproved a great deal on most of their problems, while othersseemed to make little or no progress. Some made consistent gains(or losses) across a variety of problem areas, while others mademajor improvements in some areas but regressed or stayed thesame in others.
If one looks first at those areas in which over half of the childrenin the study population were reported to have a problem, projectsappear to have had their greatest success in helping children giveand receive affection. Of those reported with a problem in thisarea, 70% were said to have improved. Closer to two-third of the

An Evaluation of Child Abuse Treatment Programs 289
children with problems interacting with adults (66%) or generalhappiness (67%) were reponed to have improved. Well over half ofthe children with short attention spans (57%) and poor self-images(57%) exhibited progress, as did those who had general interactionproblems with peers (59%) or parents with inappropriate expectations (59%). Changing parental responses to children's needs aswell as their perception of children's needs occurred in closer to40% of the families.
Beyond these problems common to 50% or more of the childrenstudied, notable improvements were seen in a number of otherareas, although the number of children exhibiting the problemtended to be small. For example, with respect to socialization problems, there was improvement in over half of the children exhibiting problems in the following areas: aggression, apathy, hypermonitoring, ability to protect self, attachment and detachment, andreactions to change. With respect to problems in interacting withfamily members, over half of the children said to have weakparent-child bonds (e.g., fearfulness toward parents, or inability toshare feelings) were judged improved. For most physical problemsidentified, more than half the children progressed. Also, at thetime of terrnination , most children had significantly higher cognitive, language, and motor-skill scores on the standardized tests administered, although they were still at the low end of the "normal"range. For over half of the children, one or two of their problemsremain unchanged, and a small proportion were reported to haveregressed in certain areas (generally less than 15%).
The study sample was too small to permit an in-depth analysis offactors which may account for the variations in improvements, although improvements are not unlike those found by other researchers (Green, 1978a). The child's family situation, the history ofabusive and neglectful behavior, as well as the type and frequencyof treatment received may help to account for the variations. Despite the uneven progress and the lack of clear explanations forthis, the sheer number and variety of problems which these children exhibited indicate the tremendous need for specific therapeutic services for children. The progress of children in the demonstration projects does indicate that therapeutic intervention canbe beneficial. It clearly would be premature to specify the types oftreatment which would most benefit these children. Instead, thisstudy demonstrates an acknowledged need for an increase in thenumber and variety of attempts to work with the abused and ne-

290 Anne Harris Cohn
glected child. A top priority of future research and demonstrationtreatment agendas should be determining how best to help thechild.
Parents
One indication of treatment effectiveness is a clinician's judgmentof whether or not a client's potential for abusive or neglectful behavior has been reduced by virtue of improvement in a number ofproblem areas. Case managers at the demonstration projects wereasked to report, for each client served, whether or not a client'spropensity for future maltreatment had been reduced by the endof treatment. Of the parents studied, 42% were judged to have areduced potential for abuse or neglect. In other words, workersreported success with less than half of their cases. Given the paucityof comparable studies, it is not known if the experiences of thedemonstration projects represent a norm for the field. However,because these projects received special resources and special attention not common in public protective service programs across thecountry, it may be fair to assume that the projects studied did atleast as well in working with clients as most other programs acrossthe country. If this is the case, it suggests that child abuse andneglect programs are not nearly as successful in long-term protection of children as we might wish.
Client characteristics did not seem to differentiate between successful and unsuccessful clients. Moreover, no one service or service package was found to be overwhelmingly related to reducedpropensity. The experiences of the demonstration projects did notpoint to a single best method of service delivery. However, clientsreceiving lay services (lay or parent aide counseling and/or ParentsAnonymous) as supplements to their service package were morefrequently reported to have reduced propensity for abuse thanclients not receiving these services. Of those provided with lay services, 53% were said to have improved during treatment, as opposed to less than 40% of the other clients.
The implications of these findings are that the children of theparents served by the demonstration projects were not necessarilyprotected from continued or future maltreatment. While supplementing a treatment package with lay services may be beneficial, wehave yet to identify replicable treatment modes that are effectivewith large numbers of clients, and thereby indirectly beneficial tothe child.

An Evaluation ofChild Abuse Treatment Programs
CONCLUSIONS
291
Children rarely received treatment services, although the childrenserved did exhibit improvement on a variety of problems demanding attention. Worker-judged success with parents by the end ofthe treatment was not the rule. While research or evaluation studiesmay shed light on solutions as they emerge, it would appear that itis time for professionals in the field to make a vigorous effort todiscover better ways of working with these families in crisis.
REFERENCES
COHN. A. H. (1975). Assessing the Impact of Health Programs Responding to Health Problems.Doctoral dissertation, University of California (Berkeley) School of Public Health.
-- (1977), Adult Client Final Report. Berkeley: Berkeley Planning Associates.ELMER, E. & GREGG, G. S. (1967), Developmental characteristics of abused children. Pediat-
rics, 40:596-602.GREEN, A. H. (1978a), Psychiatric treatment of abused children. This Journal, 17:356-371.-- (I 978b), Psychopathology of abused children. This Journal, 17:92-103.MARTIN, H. P., ed. (1976), The Abused Child. Cambridge: Ballinger.MILLER, M. K., (1977), Child Client Final Report. Berkeley: Berkeley Planning Associates.