
Amyotrophic Lateral Sclerosis
27
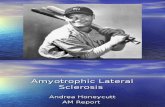
Amyotrophic lateral sclerosis From Wikipedia, the free encyclopedia "ALS" redirects here. For other uses, see ALS (disambiguation) . "Motor neurone disease" redirects here. For the broader group of diseases, see Motor neuron disease . Amyotrophic lateral sclerosis An MRI with increased signal in the posterior part of the internal capsule which can be tracked to the motor cortex consistent with the diagnosis of ALS. Classification and external resources ICD -10 G12.2 ICD -9 335.20 OMIM 105400 DiseasesDB 29148 MedlinePlus 000688 eMedicine neuro/14 emerg/24 pmr/10
description
Amyotrophic Lateral Sclerosis
Transcript of Amyotrophic Lateral Sclerosis
Amyotrophic lateral sclerosisFrom Wikipedia, the free encyclopedia"ALS" redirects here. For other uses, seeALS (disambiguation)."Motor neurone disease" redirects here. For the broader group of diseases, seeMotor neuron disease.Amyotrophic lateral sclerosis
AnMRIwith increasedsignalin the posterior part of theinternal capsulewhich can be tracked to themotor cortexconsistent with the diagnosis of ALS.
Classification and external resources
ICD-10G12.2
ICD-9335.20
OMIM105400
DiseasesDB29148
MedlinePlus000688
eMedicineneuro/14emerg/24pmr/10
Patient UKAmyotrophic lateral sclerosis
MeSHD000690
Amyotrophic lateral sclerosis(ALS), also known asLou Gehrig's diseaseandCharcot disease, is a specificdisorder that involves the death of neurons.[1]In the United Kingdom the termmotor neurone disease(MND) is commonly used,[2]while others usethat termfor a group of five conditions of which ALS is the most common.[3]ALS is characterized bystiff muscles,muscle twitching, and gradually worsening weakness due tomuscle wasting. This results in difficultyspeaking,swallowing, and eventuallybreathing.[4]The cause is not known in 90% to 95% of cases.[4]About 510% of cases areinheritedfrom a person's parents.[5]About half of these genetic cases are due to one of two specificgenes. It results in the death of the neurons that controlvoluntary muscles. The diagnosis is based on a person's signs and symptoms with testing done to rule out other potential causes.[4]There is no cure for ALS.[4]A medication calledriluzolemay extend life expectancy by about two to three months.[6]Non-invasive ventilationmay result in both improved quality and length of life.[7]The disease usually starts around the age of 60 and in inherited cases around the age of 50.[5]The average survival from onset to death is three to four years.[8]About 10% survive longer than 10 years.[4]Most die from respiratory failure. In much of the world, rates of ALS are unknown.[5]In Europe and the United States, the disease affects about 2 people per 100,000 per year.[5][9]Descriptions of the disease date back to at least 1824 byCharles Bell.[10]In 1869, the connection between the symptoms and the underlying neurological problems were first described byJean-Martin Charcot, who in 1874 began using the term amyotrophic lateral sclerosis.[10]It became well known in the United States when it affected the famous baseball playerLou Gehrig,[1]and in the 20th century whenStephen Hawkinggained fame for his scientific achievements.[11]In 2014 videos of theice bucket challengewent viral on the internet and increased public awareness.[12]Contents[hide] 1Signs and symptoms 1.1Initial symptoms 1.2Progression 1.3Late stages 1.4Eye movement 2Causes 2.1Genetics 2.1.1SOD1 2.2Other factors 3Pathophysiology 3.1Skeletal motor units 3.2Lactate and cinnamate 4Diagnosis 5Management 5.1Medications 5.2Breathing support 5.3Therapy 5.4Nutrition 5.5Palliative care 6Epidemiology 7History 7.1Etymology 8Society and culture 9Research 10References 11External linksSigns and symptoms[edit]The disorder causes muscle weakness andatrophythroughout the body due to the degeneration of theupperandlower motor neurons. Individuals affected by the disorder may ultimately lose the ability to initiate and control all voluntary movement, although bladder and bowel function and themuscles responsible for eye movementare usually spared until the final stages of the disorder.[13]Cognitive functionis generally spared for most people, although some (about 5%) also developfrontotemporal dementia.[14]A higher proportion of people (3050%) also have more subtle cognitive changes which may go unnoticed, but are revealed by detailedneuropsychological testing. Infrequently, ALS coexists in individuals who also experience dementia, degenerative muscle disorder, and degenerative bone disorder as part of a syndrome calledmultisystem proteinopathy.[15]Sensory nervesand theautonomic nervous systemare generally unaffected, meaning the majority of people with ALS maintainhearing,sight,touch,smell, andtaste.[16]Initial symptoms[edit]The start of ALS may be so subtle that the symptoms are overlooked.[17]The earliest symptoms of ALS are muscle weakness and/or muscle atrophy. Other presenting symptoms include trouble swallowing, breathing, cramping, or stiffness of affected muscles; muscle weakness affecting an arm or a leg; and/or slurred and nasal speech. The parts of the body affected by early symptoms of ALS depend on which motor neurons in the body are damaged first.About 75% of people contracting the disorder first experience weakness or atrophy in an arm or leg and this is known as "limb-onset" ALS. Awkwardness when walking or running or even tripping over or stumbling may be experienced and often this is marked by walking with a "dropped foot" which drags gently on the ground. Or if arm-onset, difficulty with tasks requiring manual dexterity such as buttoning a shirt, writing, or turning a key in a lock may be experienced. Occasionally, the symptoms remain confined to one limb for a long period of time or for the duration of the illness; this is known asmonomelic amyotrophy.About 25% of cases begin asprogressive bulbar palsytermed "bulbar-onset" ALS. Initial symptoms will mainly be of difficulty speaking clearly or swallowing. Speech may become slurred, nasal in character, or quieter. There may be difficulty in swallowing and loss of tongue mobility. A smaller proportion of people experience "respiratory-onset" ALS, where theintercostal musclesthat support breathing are affected first. A small proportion of people may also present with what appears to befrontotemporal dementia, but later progresses to include more typical ALS symptoms.Over time, people experience increasing difficulty moving, swallowing (dysphagia), and speaking or forming words (dysarthria). Symptoms of upper motor neuron involvement include tight and stiff muscles (spasticity) and exaggerated reflexes (hyperreflexia) including an overactive gag reflex. An abnormal reflex commonly calledBabinski's signalso indicates upper motor neuron damage. Symptoms of lower motor neuron degeneration include muscle weakness and atrophy, muscle cramps, and fleeting twitches of muscles that can be seen under the skin (fasciculations) although twitching is not a diagnostic symptom and more of a side effect so twitching would either occur after or accompany weakness and atrophy. Around 1545% of people experiencepseudobulbar affect, aneurological disorderalso known as "emotional lability", which consists of uncontrollable laughter, crying, or smiling, attributable to degeneration of bulbar upper motor neurons, resulting in exaggeration of motor expressions of emotion.[citation needed]For ALS to be diagnosed, symptoms of both upper and lower motor neuron damage that cannot be attributed to other causes must be present.Progression[edit]Although the order and rate of symptoms varies from person to person, most people eventually are not able to walk or use their hands and arms. They also lose the ability to speak and swallow food, while most end up on a portableventilator, called a BiPAP. The rate of progression can be measured using an outcome measure called the "ALS Functional Rating Scale Revised (ALSFRS-R)", a 12-item instrument administered as a clinical interview or patient-reported questionnaire that produces a score between 48 (normal function) and 0 (severe disability). Though the degree of variability is high and a small percentage of people have a much slower disorder, on average, patients lose about 0.9 FRS points per month. A survey-based study amongst clinicians showed that they rated a 20% change in the slope of the ALSFRS-R as being clinically meaningful.