
³&KHPLFDO %LRORJLFDO &RPSDUDWLYH &OLQLFDO
156
“Chemical, Biological and Comparative Clinical Evaluation of Linkus Kids Syrup to Determine the Safety and Efficacy for the Treatment of Cough” Hina Rehman Department of Pharmacy Practice Faculty of Pharmacy Jinnah University for Women, 5-C Nazimabad Karachi-74600, Pakistan 2016
Transcript of ³&KHPLFDO %LRORJLFDO &RPSDUDWLYH &OLQLFDO

“Chemical, Biological and Comparative Clinical Evaluation of Linkus Kids Syrup to
Determine the Safety and Efficacy for the Treatment of Cough”
Hina Rehman
Department of Pharmacy Practice
Faculty of Pharmacy
Jinnah University for Women,
5-C Nazimabad Karachi-74600, Pakistan
2016

In the Name of Allah
The most beneficent, the most merciful

“CHEMICAL, BIOLOGICAL ANDCOMPARATIVE CLINICAL EVALUATIONOF LINKUS KIDS SYRUP TO DETERMINE
THE SAFETY AND EFFICACY FOR THETREATMENT OF COUGH”
Thesis submitted in the partial fulfillment of degree of
Doctor of Philosophy (PhD) in
By
Dr.Hina Rehman.
Department of Pharmacy Practice
Faculty of Pharmacy
Jinnah University for Women,
5-C Nazimabad Karachi-74600, Pakistan
2016
“CHEMICAL, BIOLOGICAL ANDCOMPARATIVE CLINICAL EVALUATIONOF LINKUS KIDS SYRUP TO DETERMINE
THE SAFETY AND EFFICACY FOR THETREATMENT OF COUGH”
Thesis submitted in the partial fulfillment of degree of
Doctor of Philosophy (PhD) in
By
Dr.Hina Rehman.
Department of Pharmacy Practice
Faculty of Pharmacy
Jinnah University for Women,
5-C Nazimabad Karachi-74600, Pakistan
2016
“CHEMICAL, BIOLOGICAL ANDCOMPARATIVE CLINICAL EVALUATIONOF LINKUS KIDS SYRUP TO DETERMINE
THE SAFETY AND EFFICACY FOR THETREATMENT OF COUGH”
Thesis submitted in the partial fulfillment of degree of
Doctor of Philosophy (PhD) in
By
Dr.Hina Rehman.
Department of Pharmacy Practice
Faculty of Pharmacy
Jinnah University for Women,
5-C Nazimabad Karachi-74600, Pakistan
2016

APROVAL SHEET
Title Chemical, Biological and Comparative Clinical Evaluation ofLinkus Kids Syrup to Determine the Safety and Efficacy forthe Treatment of Cough
Name of Candidate Hina Rehman
Internal Examiner _____________________________________________
_____________________________________________
External Examiner ______________________________________________
______________________________________________
Date of Approval ______________________________________________

CERTIFICATE
This is to certify that the research work presented in this thesis entitled : “Chemical,
Biological and Comparative Clinical Evaluation of Linkus Kids Syrup to Determine
the Safety and Efficacy for the Treatment of Cough” has been carried out by Hina
Rehman, in the department of Department of Pharmacy Practice in the Faculty of
Pharmacy, Jinnah University for Women Karachi, Pakistan, under my supervision.She
has summited this work in partial fulfillment of the requirement for the degree of
Ph.D.The work reported in this thesis is original and to the best of my knowledge and
belief, no part of the work has been plagiarized from any where. I consider that this work
satisfies the requitement for the award of Ph.D degree in the Department of Pharmacy
Practice in the Faculty of Pharmacy,
Signature of Supervisor: __________________________________________________
Name of Supervisor: _________ Prof Dr.Usman Ghani Khan__________________
Department: Department of Pharmacy Practice in the Faculty of Pharmacy,
Date: __________________________________________________

DECLARATION
I, Hina Rehman D/o Jamil-Ur-Rehman, hereby declare that, the research work
presented in this thesis entitled: Chemical, Biological and Comparative Clinical
Evaluation of Linkus Kids Syrup to Determine the Safety and Efficacy for the
Treatment of Cough is my original work, and no part of it has been plagiarized from
any other published work. The material if derived from other sources has been properly
cited in the thesis. The work has been completed under the supervision of
Prof.Dr.Usman Ghani Khan , Departemnt of Pharmacy Practice , Faculty of
Pharmacy, Jinnah University for Women, Karachi, Pakistan and Co-supervised by
Dr.Safila Naveed of the Department of Pharmacy Practice , Faculty of Pharmacy,
Jinnah University for Women.
I understand that the University reserves the right to cancel the degree if any of the above
information is proved to be false, before or even after the award of the degree.
Signature of Candidate: __________________________________________________
Name of Candidate: _________ Hina Rehman______________________________
Department: Department of Pharmacy Practice in the Faculty of Pharmacy
Date: __________________________________________________

Dedicated
To
My Husband,
&
My Parents

ACKNOWLEDGEMENT
All praise to ALLAH, who is unique, the beneficent, and the merciful and his prophetMuhammad peace is upon him, the guide and Rehmat-ul-Alamin from whom I seekguidance to lead my life.
I am highly grateful to Mr.Wajhiuddin Ahmed, Chancellor and Prof.Dr.Naeem Farooqui,Vice Chancellor, Jinnah University for Women, Karachi, Pakistan for their encrougementand interest to pursue higher learning and research.
There is no limit of learning knowledge, notwithstanding of my present age only myrespected supervisor Prof. Dr. Usman Ghani Khan inculcate my chivalry withrejuvenated zeal to perform this task by his in valuable guidance, deep interest, coaching,sustained interest, orientation, advices, meticulous care in experimental work, pragmaticsuggestions, stimulating discussion, critic and he made me so to undertake the strenuousresearch work like young student. I pay my gratitude to my supervisor, as without hiscompassion, it was hard for me to accomplish the task.
I am most thankful to Dr. Safila Naveed, Associate Professor, Jinnah University forwomen and my co supervisor for her kind cooperation and assistance for conducting theresearch. She has taught me, both consciously and unconsciously. I appreciate for hercontributions of time, ideas, and funding to make my Ph.D. experience productive andstimulating. The joy and enthusiasm she has for her research was contagious andmotivational for me, and I am also thankful for the excellent example she has provided asa successful woman pharmacist and professor.
My sincere thanks to Dr. Ghulam Sarwer Dean, Faculty of Pharmacy for his cooperationand understanding to achieve the objectives of research for the thesis. I am grateful to Dr.M. Tanweer Alam Director, Central Drug Laboratory Karachi for his very generousassistance in research attachments. I would like to record the cooperation of all mycolleagues in Jinnah University for Women.
I am most thankful to Mr. Nadeem Khalid, Mr. Zeeshan Ahmed Sheikh, Dr. Aqib Zahoorand Dr. Saleha Suleman Khan of Herbion Pakistan (Pvt.) Ltd., for their kind cooperationand assistance to conduct some part of research in Herbion Pakistan (Pvt.) Ltd., Karachi,Pakistan.
I may not forget my elder colleagues namely Dr. Huma Ali Faculty of Pharmacy, JinnahSindh medical University whose blessings have been a great source of my vitality in myprofession all around. Lastly, I would like to thank my family for their love andencouragement especially my husband for his support and parents who raised me with alove of science and supported me in all my academic pursuits.
Hina Rehman

ix
ABSRACT
Introduction
more than 102/ ml, Enterobacteria and some other gram- negative bacteria – not more
than 102/ g, Salmonella absent in 10 ml and E. coli, Staphylococcus aureus – absent / ml.
Linkus lozenges revealed average weight (2.375g to 2.625g), weight uniformity (2.5g ±
5%), thickness (7mm ± 1mm) and diameter (17mm ± 1mm) by Vernier caliper.
Linkus cough syrup and lozenges both contains Adhatoda vasica vasicinone and
vasicine (helps to reduce cough, common cold and serve as an expectorant),root of
Glycyrrhiza glabra contains active glycyrrhizin (helps for upper respiratory tract
infections),Piper longum fruit and root contains active piperlonguminine , piperine,
piperlongumine (helps for cough and other respiratory tract infections), Hyssopus
officinalis, Alpinia galangal, Zingiber officinale and Cordia latifolia (used to control
coughing and respiratory tract infections).
In current study, Standardize Linkus syrup and lozenges have been prepared in amber
color bottle. Various Physiochemical parameters including organoleptic parameters, pH
(3.0-5.0) and Density (1.25 - 1.35 g/ml) were calculated for Syrup. On qualitative
evaluation tanning agents and ascorbic acid were confirmed however the quantitative
analysis showed total alkaloid content as vasicine were not less than 0.035 %.Microbial
purity was checked and confirmed that Bacteria – not more than 104/ ml, Fungi – not
Cough is the most common symptom in children and causes discomfort in health care
utilization .Over the counter (OTC) cold and antitussive medicine is very common in kids
under 2 to 5 years of age and almost all children experienced cough and associated
symptoms .The usefulness of anti-cough medications remains debatable in spite its wide
spread consumption. Different Mata analysis and Clinical trials are investigating their
role and claimed lack of evidence. A systematic review of randomized controlled trials on
different kinds of these medications concluded they were not superior to placebo. The
recognitions and advancements in evidence based herbal treatment have gained
popularity along with the allopathic medication. Herbal medicines have gained attraction
and captured the market during the last decades .WHO claims that 65-80% population in
developing countries prefer plants for the treatment in health care division .

For investigating the efficacy and toxicity of Linkus Syrup and lozenges in experimental
animal Albino Rats were choosing. It is a first of its kind studies to further authenticate
the safety of linkus lozenges. The Acute toxicity test for Linkus dosage foams was
performed on Albino rats Strain Haffkine with both Sex ratio 1:1.Weight was between
150 – 250 g and ages were 4 – 6 months. 0.21 g / kg is the therapeutic dose of the
preparation. 20 times (4g/kg) the therapeutic dose was tested for acute toxicity. For
chronic toxicity testing both gender albino rats with strain Haffkine ,1:1 ratio (weight
between 150 – 200 g) were selected for experimentation. The morphological examination
of organs and estimation of biochemical parameters were assessed .Recommended adult
x
The biomarker Vasicine was analyzed qualitative and quantified through HPTLC by UV
visible spectrophotometry, which was not less than 0.02 mg per lozenges and 0.080mg
respectively. The quantitative estimation of Piperine and Glycyrrhizin biomarkers via
HPLC & HPTLC method were used in Linkus Kids syrup. Chromatography included
HPTLC and HPLC has been used to determine the biomarkers included Piperine and
Glycyrrhizin using Benzene: Ethyl acetate (v/v): Methanol: Water: Formic Acid, 15:5:1:1
(v/v/v/v) as a solvent system with ultra violet light 345 for Piperine and 254 nm for
Glycyrrhizin. The HPLC chromatograms of Piperine with standard at an optimum
wavelength on 345nm at a retention time of 1-8.09 min however in HPTLC silica gel
G60F254 with the use of CAMAG Linomet 5,CAMAG Scanner method the Rf value
seemed to be <1 (0.1-0.20).
Linkus dosage foam tested for anti-microbial activity against Staphylococcus aureus,
Streptococcus pyogenes, Salmonella and Pseudomonas Aeruginosa. McFarland
principles were adopted for maintaining the turbidity in bacterial microorganism.
Antimicrobial testing was performed on agar and well diffusion method. As per disc
diffusion, the disc was 0.007 m and well prepared with the help of a cork-borer were 0.85
cm. The outcomes of the study exhibited that linkus cough shows strong sensitivity
against Staphylococcus Aureus, Streptococcus pyogenes and Salmonella in both disc and
well diffusion method and showed resistivity against Pseudomonas Aeruginosa. However
with the comparison of Amoxicillin and Ampicillin, linkus showed more sensitivity
against Salmonella and Streptococcus pyogenes.

xi
dose was 15 g/day, Dose /kg of body weight was 0.21 g/kg however the therapeutic dose
of the preparation was 20 (4g/kg) and was tested for chronic toxicity. Housed condition
was 75ºF or 25˚C ± 1˚C and nourishment at labium. No mortality and no
abnormality were seen inlinkus dosage foam and suggested it to be the safest choice
The Phase IV randomize control trial was establish to evaluate the safety and efficacy of
Linkus with other 2 arms included Aminophylline with Diphenhydramine group and
Acefyllin Piperazine with Diphenhydramine cough syrup on children having cough and
sleep difficulty associated with cough. Simple randomization pattern were adopted for
patient randomization.To determine the effects of Linkus polyherbal syrup (group A)
and compared with other parallel allopathic groups (Group B and C) for cough on
children and associated sleep quality and improvement. 360 children having cough
inducted in 3 different groups randomly selected. Ethnic groups, frequency of cough
and diseases illness (<0.05) were determine on every group on the
investigational syrup. Cough impact on child and its sleep of three different syrups (every
group) were assessed on day1 and day 14(p< 0.001) via a likert scale. For the evaluation
of pain assessment Wong baker face scale were used and level of significance in each
group (p <0.001).Significant results were observed in the Linkus Group as compared to
the other parallel groups including Aminophylline plus Diphenhydramine and Acefyllin
Piperazine with Diphenhydramine on day 14 (p<0.001).Side effects on group B and group C (Aminophylline with Diphenhydramine and Acefyllin Piperazine with Diphenhydramine) were almost similar in number however linkus syrup have minimum side effects on study duration. Polyherbal syrup Linkus shows better results in treatment of cough including side effects as compare to the other parallel groups B and C (Aminophylline with Diphenhydramine and Acefyllin Piperazine with Diphenhydramine). The interquartile ranges on the same selected marketed group were established with Linkus. It was open label multi centric simple randomize control trial. The study was conducted on different private schools of East and West Malir ,Karachi Pakistan with the special approval from the school honors .Informed consent and assents were taking before the enrollment of the study subjects .
HINA JUNAID
Highlight
HINA JUNAID
Highlight
HINA JUNAID
Highlight

xii
The study enrolled participants were 196 who evaluate on cough and associated
problems include 140± females and 56± were male.Participants were divided into
3 interventional group according to the treatment regimen .One group of participant
received Linkus Syrup however the 2nd group received Acefyllin Piperazine and
3rd group received Aminophylline Diphenhydramine group. The dosing of Linkus
syrup were 1-2 table spoon (15 ml) 3-4 times daily However the 2nd and 3rd group
taking dose as per the standard 2.5 to 5ml 3-4 times daily . One way analysis of
variance was used to compare the mean across treatment groups and Pearsonchi square
test was used to see the association of qualitative variables. Wilcoxon sign rank test
was applied to see the effect of treatment outcomes at pre and post stages, Median
and inter quartile ranges also reported along with p-values. Box plot, bar and pie chart
used to display the information in graphical way, all p-values less than 0.05 were
considered significant. The frequency of the cough on linkus Syrup was considered to be
achieved on the basis of interquartile relationship (1st and 3rd Quartile) and impact has
been observed on child and parent sleep and found significant (p <0.01). The frequency
of the side effects observed significantly reduced (p<0.01) in Linkus Group and consider
to be the effective with minimum side effects however the pharmacological treatments
are considered to be more unwanted effects on human subjects.

. کھانسی بچوں میں سب سے زیاده عام علامت ہوتی ہے اور صحت کی دیکھ بھال میں تکلیف کا سبب بنتا ہے
سال کے بچوں میں بہت عام ہے اور تقریبا تمام بچوں کو 5سے 2طب عمر کے antitussiveسردی اور
باوجود اس کے وسیع پھیلاؤ کی اینٹی کھانسی کی ادویات کی افادیت کے. کھانسی اور منسلک علامات ہوتی ہے
مختلف ماتا تجزیہ اور کلینکل ٹرائلز ان کے کردار کی تحقیقات اور ثبوت کی کمی . کھپت متنازعہ بنی ہوئی ہے
کنٹرول ٹرائلز کی ایک منظم جائزه randomizedان ادویات کے مختلف قسم کے . کے دعوی کر رہے ہیں
جڑی بوٹیوں اور ایلوپیتھک ادویات سے . سے بہتر نہیں تھے placeboلینے سے یہ نتیجہ اخذ ہوا ہے کے وه
ہربل ادویات سے علاج نے توجہ حاصل کر لی ہے اور گزشتہ . علاج نے ساتھ ساتھ مقبولیت حاصل کی ہے
٪ 80-65کا دعوی ہے کہ ترقی پذیر ممالک میں WHO. کر لی ہےcaptureکئی دہائیوں کے دوران مارکیٹ
vasicine0.035 مائکروبیل . ٪ سے کم نہیں تھےpurityکہ بیکٹیریا کی جانچ پڑتال اور تصدیق نےثابت کیا
-/ ml104ئد نہیں ، سے زاFungi-/ ml102، سے زائد نہیںEnterobacteria اور کچھ دوسرےgram -
E. coli, Staphylococcusملی میں غائب ہے اورSalmonella10سے زائد نہیں،g/102منفی بیکٹیریا
آبادی صحت کی دیکھ بھال میں علاج کے لیے پودوں کی جڑی بوٹیوں کو ترجیح دیتے ہیں.
مواد ظاہر ہوا اور alkaloid ایسڈ کی تصدیق کی گئی. تاہم مقداری تجزیہ پر کل ascorbic کے ایجنٹوں اور
پر ملی میں غائب ہیں . aureus.
شوز، وزن میں یکسانیت (2.5g ± 5%)، موٹائی (2.375g to 2.625g) اوسط وزن Linkus lozenges
ٹیسٹ Qualitative.کی مدد سے Vernier caliper (17mm ± 1mm)اور ڈایامیٹر (7mm ± 1mm)
ایسڈ کی موجودگی کی تصدیق کر رہے ہیں. ascorbic اور tannins
xiii
رنگ کی بوتل میں تیار کر رہے ہیں. amber, Lozenges شربت اور Linkus موجوده مطالعہ میں ، معیاری
اور pH (3.0-5.0 ) کے پیرامیٹرز سمیت organoleptic پیرامیٹرز اور Physiochemic مختلف
tanning تشخیص پر Qualitative .شربت کے لئے حساب کر رہے تھے Density (1.25 - 1.35 g/ml)
لئے مدد کرتا پر مشتمل ہے ( کھانسی اور دیگر سانس کی نالی کی بیماریوں کے piperlongumine،piperine
Cordia Latifolia اور Zingiber Officinale ،Alpinia galangal ،Hyssopus officinalis ہے) ،
(کھانسی اور سانس کی نالی کی بیماریوں کو کنٹرول کرنے کے لئے لئے مدد کرتا ہے).
مشتمل vasicine اور Adhatoda vasica vasicinone دونوں lozenges کھانسی شربت اور Linkus
تھا. لئے مدد کرتا کے طور پر خدمت کرنے کے expectorant کھانسی ، عام سردی کو کم کرنے اور ایک
بیماریوں کی نالی کی سانس اوپری ) ہے مشتمل پر glycyrrhizin فعال جڑ کی Glycyrrhiza glabra،
piperlonguminine، ہے) پھل اور جڑ فعال longum کے لئے مدد کرتا ہے) پائپر

کا موازنہ کے ساتھ ، لنکس نے Ampicillin اور Amoxicillin خلاف مزاحمیت دکھائی. تاہم Aeruginosa
Staphlococcous aureus, Streptococcous لنکس خوراک کا اینٹی مائکروبیل سرگرمی کے لئے تجربہ
اصول پنایا گیا McFarland .کے خلاف کیا pyogenes, Salmonella and Pseudomonas aeruginosa.
اور raga ٹیسٹنگ antimicrobial .برقرار رکھنے کے لئے Turbidity پر تھا بیکٹیریل مائکرو اورگینزم
xiv
UV visible کے ذریعے qualitative HPTLCاور کیا گیا quantified تجزیہ Biomarker Vasicine
نہیں. کم سے 0.080mg اور بلترتیب 0.02 mg per lozenges مدد سے جو spectrophotometry کی
تیراپیتھک g / kg مہینے تھے۔تیاری مین 0.21 سے 6 گرام اور عمر 4 سے 250 دیے ، جن کا وزن 150
(g/kg4) تیراپیتھک خوراک کو اکیوت ٹاکسٹي کے لیے ٹیسٹ کیا گیا جبکے کرانک باری خوراک تھی۔20
گرام) چنے گؑے سے 200 (وزن 150 ٹاکسٹي ٹیسٹ دونون جنسالبینو چوہے ساتھاسٹرین حفکینی،ریشو 1:1
کے HPLC chromatograms.254nm کے لئے Glycyrrhizin کے لئے اور Piperine روشنی 345
G60F254 سلیکا جیل HPTLC منٹ کے ساتھ, تاہم میں برقراری وقت 8.09-1 nm سٹینڈرڈ ویو لینت 345
ہونے کا <1 value سکینر کے طریقہ کار آر یف CAMAG کا استعمال CAMAG Linomet 5 کے ساتھ
) لگ رہا تھا. 0.20-0.1 )
میٹر تھا. اور اچھی ڈافیوجین کے طریقہ کار پر کیا گیا تھا. ڈسک ڈافیوجین کے مطابق. ڈسک 0.007 llew
سینٹی میٹر تھے . مطالعہ کے نتائج پتہ چلتا ہے کہ بورر کی مدد سے تیار 0.85 طرح سے ایک کارک -
Staphylococcus aureus, Streptococcus pyogenes سینسیویٹی دکھائی مضبوط نے کھانسی linkus
Pseudom anas ڈافیوجین کے طریقہ کار پر اور llew کے خلاف دونون ڈسک اور and Salmonella
بطور ایک سالوینٹ سیسٹم کے سات الٹرا والٹ Methanol: Water: Formic Acid, 15:5:1:1 (v/v/v/v)
طریقہ کار HPTLC اور HPLC کا Glycyrrhizin biomarkersاور Piperine تخمینہ Quantitative
HPLC اور HPTLC ا شامل Chromatography.شربت میں استعمال کیا گیا تھا Linkus kid کے ذریعے
Ethyl acetate (v/v): بینزین کا استعمال کرتے ہوئے Glycyrrhizin اور Piperine میں biomarkers
کے خلاف مزاحمیت دکھائی. Streptococcus pyogenes.اورSalmonella
پر انجام اکیوت ٹاکسٹي ٹیسٹ لنکسس ڈوزیج فوم کے لیے البینو چوہے اسٹرین حفکینی دونون سیکس ریشو 1:1
تجربے کے لیے۔ اعضا اور بایوکیمکل تخمیے کا جائزه کے لیے مورٖفالوجی جانچ پڑتال کی گئی۔سفارش کی
تھا۔ تہم تیراپیتھک خوراک تیاری 0.21 g / kg g / day 15تھی،ڈوز پر کلوگرام کا جسمانی وزن گئی بالٖغ خوراک
اور 25˚C ± 1˚C یا 75ºF تھی اور کرانک ٹاکسٹي کے لیے ٹیسٹ کی گئی۔ حوسڈ کنڈیشن (4 g / kg) مین 20

کے رینڈمازیشن کنٹرول ٹرائل کرنے کے لیے قائم کیا حفاظت کا اندازه کرنے کے لیے اور لنکسس کی IVفیز
گروپ کی خوراک 3 3rd اور 2nd ملی) روزانہ, تاہم چمچ (15 1-2dosing روزانہ. شربت کی 5ml بار 4
Acefyllin گروپ اور Diphenhydramine ساتھ Aminophylline کے ساتھ منسلک 2arm افادیت دیگر
کا شربت جن بچوں کے ساتھ کھانسی اور منسلک نیند کھانسی Diphenhydramine کے ساتھ Piperazine
شربت (گروپ A) کے معیار کا تعین اور موازنا دیگر متوازی polyherbal مین مشکل دکھائی دی. لنکسس
اور C) کے ساتھ بچوں پر کھانسی اور متعلقہ نیند کے معیار اور بہتر بنانے کے لئے B ایلوپیتھک گروپ ( گروپ
گروپ سے فراہم تحقیقی دوا کے بارے میں بتایا گیا تعین کر رہے تھے . کھانسی کے اثرات بچوں اور اس کی
پر جانچا کیا فریکوئنسی تحقیقی شربت پر ہر گروپ پر اس بات کا (p <0.001). دن اور 14 پیمانے کے ذریعے 1
likert نیند پر تین مختلف سیرپ (ہر گروپ) ایک
(p استعمال کیا اور ہر گروپ میں اہمیت کی سطح Wong baker face گیا تھا. درد کی تشخیص کے لئے
Aminophylline plus تھی. لنکسس گروپ میں بہترین نتائج ملے دیگر متوازی گروپوں <0.001).
کے (P <0.001) Acefyllin Piperazine Diphenhydramine 14دن اور Diphenhydramine
(Aminophylline with Diphenhydramine and پر C اور گروپ B مقابلے. ضمنی اثرات گروپ
بڑی تعداد میں تقریبا اسی طرح کے تھے تاہم لنکسس Acefyllin Piperazine with Diphenhydramine)
شربت کے اس مطالعہ مدت میں کم ضمنی اثرات رہے. دیگر متوازی گروہوں بی اور سی کے موازنہ پر
افعال اور بہتر نیند کے لیے فائده مند ہو سکتا ہے.
حدود ایک ہی منتخب مارکیٹنگ گروپ پر لنکسس ساتھ ائم کئے گئے تھے,یہ ایک لیبل کنٹرول interquartile
تجربہ تھا . مطالعہ خصوصی منظوری سے مشرق اور مغرب ملیر ، کراچی پاکستان کے مختلف نجی اسکولوں
پر منعقد کیا گیا. مطالعہ کے مضامین کے اندراج سے پہلے اجازت باخبر اور رضامندی لی.
± عورتوں اور 56 تھے جن کو کھانسی اوران سے منسلک مسائل تھے جن میں 140 مطالعہ کے شرکاء 196
انترواہی گروپ میں تقسیم کیا گیا پہلی تحقیق کے مطابق 3 regimen مرد تھے شامل تھے. شرکاء علاج ±
-
Pearson chi square test ایک طریقہ کے تجزیہ استعمال کیا گیا گروپ کے علاج کا موازنہ کرنے اورWilcoxon sign rank .کی ایسوسی ایشن کو دیکھنے کے لئے qualitative variablesاستعمال کیا گیا
ٹیسٹ پہلے اور بعد کے مراحل میں علاج کے نتائج کا اثر دیکھنے کے لئے لاگو کیا گیا تھا ،
گرافیکل Box plot, bar and pie chart, کے ساتھ ساتھ p-values تربیع بھی quartile میڈین اور انٹر
اہم سمجھا جاتا سے بھی کم 0.05 p-values طریقے میں معلومات ظاہر کرنے کے لئے استعمال کیا گیا. تمام
3rd اور 1st) .تعلقات کی بنیاد پر interquartile شربت پر تصور کیا linkus ہے. کھانسی کی فریکوئنسی
اور اثرات بچے اور والدین کی نیند پر اہم پایا گیا ہے.(p <0.01). ضمنی اثرات کے تعدد نمایاں Quartile
طور میں کم ہے لنکسس گروپ ( p <0.01) اور مؤثر ثابت ہوی.
xv

Table of Contents
1.1. Cough:....................................................................................................................................................................... 2
1.2. Pathophysiology of Cough: ....................................................................................................................................... 4
1.3. Etiology of Cough: .................................................................................................................................................... 5
1.4. Clinical Assessment of Cough: .................................................................................................................................6
1.5. Prevalence of Cough: ................................................................................................................................................ 8
1.6. Observing Cough Counts: ....................................................................................................................................... 10
1.7. Antimicrobial Assessment of Cough Syrup: ........................................................................................................... 11
1.8. Quality Parameters with Standardization of Herbal Crude Drugs: .......................................................................... 13
1.9. History of Use of Traditional Herbal Medicines: .................................................................................................... 17
1.10. Awareness, Regulation, Control on Use:................................................................................................................. 22
2. CHAPTER TWO - LITERATURE STUDY....................................................................................................... 26
2.1. Adhatoda vasica Nees: ............................................................................................................................................ 26
2.2. Piper longum Linn:.................................................................................................................................................. 28
2.3. Glycyrrhiza glabra Linn: ......................................................................................................................................... 30
2.4. Alpinia galangal (L.) ............................................................................................................................................... 33
2.5. Hyssopus officinalis (L.) ......................................................................................................................................... 35
2.6. Cordia latifolia Linn ................................................................................................................................................ 37
2.7. Viola odorata Linn .................................................................................................................................................. 39
2.8. Aims and Objectives of the Study: .......................................................................................................................... 41
3. CHAPTER THREE - METHODOLOGY .......................................................................................................... 44
3.1. Linkus...................................................................................................................................................................... 44
3.2. Quantitative Determination of Piperine and Glycyrrhizin in Linkus dosage forms (via HPLC andHPTLC)................................................................................................................................................................... 54
3.3. In Vitro Antioxidant, Reducing, Lipoxygenase and Ace Inhibition Activity of Polyherbal Drug LinkusSyrup and lozenges.................................................................................................................................................. 57
3.4. Antimicrobial Analysis of Polyherbal Formulation Linkus Syrup .......................................................................... 61
3.5. Evaluation of Efficacy and Toxicity of Poly Herbal syrup–Linkus in Experimental Animals ................................ 65
3.6. Post Marketing Phase IV Clinical Trial on Linkus Syrup: ...................................................................................... 69
3.7. An Interquartile Relationship between Polyherbal Extract Based Syrup Linkus –A Phase IVComparative Randomised Control Trial.................................................................................................................. 73
4. CHAPTER FOUR - RESULTS............................................................................................................................ 76
xvi
ACKNOWLEDGEMENT..........................................................................................................................................viii
ABSRACT……….. ..................................................................................................................................................... ix
LIST OF FIGURES .................................................................................................................................................xviii
LIST OF TABLES....................................................................................................................................................xx
1. CHAPTER ONE- INTRODUCTON...................................................................................................................2
4.1. Results of Design Development of Linkus Syrup with Biomarker Vasicine........................................................... 76
4.2. Biomarkers Present On Linkus Extract (Formed Syrup) ......................................................................................... 79
4.3. In-Vitro Antioxidant, Reducing, Lipoxygenase and Ace Inhibition Activity of Polyherbal Drug LinkusSyrup ....................................................................................................................................................................... 82
4.4. Antimicrobial Analysis of Polyherbal Formulation Linkus Cough Syrup............................................................... 85
4.5. Evaluation of Efficacy and Toxicity of Poly Herbal Syrup –Linkus In Experimental Animals: ............................. 88
4.6. Efficacy and Safety of Linkus, Aminophylline Diphenhydramine and Acefyllin Piperazine for theTreatment of Cough in Children.............................................................................................................................. 94
4.7. An Interquartile Relationship between Polyherbal Extract Based Syrup Linkus –A Phase IVComparative Randomized Control Trial. ................................................................................................................ 98
4.8. Results of SPO2, BRM with All Linkus Groups .............................................................................................. 104
5. CHAPTER FIVE - DISCUSSION ................................................................................................................109
5.1. Discussion: ........................................................................................................................................................ 109
5.2. Conclusion and Future Prospects ........................................................................................................... 115
REFRENCES........................................................................................................................................................... 117
LIST OF PAPERS IN PUBLICATION ................................................................................................................ 135
xvii

