AMR and Respiratory Paediatrics
22
AMR and Respiratory Paediatrics Richard Goodwin PaediatricIntegrated Care Pharmacist, Evelina London Children’s Hospital Pharmacy Lead, Children & Young People's Health Partnership Teacher Practitioner, University College London: School of Pharmacy #PharmacyTogether2018
Transcript of AMR and Respiratory Paediatrics

AMR and Respiratory Paediatrics
Richard Goodwin
Paediatric Integrated Care Pharmacist, Evelina London Children’s
Hospital
Pharmacy Lead, Children & Young People's Health
Partnership
Teacher Practitioner, University College London: School of Pharmacy
#PharmacyTogether2018

Declaration of Interest
#PharmacyTogether2018
I received no funding from the pharmaceutical industry
Currently employed by Great Ormond Street Hospital
Undertake primary care teaching funded through CCGs
Nothing else to declare

Todays session
#PharmacyTogether2018
Identifying which wheeze is which disease
Treatments for viral induced wheeze
Consider AMR in paediatric respiratory
Asthma isn’t serious is it?
How to monitor asthma
Treatments for asthma
Supporting holistic care

Wheezing in preschool childWheezing in preschool childWheezing in preschool childWheezing in preschool child
• Common presentation to both GP & General Paediatrics
• Significant winter burden on A&E
• 1/3 of preschool school children experience wheeze
• ~20% of these will be diagnosed as asthmatic
• Tucson Children’s Respiratory Study: 1980 to present1
Most preschool wheeze is not linked to atopy and for the vast majority will resolve by school age

The right wheeze for the right diseaseThe right wheeze for the right diseaseThe right wheeze for the right diseaseThe right wheeze for the right diseaseCommon causes of childhood wheeze:
Respiratory tract infections
GORD Asthma
Croup Bronchiolitis
ENT abnormalities Foreign body
Cystic fibrosis Bronchiectasis
Tracheobronchomalacia CHD
Tumours / vascular rings Immunodeficiency
Tracheoesphageal fistula
Asthma diagnosis red flags2

Upper Upper Upper Upper RRRRespiratory Infections / ENTespiratory Infections / ENTespiratory Infections / ENTespiratory Infections / ENTChildren > adults to receive antibiotics for self-limiting illness
• Acute otitis media in over 2 years olds: 4 days
• Acute sore throat, pharyngitis, tonsillitis 1 week
• Common cold 10 days
• Acute rhinosinusitis 18-20 days
• Acute cough/ acute bronchitis 3 weeks
Strongly consider no treatment for delayed prescribing3,4,5
Lack of confidence in treating children and risk aversion• RCGP & RCPCH provide online training
• Access to localised Antibiotic Guidance Across Primary & Secondary Care
• Public health educating families on the risk of AMR

CQUIN Paediatric Serious InfectionsCQUIN Paediatric Serious InfectionsCQUIN Paediatric Serious InfectionsCQUIN Paediatric Serious InfectionsPaediatrics is based on Days on Therapy rather than Daily Dose Units
• Ensure you are reporting the correct data
• Review process & reporting systems to reduce double reporting
• Consider increased AMS for Hospital@Home and OPAT
• Restrictive supplies of board spectrum antibiotics
• Focus on paediatric antibiotic guidance
• Tackle inappropriate post op prophylaxis
• Junior doctors & NMP more likely to prescribe Abx in children than consultants
Technology to support Sepsis 6 triggers:

Treating viral induced wheezeTreating viral induced wheezeTreating viral induced wheezeTreating viral induced wheeze
No robust evidence on when to initiate treatment
No robust evidence on initiating preventer therapy
Inhaled Salbutamol6
Prescribe
Good evidence base for reducing
hospitalisation, healthcare unitisation and
symptomatic relief.
Oral Steroids7
Avoid routine prescribingDoes not: reduce hospitalisations, GP attendance, improve
symptoms, reduced SABA use, improve self report scores or reduce
missed school days.
Reserve for severe exacerbations
Inhaled ICSPrescribe in caution
50% reduction in oral steroid requirement but no
effect on hospitalisation or duration of symptoms
with high dose budesonide 1600-3200mcg8
No benefit of lower dose ICS9
Review regularly to assess improvements
MontelukastPrescribe in caution
Recommended in BTS/SIGN Guidance2
Continuous therapy
Vs.
Pulse therapy

MontelukastMontelukastMontelukastMontelukast for Viral Induced Wheezefor Viral Induced Wheezefor Viral Induced Wheezefor Viral Induced WheezeEvidence in viral induced wheeze patients10: Montelukast Vs. Placebo
Treatment
with oral
steroids
Reduction in
wheeze
episodes
Reduced A&Eattendance
Reduced
hospital
admission
Reduce access
to healthcare
Decreased use
of reliever
Continuous
MontelukastX X X X X X
Intetmittent
MontelukastX X X X X X
Evidence in preschool wheeze11: Montelukast Vs. PlaceboContinuous Montelukast
No: change in frequency wheezy episodes, no ss difference in adverse events
Intermittent Montelukast
No: change in frequency wheezy episodes, no ss difference in adverse events

Is asthma a condition or a group of conditions
‘Phenotypes’ or reasons for asthma: patients may have more than one:
Mainly academic interest at the moment but could revolutionise paediatric
asthma care!
Inflammatory markers
of asthma:
9.Eosinophilic and
neutrophilic asthma
Asthma is Asthma RightAsthma is Asthma RightAsthma is Asthma RightAsthma is Asthma Right
Clinical presentation:
6. Pre-asthma wheezing in
infants
7. Exacerbation-prone
asthma
8. Asthma with limited
reversibility
Trigger induced:
1. Allergic
2. Non-allergic
3. Aspirin-NSAID induced
4. Infection
5. Exercise

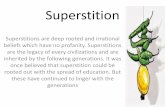
Asthma shouldn’t killAsthma shouldn’t killAsthma shouldn’t killAsthma shouldn’t kill
0
5
10
15
20
25
30
0.00
0.05
0.10
0.15
0.20
0.25
Proportion (%)10 year mortality rate per
100,000 population
10 year mortality rate
Proportion aged 6-7 with wheeze
Proportion aged 6-7 with asthma
Proportion aged 13-14 with wheeze
Proportion aged 13-14 with asthma
Directly standardised asthma mortality rate in children aged 0-14 years and proportion aged 6-7 and 13-14 Source: WHO European Mortality
Database (2000-10) and the International Study of Asthma and Allergies in Childhood (2000-03)
7 children in a capital
died from asthma in
2017

How do children talk about their asthmaHow do children talk about their asthmaHow do children talk about their asthmaHow do children talk about their asthma
Young Children Under 5
years
Children 5 – 11 years old Teenagers
(>12 years)

How do children talk about their asthmaHow do children talk about their asthmaHow do children talk about their asthmaHow do children talk about their asthmaYoung Children Under 5 years Children 5 – 11 years old Teenagers
(>12 years)
Struggle to verbalise that that their
asthma is active. Will request medicine
or provide non-specific symptoms.
‘I need my puffer’
‘My tummy hurts | My chest hurts’
‘I’m tired’
Sit very quietly
Naughty cough
Request drink after exercise
Able to verbalise specific symptoms but
struggle with change over time.
‘I feel like an elephant I sitting on my chest’
‘My throat / neck gets itchy’
‘It feels like ants tickling me’
I can’t breathe’ or ‘I can’t get enough air in’
‘I feel wheezy’ or ‘I cough’
Sense of invincibility.
Unable to explain but may answer specific
closed questions.
‘It stops me doing things like sport and I
cannot play
‘It’s not my asthma, it’s just a cough’
‘I cough and then I start getting wheezy’
‘My chest is bad’