[18]Regardless of the part of the body first affected by the disorder, muscle weakness and atrophy spread to other parts of the body as the disorder progresses. In limb-onset ALS, symptoms usually spread from the affected limb to the opposite limb before affecting a new body region, whereas in bulbar-onset ALS, symptoms typically spread to the arms before the legs.Disorder progression tends to be slower in patients who are younger than 40 at onset,[19][20]are mildly obese,[21]have disorder restricted primarily to one limb, and those with primarily upper motor neuron symptoms.[22]Conversely, progression is faster and prognosis poorer in people with bulbar-onset disorder, respiratory-onset disorder, and frontotemporal dementia.[22]TheCX3CR1allelicvariants have also been shown to have an effect on the disorder's progression and life expectancy.[23]Late stages[edit]Although respiratory support can ease problems with breathing and prolong survival, it does not affect the progression of ALS. Most people with ALS die from respiratory failure, usually within three to five years from the onset of symptoms. The median survival time from onset to death is around 39 months, and only 4% survive longer than 10 years.[24]GuitaristJason Beckerhas lived since 1989 with the disorder, while physicistStephen Hawkinghas survived for more than 50 years, but they are considered unusual cases.[25]Difficulty in chewing and swallowing makes eating very difficult and increases the risk of choking or of aspirating food into the lungs. In later stages of the disorder,aspiration pneumoniacan develop, and maintaining a healthy weight can become a significant problem that may require the insertion of a feeding tube. As the diaphragm andintercostal musclesof therib cagethat support breathing weaken, measures oflung functionsuch asvital capacityand inspiratory pressure diminish. In respiratory-onset ALS, this may occur before significant limb weakness is apparent. Most people with ALS die of respiratory failure orpneumonia.In late stages, theoculomotor nervethat controls the movements of the eye can be affected as can theextraocular muscles(EOMs). The eye movements remain unaffected largely until the later stages due to differences in the extraocular muscles compared to the skeletal muscles that are initially and readily affected. In the disease's final stages, a person's condition may resemblelocked-in syndrome.[26]Eye movement[edit]People with ALS may have difficulty in generating voluntaryfast movements of the eye.[27]The speed of eye movement is slower in people with ALS.[27]Problems in generatingsmooth pursuitand convergence movements have also been noted.[27]Testing thevestibulo-ocular reflexshould help in identifying these problems.[28]Theelectrooculography(EOG) technique measures theresting potentialof theretina. EOG findings in people with ALS show progressive changes that correlate with disorder progression, and provide a measurement for clinically evaluating the effects of disorder progression on oculomotor activity.[28]Additionally, EOG may allow earlier detection of problems with the eyes.The embryonic lineage ofEOMsdiffers from that ofsomite-derived muscles. EOMs are unique because they continuously remodel through life and maintain a population of activesatellite cellsduring aging.[29]EOMs have significantly more myogenic precursor cells than limb skeletal muscles.[29]Causes[edit]Genetics[edit]About 510% of cases are directly inherited from a person's parents.[5]Overall,first-degree relativesof an individual with ALS have a 1% risk of developing ALS.[30][31]A defect onchromosome 21, which codes forsuperoxide dismutase, is associated with about 20% of familial cases of ALS, or about 2% of ALS cases overall.[32][33][34]This mutation is believed to be transmitted in anautosomal dominantmanner, and has over a hundred different forms of mutation. The most common ALS-causing mutation is a mutantSOD1gene, seen in North America; this is characterized by an exceptionally rapid progression from onset to death. The most common mutation found in Scandinavian countries,D90A-SOD1, is more slowly progressive than typical ALS, and people with this form of the disorder survive for an average of 11 years.[35]In 2011, a genetic abnormality known as a hexanucleotide repeat was found in a region calledC9orf72, which is associated with ALS combined with frontotemporal dementia ALS-FTD,[36]and accounts for some 6% of cases of ALS among white Europeans.[37]The gene is also found in people ofFilipinodescent.[37]TheUBQLN2gene encodes production of the protein ubiquilin 2 in the cell, which is a member of the ubiquilin family and controls the degradation of ubiquitinated proteins. Mutations inUBQLN2interfere with protein degradation, leading to neurodegeneration and causing dominantly inherited, chromosome X-linked ALS and ALS/dementia.[38]To date, a number of genetic mutations have been associated with various types of ALS. The currently known associations are:TypeOMIMGeneLocusRemarks
ALS1105400SOD121q22.1The most common form of familial ALS
ALS2205100ALS22q33.1
ALS3606640?18q21
ALS4602433SETX9q34.13
ALS5602099?15q15.1q21.1Juvenile onset
ALS6608030FUS16p11.2
ALS7608031?20p13
ALS8608627VAPB20q13.3
ALS9611895ANG14q11.2
ALS10612069TARDBP1p36.2
ALS11612577FIG46q21
ALS12613435OPTN10p13
ALS13183090ATXN212q24.12
ALS14613954VCP9p13.3Recent new study shows strong link in ALS mechanism[15][39]
ALS15300857UBQLN2Xp11.23p11.1Described in one family[40]
ALS16614373SIGMAR19p13.3Juvenile onset, very rare, described only in one family[41]
ALS17614696CHMP2B3p11Very rare, reported only in a handful of people
ALS18614808PFN117p13.3Very rare, described only in a handful of Chinese families[42]
ALS19615515ERBB42q34Very rare, as of late 2013 described only in four people[43]
ALS20615426HNRNPA112q13Very rare, as of late 2013 described only in two people[44]
ALS-FTD105550C9orf729p21.2Accounts for around 6% of ALS cases among white Europeans
SOD1[edit]In 1993, scientists discovered that mutations in the gene (SOD1) that produces theCu-Znsuperoxide dismutase(SOD1) enzyme were associated with around 20% of familial ALS. This enzyme is a powerfulantioxidantthat protects the body from damage caused bysuperoxide, a toxic free radical generated in the mitochondria.Free radicalsare highly reactive molecules produced by cells during normalmetabolism. Free radicals can accumulate and cause damage to DNA and proteins within cells. To date, over 110 different mutations inSOD1have been linked with the disorder, some of which (such asH46R) have a very long clinical course, while others, such asA4V, are exceptionally aggressive. When the defenses against oxidative stress fail, programmed cell death (apoptosis) is upregulated.A defect in SOD1 could be a loss or gain of function. A loss of SOD1 function could lead to an accumulation of free radicals. A gain of SOD1 function could be toxic in other ways.[45][46]Studies involvingtransgenicmice have yielded several theories about the role ofSOD1in mutant SOD1 familial amyotrophic lateral sclerosis. Mice lacking theSOD1gene entirely do not customarily develop ALS, although they do exhibit an acceleration of age-related muscle atrophy (sarcopenia) and a shortened lifespan. This indicates the toxic properties of the mutantSOD1are a result of a gain in function rather than a loss of normal function. In addition, aggregation of proteins has been found to be a common pathological feature of both familial and sporadic ALS (proteopathy). Interestingly, in mutantSOD1mice (most commonly, theG93Amutant), aggregates (misfolded protein accumulations) of mutantSOD1were found only in diseased tissues, and greater amounts were detected during motor neuron degeneration.[47]Aggregate accumulation of mutantSOD1is suspected to play a role in disrupting cellular functions by damagingmitochondria,proteasomes, protein foldingchaperones, or other proteins.