An Evaluation of the Kessner Adequacy of Prenatal Care Index and ...
7
An Evaluation of the Kessner Adequacy of Prenatal Care Index and a Proposed Adequacy of Prenatal Care Utilization Index Milton Kotelchuck PhD, MPH Introduction Accurate assessment of prenatal care utilization is the critical first step in the development of public health programs to improve prenatal care accessibility and ultimately to improve birth outcomes. The assessment of the adequacy of prenatal care utilization is heavily shaped by the way in which utilization is measured. Currently, there are two widely used measures of adequacy of prenatal care utilization: the trimester of prenatal care initiation and the Kessner/Institute of Medicine (IOM) Adequacy of Prenatal Care Index.' Trimester of initiation will not be examined here because it provides no information about prenatal care utiliza- tion after initiation; it has been critically examined elsewhere.2'3 The Kessner In- dex-the principal adequacy of prenatal care utilization index in use in the United States today-includes information about both the timing of prenatal care initiation and prenatal care visits after initiation. It was published in 1973 as part of an IOM-supported study of infant mortality in New York City.' The Kessner Index combines two continuous numeric mea- sures (month prenatal care begins and number of visits, adjusting for length of gestation) and rigidly links them into a very easy to understand index with three levels of adequacy (Adequate, Intermedi- ate, and Inadequate). To be rated Ad- equate on the Kessner Index, one must start prenatal care in the first trimester and have nine prenatal care visits for a normal-length pregnancy. Table 1 presents the Kessner Index algorithm as initially published. In this original description, public or private obstetric service was a third factor, but this factor has been dropped by all subsequent researchers because the type of service is not noted on the standard US birth certificate and because researchers disagree with the index's assumption that care from public services can never be adequate.-7 Although Kessner et al. called their index the "Adequacy of Prenatal Care Index," their measure indicates nothing about the content or clinical adequacy of prenatal care; it is a utilization index only. The Kessner Index has been widely adopted for public health research, plan- ning, and resource allocation. However, it appears that the index was not subjected to close scrutiny prior to its widespread adoption. The accuracy of the Kessner Index is critical because any limitations may distort our perceptions about prena- tal care adequacy in the United States and may incorrectly influence programmatic efforts to improve prenatal care utiliza- tion. The Kessner Index has also been widely used to assess the association between prenatal care and birth out- comes.47 The limited positive associa- tions noted may be more a reflection of the internal characteristics of the Kessner Index than of the true strength of that relationship. The ability to measure prenatal care utilization after initiation remains under- developed. The Kessner Index does not separately isolate utilization after enroll- ment, nor does any other prenatal care index. Yet a distinction between initiation The author is with the Department of Maternal and Child Health, School of Public Health, University of North Carolina at Chapel Hill. Requests for reprints should be sent to Milton Kotelchuck, PhD, MPH, Department of Maternal and Child Health, School of Public Health, University of North Carolina at Chapel Hill, CB# 7400, Chapel Hill, NC 27599-7400. This paper was accepted September 23, 1993. Editors Note. See related editorial by Wise (p 1374) and article by Kotelchuck (p 1486) in this issue. September 1994, Vol. 84, No. 9
Transcript of An Evaluation of the Kessner Adequacy of Prenatal Care Index and ...

An Evaluation of the KessnerAdequacy of Prenatal Care Indexand a Proposed Adequacy of PrenatalCare Utilization Index
Milton Kotelchuck PhD, MPH
IntroductionAccurate assessment of prenatal care
utilization is the critical first step in thedevelopment of public health programs toimprove prenatal care accessibility andultimately to improve birth outcomes. Theassessment of the adequacy of prenatalcare utilization is heavily shaped by theway in which utilization is measured.
Currently, there are two widely usedmeasures of adequacy of prenatal careutilization: the trimester of prenatal careinitiation and the Kessner/Institute ofMedicine (IOM) Adequacy of PrenatalCare Index.' Trimester of initiation willnot be examined here because it providesno information about prenatal care utiliza-tion after initiation; it has been criticallyexamined elsewhere.2'3 The Kessner In-dex-the principal adequacy of prenatalcare utilization index in use in the UnitedStates today-includes information aboutboth the timing of prenatal care initiationand prenatal care visits after initiation. Itwas published in 1973 as part of anIOM-supported study of infant mortalityin New York City.' The Kessner Indexcombines two continuous numeric mea-sures (month prenatal care begins andnumber of visits, adjusting for length ofgestation) and rigidly links them into avery easy to understand index with threelevels of adequacy (Adequate, Intermedi-ate, and Inadequate). To be rated Ad-equate on the Kessner Index, one muststart prenatal care in the first trimesterand have nine prenatal care visits for anormal-length pregnancy.