Speaking the same language: asthma symptoms Speaking the same language: asthma symptoms Speaking the same language: asthma symptoms Speaking the same language: asthma symptoms
RCGP 3 Questions:
• Difficulty sleeping
• Daytime symptoms
• Interfered with work or school
Peak flow monitoring:
• Evidence of impact is mixed
• Poor compliance to daily continued monitoring
• Consider for targeted monitoring or diagnosis

Thinking holistically: Emotional HealthThinking holistically: Emotional HealthThinking holistically: Emotional HealthThinking holistically: Emotional HealthAsthmatic children say:
• 98% stops them doing something
• 51% had problems visiting friends
• 40% felt it stopped them having fun
Missing out – UK Wide Report. Asthma UK 2009
• 87% miss school due to asthma
• 73% struggled to engage in PE session
• 49% struggled in lessons
• 48% avoided school trips
Always think is this Asthma symptoms or Anxiety symptoms
Utilise Peak flow
Asthma action plans
Support exploring anxiety

Therapeutic
trial with
moderate
dose of ICS
Consider
salbutamol
mono-
therapy if few
symptoms
All ages Low
dose ICS
<5 years refer to
tertiary care
>5 years
Add a LABA and
increase ICS to
medium dose
Consider MART
therapy
All ages
add LTRA
Mirrors
BTS/SIGN
Guidance
Mirrors
BTS/SIGN
Guidance
NIC
E G
uid
an
ce1
2B
TS
/ S
IGN
Gu
ida
nce
2

MART Therapy in ChildrenMART Therapy in ChildrenMART Therapy in ChildrenMART Therapy in Children• Combination of a quick onset LABA and ICS
• Symbicort 100/6 & 200/6 licenced >12 years as SMART13,14
• BTS/SIGN2 not recommended for children
• NICE12 recommends in over 5 years with caveat of licensing and prescribers risk
Comparing SMART therapy, ICS and ICS/LABA fixed dose combinations14
Outcome SMART therapy Symbicort fixed dose
100/6
Budesonide
320micrograms
Exacerbation % 14 38 26
Exacerbations requiring medical attention % 8 31 20
Night-time awaking % 2.4 4.6 4.4
Symptom free days % 63.4 68.0 56.2
Asthma control days % 57.0 60.6 50.8

Corticosteroid: the good, the bad, the uglyCorticosteroid: the good, the bad, the uglyCorticosteroid: the good, the bad, the uglyCorticosteroid: the good, the bad, the ugly
Corticosteroids remain the most cost effective intervention for improving asthma2
Patents and parents concerns: I will look like a ‘shot putter’ ‘I will get fat’ ‘what about basketball!’
‘Causing shortness’ what does the evidence say16:
• Cochrane review of 25 studies totalling 8471 children were included
• Included studies of Low or Medium dose ICS over 3months
• ICS reduce growth: mean reduction of 0.61cm in year one with a mean reduction of 0.48cm/yr
Take home messages:
• Use effective doses don’t be scared
• Pick a device which works for the patient
• Don’t switch all patients to the newest therapeutic choice
• More research is needed

Thinking holistically Thinking holistically Thinking holistically Thinking holistically Child don’t smoke do they!
1%
96%
3%Don't know
No
Yes 0.0%
5.0%
10.0%
15.0%
20.0%
13 14 15 16 17 18
2%
75%
23%Don't know
No
Yes
Percentage of children who smoke
Children in smoking homes

Thinking holistically Thinking holistically Thinking holistically Thinking holistically
Weight and exercise
• Obesity contributes to poor asthma control
• Promote exercise (asthmatics should be able to undertake similar exercise to their peers) and healthily lifestyle
Vaccinate to protect
• Check vaccines on every contact
• Promote annual flu vaccine
• Check pneumococcal vaccine
Personalised asthma action plan
• Ensure every patient has one
• Use one design across the STP: Asthma UK