[48]Any such disruption, if proven, would lend significant credibility to the theory that aggregates are involved in mutantSOD1toxicity. Critics have noted that in humans,SOD1mutations cause only 2% or so of overall cases and the etiological mechanisms may be distinct from those responsible for the sporadic form of the disease. To date, the ALS-SOD1 mice remain the best model of the disease for preclinical studies, but it is hoped that more useful models will be developed.An online database is available which was designed to provide both thescientific communityand the wider public with up-to-date information on ALS genetics. This is known as ALSOD website originally designed for theSOD1gene in 1999, but since upgraded to include over 40 ALS-related genes.Other factors[edit]Where no family history of the disease is presenti.e., in around 90% of cases no cause is known for ALS. Possible associations for which evidence is inconclusive include head trauma, military service, frequent drug use, and participation in contact sports.[medical citation needed]Studies also have focused on the role ofglutamatein motor neuron degeneration. Glutamate is one of theneurotransmittersin the brain. Scientists have found, compared with healthy people, people with ALS have higher levels of glutamate in theirserumand spinal fluid.[33]Riluzoleis currently the only FDA-approved drug for ALS and targets glutamate transporters. It only has a modest effect on survival, however, suggesting that excess glutamate is not the sole cause of the disease.Certain studies suggested a link between sporadic ALS, specifically in athletes, and a diet enriched withbranched-chain amino acids, a common dietary supplement among athletes, which cause cell hyperexcitability resembling that usually observed in people with ALS. The proposed underlying mechanism is that cell hyperexcitability results in increased calcium absorption by the cell, and thus brings about cell death of neuronal cells, which have particularly low calcium buffering capabilities.[49][50]Some evidence supports superoxide dismutase 1 (SOD1) protein misfolding propagates between molecules in a similar fashion toprions.[51]Similarly, it has been proposed that incorporation of the cyanobacterial toxin -methylamino-l-alanine (BMAA) leads to anotherprion-like protein misfolding propagation.[52][53]Another very common factor associated with ALS is alesionto the motor system in areas such as the frontotemporal lobes.[54]Lesions in these areas often show signs of early deficit, which can be used to predict the loss ofmotor function, and result in the spread of ALS.[54]The mechanisms of ALS are present long before any signs or symptoms become apparent.[55]Before any muscular atrophy becomes apparent during ALS, roughly one-third of themotor neuronsmust be destroyed.[55]Many other potential risk factors including chemical exposure, electromagnetic field exposure, occupation, physical trauma, and electric shock, have been investigated, but are without consistent findings.[56]Pathophysiology[edit]The defining feature of ALS is the death of bothupperandlower motor neuronsin the motor cortex of the brain, the brain stem, and the spinal cord. Prior to their destruction, motor neurons develop protein-richinclusionsin their cell bodies andaxons. This may be partly due to defects in protein degradation.[57]These inclusions often containubiquitin, and generally incorporate one of the ALS-associated proteins: SOD1,TAR DNA binding protein(TDP-43, or TARDBP), and/orFUS.[58]Skeletal motor units[edit]Despite sharing fixed sequences of recruitment, extraocular muscles (EOMs) and skeletal muscles exhibit different characteristics. The following are characteristics of EOMs that differ from skeletal motor units.[59] One neural fiber connects with only one or two muscle fibers No ocularstretch reflexes, despite being rich inmuscle spindles No recurrent inhibition No special fast-twitch or slow-twitch muscles All eye motor neurons participate equally in all types of eye movementsnot specialized for saccades or smooth pursuitDifferences are also noted between healthy and affected EOMs. EOMs from postmortem donors preserved theircytoarchitecture, as compared to limb muscles. Healthy EOMs consist of a central global layer (GL) facing the globe and a thin orbital layer (OL) facing the walls of the orbit.[60]EOMs affected by ALS preserve the GL and OL organization.[60]EOMs possess the neurotrophic factorsbrain-derived neurotrophic factor(BDNF) andglial cell line-derived neurotrophic factor(GDNF), and these neuroprotective factors are also preserved in EOMs affected by ALS.[60]Lamininis a structural protein typically found in theneuromuscular junction(NMJ). Ln4 is a laminin isoform that is a hallmark of skeletal muscle NMJs.[61]People with ALS showed preserved Ln4 expression in EOM NMJs, but this expression was non-existent in limb muscle NMJs from the same people.[61]Preservation of laminin expression may play a role in preserving EOM integrity in people with ALS. People with sporadic ALS (sALS) have increased levels of intracelluar calcium, causing increasedneurotransmitterrelease.[62]Passive transfer of sera from people with sALS increases spontaneous transmitter release in spinal, but not EOM terminals;[62]therefore, EOMs are assumed to be resistant to changes in physiologic conditions typically found in ALS.However, some effects of the disorder were noted. EOMs affected by ALS had a larger variation in fiber size compared to those in age-matched healthy controls.[60]EOMs exhibited both clustered and scattered atrophic andhypertrophicfibers that are characteristic of disorder, but these muscles showed significantly less damage compared to limb muscles from the same donors.[60]These EOMs also showed an increase inconnective tissueand areas of fatty replacement in compensation of fiber loss and atrophy.[60]Ophthalmoplegia, a loss of neurons in and around the ocular motor nuclei, has been noted in ALS patients.[27]Additionally,myosin heavy chaincontent of the EOM fibers was altered, with a loss of normal expression of MyHCslow tonic in the GL and the OL did not contain MyHCemb, which is normally expressed in this layer.[60]This change may represent a change in innervation pattern that may include reinnervation by a different type of motor neuron or loss of multiple innervations. Changes in MyHCslow and MyHCemb are the only fiber changes seen in EOMs, leaving the EOM fiber composition relatively normal.[60]Because EOMs are normally highly innervated, any denervation is compensated for by neighbouring axons which preserve function.[60]Lactate and cinnamate[edit]Lactic acidis an end product ofglycolysisand is known to cause muscle fatigue.Lactate dehydrogenase(LDH) enzyme exerts its effects bidirectionally and is able to oxidize lactate intopyruvateso it can be used in theKrebs cycle. In EOM, lactate sustains muscle contraction during increased activity levels. EOMs that have high LDH activity are thought to be resistant to ALS.[63]Cinnamateis a blocker of lactate transport and exogenous lactate on fatigue resistance. Cinnamate is able to cause fatigue in EOM, while decreasing EOM endurance and residual force; however, cinnamate has no effect on theextensor digitorum longus musclein the leg.[63]In contrast, replacingglucosewith exogenous lactate increases fatiguability of EDL muscles but not EOMs.[63]Fatiguability in EOMs was only found when a combination of exogenous lactacte plus cinnamate replaced glucose.[63]Diagnosis[edit]