Table 1 presents the Kessner Indexalgorithm as initially published. In thisoriginal description, public or privateobstetric service was a third factor, butthis factor has been dropped by allsubsequent researchers because the typeof service is not noted on the standard US
birth certificate and because researchersdisagree with the index's assumption thatcare from public services can never beadequate.-7 Although Kessner et al.called their index the "Adequacy ofPrenatal Care Index," their measureindicates nothing about the content orclinical adequacy of prenatal care; it is autilization index only.
The Kessner Index has been widelyadopted for public health research, plan-ning, and resource allocation. However, itappears that the index was not subjectedto close scrutiny prior to its widespreadadoption. The accuracy of the KessnerIndex is critical because any limitationsmay distort our perceptions about prena-tal care adequacy in the United States andmay incorrectly influence programmaticefforts to improve prenatal care utiliza-tion. The Kessner Index has also beenwidely used to assess the associationbetween prenatal care and birth out-comes.47 The limited positive associa-tions noted may be more a reflection ofthe internal characteristics of the KessnerIndex than of the true strength of thatrelationship.
The ability to measure prenatal careutilization after initiation remains under-developed. The Kessner Index does notseparately isolate utilization after enroll-ment, nor does any other prenatal careindex. Yet a distinction between initiation
The author is with the Department of Maternaland Child Health, School of Public Health,University of North Carolina at Chapel Hill.
Requests for reprints should be sent toMilton Kotelchuck, PhD, MPH, Departmentof Maternal and Child Health, School of PublicHealth, University of North Carolina at ChapelHill, CB# 7400, Chapel Hill, NC 27599-7400.
This paper was accepted September 23,1993.
Editors Note. See related editorial byWise (p 1374) and article by Kotelchuck (p1486) in this issue.
September 1994, Vol. 84, No. 9

Prenatal Care Use
and utilization once in care may havedifferential implications for birth out-comes and for prenatal care program
practices.In this paper I examine the character-
istics and limitations of the KessnerAdequacy of Prenatal Care Index andpropose an alternative, the two-factorAdequacy of Prenatal Care UtilizationIndex.
DatbaseThe database for this paper is the
National Center for Health Statistics'1980 National Natality Survey, a represen-
tative sample of US births in 1980.8 Thissurvey uses a follow-back methodologyinvolving the collection of data from foursources: maternal retrospective informa-tion, physician and hospital records, radio-logic records, and birth and death certifi-cates. Data are available on 9941 livebirths, oversampled (4:1) for low-birth-weight infants. Responses were weightedby a poststratification ratio estimate proce-
dure to be representative of the 1980 USbirth cohort. Prenatal care information isabsent for 15% of the births. All missingdata were imputed via a categoricalmatrix hot-deck methodology. Details ofthe survey and study population are
described elsewhere.9All data used in this paper are
derived from the birth certificate datasource only. The birth certificate datawere chosen because they are readilyavailable to the public health community,they are the principal database for theassessment of a community's prenatalcare utilization adequacy, and they are
available for all married and unmarriedwomen in the 1980 National NatalitySurvey.
Kessner IndexAssessmentThe Kessner Index is a seriously
flawed index of adequacy of prenatal care
utilization. Four features merit attention.First, the Kessner Index is principally
a measure of the timing of initiation ofprenatal care. The Kessner Index algo-rithm requires that to be rated Adequate,prenatal care must begin in the firsttrimester; to be rated Intermediate, care
must begin in the second trimester; and tobe rated Inadequate, care must begin inthe third trimester or not at all. Theadditional factor in the Kessner Index, thenumber of prenatal care visits, can onlylower the rating category. This rarelyhappens. Table 2 shows that the trimesterof care overwhelmingly (for 86.2% of
women) predicts the Kessner Index rat-ing. Only 13.8% ofwomen have their rat-ings reduced owing to insufficient visits.
Second, the Kessner Index does notdistinguish inadequacy of care due to lateinitiation from inadequacy of care due toinsufficient number of visits. Table 3shows that these two implicit subscaleshave distinctive distributions. Overall,24.7% of US women would be classifieddifferently if the two were measuredseparately. More striking, 61.1% ofwomenstarting prenatal care in the secondtrimester (rated Intermediate by the Kess-
ner Index) and 45.6% of women startingprenatal care in the last trimester or not atall (rated Inadequate by the KessnerIndex) would be classified differentlybased on an index with two distinctivefactors.
