An amalgam tattoo causing local and systemic disease?
4
Click here to load reader
-
Upload
thomas-weaver -
Category
Documents
-
view
218 -
download
4
Transcript of An amalgam tattoo causing local and systemic disease?

An amalgam tattoo causing local and systemic disease? Thomas Weaver, Lieutenant Commander (DC) USN,* Paul L. Auclair, Commander (DC) USN,*** and George M. Taybos, Captain (DC) USN***
NAVAL DENTAL SCHOOL, NAVAL DENTAL CLINIC. NAVAL MEDICAL COMMAND NATIONAL CAPITAL REGION, BETHESDA, MD.
Amalgam tattoos are common oral lesions. The case presented here involved a 33-year-old woman who had had an amalgam tattoo for 2 years and complained of localized soreness and occasional swelling as well as systemic symptoms of weight loss, fatigue, sinusitis, and headaches. After excisional biopsy of the lesion, the patient’s complaints ceased dramatically. It is suggested that alterations in healing due to the presence of amalgam particles led to systemic as well as local disease. (ORAL SURG. ORAL MED. ORAL PATHOL. 1987;63:137-40)
A malgam tattoos are asymptomatic, distinct mac- ules that usually have poorly defined borders. They are blue-black to blue-gray or brown and usually cannot be palpated as distinct lesions. These tattoos result from the accidental implantation of dental amalgam in the soft tissues, and the clinical discolor- ation is due to the subsequent precipitation and dispersion of silver ions with sulfur.’ Radiopaque particles may or may not be seen at the site of the lesion, depending on the size of the particles embed- ded. Histologically, a variety of patterns is observed, depending on the size of the particles and whether or not the particles are contaminated.
Tissue reactions to embedded small, powdered amalgam particles may vary. There may be no reaction at all,z or the reaction may range from mild or moderate chronic inflammation3 to granuloma formation.4 Small particles usually cause less inflam- mation than large particles.5 Elef and Ellender and associate@ have shown that large fragments of amal- gam stimulate the formation of thick-walled capsules with poorly formed collagen. Ellender and colleagues attribute the formation of these capsules to tissue damage and impaired collagen formation.
The opinions or assertions contained herein are the private ones of the authors and are not to be construed as official or as reflecting the views of the Department of the Navy. *Resident, Oral Diagnosis Department. **Chairman, Oral Pathology Department. ***Chairman, Oral Diagnosis Department.
The following is an unusual case in which an amalgam tattoo may have caused local and systemic disease.
CASE REPORT
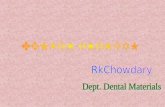
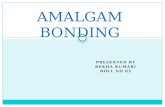
A 33-year-old white woman was first seen in the dental clinic in January 1985 in consultation for “evaluation of TMJ pain.” The patient at that time had signs and symptoms consistent with temporomandibular joint-myo- fascial pain dysfunction syndrome (TMJ-MPDS) and maxillary sinusitis. She complained of headaches, soreness in the area of the right TMJ, sinusitis, and postnasal drip. A preliminary examination was performed, during which a slightly elevated, firm, brown, nodular lesion, approxi- mately 7 x 7 mm, was discovered in the right buccal mucosa (Fig. 1). The patient indicated that the lesion has been present since about March 1983, when her buccal mucosa was “severely” lacerated during crown preparation of the maxillary right second molar. A radiograph showed the presence of radiopaque particles (Fig. 2), and a clinical diagnosis of amalgam tattoo was made. Entex was pre- scribed for the sinus congestion, and the patient was instructed to take three aspirin tablets three to four times a day. She was also instructed to place moist heat on the affected area and was given exercises to perform to decrease possible symptoms of TMJ-MPDS.
At a follow-up appointment 1 week later, the lesion and symptoms were unchanged. Ampicillin and Drixoral brand of dexbrampheniramine maleate and pseudoephedrine sul- fate (Schering Corp., Kenilworth, New Jersey) were pre- scribed for sinusitis. The patient was then scheduled for a comprehensive TMJ workup, at which time a more com-
137

138 Weaver, Auclair, and Taybos Oral Surg. January, I987
Fig. f . Preoperative photograph of right buccal mucosa and lesion. The density of the lesion in a black and white print is similar to that of the surrounding normal mucosa; however, please note the lack of vascular pattern in the area highlighted by the arrows.
Fig. 2. Preoperative radiograph of maxillary right molars. Note small radiopaque object distal to second molar.
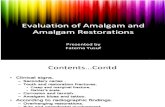
Fig. 3. A, Photomicrograph showing deposits of foreign material, chronic inflammatory cells, and muscle. (Original magnification, X100.) 3, Skeletal muscle bundles outlined by granules of foreign material. (Original magnification, X450.)