MRI (axialFLAIR) demonstrates increasedT2signal within theposterior part of the internal capsule, consistent with the diagnosis of ALS.No test can provide a definite diagnosis of ALS, although the presence of upper and lower motor neuron signs in a single limb is strongly suggestive.[4]Instead, the diagnosis of ALS is primarily based on the symptoms and signs thephysicianobserves in the person and a series of tests to rule out other diseases.[4]Physicians obtain the person's fullmedical historyand usually conduct a neurologic examination at regular intervals to assess whether symptoms such as muscle weakness, atrophy of muscles,hyperreflexia, and spasticity are worsening.[4]Because symptoms of ALS can be similar to those of a wide variety of other, more treatable diseases or disorders, appropriate tests must be conducted to exclude the possibility of other conditions.[4]One of these tests iselectromyography(EMG), a special recording technique that detects electrical activity in muscles.[4]Certain EMG findings can support the diagnosis of ALS.[4]Another common test measuresnerve conduction velocity(NCV).[4]Specific abnormalities in the NCV results may suggest, for example, that the patient has a form ofperipheral neuropathy(damage to peripheral nerves) ormyopathy(muscle disease) rather than ALS. While amagnetic resonance imaging(MRI) is often normal in people with ALS, they can reveal evidence of other problems that may be causing the symptoms, such as a spinal cord tumor,multiple sclerosis, aherniateddisk in the neck,syringomyelia, or cervicalspondylosis.[4]Based on the person's symptoms and findings from the examination and from these tests, the physician may order tests on blood andurinesamples to eliminate the possibility of other diseases, as well as routine laboratory tests.[4]In some cases, for example, if a physician suspects the person may have a myopathy rather than ALS, a muscle biopsy may be performed.[4]Viralinfectious diseasessuch as human immunodeficiency virus (HIV), human T-cell leukaemia virus (HTLV),Lyme disease,[64]syphilis[65]andtick-borne encephalitis[66]can in some cases cause ALS-like symptoms.[4]Neurological disorders such as multiple sclerosis,post-polio syndrome,multifocal motor neuropathy,CIDP,spinal muscular atrophy, andspinal and bulbar muscular atrophycan also mimic certain aspects of the disease and should be considered.[4]ALS must be differentiated from the "ALS mimic syndromes" which are unrelated disorders that may have a similar presentation and clinical features to ALS or its variants.[67]Because of the prognosis carried by this diagnosis and the variety of diseases or disorders that can resemble ALS in the early stages of the disease, patients should always obtain a specialist neurological opinion, so alternative diagnoses are clinically ruled out.However, most cases of ALS are readily diagnosed and the error rate of diagnosis in large ALS clinics is less than 10%.[68][69]In one study, 190 patients who met the MND/ALS diagnostic criteria, complemented with laboratory research in compliance with both research protocols and regular monitoring. Thirty of these patients (16%) had their diagnosis completely changed during the clinical observation development period.[70]In the same study, three patients had a false negative diagnosis,myasthenia gravis(MG), an autoimmune disease. MG can mimic ALS and other neurological disorders leading to a delay in diagnosis and treatment. MG is eminently treatable; ALS is not.[71]Myasthenic syndrome, also known as Lambert-Eaton syndrome, can mimic ALS and its initial presentation can be similar to that of MG.[72][73]Management[edit]Management of ALS attempts to relieve symptoms and extend life expectancy. This supportive care is best provided by multidisciplinary teams of health care professionals working with the person and their caregivers to keep them as mobile and comfortable as possible.Medications[edit]Riluzole(Rilutek) has been found to modestly improve survival.[74]It lengthens survival by several months, and may have a greater survival benefit for those with abulbaronset. It also extends the time before a person needs ventilation support. People taking it must be monitored for liver damage (occurring in about 10% of people taking the drug).[75]It is approved byFood and Drug Administration(US) and recommended by theNational Institute for Clinical Excellence(UK). Riluzole does not reverse damage already done to motor neurons.[76]Other medications may be used to help reduce fatigue, ease muscle cramps, control spasticity, and reduce excess saliva andphlegm. Drugs also are available to help patients with pain, depression, sleep disturbances, dysphagia, and constipation.Baclofenanddiazepamare often prescribed to control the spasticity caused by ALS, andtrihexyphenidyloramitriptylinemay be prescribed when people with ALS begin having trouble swallowing their saliva.[13]Breathing support[edit]When the muscles that assist in breathing weaken, use of ventilatory assistance (intermittent positive pressure ventilation,bilevel positive airway pressure(BiPAP), orbiphasic cuirass ventilation(BCV) may be used to aid breathing. Such devices artificially inflate the person's lungs from various external sources that are applied directly to the face or body. When muscles are no longer able to maintain oxygen and carbon dioxide levels, these devices may be used full-time. BCV has the added advantage of being able to assist in clearing secretions by using high-frequency oscillations followed by several positive expiratory breaths.[77]People may eventually consider forms of mechanical ventilation (respirators) in which a machine inflates and deflates the lungs. To be effective, this may require a tube that passes from the nose or mouth to the windpipe (trachea) and for long-term use, an operation such as atracheotomy, in which a plasticbreathing tubeis inserted directly in the person's windpipe through an opening in the neck.Persons and their families should consider several factors when deciding whether and when to use one of these options. Ventilation devices differ in their effect on the person's quality of life and in cost. Although ventilation support can ease problems with breathing and prolong survival, it does not affect the progression of ALS. Patients need to be fully informed about these considerations and the long-term effects of life without movement before they make decisions about ventilation support and have deep discussions on quality of life. Some persons under long-term tracheotomy intermittent positive pressure ventilation with deflated cuffs or cuffless tracheotomy tubes (leak ventilation) are able to speak, provided their bulbar muscles are strong enough, though in all cases speech will be lost as the disease progresses. This technique preserves speech in some persons with long-term mechanical ventilation. Other persons may be able to use a speaking valve such as a Passey-Muir speaking valve with the assistance and guidance of a speech-language pathologist.External ventilation machines that use the ventilation mode of BiPAP are frequently used to support breathing, initially at night, and later during the daytime, as well. The use of BPAP (more often referred to as noninvasive ventilation, NIV) is only a temporary remedy, however, and long before BPAP stops being effective, persons should decide whether to have atracheotomyand long-term mechanical ventilation. At this point, some persons choosepalliative hospice care.Therapy[edit]Physical therapyplays a large role in rehabilitation for individuals with ALS. Specifically, physical and occupational therapists can set goals and promote benefits for individuals with ALS by delaying loss of strength, maintaining endurance, limiting pain, preventing complications, and promoting functional independence.