Third, the Kessner Index is unable to
adequately characterize prenatal care uti-lization for normal-gestation and postma-ture births. For all normal-length pregnan-cies (more than 36 weeks' gestation), theKessner Index requires only nine visits forcare to be Adequate. Yet up to 36 weeks'gestation, the Kessner Index adjusts the
American Journal of Public Health 1415
TABLE 1 Three-Factor Health Services Index Controlled for Gestation andBased on Number of Prenatal Visits, Interval to First Prenatal Visit,and Type of Hospital Service
GestationMedical Care Index (Weeks) Number of Prenatal Visits
Adequatea 13 or less and 1 or more or not stated14-17 and 2 or more18-21 and 3 or more22-25 and 4 or more26-29 and 5 or more30-31 and 6 or more32-33 and 7 or more34-35 and 8 or more36 or more and 9 or more
Inadequateb 14-21C and 0 or not stated22-29 and 1 or less or not stated30-31 and 2 or less or not stated32-33 and 3 or less or not stated34 or more and 4 or less or not stated
Intermediate All combinations other than specified above
aln addition to the specific number of visits indicated for adequate care, the interval to the firstprenatal visit had to be 13 weeks or less (first trimester), and the delivery must have taken place ona private obstetrical service.
bin addition to the specific number of visits indicated for inadequate care, all women who startedtheir prenatal care during the third trimester (28 weeks or later) were considered inadequate.
cFor this gestation group, care was considered inadequate if the time of the first visit was not stated.Source. Reprinted with permission from Infant Death: An Analysis by Maternal Risk and Health Care
(Table 2-3, p 59). Copyright 01973, National Academy of Sciences. Courtesy of the NationalAcademy Press, Washington, DC.
TABLE 2-Ratings Assigned to Births According to the Kessner Adequacy ofPrenatal Care Index, by the Trimester of Initiation of Prenatal Care
Trimester ofKessner Index Rating % Of
Initiation of Care Inadequate, % Intermediate, % Adequate, % Total Births
1 1.4 10.6 65.9 77.92 1.8 15.7 ... 17.53ornocare 4.6 ... ... 4.6
% of total births 7.7 26.3 65.9
Note. Percentages are those of all US births. Concordance of trimester and index rating = 86.2%.Percentages may not add to 100 because of rounding.
Source. Percentages are based on an analysis of birth certificate data from the 1980 NationalNatality Survey.8
September 1994, Vol. 84, No. 9

required number of visits according to thewell-established American College of Ob-stetricians and Gynecologists (ACOG)recommendations (one visit per monththrough 28 weeks' gestation, one visitevery 2 weeks through 36 weeks' gesta-tion, and one visit per week thereafter).10No discussion of the rationale for stop-ping at nine visits is presented.
It would appear that the index stopsat nine visits because only one digit was
allocated to record the number of prena-
tal care visits on the 1968 New York Citycomputerized birth certificate file used inthe Kessner et al. analyses.' According toACOG, nine visits corresponds to therecommended number of visits at 36weeks' gestation; hence the index's adjust-ments for gestational age stop at thatpoint. Thus, the Kessner Index is con-
structed on the basis of an outdatedcomputer data storage limitation. Full-term births can, therefore, be rated as
having Adequate prenatal care even ifthey have had fewer than the ACOG-recommended number ofvisits. The longerthe pregnancy, the smaller the percentageof recommended visits needed for care tobe rated Adequate. Only premature births(36 weeks' gestation and less) are assessedfully against the ACOG standards.
If one extrapolates the original Kess-ner Index algorithm beyond the ninevisits, using the ACOG standards (e.g., 10visits by 37 weeks, 11 visits by 38 weeks,etc.), a major redistribution of prenatalcare utilization adequacy would occur
(Table 4). There would be more thantwice the number of women with Inad-equate care, a major increase and shift toIntermediate care, and many fewerwomenwith Adequate prenatal care. Indeed,44% of all women would now be classifiedas having less adequate prenatal care thanpreviously classified. If one examines theextrapolation stratified by weeks' gesta-tion at delivery, as in Table 5, one sees
that this miscategorization increases as
gestational age advances.Finally, the lack of adequate initial
documentation for the Kessner Index hasled to nonstandardized definitions anddiscrepancies in its calculations. Thealgorithm presented in Table 1 appears tobe the sole documentation for the Kess-ner Index. This is clearly inadequate. Inparticular, there is insufficient descriptionof how to treat records with missinggestational age, missing visits, missinginitiation date, etc." The result is thateach public health entity has had toprogram the index itself, with resultantinconsistencies. For example, many states
1416 American Journal of Public Health
Kotelchuck
TABLE 3-Ratings Assigned to Births According to the Number of VisitsComponent of the Kessner Adequacy of Prenatal Care Index, by theTrimester of Initiation of Prenatal Care
Number of VisitsTrimester of
Initiation Inadequate Intermediate Adequate %ofof Care (< 5), % (5-8),% (. 9), % Total Births
1 1.4 10.6 65.9 77.92 1.8 6.9 8.9 17.53 or no care 2.5 1.3 0.8 4.6
% of total births 5.7 18.8 75.5
Note. Percentages are those of all US births. Concordance of trimester and number of visits =75.3%. Percentages may not add to 100 because of rounding.