Volume 63 Number 1
Amalgam tattoo 139
Fig. 4. Photomicrograph showing multinucleated foreign body giant cell and fragments of foreign material. (Original magnification, X450.)
prehensive history and physical examination would be performed.
At the next appointment, the patient related that, after the dentist had severely injured the tissue in the area of the tooth during crown preparation, the tissue was very sore for a few days and then became sore again in about a week. She indicated that the later pain was different from the pain that followed the initial trauma. Shortly after delivery of the crown, the patient’s husband was transferred from the West Coast to the East Coast. During the transit across country, the patient noticed a “boil” on her right cheek. A physician treated the lesion with tetracycline. At that time, the patient did not connect the presence of the “boil” with the intraoral trauma. When asked by the physician if she had traumatized the area, she said that she had not.
During the history taking, the patient stated: “This may sound funny, but whenever I get antibiotics for something else, the headaches, sinusitis, postnasal drip, and soreness go away but come back in about a week after 1 run out of the antibiotics.” During the examination, the soreness was localized in the area of the lesion in the right buccal mucosa.
Because of the history and findings, an excisional biopsy was performed on April 19, 1985, with the patient under local anesthesia. A 1 cm oval wedge of brown soft tissue was submitted to the Pathology Department of the Naval Dental School for microscopic diagnosis. Histologic exam- ination revealed elliptical sections of mucosa covered with stratified squamous epithelium. Beneath the epithelium there were clumps and granules of black to gotden brown foreign material, some of which were seen within the walls of the blood vessels and deep within muscle tissue. Also present was a focally dense infiltrate of chronic inflamma- tory cells, including lymphocytes, plasma cells, and histio- cytes, some of which were multinucleated. Mucous sali- vary glands were also noted. The diagnosis was “amalgam tattoo with chronic myositis” (Figs. 3 and 4). A tissue
Fig. 5. Area of lesion 2 weeks postoperatively. The area appears slightly darkened because of recent occlusal trau- ma to the mucosa.
Gram stain performed by the Oral Pathology Department was nonreactive.
The patient was seen at a follow-up appointment on June 11, 1985. She indicated that after the tissue was removed and initial healing was completed she had experi- enced no headaches, postnasal drip, sinusitis, or soreness. She also stated that she “felt better” and that she did not realize she had been “run down” for a long time until she noticed a dramatic change after the biopsy. She also stated that she was able to gain some weight, something she had been unsuccessfuliy attempting to do for more than 18 months. There was a clinical impression of increased opening because the postoperative photographs (Fig. 5) had been easier to take. The patient stated that she had taken no medications since the procedure, other than analgesics for 1 day following the biopsy.

140 Weaver, Auclair, and Taybos
DISCUSSION
It is hypothesized that the lesion and accompany- ing symptoms can be explained as follows: The buccal mucosa became contaminated, either at the time of the trauma or shortly thereafter, as evidenced by the return of pain after initial healing. The injury initiated the healing process. However, because of the relatively large fragment (as seen radiographical- ly) as well as the deep involvement (indicated by myositis), the capsule wall surrounding the fragment was poorly formed. This diffuse, deep-seated process may have allowed a colony of bacteria to maintain itself without fatal interference from the body’s defenses, and it may also have allowed the slow release of bacteria into the patient’s system, produc- ing the local and systemic effects. Although a culture was not taken, the contamination probably was bacterial, in view of the remission of symptoms during times of antibiotic therapy.
This case is instructive for several reasons. This woman had seen many practitioners and had given essentially the same history to all. Because of the location of the pain, all of those clinicians told the patient that she was suffering from stress-induced TMJ-MPDS. The intraoral lesion was usually dis- missed as an innocuous amalgam tattoo. In this case, the history was the important determinant in diagno- sis. Second, the fact that one entity such as an amalgam tattoo is present is no reason why a second or third entity (bacterial contamination) cannot be responsible for the signs and symptoms of disease.
Oral Surg. January, 1987
Third, when patients stated, “This may sound funny, but . . .,” they may just be indicating exactly what is wrong. This phenomenon appears to be borne out in casual conversations with other clinicians. Finally, even lesions that are easily recognized clinically may still require biopsy which, surprisingly, may turn out to be curative as well as diagnostic.
The authors want to thank the Publications Division at the Naval Dental School for assistance in the preparation of this article.
REFERENCES
1.
2.
3.
4.
5.
6.
Hatch CL, Terezhalmy GT, Krolls SO: Amalgam tattoos of the oral soft tissue. Ear Nose Throat J 63: 19-29, 1984. Buchner A, Hansen LS: Amalgam pigmentation of the oral mucosa. ORAL SURG ORAL MED ORAL PATHOL 49: 139-147, 1980. Hansen LS, Silverman S: Localized tissue reaction to implanted amalgam: a review. Calif Dent Assoc J IO: 33-36, 1982. Eley BM: Tissue reactions to implanted dental amalgam, including assessment by energy dispersive x-ray microanaly- sis. J Pathol 138: 251-272, 1982. Cataldo E, Santis H: Response of the oral tissue to exogenous foreign materials. J Pediodontal 45: 93-106, 1973. Elender G, Ham KN, Harcourt JK: Toxic effects of dental amalgam implants: optical, histological, and histochemical observations. Aust Dent J 23: 395-399, 1978.
Reprint requests to: Captain George M. Taybos Oral Diagnosis Department Naval Dental School Naval Dental Clinic Naval Medical Command National Capital Region Bethesda, MD 20814-5077