[78]Occupational therapy and special equipment such asassistive technologycan also enhance patients' independence and safety throughout the course of ALS. Gentle, low-impactaerobic exercisesuch as performing activities of daily living, walking, swimming, andstationary bicyclingcan strengthen unaffected muscles, improve cardiovascular health, and help patients fight fatigue and depression. Range of motion and stretching exercises can help prevent painful spasticity and shortening (contracture) of muscles. Physical and occupational therapists can recommend exercises that provide these benefits without overworking muscles. They can suggest devices such as ramps, braces, walkers, bathroom equipment (shower chairs, toilet risers, etc.), and wheelchairs that help patients remain mobile. Occupational therapists can provide or recommend equipment and adaptations to enable people to retain as much safety and independence in activities of daily living as possible.ALS patients who have difficulty speaking may benefit from working with aspeech-language pathologist. These health professionals can teach patients adaptive strategies such as techniques to help them speak louder and more clearly. As ALS progresses, speech-language pathologists can recommend the use ofaugmentative and alternative communicationsuch as voice amplifiers, speech-generating devices (or voice output communication devices) and/or low tech communication techniques such asalphabet boardsor yes/no signals.Nutrition[edit]Patients and caregivers can learn from dieticians how to plan and prepare numerous small meals throughout the day that provide enough calories, fiber, and fluid and how to avoid foods that are difficult to swallow. Patients may begin using suction devices to remove excess fluids or saliva and prevent choking. Occupational therapists can assist with recommendations for adaptive equipment to ease the physical task of self-feeding. Speech-language pathologists make food choice recommendations that are more conducive to their unique deficits and abilities. When patients can no longer get enough nourishment from eating, doctors may advise inserting afeeding tubeinto the stomach. The use of a feeding tube also reduces the risk of choking and pneumonia that can result from inhaling liquids into the lungs. The tube is not painful and does not prevent patients from eating food orally if they wish.Researchers have stated, "ALS patients have a chronically deficient intake of energy and recommended augmentation of energy intake"[79]and have a severe loss of appetite.[80]Both animal[81]and human research[79][unreliable medical source?][82][unreliable medical source?]suggest that ALS patients should be encouraged to consume as many calories as possible and not to restrict their caloric intake. As of 2012, "a lack of robust evidence for interventions" remained for the management of weight loss.[83]Palliative care[edit]Social workersand home care andhospicenurses help people with ALS, their families, and caregivers with the medical, emotional, and financial challenges of coping, particularly during the final stages of the disease. Social workers provide support such as assistance in obtaining financial aid, arranging durablepower of attorney, preparing aliving will, and finding support groups for patients and caregivers. Home nurses are available not only to provide medical care, but also to teach caregivers about tasks such as maintaining respirators, giving feedings, and moving patients to avoid painful skin problems and contractures. Home hospice nurses work in consultation with physicians to ensure proper medication, pain control, and other care affecting the quality of life of patients who wish to remain at home. The home hospice team can also counsel patients and caregivers about end-of-life issues.Epidemiology[edit]In much of the world, rates of ALS are unknown.[5]In Europe, the disease affects about 2.2 people per 100,000 per year.[5]In the United States, more than 5,600 are diagnosed every year, and up to 30,000 Americans are currently affected. ALS is responsible for two deaths per 100,000 people per year.[84]ALS is classified as a rare disease, but is the most common motor neuron disease. People of all races and ethnic backgrounds are affected. One or two of 100,000 people develop ALS each year.[85]Amyotrophic lateral sclerosis affects around 30,000 Americans.[86]ALS cases are estimated at 1.24.0 per 100,000 individuals in Caucasian populations with a lower rate in other ethnic populations.[87]Filipinosare second to Caucasians in terms of ALS prevalence with 1.1-2.8 per 100,000 individuals.[86]Reports have been made of several "clusters" including threeAmerican footballplayers from theSan Francisco 49ers, more than 50association footballplayers in Italy,[88]three association football-playing friends in the south of England,[89]and conjugal (husband and wife) cases in the south of France.[90][91][92][93][94]Although many authors consider ALS to be caused by a combination of genetic and environmental risk factors, so far the latter have not been firmly identified, other than a higher risk with increasing age.History[edit]Descriptions of the disease date back to at least 1824 byCharles Bell.[10]It became well known in the United States when it affected famous baseball playerLou Gehrig,[95]and later when theice bucket challengebecame popular in 2014.[96]English scientistAugustus Wallerdescribed the appearance of shriveled nerve fibers in 1850. In 1869, the connection between the symptoms and the underlying neurological problems were first described byJean-Martin Charcot, who introduced the termamyotrophic lateral sclerosisin his 1874 paper.[10]In 1881, the article was translated into English and published in a three-volume edition ofLectures on the Diseases of the Nervous System.ALS became acause clbrein the United States in 1939 when baseball legendLou Gehrig's career, and two years later, his life, was ended by the disease.[95]In the 1950s, an ALSepidemicoccurred among theChamorro peopleonGuam.By 1991, researchers had linked chromosome 21 to familial ALS (FALS). In 1993, theSOD1gene on chromosome 21 was found to play a role in some cases of FALS. In 1996, riluzole became the first FDA-approved drug for ALS.In 1998, the El Escorial criteria were developed as the standard for classifying ALS patient in clinical research. The next year, the revised ALS Functional Rating Scale was published and soon becomes a gold standard for rating the declines in ALS patient in clinical research. Noncoding repeat expansions inC9ORF72were found to be a major cause of ALS and frontotemporal dementia in 2011.Etymology[edit]Amyotrophic comes from theGreekwordamyotrophia:a-means "no",myorefers to "muscle", andtrophiameans "nourishment";amyotrophiatherefore means "no muscle nourishment," which describes the characteristicatrophyof the sufferer's disused muscle tissue. Lateral identifies the areas in a person's spinal cord where affected portions of the nerve cells are located. Degeneration in this area leads to scarring or hardening ("sclerosis").Society and culture[edit]See also:Category:People with motor neurone diseaseIn August 2014, a challenge wentviralonline which was commonly known as the "ALS Ice Bucket Challenge".[96]Contestants fill a bucket full of ice and water, then state who nominated them to do the challenge, and nominate three other individuals of their choice to take part in it. The contestants then dump the buckets of ice and water onto themselves. However, it can be done in a different order. The contestants then donate at least US$10 (or a similar amount in their local currency) to ALS research at theALS Association, orMotor Neurone Disease Associationin the UK. Any contestants who refuse to have the ice and water dumped on them are expected to donate at least US$100 to ALS research. As of August 25, the Ice Bucket Challenge raised $79.7 million for the ALS Association, compared to $2.5 million raised over the same period in 2013. Many celebrities have taken part in the challenge.[97]ALS is the central topic of the 2014 movieYou're Not You, directed byGeorge C. Wolfe, withHilary Swank,Emmy RossumandJosh Duhamelplaying the main characters.[98]Research[edit]A number ofclinical trialsare underway globally for ALS; a comprehensive listing of trials in the US can be found atClinicalTrials.gov. The world's largest genetic study, calledproject MinE, initiated by two people with ALS is going on currently. It is a crowdfunded research project with many countries involved to discover more genes.[99]A phase-II trial on tirasemtiv has been completed with a follow-on phase-IIb study in progress under the name "BENEFIT-ALS". Results of the first study are available here.