Source. Percentages are based on an analysis of birth certificate data from the 1980 NationalNatality Survey.8
TABLE 4-Ratings Assigned to Births According to the Kessner Adequacy ofPrenatal Care Index, Original and Extrapolated beyond Nine PrenatalCare Visits
Rating Original Kessner Extrapolated Kessnera
Adequate,% 65.9 29.2Intermediate, % 26.3 54.5Inadequate, % 7.7 16.3
Note. Percentages are those of all US births; they may not add to 100 because of rounding.Source. Percentages are based on an analysis of birth certificate data from the 1980 National
Natality Survey.8aRatings are based on trimester prenatal care began plus proportion of total visits recommended byAmerican College of Obstetricians and Gynecologists received (all recommended visits receivedfor a rating of Adequate and fewer than half the recommended visits received for a rating ofInadequate).
TABLE 5-Ratings Assigned to Births According to the Kessner Adequacy ofPrenatal Care Index, Original and Extrapolated beyond Nine PrenatalCare Visits, by Week of Gestation at Delivery
Week of Adequate Intermediate InadequateGestation Kessner, Extrapolated, Kessner, Extrapolated, Kessner, Extrapolated,at Delivery % % % % % %
35 57.7 57.7 27.8 27.8 14.5 14.536 53.5 53.5 33.1 29.7 13.4 16.837 55.7 47.2 31.7 36.6 12.6 16.738 61.3 39.8 29.9 44.4 8.8 15.839 69.5 38.9 24.6 49.2 5.9 11.940 67.0 21.8 26.0 61.5 7.0 16.741 73.3 18.5 20.4 68.8 6.4 12.842 69.9 13.1 24.6 65.7 5.5 21.143 66.8 8.9 23.0 70.4 10.1 20.744 66.5 5.5 28.0 68.5 6.6 26.045 58.7 3.5 37.4 66.6 3.9 29.9
% of total 65.9 29.2 26.3 54.5 7.7 16.3births
Note. Percentages are those of all US births; they may not add to 100 because of rounding.Source. Percentages are based on an analysis of birth certificate data from the 1980 National
Natality Survey.8
September 1994, Vol. 84, No. 9

Prenatal Care Use
have added an "unknown" category ifnumber of prenatal care visits or timing offirst visit is unknown, while others stillfollow the original recommendations andrecord such births as having received"inadequate" care. Some states imputemissing gestational age on the basis ofbirthweight, whereas others (e.g., NewYork) disregard all such records or disre-gard only those that cannot be rated as"inadequate" (L. Dellehunt, written com-munication, September 29, 1986). Thestate of Missouri and others have furthersimplified the definition of the Adequaterating of the Kessner Index to eight visitsfor full-term birth and five visits forpremature births (J. W. Stockbauer, writ-ten communication, September 26, 1986).Thus, the Kessner Index ratings may notbe comparable across sites.
Adequacy ofPrenatal CareUtilization Inde
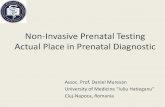
The weaknesses of the Kessner In-dex led the author to try to develop analternative prenatal care utilization algo-rithm, based on birth certificate data. Theproposed Adequacy of Prenatal CareUtilization (APNCU) Index attempts tocharacterize prenatal care utilization ontwo independent and distinctive dimen-sions: Adequacy of Initiation of PrenatalCare and Adequacy of Received Services(once prenatal care has begun). Thistwo-factor index does not assess thequality of the prenatal care that isdelivered, but simply its utilization.
The initial dimension, Adequacy ofInitiation of Prenatal Care, characterizesthe adequacy of the timing of initiation ofcare. The month prenatal care begins,which is recorded on the birth certificate,corresponds directly to the adequacy oftiming of initiation of prenatal care. Theunderlying assumption is that the earlierthe initiation, the more adequate theprenatal care. The month in which care isinitiated is grouped not by trimester, butinto four slightly different adequacy group-ings: months 1 and 2, months 3 and 4,months 5 and 6, and months 7 through 9.The second trimester was felt to cover toobroad a time period to be useful as asingle initiation date category. No prena-tal care, which can be isolated in thisindex, is grouped in the late or inadequatecare category for this dimension.
