An analysis of risk factors for upper urinary tract deterioration in patients with myelodysplasia
4
BJU International (1999), 84, 679–682 An analysis of risk factors for upper urinary tract deterioration in patients with myelodysplasia N. SEKI, K. AKAZAWA*, K. SENOH, S. KUBO, T. TSUNODA, Y. KIMOTO and S. NAITO Department of Urology, Fukuoka City Medical Center for Sick Children and Infectious Disease, *Department of Medical Informatics and Urology, Faculty of Medicine, Kyushu University, Fukuoka, Japan Objective To identify the risk factors for upper urinary Results The univariate analysis showed low vesical com- pliance, a high level of MUCP and the presence of DSD tract deterioration in a retrospective study of patients with myelodysplasia. to be significant factors for the incidence of VUR. Low vesical compliance and a high level of MUCP also Patients and methods The medical history, radiographic studies and urodynamic results from 39 children with correlated with the incidence of hydronephrosis. The multivariate analysis showed a significant relationship myelodysplasia who were treated at our hospital were reviewed retrospectively to obtain more accurate data between urodynamic values and upper urinary tract deterioration. The incidence of VUR was strongly in the prognosis of such patients. The upper urinary tracts were assessed by cysto-urethrography and correlated with a high MUCP and the presence of DSD. A high MUCP was also a significant factor in the excretory urography to determine the incidence of vesico-ureteric reflux (VUR) and hydronephrosis. The incidence of hydronephrosis. Conclusion Urodynamic results associated directly with relationships between the urodynamic variables, including vesical compliance, detrusor hyper-reflexia, the abnormal function of urethral control are signifi- cantly correlated with the cause of upper tract deterior- detrusor-sphincter dyssynergia (DSD) and the maxi- mum urethral closing pressure (MUCP) to such upper ation in patients with myelodysplasia. Keywords Myelodysplasia, vesico-ureteric reflux, tract deterioration were evaluated using both univari- ate and multiple logistic regression analysis. detrusor-sphincter dyssynergia, prognosis an objective statistical analysis to determine whether Introduction these multiple risk factors, mainly obtained from urodyn- amic testing, had any significant correlation with upper It is generally accepted that upper urinary tract deterior- ation is closely related to an elevated intravesical press- urinary tract damage observed in myelodysplastic patients, based on a stepwise logistic regression analysis. ure in patients with myelodysplasia. The prognostic value and usefulness of urodynamics remain contro- versial. However, urodynamics are still used to detect Patients and methods the behaviour of the lower urinary tract and to diagnose myelodysplastic patients at high risk of upper urinary The clinical history, radiographic studies and urodyn- amic results from 63 patients with myelodysplasia tract deterioration. The urodynamic variables which seem to be linked to upper tract deterioration have been treated at Fukuoka City Medical Center for Sick and Infectious Diseases during 1984–1996 were reviewed described by diCerent authors to include the leak-point pressure [1–3], detrusor-sphincter dyssynergia (DSD) retrospectively. In all, 39 myelodysplastic patients (23 males and 16 females, mean age 5.8 years, range 0–18) [4,5], the maximum urethral closure pressure (MUCP) [6], detrusor hyper-reflexia [5] and vesical compliance (Fig. 1) were assessed. To be included in the study, all patients had to present a clinical course which had not [2,7]. The eCect of these studies is reflected in the popular use of a urodynamic assessment for myelodysplastic been managed by either intermittent or indwelling cath- eterization before being referred to our hospital. The patients and in the adopted practice of an early urodyn- amic investigation for infants with myelodysplasia. basic evaluations for inclusion in the study were an excretory urogram, a voiding cysto-urethrogram and a However, these factors are often correlated and their combined statistical importance should be investigated baseline urodynamic study which had been performed within 30 days after the first visit. None of the patients in a multivariate analysis. In this study, we conducted were managed using any oral anticholinergic agents during the evaluation. Water cystometry at a filling rate Accepted for publication 6 May 1999 679 © 1999 BJU International