[100][unreliable medical source?][101][verification needed]The current trial is an international, placebo-controlled, multiple-center study on 680 participants. This makes it one of the largest studies to date. A phase-II trial onozanezumabis in progress. It is a large multiple-site international research project sponsored byGlaxoSmithKline.A phase-II clinical trial is being conducted by BrainStorm Cell Therapeutics at theHadassah Medical Centerin Israel and interim results "demonstrated a tendency toward stabilization in some parameters in the ALS Functional Rating Scale."[102][103]People in the trial have bone marrow stem cells removed and differentiated in a clean room into cells that express neurotropic factors. The cells are injected back into the same person by intrathecal and intramuscular injections. A second phase-II trial is expected to open in the United States at several institutions including theMayo Clinic.[104]References[edit]1. ^Jump up to:abKelly, Evelyn B. (2013).Encyclopedia of human genetics and disease. Santa Barbara, Calif.: Greenwood. pp.7980.ISBN978-0-313-38713-5.2. Jump up^"Motor neurone disease".http://www.nhs.uk/. Retrieved2 January2015.3. Jump up^Ellison, edited by Seth Love, David N. Louis, David W. (2008).Greenfield's neuropathology(8th ed. ed.). London: Hodder Arnold. p.947.ISBN978-0-340-90681-1.4. ^Jump up to:abcdefghijklmnopq"Motor Neuron Diseases Fact Sheet". National Institute of Neurological Disorders and Stroke (NINDS). Retrieved7 November2010.5. ^Jump up to:abcdefgKiernan, MC; Vucic, S; Cheah, BC; Turner, MR; Eisen, A; Hardiman, O; Burrell, JR; Zoing, MC (12 March 2011). "Amyotrophic lateral sclerosis.".Lancet377(9769): 94255.doi:10.1016/s0140-6736(10)61156-7.PMID21296405.6. Jump up^Miller, RG; Mitchell, JD; Moore, DH (14 March 2012). "Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND).".The Cochrane database of systematic reviews3: CD001447.doi:10.1002/14651858.CD001447.pub3.PMID22419278.7. Jump up^McDermott, CJ; Shaw, PJ (22 March 2008). "Diagnosis and management of motor neurone disease.".BMJ (Clinical research ed.)336(7645): 65862.doi:10.1136/bmj.39493.511759.be.PMID18356234.8. Jump up^Malamut, edited by Joseph I. Sirven, Barbara L. (2008).Clinical neurology of the older adult(2nd ed. ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p.421.ISBN978-0-7817-6947-1.9. Jump up^"Epidemiology of Sporadic ALS".http://aces.stanford.edu/. Retrieved2 January2015.10. ^Jump up to:abcdRowland LP (March 2001)."How amyotrophic lateral sclerosis got its name: the clinical-pathologic genius of Jean-Martin Charcot".Arch. Neurol.58(3): 5125.doi:10.1001/archneur.58.3.512.PMID11255459.11. Jump up^Youngson, David B. Jacoby, Robert M. (2004).Encyclopedia of family health(3rd ed. ed.). Tarrytown, NY: Marshall Cavendish. p.1256.ISBN978-0-7614-7486-9.12. Jump up^Song, P (August 2014). "The Ice Bucket Challenge: The public sector should get ready to promptly promote the sustained development of a system of medical care for and research into rare diseases.".Intractable & rare diseases research3(3): 946.doi:10.5582/irdr.2014.01015.PMID25364651.13. ^Jump up to:abDugdale DC, Hoch DB, Zieve D (27 August 2010)."Amyotrophic lateral sclerosis".A.D.A.M. Medical Encyclopedia.14. Jump up^Phukan J, Pender NP, Hardiman O (2007)."Cognitive impairment in amyotrophic lateral sclerosis".Lancet Neurol6(11): 9941003.doi:10.1016/S1474-4422(07)70265-X.PMID17945153.15. ^Jump up to:abJohnson JO, Mandrioli J, Benatar M, Abramzon Y, Van Deerlin VM, Trojanowski JQ, Gibbs JR, Brunetti M, Gronka S, Wuu J, Ding J, McCluskey L, Martinez-Lage M, Falcone D, Hernandez DG, Arepalli S, Chong S, Schymick JC, Rothstein J, Landi F, Wang YD, Calvo A, Mora G, Sabatelli M, Monsurr MR, Battistini S, Salvi F, Spataro R, Sola P, Borghero G, Galassi G, Scholz SW, Taylor JP, Restagno G, Chi A, Traynor BJ (2010)."Exome Sequencing Reveals VCP Mutations as a Cause of Familial ALS".Neuron68(5): 857864.doi:10.1016/j.neuron.2010.11.036.PMC3032425.PMID21145000.16. Jump up^http://www.ninds.nih.gov/disorders/amyotrophiclateralsclerosis/17. Jump up^Amyotrophic Lateral Sclerosis (ALS) Fact Sheet18. Jump up^Castrillo-Viguera C, Grasso DL, Simpson E, Shefner J, Cudkowicz ME (2010). "Clinical significance in the change of decline in ALSFRS-R".Amyotroph Lateral Scler(Journal Article)11(12): 17880.doi:10.3109/17482960903093710.PMID19634063.19. Jump up^Sabatelli M, Madia F, Conte A, Luigetti M, Zollino M, Mancuso I, Lo Monaco M, Lippi G, Tonali P (16 September 2008). "Natural history of young-adult amyotrophic lateral sclerosis".Neurology71(12): 87681.doi:10.1212/01.wnl.0000312378.94737.45.PMID18596241.20. Jump up^[Survival in amyotrophic lateral s... [Srp Arh Celok Lek. 1997 Jan-Feb] - PubMed NCBI21. Jump up^Mild Obesity Appears to Improve Survival in ALS Patients | HMS22. ^Jump up to:abChi A, Calvo A, Moglia C, Mazzini L, Mora G (2011). "Phenotypic heterogeneity of amyotrophic lateral sclerosis: A population based study".Journal of Neurology, Neurosurgery & Psychiatry82(7): 740746.doi:10.1136/jnnp.2010.235952.PMID21402743.23. Jump up^Lopez-Lopez A, Gamez J, Syriani E, Morales M, Salvado M, Rodrguez MJ, Mahy N, Vidal-Taboada JM (2014)."CX3CR1 Is a Modifying Gene of Survival and Progression in Amyotrophic Lateral Sclerosis".PLoS ONE9(5): e96528.doi:10.1371/journal.pone.0096528.PMC4013026.PMID24806473.24. Jump up^Turner MR, Parton MJ, Shaw CE, Leigh PN, Al-Chalabi A (2003)."Prolonged survival in motor neuron disease: a descriptive study of the King's database 19902002".J Neurol Neurosurg Psychiatry74(7): 995997.doi:10.1136/jnnp.74.7.995.PMC1738535.PMID12810805.25. Jump up^"Stephen Hawking serves as role model for ALS patients". CNN. 2009-04-20.26. Jump up^James L. Bernat: Ethical Issues in Neurology, p. 336http://books.google.pl/books?id=o732GWGjPQ4C&pg=PA33627. ^Jump up to:abcdCohen B, Caroscio J. Eye movements in amyotrophic lateral sclerosis. J Neural Transm Suppl. 1983;19:305-1528. ^Jump up to:abPalmowski A, Jost WH, Prudlo J, Osterhage J, Ksmann B, Schimrigk K, Ruprecht KW (1995). "Eye movement in amyotrophic lateral sclerosis: a longitudinal study".Ger J Ophthalmol4(6): 35562.PMID8751101.29. ^Jump up to:abKallestad KM, Hebert SL, McDonald AA, Daniel ML, Cu SR, McLoon LK (2011)."Sparing of extraocular muscle in aging and muscular dystrophies: a myogenic precursor cell hypothesis".Exp. Cell Res.317(6): 87385.doi:10.1016/j.yexcr.2011.01.018.PMC3072110.PMID21277300.30. Jump up^Cookson, Mark R.; Wingo, Thomas S.; Cutler, David J.; Yarab, Nicole; Kelly, Crystal M.; Glass, Jonathan D. (2011). "The Heritability of Amyotrophic Lateral Sclerosis in a Clinically Ascertained United States Research Registry".PLoS ONE6(11): e27985.doi:10.1371/journal.pone.0027985.ISSN1932-6203.31. Jump up^Sontheimer, Harald (2015).Diseases of the Nervous System. Academic Press. p.170.ISBN978-0-12-800403-6. Retrieved2015-05-02.32. Jump up^Conwit RA (December 2006). "Preventing familial ALS: A clinical trial may be feasible but is an efficacy trial warranted?".Journal of the Neurological Sciences251(12): 12.doi:10.1016/j.jns.2006.07.009.ISSN0022-510X.PMID17070848.33. ^Jump up to:abAl-Chalabi A, Leigh PN (August 2000). "Recent advances in amyotrophic lateral sclerosis".Current Opinion in Neurology13(4): 397405.doi:10.1097/00019052-200008000-00006.ISSN1473-6551.PMID10970056.34. Jump up^Battistini S, Ricci C, Lotti EM, Benigni M, Gagliardi S, Zucco R, Bondavalli M, Marcello N, Ceroni M, Cereda C (June 2010). "Severe familial ALS with a novel exon 4 mutation (L106F) in the SOD1 gene".Journal of the Neurological Sciences293(1): 112115.doi:10.1016/j.jns.2010.03.009.PMID20385392.35. Jump up^Andersen PM, Forsgren L, Binzer M, Nilsson P, Ala-Hurula V, Kernen ML, Bergmark L, Saarinen A, Haltia T, Tarvainen I, Kinnunen E, Udd B, Marklund SL (1996). "Autosomal recessive adult-onset amyotrophic lateral sclerosis associated with homozygosity for Asp90Ala CuZn-superoxide dismutase mutation, A clinical and genealogical study of 36 patients".Brain119(4): 11531172.doi:10.1093/brain/119.4.1153.PMID8813280.36. Jump up^DeJesus-Hernandez M, Mackenzie IR, Boeve BF, Boxer AL, Baker M, Rutherford NJ, Nicholson AM, Finch NA, Flynn H, Adamson J, Kouri N, Wojtas A, Sengdy P, Hsiung GY, Karydas A, Seeley WW, Josephs KA, Coppola G, Geschwind DH, Wszolek ZK, Feldman H, Knopman DS, Petersen RC, Miller BL, Dickson DW, Boylan KB, Graff-Radford NR, Rademakers R (2011)."Expanded GGGGCC Hexanucleotide Repeat in Noncoding Region of C9ORF72 Causes Chromosome 9p-Linked FTD and ALS"(PDF).Neuron72(2): 24556.doi:10.1016/j.neuron.2011.09.011.PMC3202986.PMID21944778.37. ^Jump up to:abMajounie E, Renton AE, Mok K, Dopper EG, Waite A, Rollinson S, Chi A, Restagno G, Nicolaou N, Simon-Sanchez J, van Swieten JC, Abramzon Y, Johnson JO, Sendtner M, Pamphlett R, Orrell RW, Mead S, Sidle KC, Houlden H, Rohrer JD, Morrison KE, Pall H, Talbot K, Ansorge O, Hernandez DG, Arepalli S, Sabatelli M, Mora G, Corbo M, Giannini F, Calvo A, Englund E, Borghero G, Floris GL, Remes AM, Laaksovirta H, McCluskey L, Trojanowski JQ, Van Deerlin VM, Schellenberg GD, Nalls MA, Drory VE, Lu CS, Yeh TH, Ishiura H, Takahashi Y, Tsuji S, Le Ber I, Brice A, Drepper C, Williams N, Kirby J, Shaw P, Hardy J, Tienari PJ, Heutink P, Morris HR, Pickering-Brown S, Traynor BJ (2012)."Frequency of the C9orf72 hexanucleotide repeat expansion in patients with amyotrophic lateral sclerosis and frontotemporal dementia: a cross-sectional study".Lancet Neurol11(4): 32330.doi:10.1016/S1474-4422(12)70043-1.PMC3322422.PMID22406228.38. Jump up^Han-Xiang Deng, Wenjie Chen, Seong-Tshool Hong,et al.