The second dimension, Adequacy ofReceived Services, characterizes the ad-equacy of the prenatal care visits receivedduring the time the woman is actually inprenatal care (i.e., from initiation until
the delivery). The expected number ofvisits is based on the ACOG prenatal carevisitation standards for uncomplicatedpregnancies,12 adjusted for the gestationalage at initiation of care and for thegestational age at delivery. The measurefor Adequacy of Received Services is theratio of the actual number of visits to theexpected number of visits.
The expected number of visits foreach pregnancy can be calculated easily(by computer or by hand) by noting thenumber of ACOG-recommended prena-tal care visits for a pregnancy of a givengestation and then adjusting or reducingthat number based on the gestational ageat initiation of care (missed visits areassumed not to be made up). Essentially,this procedure measures a segment of afixed recommended prenatal care utiliza-tion metric, but in contrast to the KessnerIndex, it is adjusted at two places: whenthe woman begins prenatal care and whenshe delivers. For example, for a 40-weekpregnancy, ACOG recommends 14 visits;if care began in month 4 (three missedvisits), then the expected number of visitswould be 11. The number of actual orobserved visits can be directly recordedfrom the birth certificate (or any otherprenatal care data source). The ratio ofobserved to expected visits is then groupedinto four categories: Inadequate (lessthan 50% of expected visits), Intermedi-ate (50%-79%), Adequate (80%-109%),and Adequate Plus (.110%). A similarratio concept is implicit in the existingKessner Index, wherein inadequate visitsequal approximately 50% of adequatevisits. These four percentage categoriesallow for a slightly broader range ofnumbers of visits to be rated as Adequatecare (80%-109%) and provide, for thefirst time, a measurement of prenatal careutilization that exceeds ACOG standards.This dimension of Adequacy of ReceivedServices is independent of the previouslydescribed dimension of Adequacy ofInitiation of Prenatal Care.
The two dimensions can be com-bined into a single summary prenatal careutilization index. Inadequate utilization isdefined as either late initiation (after the4th month of pregnancy) or less than 50%of recommended visits. All other catego-ries require initiation of care by the 4thmonth of pregnancy and then are codedaccording to the extent of received ser-vices (e.g., to be rated Adequate Plusrequires initiation of care between 1 and 4months and more than 110% of theexpected ACOG-recommended visits,
etc.). Figure 1 portrays the construction ofthe summaryAPNCU Index.
A descriptive outline of the proposedindex and its two factors is presented inTable 6. (A more detailed description ofthe APNCU Index and its coding assump-tions and an SAS Program for its compu-tation are available from the author.)
Table 7 presents a comparison of theAPNCU and Kessner Index ratings. Only71.5% of women in the United Stateswould be rated the same on the twoindexes (assuming the APNCU's "Ad-equate and Adequate Plus" equal Kess-ner's "Adequate"), with 21.1% achievinga poorer rating and 7.4% an improvedrating. Women whose care was ratedIntermediate on the Kessner Index wouldbe the most likely to be recategorized:34% would now be rated Inadequate and28% rated Adequate or Adequate Plus.
In a related paper in this issue of theJournal I apply the APNCU Index to the1980 National Natality Survey data toassess the adequacy of prenatal care
utilization in the United States and itsassociation with low birthweight.13
DiscussionThe assessment of the adequacy of
prenatal care utilization is heavily shapedby the way in which utilization is mea-
sured. One of the major strategic andprogrammatic thrusts to reduce infantmortality in this era is to increase earlyinitiation of prenatal care. Healthy People
American Journal of Public Health 1417
7-9 Month
E 5.6Month I
1-2Month
Under.W0% 50-79% 80-109% 110% +
Adequacy of lReceived Services
Summary Index
El Adequate Plus
!~ qS ~ S n
1.2 Monthtwndkf
Inadequate
FIGURE I-The summaryAdequacy of PrenatalCare Utilization Index.
September 1994, Vol. 84, No. 9

Kotelchuck
2000's goal 14.11 is to increase first-trimester prenatal care to at least 90% oflive births.'4 By contrast, continuity ofprenatal care once enrolled is much lessemphasized. Professional and public atten-tion has been drawn to the theme of earlyaccess to care, I believe, because we havebeen able to marshal clear evidence aboutprenatal care initiation but we lack any
readily available measures of care afterenrollment. Both current popular mea-
sures of prenatal care adequacy, trimesterof initiation of care (by definition) and theKessner Index (by algorithmic biases), are
basically measures of initial access to care.