LIST OF FIGURES
Figure 1: Cough in Child and Length of Cough........................................................................................... 3
Figure 2. Klebsiella pneumoniae................................................................................................................ 11
Figure 3. Pseudomonas aeruginosa............................................................................................................ 11
Figure 4. Staphylococcus aureus................................................................................................................ 12
Figure 5. Enterococcus faecalis ................................................................................................................. 12
Figure 6. Escherichia coli........................................................................................................................... 12
Figure 7. Salmonella spp ............................................................................................................................ 13
Figure 8. Salmonella paratyphi .................................................................................................................. 13
Figure 9.Adhatoda vasica Nees (Whole Plant)........................................................................................... 27
Figure 10. Fresh Leaves of Adhatoda vasica Nees..................................................................................... 27
Figure 11. Flower of Adhatoda vasica Nees............................................................................................... 28
Figure 12. Chemical Structure of Vasicine................................................................................................. 28
Figure 13. Fresh Leaves of Piper longum .................................................................................................. 29
Figure 14. Unripe Fruit of Piper longum ................................................................................................... 29
Figure 15. Dried mature fruit of Piper longum .......................................................................................... 30
Figure 16.Chemical Structure of Piperine.................................................................................................. 30
Figure 18. Fruit of Licorice plant(Glycyrrhiza glabra) ............................................................................. 32
Figure 17. Licorice plant (Glycyrrhiza glabra).......................................................................................... 31
Figure 19. Root of Licorice plant (Glycyrrhiza glabra) ............................................................................. 32
Figure 20. Chemical structure of Glycyrrhizin........................................................................................... 33
Figure 21. Fresh Leaves of Alpinia galangal ............................................................................................. 34
Figure 22. Flower of Alpinia galangal ....................................................................................................... 34
Figure 24. Chemical structure of 1’-acetoxychavical acetate .................................................................... 35
Figure 25. Chemical structure of Galanolactone ....................................................................................... 35
Figure 23. Root of Alpinia Galangal .......................................................................................................... 34
Figure 26. Fresh Leaves of hyssopus officinalis......................................................................................... 36
Figure 27. Flower of hyssopus officinalis................................................................................................... 36
Figure 28. Dried Herb of hyssopus officinalis............................................................................................ 36
Figure 29. Chemical structure of Apigenin & Luteolin .............................................................................. 37
Figure 30. Chemical structure of Quercetin & Rutin ................................................................................. 37
Figure 31. Fresh Leaves of Cordia latifolia ............................................................................................... 38
Figure 32. Flower of Cordia latifolia ......................................................................................................... 38
xviii

Figure 33. Flower of Cordia latifolia ......................................................................................................... 38
Figure 34.Structure of Cordifolic acid ....................................................................................................... 39
Figure 35. Fresh Leaves of Viola odorata Linn.......................................................................................... 40
Figure 36. Flower (Purple) of Viola odorata Linn..................................................................................... 40
Figure 37. Flower (White) of Viola odorata Linn ...................................................................................... 40
Figure 38: Structure of 5, 6, 7, 7a-tetrahydro-4, 4, 7a-trimethyl-2(4H)-benzofuranone ........................... 41
Figure 39. Steps Showing from Randomization to Analysis ....................................................................... 72
Figure 40. TLC Plate with Standard and Sample Spots ............................................................................. 77
Figure 41. Plate with Standard and Sample Spots Developed ................................................................... 77
Figure 42.Vasicine Standard ...................................................................................................................... 78
Figure 43. Vasicine Sample ........................................................................................................................ 78
Figure 44. Peak Response of Piperine in Linkus Syrup.............................................................................. 80
Figure 45. Peak Response of Piperine Standard ........................................................................................ 80
Figure 46: Peak Response of Glycyrrhizin in Linkus Syrup ....................................................................... 81
Figure 47: Peak response of Glycyrrhizin and Standard ........................................................................... 82
Figure 48: Antimicrobial Analysis of the Linkus ........................................................................................ 86
Figure 49: Comparative Zone of Anti-microbial inhibition of Linkus versus Ampicillin and
Amoxicillin .................................................................................................................................................. 88
Figure 50: Comparison First Visit (Day 1) versus Last day (Day 14) ....................................................... 97
Figure 51. Inter Quartile Range Before and After the Treatment of Linkus............................................. 100
Figure 52: Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine ...................... 101
Figure 53: Inter Quartile Range Before and After the Treatment of Treatment of Aminophylline .......... 102
Figure 54: Comparison of Toxic Effects on Lipid Profile ........................................................................ 103
Figure 55. Box Plot for differentVariables ............................................................................................... 106
Figure 56.The Child Sleep disturbance due to Cough Before and After the Treatment. .......................... 106
Figure 57. Pain Before and After the Treatment ...................................................................................... 107
xix

LIST OF TABLES
Table 1. Agent that Induce Cough in Human beings .................................................................................... 5
Table 2: Causes of Assessment of Acute Cough ........................................................................................... 7
Table 3. Cough Sympton Score..................................................................................................................... 9
Table 4: The global nutrition products industry in 1999, including herbal and botanical
products” (in millions of US $) (70) ........................................................................................................... 19
Table 5: Trends in the global nutrition products industry, 1997–2000” (in millions of US $)(70) ........... 20
Table 6: Top Selling Herbs in US, (in million USD) (70)........................................................................... 21
Table 7: Top 10 Most Famous Herbal Solutions in Canada (70)............................................................... 21
Table 8. Composition of Linkus Syrup........................................................................................................ 45
Table 9. Plant Parts Used in Linkus Syrup................................................................................................. 46
Table 10. Manufacturing Steps of Linkus Syrup ......................................................................................... 47
Table 11. Formulation Parameters of Linkus Syrup................................................................................... 51
Table 12 . Composition of Linkus Lozenges ............................................................................................... 52
Table 13 .Plant Parts Used in Linkus Lozenges ......................................................................................... 52
Table 14 .Manufacturing Steps of Linkus Lozenges ................................................................................... 53
Table 15.Formulation Parameters of Linkus Lozengs................................................................................ 54
Table 16. Pharmacological Actions of Herbs............................................................................................. 63
Table 17. In-vitro Antioxidant Activity of Linkus Formulation................................................................... 84
Table 18. Linkus Syrup Reducing Ability with reference to Standard ........................................................ 84
Table 19. Antiurease Activity of Linkus Syrup with reference to Standard ................................................ 84
Table 20. Lipoxygenase Inhibiting Activity by Polyherbal Formulation Linkus. ....................................... 85
Table 21. Content of Linkus Syrup and its Anti-microbial Effects.............................................................. 85
Table 22: Zone of Inhibition on Sample A (Linkus Cough Syrup).............................................................. 87
Table 23: Zone of inhibition on Sample B (Linkus Cough Syrup) .............................................................. 87
Table 24. 1 gm /Kg Citric Acid + Linkus Extract on Female Rats ............................................................ 88
Table 25. 1 gm/kg Citric Acid+ Diphenhydramine and Acefyllin Piperazine ........................................... 89
Table 26. 1 gm/kg Citric Acid + Linkus Extract ........................................................................................ 89
Table 27: Citric Acid + Dextromethorphan, Diphenhydramine................................................................. 89
Table 28: Effect of Linkus Syrup on Body Weight (Dose 4 gm/kg)............................................................. 90
Table 29: Effect of Linkus Syrup on Biochemical Parameters (Dose 4 gm /kg)........................................ 91
Table 30: Effect of Linkus Syrup on Hematological Parameters (Dose 4 gm/ kg)..................................... 91
Table 31: Chronic Toxicity Effect of Linkus Syrup on Body Weight .......................................................... 92
Table 32. Average Weight of Body Organs................................................................................................ 93
xx

Table 33. Comparison of Toxic Effects on Lipid Profile ............................................................................ 93
Table 34. Comparison Of Hematological Toxicities .................................................................................. 94
Table 35. Comparison of Toxic Effects of Linkus Aminophylline & Acefyllin on Lipid Profile ................. 95
Table 36. Comparison First Visit (Day 1) versus Last day (Day 14) ......................................................... 96
Table 37. Comparison of the 5 Level Symptoms Criteria ........................................................................... 97
Table 38: Comparison of Side Effects all 3 Parallel Groups ..................................................................... 98
Table 39. Baseline Characteristics of Studied Sample ............................................................................... 99
Table 40. Inter Quartile Range Before and After the Treatment of Linkus .............................................. 100
Table 41. Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine......................... 101
Table 42: Inter Quartile Range Before and After the Treatment of Aminophylline ................................. 102
Table 43: Comparison (After – before) Linkus......................................................................................... 104
Table 44 : Comparison (After – Before) Acefyllin Piperazine.................................................................. 105
Table 45 : Comparison (After – Before) Dextromethorphan, Diphenhydramine ..................................... 105
xxi

1
CHAPTER 1
INTRODUCTION

2
1. CHAPTER ONE- INTRODUCTON
1.1.Cough:
Cough is a sudden reflex which can be produced because of aggravation in the respiratory
entry portrayed by a sound (1). It happens regularly in children(2) which can lead them to
consult the medicinal services clinics and utilization of over-the-counter cough and cold
medicines.(3). Therefore Health, Food and Drug Administration hence forth changed their
positions with respect to these items in 2008 on account of expanding concerns about the
safety and viability of these medicine in kids (4). In adverse reason and time, customers paid a
high sum to buy of such over the counter (OTC) medications to treat cough. That purchasing
OTC prescriptions afforded a credible evidence for the impact of these medications as such no
restorative option but turned out to be ideal (5, 6).
1.1.1 Acute Cough:
Intense cough mostly occurs because of the upper respiratory tract infection (7) and it can
prolong for 3 weeks. In 1999 in Australia, intense/acute cough required 7.5% general
consultation to be treated (8). It can rise grimness rate and indications like weariness,
sweating, urinary incontinence, rapines, musculoskeletal agony and sleep deprivation (9, 10).
Pain can be felt because of pressure applied on the organ frameworks the period during of
cough. Cough creates such antagonistic impacts that can interfere with a patient's normal life
(10).
1.1.2 Chronic Cough:
According to Australian (11) and the US cough rules, chronic unending cough in youngsters
is characterized as cough enduring >4 weeks. Intense and extended intense cough are
characterized as cough enduring <2 and 2-4 weeks, individually (12). Interestingly, British
rules characterize chronic cough in youngsters as cough enduring >8 weeks. Contemplates
have proposed that intense cough in youthful kids has determined by 3 weeks (13, 14) and
diminished the morbidity rate if the chronic cough is dealt with inside 30 days (15). The path
way of cough can be seen Figure 1,where in details schematic representation shown to
understand the subject matter and the potential steps involved are quite exclamatory.

3
Figure 1: Cough in Child and Length of Cough
3
Figure 1: Cough in Child and Length of Cough
3
Figure 1: Cough in Child and Length of Cough

4
1.1.2. Wet Versus Dry Cough:
Turbulence in the lapsed air creates a sound that prompts vibration of huge airways and
laryngeal structures went with emissions from inside the airways (16). The laminar move
through little airways is in capable of being heard. The sound of cough is likewise affected by
mucous (17). In kids, the secretion amount that produces wet cough is obscure. The terms
used to depict cough connected with lower airways secretions are "wet or moist" cough in
youngsters and "productive cough" in grown-ups. For insignificant or no lower airways
discharge secretions term "dry cough" is utilized. The wet and dry cough are the real sign and
manifestation to anticipate the specific cause and treatment of cough in kids (18, 19).
1.2.Pathophysiology of Cough:
The cough reaction and its industriousness should be known. The particulate matter or
mucous disfigures the airway epithelium which incites the vagal essential afferent nerves, for
example, bronchopulmonary quickly acting receptors present in larynx, trachea and carina
(20, 21). In the cognizant state chemicals, for example, bradykinin and capsaicin initiates the
bronchopulmonary C fibers prompting cough (22). Core tractus solitarius in the brainstem is
considered as cough core interest. In any case it is not all around acknowledged to be so.
Projections are made with different optional neurons those nuclei which are connected with
control of breathing (23).
Cough connected with the gastroesophageal reflux can be useful to comprehend the
instrument of cough incited by the refluxate (24) and the cough receptors of the upper airways
can be straightforwardly empowered by parts of the refluxate different sensory nerve
subtypes in the brain forms the focal refinement/central sensitization bringing about the
misrepresented/exaggerated reflexes (25). Cough reflex and its determination can be affected
by substance P (26), see Table 1.The releases of provocative go between, for example,
bradykinins and prostaglandins might be in direct interaction with the cough/hack receptors
and are relied upon to improve the cough reflex component (27, 28).In the table the chemical
irritants, osmotic/chloride diffucient solution, inflammatory mediators and mechanical agents
involved are depicted as reported into cough data.

5
Table 1. Agent that Induce Cough in Human beings
ChemicalIrritants
Osmotic/Chloride-deficient solutions
Inflammatorymediators
Mechanical Agents
Capsaicin Hypertonic saline solution Histamine Instrumentation
Citric Acid Distilled Water Prostaglandin E2 Lactose
Acetic Acid Sugar Solutions Prostaglandin F2α Aerosols
Tartaric Acid Urea Solutions Dust
Acetylcholine Bronchoconstriction
Nicotine
Metabisulfite
Sulfur dioxide
Data from Fuller RW.Cough 1991:1961-7
1.3. Etiology of Cough:
Cough is identified on the basis of its span. Intense cough goes on for 3 weeks. (29) Sub
intense cough has a term of 3 to 8 weeks.
1.3.1. Causes of Hack in Youngsters:
a).Infectious intense, sub-acute viral disease, mycoplasma, chlamydia, pneumocystitis and so
on. b).Chronic tuberculosis, non-TB mycobacterium and contagious contaminations. c).Cystic
fibrosis, ciliary dyskinesia, postpneumonia, immunodeficiency (essential or optional).
d).Asthma, postviral, nasal space infection, esinophilic bronchitis.
e).Aspiration: Primary: bulbar sores, laryngopalatal discoordination, cerebral paralysis, vocal
string paralysis. Secondary: gastro esophageal reflux. Anatomical: laryngeal split, trachea-
esophageal fistula, tonsil-adenoid hypertrophy.
f).Airway sores Primary; laryngomalacia, bronchomalacia, tracheomalacia. Secondary:
outside pressure (vascular slings, tumors and so on), intraluminal sores, remote body.
Pulmonary toxicants.Tobacco. Particulate matter and vaporous. Biomass ignition. Pulmonary
lung infection. Interstitial lung infection, pulmonary hypertension, pulmonary vascular clog,
tumors, congenital bronchiolitis of outset.
g).Angiotensin Converting Enzyme Inhibitors. (Expert inhibitors) h).Arrhythmias.
i).Psychogenic hack).Gastro-esophageal reflux without desire (30).

6
1.3.2. Causes of Acute Cough:
The unprecedented reasons for acute cough are pertussis and mycoplasma contamination.
Aspiratory embolus, cardiogenic aspiratory edema, pneumonia are life debilitating sicknesses
with are obvious to bring about acute cough. The treatment incorporates antitussive
specialists. Expectorants and mucolytic have not been turned out to be helpful. More current
era non-steadying antihistamines are less successful in decreasing acute cough than the older,
first-generation antihistamine-in addition to decongestant arrangements (30).
1.4.Clinical Assessment of Cough:
Regular cold alongside cough is self-restricting. Self-medicines are generally utilized by the
people (31-33). Smoking is firmly identified with the cough and it has turned into a routine in
the of smokers (34). Cough has turned into motivation to get restorative consideration that is
medical attention on immediate basis (35). Patients that need medicinal support regularly
report the issue of sleep deprivation and have turned out to be marginally more cognizant
(36). Severity of cough has led to vomiting, incontinence, syncope and has seriously had a
bad effect on the patient's quality life (37) see Table 2.
1.4.1 Clinical Assessment:
Throughout the clinical evaluation of cough history, length, sputum creation, cough
properties, smoking record and drug record should be calculated (38).
1.4.2 Substantial Examination:
The substantial examination can exhibit the indications of obstreperous lung infection, lung
malignancy, bronchiectasis, pneumonic fibrosis or heart disappointment, rhinitis and
pharyngitis, excited nasal mucosa, back pharynx and discharges (39). The 76 youthful grown-
ups with basic cold have been accounted for with lung illness after the high determination
with computer topographic (CT) finding (40). It is extremely basic to have intense cough in
pneumonia and in which physical examination incorporates bluntness on crackles on
auscultation. Bullous myringitis in patients with a Mycoplasma pneumonia tainting and sub-
conjunctival hemorrhages every so often appeared on the examination.

7
Table 2: Causes of Assessment of Acute Cough
Yes
No
No
Yes
No
Consider an
Additional
diagnosis acting
simultaneously
History of Physical Examination
Is Patient taking on ACE-I?Stop ACE-Iand consideralternative to
ACE-I Reviewin 3 monthsChest radiograph
Spirometry +Reversibility testing (hospital setting)Home PEF Recording (general practice or
spirometry unavailable)
Any obvious primary pulmonary pathology?
Is patient currently taking any therapy forcough?
Does patient have a symptomcomplex suggestive of PNDS or
GORDS?
Diagnostic testing in thefollowing order:1. PNDS2. Asthma-induced sputum ifbronchoprovacation3.GORD
Manage according totreatment guidelines
Cough stillpresent
Coughresolved
Empirical trial oftherapy
Review
Stop therapy
Coughworse
Coughpersists
Reintroducetherapy,ensure
compliance,maximize dose and cinsideradditional diagnosis
Review
Partialresolution
No resolution
Additional investigation:Fibre-opticbronchoscop,high-resolution CT
thorax,cardic studies,paychlatric appraisal
Completeresolution
Cough stillpresent
Coughresolved
Diagnostic testing 'Empiricaltherapy

8
1.5. Prevalence of Cough:
In Pakistan, cough has been the major purpose behind increasing patient's visit to the
outpatient division (41). Cough can prompt anatomical and physiological problems and
complications.
1.5.1 Epidemiological Studies of Cough in Pakistan:
1.5.2 Measurement of Cough:
The position and seriousness of cough must be checked in order to assess the infection and
sickness state. A direct cough side effect score scale has been broadly used to gauge the
seriousness of cough (50, 51).
Following points should be followed to measure the severity:
1. Patient Clinical record
2. Symptom score of cough symptom (see Table 3)
3. Quality of life Cough-specific
4. Ambulatory counts of cough
5. Ambulatory intensity of cough
6. Spectral assessment of cough resonance
7. Cough feeling (citric acid or capsaicin)
As reported by United Nations, In Pakistan 18,000 people die every year from air borne
pollution (42). The population of microorganisms has been increase largely in number from
hot to humid climate (43). In previous years of Karachi, it was concluded that Nasal allergies
have increase rapidly (44). Due to continuous changing in Environment, the causation factor
of respiratory infections has specialty focused(44, 45). In spite of continuously attention on
cough and associated factors, No data were available in epidemics at Karachi. Researchers are
striving to come up with the evidence and results on the progressive condition in various areas
of Karachi (46). In another study it was revealed that the cough and its types have been high
in specific occupations included Gem cutters, textile workers and those who involves in brick
kilns (47, 48). However in Rural areas of Karachi, cough lasting > 2 weeks and leads to major
pulmonary issues (49).

9
Time Severity Score
Day time
No cough 0
Cough for more than one short period 1
Cough for more than two short periods 2
Frequent cough not interfering with usual activities 3
Frequent cough interfering with usual activities 4
Distressing cough most of the day 5
Night time
No cough 0
Cough on walking only/cough on going to sleep 1
Awoken once or woken early due to coughing 2
Frequent waking due to coughing 3
Frequent coughs most of the night 4
Distressing cough 5
1.5.3 Monitoring Cough Counts:
For the evaluation of various illnesses due to cough and its adequacy of treatment ought to be
measure quantitatively (52-57). The cough number measuring technique have been utilized to
record cough during sitting position and for shorter timeframe (58).
1.5.4 Cough Evaluation in Children:
Arrangement of cough of respiratory ailment that can be exceptionally irritating and meddling
in rest and can be an indication of a fundamental infection. The etiology and right
determination of cough is of prime significance for a consultants and physician. Cough has
been arranged into below classifications: (58)
Table 3. Cough Sympton Score

10
Common (Normal).
A serious sickness, for example, cystic fibrosis.
A flip yet possible cause.
A child among an asthma disorder.
Overestimation of manifestations for mental or different reasons by either or both
youngster or family.
A non-respiratory cause, for example, periodic or habitual cough, interventions,
medications (ACE inhibitors), and so forth.
1.6. Observing Cough Counts:
The measurable sound track of cough over a delegate timeframe is important for the target
assessment of cough connected with various diseases in addition for the evaluation of the
competence of various treatments for chronic cough. Primary strategies documented cough in
non-ambulatory patients, generally restricted to brief timeframes. An assortment of techniques
have been created at first soundtrack of cough in the non-wandering subject although sitting
in a room in addition to normally constrained to brief timeframes by taking an eyewitness
consider cough sounds occur. Such soundtracks are restricted in light of the fact that the
patients are not presented to the assumed jussive jolts that they experience in their day by day
exercises. Perceiving of patients by cold though sitting in a room establishes that cough
checks reduction altogether over the initial 1 hour (58).
1.6.1 Assessment in Children
Cough is an extremely basic manifestation of respiratory disease. Cough is capable of being
heard and can meddle with rest and may speak to genuine fundamental issue, for example,
fibrosis in cysts , which is not amazing that custodians are regularly on edge when taking with
kids ‘Cough and frequently look for restorative counsel and cure. Parental concerns may
contrast fundamentally from doctors' worries. Doctors are typically worried around the
etiology of Cough in addition to getting the right finding. Maternal concerns, notwithstanding,
regularly identify with their apparent impacts of hack on their tyke (rest, gagging, changeless
mid-section damage) (59). In choosing the etiology of the tyke's Cough, Bush proposes that
the youngster's hack can be put in the classifications as under:

11
Common (Normal)
A serious sickness, for example, cystic fibrosis (uncommon yet key to get right).
An unserious yet treatable cause.
A kid with an asthma disorder.
Overestimation of manifestations for mental or different reasons by either or both
youngster or family.
A non-respiratory cause, for example, periodic or habitual cough, interventions,
medications (ACE inhibitors), and so forth.
1.7. Antimicrobial Assessment of Cough Syrup:
Antimicrobial action of extracts of indigenous cough combinations on upper respiratory tract
(URT) bacterial pathogens are mentioned as follows (60).
Figure 2. Klebsiella pneumoniae
Figure 3. Pseudomonas aeruginosa
11
Common (Normal)
A serious sickness, for example, cystic fibrosis (uncommon yet key to get right).
An unserious yet treatable cause.
A kid with an asthma disorder.
Overestimation of manifestations for mental or different reasons by either or both
youngster or family.
A non-respiratory cause, for example, periodic or habitual cough, interventions,
medications (ACE inhibitors), and so forth.
1.7. Antimicrobial Assessment of Cough Syrup:
Antimicrobial action of extracts of indigenous cough combinations on upper respiratory tract
(URT) bacterial pathogens are mentioned as follows (60).
Figure 2. Klebsiella pneumoniae
Figure 3. Pseudomonas aeruginosa
11
Common (Normal)
A serious sickness, for example, cystic fibrosis (uncommon yet key to get right).
An unserious yet treatable cause.
A kid with an asthma disorder.
Overestimation of manifestations for mental or different reasons by either or both
youngster or family.
A non-respiratory cause, for example, periodic or habitual cough, interventions,
medications (ACE inhibitors), and so forth.
1.7. Antimicrobial Assessment of Cough Syrup:
Antimicrobial action of extracts of indigenous cough combinations on upper respiratory tract
(URT) bacterial pathogens are mentioned as follows (60).
Figure 2. Klebsiella pneumoniae
Figure 3. Pseudomonas aeruginosa

12
Figure 4. Staphylococcus aureus
Figure 5. Enterococcus faecalis
Figure 6. Escherichia coli
12
Figure 4. Staphylococcus aureus
Figure 5. Enterococcus faecalis
Figure 6. Escherichia coli
12
Figure 4. Staphylococcus aureus
Figure 5. Enterococcus faecalis
Figure 6. Escherichia coli

13
Figure 7. Salmonella spp
Figure 8. Salmonella paratyphi
1.8.Quality Parameters with Standardization of Herbal Crude Drugs:
1.8.1 Processes and Procedures:
WHO has set up the guidelines for the standardization in addition to quality control of herbal
drugs? This includes the selection, handling of crude drugs, evaluation and documentation of
the safety, efficacy and risks of the final product provided by the consumer. Following tests
are required to be performed in order to evaluate thy quality of both the crude drug and
finished herbal product.
Microscopic examination: Use to identify the adulterants.
Extraneous organic matter: In order to get the pure form of a drug, identification and
removal of the foreign particle is necessary.
13
Figure 7. Salmonella spp
Figure 8. Salmonella paratyphi
1.8.Quality Parameters with Standardization of Herbal Crude Drugs:
1.8.1 Processes and Procedures:
WHO has set up the guidelines for the standardization in addition to quality control of herbal
drugs? This includes the selection, handling of crude drugs, evaluation and documentation of
the safety, efficacy and risks of the final product provided by the consumer. Following tests
are required to be performed in order to evaluate thy quality of both the crude drug and
finished herbal product.
Microscopic examination: Use to identify the adulterants.
Extraneous organic matter: In order to get the pure form of a drug, identification and
removal of the foreign particle is necessary.
13
Figure 7. Salmonella spp
Figure 8. Salmonella paratyphi
1.8.Quality Parameters with Standardization of Herbal Crude Drugs:
1.8.1 Processes and Procedures:
WHO has set up the guidelines for the standardization in addition to quality control of herbal
drugs? This includes the selection, handling of crude drugs, evaluation and documentation of
the safety, efficacy and risks of the final product provided by the consumer. Following tests
are required to be performed in order to evaluate thy quality of both the crude drug and
finished herbal product.
Microscopic examination: Use to identify the adulterants.
Extraneous organic matter: In order to get the pure form of a drug, identification and
removal of the foreign particle is necessary.

14
Ash values: the purity of the drug can be identified by the help of the ash values, total
ash, sulfated ash and acid insoluble ash.
Moisture content: To get the actual weight of the crude drug, the moisture content is
evaluated. It is observed that the drug or product having low moisture content is less
likely to get degraded.
Extractive values: After the crude drug has undergone different solvent environments
these are values are obtained.
Crude fiber: Use to identify woody material in order to evaluate the purity of the
crude drug.
Qualitative chemical assessment: The crude drugs are identified and characterized on
the basis of phytochemical constituents present in the drug. Different analytical
techniques, phytochemical screenings are applied to identify and isolate the active drug
constituents who are extracted and made to use for pharmaceutical preparations.
Chromatographic investigation: On the basis of major chemical constituents, the
crude drugs are identified.
Quantitative chemical assessment: It is use to evaluate the amount of major
constituents.
Toxicological studies: The toxicological studies are important to determine the
residues, toxic elements, lethal dose and microbial assay which help to identify the
absence or presence of harmful microorganisms.
The mentioned characteristics on page 14 features for standardization include a wide variety
of techniques such as:
1.8.2 Physical Evaluation:
The physical evaluation is accomplished by evaluating the physical characteristics of plants
along with their images in order to get a visual document of the drug. This helps to ensure to
identity and purity of drug.
1.8.3 Microscopic Evaluation:
It is applied to get the complete and detailed examination of the crude drug. However, it is
inapplicable if performed at the initial stages for the impurity testing.

15
1.8.4 Chemical Evaluation:
The chemical constituents are screened, identified, isolated and purified to get the vegetable
material of its active principles. This may include color reaction test to establish the identity
and purity of the drug.
1.8.5 Biological Evaluation:
Biological assays are performed on animals (intact or their organs) to assess the
pharmacological activity of the drug.
1.8.6 Purity Determination:
It is used to determine the purity of the drug substance.
1.8.7 Analytical Methods:
Basic to consistence by any monograph standard quality is the requirement for fitting
expository techniques for deciding character, quality, and relative strength. There are a plenty
of explanatory strategies accessible. In that way, it is frequently hard to know which the
maximum suitable to utilize is, yet basic amongst know is the analytical apparatuses in which
monograph institutionalization used on basis of chromatography.
1.8.8 Chromatography:
Chromatography is a technique employed to isolate the molecules of the compound on the
basis of their structure and composition. The test material is run over the stationary bed and
after different types of interaction similar molecules are separated. The molecules which
move slowly have strong interaction with the stationary bed and those molecules which have
weaker interactions move faster. Immobilized silica on glass plates (thin layer
chromatography), very sensitive High Performance Thin Layer Chromatography
(HPTLC), volatile gases (gas chromatography), paper (paper chromatography), and
liquids which may incorporate hydrophilic, insoluble molecules (liquid chromatography)
are widely used as stationary supports. HPTLC is mostly employed in determining the amount
of constituents of the botanical materials. The samples can then be analyzed by observing
them on different wave lengths in order to get the more accurate finding on that plant. It is a
time saving analytical method because a number of samples can be run simultaneously.

16
1.8.9 Quantitative Analysis:
Quantitative methods are used to get the amount of compounds that have some
pharmacological activities that exhibit the efficiency parameters (61, 62).
1.8.10 Resurgence of Herbal Medicines:
The plant extracts in the herbal medicines contains various constituents that can have a
synergistic effect.
o Following are the reason of resurgence of the herbal medicines among the people:
o Plant based medicines have been proven to be effective.
o Used as an alternative therapy for the allopathic medicines.
o Less side effects no adverse effects and more economical.
o Extraction Technologies have been used to improve the efficacy and quality of theherbal medicines.
o Self-medication has increased in the use of herbal medicines among the patients (63).
Reasons like herbal medicines are safer, more effective and offer more cure and promote
health and prevent disease as compared to orthodox medicine, it is these reasons increased the
public interest for the use of herbal medicines.
Unlike pharmaceutical products, herbal medicines have now been evaluated for clinical
efficiency and quality product as evidence based medicine.
The following points can be helpful in the better understanding of the resurgence of the herbal
medicines:
o Herbal medicines are being used by the patient as the socio-culture onset for the health
awareness.
o Bears less side effects or adverse drug reaction and in expensive than the modern
medicines it is with these reasons the WHO has acclaimed that 67.3% of the
population of the world use traditional medicines in their primary health care.
o Easily available in both modern and Unani dosage form design (64).

17
1.9. History of Use of Traditional Herbal Medicines:
The use of herbal remedies includes a detailed usage of medicines which are mostly
appropriate to be used for the preparation of many products. In the developing countries, a
considerable amount of population has faith in the traditional medicines and their related
products and resources to fulfill the health care requirements. The herbal medicines run along
with the modern medicines because of social and cultural reasons. These products have been
widely available the crude out the developing countries. In such high profile settings, the
herbal medicines are used for those purposes they were not thought to be used. Like in the
case of ephedra (=Ma huang) which is used to lose weight or to improve the athletic
performance (65). While in the other countries the manufacturing of the herbal medicines is
quite accurate. However it’s not followed ubiquitously. The herbal remedies are termed as
“phyto remedies” in German and they are sold by following the similar standards of
effectiveness and superiority like the additional medicines but in developed countries, the case
is slightly different. The herbal remedies are advertised, promoted and sold as nutritional
complements, a class of products that are not endangered to pre-approval for any of these
standards. These points are discussed further below.
1.9.1 Herbal Remedies for Healing:
The modern behavior of sickness underway prior with the practices of herbs (66). These herbs
or aromatic plants have been used normally for healing purpose since time immemorial.
1.9.2 Traditional Chinese Medicine:
From ancient times, traditional Chinese medicines have been used by the Chinese people.
Despite the animals and mineral materials, herbals are a major source of the remedies.
Additional 12000 crops castoff by outdated naturopaths , around 500 are in communal
usage (67). The botanical crops are castoff and subsequently they have experienced the
procedures like mix singing or absorbing vinegar or wine. In the clinical practice,
complex medicines are used for traditional and individualized care. Traditional Chinese
prescriptions are still use in the same manner in China.