Transcript of An analysis of risk factors for upper urinary tract deterioration in patients with myelodysplasia

BJU International (1999), 84, 679–682
An analysis of risk factors for upper urinary tractdeterioration in patients with myelodysplasiaN. SEKI, K. AKAZAWA*, K. SENOH, S. KUBO, T. TS UNODA, Y. KIMOTO† and S. NAITO†Department of Urology, Fukuoka City Medical Center for Sick Children and Infectious Disease, *Department of Medical Informaticsand †Urology, Faculty of Medicine, Kyushu University, Fukuoka, Japan
Objective To identify the risk factors for upper urinary Results The univariate analysis showed low vesical com-pliance, a high level of MUCP and the presence of DSDtract deterioration in a retrospective study of patients
with myelodysplasia. to be significant factors for the incidence of VUR. Lowvesical compliance and a high level of MUCP alsoPatients and methods The medical history, radiographic
studies and urodynamic results from 39 children with correlated with the incidence of hydronephrosis. Themultivariate analysis showed a significant relationshipmyelodysplasia who were treated at our hospital were
reviewed retrospectively to obtain more accurate data between urodynamic values and upper urinary tractdeterioration. The incidence of VUR was stronglyin the prognosis of such patients. The upper urinary
tracts were assessed by cysto-urethrography and correlated with a high MUCP and the presence of DSD.A high MUCP was also a significant factor in theexcretory urography to determine the incidence of
vesico-ureteric reflux (VUR) and hydronephrosis. The incidence of hydronephrosis.Conclusion Urodynamic results associated directly withrelationships between the urodynamic variables,
including vesical compliance, detrusor hyper-reflexia, the abnormal function of urethral control are signifi-cantly correlated with the cause of upper tract deterior-detrusor-sphincter dyssynergia (DSD) and the maxi-
mum urethral closing pressure (MUCP) to such upper ation in patients with myelodysplasia.Keywords Myelodysplasia, vesico-ureteric reflux,tract deterioration were evaluated using both univari-
ate and multiple logistic regression analysis. detrusor-sphincter dyssynergia, prognosis
an objective statistical analysis to determine whetherIntroduction
these multiple risk factors, mainly obtained from urodyn-amic testing, had any significant correlation with upperIt is generally accepted that upper urinary tract deterior-
ation is closely related to an elevated intravesical press- urinary tract damage observed in myelodysplasticpatients, based on a stepwise logistic regression analysis.ure in patients with myelodysplasia. The prognostic
value and usefulness of urodynamics remain contro-versial. However, urodynamics are still used to detect
Patients and methodsthe behaviour of the lower urinary tract and to diagnosemyelodysplastic patients at high risk of upper urinary The clinical history, radiographic studies and urodyn-
amic results from 63 patients with myelodysplasiatract deterioration. The urodynamic variables whichseem to be linked to upper tract deterioration have been treated at Fukuoka City Medical Center for Sick and
Infectious Diseases during 1984–1996 were revieweddescribed by diCerent authors to include the leak-pointpressure [1–3], detrusor-sphincter dyssynergia (DSD) retrospectively. In all, 39 myelodysplastic patients (23
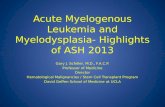
males and 16 females, mean age 5.8 years, range 0–18)[4,5], the maximum urethral closure pressure (MUCP)[6], detrusor hyper-reflexia [5] and vesical compliance (Fig. 1) were assessed. To be included in the study, all
patients had to present a clinical course which had not[2,7]. The eCect of these studies is reflected in the popularuse of a urodynamic assessment for myelodysplastic been managed by either intermittent or indwelling cath-
eterization before being referred to our hospital. Thepatients and in the adopted practice of an early urodyn-amic investigation for infants with myelodysplasia. basic evaluations for inclusion in the study were an
excretory urogram, a voiding cysto-urethrogram and aHowever, these factors are often correlated and theircombined statistical importance should be investigated baseline urodynamic study which had been performed
within 30 days after the first visit. None of the patientsin a multivariate analysis. In this study, we conductedwere managed using any oral anticholinergic agentsduring the evaluation. Water cystometry at a filling rateAccepted for publication 6 May 1999
679© 1999 BJU International