Improving birth outcomes, however, maybe dependent on other features of prena-tal care (such as content, timing, andnumber of visits). One utilization measuremay not capture all facets of prenatalcare.
The Kessner Index was a majorachievement in perinatal health serviceresearch, transforming two technicallyavailable but continuous and complexdata items on birth certificates into a
simple three-point utilization scale. Itsoriginal rationale and basic algorithmseemed clear and clinically reasonable.Unfortunately, the Kessner Index appearsto be seriously flawed; it maybe leading usto misperceive the nature of prenatal care
utilization in the United States. Fourlimitations were noted in this paper.
First, the Kessner Index is over-
whehningly a measure of the initiation ofprenatal care. Only 14% of women re-
ceive fewer visits than the number re-
quired for the trimester they enter care.
This initiation bias may explain why thosewho have used both the Kessner Indexand the trimester of prenatal care initia-
tion note so little difference between themin most analyses; the latter measure istherefore preferred because it does not
require the often inaccurately recorded or
missing gestational age variable in itscalculations (J.C. Kleinman, PhD, verbalcommunication, November 6, 1987). Sec-ond, the Kessner Index does not distin-guish between inadequacy due to lateinitiation and inadequacy due to an
inadequate number ofvisits. Although thesummary Kessner Index was not devel-oped to measure these components sepa-
rately, the absence of independent mea-
sures results in the loss of importantinformation about the nature of prenatalcare adequacy, especially since 24% ofwomen would be rated differently on
these two dimensions. Neither of thesefirst two observations about the KessnerIndex, through interesting, would seem towarrant its dismissal.
The limitation of the Kessner Indexto nine visits is, however, critical. Thislimitation is totally arbitrary and notclinically derived; it is the direct result of acomputer data capacity limitation of the1968 New York City birth file. For 20years, the US public health profession hasbased its major index of prenatal care
adequacy on an algorithm developed toaccommodate this single-digit limitationin the counting of the number of prenatalcare visits.
Because of the nine-visit limitation,the Kessner Index incorrectly assesses
prenatal care utilization adequacy fornormal and post-term births, the vastmajority of births in the United States.The extrapolated Kessner Index algo-rithm would indicate that only 29%, not66%, of births receive "adequate" care.
This is not a minor difference in our
perception of the extent of prenatal care
adequacy in the United States. Accurateassessment of prenatal care utilization forterm infants may be particularly impor-tant, given the significant racial disparitiesin birth outcomes for normal-birthweightinfants15 and the recent observations thatthere are significant Black-White differ-ences in the utilization of prenatal care atthe end of pregnancy.'6'17 Moreover, thelimitation to nine visits also biases theassessment of the relationship of prenatalcare and birth outcomes. Full-term ba-bies, which are bigger and more fre-quently healthy, are more readily rated as
having received "adequate" care than are
preterm babies, thus artificially enhancingthe association of positive birth outcomeswith more positive prenatal care adequacyratings.18 This bias suggests that the
September 1994, Vol. 84, No. 91418 American Journal of Public Health
TABLE 6-Outline of the Adequacy of Prenatal Care Utilization Index
I. Month prenatal care began (Adequacy of Initiation of Prenatal Care)Adequate Plus: 1 st or 2nd monthAdequate: 3rd or 4th monthIntermediate: 5th or 6th monthInadequate: 7th month or later, or no prenatal care
II. Proportion of the number of visits recommended by the American College ofObstetricians and Gynecologists received from the time prenatal care
began until delivery (Adequacy of Received Services)Adequate Plus: 110%Adequate: 80-109%Intermediate: 50-79%Inadequate: <50%
Ill. Summary Adequacy of Prenatal Care Utilization IndexAdequate Plus: Prenatal care begun by the 4th month and 1 10% or
more of recommended visits receivedAdequate: Prenatal care begun by the 4th month and 80/-1 09% ofrecommended visits received
Intermediate: Prenatal care begun by the 4th month and 50%-79%of recommended visits received
Inadequate: Prenatal care begun after the 4th month or less than 50%of recommended visits received
TABLE 7-Ratings Assigned to Births According to the Adequacy of PrenatalCare Utilization Index Compared with the Kessner Index
Adequacy of Prenatal Care Utilization Index
Kessner Inadequate, Intermediate, Adequate, Adequate Plus, % ofIndex % % % % Total Births
Inadequate 7.7 0.0 0.0 0.0 7.7Intermediate 8.9 10.1 5.0 2.4 26.3Adequate .1 12.1 38.3 15.4 65.9
% of total births 16.7 22.2 43.4 17.7 100.0
Note. Percentages are those of all US births; they may not add to 100 because of rounding.Source. Percentages are based on an analysis of birth certificate data from the 1980 National
Natality Survey.8

current literature using the Kessner Indexmay be overstating the limited but positiveassociation previously noted.3'19
Finally, the lack of documentationfor the Kessner Index, not surprising in aless computer-intensive era, has resultedin different computations of the KessnerIndex in different localities. Alexander etal.11 have shown in great detail howdifferent coding conventions regardingmissing data can result in major differ-ences in the measurement of prenatalcare adequacy and the evaluation ofperina-tal care programs such as Medicaid.