18
Most of the population use traditional medicines and it is getting higher in the country
sides. Almost 4 hundred thousand plus traditional medicines are accessible from China
that represents around 1/5 of the entire Chinese pharmacological business sector. It is
with these reason the traditional Chinese system has gained momentum, and China is the
largest producer of these medicine (67).
1.9.3 Japanese Customary Prescription:
A large number of traditional medicines have been adopted by the Japanese system of
traditional healing known as Kampo-Yaku. In 9th Century local herbs of this country was
named top pharmacopeia of “Traditional Japanese Medication” Japan has develop their
customary traditional medicines and it is being practiced to ward of ailment in modern
days hospital. Japan in many respect has given priority to execute quality research in
herbal medicines to treat both acute and chronic disease (68).
1.9.4 Indian Customary Solution:
Ayurveda is the medical practice system entrenched in India and the land of India has been
known about the use of medicinal herbs for almost 5 thousand years in ambiguity. It
encompasses of nourishment including the dietary food as well as herbal remedies however
when focusing on the physique, brain and soul in the remedy or treatment. India is gaining
popularity to produce medicinal and health care product and has developed Indian system of
medicine that include Ayurveda, Unani, Siddha and homeopathy to cover health for all (69).
1.9.5 Patterns Being Used:
Many data has been available throughout the globe on about plant industry and their frequent
uses as mention in Table 4 which shows the global nutrition products industry including
herbal and botanical products during the year 1999.table shows country wide financial values
they spend. USA and Europe is the biggest consumer of herbal products. Asia is also one of
the leading continents where herbal medicines used for curing sickness, Japan as individual
country is very famous for herbal treatments. This can clearly been observed in the data
shown in table 4.

19
Table 4: The global nutrition products industry in 1999, including herbal and botanicalproducts” (in millions of US $) (70)
CountryVitamins
/Minerals
Herb/botanicals
Sports, mealreplacement,homeopathy,
specially
Naturalfoods
Naturalpersonal
care
Functionalfoods
Total
USA 7070 4070 4320 9470 3590 16080 44600
Europe 5670 6690 2510 8280 3660 15390 42200
Japan 3200 2340 1280 2410 2090 11830 23150
Canada 510 380 250 700 330 1500 3670
Asia 1490 3170 970 710 880 1450 8670
Latin America 690 260 250 460 250 360 2270
Australia & NewZealand
300 190 90 340 140 540 1600
East. Europe &Russian Fed.
350 220 250 180 40 269 1309
Middle East 180 90 60 70 30 140 570
Africa 160 80 70 80 10 120 520
Total Global 19620 17490 10050 22700 11020 47679 128559
Sales of dietary supplement products, including herbal products and herbal supplements, in
the USA increased drastically during the 1990s, fortified in the last part of the decade by the
Dietary Herbal products have a vast variety that’s why the sales of herbal and nutritional
products has been increase in 20th century and being continuously increase in American
market during 1990s. The Health education act of dietary supplement 1994 has fortified the
use of herbal medications (DSHEA)(70). The example of development has been available as
shown in table 5.In the monograph of European Union (EU) all herbal products and their
remedies are mentioned for market the drug and as controlled medication however the

20
products which is not found in the monograph considered to be the nutritional and dietary
products or cosmetics.
For the herbal market the drug make more investigative and aligned for herbal market. All
indication that has been made on herbs are specifically classified ,their mechanism of action
has been knows as other modern pharmacological products (71).
Table 5: Trends in the global nutrition products industry, 1997–2000” (in millions of US $)(70)
Description 1997 1998 1999 2000
Vitamins / Minerals 18000 18870 19620 20440
Herb/ botanicals 15990 16980 17490 18070
Sports, meal replacement,homeopathy, specially
8760 9310 9960 10710
Natural foods 16690 19910 22700 25420
Natural personal care 9620 10280 11020 11850
Functional foods 40320 43940 47670 51480
Total 109380 119290 128460 137970
In the last century when the “Dietary Supplements Health and Education Act (DSHEA)” was
approved near about half of the population across the nation was using the dietary
supplements and often business is about 4 billion. The sales have been increasing widely
including vitamins, minerals and other herbal products on different areas of the world. In the
year of 2000 most of the data are available and the sales of the herbal and dietary products
have been increase near about $15 billion; which represents almost 33% of the sales .As per
Table 6 the pattern of herbal supplements from 1997 to 2000 has been shown.

21
Table 6: Top Selling Herbs in US, (in million USD) (70)
Description 1997 1998 1999 2000
Combination herbs 1659 1762 1740 1821
Ginkgo biloba 227 300 298 248
Echinacea 203 208 214 210
Garlic (Allium sativa) 216 198 176 174
Ginseng 228 217 192 173
St John wort (Hypericum perforatum) 100 308 233 170
Saw palmetto (Serenoa repens) 86 105 117 131
Soy (soya) NA NA 36 61
Valerian (Valeriana officinalis) 30 41 57 58
Kava-kava 22 44 70 53
Total herbal supplements NA NA 4070 4130
The traditional and herbal medicine has largely been used in Canada. Berger (64)
distinguished, in exactness the significances of a 2001 study of 2500 Humans, in which the
participants were 15 years old and older, those herbal treatments were castoff by 38% of
respondents in 1999. A study in 1998 of the most well-known treatments testified in Canada
is given in Table 7.
Table 7: Top 10 Most Famous Herbal Solutions in Canada (70)
Herb% who use among
herbal users% users in
generalpopulation
Echinacea 54 19
Garlic (Allium sativa) 52 18
Ginseng 42 15
Chamomile (Chamomilla recutita) 38 13
Ginkgo biloba 20 7
Evening primrose (Oenothera biennis) 20 7
Devil's claw (Harpagoghytum procumbens) 17 6
St John wort (Hypericum perforatum) 17 6
Tea tree oil (Melaleuca alterifolia)15 5
Valerian (Valeriana officinalis) 13 5

22
In 1994, the herbal drug business of Europe sector was worth over “US dollar 2.8 billion at trade
selling costs. In spite of the fact that the UK business sector was lower than that of Germany, it had
one of the most important estimate growth the rates in Europe (72).
1.10. Awareness, Regulation, Control on Use:
1.10.1 WHO Recommendations for Herbal Medicines:
In 1992, the Office of WHO for the Region of Western Pacific respected a social affair of
professionals to arrange rule and regular rules to demonstrate research take a shot at assessing
natural things (73). 'A few regular drugs have examined and tried, in any case others are used
fundamentally for routine motivations to ensure, reestablish, or enhance suitability. Most
common things still should be engaged cleverly; paying little respect to the way that the
experience picked up from their traditional utilizes the rough out the years ought not to be
released. As there is lacking confirmation passed on by normal investigative ways to deal with
oversee answer solicitation of reasonability and sufficiency about by a long shot the greater
part of the home developed things now being used. The record covers such focuses as
traditions for clinical studies connected on customary things, reviewing home developed
arrangement assessment, rules for quality determinations of plant materials and game plans,
and principles for pharm coactive and general pharmacological examinations of home
developed things and for ruinous tendency evaluations of home developed things. WHO has
moreover issued Guidelines for the assessment of Herbal Medicines (74). The standards
portrayed the key criteria for the assessment of worth, and sufficiency of normal things with
the purpose of helping national managerial forces, honest to goodness affiliations and creators
in looking over documentation, entries and dossiers in vitality about such things. It was
prescribed that such evaluations consider whole deal use in the nation, any delineation in the
remedial and pharmaceutical structure or commensurate sources or documentation of data on
the use of a home developed solutions, and advancing supports for all intents and purposes
indistinguishable things. Yet postponed and clearly uneventful use of a substance generally
evidence of its suitability, evaluation of the harmful nature of truly episode substances may
reveal until now unsuspected issues. It was correspondingly proposed that managerial forces
can react right away to new information on lethality by assessing or compelling the licenses of

23
enlisted things containing suspect substances, or by naming the substances to keep their use to
restorative cure. The precepts focused on the essential for appraisal of reasonability including
the determination of pharmacological and clinical effects of the dynamic fixings, and
stamping which fuses a quantitative once-over of element ingredient(s), dosage, and
contraindications.
1.10.2 The European Union:
The Association of European Pharmaceutical Grand Public has completed a study for the
European Commission on natural items restorative items in the European Union (EU)
(71).The significance of natural items differs nation to nation. These items are not a
homogeneous gathering. For the most part, they are either totally approved helpful items with
viability showed by clinical studies or by references to circulated exploratory composition
(75). On the other hand are accessible as items with a demonstrated adequacy as per by their
nearby utilize.
1.10.3 Classification of Herbal Medicinal Goods:
According to European Economic Community Council Directive 65/65/EEC (75) which has
been actualized in national law in all Member States, therapeutic products require prior
marketing approval before accessing the business sector. In all Member States, herbal
restorative products are considered as therapeutic products, and are, on a basic level, subject
to the general regulations for medicines as set down in the different national pharmaceutical
laws. As a rule, a specific meaning of herbal products is available, which is in accordance
with the EU Guideline 'Nature of Herbal Medicinal Products'. This includes plants, parts of
plants and their preparations, generally gave restorative or prophylactic cases. Different
groups of therapeutic products containing plant preparations exist or are being made. For
example, draft enactment in Spain includes the definitions 'herbal products' and
'phytotraditional products'. The last are not considered as 'pharmaceutical claims to fame's
also, thus are not classified as herbal medicinal products.
1.10.4 Classification of Herbal Products:
By and large, grown herbal items are grouped helpful items if they apply therapeutic or
prophylactic symptoms, and are not marked as remedial items when they won't make these

24
product cases. Items not grouped remedial when in doubt have a spot with the dietary
supplement or beauty care products ranges, despite the way that they as a less than
dependable rule can be advertised as supplement for dietary. Particular categories of non-
traditional plant items exist in some Member States, for instance, the claimed 'supportive
supplement items' in Austria. In Spain , Ireland and UK, there exist arrangements portrayed as
remedial items, which are under particular conditions absolved from allowing powers of these
cases was generally great (76).
1.10.5 Market of Herbal Medicine Scenario in Pakistan
In Pakistan traditional medicine have been a strong bit of our social legacy and expecting an
essential part in giving therapeutic administrations to a broad part of the population.
Fundamentally the major focused area in Pakistani market are Tibb-e-Unani, Ayurveda and
Homeopathy and Chinese Traditional System however Reiki, Acupuncture and aroma
therapy treatment has been displayed in certain parts of the country in the latest couple of
years (77)
As per WHO tag line “Health for all” in 2000, the Government of Pakistan in last two
decades for giving a broad and reasonable equitable health care administrations to each and
every Pakistani national and has reported its official methodology on Traditional Medicines
(TRM) as a part of National Health Policy.
As per National Health Policy 2001 some amendments of Unani, Ayurveda and Homeopathic
(UAH) Act of 1965 has been suggested which has now been incorporated for the successful
future of traditional alternative medicine. The trend of Pakistani population shows that 51%
population prefer to use Traditional and complementary medication while 48% percent picked
biomedicine. Population who chose TCAM 20% utilized biomedicine likewise; 16%
homeopathy, 12% Unani pharmaceutical, 2% mind– body, less than one percent herbal based
practices (home cures, eating regimen and dietary supplement) then 1% imperativeness
pharmaceutical (Reiki), < 1% Traditional Chinese Medicine, and afterward 1% aromatherapy
(78). However the research of TCAM has not been fully established for sustainable growth of
floral wealth. Continuous effort and precise target can enhance the scenario in current
scenario of Pakistan.

25
CHAPTER 2
LITERATURE STUDY

26
2. CHAPTER TWO - LITERATURE STUDY
In this chapter detail literature of different herbs related to the cough is being discussed along with
their chemical structure, their description of plants and their pictorial also added for better
understanding.
Total of seven herbs addressed which used in the formation of linkus which are as follows.
1. Adhatoda vasica Nees, 2. Piper longum Linn,
3. Glycyrrhiza glabra Linn 4. Alpinia galangal (L.)
5. Hyssopus officinalis 6. Cordia latifolia Linn
7. Viola odorata Linn
2.1. Adhatoda vasica Nees:
Adhatoda vasica Nees is related to Acanthaceae family generally recognized as Adosa.
Mostly Adosa is originate in several parts of India and also available in different regions of
the world, with a multiple use of conventional Ayurveda. Vasica is very well-recognized and
effective in circumstances of respiratory treatment. The fresh leaves of Vasica are
masticating, at times with, by yogis, sadhus or ginger, as they had a very stimulant results on
the system of respiratory. Vasica is an expectorant and antispasmodic, and had a reputation of
been successful for century’s once treat asthma, enduring bronchitis, also additional
respirational circumstances (79).
2.1.1 Plant Description:
Adhatoda vasica Nees is a part of the medicinal family of Acanthaceae. It is a shrub of one to
three feet height consists of opposite long evergreen branches. Its Leaves was large and
shaped like a lance. Below is a woody Stem and above part is herbaceous. exstipulate and
opposite leaves. Flower shapes spikes or sometime panicles, bisexual, small irregular
zygomorphic, and hypogynous (80) . It had four seeded fruits like capsular. Normally flowers
are either in purple or white color. The trade name is Vasaka which is Sanskrit name based
(81). Inflorescences in axillary spicate cymes, heavily flowered; peduncles short; bracts
broadly ovate, foliaceous. The parts of plants like flowers, leaves, fruit and roots are widely

27
draw on for curing whooping cough, cold cough, chronic bronchitis and asthma, as sedative,
antispasmodic and expectorant (82).
Figure 9.Adhatoda vasica Nees (Whole Plant)
Figure 10. Fresh Leaves of Adhatoda vasica Nees.
27
draw on for curing whooping cough, cold cough, chronic bronchitis and asthma, as sedative,
antispasmodic and expectorant (82).
Figure 9.Adhatoda vasica Nees (Whole Plant)
Figure 10. Fresh Leaves of Adhatoda vasica Nees.
27
draw on for curing whooping cough, cold cough, chronic bronchitis and asthma, as sedative,
antispasmodic and expectorant (82).
Figure 9.Adhatoda vasica Nees (Whole Plant)
Figure 10. Fresh Leaves of Adhatoda vasica Nees.

28
Figure 11. Flower of Adhatoda vasica Nees.
2.1.2 Phytochemistry:
The inconceivable assortment of pharmacological use of Adhatoda vasica is accepted to be
the output of its rich grouping of alkaloids (83, 84). In Adhatoda vasica the alkaloid found in
leaves is the quinazoline alkaloid which is termed as vasicine (85).
Figure 12. Chemical Structure of Vasicine
2.2.Piper longum Linn:
An alkaloid is Piperine presented in plants belong to the family of Piperaceae, best example is
Piper nigrum L (86) , also recognized as dark pepper . Piperine is generally utilized as a part
of different home grown hack syrups for its powerful against tussive action in addition to
having bronchodilator properties (87). The dried juvenile foods and the ground root as
28
Figure 11. Flower of Adhatoda vasica Nees.
2.1.2 Phytochemistry:
The inconceivable assortment of pharmacological use of Adhatoda vasica is accepted to be
the output of its rich grouping of alkaloids (83, 84). In Adhatoda vasica the alkaloid found in
leaves is the quinazoline alkaloid which is termed as vasicine (85).
Figure 12. Chemical Structure of Vasicine
2.2.Piper longum Linn:
An alkaloid is Piperine presented in plants belong to the family of Piperaceae, best example is
Piper nigrum L (86) , also recognized as dark pepper . Piperine is generally utilized as a part
of different home grown hack syrups for its powerful against tussive action in addition to
having bronchodilator properties (87). The dried juvenile foods and the ground root as
28
Figure 11. Flower of Adhatoda vasica Nees.
2.1.2 Phytochemistry:
The inconceivable assortment of pharmacological use of Adhatoda vasica is accepted to be
the output of its rich grouping of alkaloids (83, 84). In Adhatoda vasica the alkaloid found in
leaves is the quinazoline alkaloid which is termed as vasicine (85).
Figure 12. Chemical Structure of Vasicine
2.2.Piper longum Linn:
An alkaloid is Piperine presented in plants belong to the family of Piperaceae, best example is
Piper nigrum L (86) , also recognized as dark pepper . Piperine is generally utilized as a part
of different home grown hack syrups for its powerful against tussive action in addition to
having bronchodilator properties (87). The dried juvenile foods and the ground root as

29
decoction are broadly utilized as a part of intense and interminable bronchitis appeared with
cough and found to give progressive help in all cases (88).
2.2.1 Plant Description:
The Piper longum Linn is a thin, moving, underneath bush, crawling and establishing root
underneath. The undeveloped shoots are in down position; length of the shrubberies are five
to nine centimeter with five centimeter of width, praise, cordite by comprehensive adjusted
projections on the base, deputize-intense, . The plant exhibit uni-sexual blooms in introverted,
rigid thorns amid before soon afterward blustery season. The virile spines stand bigger, thin in
addition with the length of 0.0025 to 0.0075 m, however the female spikes are in length
between two centimeter when in blossom, increasing about three centimeter when in fruitlet
(89).The fruit is orange ,ovoid, , waterlogged in thick rachis around 0.002 m in distance
across (90).
Figure 13. Fresh Leaves of Piper longum
Figure 14. Unripe Fruit of Piper longum
29
decoction are broadly utilized as a part of intense and interminable bronchitis appeared with
cough and found to give progressive help in all cases (88).
2.2.1 Plant Description:
The Piper longum Linn is a thin, moving, underneath bush, crawling and establishing root
underneath. The undeveloped shoots are in down position; length of the shrubberies are five
to nine centimeter with five centimeter of width, praise, cordite by comprehensive adjusted
projections on the base, deputize-intense, . The plant exhibit uni-sexual blooms in introverted,
rigid thorns amid before soon afterward blustery season. The virile spines stand bigger, thin in
addition with the length of 0.0025 to 0.0075 m, however the female spikes are in length
between two centimeter when in blossom, increasing about three centimeter when in fruitlet
(89).The fruit is orange ,ovoid, , waterlogged in thick rachis around 0.002 m in distance
across (90).
Figure 13. Fresh Leaves of Piper longum
Figure 14. Unripe Fruit of Piper longum
29
decoction are broadly utilized as a part of intense and interminable bronchitis appeared with
cough and found to give progressive help in all cases (88).
2.2.1 Plant Description:
The Piper longum Linn is a thin, moving, underneath bush, crawling and establishing root
underneath. The undeveloped shoots are in down position; length of the shrubberies are five
to nine centimeter with five centimeter of width, praise, cordite by comprehensive adjusted
projections on the base, deputize-intense, . The plant exhibit uni-sexual blooms in introverted,
rigid thorns amid before soon afterward blustery season. The virile spines stand bigger, thin in
addition with the length of 0.0025 to 0.0075 m, however the female spikes are in length
between two centimeter when in blossom, increasing about three centimeter when in fruitlet
(89).The fruit is orange ,ovoid, , waterlogged in thick rachis around 0.002 m in distance
across (90).
Figure 13. Fresh Leaves of Piper longum
Figure 14. Unripe Fruit of Piper longum

30
2.2.2 Photochemistry:
The natural products like fruit gave constructive tests for the occurrence of oil which is
volatile, having arrowroot , protein and sweeties, alkaloids, saponin, as well as amygdalin
though not any tannins (91). Real substance ingredients are alkaloids piperlongumine,
piperine, , piperlonguminine furthermore methyl-3, 4, 5 –trimehoxycinnamate (92)
Figure 16.Chemical Structure of Piperine
2.3.Glycyrrhiza glabra Linn:
Glycyrrhiza is a Greek word termed as glykos, which means sweet, and rhiza, which means
root have a place with family Leguminosae. several quantities of customary healers have
guaranteed the efficacy of Glycyrrhiza species for an assortment of pathological/neurotic
conditions as a choleretic, diuretic and utilized as bug spray and showed as a part of
conventional prescription for cough, colds and difficult swellings (93). Customarily the plant
Figure 15. Dried mature fruit of Piper longum
30
2.2.2 Photochemistry:
The natural products like fruit gave constructive tests for the occurrence of oil which is
volatile, having arrowroot , protein and sweeties, alkaloids, saponin, as well as amygdalin
though not any tannins (91). Real substance ingredients are alkaloids piperlongumine,
piperine, , piperlonguminine furthermore methyl-3, 4, 5 –trimehoxycinnamate (92)
Figure 16.Chemical Structure of Piperine
2.3.Glycyrrhiza glabra Linn:
Glycyrrhiza is a Greek word termed as glykos, which means sweet, and rhiza, which means
root have a place with family Leguminosae. several quantities of customary healers have
guaranteed the efficacy of Glycyrrhiza species for an assortment of pathological/neurotic
conditions as a choleretic, diuretic and utilized as bug spray and showed as a part of
conventional prescription for cough, colds and difficult swellings (93). Customarily the plant
Figure 15. Dried mature fruit of Piper longum
30
2.2.2 Photochemistry:
The natural products like fruit gave constructive tests for the occurrence of oil which is
volatile, having arrowroot , protein and sweeties, alkaloids, saponin, as well as amygdalin
though not any tannins (91). Real substance ingredients are alkaloids piperlongumine,
piperine, , piperlonguminine furthermore methyl-3, 4, 5 –trimehoxycinnamate (92)
Figure 16.Chemical Structure of Piperine
2.3.Glycyrrhiza glabra Linn:
Glycyrrhiza is a Greek word termed as glykos, which means sweet, and rhiza, which means
root have a place with family Leguminosae. several quantities of customary healers have
guaranteed the efficacy of Glycyrrhiza species for an assortment of pathological/neurotic
conditions as a choleretic, diuretic and utilized as bug spray and showed as a part of
conventional prescription for cough, colds and difficult swellings (93). Customarily the plant
Figure 15. Dried mature fruit of Piper longum

31
has been prescribed as a prophylaxis for gastric and duodenal ulcers and dyspepsia as a
mitigating specialist amid allergenic responses(94). In traditional medication, it is utilized as a
purgative, emmenagogue, preventative, galactagogue, hostile to asthmatic medication and
antiviral operator (95). Glycyrrhiza roots are utilized for its demulcent and expectorant
property (96).It is helpful in sickliness, gout, throat sores ,tonsillitis, fart, sexual weakness,
hyperdypsia, fever, hacks, skin ailments, swellings, sharpness, leucorrhoea, dying, jaundice,
hiccough, dryness, bronchitis, vitiated states of vata dosha, gastralgia and so forth (95). It is
an imperative fixing in restorative oils for the epilepsy, loss of motion, ailment, hemorrhagic
maladies furthermore utilized as a part of the treatment of looseness of the bowels, fever with
incoherence and anuria (97).
2.3.1 Plant Description
It is an enduring herb, which is 3-5 feet in tallness, smooth ascending from thick rhizome.
Leaves are pinnate with 4-7 sets of leaflets which are applaud fit as a fiddle/abate shape.
flower/Blooms are in axillary spikes, papilionaceous and lavender to violet in shading. The
botanical structures and products of this family represent the method of cross-fertilization, for
the most part by bug pollinators (98, 99)
Figure 17. Licorice plant (Glycyrrhiza glabra)
31
has been prescribed as a prophylaxis for gastric and duodenal ulcers and dyspepsia as a
mitigating specialist amid allergenic responses(94). In traditional medication, it is utilized as a
purgative, emmenagogue, preventative, galactagogue, hostile to asthmatic medication and
antiviral operator (95). Glycyrrhiza roots are utilized for its demulcent and expectorant
property (96).It is helpful in sickliness, gout, throat sores ,tonsillitis, fart, sexual weakness,
hyperdypsia, fever, hacks, skin ailments, swellings, sharpness, leucorrhoea, dying, jaundice,
hiccough, dryness, bronchitis, vitiated states of vata dosha, gastralgia and so forth (95). It is
an imperative fixing in restorative oils for the epilepsy, loss of motion, ailment, hemorrhagic
maladies furthermore utilized as a part of the treatment of looseness of the bowels, fever with
incoherence and anuria (97).
2.3.1 Plant Description
It is an enduring herb, which is 3-5 feet in tallness, smooth ascending from thick rhizome.
Leaves are pinnate with 4-7 sets of leaflets which are applaud fit as a fiddle/abate shape.
flower/Blooms are in axillary spikes, papilionaceous and lavender to violet in shading. The
botanical structures and products of this family represent the method of cross-fertilization, for
the most part by bug pollinators (98, 99)
Figure 17. Licorice plant (Glycyrrhiza glabra)
31
has been prescribed as a prophylaxis for gastric and duodenal ulcers and dyspepsia as a
mitigating specialist amid allergenic responses(94). In traditional medication, it is utilized as a
purgative, emmenagogue, preventative, galactagogue, hostile to asthmatic medication and
antiviral operator (95). Glycyrrhiza roots are utilized for its demulcent and expectorant
property (96).It is helpful in sickliness, gout, throat sores ,tonsillitis, fart, sexual weakness,
hyperdypsia, fever, hacks, skin ailments, swellings, sharpness, leucorrhoea, dying, jaundice,
hiccough, dryness, bronchitis, vitiated states of vata dosha, gastralgia and so forth (95). It is
an imperative fixing in restorative oils for the epilepsy, loss of motion, ailment, hemorrhagic
maladies furthermore utilized as a part of the treatment of looseness of the bowels, fever with
incoherence and anuria (97).
2.3.1 Plant Description
It is an enduring herb, which is 3-5 feet in tallness, smooth ascending from thick rhizome.
Leaves are pinnate with 4-7 sets of leaflets which are applaud fit as a fiddle/abate shape.
flower/Blooms are in axillary spikes, papilionaceous and lavender to violet in shading. The
botanical structures and products of this family represent the method of cross-fertilization, for
the most part by bug pollinators (98, 99)
Figure 17. Licorice plant (Glycyrrhiza glabra)
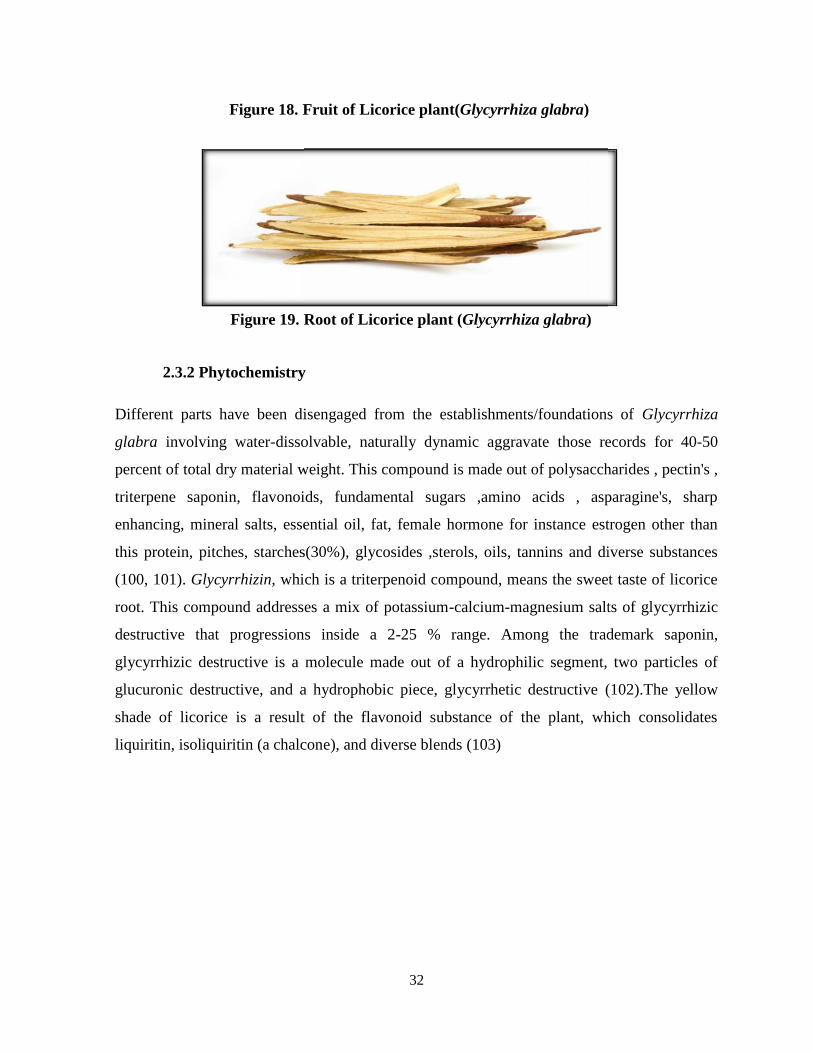
32
Figure 18. Fruit of Licorice plant(Glycyrrhiza glabra)
2.3.2 Phytochemistry
Different parts have been disengaged from the establishments/foundations of Glycyrrhiza
glabra involving water-dissolvable, naturally dynamic aggravate those records for 40-50
percent of total dry material weight. This compound is made out of polysaccharides , pectin's ,
triterpene saponin, flavonoids, fundamental sugars ,amino acids , asparagine's, sharp
enhancing, mineral salts, essential oil, fat, female hormone for instance estrogen other than
this protein, pitches, starches(30%), glycosides ,sterols, oils, tannins and diverse substances
(100, 101). Glycyrrhizin, which is a triterpenoid compound, means the sweet taste of licorice
root. This compound addresses a mix of potassium-calcium-magnesium salts of glycyrrhizic
destructive that progressions inside a 2-25 % range. Among the trademark saponin,
glycyrrhizic destructive is a molecule made out of a hydrophilic segment, two particles of
glucuronic destructive, and a hydrophobic piece, glycyrrhetic destructive (102).The yellow
shade of licorice is a result of the flavonoid substance of the plant, which consolidates
liquiritin, isoliquiritin (a chalcone), and diverse blends (103)
Figure 19. Root of Licorice plant (Glycyrrhiza glabra)
32
Figure 18. Fruit of Licorice plant(Glycyrrhiza glabra)
2.3.2 Phytochemistry
Different parts have been disengaged from the establishments/foundations of Glycyrrhiza
glabra involving water-dissolvable, naturally dynamic aggravate those records for 40-50
percent of total dry material weight. This compound is made out of polysaccharides , pectin's ,
triterpene saponin, flavonoids, fundamental sugars ,amino acids , asparagine's, sharp
enhancing, mineral salts, essential oil, fat, female hormone for instance estrogen other than
this protein, pitches, starches(30%), glycosides ,sterols, oils, tannins and diverse substances
(100, 101). Glycyrrhizin, which is a triterpenoid compound, means the sweet taste of licorice
root. This compound addresses a mix of potassium-calcium-magnesium salts of glycyrrhizic
destructive that progressions inside a 2-25 % range. Among the trademark saponin,
glycyrrhizic destructive is a molecule made out of a hydrophilic segment, two particles of
glucuronic destructive, and a hydrophobic piece, glycyrrhetic destructive (102).The yellow
shade of licorice is a result of the flavonoid substance of the plant, which consolidates
liquiritin, isoliquiritin (a chalcone), and diverse blends (103)
Figure 19. Root of Licorice plant (Glycyrrhiza glabra)
32
Figure 18. Fruit of Licorice plant(Glycyrrhiza glabra)
2.3.2 Phytochemistry
Different parts have been disengaged from the establishments/foundations of Glycyrrhiza
glabra involving water-dissolvable, naturally dynamic aggravate those records for 40-50
percent of total dry material weight. This compound is made out of polysaccharides , pectin's ,
triterpene saponin, flavonoids, fundamental sugars ,amino acids , asparagine's, sharp
enhancing, mineral salts, essential oil, fat, female hormone for instance estrogen other than
this protein, pitches, starches(30%), glycosides ,sterols, oils, tannins and diverse substances
(100, 101). Glycyrrhizin, which is a triterpenoid compound, means the sweet taste of licorice
root. This compound addresses a mix of potassium-calcium-magnesium salts of glycyrrhizic
destructive that progressions inside a 2-25 % range. Among the trademark saponin,
glycyrrhizic destructive is a molecule made out of a hydrophilic segment, two particles of
glucuronic destructive, and a hydrophobic piece, glycyrrhetic destructive (102).The yellow
shade of licorice is a result of the flavonoid substance of the plant, which consolidates
liquiritin, isoliquiritin (a chalcone), and diverse blends (103)
Figure 19. Root of Licorice plant (Glycyrrhiza glabra)
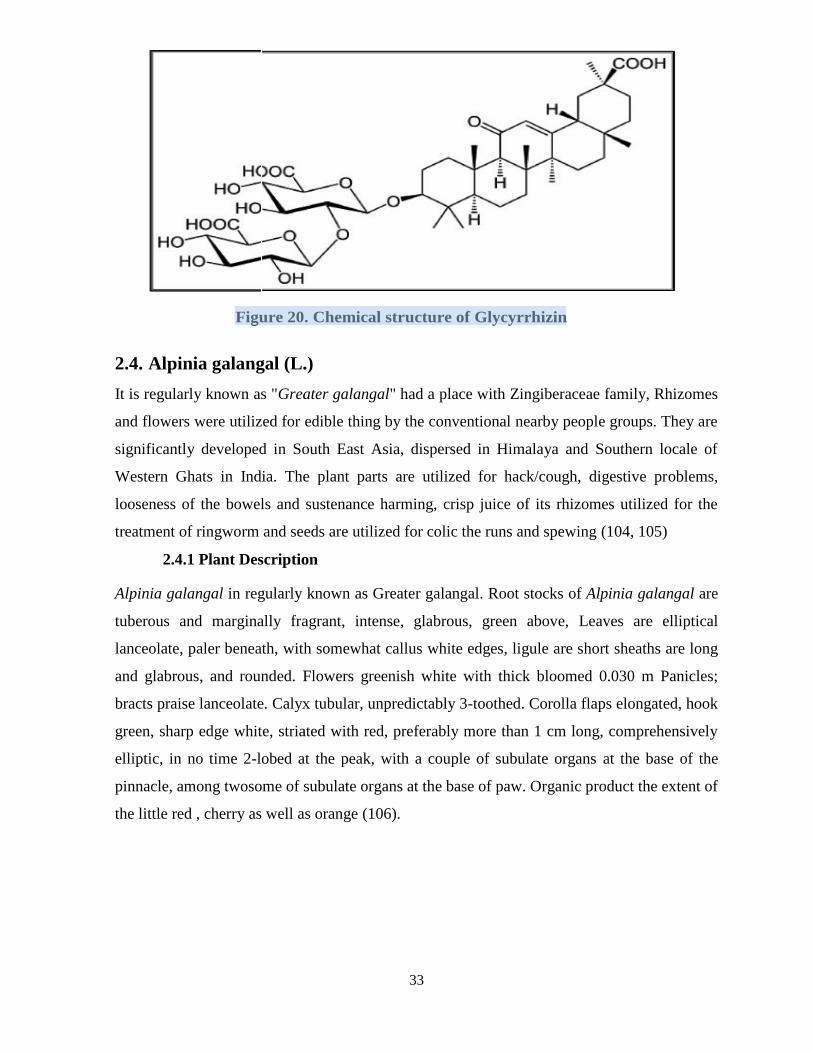
33
Figure 20. Chemical structure of Glycyrrhizin
2.4. Alpinia galangal (L.)
It is regularly known as "Greater galangal" had a place with Zingiberaceae family, Rhizomes
and flowers were utilized for edible thing by the conventional nearby people groups. They are
significantly developed in South East Asia, dispersed in Himalaya and Southern locale of
Western Ghats in India. The plant parts are utilized for hack/cough, digestive problems,
looseness of the bowels and sustenance harming, crisp juice of its rhizomes utilized for the
treatment of ringworm and seeds are utilized for colic the runs and spewing (104, 105)
2.4.1 Plant Description
Alpinia galangal in regularly known as Greater galangal. Root stocks of Alpinia galangal are
tuberous and marginally fragrant, intense, glabrous, green above, Leaves are elliptical
lanceolate, paler beneath, with somewhat callus white edges, ligule are short sheaths are long
and glabrous, and rounded. Flowers greenish white with thick bloomed 0.030 m Panicles;
bracts praise lanceolate. Calyx tubular, unpredictably 3-toothed. Corolla flaps elongated, hook
green, sharp edge white, striated with red, preferably more than 1 cm long, comprehensively
elliptic, in no time 2-lobed at the peak, with a couple of subulate organs at the base of the
pinnacle, among twosome of subulate organs at the base of paw. Organic product the extent of
the little red , cherry as well as orange (106).
33
Figure 20. Chemical structure of Glycyrrhizin
2.4. Alpinia galangal (L.)
It is regularly known as "Greater galangal" had a place with Zingiberaceae family, Rhizomes
and flowers were utilized for edible thing by the conventional nearby people groups. They are
significantly developed in South East Asia, dispersed in Himalaya and Southern locale of
Western Ghats in India. The plant parts are utilized for hack/cough, digestive problems,
looseness of the bowels and sustenance harming, crisp juice of its rhizomes utilized for the
treatment of ringworm and seeds are utilized for colic the runs and spewing (104, 105)
2.4.1 Plant Description
Alpinia galangal in regularly known as Greater galangal. Root stocks of Alpinia galangal are
tuberous and marginally fragrant, intense, glabrous, green above, Leaves are elliptical
lanceolate, paler beneath, with somewhat callus white edges, ligule are short sheaths are long
and glabrous, and rounded. Flowers greenish white with thick bloomed 0.030 m Panicles;
bracts praise lanceolate. Calyx tubular, unpredictably 3-toothed. Corolla flaps elongated, hook
green, sharp edge white, striated with red, preferably more than 1 cm long, comprehensively
elliptic, in no time 2-lobed at the peak, with a couple of subulate organs at the base of the
pinnacle, among twosome of subulate organs at the base of paw. Organic product the extent of
the little red , cherry as well as orange (106).
33
Figure 20. Chemical structure of Glycyrrhizin
2.4. Alpinia galangal (L.)
It is regularly known as "Greater galangal" had a place with Zingiberaceae family, Rhizomes
and flowers were utilized for edible thing by the conventional nearby people groups. They are
significantly developed in South East Asia, dispersed in Himalaya and Southern locale of
Western Ghats in India. The plant parts are utilized for hack/cough, digestive problems,
looseness of the bowels and sustenance harming, crisp juice of its rhizomes utilized for the
treatment of ringworm and seeds are utilized for colic the runs and spewing (104, 105)
2.4.1 Plant Description
Alpinia galangal in regularly known as Greater galangal. Root stocks of Alpinia galangal are
tuberous and marginally fragrant, intense, glabrous, green above, Leaves are elliptical
lanceolate, paler beneath, with somewhat callus white edges, ligule are short sheaths are long
and glabrous, and rounded. Flowers greenish white with thick bloomed 0.030 m Panicles;
bracts praise lanceolate. Calyx tubular, unpredictably 3-toothed. Corolla flaps elongated, hook
green, sharp edge white, striated with red, preferably more than 1 cm long, comprehensively
elliptic, in no time 2-lobed at the peak, with a couple of subulate organs at the base of the
pinnacle, among twosome of subulate organs at the base of paw. Organic product the extent of
the little red , cherry as well as orange (106).
HINA JUNAID
Highlight