680 N. S EKI et al.
shown in Table 1; three factors, including patient age,vesical compliance and MUCP, were considered to becontinuous. The Mann–Whitney U-test for continuousand the chi-square test for categorical factors were usedto determine the risk factors which were significant onunivariate analysis for the occurrence of VUR and hydro-nephrosis, respectively. Next, multiple logistic regressionanalyses using the forward stepwise regression methodwere used to select a set of risk factors from the sixassessed [8]. A dependent variable was the presence ofupper urinary tract deterioration. Likelihood ratio testswith a significance level of 0.05 were used to enter orremove any factors at each step. The odds ratio (OR)shows the magnitude of the association between thefactors and upper urinary tract deterioration. The largerthe OR (or when its reciprocal was <1) the greater themagnitude of the eCect. An OR of 1 indicated nocorrelation between that factor and upper urinary tractdeterioration; when <1, an inverse correlation was
1Age at the initial evaluation (years)2 4 6 8 10 12 14 16 18
Nu
mb
er o
f p
atie
nts
2
4
6
8
0
considered to exist between the factor and the upperFig. 1. The sex distribution (male, green; female, red) with age ofthe patients with spina bifida at the initial evaluation. tract changes. The statistical analysis used was that
described by Engelman [9].of 10–30 mL/min was carried out with the patientsupine. A slower infusion was used for children <1 year
Resultsold. A 7 F single lumen catheter with four side-holeswas used to fill and measure the bladder and record Of the 39 patients, 15 (39%) showed some degree of
VUR and hydronephrosis was identified in five patientsurethral pressures (a 5 F feeding tube was used forinfants). Detrusor hyper-reflexia was defined as intraves- (13%) at evaluation. The results of the analysis presented
in Table 1 show a low vesical compliance, a high levelical phasic pressure waves of >15 cmH2O. Vesical com-
pliance was determined by calculating the volume of of MUCP and the presence of DSD to be significant factorsfor the incidence of VUR. The low vesical complianceinfused saline for each 1 cmH
2O pressure change before
the steep terminal pressure increase. The MUCP was and a high level of MUCP were statistically significantlyassociated with the incidence of hydronephrosis. Thedetermined from the urethral pressure profile, compared
with a perfusion rate of 2–4 mL/min by manual with- results of a stepwise logistic regression analysis arepresented in Table 2. The high level of MUCP and thedrawal after the bladder was emptied. Adhesive perineal
skin electrodes were used to record the sphincter EMG. presence of DSD were selected as having the mosteCective combination of factors for the incidence of VURThe bio-electrical activity was interpreted from standard
EMG criteria. DSD was diagnosed if the EMG activity (Table 2). A high level of MUCP was also selected as asignificant factor which correlated with the incidence offailed to decrease on contraction of the bladder during a
sustained increase in intravesical pressure. Both excret- hydronephrosis (Table 2). The OR of the selected factorswere all >1, indicating that the presence of DSD and aory urography and voiding cystography were performed
(with voiding attempted using Valsaeva’s manoeuvre) at high level of MUCP increased the risk of upper urinarytract deterioration.the initial evaluation to analyse upper urinary tract
changes. A deterioration of the upper urinary tract wasconsidered to imply hydronephrosis and VUR. Patients
Discussionwith hydronephrosis secondary to high-grade reflux wereclassified as having reflux only. All radiographs were Upper urinary tract deterioration is a major potential
complication in myelodysplastic patients with neuro-reviewed by one physician. All patients showing hydro-nephrosis on the excretory urogram with no high-grade genic bladder impairment. VUR was detected in 39% of
the present patients, an incidence similar to thosereflux (i.e. grade >3 according to the internationalclassification) were judged to be positive for hydroneph- reported previously [10–12]. As suggested by Kurzrock
et al. [10], the lower incidence of hydronephrosisrosis. In addition any patients who had VUR (grade >1)were classified as reflux-positive. observed in the present study (13%) than that reported
in others [1,4,5,13,14] might be because other studiesThe six potential risk factors used in the analysis are
© 1999 BJU International 84, 679–682

MYELODYS PLASIA RIS K IN UPPER URINARY TRACT DETERIORATION 681
Table 1 A univariate analysis of the incidence of VUR and hydronephrosis vs various factors
VUR Hydronephrosis
Variables Absent Present Absent Present
Age (years) 3.5 (2.4, 8.9) 4.2 (1.3, 9.9) 3.5 (2.1, 9.4) 5.7 (1.8, 6.2)Compliance (mL/cmH
2O) 8.5 (5.0, 16.0) 3.5 (2.0, 5.9)* 6.3 (3.7, 14.2) 2.2 (1.9, 3.3)*
MUCP (cmH2O) 30 (24, 39) 48 (35, 61)† 36 (27, 47) 60 (50, 61)*
SexM 14 9 21 2F 10 6 13 3Detrusor sphincter dyssynergiaAbsent 20 4‡ 23 1Present 4 11 11 4Detrusor hyper-reflexiaAbsent 20 9 25 4Present 4 6 9 1
Continuous variables are expressed as the median (25th percentile, 75th percentile) and were tested using the Mann–Whitney test;categorical variables were tested using the chi-square test. *P<0.05, †P<0.01, ‡ P<0.001.