(8 September 2011)."Mutations in UBQLN2 cause dominant X-linked juvenile and adult-onset ALS and ALS/dementia".Nature477(7363): 211215.doi:10.1038/nature10353.PMC3169705.PMID21857683.39. Jump up^Buchan JR, Kolaitis RM, Taylor JP, Parker R (20 June 2013)."Eukaryotic stress granules are cleared by autophagy and Cdc48/VCP function".Cell153(7): 146174.doi:10.1016/j.cell.2013.05.037.PMC3760148.PMID23791177.40. Jump up^Deng HX, Chen W, Hong ST, Boycott KM, Gorrie GH, Siddique N, Yang Y, Fecto F, Shi Y, Zhai H, Jiang H, Hirano M, Rampersaud E, Jansen GH, Donkervoort S, Bigio EH, Brooks BR, Ajroud K, Sufit RL, Haines JL, Mugnaini E, Pericak-Vance MA, Siddique T (2011)."Mutations in UBQLN2 cause dominant X-linked juvenile and adult-onset ALS and ALS/dementia".Nature477(7363): 211215.doi:10.1038/nature10353.PMC3169705.PMID21857683.41. Jump up^Al-Saif A, Al-Mohanna F, Bohlega S (2011). "A mutation in sigma-1 receptor causes juvenile amyotrophic lateral sclerosis".Annals of Neurology70(6): 913919.doi:10.1002/ana.22534.PMID21842496.42. Jump up^Wu CH, Fallini C, Ticozzi N, Keagle PJ, Sapp PC, Piotrowska K, Lowe P, Koppers M, McKenna-Yasek D, Baron DM, Kost JE, Gonzalez-Perez P, Fox AD, Adams J, Taroni F, Tiloca C, Leclerc AL, Chafe SC, Mangroo D, Moore MJ, Zitzewitz JA, Xu ZS, van den Berg LH, Glass JD, Siciliano G, Cirulli ET, Goldstein DB, Salachas F, Meininger V, Rossoll W, Ratti A, Gellera C, Bosco DA, Bassell GJ, Silani V, Drory VE, Brown RH, Landers JE (2012)."Mutations in the profilin 1 gene cause familial amyotrophic lateral sclerosis".Nature488(7412): 499503.doi:10.1038/nature11280.PMC3575525.PMID22801503.43. Jump up^Takahashi Y, Fukuda Y, Yoshimura J, Toyoda A, Kurppa K, Moritoyo H, Belzil VV, Dion PA, Higasa K, Doi K, Ishiura H, Mitsui J, Date H, Ahsan B, Matsukawa T, Ichikawa Y, Moritoyo T, Ikoma M, Hashimoto T, Kimura F, Murayama S, Onodera O, Nishizawa M, Yoshida M, Atsuta N, Sobue G, Fifita JA, Williams KL, Blair IP, Nicholson GA, Gonzalez-Perez P, Brown RH, Nomoto M, Elenius K, Rouleau GA, Fujiyama A, Morishita S, Goto J, Tsuji S (2013)."ERBB4 mutations that disrupt the neuregulin-ErbB4 pathway cause amyotrophic lateral sclerosis type 19".Am. J. Hum. Genet.93(5): 9005.doi:10.1016/j.ajhg.2013.09.008.PMC3824132.PMID24119685.44. Jump up^Kim HJ, Kim NC, Wang YD, Scarborough EA, Moore J, Diaz Z, MacLea KS, Freibaum B, Li S, Molliex A, Kanagaraj AP, Carter R, Boylan KB, Wojtas AM, Rademakers R, Pinkus JL, Greenberg SA, Trojanowski JQ, Traynor BJ, Smith BN, Topp S, Gkazi AS, Miller J, Shaw CE, Kottlors M, Kirschner J, Pestronk A, Li YR, Ford AF, Gitler AD, Benatar M, King OD, Kimonis VE, Ross ED, Weihl CC, Shorter J, Taylor JP (28 March 2013)."Mutations in the prion-like domains of hnRNPA2B1 and hnRNPA1 cause multisystem proteinopathy and ALS".Nature495(7442): 46773.doi:10.1038/nature11922.PMC3756911.PMID23455423.45. Jump up^Bruijn LI, Houseweart MK, Kato S, Anderson KL, Anderson SD, Ohama E, Reaume AG, Scott RW, Cleveland DW (1998). "Aggregation and motor neuron toxicity of an ALS-linked SOD1 mutant independent from wild-type SOD1".Science281(5384): 18514.doi:10.1126/science.281.5384.1851.PMID9743498.46. Jump up^Reaume AG, Elliott JL, Hoffman EK, Kowall NW, Ferrante RJ, Siwek DF, Wilcox HM, Flood DG, Beal MF, Brown RH, Scott RW, Snider WD (1996). "Motor neurons in Cu/Zn superoxide dismutase-deficient mice develop normally but exhibit enhanced cell death after axonal injury".Nat Genet13(1): 437.doi:10.1038/ng0596-43.PMID8673102.47. Jump up^Furukawa Y, Fu R, Deng HX, Siddique T, O'Halloran TV (2006)."Disulfide cross-linked protein represents a significant fraction of ALS-associated Cu, Zn-superoxide dismutase aggregates in spinal cords of model mice".Proc Natl Acad Sci USA103(18): 714853.doi:10.1073/pnas.0602048103.PMC1447524.PMID16636274.48. Jump up^Boille S, Vande Velde C, Cleveland DW (2006). "ALS: a disease of motor neurons and their nonneuronal neighbors".Neuron52(1): 3959.doi:10.1016/j.neuron.2006.09.018.PMID17015226.49. Jump up^Manuel M, Heckman CJ (March 2011)."Stronger is not always better: could a bodybuilding dietary supplement lead to ALS?".Exp Neurol(Review)228(1): 58.doi:10.1016/j.expneurol.2010.12.007.PMC3049458.PMID21167830.50. Jump up^Carunchio I, Curcio L, Pieri M, Pica F, Caioli S, Viscomi MT, Molinari M, Canu N, Bernardi G, Zona C (2010). "Increased levels of p70S6 phosphorylation in the G93A mouse model of amyotrophic lateral sclerosis and in valine-exposed cortical neurons in culture".Experimental Neurology226(1): 218230.doi:10.1016/j.expneurol.2010.08.033.PMID20832409.51. Jump up^Fernndez-Borges N, Eraa H, Elezgarai SR, Harrathi C, Gayosso M, Castilla J (25 September 2013)."Infectivity versus seeding in neurodegenerative diseases sharing a prion-like mechanism".Int J Cell Biol.2013: 583498.doi:10.1155/2013/583498.PMC3800648.PMID24187553.52. Jump up^Holtcamp, W. (2012)."The emerging science of BMAA: do cyanobacteria contribute to neurodegenerative disease?".Environmental health perspective120(3).doi:10.1289/ehp.120-a110.PMC3295368.PMID22382274.53. Jump up^Rodgers KJ (March 2014). "Non-protein amino acids and neurodegeneration: The enemy within".Experimental Neurology253: 192196.doi:10.1016/j.expneurol.2013.12.010.PMID24374297.54. ^Jump up to:abRosenbohm, A., Kassubek, J., Weydt, P., Marroquin, N., Volk, A., Kubisch, C., Huppertz, H., & Weber, M. (2014). Can lesions to the motor cortex induce amyotrophic lateral sclerosis? . J Neurol, 261, 283-290.55. ^Jump up to:abWalling A (1999). "Amyotrophic lateral sclerosis: Lou Gehrig's disease".American Family Physician59(6): 148996.56. Jump up^Sutedja NA, Fischer K, Veldink JH, van der Heijden GJ, Kromhout H, Heederik D, Huisman MH, Wokke JJ, van den Berg LH (2009). "What we truly know about occupation as a risk factor for ALS: a critical and systematic review".Amyotrophic Lateral Sclerosis10(56): 295301.doi:10.3109/17482960802430799.PMID19922116.57. Jump up^Deng HX, Chen W, Hong ST, Boycott KM, Gorrie GH, Siddique N, Yang Y, Fecto F, Shi Y, Zhai H, Jiang H, Hirano M, Rampersaud E, Jansen GH, Donkervoort S, Bigio EH, Brooks BR, Ajroud K, Sufit RL, Haines JL, Mugnaini E, Pericak-Vance MA, Siddique T (2011-08-21)."Mutations in UBQLN2 cause dominant X-linked juvenile and adult onset ALS and ALS/dementia".Nature477(7363): 2115.doi:10.1038/nature10353.PMC3169705.PMID21857683.58. Jump up^Deng HX, Zhai H, Bigio EH, Yan J, Fecto F, Ajroud K, Mishra M, Ajroud-Driss S, Heller S, Sufit R, Siddique N, Mugnaini E, Siddique T. (June 2010). "FUS-immunoreactive inclusions are a common feature in sporadic and non-SOD1 familial amyotrophic lateral sclerosis".Ann Neurol.67(6): 73948.doi:10.1002/ana.22051.PMID20517935.59. Jump up^Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science. McGraw-Hill; 200060. ^Jump up to:abcdefghiAhmadi M, Liu JX, Brnnstrm T, Andersen PM, Stl P, Pedrosa-Domellf F. Human extraocular muscles in ALS. Invest Ophthalmol Vis Sci. 2010;51(7):3494-50161. ^Jump up to:abLiu JX, Brnnstrm T, Andersen PM, Pedrosa-Domellf F. Different Impact of ALS on Laminin Isoforms in Human Extraocular Muscles Versus Limb Muscles. Invest Ophthalmol Vis Sci. 201162. ^Jump up to:abMosier DR, Sikls L, Appel SH. Resistance of extraocular motoneuron terminals to effects of amyotrophic lateral sclerosis sera. Neruology. 