34
Figure 21. Fresh Leaves of Alpinia galangal
Figure 22. Flower of Alpinia galangal
Figure 23. Root of Alpinia Galangal
34
Figure 21. Fresh Leaves of Alpinia galangal
Figure 22. Flower of Alpinia galangal
Figure 23. Root of Alpinia Galangal
34
Figure 21. Fresh Leaves of Alpinia galangal
Figure 22. Flower of Alpinia galangal
Figure 23. Root of Alpinia Galangal
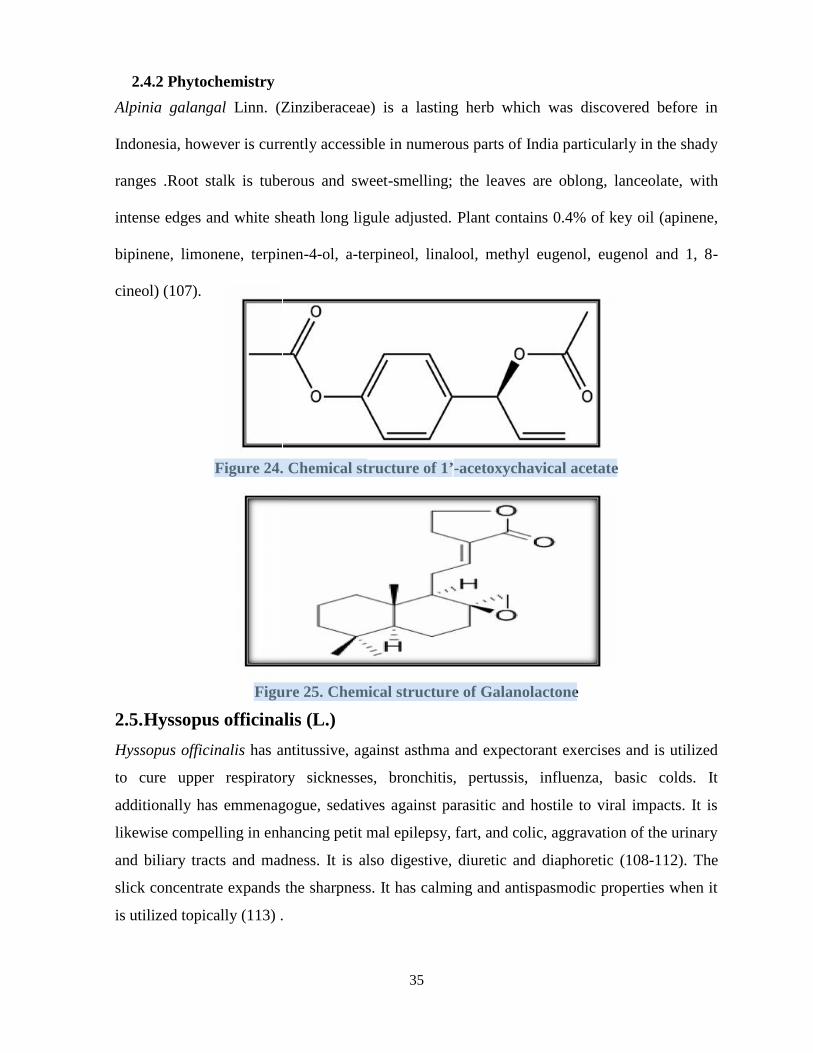
35
Alpinia galangal Linn. (Zinziberaceae) is a lasting herb which was discovered before in
Indonesia, however is currently accessible in numerous parts of India particularly in the shady
ranges .Root stalk is tuberous and sweet-smelling; the leaves are oblong, lanceolate, with
intense edges and white sheath long ligule adjusted. Plant contains 0.4% of key oil (apinene,
bipinene, limonene, terpinen-4-ol, a-terpineol, linalool, methyl eugenol, eugenol and 1, 8-
cineol) (107).
2.5.Hyssopus officinalis (L.)
Hyssopus officinalis has antitussive, against asthma and expectorant exercises and is utilized
to cure upper respiratory sicknesses, bronchitis, pertussis, influenza, basic colds. It
additionally has emmenagogue, sedatives against parasitic and hostile to viral impacts. It is
likewise compelling in enhancing petit mal epilepsy, fart, and colic, aggravation of the urinary
and biliary tracts and madness. It is also digestive, diuretic and diaphoretic (108-112). The
slick concentrate expands the sharpness. It has calming and antispasmodic properties when it
is utilized topically (113) .
35
Alpinia galangal Linn. (Zinziberaceae) is a lasting herb which was discovered before in
Indonesia, however is currently accessible in numerous parts of India particularly in the shady
ranges .Root stalk is tuberous and sweet-smelling; the leaves are oblong, lanceolate, with
intense edges and white sheath long ligule adjusted. Plant contains 0.4% of key oil (apinene,
bipinene, limonene, terpinen-4-ol, a-terpineol, linalool, methyl eugenol, eugenol and 1, 8-
cineol) (107).
2.5.Hyssopus officinalis (L.)
Hyssopus officinalis has antitussive, against asthma and expectorant exercises and is utilized
to cure upper respiratory sicknesses, bronchitis, pertussis, influenza, basic colds. It
additionally has emmenagogue, sedatives against parasitic and hostile to viral impacts. It is
likewise compelling in enhancing petit mal epilepsy, fart, and colic, aggravation of the urinary
and biliary tracts and madness. It is also digestive, diuretic and diaphoretic (108-112). The
slick concentrate expands the sharpness. It has calming and antispasmodic properties when it
is utilized topically (113) .
35
Alpinia galangal Linn. (Zinziberaceae) is a lasting herb which was discovered before in
Indonesia, however is currently accessible in numerous parts of India particularly in the shady
ranges .Root stalk is tuberous and sweet-smelling; the leaves are oblong, lanceolate, with
intense edges and white sheath long ligule adjusted. Plant contains 0.4% of key oil (apinene,
bipinene, limonene, terpinen-4-ol, a-terpineol, linalool, methyl eugenol, eugenol and 1, 8-
cineol) (107).
2.5.Hyssopus officinalis (L.)
Hyssopus officinalis has antitussive, against asthma and expectorant exercises and is utilized
to cure upper respiratory sicknesses, bronchitis, pertussis, influenza, basic colds. It
additionally has emmenagogue, sedatives against parasitic and hostile to viral impacts. It is
likewise compelling in enhancing petit mal epilepsy, fart, and colic, aggravation of the urinary
and biliary tracts and madness. It is also digestive, diuretic and diaphoretic (108-112). The
slick concentrate expands the sharpness. It has calming and antispasmodic properties when it
is utilized topically (113) .
2.4.2 Phytochemistry2.4.2 Phytochemistry2.4.2 Phytochemistry
Figure 25. Chemical structure of Galanolactone
Figure 24. Chemical structure of 1’-acetoxychavical acetate
HINA JUNAID
Highlight
HINA JUNAID
Highlight

36
2.5.1 Plant Description
Hyssop (Hyssopus officinalis) is a lasting subshrub having a place with family Lamiaceae. Its
dried blossoming shoots are utilized as a part of tea mixes for cough alleviation, for
antispasmodic impacts, and to relieve catarrh. The hydro distilled key oil from the shoot part
is generally utilized as a part of the nourishment, pharmaceutical and beautifiers businesses
(113, 114). The oil got from Hyssopus officinalis ssp.officinalis developed as a yearly harvest
is vapid and has a sweet camphoraceaous scent. This plant is a normal xerophyte and is very
much adjusted to dry season and low information conditions (115, 116).
Figure 26. Fresh Leaves of Hyssopus officinalis
Figure 27. Flower of Hyssopus officinalis
Figure 28. Dried Herb of Hyssopus officinalis
36
2.5.1 Plant Description
Hyssop (Hyssopus officinalis) is a lasting subshrub having a place with family Lamiaceae. Its
dried blossoming shoots are utilized as a part of tea mixes for cough alleviation, for
antispasmodic impacts, and to relieve catarrh. The hydro distilled key oil from the shoot part
is generally utilized as a part of the nourishment, pharmaceutical and beautifiers businesses
(113, 114). The oil got from Hyssopus officinalis ssp.officinalis developed as a yearly harvest
is vapid and has a sweet camphoraceaous scent. This plant is a normal xerophyte and is very
much adjusted to dry season and low information conditions (115, 116).
Figure 26. Fresh Leaves of Hyssopus officinalis
Figure 27. Flower of Hyssopus officinalis
Figure 28. Dried Herb of Hyssopus officinalis
36
2.5.1 Plant Description
Hyssop (Hyssopus officinalis) is a lasting subshrub having a place with family Lamiaceae. Its
dried blossoming shoots are utilized as a part of tea mixes for cough alleviation, for
antispasmodic impacts, and to relieve catarrh. The hydro distilled key oil from the shoot part
is generally utilized as a part of the nourishment, pharmaceutical and beautifiers businesses
(113, 114). The oil got from Hyssopus officinalis ssp.officinalis developed as a yearly harvest
is vapid and has a sweet camphoraceaous scent. This plant is a normal xerophyte and is very
much adjusted to dry season and low information conditions (115, 116).
Figure 26. Fresh Leaves of Hyssopus officinalis
Figure 27. Flower of Hyssopus officinalis
Figure 28. Dried Herb of Hyssopus officinalis

37
2.5.2 Photochemistry
The phytochemical investigation of the aerial part/airborne parts of Hyssopus officinalis
uncovered isolation or detachment of 2 different flavonoid glycosides in addition to 9 other
known flavonoids from the ethanol concentrate of the plant. The new chemicals were
recognized as;
“Quercetin 7-O-b-Dapiofuranosyl-(1→2)-b dxylopyranoside (1)” ,“Quercetin 7-O-b-D-
apiofuranosyl-(1→2)-b-D-xylopyranoside 30-Ob-D-glucopyranoside (2)”, “Together with
nine known flavonoids apigenin (3)”, “Apigenin 7-O-b-Dglucopyranoside (4)”, “Apigenin 7-
O-b-Dglucuronopyranoside methyl ester (5)”, “Luteolin (6)”,“Apigenin 7-O-b-D-glucuronide
(7)”, “Apigenin 7-O-b-Dglucuronopyranoside butyl ester (8)”, “Luteolin 7-O-b-
Dglucopyranosid (9)”, “Diosmin (10)” “Acacetin 7-O-a-Lrhamnopyranosyl-(1→6)-b-D-
glucopyranoside (11)” (117) .
2.6. Cordia latifolia Linn
Cordia latifolia is vernacularly known as Sepestan and its normal name is Latifolia (118)
considered Cordia curassavica, which is utilized to treat gastrointestinal, respiratory and
dermatological scatters .
37
2.5.2 Photochemistry
The phytochemical investigation of the aerial part/airborne parts of Hyssopus officinalis
uncovered isolation or detachment of 2 different flavonoid glycosides in addition to 9 other
known flavonoids from the ethanol concentrate of the plant. The new chemicals were
recognized as;
“Quercetin 7-O-b-Dapiofuranosyl-(1→2)-b dxylopyranoside (1)” ,“Quercetin 7-O-b-D-
apiofuranosyl-(1→2)-b-D-xylopyranoside 30-Ob-D-glucopyranoside (2)”, “Together with
nine known flavonoids apigenin (3)”, “Apigenin 7-O-b-Dglucopyranoside (4)”, “Apigenin 7-
O-b-Dglucuronopyranoside methyl ester (5)”, “Luteolin (6)”,“Apigenin 7-O-b-D-glucuronide
(7)”, “Apigenin 7-O-b-Dglucuronopyranoside butyl ester (8)”, “Luteolin 7-O-b-
Dglucopyranosid (9)”, “Diosmin (10)” “Acacetin 7-O-a-Lrhamnopyranosyl-(1→6)-b-D-
glucopyranoside (11)” (117) .
2.6. Cordia latifolia Linn
Cordia latifolia is vernacularly known as Sepestan and its normal name is Latifolia (118)
considered Cordia curassavica, which is utilized to treat gastrointestinal, respiratory and
dermatological scatters .
37
2.5.2 Photochemistry
The phytochemical investigation of the aerial part/airborne parts of Hyssopus officinalis
uncovered isolation or detachment of 2 different flavonoid glycosides in addition to 9 other
known flavonoids from the ethanol concentrate of the plant. The new chemicals were
recognized as;
“Quercetin 7-O-b-Dapiofuranosyl-(1→2)-b dxylopyranoside (1)” ,“Quercetin 7-O-b-D-
apiofuranosyl-(1→2)-b-D-xylopyranoside 30-Ob-D-glucopyranoside (2)”, “Together with
nine known flavonoids apigenin (3)”, “Apigenin 7-O-b-Dglucopyranoside (4)”, “Apigenin 7-
O-b-Dglucuronopyranoside methyl ester (5)”, “Luteolin (6)”,“Apigenin 7-O-b-D-glucuronide
(7)”, “Apigenin 7-O-b-Dglucuronopyranoside butyl ester (8)”, “Luteolin 7-O-b-
Dglucopyranosid (9)”, “Diosmin (10)” “Acacetin 7-O-a-Lrhamnopyranosyl-(1→6)-b-D-
glucopyranoside (11)” (117) .
2.6. Cordia latifolia Linn
Cordia latifolia is vernacularly known as Sepestan and its normal name is Latifolia (118)
considered Cordia curassavica, which is utilized to treat gastrointestinal, respiratory and
dermatological scatters .
Figure 29. Chemical structure of Apigenin & Luteolin
Figure 30. Chemical structure of Quercetin & Rutin
HINA JUNAID
Highlight
HINA JUNAID
Highlight

38
2.6.1 Plant Description
Cordia latifolia (Boraginaceae) is a little deciduous tree developing almost everywhere
throughout the Indo–Pak subcontinent. whereas all parts like leaves, roots etc. of the tree is
accounted for its medicinal /therapeutic quality in the indigenous arrangement of medication
(119).
Figure 31. Fresh Leaves of Cordia latifolia
Figure 32. Flower of Cordia latifolia
Figure 33. Flower of Cordia latifolia
2.6.2 Phytochemistry
The substance constituents and reported distinctive classes of mixes, which incorporate greasy
acids, sterols,(120) carbohydrate,(121-123) flavanone and flavanone glycosides, (124-128)
triterpenoids and glycosides(129, 130) and pyrrolizidine alkaloids.
38
2.6.1 Plant Description
Cordia latifolia (Boraginaceae) is a little deciduous tree developing almost everywhere
throughout the Indo–Pak subcontinent. whereas all parts like leaves, roots etc. of the tree is
accounted for its medicinal /therapeutic quality in the indigenous arrangement of medication
(119).
Figure 31. Fresh Leaves of Cordia latifolia
Figure 32. Flower of Cordia latifolia
Figure 33. Flower of Cordia latifolia
2.6.2 Phytochemistry
The substance constituents and reported distinctive classes of mixes, which incorporate greasy
acids, sterols,(120) carbohydrate,(121-123) flavanone and flavanone glycosides, (124-128)
triterpenoids and glycosides(129, 130) and pyrrolizidine alkaloids.
38
2.6.1 Plant Description
Cordia latifolia (Boraginaceae) is a little deciduous tree developing almost everywhere
throughout the Indo–Pak subcontinent. whereas all parts like leaves, roots etc. of the tree is
accounted for its medicinal /therapeutic quality in the indigenous arrangement of medication
(119).
Figure 31. Fresh Leaves of Cordia latifolia
Figure 32. Flower of Cordia latifolia
Figure 33. Flower of Cordia latifolia
2.6.2 Phytochemistry
The substance constituents and reported distinctive classes of mixes, which incorporate greasy
acids, sterols,(120) carbohydrate,(121-123) flavanone and flavanone glycosides, (124-128)
triterpenoids and glycosides(129, 130) and pyrrolizidine alkaloids.

39
2.7. Viola odorata Linn
Viola odorata is widely therapeutic/medicinal plants used by the traditional practitioners.
Without a doubt, the flower/blossoms are utilized as demulcent, diaphoretic, diuretic,
purgative and root is utilized as emetic as a part of bigger dosages. The entire aeronautical
part including stem, blooms and leaves are utilized as a part of bronchitis, tumor, hack, fever,
urinary diseases, stiffness, sniffling, kidney and liver issue(131, 132).
2.7.1 Plant Description
The plant ‘Viola odorata Linn’. (Violaceae) is a prominently known as "Banafshah" and
sweet violet in Europe as well as Asia . It is a long rambling Plant of less than 6 inches in
height. The Plant has textured subversive stem, with establishing runners rooting. It has a
heart formed leaves with scalloped or marginally notched edges corners are dull green,
smooth or in some cases downy underneath, and develop in a decoration at the base of plant.
Flower Blooms are profound purple or bluish pink or yellowish white in color (133, 134)
39
2.7. Viola odorata Linn
Viola odorata is widely therapeutic/medicinal plants used by the traditional practitioners.
Without a doubt, the flower/blossoms are utilized as demulcent, diaphoretic, diuretic,
purgative and root is utilized as emetic as a part of bigger dosages. The entire aeronautical
part including stem, blooms and leaves are utilized as a part of bronchitis, tumor, hack, fever,
urinary diseases, stiffness, sniffling, kidney and liver issue(131, 132).
2.7.1 Plant Description
The plant ‘Viola odorata Linn’. (Violaceae) is a prominently known as "Banafshah" and
sweet violet in Europe as well as Asia . It is a long rambling Plant of less than 6 inches in
height. The Plant has textured subversive stem, with establishing runners rooting. It has a
heart formed leaves with scalloped or marginally notched edges corners are dull green,
smooth or in some cases downy underneath, and develop in a decoration at the base of plant.
Flower Blooms are profound purple or bluish pink or yellowish white in color (133, 134)
39
2.7. Viola odorata Linn
Viola odorata is widely therapeutic/medicinal plants used by the traditional practitioners.
Without a doubt, the flower/blossoms are utilized as demulcent, diaphoretic, diuretic,
purgative and root is utilized as emetic as a part of bigger dosages. The entire aeronautical
part including stem, blooms and leaves are utilized as a part of bronchitis, tumor, hack, fever,
urinary diseases, stiffness, sniffling, kidney and liver issue(131, 132).
2.7.1 Plant Description
The plant ‘Viola odorata Linn’. (Violaceae) is a prominently known as "Banafshah" and
sweet violet in Europe as well as Asia . It is a long rambling Plant of less than 6 inches in
height. The Plant has textured subversive stem, with establishing runners rooting. It has a
heart formed leaves with scalloped or marginally notched edges corners are dull green,
smooth or in some cases downy underneath, and develop in a decoration at the base of plant.
Flower Blooms are profound purple or bluish pink or yellowish white in color (133, 134)
Figure 34.Structure of Cordifolic acid
HINA JUNAID
Highlight

40
Figure 35. Fresh Leaves of Viola odorata Linn
Figure 36. Flower (Purple) of Viola odorata Linn
Figure 37. Flower (White) of Viola odorata Linn
40
Figure 35. Fresh Leaves of Viola odorata Linn
Figure 36. Flower (Purple) of Viola odorata Linn
Figure 37. Flower (White) of Viola odorata Linn
40
Figure 35. Fresh Leaves of Viola odorata Linn
Figure 36. Flower (Purple) of Viola odorata Linn
Figure 37. Flower (White) of Viola odorata Linn

41
2.7.2 Phytochemistry
The natural organizations of the different parts (stem, leaves, petiole and blossom) have been
examined for location of different components like oxygen, carbon, sodium, aluminum,
calcium, silicon, magnesium, chloride and iron. It is a rich wellspring of these components
(135) .The “Viola betonicifolia” different parts (like leaves, bloom petioles, roots and entire
plant dust) rough methanol concentrate as well as its consequent dissolvable portion have
been accounted for different large scale and small scale supplements (for example chromium,
zinc, lead, cadmium, Cu, , nickel, Mg, Ca, Na and K) (136, 137).“The GC-MS analysis of
active fraction revealed the presence of methanol and ethanol extracts of Viola odorata
showed the presence of Pentane 2,3,4- Trimethyl (45%), N-Hexadecanoic acid 28.85%), 10-
Undecyn-1-ol (14.43%) and Pentadecanoic acid (8.14%)” (138)
2.8. Aims and Objectives of the Study:
The aim of the study establishment was to develop an oral polyherbal formulation and
evaluate its chemical and biological parameters to determine the safety and efficacy for the
treatment of cough .The named Linkus consist of the poly herbal formulation included
Adhatoda vasica Nees. , Piper longum L., Glycyrrhiza glabra L, Alpinia galangal (L.) Wild,
Hyssopus officinalis L.
41
2.7.2 Phytochemistry
The natural organizations of the different parts (stem, leaves, petiole and blossom) have been
examined for location of different components like oxygen, carbon, sodium, aluminum,
calcium, silicon, magnesium, chloride and iron. It is a rich wellspring of these components
(135) .The “Viola betonicifolia” different parts (like leaves, bloom petioles, roots and entire
plant dust) rough methanol concentrate as well as its consequent dissolvable portion have
been accounted for different large scale and small scale supplements (for example chromium,
zinc, lead, cadmium, Cu, , nickel, Mg, Ca, Na and K) (136, 137).“The GC-MS analysis of
active fraction revealed the presence of methanol and ethanol extracts of Viola odorata
showed the presence of Pentane 2,3,4- Trimethyl (45%), N-Hexadecanoic acid 28.85%), 10-
Undecyn-1-ol (14.43%) and Pentadecanoic acid (8.14%)” (138)
2.8. Aims and Objectives of the Study:
The aim of the study establishment was to develop an oral polyherbal formulation and
evaluate its chemical and biological parameters to determine the safety and efficacy for the
treatment of cough .The named Linkus consist of the poly herbal formulation included
Adhatoda vasica Nees. , Piper longum L., Glycyrrhiza glabra L, Alpinia galangal (L.) Wild,
Hyssopus officinalis L.
41
2.7.2 Phytochemistry
The natural organizations of the different parts (stem, leaves, petiole and blossom) have been
examined for location of different components like oxygen, carbon, sodium, aluminum,
calcium, silicon, magnesium, chloride and iron. It is a rich wellspring of these components
(135) .The “Viola betonicifolia” different parts (like leaves, bloom petioles, roots and entire
plant dust) rough methanol concentrate as well as its consequent dissolvable portion have
been accounted for different large scale and small scale supplements (for example chromium,
zinc, lead, cadmium, Cu, , nickel, Mg, Ca, Na and K) (136, 137).“The GC-MS analysis of
active fraction revealed the presence of methanol and ethanol extracts of Viola odorata
showed the presence of Pentane 2,3,4- Trimethyl (45%), N-Hexadecanoic acid 28.85%), 10-
Undecyn-1-ol (14.43%) and Pentadecanoic acid (8.14%)” (138)
2.8. Aims and Objectives of the Study:
The aim of the study establishment was to develop an oral polyherbal formulation and
evaluate its chemical and biological parameters to determine the safety and efficacy for the
treatment of cough .The named Linkus consist of the poly herbal formulation included
Adhatoda vasica Nees. , Piper longum L., Glycyrrhiza glabra L, Alpinia galangal (L.) Wild,
Hyssopus officinalis L.
Figure 38: Structure of 5, 6, 7, 7a-tetrahydro-4, 4, 7a-trimethyl-2(4H)-benzofuranone
HINA JUNAID
Highlight

42
Cordia latifolia and Viola odorata L. The formulation has been developed in two dosage
foams included Syrup and lozenges. The developed formulation established with the standard
quality parameters including reproducibility and validation.
2.8.1 Chemical Evaluation
Linkus dosage foam has been evaluated on the following parameters included
o Qualitative and Quantitative Estimation of Biomarkers included
o Vasicine
o Glycyrrhizin
o Piperine
2.8.2 Biological Evaluation
For biological Evaluation following parameters were adopted
o In-Vitro Antioxidant Activity
o In-Vitro Reducing Ability
o In-Vitro Enzyme inhibition included
o Anti-urease
o lipoxygenase inhibition
o In-Vitro antimicrobial analysis
o In-Vitro Evaluation of Efficacy and Chronic Toxicity
2.8.3 Clinical Evaluation
For establishment of clinical evaluation on Linkus, A Phase IV open label Clinical trial was
conducted on children’s 2-11 years of age for the treatment of cough. For the establishment of
clinical trials 2 successful marketed brands were selected included Aminophylline,
Diphenhydramine and Acefyllin Piperazine. Sleep disturbance of parents and children due to
cough was also the tool for the effective evaluation of the all treatments arms. Treatment
effectiveness further evaluated on the basis of interquartile relationship of the treatments
groups for gauging the clinical evaluation.