The proposed APNCU Index at-tempts to correct these four limitations ofthe Kessner Index. The independentassessment of prenatal care utilizationafter initiation, adjusted for the full rangeof gestational ages, is clearly the mostimportant new feature of the APNCUIndex. It provides information and aperspective on prenatal care utilizationthat is not presently available to the USpublic health community. This is impor-tant because many maternal and childhealth intervention programs are targetedtoward continuity of prenatal care ser-vices or enhancement of services once awoman has entered care (e.g., case man-agement, risk screening, home visita-tions). This new component should allowfor a more direct assessment of theseinitiatives, independent of the timing ofinitiation of care. Recent Medicaid en-hancements appear to have differentialeffects on the two different components ofprenatal care utilization.20'21
The establishment of an AdequatePlus category, another innovative featureof the APNCU Index, provides a means todirectly estimate the number of womenreceiving more than the ACOG-recom-mended number of visits, adjusted for thetiming of care initiation. It appears that itis important to isolate this fairly largegroup of high-risk women because theyhave a disproportionate number of thelow-birthweight babies.13 Efforts to isolatethis high-risk group based simply on anabsolute number of visits (13+) will notbe accurate, incorrectly classifying manywomen who start prenatal care late orwho are post-term.
Though not emphasized in the datapresentations in this paper, the APNCUIndex does allow for the direct ascertain-ment of the extent of "no prenatal care"as a subcategory of Inadequate prenatalcare. Several perinatal analysts have em-phasized the importance of distinguishingbetween these two groups.22"-3
September 1994, Vol. 84, No.9
The proposed APNCU Index can beseen as a second-generation prenatal careadequacy index. The APNCU Index wasdeveloped in 1987 and improved throughfeedback from multiple early users. Thecurrent version (III) includes an Ad-equate Plus category in the SummaryIndex; distinguishes "no prenatal care"within the Inadequate care category; hasfurther clarified the coding of "no data,""missing data," and unusual data combina-tions; and allows users to adapt thecomputer program for unusual codingconventions in their own databases. Thepresent version is basically a very minorrevision of the prior APNCU Index'salgorithms.
There are limitations to this newAPNCU Index. First, it does not measurethe adequacy of the content of prenatalcare, but merely that of the utilization ofprenatal care; hence its name. Second, theAPNCU Index is only as accurate as thedata (birth certificate or otherwise) usedto calculate it. Inaccuracies in birthcertificate data have been well docu-mented, especially for prenatal care infor-mation2 and gestational age.24 Third, thisindex has the opposite bias of the KessnerIndex: the longer the pregnancy, the moreopportunity to miss prenatal care visits,and hence the less likelihood of a rating ofAdequate or Adequate Plus.18 This bias isnot, however, built into the structure ofthe index; the adequacy ratings accuratelyreflect the increasing difficulty thatwomenhave in meeting the demanding ACOGrecommendations as the pregnancy contin-ues. Fourth, the present APNCU Indexdoes not adjust for the risk conditions ofthe mother. The ACOG recommenda-tions are for women with uncomplicatedpregnancies; thus, the APNCU Indexproduces a slightly conservative estimateof inadequate prenatal care utilizationbecause it underestimates the true needfor prenatal care visits.
ConwlusionsThe proposed APNCU Index, with
its two components, provides a moreaccurate and comprehensive set of mea-sures of prenatal care utilization than thewidely used Kessner Index. The accuratemeasurement of prenatal care utilizationis a critical step in the development ofpublic health programs to improve prena-tal care services and ultimately to improvebirth outcomes. O
Prenatal Care Use
AcknowledgmentsAn earlier version of this paper was presentedat the 115th Annual Meeting of the AmericanPublic Health Association, New Orleans, La,October 18-21, 1987.
The author wishes to thank Paul Wise,Chris Costello, Diane Ramsey, and the manyusers of early versions of the APNCU Indexwho made suggestions to improve its versatilityand accuracy.