2000;54(1):252-563. ^Jump up to:abcdAndrade FH, McMullen CA (2006). "Lactate is a metabolic substrate that sustains extraocular muscle function".Pflugers Arch.452(1): 1028.doi:10.1007/s00424-005-0010-0.PMID16328456.64. Jump up^Hnsel Y, Ackerl M, Stanek G (1995). "ALS-like sequelae in chronic neuroborreliosis".Wien Med Wochenschr.145(78): 1868.PMID7610670.65. Jump up^el Alaoui-Faris M, Medejel A, al Zemmouri K, Yahyaoui M, Chkili T (1990). "Amyotrophic lateral sclerosis syndrome of syphilitic origin. 5 cases".Rev Neurol (Paris)146(1): 414.PMID2408129.66. Jump up^Umaneki KG, Dekonenko EP (1983). "Structure of progressive forms of tick-borne encephalitis".Zh Nevropatol Psikhiatr Im S S Korsakova.83(8): 11739.PMID6414202.67. Jump up^Silani V, Messina S, Poletti B, Morelli C, Doretti A, Ticozzi N, Maderna L (2011). "The diagnosis of Amyotrophic lateral sclerosis in 2010".Archives italiennes de biologie149(1): 527.doi:10.4449/aib.v149i1.1260.PMID21412713.68. Jump up^Eisen, A. (2002)."Amyotrophic lateral sclerosis: A review".BCMJ44(7): 362366.69. Jump up^Davenport RJ, Swingler RJ, Chancellor AM, Warlow CP (1996)."Avoiding false positive diagnoses of motor neuron disease: lessons from the Scottish Motor Neuron Disease Register".J. Neurol. Neurosurg. Psychiatr.60(2): 14751.doi:10.1136/jnnp.60.2.147.PMC1073793.PMID8708642.70. Jump up^Chieia MA, Oliveira AS, Silva HC, Gabbai AA (2010)."Amyotrophic lateral sclerosis: Considerations on diagnostic criteria"(PDF).Arquivos de Neuro-Psiquiatria68(6): 837842.doi:10.1590/S0004-282X2010000600002.PMID21243238.71. Jump up^Al-Asmi A, Nandhagopal R, Jacob PC, Gujjar A (2012)."Misdiagnosis of Myasthenia Gravis and Subsequent Clinical Implication: A case report and review of literature".Sultan Qaboos University medical journal12(1): 103108.doi:10.12816/0003095.PMC3286704.PMID22375266.72. Jump up^"Lambert-Eaton Myasthenic Syndrome (LEMS)". Misc.medscape.com. Retrieved18 April2013.73. Jump up^"LEMS.com, Lambert-Eaton Myasthenic Syndrome: About". Lems.com. Retrieved18 April2013.74. Jump up^Carlesi C, Pasquali L, Piazza S, Lo Gerfo A, Caldarazzo Ienco E, Alessi R, Fornai F, Siciliano G (March 2011). "Strategies for clinical approach to neurodegeneration in Amyotrophic lateral sclerosis".Archives italiennes de biologie149(1): 15167.doi:10.4449/aib.v149i1.1267.PMID21412722.75. Jump up^Miller RG, Mitchell JD, Lyon M, Moore DH (2007). Miller, Robert G, ed. "Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND)".Cochrane Database of Systematic Reviews(1): CD001447.doi:10.1002/14651858.CD001447.pub2.PMID17253460.76. Jump up^Russell P, Harrison R (2014)."What is amyotrophic lateral sclerosis".Clinical Pharmacist6(7).77. Jump up^Sviri S, Linton DM, van Heerden PV (Jun 2005). "Non-invasive Mechanical Ventilation Enhances Patient Autonomy in Decision-Making Regarding Chronic Ventilation".Critical Care and Resuscitation7(2): 116118.PMID16548804.78. Jump up^Lewis M, Rushanan S (2007). "The role of physical therapy and occupational therapy in the treatment of Amyotrophic Lateral Sclerosis".NeuroRehabilitation22(6): 451461.PMID18198431.79. ^Jump up to:abKasarskis EJ, Berryman S, Vanderleest JG, Schneider AR, McClain CJ (Jan 1996)."Nutritional status of patients with amyotrophic lateral sclerosis: relation to the proximity of death".Am J Clin Nutr.63(1): 1307.PMID8604660.80. Jump up^Holm T, Maier A, Wicks P, Lang D, Linke P, Mnch C, Steinfurth L, Meyer R, Meyer T (Apr 2013)."Severe Loss of Appetite in Amyotrophic Lateral Sclerosis Patients: Online Self-Assessment Study".Interact J Med Res2(1): e8.doi:10.2196/ijmr.2463.PMC3632382.PMID23608722.81. Jump up^Hamadeh MJ, Rodriguez MC, Kaczor JJ, Tarnopolsky MA (Feb 2005). "Caloric restriction transiently improves motor performance but hastens clinical onset of disease in the Cu/Zn-superoxide dismutase mutant G93A mouse".Muscle Nerve31(2): 21420.doi:10.1002/mus.20255.PMID15625688.82. Jump up^Slowie LA, Paige MS, Antel JP (Jul 1983). "Nutritional considerations in the management of patients with amyotrophic lateral sclerosis (ALS)".J Am Diet Assoc83(1): 447.PMID6863783.83. Jump up^Payne, C; Wiffen, PJ; Martin, S (18 January 2012). "Interventions for fatigue and weight loss in adults with advanced progressive illness.".The Cochrane database of systematic reviews1: CD008427.doi:10.1002/14651858.cd008427.pub2.PMID22258985.84. Jump up^ALS Association.Quick Facts About ALS & The ALS Association.85. Jump up^"ALS Topic Overview".Archivedfrom the original on 1 May 2008. Retrieved2008-05-01.86. ^Jump up to:abWalling AD (1999). "Amyotrophic lateral sclerosis: Lou Gehrig's disease".American Family Physician59(6): 14891496.PMID10193591.87. Jump up^Gordon, Paul. "Amyotrophic Lateral Sclerosis. Pathophysiology, Diagnosis and Management." CNS Drugs, 25.1 (2011):1-15.88. Jump up^"Sla, indagini nei club. Pesticidi nel mirino".Archivedfrom the original on 3 October 2008. Retrieved2008-10-02.89. Jump up^Wicks P, Abrahams S, Masi D, Hejda-Forde S, Leigh PN, Goldstein LH (2005). "The Prevalence of Depression and Anxiety in MND".Amyotrophic Lateral Sclerosis and Other Motor Neuron Disorders6(Supplement 1): 147.ISSN1466-0822.90. Jump up^Rachele MG, Mascia V, Tacconi P, Dessi N, Marrosu F, Giagheddu M (April 1998). "Conjugal amyotrophic lateral sclerosis: a report on a couple from Sardinia, Italy".Ital J Neurol Sci.19(2): 97100.doi:10.1007/BF02427565.PMID10935845.91. Jump up^Poloni M, Micheli A, Facchetti D, Mai R, Ceriani F, Cattalini C (April 1997). "Conjugal amyotrophic lateral sclerosis: toxic clustering or change?".Ital J Neurol Sci.18(2): 10912.doi:10.1007/BF01999572.PMID9239532.92. Jump up^Camu W, Cadilhac J, Billiard M (March 1994). "Conjugal amyotrophic lateral sclerosis: a report on two couples from southern France".Neurology44(3 Pt 1): 5478.doi:10.1212/WNL.44.3_Part_1.547.PMID8145930.93. Jump up^Cornblath DR, Kurland LT, Boylan KB, Morrison L, Radhakrishnan K, Montgomery M (November 1993). "Conjugal amyotrophic lateral sclerosis: report of a young married couple".Neurology43(11): 237880.doi:10.1212/WNL.43.11.2378.PMID8232960.94. Jump up^Corcia P, Jafari-Schluep HF, Lardillier D, Mazyad H, Giraud P, Clavelou P, Pouget J, Camu W (November 2003). "A clustering of conjugal amyotrophic lateral sclerosis in southeastern France".Neurol.60(4): 5537.doi:10.1001/archneur.60.4.553.PMID12707069.95. ^Jump up to:ab"Farewell Speech". lougehrig.com. 4 July 1939.Archivedfrom the original on 12 April 2008. Retrieved16 April2008.96. ^Jump up to:ab"George Bush delivers possibly the best ALS ice bucket challenge yet".Independent(Independent). Retrieved20 August2014.97. Jump up^Alexander, Ella. "Ice Bucket Challenge: Lady Gaga, Justin Bieber, G-Dragon and Oprah the most entertaining reactions so far".98. Jump up^You're Not Youat theInternet Movie Database99. Jump up^Press release project MinE, june 21st 2013:https://projectmine.com/contents/uploads/press-release-project-mine-21-06-2013.pdf100. Jump up^http://www.cytokinetics.com/pdf/2013-MDA_Jinsy.pdf101. Jump up^Shefner JM, Watson ML, Meng L, Wolff AA (December 2013). "A study to evaluate safety and tolerability of repeated doses of tirasemtiv in patients with amyotrophic lateral sclerosis".Amyotroph Lateral Scler Frontotemporal Degener.14(78): 57481.doi:10.3109/21678421.2013.822517.PMID23952636.102. Jump up^"BrainStorm Reports Outstanding ALS Interim Clinical Trial Results".FierceBiotech. Retrieved2013-08-12.103. Jump up^"Autologous Cultured Mesenchymal Bone Marrow Stromal Cells Secreting Neurotrophic Factors (MSC-NTF), in Patients With Amyotrophic Lateral Sclerosis (ALS)".ClinicalTrials.gov. Retrieved2013-08-12.104. Jump up^"Mayo Clinic to hold trial for BrainStorm's ALS stem cell therapy".Reuters. 18 March 2013.









![NFL Football & Amyotrophic Lateral Sclerosis [ALS]](https://static.fdocuments.us/doc/165x107/559430511a28ab4c3d8b4747/nfl-football-amyotrophic-lateral-sclerosis-als.jpg)