43
CHAPTER 3
METHODOLOGY

44
3. CHAPTER THREE - METHODOLOGY
Design Development and Quality Evaluation of Linkus
3.1. Linkus
3.1.1 Collection of Herbs
Herbs samples were purchased from Insaf kirana store Karachi, dried storage conditions was
maintained with respect to light and temperature. The herbs were identified and compared
with authentic specimen by a team of taxonomists available at the Karachi University
Herbarium (KUH). For minimize the errors, the verification is also carried out by “Prof. Dr.
Anjum Perveen”, Director of Centre for Plant Conservation, University of Karachi. Similarly
it was also made sure that every other material including solvents, reagents and chemicals
must be of pure analytical grade and acquired with proper documentation of certificate of
authenticity (COA) and Material Safety Data Sheet (MSDS) forms through local supplier.
3.1.2 Preparation of Extract
The herbs was grinded, crushed, weighed accurately and put in extractor with deionized water
in a set ratio of 1: 8.57. The extractor was heated with continuous Stirring till boiling. The
temperature was maintained within “110 - 120 C”. Then the temperature was reduce as well
as sustained up to “90-100 C” for 03 hours. After addition of Glycyrrhiza glabra extracts, it
was filtered and passed through the mesh No. 100.After the completion of evaporation
process the preservatives propyl and methyl paraben were added to the thick aqueous extract.
Thereafter 10 minutes of stirring temperature was maintained at 1100C. It was taken care that
aqueous extract was not dried of more than 20% of the total extract weight.
Linkus consists of Adhatoda vasica Glycycrrhiza glabra, Piper longum,Viola
adorata,Hyssopus officinalis, Alpinia galangal and Cordia latifolia. The composition of
Linkus syrup is given in Table 8 along with quantity and excipients utilize to formulate the
product. In table 9 plant parts used in Linkus syrup is given with vernacular names specified.
In Table 10 Manufacturing steps are delineated herewith and addition of preservative and
additives shown and stepwise manufacturing strategy in detail are analyzed. In table 10.1

45
formulation parameters of linkus are presented where in standard and methods applied are
mentioned in detail. Each 10 ml Extract of Linkus Syrup (90ml) contains
Table 8. Composition of Linkus Syrup
Ingredient’s name Quantity
Active ingredients:Dry aqueous extract of leaves of Adhatoda vasica Nees(4.29 : 1) (Acanthaceae)
600 mg
Dry aqueous extract of roots of Glycyrrhiza glabra L.(5 : 1) (Papilionaceae)
75 mg
Dry aqueous extract of fruit and roots of Piper longumL. (4.35 : 1) (Piperaceae)
100 mg
Dry aqueous extract of flowers of Viola odorata L.(4.17 : 1) (Violaceae) 25 mg
Dry aqueous extract of leaves of Hyssopus officinalis L.(4.17 : 1) (Lamiaceae) 50 mg
Dry extract of roots and rhizomes of Alpinia galangal(L.) (4.17 : 1) (Zingiberaceae) 50 mg
Dry aqueous extract of fruits of Cordia latifolia(4.35 : 1) (Boraginaceae) 100 mg
Excipients :
Sodium saccharine 15 mg
Citric acid 20 mg
Glycerol 1 g
Propylene glycol 1.252 g
70% sorbitol solution 4 g
Methyl parahydroxy benzoate 10.928 mg
Propylpara hydroxyl benzoate 2.168 mg
Peppermint oil 2.75 µl
Clove oil 1.25µl
Purified water Up to10 ml
The composition of Linkus syrup is given in Table 8 along with quantity and excipients utilizeto formulate the product

46
Plants parts of Linkus Syrup can see in table 9.
Table 9. Plant Parts Used in Linkus Syrup
In table 9 plant parts used in Linkus syrup is given with vernacular names specified
S.No Herbs Part Used Vernacular name
01 Adhatoda vasica Dry leaves Bansa, Arusa Malabar
02 Glycyrrhiza glabra Dry root Mulethi, Mulaithi
03 Piper longum Dry fruit FilfilDaraz, Piplamol
04 Viola odorataDry Leaves &
flowersBanafsha
05 Hyssopus officinalis Flowering tops Zufa
06 Cordia latifolia Dry fruit Sapistan, Lasorda
07 Alpinia galangal Dry rhizome Khulanjan galangal

47
Table 10. Manufacturing Steps of Linkus Syrup
MANUFACTURING STEPS
STEP NO. PROCESS / PROCEDURE
STEP 1
SYRUP MANUFACTURING:
Take 900 liter D.I. water in 2500 liter manufacturing tank. Heat to boil for 45 to 60minutes. when boiling starts add 1750 kg sugar in portions as follows with constant
stirring:
Add 350 kg sugar and stir for 20 minutes
When it dissolved, add 350 kg sugar and stir for 25 minutes
When it dissolved, add 350 kg sugar and stir for 30 minutes
When it dissolved, add 350 kg sugar and stir for 35 minutes
When it dissolved, add 350 kg sugar
Continue heating for 1 hour with constant stirring or till it becomes transparentsyrup.
STEP 2
ADDITION OF PRESERVATIVES AND ADDITIVES:
Separately dissolve following material one by one in 100 Liters of D.I. water
Methyl Paraben:
Propyl Paraben:
Glycerin:
Citric acid:
Heat to boil & mix thoroughly.
When mixed, filter the solution and add the filtrate to STEP 1 and stir for 20minutes.
Contd..

48
Contd..
STEP 3
DECOCTION OF ADHATODA VASICATake 200 Liter D.I. Water in jacketed kettle and place 25 kg Adhatoda vasica in it. Heat
to boil for one Hour.
Filter the solution and collect the filtrate in a separate container. Mark it as Decoction
STEP 4
DECOCTION OF PIPER LONGUM:
Take 200 Liter D.I. Water in jacketed kettle and place 25 kg Piper longum in it. Heat toboil for one Hour.
Filter the solution and collect the filtrate in the Decoction Container in STEP 3
STEP 5
DECOCTION OF ALPINIA GALANGA,HYSSOPUS OFFICINALIS, CORDIALATIFOLIA AND VIOLA ODORATA
Take 100 Liter D.I. Water in jacketed kettle and place half of Alpinia galangal,Hyssopus officinalis, Cordia latifolia and Viola odorata in it Heat to boil for one Hour.
Filter the solution and collect the filtrate in the Decoction Container in STEP 3
Again take 100 Liter D.I. Water in jacketed kettle and place remaining half of Gaozabanin it. Heat to boil for one Hour.
Filter the solution and collect the filtrate in the Decoction Container in STEP 3
STEP 6
FILTRATION OF ALL DECOCTIONS:
Finally filter the mixed decoctions from step 3, Step 4 and Step 5.
Transfer the filtered solution to STEP 1 with continuous stirring
STEP 7
ADDITION OF GLYCYRRHIZA GLABRA (MULETHI) EXTRACT:
Take 50 Liters D.I. Water in jacketed kettle and add 18.75 kg Mulethi extract in it. Heatto boil or until the extract fully dissolve in the water.
Then filter the solution.
Transfer the filtered solution to STEP 1 with continuous stirring
STEP 8
Addition of Linkus Extract:
Take 50 Liters of D. I. water and add to it Linkus extract. Heat till fully dissolved.Then filter the solution.
Transfer the filtered solution to STEP 1 with continuous stirring
Contd...

49
Contd...
STEP 9 MIXING:
After all the additions to STEP 1, finally mix for one hour
STEP 10
COOLING OF SYRUP:
After mixing, start chilled water circulation to allow the syrup to cool down.
Circulation continued until the temperature of the syrup reached to “ROOM
TEMPERATURE”
STEP 11
ADDITION OF FLAVOURS:
In a separate container, mix one-by-one the following ingredients.
Peppermint Oil
Clove Oil
Propylene glycol
Add the blend of flavors to STEP 1 with vigorous mixing
STEP 12VOLUME MAKE-UP:
Make the volume of the syrup to 2500 Liters.
D.I. Water added for Volume Make-up
STEP 13
FINAL MIXING:
After volume make-up finally mix for another half an hour.
Contd...

50
Contd...
PACKAGING STEPS
STEPNO. PROCESS / PROCEDURE
STEP1
BOTTLE BLOWING:
Blow the bottle to remove dust particles through properly operative bottle blowing machineCompliance was ensured
STEP2
SYRUP FILLING:
Machine adjusted on desired Volume per bottleEnsure compliance after filling .
STEP3
CAPPING:
Capping machine functioning properlyEnsure compliance after capping .
STEP4
LABELING:
Labeling the filled bottle with particular label of the particular product.Ensure compliance after labeling.
STEP5
OVERPRINTED CARTON & INSERT:
Pack the labeled bottle in printed carton with insert of appropriate station.Ensure the compliance.
STEP6
SHIPPER & PIGEON HOLES:
Finally pack the bottles in master carton (with pigeon holes)Again ensure the compliance.
In Table 10 Manufacturing steps are delineated herewith and addition of preservative andadditives shown and stepwise manufacturing strategy in detail are analyzed
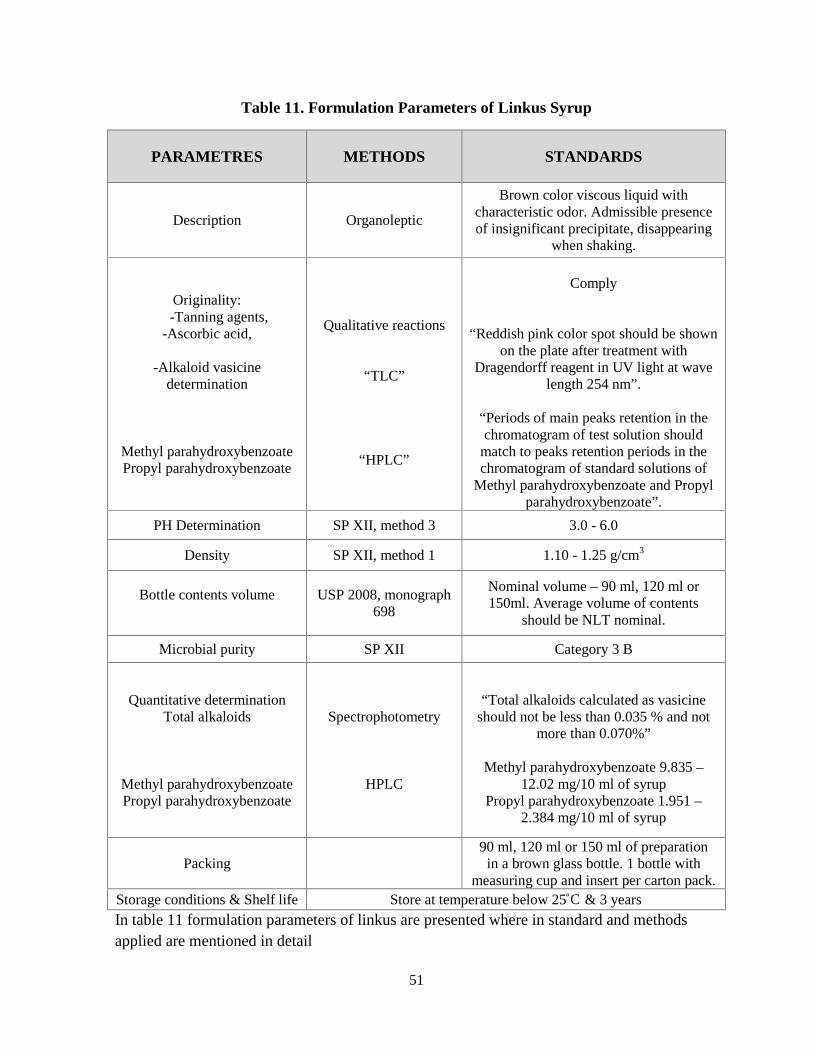
51
Table 11. Formulation Parameters of Linkus Syrup
PARAMETRES METHODS STANDARDS
Description Organoleptic
Brown color viscous liquid withcharacteristic odor. Admissible presenceof insignificant precipitate, disappearing
when shaking.
Originality:-Tanning agents,
-Ascorbic acid,
-Alkaloid vasicinedetermination
Methyl parahydroxybenzoatePropyl parahydroxybenzoate
Qualitative reactions
“TLC”
“HPLC”
Comply
“Reddish pink color spot should be shownon the plate after treatment with
Dragendorff reagent in UV light at wavelength 254 nm”.
“Periods of main peaks retention in thechromatogram of test solution should
match to peaks retention periods in thechromatogram of standard solutions of
Methyl parahydroxybenzoate and Propylparahydroxybenzoate”.
PH Determination SP ХII, method 3 3.0 - 6.0
Density SP ХII, method 1 1.10 - 1.25 g/cm3
Bottle contents volume USP 2008, monograph698
Nominal volume – 90 ml, 120 ml or150ml. Average volume of contents
should be NLT nominal.
Microbial purity SP XII Category 3 B
Quantitative determinationTotal alkaloids
Methyl parahydroxybenzoatePropyl parahydroxybenzoate
Spectrophotometry
HPLC
“Total alkaloids calculated as vasicineshould not be less than 0.035 % and not
more than 0.070%”
Methyl parahydroxybenzoate 9.835 –12.02 mg/10 ml of syrup
Propyl parahydroxybenzoate 1.951 –2.384 mg/10 ml of syrup
Packing90 ml, 120 ml or 150 ml of preparation
in a brown glass bottle. 1 bottle withmeasuring cup and insert per carton pack.
Storage conditions & Shelf life Store at temperature below 25˚C & 3 years
In table 11 formulation parameters of linkus are presented where in standard and methodsapplied are mentioned in detail

52
The composition of Linkus lozenges, the plants part used, manufacturing steps , formulationspecification and packing standard of linkus are mentioned in table 12 and 13.
Table 12 . Composition of Linkus Lozenges
Name of thick Aqueous Extracts Quantity of Extract per Lozenges
Adhatoda vasica Nees. 109.1 mg
Piper longum L. 18.18 mg
Glycyrrhiza glabra L 1.78 mg
Alpinia galangal (L.) Wild 9.1 mg
Hyssopus officinalis L. 9.1 mg
Cordia latifolia 18.18 mg
Viola odorata L. 4.55 mg
Table 13 .Plant Parts Used in Linkus Lozenges
Name of thick aqueous extracts Local name Parts Used
Adhatoda vasica Nees.Bansa,ArusaMalabar,Behkar
Leaves
Piper longum L.FilfilDaraz,Piplamol
Fruit and root
Glycyrrhiza glabra L “ Mulethi, Mulaithi Roots
Alpinia galangal (L.) WildKhulanjan,galangal
Rhizome
Hyssopus officinalis L. Zufa Leaves
Cordia latifolia Sapistan, Lasorda Fruit
Viola odorata L. Banafshan Flowers

53
Table 14 .Manufacturing Steps of Linkus Lozenges
S. NO PROCESS
STEP 1WEIGHING & COOL MIXING:
Take D.I water, sugar and Liquid glucose according to recipe in weigh tankby auto weighing and mix by stirrer.
STEP 2
PREPARATION OF SYRUP IN WARM MIXER:
Transfer the contents from weigh tank to storage jacketed tank with hot watertemperature 60 to 80°C.
Feeding the sugar syrup to the cooker through production Pump cookedproduct up to 143 to 145°C collect at the bottom up to certain level in flash
off vessel equipped with wall scraper stirrer.
STEP 3
COOKING UNDER VACUUM:
Flowing product through the conical shaped valve with micrometeradjustment from flash off vessel to vacuum chamber. Cooked product suck by
mean of vacuum maintain 760mm of Hg in to vacuum chamber. A countercompares the number of revolution of product pump shaft with number set by
the operator to determine the lot size should be 30 Kg.Production pump reaches the set number the opening the flash off vessel
chamber is automatically closed and vacuum is released. Bowl moves downby gravity due to weigh of cooked mass.
STEP 4
ADDITION OF LOZENGES EXTRACT:
Add Linkus lozenges powder extract mixture in water dozing through thedozing pump in flash off vessel mixed in sugar syrup with wall scraper stirrer
before vacuum
STEP 5
COMPOUND PREPARATION:In a separate container take Spearmint, Eucalyptus oil, Triacetin, grinded
crystal mint, Honey flavor and Lemon flavor can be added.
STEP 6ADDITION OF ACIDS AND COMPOUND :
When solution is condensed, add Ascorbic acid, Citric acid and flavorcompound and mix it.
STEP 7
KNEADING:Product mass transfer form bowl to kneading plate through pan trolley. Add
flavor compound and acid(s) to achieve the hardness of product mass byusing the chilled water, talc powder used for de moisture.
STEP 8 ROPING & SIZING:
Transfer the mass to batch roller then pass for roping to Rope sizing machine.The operator set rope for uni-plast machine.

54
Table 15.Formulation Parameters of Linkus Lozenges
Formulation evaluation details
Parameter Sampling Plan Specification Testing Method
Bulk Product
AppearanceOne sample from
beginning in each lot thanfrom middle and end.
Brown colourlozenges with
characteristic odourOrganoleptic
AverageWeight
One sample frombeginning in each lot than
from middle and end.
From 2.375g to2.625g
BritishPharmacopoeia
WeightUniformity
20 lozenges frombeginning in each lot than
middle and end.2.5g ± 5%
BritishPharmacopoeia
Thickness andDiameter
10 lozenges samples fromeach lot from beginning
than middle and end.
Thickness7mm ± 1mm
Diameter17mm ± 1mm
Verniercalliper
Assay10 lozenges samples eachfrom beginning, Middleand end from each batch
Total Alkaloids asVasicine
NLT 0.080Spectrophotometer
Finished Product
BlisterAppearance
10 lozenges samples fromeach lot at beginning than
middle and end.As per standard Visual
Leak test
10 lozenges samples ineach lot taken from
beginning than middle andend of blistering process.
No leakage Vacuum desiccator
3.2.Quantitative Determination of Piperine and Glycyrrhizin in Linkus
dosage forms (via HPLC and HPTLC)
3.2.1 Chemicals:
Benzene has been purchased from Merck, Pakistan while Ethyl acetate, Methanol and Formic
Acid of analytical grade from Merck, Darmstadt, Germany have used. Reference standards
Piperine and Glycyrrhizin have been used from Sigma-Aldrich GmbH, Germany. For

55
maintaining the quality, quantity and therapeutic effects the chemicals of high analytical
grades have been used.
3.2.2 Apparatus:
“TLC Scanner 3 linked to Win Cats software (CAMAG), 0.2 mm thickness pre-coated with
silica gel 60 F254 (Merck) have been used. Other than TLC scanner , Linomat V Automatic
Sample Spotter (CAMAG, Muttenz, Switzerland), 100 μL syringe (Hamilton, Bonaduz,
Switzerland), chromatography column Hibar 250-4,6 Purospher Star RP-18e (5 μm) by
Merck and glass twin trough chamber (20 cm × 10 cm × 4 cm) (CAMAG) were the essential
elemental apparatus in this study. The relative humidity was 40% while temperature
maintained at 25±2 °C”.
3.2.3 Quantitative estimation of Piperine and Glycyrrhizin:
3.2.3.1 Standard preparation of Piperine:
Dried ground fruits of crude herb (Piper longum) in 2gm/30 ml methanol and reflux the
mixture for 30 min at 70 °C. The resulting solution was filtered and washed the residue with 5
ml methanol, collected the filter in a 100 ml conical flask and concentrated to 2 ml for making
standard solution of Piperine.
3.2.3.2 Sample preparation of Piperine:
Dissolved thick extra of in 5g/50 ml of methanol and sonicated the mixture for 15 – 20 mins.
Filtered the resulting solution, washed the residue through 5 ml of methanol. Subsequently
evaporation, the dry deposit was dissolved in 30 ml of 10 % sodium carbonate (Na2CO3).
Transferred the mixture into separating funnel and extracted with 50 ml of ethyl acetate. After
complete separation of layers collect upper layer (ethyl acetate phase) in conical flask, repeat
extraction of aqueous layer with (50 ml × 2) ethyl acetate, collected in the same flask. Poured
the total volume of ethyl acetate in separating funnel and washed with (10 ml × 2) of water.
Filtered combined ethyl acetate fraction concluded the filter paper with anhydrous NasSO4.
The Evaporate mutual ethyl acetate fraction under emptiness to dryness. Dissolved the dry
residue in 5 milliliter of MeOH.

56
3.2.3.3 Standard Preparation of Glycyrrhizin:
“Prepared standard solution of known concentration (0.4 miligram/milliliter) by dissolving 4
mg of glycyrrhizin ammonical hydrate in 10 mililiter of 70% HPLC grade methanol by
heating”.
3.2.3.4 Sample Preparation of Glycyrrhizin:
Transferred approx. 12 g polyherbal solution to 25 ml volumetric flask. Added 10 ml of 70 %
HPLC grade methanol in to the flask and sonicated for 15 minutes. After sonication, make the
volume up to the mark with 70 % methanol. Mixed the content and filter the solution
prudently through Whatman filters paper No. 44.
3.2.3.5 Procedure:
“Analysis was performed on 20 cm × 10 cm HPTLC silica gel G60 F254 plates with
fluorescent indicator. Before starting the analysis, HPTLC plates were cleaned by
predevelopment with methanol by ascending method. HPTLC plate was immersed in a
CAMAG glass chamber (20 cm × 10 cm), containing 30 mL methanol (HPLC grade) as
solvent system. The chamber was covered with glass lid and left till development of the plate
to the top with methanol. After complete development, the plate was removed from TLC glass
chamber and dried in an oven at 105 °C for 5 mins. Three spots of 10 μL were applied (in the
form of band) of standard preparation along with three spots of 10 μL of sample preparation
as the bands on the same plate by means of a CAMAG Linomat 5 (automated spray-on
applicator equipped with a 100 μL syringe and operated with the settings band length 6 mm,
distance between band 15 mm, distance from the plate side edge 15 mm, and distance from
the bottom of the plate 15 mm”.
3.2.3.6 TLC Development and Scanning for Piperine:
Applied both solutions (10µl) in the form of spots separately on silica gel 60 F254 coated
plate. Solvent system: Benzene: Ethyl acetate (2: 1) is use to develop TLC plate up to 8-9 cm,
dry the plate in air. Visualize the plate under ultra violet light at 254 nm. After derivatization
the plate with Dragendorff’s reagent it was dried in air. The reddish pink color spot obtained
from the sample solution corresponds to those obtained from the standard solution.

57
3.2.3.6 TLC Development and Scanning for Glycyrrhizin:
“Developed the plate by immersing sample HPTLC Plate in a CAMAG glass chamber (20 x
10 cm) contained the solvent system (ethyl acetate: methanol: water: formic acid (15: 5: 1: 1),
wait to develop the plate to a distance of 8 to 9 cm.
After complete development, allowed the plate to dry by keeping in fume cupboard for 10
minutes and then keep in hot air oven for 5 min at 105 °C”.
Scan the plate in the densitometer by linear scanning at 254 nm by use of a TLC Scanner III
CAMAG and integrate the area of the spots corresponding to Glycyrrhizin standard. Calculate
the amount of Glycyrrhizin in mg per 10 ml by following formula.
Content of Glycyrrhizin: ASMP x WSTD x f x Dilution of Smp x P x D x 10ASTD x Dilution of Std x WSMP x 100
ASMP = Avg. Area of Sample,
ASTD = Avg. Area of Standard
WSTD = Weight of Standard, mg
WSMP = Weight of Sample, g
P = Percent purity of Standard
D = Density of Linkus Syrup, g/ml
f (0.8849) = Conversion factor of Glycyrrhizin
Ammonical Hydrate to glycyrrhizin
3.3. In Vitro Antioxidant, Reducing, Lipoxygenase and Ace Inhibition
Activity of Polyherbal Drug Linkus Syrup and lozenges
3.3.1 Plant Material and Techniques:
Herb extracts and mentioned chemical constituents of Linkus Syrup and lozenges were
analyzed for organoleptic evaluation, qualitative reaction of glycyrrhizic acid and quantitative

58
determination with spectrophotometric evaluation has been observed in which total
flavonoids contents as luteolin-7-glucoside was not less than 0.080 mg/lozenge.
3.3.2 Preparation of Plant Extract:
The herbs of Linkus were supplied by the Insaf Kirana store, Karachi and all these individual
herbs were taken separately, cleaned, grinded, weighed and distill water; sugar and liquid
glucose were added. The ingredients were transferred from weigh tank to storing tank and the
temperature was kept at 110-120 0C for syrup and 60 to 80°C for Syrup. The Syrup required
boiling and vacuum cooking was done as per the needed. Kneading, roping and sizing were
the next step with the help of uni-plast machine. Syrup were finally passed through cooling
tunnel to get the desired hardness. For syrup hot water filtrate was evaporated via a condenser.
Methyl paraben land Propyl paraben and flavoring agents were added after completion of the
process.
3.3.3 Chemicals and Reagents:
All chemicals were HPLC grade. The 1, 1-diphenyl-2-picrylhydrazyl was obtained from
Merck Pakistan and used for reduction whereas “2,2’-diphenyl-1-picryl hydrazyl (DPPH) for
antioxidant activity was procured from , Sigma-Aldrich Chemie (Buchs, Switzerland)”.
3.3.4 Scavenging Activity by DPPH Radical:
“The antioxidant activity was measured by the scavenging aptitude of the formulations dosage
on free radical (DPPH). Antiradical activity was analyzed which depends on the reduction of
DPPH. Its free radicals showed strong absorption at 517 nm due to odd electrons. When this
electron paired in the company of hydrogen donor for example any antioxidant, the
absorption strength is decreased, and color changed from purple to yellow, w.r.t the number
of electrons captured (139). The experimental was performed according to the process 2, 2-
Diphenyl-1-(2, 4, 6-trinitrophenyl) hydrazyl (M.W= 394.24) (Sigma) was prepared in ethanol
in the concentration of 3mM. Each well in 96 well plate was labeled as control, blank and test
compound of various concentrations. The DPPH solution (95 µl) was added in the labeled
wells. The test compound (5 µl) of concentration 10- 1000 µM in DMSO) was then added in
DPPH solution and reaction mixture was mixed for few seconds. After the reaction has taken
place in wells when 96 well plates were incubated at 37° C for thirty minutes. The micro titer
plate read at the absorbance of 515 nm (Spectramax plus 384 Molecular Device, USA) after

59
thirty minutes. The percentage of radical scavenging activity was considered with respect to
DMSO treated control. Butylated hydroxyanisole (BHA) was taken as standard.” The DPPH
activity were performed as per the following equation
“DPPH radical scavenging effect (%) =Ac-As/Ac x 100”
Where
As = Absorbance of Standard
Ac = Absorbance of Control
Reducing ability by the conversion of ferric into ferrous state
“The reducing ability was determined by the conversion of ferric into ferrous state by
antioxidant designated compounds using the method of Oyaizu (140) Each test compound
(100 µl: 10-1000 µM) prepared in DMSO/ was mixed with phosphate buffer (250 µl: pH 6.6:
0.2 M). Potassium ferricyanide (250 µl: 1%) was then added to the contents in the test tube.
This mixture then incubated at 50 C for twenty minutes in water bath and was centrifuged for
ten minutes at 3000 rpm. Subsequently on centrifugation, the top layer of solute (250 µl) was
separated in another set of test tubes and mixed with equal volume of DMSO (250 µl). Ferric
chloride (0.1 %: 50 µl) was added to the mixture with absorbance at 700 nm on
spectrophotometer (Specord 2000, Germany). The percent reduction ability was determined in
terms of percentage w.r.t BHA used as standard”.
Percent Reduction Activity = At x 100As
Where
As= Absorbance of standard
At = Absorbance of test
3.3.5 Anti-Urease Activity:
“By using the indophenol method, the Urease activity was evaluated by ammonia
production as described by (141). Reaction mixtures encompassing 25 μL of enzymatic
(Jack bean Urease) solution and 55 μL of buffers comprising 100 mM urea were

60
incubated with 5 μL of test compounds for 15 min at 30oC in 96-well plates. With the
help of indophenol method, activity was determined by measuring ammonia production.
1. After that 45 μL of phenol reagent “(1% w/v phenol and 0.005% w/v sodium
nitroprusside)
2. 70 μL of alkali reagent (0.5% w/v NaOH and 0.1 % active chloride NaOCl) was added in
each well.
3. By using a microplate reader (Molecular Device, USA), the absorbance at 630 nm was
measured after 50 min. In a final volume of 200 μL, all reactions were performed in
triplicate.
4. By using SoftMax Pro software (Molecular Device, USA), the results (change in
absorbance per min) were processed.
5. All the assays were performed with (0.01 M K2HPO4.3H2O, 1 mM EDTA and 0.01 M
LiCl2) at pH 8.2.
6. The percentage inhibitions were determined by the formula 100–(ODtestwell/ODcontrol)
x100. As the standard inhibitor of urease, thiourea was used for the experiments”
3.3.6 Lipoxygenase Inhibition Activity:
“Lipoxygenases are family of iron encompassing dioxygenases that convert the adding of
molecular oxygen to fatty acid comprising a cis-1, 4- pentadiene classification. The prime
product of this response is a 4-hydroperoxycis trans-1, 3-conjugated pentadienyl moiety
within unsaturated fatty acid. This assay processes the hydroperoxides produced in the
lipoxygenation reaction using a purified lipoxygenase with lionoleic acid as substrate. In the
proposed method Lipoxygenase enzyme solution was prepared in sodium phosphate buffer
with such concentration to give 130 U per well. Sodium phosphate buffer (pH 8.0: 160µl:100
mM) was occupied in each well of plate labeled as Blank named Bsubstrate and B enzyme, as
control and Test. Test compound solution in methanol (10-1000 M: 10 l) was addedin
each well labeled as test. Lipoxygenase solution (LOX: 20l) was added in each well
including B enzyme, Control and Test except B substrate and the mixture was incubated at 25
C for ten minutes. Substrate solution was prepared by adding linoleic acid (155 µl:0.5 mM)
into 0.12 % w/v tween 20 (257 µl). The mixture was mixed and 0.6 ml NaOH (1N) was added
to remove turbidity and volume was making up to 20 ml with deionized water. This mixture
was dispersed with the nitrogen gas to evade autoxidation before adding to each other. The