Table 2 A multivariate analysis of the incidence of VUR and that the most important risk factor for upper tracthydronephrosis against various factors. Age, sex, compliance and damage was bladder pressure at the time of urethralUIC gave no significant values (NS) with either incidence leakage (leak-point pressure). The maximum urethral
pressure measured at rest in patients with no reflexVariables CoeBcient sem OR P
detrusor activity was almost the same as the urethralopening pressure, which thus indicated that the MUCPVURmeasured with an empty bladder represented the leak-MUCP 0.10 0.04 1.10 0.013
DSD 2.93 1.04 18.76 0.005 point pressure (urethral opening pressure) in theseHydronephrosis patients. In this study, we therefore selected MUCP asMUCP 0.07 0.03 1.08 0.034 an index to represent the urethral function in theseDSD NS NS NS 0.074 patients. Bauer et al. [4] showed a close correlation
between the presence of DSD and upper tract deterior-ation in myelodysplastic infants. Vesical compliance[2,7,10,18] and detrusor hyper-reflexia [5] have alsodid not distinguish between patients with high-grade
reflux and hydronephrosis. been advocated as factors influencing the developmentof upper tract damage in these patients. In the presentThere are some clinical, radiological and urodynamic
factors which may help to predict which patients are at study, the univariate analysis showed that detrusorhyper-reflexia was not significantly associated with therisk of upper urinary tract deterioration. The incidence
of upper tract damage has been shown to increase with incidence of upper urinary tract deterioration. There wasa large diCerence between the proportions with VURpatient age [15]. In untreated patients, Smith [16]
showed that there was a gradual deterioration of the present in those with or without detrusor hyper-reflexia(31% and 60%, respectively), and thus the analysisupper and lower urinary tracts. In the present study,
patient age was not a significant factor. Although the showed no statistical significance between the groups,possibly because there were too few patients to detect it,aetiology remains uncertain, several previous studies
reported a higher incidence of VUR in female patients, even though there may have been a large diCerence.In a multivariate analysis, the ORs for the incidencewith no significant diCerences in the urodynamic vari-
ables, thus suggesting that females may be at higher of VUR and hydronephrosis for the patients with a MUCPat the 75th percentile vs the 25th percentile were 9.03risk for developing VUR [6,10,17]. However, there were
no diCerences between the sexes in the upper tract and 4.66, respectively. The OR for the incidence ofhydronephrosis for the patients with DSD vs patientschanges in the present statistical analysis.
The urodynamic variables that seem to induce a high without was 18.76. These results suggest that a highMUCP and the presence of DSD are significantly associ-intravesical pressure in the urinary storage phase have
been postulated to be factors relevant to the incidence ated with the incidence of upper urinary tract deterior-ation. However, low vesical compliance was a significantof upper tract deterioration. McGuire et al. [1] suggested
© 1999 BJU International 84, 679–682