ReferencesReferencesReferencesReferences1. Taussig LM, Wright AL, Holberg CJ, et al. Tucson Children’s Respiratory Study: 1980 to present. J Allergy Clin Immunol 2003;111:661-75
2. British Thoracic Society and Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma – A National Clinical Guideline. Edinburgh2016
3. Spurling GKP, Del Mar CB, Dooley L, Foxlee R, Farley R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database of Systematic Reviews 2017, Issue 9. Art. No.:
CD004417. DOI: 10.1002/14651858.CD004417.pub5
4. Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database of Systematic Reviews 2015, Issue 6. Art. No.:
CD000219. DOI: 10.1002/14651858.CD000219.pub4
5. Niamh M Redmond, Sophie Turnbull, Beth Stuart, Hannah V Thornton, Hannah Christensen, Peter S Blair, Brendan C Delaney, Matthew Thompson, Tim J Peters, Alastair D Hay and
Paul Little. Br J Gen Pract 2018; 68 (675): e682-e693. DOI: https://doi.org/10.3399/bjgp18X698873
6. Baraldi BP, Bisgaard H, Boner A ,et al. Definition, assessment and treatment of wheezing disorders in preschool children: an evidence-based approach. E Respir J. 2008;32(4)1096-
1110
7. Panickar J, Lakhanpaul M, Lambert PC et al. Oral Prednisolone for Preschool Children with Acute Virus-Induced Wheezing. NEJM, 2009 Volume 360:329-338
8. Kaditis AG, Winnie G, Syrogiannopoulos GA. Anti-inflammatory pharmacotherapy for wheezing in preschool children. Pediatr Pulmonol 2007;42:407–420.
9. McKean M, Ducharme F. Inhaled steroids for episodic viral wheeze of childhood. Cochrane Database Syst Rev 2000;Issue 1:CD001107
10. Brodlie M, Gupta A, Rodriguez-Martinez CE, Castro-Rodriguez JA, Ducharme FM, McKean MC. Leukotriene receptor antagonists as maintenance and intermittent therapy for
episodic viral wheeze in children. Cochrane Database of Systematic Reviews 2015, Issue 10. Art. No.: CD008202. DOI: 10.1002/14651858.CD008202.pub2.
11. Hussein, H.R., Gupta, A., Broughton, S. et al. Eur J Pediatr (2a017) 176: 963. https://doi.org/10.1007/s00431-017-2936-6
12. National Institute for Health and Care Excellence (2017) Asthma: diagnosis, monitoring and chronic asthma management (NICE Guideline N80). Available at:
https://www.nice.org.uk/guidance/ng80 [Accessed 01 Jan 2018].
13. Electronic medicines compendium (2017) Symbicort Turbohaler 100/6 dry powder SPC. Available at: https://www.medicines.org.uk/emc/product/1326 [Accessed 01 Jan 2018].
14. Electronic medicines compendium (2017) Symbicort Turbohaler 200/6 dry powder SPC. Available at: https://www.medicines.org.uk/emc/product/1326 [Accessed 01 Jan 2018].
15. Bisgaard H, Le Roux P, Bjamer D, Dymek A, Vermeulen JH, Hultquist C. 1 Budesonide/formoterol maintenance plus reliever therapy: a new strategy in paediatric asthma. Chest.
2006; 130(6):1733-1743
16. Zhang L, Prietsch SOM, Ducharme FM. Inhaled corticosteroids in children with persistent asthma: effects on growth. Cochrane Database of Systematic Reviews 2014, Issue 7. Art.
No.: CD009471. DOI: 10.1002/14651858.CD009471.pub2

Any questions?We value your opinion, so please don’t forget to fill in the evaluation form!
pharman.co.uk
@pharman
ukclinicalpharmacy.org
@ukcpa
@RichardJGoodwin
#PharmacyTogether2018