61
response was started by the adding of 10 <l substrate in each well except enzyme B as well as
the absorbance was measured at 234 nm for 5 minutes”.
3.4. Antimicrobial Analysis of Polyherbal Formulation Linkus Syrup
3.4.1 Apparatus:
High-efficiency particulate arrestance (HEPA) filter used with air cleaning specification, ISO
4644-1( Class 3),EC-GMP (A),FS-209E (Class 1) with H 14 (>99.999% )efficacy, Sanyo lab
Auto clave used with MLS-3780-SV,Japan.Vertical pressure steam sterilizer with vessel
volume 35L (Working pressure 0.22 Mpa and temperature 134C),Oven 55 LTR (MMM)
Germany with 5C above ambient temperature up to 250 C (stainless steel, mat No.14301
(AISI 304),Incubator 55 LTR (MMM) Germany with 5Cabove ambient temperature up to
70.0 C/99.9 C, .Laminar flow with H14 filters with micromesh downstream, lightning >800
lux, Volumetric flask, metallic borer ,Petri dish and all glass ware were type A pre sterilized
.Temperature tank (Digital constant) with RPM 60-230 +10 by Germany used in experiment.
3.4.2 Test for Microorganism:
For the establishment of antimicrobial activity, Gram positive organisms were the part of the
experiment including Staphylococcus Aureus, Streptococcus pyogenes and Salmonella spp.
However the gram negative bacterial culture was Pseudomonas Aeruginosa used for the
polyherbal antimicrobial activity. All the cultures were obtained from Dr. Ehsanullah Lab.
3.4.3 Reference Adjustment:
McFarland principles were adopted for maintaining the turbidity in bacterial microorganism.
For preparing the standards, Barium chloride and sulfuric acid were added for obtaining the
precipitates of barium Sulphate by maintain the bacterial quantity inside suspension. For
matching the bacterial cell density (1.5×108 CFU/ml) ,BCl 0.5 ml and H2SO4 99.5ml were
taking to make 100 ml .Absorbance have been noted by Spectrophotometer (Spekol 2000
series, Analytikjena)(0.124 AU) (142, 143)
3.4.4 Remel Tryptic Soy Agar (TSA) for qualitative procedure:
TSA is recommended for clinical laboratories for susceptibility testing procedures and
maintenance of microbial culture (144-147). By provided specification (OXOID, USA)

62
medium were prepared and substance were inoculated after sterilization. Culture were
prepared at 36ºC ± 1ºCover nightly and diluted with sterile physiological solution (108
CFU/ml).
3.4.5 Antimicrobial Assay:
The antimicrobial assay was performed by two methods viz.
1. “Agar Well Diffusion Method”
2. “Agar Disc Diffusion Method”
Before the microbial assay we performed the sterility test
3.4.6 Sterility Test:
The sterility test performed on, MacConkey Agar , & Brain Heart Infusion Broth i.e.
inoculated with the given samples and poured into the Petri plate & by streaking on Blood
Agar plate and place in an incubator for incubation at 37 c for 48 hr. .After incubation no
microbial growth observed on plates.
3.4.7 Agar Disc Diffusion Method:
“The molten Mueller Hinton agar was inoculated with 100 μl of the inoculums (1 x 10
8cfu/ml) of (Staphylococcus aureus, Streptococcous pyogenes, Pseudomonas aeriginosa,
Salmonella) and poured into the Petri plate (Hi-media). For agar disc diffusion method, the
disc (0.7 cm) (Hi-Media) was saturated with 10 μl (0.6mg) of the test compound, allowed to
dry and was introduced on the upper layer of the seeded agar plate”.
3.4.8 Agar Well Diffusion Method:
“For antimicrobial analysis agar well diffusion method were performed(148, 149). A well was
prepared in the plates with the help of a cork-borer (0.85 cm). 100 μl (6 mg) of the test
compound was introduced into the well. The plates were incubated overnight at 37 °C.
Microbial growth was determined by measuring the diameter of zone of inhibition. The result
was obtained by measuring the zone diameter. The experiment was done three times for mean
values”Linkus syrup formulation ingredients with parts used vernacular names of medicinal

63
plants components and their salient pharmacological action with particular reference to
bronchodilator, expectorant, antiasthematic effect, bronchitis whooping cough, anti-
inflammatory, spasmodic cough relief fever, flu, cough and related disorder along with
literature reference has been mentioned so as to substantiate its validity and its use in cough
documents are given to prove that the desired broacforty is thus expected and efficacy
parameters are expected to show its onsets on animal and human subjects. These
pharmacological actions of herbs employed.
Table 16. Pharmacological Actions of Herbs
3.4.9 Qualitative and Qualitative Evaluation of Linkus.
3.4.9.1 Qualitative Identification
Take 4 Syrup and dissolve in distilled water to make 100 ml solution filter the obtained
solution through a folded ash less filter paper (Solution A).
S.No
Herbs Part UsedVernacular
namePharmacological Action
01Adhatoda
vasicaDry
leaves
Bansa,Arusa
Malabar
Dhuley report the Bronchodilator and expectoranteffect,(150) Anti-asthmatic and used in respiratorydisorder (151)used as respiratory ailments inasthma, bronchitis, whooping cough and commoncough
02 Glycyrrhiza glabra Dry rootMulethi,Mulaithi
Anti-inflammatory, reduction in respiratory tractinflammation, spasmodic cough relieve (152)
03 Piper longum Dry fruitFilfilDaraz,Piplamol
Prevents recurrent attacks of bronchial asthma,(153) prevent bronchospasm and anti-asthmatic,(154)
04 Viola odorataDry
Leaves &flowers
BanafshaFlowers is effective in fever, flu, cough, pneumoniaand body pain (155)
05Hyssopusofficinalis
Flowering tops
ZufaReliever for cough, expectorant, also anti-inflammatory(156)
06Cordialatifolia
Dry fruitSapistan,Lasorda
Against H. Influenza (157)
07 Alpinia galangalDry
rhizomeKhulanjangalangal
Used for cold, chronic cough, asthma and lungdiseases (158)Respiratory diseases (159)Anti-inflammation, antimicrobial activity(160)

64
Add 5 drops of 3% solution of ferric chloride to 3 ml of solution A; yellowish green color will
appear (Tanning agents).Put 5 ml of solution A in a test tube and add 1.5 ml of concentrated
sulphuric acid, red-orange color will gradually appear at the bottom (Glycyrrhizic acid).
Vasicine: The reddish pink colour spot referred vasicine alkaloid presented in the
chromatogram.
3.4.9.2 Quantitative Determination for Flavonoids
The quantitative determination was performed by spectrophotometry for flavonoids. Sample
preparation: For the determination, the test solution was prepared with 20 numbers of Syrup
crushed and then take 10 g into 200 ml flat bottomed flask, added 50ml of 30% ethanol
solution. To complete the disintegration process, it was kept for 2 hours and then filtered.
Method: The 10 ml of the tested solution were taken in two, 25 millilitre volumetric flasks
each. After that 2 millilitre of 3% aluminium chloride solution in 30 precent ethanol into the
1st flask and 2 millilitres of 0.1 Molar of HCl solutions in the 2nd flask were added . Then
the volume was made up to the mark with 30 precent ethanol. The optical density of the first
flask solution within 40 minutes in a cuvette with 10 mm layer at the λ of 395 nm was
determined, and 2nd flask solution was uses for a comparison. Aggregate flavonoids in 1
tablet substance in mg (x) as luteolin-7-glucoside is figured as per the accompanying recipe:
10 x 25 x 50 x D x M0 1250 x D x M0
X = ------------------------------ = -------------------
10 x M x 401 401 x M
Where D – Optical thickness of arrangement.
401 – Specific ingestion files of aluminium complex of luteolin - 7 –
glucoside at the wavelength of 395 nm.
M0 – Average capsule weight.
M – Preparation weight.
Aggregate flavonoids substance as luteolin-7-glucoside ought to be
not less than.

65
3.4.9.3 Quantitative determination of Vasicine (Adhatoda vasica) by HPTLC
CAMAG Linomat 5, CAMAG Scanner III equipment was used for the quantitative
determination in which HPTLC silica gel G60F254 was utilized with solvent system EtOAc:
CHCl3: EtOH: NH3 (6:3:1:1) system and observed at 254 nm UV/ Wave length.
Sample Preparation: Take 20 tablets (exact weight) dissolve in 50 ml of water and transferred
it in a 250 ml dividing funnel. Add 3 ml of hydrous ammonia. Add 25 millilitre of chloroform
to the obtained solution in the funnel. Shake carefully during 3 minutes. After full division of
layers filter lower chloroformic layer through the paper filter with anhydrous sodium sulphate
(about 10 g) in 500 ml round bottom flask. Repeat the extraction process 4 times combined
chloroformed extraction steamed to dryness on a water bath under vacuum. Dissolve the dry
residue in 5 ml of methanol. Solution was used as a sample.
Vasicine standard solution preparation: Place about 1.4 mg of vasicine in a 10 ml volumetric
flask and dissolve in methanol. Make the solution’s volume to the mark with methanol.
After TLC preparation and development the plate was scanned in the densitometer by linear
scanning at 256 nm by use of a TLC Scanner III CAMAG with D2 & W absorption, and
integrates the area of the spots corresponding to Vasicine standard.
Vasicine content in Linkus Syrup is calculated by the following formula:
ASMP × WSTD × Sample dilution × P
X = ---------------------------------------------------M
ASTD × Standard dilution × WSMP × 100
The content of the vasicine was found not less than 0.02 mg per Syrup.
3.5.Evaluation of Efficacy and Toxicity of Poly Herbal syrup–Linkus in
Experimental Animals
3.5.1 Preparation of linkus Extract and Syrup:
“Herbs were purchased through Inventory network Bureau of the Herbion Pakistan (Pvt.)
Restricted, Karachi from the nearby market. All examples were put away in dim at 23˚C. The
herbs used in Linkus syrup were morphologically contrasted and the genuine example

66
accessible at QC division of Herbion Pakistan Pvt. Ltd., their points of interest are as per the
following, Adhatoda vasica reference No. B18, Glycyrrhiza glabra reference No.M4, Piper
longum reference No. F1, Viola odorata reference No. B2, Hyssopus officinalis reference
No.Z1, Alpinia galangal reference No.A2. The various chemicals and reagents were of
unadulterated systematic review and acquired from nearby supplier”.
3.5.2 Preparation of Extracts:
Place Herbs (Barring Mulethi remove) with interim into processor. In the wake of squashing
of herbs blend with refined water (D. I.) water in extractor and put pounded herbs and Mulethi
remove independently. Mixed and after that heated till simmering. The temperature ought to
be between 110 - 1200 C. At that point moderate down the temperature and kept up to 90-100
C for 2.5 hours. After filtration the filtrate was exchanged to Vanish Include methyl paraben
and Propyl paraben to the concentrated thick concentrate & mixed for 10 minutes.
3.5.3 Manufacturing:
“The D.I water, sugar and Fluid glucose were put in a tank via auto measuring and blended by
stirrer. Exchanged the substance from measure tank to capacity jacketed tank with high temp
water temperature 60 to 80°C.Feed the sugar syrup to the cooker through generation Pump
concocted item to 148 to 153°C and gathered at the base up to certain level in blaze off vessel
outfitted with divider scrubber stir. Product transferred through the conical shaped valve with
micrometer adjustment from flash off vessel to vacuum chamber. Extract scrap with flavor
should not more than 3% of Lot size. Production pump reached the set number and open the
flash off vessel chamber which was automatically closed and vacuum released. Bowl moved
down by gravity due to weigh of cooked mass. Product mass transferred from bowl to
kneading plate through pan trolley. Add flavored compound and acid(s) to achieve the
hardness of product mass by using the chilled water, talc powder used for de moisture.
Transferred the mass to batch roller then pass for roping to Rope sizing machine. The set rope
for uni-plast machine was assembled and sized mass was stamped to give shape of Syrup in
compression machine and maintained .Syrup were finally passed through cooling tunnel to get
the desired hardness”.

67
3.5.4 Efficacy:
The efficacy of the linkus Syrup evaluated by Citric acid and linkus Syrup extracts. First
cough was induced by citric acid inhalation for 7 minutes with the ratio of 0.15mg/ml .The
mice individually were placed in a closed plexiglass chamber (20 × 10 × 10 cm). The cough
reflexes were counted for 7 minutes and compared to the cough with citric acid +linkus
extract, linkus extract + Diphenhydramine and Acefyllin Piperazine and linkus extract +
Dextromethorphan, Diphenhydramine.
3.5.5 Acute Toxicity:
Acute toxicity test of Linkus was performed on Mice of either sex (20-30 g). The animals
were treated with two doses (0.23 g dissolved in 1 ml of distilled water and 0.46 g / ml / kg of
body weight of Mice) of tablets, which were administered orally. These doses were selected
by considering the dosage of tablet in human adult and children, i.e. one tablet 3-4 times / day
(4 tablet / day) and maximum up to eight tablet / day. In another group of animals (Control)
0.9 % saline (0.46 ml / kg of body weight of mice, orally) was given. The animals were
continuously observed for 4 hours and changes in various autonomic and behavioral
responses were noted. Mice were kept under observation for a further period of 15 days to
check their general behavioral mortality. The used animal species were Albino rats, Strain
were Haffkine with both sexes male and female with 1:1 ratio. Weights were 150 – 250 g and
ages were between 4-6 months. Animals were fed with the pelleted animal food supplied by
animal feed industry. The water was given ad. Libitum.
Animals were caged and housed in the animal house of the Research and Development
Department, Herbion Pvt. Ltd., for 15 days. They were acclimatized for experimental work
purpose and were observed for normal behavior. Body weights between 150-200 g were
included with free from any fungal infection or any other disease and no injuries on their
body. However the animals with normal physiological functions were included. Body weights
below 150 g or above 200 g were considered to be excluded. Pregnant female rats, injured and
or fungal infections were also excluded.

68
3.5.6 Experimental Design:
Controlled single blind randomized study followed by morphological examination of organs
after 48 hours and estimation of biochemical parameters at the end of the study. Initial body
weight of each animal was recorded for dose calculation. Recommended adult dose was 1
lozenge (2.5 g) 6 times a days Or 15 g/day. Average body weight of an adult person was
considered 70 kg however the dose /kg of body weight were 15/70 = 0.21 g/kg.20 times
(4g/kg) the therapeutic dose was tested for acute toxicity. The drug was administered orally
with an oral syringe, by making the solution with distilled water. The number of animals
included in each group was 11.The control group of animals was administered water in rats.
The animals were kept under observation for 48 hours. Mortality and other abnormal signs
and symptoms of behavior, central nervous system, respiratory system, cardiovascular system,
and gastrointestinal system were noted. The animals were observed for their altered immune
response by noting the incidence of infections and inflammation and having chances of easy
lacerations. The animals were also observed for their abnormal locomotors behavior. At the
end of 48 hours body weight of each animal was recorded. The animals were sacrificed under
light ether anesthesia. The blood was collected. Different hematological parameters were
estimated. The serum was separated and processed for Biochemical parameters.
Hematological Parameters estimated included total RBC and WBC count, Hemoglobin (Hb)
estimation, Differential cell count , Biochemical estimations, Blood glucose, Serum total
protein, Serum cholesterol, Serum SGPT, Serum SGOT, Serum alkaline phosphatase, Total
bilirubin, Blood urea, Serum creatinine. The animals were dissected. The viscera of the drug
treated groups were compared with the control group of animals for inflammation, bleeding
and alterations of organs morphologically. All methodology including creatures was evaluated
and endorsed by the institutional creature consideration of Jinnah University for Women. The
creature convention was intended to minimize agony or uneasiness to the creatures.
3.5.7 Chronic Toxicity Testing:
The animal species for chronic toxicity testing were including Albino rats; strain Haffkine
with Sex ratio 1:1 with weight between 150 – 200 g and ages between 2 – 3 months. Body
weight between 150-200 g, free from any fungal infection and other diseases and injuries on
the body were included. Body weight below 150 g or above 200 g, Injuries on their body or

69
with fungal infections was excluded. The animals with abnormal respiratory, cardiovascular,
gastrointestinal, excretory and central nervous system functions were excluded from the
study. The animals were also observed for their abnormal behavior and excluded from the
study. The animals were caged and housed in the animal house of Department of
Pharmacology, Faculty of Pharmacy, Karachi University, for 15 days. They were estimated
for experimental work purpose and were watched for normal behavior
3.5.8 Experimental Design:
Controlled single blind randomized study followed by morphological examination of organs
and estimation of biochemical parameters at the end of the study. Initial body weight of each
animal was recorded for dose calculation. Recommended adult dose was 1 (2.5 g) 6 times a
days or 15 g/day, Average body weight of an adult person considered to be 70 kg and Dose
/kg of body weight were 0.21 g/kg as therapeutic dose.20 (4g/kg) times the therapeutic dose
was tested for chronic toxicity. The drug was administered orally with an oral syringe. The
drug was given daily up to 2 months. The control group of animals was given distilled water.
Body weight of animals was recorded every 15 days up to 2 months. Animals were kept under
constant observation. Mortality, if any was recorded. Any abnormal sign & symptoms of
behavior, respiratory system, central nervous system and cardiovascular system were noted.
The animals were observed for their altered immune response by noting infections and
inflammation. At the end of the 2 months, animals were sacrificed under light ether
anesthesia. The blood was collected by extravasation after decapitation. The serum was also
tested for Lipid profile& Biochemical parameters included Serum Lipid Profile, Biochemical
Parameters and Hematological Estimations
3.6. Post Marketing Phase IV Clinical Trial on Linkus Syrup:A phase IV randomized, open label clinical trial was conducted on different private schooling
systems. External IRB (institutional review board) approval has been taken from Darul Sehat
Hospital Karachi, Pakistan. The clinical trial was registered on FDA site clinicaltrial.gov with
unique protocal ID LINKUS-HR-01. For conducting a clinical trials multiple certified
clinical research associate (CRA) were hired. Children of 2-11 years age with oral assents
were included in the study. Written informed consent was taken by guardians and they were
free to quit any point in time. Children having history of bronchopulmonary dysplasia,
asthma, chronic bronchitis, cystic fibrosis and allergic rhinitis were excluded. Patients
having auto immune diseases and
HINA JUNAID
Highlight

70
At the time of patient enrolment, demographics, duration of illness, cough frequency score per
day were gauged with the help of parents and guardian with the help of 5 level likert scales.
After recruitment, patients were randomly divided into 3 groups. First group of study’s
subject were on Linkus syrup (Herbal medicine), However 2rd group of random picked
subjects were on Aminophylline with Diphenhydramine (allopathic medicine) and 3th groups
were taking Acefyllin Piperazine with Diphenhydramine (allopathic medication). After 14
days of treatment cough frequency and impact were assessed on subjects and juvenile life.
Enrolment duration was 5 months from private schooling system of East Karachi, Pakistan .In
every site with Linkus syrup (group 1) other 2 brands of allopathic syrup (Aminophylline
Diphenhydramine (group 2) and Acefyllin Piperazine with Diphenhydramine (group 3))
identical appearance with sweet taste were placed. Simple randomization was
prepared from computerized generated system. After enrolment a subject study code
was given to thepatients for further follow up and consultation. The guardian/parents were
fully aware about the concept of the study and the drug. Due to spillage of
investigational drug, two complementary bottles with dosing spoon were given for the
proving the adherence .Contact information of principal investigator and CRAs were shared
with the guardian/parents. Third follow-up visits were mandatory for each patient. Dosing
instructions were given by clinical investigator and CRAs recommended by the
manufacturing company of all 3 groups (National and multinational Pharma). Children
having 2-6 years (Aminophylline, Diphenhydramine) were taking 1.25-2.5 of 5ml teaspoon
every 4-6 hours however 6-12 yearschildren were on 0.75-1.5 ml teaspoon on every 4-6
hours. Children having 2-3 years
having allergic reaction /hypersensitivity from any herbal products were also excluded in the
study. Children on supplementations including heavy metals, iron, zinc and any other
alternative and herbal medication were considered to be excluded. Only one child from each
family was incorporate in the study. Children were inducted through the seasonal camps on
private schools. After successful completion of inclusion criteria, patients were recruited in
the study. Medical records and history were completely checked and reviewed. Cough impact
on children sleep assessed by the guardian. Investigational brochure was distributed in each
patient for awareness on each and every active ingredient present in the study drug. After
physical examination and details history patients were inducted in the study.
HINA JUNAID
Highlight

71
(Acefyllin Piperazine with Diphenhydramine) were taking 2.5 ml 3 times daily and 3-12 years
were taking 5ml 3-4 times daily .The third group of study subjects were taken Linkus syrup 1-
2 teaspoon 3-4 times daily . The Investigators and clinical research coordinator contact
information shared with every study subject/ guardian/ Parents for 24/7 contact in case of any
side effects and ADRs reporting. The parents/guardians were asked to note patients sleep
quality and frequency of cough from day 1 to day 14. Frequency was measured on the basis of
cough last night before treatment on day 1 and after treatment on day 14 on the basis of Likert
Scale (from 5 to 1). Child sleep disturbance and effects on parents sleep were rated on the
same on all four groups. For the determination of severity of cough a validated Wong baker
pain scale used in the study. The parents were asked to note any concomitant medication if
case of fever and other upper respiratory tract infection.

72
Figure 39. Steps Showing from Randomization to Analysis
Primary study outcomes were the duration and severity of upper respiratory infections (URIs)
and adverse events. However the efficacy of the investigational products were determine on
day 0-14 with the measurement of pain scale, gauging cough frequency and cough impact on
child and parent sleep. For measuring the symptoms 4 level scale were used to assess changes
from 1-5 (poor-excellent) on irritating cough, bronchitis and respiratory tract diseases with
mucus with respect to strength of stimulation, amount and consistency with ease of
expectorant (161).
Randomization N=360
(GP=A)
LINKUS
120 assigned to takeLinkus
- 26 withdraw before lastvisit
- 17 confussed toparticipate
-10 loss to followup
( 65)
Out of 67 only 65included in Analysis
(GP=2)
Aminophylline,Diphenhydramine
120 assigned toAminophylline,
Diphenhydramine
-17 withdraw before lastvisit
- 27 confussed toparticipate
- 17 loss to followup
(65)
All 65 included inAnalysis
(GP=3)
Acefyllin Piperazine,Diphenhydramine
120 assigned to takeAcefyllin Piperazine,Diphenhydramine
- 15 withdraw before lastvisit
-13 confussed toparticipate
-23 loss to followup
(65)
Out of 69 only 65included in Analysis
Induction
Loss to follow up
Analysis

73
The objective of the study is to determine an interquartile relationship between Polyherbal
Syrup Linkus with Acefyllin Piperazine, Diphenhydramine group and Aminophylline
Diphenhydramine group. In all four groups, Phase IV Comparative Randomised Control Trial
was established for determine the effectiveness of interquartile relations.
3.7.1 Methodology:
3.7.1.1 Participants:
All participants have given written informed consent from the parents after explaining the
nature, objective, intended outcome and assents from the children .They all have complained
of acute cough and has been previously episodes of cough ( last 3-4 days) or sudden onset .
Patients were not included in the study that has hypersensitive previously from any herbal
drug and not given consents.
Simple randomization was adopted to assign participants on either group including Linkus,
Acefyllingroup, and aminophylline diphenhydramine group.
The study was un blinded because all 3 treatments groups have different actives and different
dosing regimen. However, for analysis statistician was performed it blinded on codes.
The study was approved on IRB (Institutional review board) of Darul Sehat Hospital, Liaquat
medical and dental college Karachi, Pakistan. Study protocol, Case report form, informed
consent English and Urdu were presented in front of IRB before start of clinical trial. ICH and
GCP godliness (international conference of harmonization and good clinical practices) was
adopted.
3.7.An Interquartile Relationship between Polyherbal Extract Based Syrup
Linkus –A Phase IV Comparative Randomised Control Trial.
A randomize control trial was conducted from January to Sept 2016 in the private schools of
Pakistan , Including East Malir and West Malir Karachi Pakistan. Simple randomization
technique were adopted for randomization. A special approval has beentaken from the
schools with the explanation of intent and objective of study. A total 196patients were
included from different private schools, 56 male and 140 females with the meanage of 9
±1.82 were randomly assigned in 3 groups, 65 in linkus group, 65 in Acefyllin and 65in
Aminophylline Diphenhydramine group.
HINA JUNAID
Highlight
HINA JUNAID
Highlight
HINA JUNAID
Highlight

74
3.7.1.2 Procedure:
Patient’s demographics and basic information including nature of cough , frequency of cough
and severity of cough (minor, moderate and severe) asked and filled in Case report form with
the help of registered medical practitioner. Recurrence was measured on the premise of hack
the previous evening before treatment and after treatment on the premise of in particular, a ton
, to some degree , minimal incidental and not in any way ( from number 5 to 1).Child sleep
disturbance and effects on parents sleep were rated on the same on all three groups.
The phytochemical based syrup linkus recommended 10 ml given thrice daily for 14 days on
acute cough , however in comparison of quadruple therapy the acefyllin group recommended
to take 10 ml TDS and same with aminophylline diphenhydramine group.
The dose selection was implemented on the basis of standard practice. All study participants
were advised to take not any other medications except the investigational study drug. Linkus
syrup’s herb were purchased from the Joria market, Karachi and identified on the herbal
expert from university of Karachi.
3.7.1.3 Outcome Measure:
The outcomes of cough frequency was observed after 14 days treatment of syrups in 4 groups,
Children sleep disturbance and child cough impact on parent’s sleep was observed from 5 to 1
scale mentioned above on all 3 treatment groups. Medical practitioner filled out case report
form regarding demographics data , such as name, gender , severity of cough , frequency of
child’s cough before and after and its impact of parents sleep before and after . After 14 days
of treatment, adverse events and side effects were asked.
75
CHAPTER 4
RESULTS
76
4. CHAPTER FOUR - RESULTS
United Nations reported that, In Pakistan 18,000 people die every year from upper respiratory
tract infection. Pakistan is responsible for 20-30 % death of children under 5 years of age due
to the acute respiratory infection (162).Cough considered to be the acute respiratory infection
which has been increases day by day. In last years it was reported that in Karachi the Nasal
allergies have been increases rapidity. Due to continuous changing in Environment, the
causation factor of respiratory infections has gained attention. As per the WHO officials for
the years of 2000, Pakistan considered to the 5th country who the killer of children having
upper respiratory tract infections (163).
Cough medications is available under the category of OTC medication in Pakistan. Over the
counter (OTC) medication includes codeine and dextromethorphan are the most common
antitussive agents . Due to lack of proven evidences, over dosing cases and toxicity on cough
agents, The American Academy of Pediatrics not supported these agents(164, 165). Food and
drug administration (FDA) acclaims that OTC products include cough and related agents not
to be used for children under 2 years of age due to serious life threating effects(166). The
Herbal products has widely use throughout the globe since 5,000 years and considered to the
safest choice. In this Era of health care, Billions of dollars per year spend on OTC products
specifically for cough. The only paucity on OTC products is the availability of sound research
as unfortunately no clear evidence achieved on alternate medication.
To view all the claimed, the polyherbal formulation has been designed. The chemical,
biological and clinical evaluation with the standard successful market competitor has been
established to ensure that the herbal brand have full scientific ensured and published claims.
4.1. Results of Design Development of Linkus Syrup with Biomarker
Vasicine
The poly herbal linkus Syrup for sore throat and cough contains extracts of Adhatoda vasica
Nees. (Bansa), Glycyrrhiza glabra L.(Mulethi), Piper longum L. (Filfil Daraz),Alpinia
galangal (Khulanjan), Hyssopus officinalis (Zufa), Viola odorata (Banafshan) and Cordia

77
latifolia (Lasorda).Bioactive components of the herbs used in the poly- Herbal formulation
biomarker was identified and estimated for standardization . The determination in
appearance, weight, uniformity, diameter and thickness was analysed organoleptic ally. Assay
accomplished by HPTLC for the determination of vasicine contents was not less than 0.02 mg
per Syrup.While finished product specification included blister pack, leak test and
microbiological testing .See (Table 09) for details of evaluation
4.1.1 TLC Plate for HPTLC Vasicine
The Sample TLC plate and standard TLC were prepared with Methanol. Multiple dilutions
have prepared with herbal Syrup for test for less chances of error.
Figure 40. TLC Plate with Standard and Sample Spots
Figure 41. Plate with Standard and Sample Spots Developed
77
latifolia (Lasorda).Bioactive components of the herbs used in the poly- Herbal formulation
biomarker was identified and estimated for standardization . The determination in
appearance, weight, uniformity, diameter and thickness was analysed organoleptic ally. Assay
accomplished by HPTLC for the determination of vasicine contents was not less than 0.02 mg
per Syrup.While finished product specification included blister pack, leak test and
microbiological testing .See (Table 09) for details of evaluation
4.1.1 TLC Plate for HPTLC Vasicine
The Sample TLC plate and standard TLC were prepared with Methanol. Multiple dilutions
have prepared with herbal Syrup for test for less chances of error.
Figure 40. TLC Plate with Standard and Sample Spots
Figure 41. Plate with Standard and Sample Spots Developed
77
latifolia (Lasorda).Bioactive components of the herbs used in the poly- Herbal formulation
biomarker was identified and estimated for standardization . The determination in
appearance, weight, uniformity, diameter and thickness was analysed organoleptic ally. Assay
accomplished by HPTLC for the determination of vasicine contents was not less than 0.02 mg
per Syrup.While finished product specification included blister pack, leak test and
microbiological testing .See (Table 09) for details of evaluation
4.1.1 TLC Plate for HPTLC Vasicine
The Sample TLC plate and standard TLC were prepared with Methanol. Multiple dilutions
have prepared with herbal Syrup for test for less chances of error.
Figure 40. TLC Plate with Standard and Sample Spots
Figure 41. Plate with Standard and Sample Spots Developed

78
4.1.2 Chromatograms of Vasicine by HPTLC.
Figure 42.Vasicine Standard
Figure 43. Vasicine Sample
78
4.1.2 Chromatograms of Vasicine by HPTLC.
Figure 42.Vasicine Standard
Figure 43. Vasicine Sample
78
4.1.2 Chromatograms of Vasicine by HPTLC.
Figure 42.Vasicine Standard
Figure 43. Vasicine Sample

79
The overall measures taken for the analysis of qualitative, quantitative and physical
parameters at bulk and finished stage expose the adherence with the processes developed and
adopted are in compliance with the standard of GMP guidelines and requirements
consequently supporting the impression that poly herbal Syrup can compete with the good
standard products. In another study it was sited and concluded that herbal linkus syrup was
analysed by the quantitative and qualitative manner for determination of biomarker and used
for the validation of vasicine(167).Study of the manufacturing process of Vasu syrup for
cough was validated which used the poly herbal formulation with adherence to
reproducibility(168).
4.2. Biomarkers Present On Linkus Extract (Formed Syrup)
This experimental study includes quantitative estimation of Piperine and Glycyrrhizin in poly
herbal formulation named ‘Linkus Cough Syrup’. “Piperine is the trans stereoisomer of 1-
piperoylpiperidine. It is also known as (E, E)-1- piperoylpiperidine and (E, E)-1- [5-(1, 3-
benzodioxol-5-yl)-1-oxo-2, 4-pentdienyl] piperidine. Piperine is widely used in various herbal
cough syrups for its potent anti-tussive and bronchodilator properties .As in literature survey
5-13 clearly reveals that there is no proper analytical method available for the quantitative
estimation of Piperine in herbal cough syrups; this reproductive quantitative estimation
reveals Piperine as shown in figure 1”. For optimization, different mobile phase compositions
have been used for separation including Benzene: Ethyl acetate 2:1 (v/v) with ultra violet light
345 nm in HPLC method.
The techniques including simple chromatographic technique like Thin layer chromatography
is used to identify the contaminants in plants materials. Chromatograms are the finger prints
which are used to determine the different constituents of plants materials and impurities.
HPTLC is the key techniques for the separation of volatile substance with the absorbance of
UV visible range. These complex methods give a compound unique finger impression to the
way of chemicals or contaminations present in the plant or concentrate. In view of the idea of
photograph proportionality, the chromatographic fingerprints of natural drugs can be utilized
to address the issue of value control, confirmation and homogenize the plant extract .Herbal
research moves a step towards innovation with quality standards in health care division and
achieving a great market share. This study encountered Poly herbal formulation which is the
demand of current market.