References1. Kessner DM, Singer J, Kalk CE, Schle-
singer ER. Infant Death: An Analysis byMatemal Risk and Health Care. Washing-ton, DC: Institute of Medicine and Na-tional Academy of Sciences; 1973:chap 2.
2. Forrest JD, Singh S. Timing of prenatalcare in the United States: how accurate areour measurements? Health Serv Res. 1987;22:235-253.
3. Liberatos P, Kiely JL. Selected issues in theevaluation of prenatal care. In: Kiely M,ed. Reproductive and Perinatal Epidemiol-ogy. Boca Raton, Fla: CRC Press; 1991:79-98.
4. Gortmaker SL. The effects of prenatal careupon the health of the newborn. Am JPublic Health. 1979;69:653-660.
5. Quick JD, Greenlick MR, Roghmann KJ.Prenatal care and pregnancy outcome in anHMO and general population: a multivari-ate cohort analysis. Am J Public Health.1981;71:381-390.
6. Showstack JA, Budetti PP, Minkler D.Factors associated with birthweight: anexploration of the roles of prenatal careand length ofgestation.Am JPublic Health.1984;74:1003-1008.
7. Murray JL, Bemfield M. The differentialeffect of prenatal care on the incidence oflow birthweight among whites and blacks ina prepaid health care plan. N Engl J Med.1988;319:1385-1391.
8. Placek PJ. The 1980 National Natality andFetal Mortality Surveys. Public Health Rep.1984;99:111-116.
9. Keppel KG, Heuser RL, Placek PJ. Meth-ods and response characteristics, 1980National Natality and Fetal MortalitySurveys. VitalHealth Stat [2]. 1986; no. 100.DHHS publication PHS 86-1374.
10. Manual of Standards in Obstetric-Gyneco-logic Practice. 2nd ed. Chicago, Ill: Ameri-can College of Obstetricians and Gynecolo-gists; 1965.
11. Alexander GR, Tompkins ME, PetersenDJ, Weiss J. Sources of bias in prenatalcare utilization indices: implications forevaluating the Medicaid expansion. Am JPublic Health. 1991;81:1013-1016.
12. Standards for Obstetric-Gynecologic Ser-vices. 6th ed. Washington, DC: AmericanCollege of Obstetricians and Gynecolo-gists; 1985.
13. Kotelchuck M. The adequacy of prenatalcare utilization index: its US distributionand association with low birthweight.Am JPublic Health. 1994;84:1486-1489.
14. HealthyPeople2000: National Health Promo-tion and Disease Prevention Objectives.Washington, DC: US Dept of Health andHuman Services; 1991. DHHS publicationPHS 91-50212.
15. Hogue CJ, Buehler JW, Strauss LT, Smith
American Journal of Public Health 1419

Kotelchuck
JC. Overview of the national infant mortal-ity surveillance project-design, methodand results. Public Health Rep. 1987;102:126-138.
16. Kotelchuck M, Costello CA, Wise PH.Race differences in utilization of prenatalcare services in the U.S. Presented at the115th Annual Meeting of the AmericanPublic Health Association; October 18-21,1987; New Orleans, La.
17. Kogan MD, Kotelchuck M, Johnson S.Racial differences in late prenatal carevisits. JPerinatol. 1993;13:14-21.
18. Kleinman JC. Methodological issues in theanalysis of vital statistics. In: Kiely M, ed.
Reproductive and Pennatal Epidemiology.Boca Raton, Fla: CRC Press; 1991:447-468.
19. Institute of Medicine. PreventingLowBirth-weight. Washington, DC: National Acad-emy Press; 1985.
20. Braveman P, Bennett T, Lewis C, et al.Access to prenatal care following majorMedicaid eligibility expansions. JAMA.1993;269:1285-1289.
21. Krieger JW, Connell FA, LoGerfo JP.Medicaid prenatal care: a comparison ofuse and outcomes in fee-for-service andmanagedcare.AmJPublicHealth. 1992;82:185-190.
22. Harris JE. Prenatal medical care andinfant mortality. In: Fuchs VR, ed. Eco-nomic Aspects of Health. Chicago, Ill:University of Chicago Press; 1982:15-52.
23. Alexander GR, Comely DA. Prenatal careutilization: its measurement and relation-ship to pregnancy outcome.Am JPrev Med.1987;3:243-253.
24. Fingerhut A, Kleinman JC. Comparabilityof reporting between the birth certificateand the 1980 National Natality Survey.Vital Health Stat [2]. 1985; no. 99. DHHSpublication PHS 86-1373.
InfuatMoraty
....Alth ug su de inan death.....s..n
1420 American Journal of Public Health September 1994, Vol. 84, No. 9