682 N. S EKI et al.
8 Hosmer DW, Lemeshow S. Applied Logistic Regression. Newrisk factor for upper tract deterioration based on theYork: John Wiley and Sons, 1989: 141–5univariate analysis, but it was not statistically significant
9 Engelman L. Stepwise logistic regression. In Dixon WJ,in the multivariate analysis. Therefore vesical complianceBrown MB, Engelman L, Jennrich RI eds, BMDP Statisticalis not an independent significant factor for the upperSoftware Manual. Berkeley: University California Press,tract changes after simultaneously adjusting for the1990: 1013–46
eCects of other various factors. These findings indicate10 Kurzrock EA, Polse S. Renal deterioration in myelodysplastic
that poor compliance alone cannot explain the deterior- children: urodynamic evaluation and clinical correlates.ation of the upper tracts seen in these patients. Even if J Urol 1998; 159: 1657–61the vesical compliance in the filling phase was poor, the 11 Sidi AA, Peng W, Gonzalez R. Vesicoureteral reflux inupper urinary tract would be protected, provided that children with myelodysplasia: natural history and results
of treatment. J Urol 1986; 136: 329–31the outlet resistance remained low. Furthermore,12 Flood HD, Ritchey ML, Blood DA, Huang C, McGuiredetrusor hyper-reflexia showed no significant correlation
EJ. Outcome of reflux in children with myelodysplasiawith the incidence of upper tract damage.managed by bladder pressure monitoring. J Urol 1994;These results clinically confirm a significant corre-152: 1574–7lation in myelodysplastic patients between the degree of
13 Galloway NTM, Mekras JA, Helms M, Webster GD. Anupper urinary tract deterioration and abnormal lowerobjective score to predict upper tract deterioration in
urinary tract function, especially for the disordered func-myelodysplasia. J Urol 1991; 145: 535–7
tion of the urethral control mechanism. 14 Wang SC, McGuire EJ, Bloom DA. A bladder pressuremanagement system for myelodysplasia – clinical outcome.J Urol 1988; 140: 1499–502
15 Wilcock AR, Emery JL. Deformities of the renal tract inReferences children with meningomyelocele and hydrocephalus, com-
1 McGuire EJ, Woodside JR, Borden TA, Weiss RM. Prognostic pared with those of chidlren showing no such centralvalue of urodynamic testing in myelodysplastic patients. nervous system deformities. Br J Urol 1970; 42: 152–7J Urol 1981; 126: 205–9 16 Smith ED. Urinary prognosis in spina bifida. J Urol 1972;
2 Ghoniem GM, Roach MB, Lewis VH, Harmon EP. The 108: 815–7value of leak point pressure and bladder compliance in the 17 Teichman JMH, Scherz HC, Kim KD, Cho DH, Packer MG,urodynamic evaluation of meningomyelocele patients. Kaplan GW. An alternative approach to myelodysplasiaJ Urol 1990; 144: 1440–2 management; aggressive observation and prompt inter-
3 McGuire EJ, Woodside JR, Borden TA. Upper urinary tract vention. J Urol 1994; 152: 807–11deterioration in patients with myelodysplasia and detrusor 18 Sidi AA, Dykstra DD, Gonzalez R. The value of urodynamichypertonia: a follow-up study. J Urol 1983; 129: 823–6 testing in the management of neonates with myelodyspla-
4 Bauer SB, Hallett M, Khoshbin S et al. Predictive value of sia; a prospective study. J Urol 1986; 135: 90–3urodynamic evaluation in newborns with myelodysplasia.JAMA 1984; 252: 650–2
Authors5 McLorie GA, Perez-Marero R, Csima A, Churchill BM.Determinants of hydronephrosis and renal injury in patients N. Seki, MD, PhD, Clinical Fellow.
K. Akazawa, PhD, Assistant Professor.with myelomeningocele. J Urol 1988; 140: 1289–926 Kobayashi S, Shinno Y, Kakizaki H, Matsumura K, K. Senoh, MD, PhD, Head of Department.
S. Kubo, MD, Clinical Fellow.Koyanagi T. Relevance of detrusor hyperreflexia, vesicalcompliance and urethral pressure to the occurrence of T. Tsunoda, MD, Resident.
Y. Kimoto, MD, PhD, Assistant Professor.vesicoureteral reflux in myelodysplastic patients. J Urol1992; 147: 413–5 S. Naito, MD, PhD, Professor and Director of Department.
Correspondence: Dr N. Seki, Department of Urology, Kyushu7 Ghoniem GM, Bloom DA, McGuire EJ, Stewart KL. Bladdercompliance in meningomyelocele children. J Urol 1989; University School of Medicine, 3–1-1 Maidashi, Higashi-ku,
Fukuoka, 812–8582, Japan.141: 1404–6
© 1999 BJU International 84, 679–682