80
The retention time found to be 1-8.100 with the recovery of 100% Piperine in polyherbal
syrup however the mAU OF 32.0 as shown in fig. 44 and 45 below.
Figure 44. Peak Response of Piperine in Linkus Syrup
Figure 45. Peak Response of Piperine Standard

81
Along side it Glycyrrhiza glabra has broad pharmacological impacts for individuals. The most
widely recognized restorative use is for treating upper respiratory illnesses including hacks,
dryness, sore throat and bronchitis(169, 170) By performing investigation on HPTLC silica
gel ,TLC chamber has created. The dissolvable framework incorporates Ethyl acetic acid
derivation: Methanol: Water: Formic Acid, 15:5:1:1 (v/v/v/v) as a dissolvable framework with
ultra violet light 254 nm. The TLC plate was observed and Rf value was found to be 0.18 in
linkus syrup and standard shown in table 4. The establishment of biomarkers identification
has been developed in linkus cough syrup. There were no interaction has been found between
the compounds and excipients. This method was having high recovery and reproducibility in
any polyherbal formulation.
Figure 46: Peak Response of Glycyrrhizin in Linkus Syrup
81
Along side it Glycyrrhiza glabra has broad pharmacological impacts for individuals. The most
widely recognized restorative use is for treating upper respiratory illnesses including hacks,
dryness, sore throat and bronchitis(169, 170) By performing investigation on HPTLC silica
gel ,TLC chamber has created. The dissolvable framework incorporates Ethyl acetic acid
derivation: Methanol: Water: Formic Acid, 15:5:1:1 (v/v/v/v) as a dissolvable framework with
ultra violet light 254 nm. The TLC plate was observed and Rf value was found to be 0.18 in
linkus syrup and standard shown in table 4. The establishment of biomarkers identification
has been developed in linkus cough syrup. There were no interaction has been found between
the compounds and excipients. This method was having high recovery and reproducibility in
any polyherbal formulation.
Figure 46: Peak Response of Glycyrrhizin in Linkus Syrup
81
Along side it Glycyrrhiza glabra has broad pharmacological impacts for individuals. The most
widely recognized restorative use is for treating upper respiratory illnesses including hacks,
dryness, sore throat and bronchitis(169, 170) By performing investigation on HPTLC silica
gel ,TLC chamber has created. The dissolvable framework incorporates Ethyl acetic acid
derivation: Methanol: Water: Formic Acid, 15:5:1:1 (v/v/v/v) as a dissolvable framework with
ultra violet light 254 nm. The TLC plate was observed and Rf value was found to be 0.18 in
linkus syrup and standard shown in table 4. The establishment of biomarkers identification
has been developed in linkus cough syrup. There were no interaction has been found between
the compounds and excipients. This method was having high recovery and reproducibility in
any polyherbal formulation.
Figure 46: Peak Response of Glycyrrhizin in Linkus Syrup

82
Figure 47: Peak response of Glycyrrhizin and Standard
Linkus is a poly herbal formulation analyzed for antioxidant, reducing, and lipoxygenase and
ACE inhibition activity with different concentration (10μl/ml, 50μl/ml, 100μl/ml) on 2 dosage
different dosage forms comprising of Syrup and syrup. “When formulations of syrup and
Syrup were compared at various concentrations (10 μl/ml, 50 μl/ml,100 µg/ml), DPPH radical
scavenging activity increased in a dose dependent manner for both formulations just like
standard BHA as shown in table. It clearly displayed that both dosage forms including syrup
and Lozenges have good antioxidant potential i.e. 23.4%, 45.7%, 65.0% w.r.t standard BHA”.
For determining the reducing activity ferrous was the leading component. Both dosage forms
syrup and Lozenges have some reducing ability as compare to standard as shown in table
4.For protecting the gastric mucosa ,the Lozenges and Syrup have some anti-urease activity
82
Figure 47: Peak response of Glycyrrhizin and Standard
Linkus is a poly herbal formulation analyzed for antioxidant, reducing, and lipoxygenase and
ACE inhibition activity with different concentration (10μl/ml, 50μl/ml, 100μl/ml) on 2 dosage
different dosage forms comprising of Syrup and syrup. “When formulations of syrup and
Syrup were compared at various concentrations (10 μl/ml, 50 μl/ml,100 µg/ml), DPPH radical
scavenging activity increased in a dose dependent manner for both formulations just like
standard BHA as shown in table. It clearly displayed that both dosage forms including syrup
and Lozenges have good antioxidant potential i.e. 23.4%, 45.7%, 65.0% w.r.t standard BHA”.
For determining the reducing activity ferrous was the leading component. Both dosage forms
syrup and Lozenges have some reducing ability as compare to standard as shown in table
4.For protecting the gastric mucosa ,the Lozenges and Syrup have some anti-urease activity
82
Figure 47: Peak response of Glycyrrhizin and Standard
Linkus is a poly herbal formulation analyzed for antioxidant, reducing, and lipoxygenase and
ACE inhibition activity with different concentration (10μl/ml, 50μl/ml, 100μl/ml) on 2 dosage
different dosage forms comprising of Syrup and syrup. “When formulations of syrup and
Syrup were compared at various concentrations (10 μl/ml, 50 μl/ml,100 µg/ml), DPPH radical
scavenging activity increased in a dose dependent manner for both formulations just like
standard BHA as shown in table. It clearly displayed that both dosage forms including syrup
and Lozenges have good antioxidant potential i.e. 23.4%, 45.7%, 65.0% w.r.t standard BHA”.
For determining the reducing activity ferrous was the leading component. Both dosage forms
syrup and Lozenges have some reducing ability as compare to standard as shown in table
4.For protecting the gastric mucosa ,the Lozenges and Syrup have some anti-urease activity
4.3. In-Vitro Antioxidant, Reducing, Lipoxygenase and ACE
InhibitionActivity of Polyherbal Drug Linkus Syrup

83
too as shown in table 5. Lipoxygenase compounds are the derivatives of arachadonic acid
.After analysis it was determined that the Syrup and capsules have some efficacy for the
reduction of inflammation, results are shown in table below.
4.3.1 Methodology:
Oxidant damage to proteins, macromolecules and DNA and it causes many damages in
human tissues including aging (171). Currently available antioxidant compound including
BHA (butylated hydroxyanisole) and BHT (butylated hydroxytoluene) have negative impact
on human health (172). For reducing the impact of oxidants, the natural occurring plants have
been used for medical purpose(173).Various plant species have been explored for antioxidant
activity (139, 174, 175)The DPPH is sensitive method for antioxidant screening for plant
extracts. For the determination of the antioxidant activity in poly herbal formulation
scavenging ability has been employed. Absorption has been noted at 517 nm due to odd
electron. Good antioxidant activity has been observed in both dosage forms. For
determination of reducing activity Fe +3–Fe+2 was the investigating point (176). The
antioxidant activity the decreasing potential of a compound seems to be a substantial indicator
(177). The par cent reducing ability was determined by the BHA standard formula and the
results found exhibited good reducing ability in the poly herbal formulation.
Free radical and lipid per oxide play a vital role for the development of ulcer in human (177).
Linkus poly herbal formulation shows a good gastric protection. The herbal formulations have
anti-inflammatory activity including many disorders such as cough ,chronic laryngitis and
many other malaise (178, 179).Beside all the functions and activities of linkus formulation
showed good lipoxygenase inhibition activity Cough is the common today’s symptom seen
in overall family practice. Clinically, a cough is nearly a symptom of an underlying illness. It
is significant to look beyond it to treat the cause and, hence achieve the maximal relief from
cough and related symptoms. Studies have shown that there is an interaction between
respiratory tract infections and antioxidant activities (180) and oxidative stress present in
blood due to respiratory infections (181).Lipoxygenase and leukotriene are the key factors for
the inflammatory responses and respiratory distress. Multiple events suggested that
lipoxygenase have strong relation in physiological event in respiratory tract infection(182).

84
This study has verified the visible antioxidant, urease and lipoxygenase activities in poly
herbal formulation Linkus Cough Syrup and Syrup. These dosage forms have contributing
factors towards the indication cough as antioxidant and anti-inflammatory activity. These
types of activities are due to free radical 2, 2’-diphenyl-1-picryl hydrazyl, conversion of ferric
into ferrous state, ammonia production using the indophenol method and hydroperoxides
produced in the lipoxygenation reaction.
Table 17. In-vitro Antioxidant Activity of Linkus Formulation
S.NoConcentration
tested
Percent Activity
(%)(syrup) ± SEM
Percent Activity ±
SEM
(%)(Lozenges)
Percent
Activity ± SEM
(%)(standard)
1 10 μg/ml 33.4±0.9464 21.2±0.421 71.2± 0.41
2 50 μg/ml 45.7 ± 0.6454 40.7 ± 0.443 87.9± 0.45
3 100 μg/ml 65.0±0.9124 58.0±0.512 96.8± 0.51
Table 18. Linkus Syrup Reducing Ability with reference to Standard
S.NoConcentration
tested
Percent Activity
(%)(syrup) ± SEM
Percent Activity
(%)(capsules) ) ±
SEM
Percent Activity
(%)(standard) ) ±
SEM
1 10 μg/ml 12.8 ± 0.312 10.3 ± 0.131 43.7 ± 0.421
2 50 μg/ml 34.5 ±0.412 24.7± 0.213 65.8 ± 0.321
3 100 μg/ml 43.6± 0.561 34.6 ± 0.312 87.4 ± 0.112
Table 19. Antiurease Activity of Linkus Syrup with reference to Standard
S.No
Concentration
tested
Percent Activity
(%)(syrup) ±
SEM
Percent Activity
(%)(capsules) ) ±
SEM
Percent Activity
(%)(standard) ) ±
SEM
1 10 μg/ml 13.9 ± 0.121 10.8 ±0.210 64.5± 0.321
2 50 μg/ml 44.9 ±0.321 35.7± 0.412 76.5± 0.213
3 100 μg/ml 65.9± 0.213 50.8 ± 0.312 89.9 ± 0.312

85
Table 20. Lipoxygenase Inhibiting Activity by Polyherbal Formulation Linkus.
S.No Concentration testedPercent Activity
(%)(syrup) ± SEM
Percent Activity
(%)(capsules) ) ±
SEM
Percent Activity
(%)(standard) ) ±
SEM
1 10 μg/ml 14.9 ± 0.213 12.2 ± 0.312 64.5± 0.410
2 50 μg/ml 46.8 ±0.611 31.0± 0.410 76.5± 0.612
3 100 μg/ml 56.1± 0.412 40.8 ± 0.312 89.9 ± 0.712
4.4. Antimicrobial Analysis of Polyherbal Formulation Linkus Cough Syrup
Linkus is the excellent blend of polyherbal formulation for cough and related symptoms. The
main herbs of Linkus syrup is mentioned in below table 21.The mentioned herbs were using
for cough since decays. For maintaining the flavors acceptability and palatability have
established with the help of sugar, peppermint oil, citric acid and clove oil.
Table 21. Content of Linkus Syrup and its Anti-microbial Effects
S. NO INGREDIENTS QUANTITY/ 120 ml
ANTIMICROBIAL ACTION
1. Adhatoda vasica – Bansa 7.2 g
Work against Staphylococcus aureus,Streptococcus pyogens, Escherichia coli,
Pseudomonas aeruginosa, Proteus vulgarisand Klebsiella pneumonia (150)
2. Piper longum – Filfil Daraz 1.2 gActivity against S.aureus, E.coli,
B.megaterium, B.sphaericus, B. polymyxa(117, 183)
3. Cordia latifolia – Sapistan 1.2 g Work against Staphylococcus aureus (152)
4.Glycyrrhiza glabra – Mulethi
Extract900 mg
Works against S.aureus, E.faecalis, andE.coli, A.viscosus and S.sanguis (153)
5. Hyssopus officinalis – Zufa 600 mgAct against S. pyogenes, S.aureus,C.albicans
and E.coli.(184)
6. Alpinia galangal – Khulanjan 600 mg
Work against Escherichia coli,Salmonellaenteriditis, Clostridium perfringens,
Staphylococcus aureus, Campylobacterjejuni, Bacillus cereus and fungi such asSaccharomyces cerevisiae, Hansenulaanomala, Mucor mucedo and Candida
albicans (155)
7.Onosma bracteatum –
Gaozaban1.2 g
S.aureus ,P.aeruginosa ,E.coli and Spneumonia (156)

86
Antimicrobial activity of the Linkus was evaluated on different microorganisms included
Gram positive and gram negative .The method which was adopted for antimicrobial analysis
was well and disc diffusion method as shown in figure no 48. Sensitivity on both methods is
clearly shown below.
Figure 48: Antimicrobial Analysis of the Linkus
The test micro-organism included Staphylococcus aureus, Streptococcus pyogenes,
Salmonella spp and Pseudomonas aeruginosa was checked on Linkus cough syrup .The anti-
microbial analysis was performed on sample A and B. Both test drugs became sterile on auto
clave. Gram positive micro-organisms included Staphylococcus aureus, Streptococcus
pyogenes and Salmonella spp however gram negative micro-organisms included
Pseudomonas aeruginosa were appraised as shown in table 17 and 18.
86
Antimicrobial activity of the Linkus was evaluated on different microorganisms included
Gram positive and gram negative .The method which was adopted for antimicrobial analysis
was well and disc diffusion method as shown in figure no 48. Sensitivity on both methods is
clearly shown below.
Figure 48: Antimicrobial Analysis of the Linkus
The test micro-organism included Staphylococcus aureus, Streptococcus pyogenes,
Salmonella spp and Pseudomonas aeruginosa was checked on Linkus cough syrup .The anti-
microbial analysis was performed on sample A and B. Both test drugs became sterile on auto
clave. Gram positive micro-organisms included Staphylococcus aureus, Streptococcus
pyogenes and Salmonella spp however gram negative micro-organisms included
Pseudomonas aeruginosa were appraised as shown in table 17 and 18.
86
Antimicrobial activity of the Linkus was evaluated on different microorganisms included
Gram positive and gram negative .The method which was adopted for antimicrobial analysis
was well and disc diffusion method as shown in figure no 48. Sensitivity on both methods is
clearly shown below.
Figure 48: Antimicrobial Analysis of the Linkus
The test micro-organism included Staphylococcus aureus, Streptococcus pyogenes,
Salmonella spp and Pseudomonas aeruginosa was checked on Linkus cough syrup .The anti-
microbial analysis was performed on sample A and B. Both test drugs became sterile on auto
clave. Gram positive micro-organisms included Staphylococcus aureus, Streptococcus
pyogenes and Salmonella spp however gram negative micro-organisms included
Pseudomonas aeruginosa were appraised as shown in table 17 and 18.

87
Table 22: Zone of Inhibition on Sample A (Linkus Cough Syrup)
Sample "A"Sterility Test Product is sterile.
S.No
StaphylococcusAureus
Streptococcuspyogenes
PseudomonasAeruginosa Salmonella
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
1 27mm 12mm 26mm 17mm 0 (R) 0 (R) 41mm 0 (R)
2 26mm 11mm 37mm 16mm 0 (R) 0 (R) 42mm 0 (R)
3 25m 11mm 35mm 16mm 0 (R) 0 (R) 43mm 0 (R)
On every sample analysis (test product A and B Linkus), the test was performed 3 times for
minimizing the human errors on both disc and well diffusion method.
Table 23: Zone of inhibition on Sample B (Linkus Cough Syrup)
Sample "B"Sterility Test Product is sterile.
S.No
Staphylococcusaureus
Streptococcuspyogenes
Pseudomonasaeruginosa Salmonella spp
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
WellDiffusionMethod
DiscDiffusionMethod
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
100ul(6 mg)
10ul(0.6 mg)
1 26mm 10mm 37mm 18mm 0 (R) 0 (R) 40 0 (R)
2 25mm 10mm 38mm 16mm 0 (R) 0 (R) 40 0 (R)
3 27mm 10mm 37mm 18mm 0 (R) 0 (R) 41 0 (R)
The test drug Linkus is compared with the given MIC concentration of standard amoxicillin
and ampicillin. Fig.49 Linkus shows more sensitivity on Streptococcus pyogenes and
Salmonella spp as compared to the other marked generic which is recommended for the upper
respiratory tract infections and cough. However it was evaluated that Pseudomonas
Aeruginosa showed resistant in both disc diffusion and agar method.

88
Figure 49: Comparative Zone of Anti-microbial inhibition of Linkus versus Ampicillin andAmoxicillin
4.5.Evaluation of Efficacy and Toxicity of Poly Herbal Syrup –Linkus In
Experimental Animals:
The linkus Syrup efficacy was developed on 3 different models including citric acid +linkus
extract with both sexes. Citric acid was used to developed cough reflexes and then minimize
by linkus syrup as shown in table 19
Table 24. 1 mg /Kg Citric Acid + Linkus Extract on Female Rats
AnimalsCough Reflexes
Control 10mg/kg 20mg/kg 50mg/kg 100mg/kg 200mg/kg 300mg/kg
1 129 - 220 204 167 147 141
2 235 170 141 197 181 161 153
3 254 227 260 201 144 189 127
4 241 263 201 120 169 137 106
5 194 277 128 206 172 190 184
Mean 211 234 190 186 167 165 142
12.83
35.00
0.00
41.17
12
23
13
2021.8
14.517
15
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
StraphlococcousAureus
Streptococcous PseudomonasAeriginosa
Salmonella
Dia
met
er o
f zo
ne o
f in
hibi
tion
(in
mm
)
Test Organisms
Comparative Zone of Inhibition
Linkus
Ampicillin
Amoxicillin

89
However the reference drug was a combination of Diphenhydramine with Acefyllin
Piperazine and citric acid for cough reflexes in male rats were shown in table 20
Table 25. 1 gm/kg Citric Acid+ Diphenhydramine and Acefyllin Piperazine
AnimalsCough Reflexes
Control 150µl/kg 500µl/kg
1 129 208 131
2 235 304 262
3 254 177 226
4 241 243 141
5 194 212 166
Mean 211 229 185
The cough reflexes on Male rats with citric acid Dextromethorphan and Diphenhydramine in
table 21 and 22.
Table 26. 1 gm/kg Citric Acid + Linkus Extract
AnimalsCough Reflexes
Control 10mg/kg 20mg/kg 50mg/kg 100mg/kg 200mg/kg 300mg/kg
1 240 294 203 154 138 153 185
2 255 191 284 187 158 163 101
3 248 134 222 250 175 173 105
4 129 150 191 164 151 164 99
5 264 262 152 227 106 182 173
Mean 227 206 210 196 146 167 133
Table 27: Citric Acid + Dextromethorphan, Diphenhydramine
AnimalsCough Reflexes
150µl/kg 500µl/kg
1 266 164
2 181 131
3 235 172
4 187 103
5 266 111
Mean 227 136

90
The cough reflexes induced by citric acid were reduced in both sexes with the help of linkus
syrup. The acute and chronic toxicity has been observed on different body weights,
biochemical parameters and hematological parameters in table 23, 24 and 25.
Table 28: Effect of Linkus Syrup on Body Weight (Dose 4 gm/kg)
Control Group Experimental Group
AnimalInitial
Weight(gms)
Weight After48 Hrs Of
AdministrationAnimal
InitialWeight(gms)
Weight After 48 HrsOf Administration
1 245 243 1 223 222
2 248 245 2 225 225
3 219 221 3 236 235
4 243 240 4 241 242
5 233 233 5 210 212
6 242 241 6 229 230
7 230 229 7 233 232
8 239 239 8 226 226
9 210 211 9 239 238
10 225 225 10 235 236
11 211 210 11 231 231
Mean, Standard Deviation, Standard Error of Mean.
Mean 231.36 230.64 Mean 229.82 229.91
S.D. 12.39 11.06 S.D. 9.20 8.83
S.E.M. 3.74 3.34 S.E.M. 2.77 2.66

91
Table 29: Effect of Linkus Syrup on Biochemical Parameters (Dose 4 gm /kg)
Parameters Control GroupExperimental
Group p value
Glucose % g 87.2 ± 3.21 86.78 ± 2.26 _
Total protein g/dl 5.55 ± 0.18 5.96 ± 2.16 _
Cholesterol 82.56 ± 4.96 86.96 ± 5.96 _
SGPT U/l 15.96 ± 12.63 17.86 ± 6.96 _
SGOT U/l 22.96 ± 1.11 25.96 ± 4.96 _
Alkalinephosphatase
19.74 ± 14.85 18.63 ± 11.74 p <0 .01
Urea mg/dl 30.63 ± 6.96 32.85 ± 4.63 _
Creatinine mg/dl 0.86 ± 1.23 0.91 ± 2.96 _
Total bilirubinmg/dl
0.88 ± 0.02 0.87 ± 0.36 _
n=11Table 30: Effect of Linkus Syrup on Hematological Parameters (Dose 4 gm/ kg)
ParametersControl Group
(Mean± S.E.M.)
Experimental Group(Mean ± S.E.M.)
Hb %g 15.23 ± 0.36 14.63 ± 1.25
Total RBC count mill/mm3 8.56 ± 2.366 7.98 ± 4.63
Total WBC count housd/mm3 12.58 ± 4.52 13.52 ± 1.2
Neutrophils % 70.12 ± 5.26 69.75 ± 4.63
Lymphocytes % 25.63 ± 1.63 24.63 ± 1.63
Eosinophill % 2.12 ± 1.26 2.63 ± 5.36
Monocytes % 2.23 ± 4.12 2.63 ± 4.96
Basophill % 0.23 ± 4.63 0.22 ± 4.13

92
In Chronic toxicity testing no abnormality was observed in the animals when drug was
administered for 2 months. The function of respiratory system, cardiovascular system, Central
nervous system and gastrointestinal system were normal. No abnormal behavior of the
animals was noted. Biochemical, lipid profile & hematological parameters have not
significantly altered, thereby confirming the safety of the drug. The increase in the weights of
spleen and skeletal muscles are statistically significant. There was no statistical significant
change in body weights of the animal. The functions of central nervous system,
cardiovascular system, respiratory system, gastrointestinal system and excretory system were
all normal. No abnormalities in the behavior of the animals were seen. Different biochemical
parameters estimated in rats belonging to test group were complete to respective biochemical
parameters in the control group of rats. No mortality was seen as shown in table 31
Table 31: Chronic Toxicity Effect of Linkus Syrup on Body Weight
Control Group Experimental Group
Initial Weight (G)(Mean ± S.E.M)
Weight After 2Months Of
Administration(Mean ± S.E.M)
Initial Weight (G)(Mean ± S.E.M)
Weight After 2 MonthsOf Administration
(Mean ± S.E.M)
179 ± 0.23 227 ± 0.36 190 ± 1.41 243 ± 0.96
n = 11

93
Table 32. Average Weight of Body Organs
Body Organ Control Group(Mean ± S.E.M)
Experimental Group(Mean ± S.E.M)
Heart 0.61 ± 0.21 0.72 ± 4.63
Liver 4.53 ±0.36 6.13 ± 5.13
Spleen 0.346 ± 2.50 * 0.64 ± 4.13
Kidney 1.32 ± 4.63 1.42 ± 0.42
Adrenals 0.12 ± 1.63 0.15 ± 3.46
Skeletal muscles 0.46 ± 3.95 * 0.76 ± 1.46
“n = 11, Average value ± S.E.M, * p < 0.05 as compare to control, ** p < 0.005 as compare tocontrol”
Table 33. Comparison of Toxic Effects on Lipid Profile
Parameters Control Group Experimental Group
Blood glucose mg/dl 56.63 ± 2.63 57.65 ± 4.62
Bilirubin mg/dl 0.62 ± 0.21 0.63 ± 0.42
Alkaline phosphatase U/l 9.97 ± 5.62 9.78 ± 4.16
SGPT U/l 33.65 ± 4.78 32.95 ± 10.23
Creatinine mg/dl 0.89 ± 1.23 0.87 ± 4.62
Total protein g/dl 5.46 ± 4.13 5.56 ± 5.79
Urea mg/dl 29.46 ± 7.63 30.62 ± 8.54
“n = 11, Average value ± S.E.M, * p < 0.05 as compare to control, ** p < 0.005 as compareto control”

94
Table 34. Comparison Of Hematological Toxicities
Parameters Control Group Experimental Group
Hemoglobin mg/dl 15.96 ± 5.63 15.45 ± 7.62
Total RBC count 8.36 ± 8.62 9.12 ± 10.21
Total WBC count 9.5 ± 11.21 9.45 ± 5.84
Differential WBC count (%)
Neutrophill 29.33 ± 2.63 28.52 ± 8.45
Lymphocytes 65.23 ± 5.96 64.85 ± 12.63
Eosinocytes 5.16 ± 4.75 5.98 ± 16.52
Monocytes 2.0 ± 1.23 2.67 ± 7.95
Basophills 0.62 ± 7.65 0.76 ± 10.89
4.6. Efficacy and Safety of Linkus, Aminophylline Diphenhydramine and
Acefyllin Piperazine for the Treatment of Cough in Children
A total of 360 participants were inducted in the study. Overall rate of patient participation
from induction to analysis were 54.1%.The analysis based on 65 patients in each
groups(total=195(65+65+65)) who were completed the follow up. Patient randomization,
recruitment , selection nad analysis can be seen in figure 39.The patient who moves to the
foreign country ,switched school, felt discomfort, required other benefits to come again were
considered to lose of follow up .The demographics of the completed study population were
mentioned in Table 28.Duration of illness ,cough frequency score before treatment ,cough
impact on child sleep and parents quality were also mentioned in the same table. On all 3
interventional groups, age, ethnic group were found to be the more significant (p<0.001).
From randomization, to analysis.
HINA JUNAID
Highlight
HINA JUNAID
Highlight
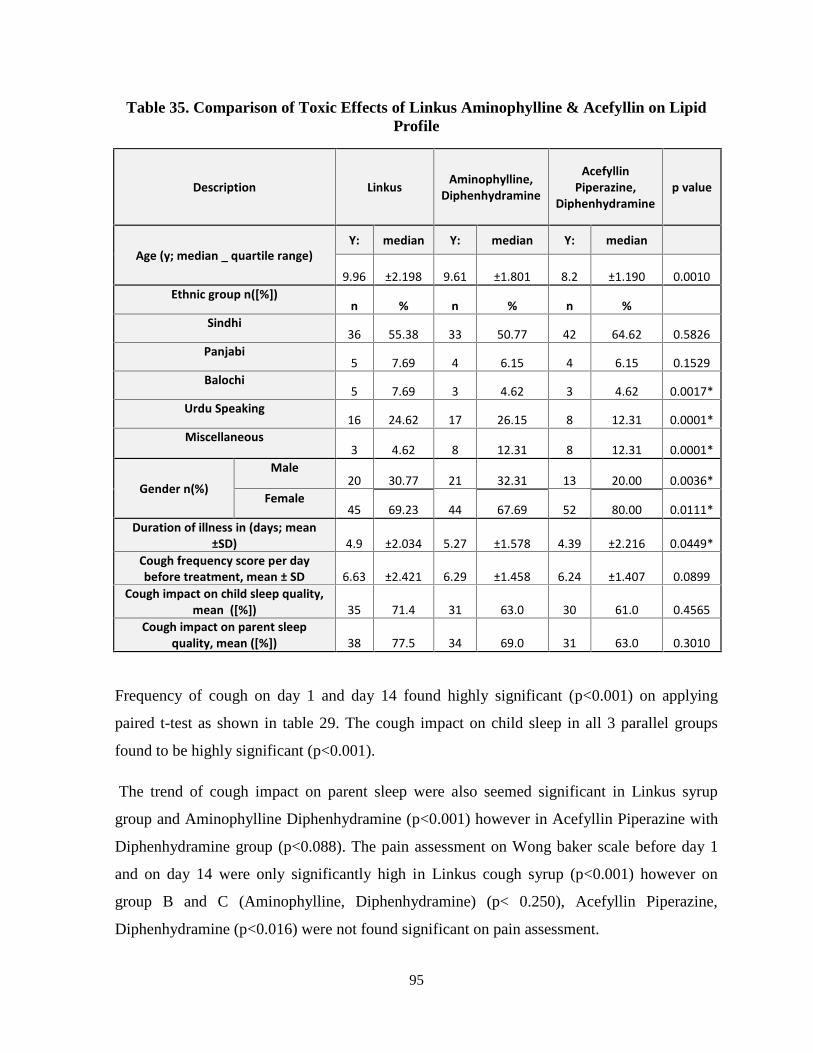
95
Table 35. Comparison of Toxic Effects of Linkus Aminophylline & Acefyllin on LipidProfile
Description Linkus Aminophylline,Diphenhydramine
AcefyllinPiperazine,
Diphenhydraminep value
Age (y; median _ quartile range)Y: median Y: median Y: median
9.96 ±2.198 9.61 ±1.801 8.2 ±1.190 0.0010Ethnic group n([%])
n % n % n %Sindhi
36 55.38 33 50.77 42 64.62 0.5826Panjabi
5 7.69 4 6.15 4 6.15 0.1529Balochi
5 7.69 3 4.62 3 4.62 0.0017*Urdu Speaking
16 24.62 17 26.15 8 12.31 0.0001*Miscellaneous
3 4.62 8 12.31 8 12.31 0.0001*
Gender n(%)
Male20 30.77 21 32.31 13 20.00 0.0036*
Female45 69.23 44 67.69 52 80.00 0.0111*
Duration of illness in (days; mean±SD) 4.9 ±2.034 5.27 ±1.578 4.39 ±2.216 0.0449*
Cough frequency score per daybefore treatment, mean ± SD 6.63 ±2.421 6.29 ±1.458 6.24 ±1.407 0.0899
Cough impact on child sleep quality,mean ([%]) 35 71.4 31 63.0 30 61.0 0.4565
Cough impact on parent sleepquality, mean ([%]) 38 77.5 34 69.0 31 63.0 0.3010
Frequency of cough on day 1 and day 14 found highly significant (p<0.001) on applying
paired t-test as shown in table 29. The cough impact on child sleep in all 3 parallel groups
found to be highly significant (p<0.001).
The trend of cough impact on parent sleep were also seemed significant in Linkus syrup
group and Aminophylline Diphenhydramine (p<0.001) however in Acefyllin Piperazine with
Diphenhydramine group (p<0.088). The pain assessment on Wong baker scale before day 1
and on day 14 were only significantly high in Linkus cough syrup (p<0.001) however on
group B and C (Aminophylline, Diphenhydramine) (p< 0.250), Acefyllin Piperazine,
Diphenhydramine (p<0.016) were not found significant on pain assessment.

96
Table 36. Comparison First Visit (Day 1) versus Last day (Day 14)
Description First Visit ( Day 1) Last Visit ( Day 14) pvalue
Cough frequency
Linkus 5.96 ±1.870 3.08 ±1.115 0.001*
Aminophylline, Diphenhydramine 6.53 ±1.401 4.88 ±1.379 0.001*Acefyllin Piperazine,Diphenhydramine 5.94 ±2.313 3.98 ±1.377 0.001*
Cough impact on child sleep
Linkus 3.86 ±0.957 2.88 ±8.57 0.001*
Aminophylline, Diphenhydramine 3.86 ±0.957 3.12 ±1.11 0.001*Acefyllin Piperazine,Diphenhydramine 3.86 ±.816 3.29 ±0.764 0.001*
Cough impact on parent sleep
Linkus 2.96 ±0.889 1.69 ±0.812 0.001*
Aminophylline, Diphenhydramine 2.24 ±1.677 2.08 ±1.426 0.001*Acefyllin Piperazine,Diphenhydramine 2.41 ±1.171 2.02 ±1.127 0.088*
Wong Baker Face scale n(%)
Linkus n(%)No Pain Worst Pain ever No Pain Worst Pain ever
0.00125 51.00 24 48.90 38 51.0 11 22.40
Aminophylline, Diphenhydraminen(%)
No pain Worst Pain ever No pain Worst Pain ever0.250
28 57.14 21 42.85 28 57.14 18 36.73
Acefyllin Piperazine,Diphenhydramine n(%)
No pain Worst Pain ever No pain Worst Pain ever0.016
18 36.73 31 36.26 25 51.10 24 48.97
The 5 level symptoms criteria were observed with the help of Likert Scale (5
=Excellent,v.good-4, good-3, fair -2,Poor =1) on Strength of stimulus towards cough, Amount
of expectorant ,consistency of the expectoration, Ease of expectoration, Bronchitis and
respiratory tract diseases with the formation of Mucus on Linkus syrup .Strength of stimulus
towards cough with irritating cough ,with bronchitis and respiratory tract diseases with
formation of mucus were found highly significant (<0.01).The symptoms score were
previously used and validated (5).Comparison of interventional group with the visits of day 1
to day 14 were mentioned in figure 50.The children in the Linkus treatment group improved
as compare to other interventional drug (<0.001).

97
Table 37. Comparison of the 5 Level Symptoms Criteria
Description Irritating cough (with or without common cold)n=29
Bronchitis (Acute or chronic)N=11
Respiratory tract disease with formation ofmucus n=09
Strength ofstimulustowardscough
5 4 3 2 1 Mean ±S.Dp-
value 5 4 3 2 1 Mean±S.D
p-value 5 4 3 2 1 Mean ±S.D
p-value
Day 10 9
10
10 0 3 ±0.810.001
0 9 1 1 0 2.18±0.4
10.001
0 7 1 1 0 2.3 ±0.710.008
Day 1419 2 4 3 1 1.6 ±1.06 9 1 0 0 1 1.09
±0.30
6 1 1 0 1 1.3 ±0.71
Amount ofexpectorant
5 4 3 2 1 Mean ±S.Dp-
value 5 4 3 2 1 Mean±S.D
p-value 5 4 3 2 1 Mean ±S.D
p-value
Day 16
17
5 1 0 2.03 ±0.730.001
0 5 4 2 0 2.7±0.7
80.002
0 4 3 4 0 3 ±0.890.001
Day 1421 5 1 0 2 1.24 ±0.51 5 2 2 0 2 1.54
±0.82
5 1 1 0 2 1.3 ±0.70
Consistencyof the
expectoration5 4 3 2 1 Mean ±S.D p-
value 5 4 3 2 1 Mean ±S.D
p-value 5 4 3 2 1 Mean ±S.D p-
value
Day 14
10
8 7 0 2.6 ±1.00.002
0 4 4 1 0 2.5±0.5
30.001
0 5 2 1 0 2.5 ±0.750.002
Day 1415 4 6 1 3 1.6 ±0.93 6 1 0 0 2 1.11
±0.33
5 1 1 0 2 1.3 ±0.70
Ease ofexpectoration
5 4 3 2 1 Mean ±S.D p-value
5 4 3 2 1 Mean ±S.D
p-value
5 4 3 2 1 Mean ±S.D p-value
Day 15
10
8 6 0 2.5 ±1.50.009
2 5 4 0 0 2.18±0.7
50.014
0 5 3 1 0 2.5 ±0.720.001
Day 1419 5 2 1 2 1.4 ±0.77 6 2 1 0 2 1.36
±0.67
6 1 0 0 2 1.1 ±0.33
Figure 50: Comparison First Visit (Day 1) versus Last day (Day 14)
5.96
6.53
5.94
3.86
3.86
3.86 2.96 2.24
2.41
3.08
4.88 3.98
2.88
3.12
3.29
1.692
2.08
2.02
0
1
2
3
4
5
6
7
Link
us
Amin
ophy
lline
,Di
phen
hydr
amin
e
Acef
yllin
Pip
eraz
ine,
Diph
enhy
dram
ine
Link
us
Amin
ophy
lline
,Di
phen
hydr
amin
e
Acef
yllin
Pip
eraz
ine,
Diph
enhy
dram
ine
Link
us
Amin
ophy
lline
,Di
phen
hydr
amin
e
Acef
yllin
Pip
eraz
ine,
Diph
enhy
dram
ine
Cough frequency Cough impact on child sleep Cough impact on parent sleep
First Visit(Day 1)
Last Visit (Day 14)

98
Children were asked about the adverse effects on day 14. Through the telephonic conversation
with the parents, day to day report collected during the study period. In the interventional
group (all 3 parallel groups), Linkus has fewer side effects as compare to other groups as
shown in table 31.
Table 38: Comparison of Side Effects all 3 Parallel Groups
Side EffectsLinkus
Aminophylline,Diphenhydramine
AcefyllinPiperazine,
Diphenhydramine(n) % (n) % (n) %
Stomachache 0 0.00 3 4.62 0 0.00
Headache 1 1.54 4 6.15 7 10.77
Drowsiness/Sleepiness 4 6.15 7 10.77 11 16.92
Rashes 1 1.54 0 0.00 1 1.54
Other 0 0.00 0 0.00 0 0.00
No side effects 59 90.77 51 78.46 46 70.77
65 100.00 65 100.00 65 100.00
4.7.An Interquartile Relationship between Polyherbal Extract Based Syrup
Linkus –A Phase IV Comparative Randomized Control Trial.
Data were stored and analyzed using SPSS version 16.0, mean and standard deviation are
reported for age, duration of illness and cough frequency per day before the treatment, count
and percentages are given for qualitative data sets like gender, severity of cough and observed
side effect of treatment. One way analysis of variance was used to compare the mean across
treatment groups and Pearson chi square test was used to see the association of qualitative
variables. Wilcoxon sign rank test was applied to see the effect of treatment outcomes at pre
and post stages, Median and inter quartile ranges also reported along with p-values. Box plot,
bar and pie chart used to display the information in graphical way, all p-values less than 0.05
were considered significant.

99
Table 39. Baseline Characteristics of Studied Sample
CharacteristicsLinkus
AcefyllinPiperazine,
Diphenhydramine
Aminophylline,Diphenhydramine p -value
Mean S.D Mean S.D Mean S.D
Age(years) 9.96 2.19 8.2 1.19 8.22 2.13<0.01*
Gender n % n % n %
Male 16 32.7 10 20.4 14 28.60.49
Female 33 67.3 39 79.6 35 71.4
Severity of cough
Minor 21 42.9 20 40.8 20 40.8
0.98Moderate 19 38.8 20 40.8 19 38.8
Severe 9 18.4 9 18.4 10 20.4
Side Effects
Stomach ache - - 3 6.1 1 2 <0.01*
Nausea - - 3 6.1 - -
Nervousness - - 1 2 - -
Insomnia - - - - - -
Hyperactivity - - - - - -
Headache 1 2 4 8.2 2 4.1
Drowsiness /sleepy - - 3 6.1 12 24.5
Disorientation - - - - - -
No side effects 48 98 35 71.4 34 69.4
*p<0.05 considered significant
( - ) o side Effect found.
Table 32 reports the baseline characteristics of studied sample, it was found that mean age and
standard deviation of child on Linkus treatment was 9.96 ± 2.19 years, a significant p-value
obtained using ANOVA that showed mean age of children across the group was not same.
On average child cough frequency before the treatment was found more than six times in
linkus and Aminophylline, Diphenhydramine and more than five times in Acefyllin
Piperazine, Diphenhydramine however there was not any significant changes observed for the
mean cough before the treatment.
More samples on the treatment were found with female gender, minor severity of cough and
without impact on child sleep; however Gender, severity of cough and impact on child sleep
did not give any association with the treatment group.
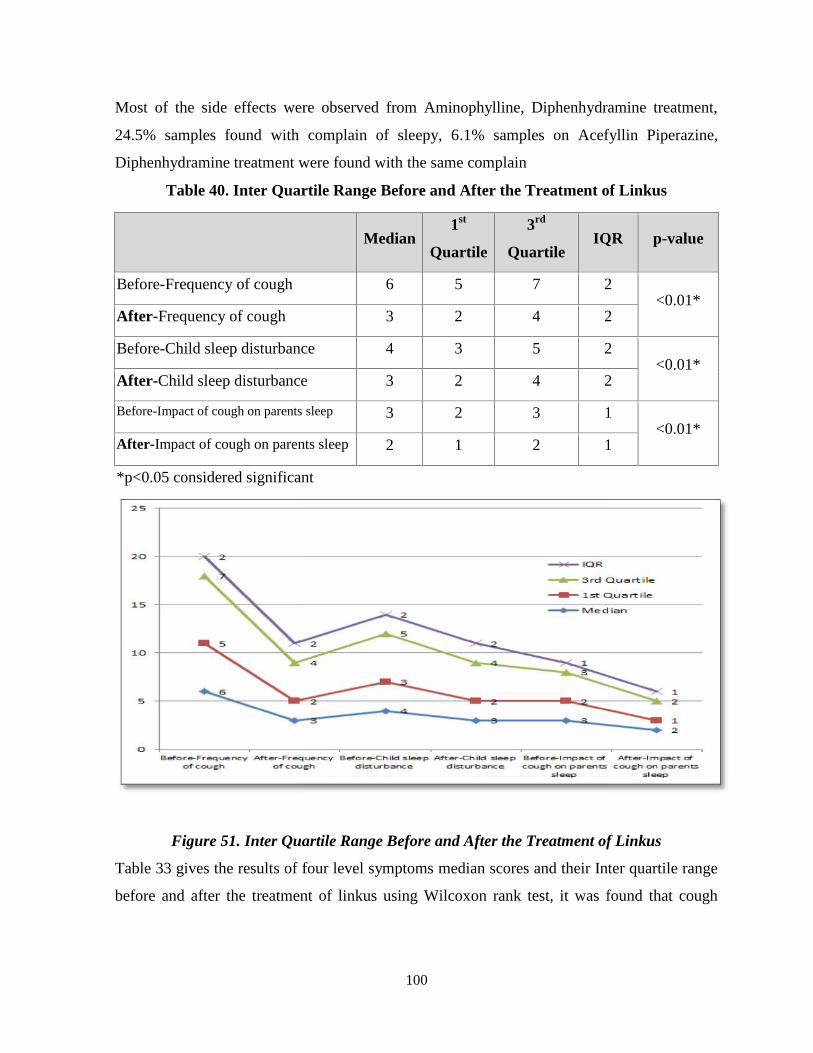
100
Most of the side effects were observed from Aminophylline, Diphenhydramine treatment,
24.5% samples found with complain of sleepy, 6.1% samples on Acefyllin Piperazine,
Diphenhydramine treatment were found with the same complain
Table 40. Inter Quartile Range Before and After the Treatment of Linkus
Median1st
Quartile
3rd
QuartileIQR p-value
Before-Frequency of cough 6 5 7 2<0.01*
After-Frequency of cough 3 2 4 2
Before-Child sleep disturbance 4 3 5 2<0.01*
After-Child sleep disturbance 3 2 4 2
Before-Impact of cough on parents sleep 3 2 3 1<0.01*
After-Impact of cough on parents sleep 2 1 2 1
*p<0.05 considered significant
Figure 51. Inter Quartile Range Before and After the Treatment of Linkus
Table 33 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of linkus using Wilcoxon rank test, it was found that cough
100
Most of the side effects were observed from Aminophylline, Diphenhydramine treatment,
24.5% samples found with complain of sleepy, 6.1% samples on Acefyllin Piperazine,
Diphenhydramine treatment were found with the same complain
Table 40. Inter Quartile Range Before and After the Treatment of Linkus
Median1st
Quartile
3rd
QuartileIQR p-value
Before-Frequency of cough 6 5 7 2<0.01*
After-Frequency of cough 3 2 4 2
Before-Child sleep disturbance 4 3 5 2<0.01*
After-Child sleep disturbance 3 2 4 2
Before-Impact of cough on parents sleep 3 2 3 1<0.01*
After-Impact of cough on parents sleep 2 1 2 1
*p<0.05 considered significant
Figure 51. Inter Quartile Range Before and After the Treatment of Linkus
Table 33 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of linkus using Wilcoxon rank test, it was found that cough
100
Most of the side effects were observed from Aminophylline, Diphenhydramine treatment,
24.5% samples found with complain of sleepy, 6.1% samples on Acefyllin Piperazine,
Diphenhydramine treatment were found with the same complain
Table 40. Inter Quartile Range Before and After the Treatment of Linkus
Median1st
Quartile
3rd
QuartileIQR p-value
Before-Frequency of cough 6 5 7 2<0.01*
After-Frequency of cough 3 2 4 2
Before-Child sleep disturbance 4 3 5 2<0.01*
After-Child sleep disturbance 3 2 4 2
Before-Impact of cough on parents sleep 3 2 3 1<0.01*
After-Impact of cough on parents sleep 2 1 2 1
*p<0.05 considered significant
Figure 51. Inter Quartile Range Before and After the Treatment of Linkus
Table 33 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of linkus using Wilcoxon rank test, it was found that cough

101
frequency significantly got down after the treatment of linkus; it also gives significant impact
on child sleep and their parents sleep.
Table 41. Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Acefyllin Piperazine,
DiphenhydramineMedian 1st Quartile 3rd Quartile
IQR p-value
Before-Frequency of cough 7 6 8 2<0.01*
After-Frequency of cough 4 3 5 2
Before-Child sleep disturbance 4 3 4 1<0.01*
After-Child sleep disturbance 3 3 4 1
Before-Impact of cough on
parents sleep3 2 3 1
<0.01*After-Impact of cough on
parents sleep2 1 3 2
*p<0.05 considered significant
Figure 52: Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Table 34 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of Acefyllin Piperazine, Diphenhydramine using Wilcoxon rank
test, it was found that cough frequency significantly got down after the treatment of Acefyllin
101
frequency significantly got down after the treatment of linkus; it also gives significant impact
on child sleep and their parents sleep.
Table 41. Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Acefyllin Piperazine,
DiphenhydramineMedian 1st Quartile 3rd Quartile
IQR p-value
Before-Frequency of cough 7 6 8 2<0.01*
After-Frequency of cough 4 3 5 2
Before-Child sleep disturbance 4 3 4 1<0.01*
After-Child sleep disturbance 3 3 4 1
Before-Impact of cough on
parents sleep3 2 3 1
<0.01*After-Impact of cough on
parents sleep2 1 3 2
*p<0.05 considered significant
Figure 52: Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Table 34 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of Acefyllin Piperazine, Diphenhydramine using Wilcoxon rank
test, it was found that cough frequency significantly got down after the treatment of Acefyllin
101
frequency significantly got down after the treatment of linkus; it also gives significant impact
on child sleep and their parents sleep.
Table 41. Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Acefyllin Piperazine,
DiphenhydramineMedian 1st Quartile 3rd Quartile
IQR p-value
Before-Frequency of cough 7 6 8 2<0.01*
After-Frequency of cough 4 3 5 2
Before-Child sleep disturbance 4 3 4 1<0.01*
After-Child sleep disturbance 3 3 4 1
Before-Impact of cough on
parents sleep3 2 3 1
<0.01*After-Impact of cough on
parents sleep2 1 3 2
*p<0.05 considered significant
Figure 52: Inter Quartile Range Before and After the Treatment of Acefyllin Piperazine
Table 34 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of Acefyllin Piperazine, Diphenhydramine using Wilcoxon rank
test, it was found that cough frequency significantly got down after the treatment of Acefyllin

102
Piperazine Diphenhydramine, it also gives significant impact on child sleep and their parents
sleep.
Table 42: Inter Quartile Range Before and After the Treatment of Aminophylline
Aminophylline,
DiphenhydramineMedian 1st Quartile 3rd Quartile IQR p-value
Before-Frequency of
cough7 4 8 4
<0.01*After-Frequency of
cough5 4 6 2
Before-Child sleep
disturbance4 3 5 2
<0.01*After-Child sleep
disturbance3 2 4 2
Before-Impact of cough
on parents sleep2 1 4 3
0.08After-Impact of cough
on parents sleep2 1 3 2
*p<0.05 considered significant
102
Piperazine Diphenhydramine, it also gives significant impact on child sleep and their parents
sleep.
Table 42: Inter Quartile Range Before and After the Treatment of Aminophylline
Aminophylline,
DiphenhydramineMedian 1st Quartile 3rd Quartile IQR p-value
Before-Frequency of
cough7 4 8 4
<0.01*After-Frequency of
cough5 4 6 2
Before-Child sleep
disturbance4 3 5 2
<0.01*After-Child sleep
disturbance3 2 4 2
Before-Impact of cough
on parents sleep2 1 4 3
0.08After-Impact of cough
on parents sleep2 1 3 2
*p<0.05 considered significant
102
Piperazine Diphenhydramine, it also gives significant impact on child sleep and their parents
sleep.
Table 42: Inter Quartile Range Before and After the Treatment of Aminophylline
Aminophylline,
DiphenhydramineMedian 1st Quartile 3rd Quartile IQR p-value
Before-Frequency of
cough7 4 8 4
<0.01*After-Frequency of
cough5 4 6 2
Before-Child sleep
disturbance4 3 5 2
<0.01*After-Child sleep
disturbance3 2 4 2
Before-Impact of cough
on parents sleep2 1 4 3
0.08After-Impact of cough
on parents sleep2 1 3 2
*p<0.05 considered significant
Figure 53: Inter Quartile Range Before and After the Treatment of Treatment ofAminophylline

103
Table 40 gives the results of four level symptoms median scores and their Inter quartile range
before and after the treatment of Aminophylline, Diphenhydramine using Wilcoxon rank test,
it was found that cough frequency significantly got down after the treatment of
Aminophylline, Diphenhydramine, it also gives significant impact on child sleep but their
parents sleep did not received the impact of treatment and it was found in significant.
4.7.1 Box Plot for different variables
Figure 54: Comparison of Toxic Effects on Lipid Profile

104
The box plots showed that distribution of cough before and after treatment were not same
however the sample size is distribution equally with no outlier found
The result of additional symptoms scores of all four treatment groups, it was found that in
linkus group see table 36 Wong backer face scale found significant difference in outcome
after the treatment, strength of stimulation SPO2, and FEV also give significant p-value.
Beats per minutes were found insignificant.
In Acefyl group only SPO2 takes the effect of treatment and results found significant see table
37, in Hydrilin treatment groups changes were observed only for FEV outcomes with
significant p-value see table 38,
Table 43: Comparison (After – before) Linkus
Comparison (After – before) Linkus N Mean Rank p-value
Wong baker face scale
Negative Ranks 25 18.50
0.02*Positive Ranks 11 18.50
Ties 13
Strength of stimulationtowards cough
Negative Ranks 0 .00
<0.01*Positive Ranks 25 13.00
Ties 4
Beats per minutes
Negative Ranks 28 23.00
0.37Positive Ranks 19 25.47
Ties 2
SPO2
Negative Ranks 9 22.94
0.02*Positive Ranks 28 17.73
Ties 12
FEV
Negative Ranks 1 6.00
<0.01*Positive Ranks 48 25.40
Ties 0
4.8.Results of SPO2, BRM with All Linkus Groups

105
Table 44 : Comparison (After – Before) Acefyllin Piperazine
Comparison (After – before) Acefyl N Mean Rank p-value
Wong baker face scale
Negative Ranks 23 20.00
0.26Positive Ranks 16 20.00
Ties 10
Strength of stimulationtowards cough
Negative Ranks 29 22.81
N.APositive Ranks 19 27.08
Ties 1
Beats per minutes
Negative Ranks 2 15.25
0.45Positive Ranks 17 9.38
Ties 30
SPO2
Negative Ranks 3 29.67
<0.01*Positive Ranks 29 15.14
Ties 17
Table 45 : Comparison (After – Before) Dextromethorphan, Diphenhydramine
Comparison (After – before) Hydrillin N Mean Rank p-value
Wong baker face scaleStrength of stimulationtowards cough
Negative Ranks 21 20.00
0.63Positive Ranks 18 20.00
Ties 10
Beats per minutes
Negative Ranks 31 25.65
N.APositive Ranks 18 23.89
Ties 0
SPO2
Negative Ranks 37 23.74
0.06Positive Ranks 5 4.90
Ties 7
FEV
Negative Ranks 21 19.31
<0.01Positive Ranks 9 6.61
Ties 19

106
Figure 55. Box Plot for different Variables
The above figure shows that no outlier found in the study. All data lie in the normal range
however the frequency of cough before the investigational drug was more.
106
Figure 55. Box Plot for different Variables
The above figure shows that no outlier found in the study. All data lie in the normal range
however the frequency of cough before the investigational drug was more.
106
Figure 55. Box Plot for different Variables
The above figure shows that no outlier found in the study. All data lie in the normal range
however the frequency of cough before the investigational drug was more.
Figure 56.The Child Sleep disturbance due to Cough Before and After the Treatment.

107
treatment. It shows that the data was in normal range with an outlier which was found in
Placebo group. However all the treatment group showed significant relationship (<0.05).
Figure 57. Pain Before and After the Treatment
Above mentioned figure shows the Pain before and after the treatment of different marketed
cough syrup, Placebo and Linkus .More pain relieved by the Linkus as compare to other
investigational product with diphenhydramine and aminophylline.
The above figure shows the child sleep disturbance due to cough before and after the
108
CHAPTER 5
DISCUSSION

109
5. CHAPTER FIVE - DISCUSSION
5.1. Discussion:
The ‘Linkus’ poly herbal extract based Syrups have exhibited good quality in appearance and
high acceptability for taste The quantity determination of vasicine and flavonoids has been
analyzed by HPTLC for the quality assurance .The study has endorsed the quality and
effectiveness of the poly herbal extract lozenges with its active indigents and specifications.
This study revealed that linkus lozenges is a suitable dosage form in symptomatic relief .The
standardization provide a specific and rapid tool to set the quality standard identity, specificity
and reproducibility in linkus lozenges.
Current trend of herbal market and the visible financial growth with evident therapeutic graph
has proven its effectiveness. Minimum side effects make the herbal and alternative medication
more attractive for the end users. This poly herbal extract based lozenges have proven the
quality by both protocols including qualitatively via organoleptic attributes and quantitatively
by HPTLC and spectrophotometry.
Cough is the troublesome symptoms for children including upper respiratory tract infections.
Every year in United States numerous cases related to ambulatory has been reported(39) .The
era of health care continuously intensify the consumer’s billion of dollar per year on over the
counter medications (OTC) for cough (6, 185). “The desire to give or take a medicine
commonly compensates the scarcity of sound research on the effect of these drugs or the
conditions that require them but unfortunately, there are no clearly proven therapeutic
alternatives. The current lack of clarity regarding symptomatic care in children with cough as
a result of URIs has created an environment in which many pediatricians prescribe (186)
many Internet sites recommend and many parents administer cough suppressants or
antihistamines to relieve these symptoms (187)”.
The rural and urban tribes has become an imperative resources in health care division with
respective to traditional and herbal medicine (155) .Herbal formulation have extensive
acceptability for the symptoms of cough and common cold. “Common cold is the most
prevalent illness known to mankind. It has been reported that about 25% of population

110
experiences 4-5 episodes of infections every year, 50% suffers 2-3 attacks and the remaining
25% suffers 0-1 infections per year (188). Herbal medicines are the mixture of one or more
phytochemical constituents with single or multiple plants or species (189). Correct
identification of biomarkers is the elemental specialty for the reproducibility in herbal
medicine (190). Standardization is the technique for gauging the quality of poly herbal
formulation with different and unique techniques. By using the technique standardization, the
active phytochemical constituents can be quantifying precisely. For enumerating the
technique of standardization preliminary phytochemical screening, chemo-profiling and
biomarkers analyzed by using state-of-the-art techniques. Chromatographic techniques has
been used for standardize the phytochemical constituents present in the Linkus Kids syrup and
widely used for quantify the variety of herbal marketed drugs (191).
This experimental model of study focused on Linkus Kids Syrup, a polyherbal formulation
with excellent blends of multiple biomarkers. Piperine and Glycyrrhizin were the focused
biomarkers identified by HPLC and HPTLC method with standard specifications. It is the
combinations of herbs includes Adhatoda vasica – Bansa, Glycyrrhiza Glabra - Mulethi
Crude, Piper longum - Filfil Daraz, Cordia latifolia – Sapistan, Althea officinalis – Khatmi,
Zizyphus vulgaris – Unnab and Viola odorata – Banafshan. Published research studies have
shown that used herbs are effectively reducing the cough and related symptoms including
upper respiratory tract symptoms.
Piperine and Glycyrrhizin are the biomarkers present in Piper longum and Glycyrrhiza glabra.
HPLC and HPTLC were the techniques which were used to quantify with the help of
chromatogram on 345 and 254 nm. The retention time of piperine for 100% recovery was 1-
8.093 in HPLC method. However in HPTLC method the Rf value of glycyrrhizin was 0.10-
0.20. From centuries; Liquor ice (Glycyrrhiza glabra) is used as a home remedial measure for
treating hoarseness of voice and bad throat as a demulcent. It is also used in throat infections
(192). It is a mild laxative, which soothes and tones the mucous membranes and relieves
muscle spasms. It is rich in flavonoids and an antioxidant, cancer protecting, botanical
boosting and an anti-mutagen, preventing damage to genetic material that can eventually
result in cancer (193, 194) Piper longum L. fruits and roots are attributed with numerous

111
medicinal uses, and may be used for diseases of respiratory tract, viz. cough, bronchitis,
asthma etc.; as counter-irritant and analgesic when applied locally for muscular pains and
inflammation; as snuff in coma and drowsiness and internally as carminative (195). Long
pepper (Piper longum), which is claimed to be of great value in any respiratory trouble in age
old text books of Ayurveda has also proved its worth as a bronchodilator, muco-lytic,
expectorant and, of late, as a bioavailability enhancer for therapeutically active drug
molecules (196).Both of the biomarkers were systematically isolated and optimize with the
used of solvents phases”.
Researches have proved that chromatographic methods are the reliable and convenient
method for quantification (197) Simplicity, selectivity and accuracy is the key elements of
HPLC & HPTLC in herbal formulation (198). An accurate HPLC & HPTLC method for
estimation of biomarkers in Linkus Kids syrup has been established with good peak shapes
including reproducibility, transparency with individuality.
In this study antioxidant, reducing, lipoxygenase and ACE inhibition activity of polyherbal
drug Linkus were evaluated. The results obtained concerning antioxidant, lipoxygenase and
enzyme inhibition that all the test were found effective. Linkus plants definition showed great
cancer prevention agent movement by successfully decreasing diminishing Fe3+/ferricyanide
complex, rummaging of different free radicals, for example, DPPH• and H2O2 radicals.
Besides, these concentrates were likewise found to have the ACE restraint movement and
lipoxygenase action In-Vitro. Subsequently, it might be reasoned that the counter oxidant and
ACE restraint movement and lipoxygenase inhibitory activity of Poly home grown
concentrates would be utilized for the future remedial hack and related manifestations because
of nearness of potential bioactive mixes.
Alternative and herbal medications are widely used all over the world. Herbs all over the
world including Adhatoda vasica, Onosma bracteatum, Piper longum, Cordia latifolia, Alpinia
galangal, Hyssopus officinalis and Glycyrrhiza glabra (117, 150, 183) all are works against
microbial activity specifically Staphylococcus aureus, Streptococcus pyogens, Salmonella spp
and P. aeruginosa. The composition of Linkus syrup based on above mentioned herbs with
active constituents contains vasicinone, vasicine and glycyrrhizin which helps against cough,
112
common cold and URI (upper respiratory tract infections) and serve as an expectorant
(158).Piper longum actively contains piperlonguminine ,piperine and piperlongumine helps
for cough and other URI (199). Hyssopus officinalis, Alpinia galangal, Zingiber officinale,
Cordia latifolia are used to control coughing and respiratory tract infections (194, 200-
202).Cough is very frequent symptoms in all age groups and has been missed used all over in
the world .The specifications and authenticity should be address. The poly herbal linkus syrup
has proved its potential on anti-microbial activity against Staphylococcus Aureus,
Streptococcus pyogenes, Salmonella spp and Pseudomonas aeruginosa.
The poly-herbal Linkus syrup exhibit excellent properties against pathogenic microbes
therefore these herbs base (Linkus) able to be used as antimicrobial agent for treatment of
various infectious diseases of gastrointestinal tract. Furthermore additives that are present in
these formulations and the relevance of heat in the extraction method did not influence the
antimicrobial activity.
The Linkus lozenges containing Adhatoda vasica, Glycyrrhiza glabra, Piper longum, Viola
odorata, Hyssopus officinalis, Alpinia galangal, were studied for their acute and chronic
toxicity in Albino rats. In all animals, the drug was administered orally at the dose of 4
gms/kg. The animals were kept under observation for 48 hrs. For chronic toxicity testing body
weight was counted for 2 months with given dose of 4gms/kg. After treatment there were no
abnormalities observed in behavior of the animals. There was no statistical significant change
in body weights of the animals. The functions of central nervous system, cardiovascular
system, respiratory system, gastrointestinal system and excretory system were all normal. No
abnormalities in the behavior of the animals were seen. Different biochemical parameters
estimated in rats belonging to test group were complete to respective biochemical parameters
in control group of rats. No mortality was seen. Average values of different biochemical
parameters in test group were comparable to the average values of respective biochemical
parameters in control group of animals. The Linkus lozenges are safe when given orally at the
Dose of 4 gms/kg, which is 20 times the normal therapeutic dose.
The efficacy of linkus lozenges was established by inducing cough with citric acid 1g/kg. On
100mg/kg extract the cough reflexes were 167 as shown in table 1. With citric acid induction

113
with the remedy of Diphenhydramine and Acefyllin Piperazine found to be 229 as shown in
table 2. Male albino wristlet rat on 150µg/kg with Dextromethorphan and Diphenhydramine
were found to be 227 and linkus were 167 as shown in table 4. The Linkus extract were more
efficacious as compared to the other formulation as mentioned in table 1-4.
There is an expanding utilization of natural or customary prescription everywhere throughout
the developing nations because of their prevalence and security on long haul use (203-205).
Despite the fact that home grown drugs are being utilized for a considerable length of time, in
today’s world, there are security issues that these meds could conceivably deliver impact on
liver, mind or kidneys and subsequently cause irregularity (206, 207). There are different
home grown solutions accessible, however not very many have been taken for clinical and
preclinical trial studies to affirm their security and adequacy (208). The behavioral analysis
has proven the safety however toxicity testing the body weights of essential organ for acute
toxicity on linkus extract versus control were found significant safe as shown in table 5 and
the biochemical parameters and hematological parameters were also significantly safe as
shown in table 6 and 7 and alkaline phosphate value was <0.01.While the chronic toxicity
was significantly safe as compared to linkus versus control i.e. 243±0.96,227±0.36 as shown
in table 08.The average organ weight including spleen and skeletal muscles were found to be
significant <0.05 as shown in table 09.The toxic effect as compare to control considered to be
safest as shown in table 10 While the biochemical and hematological parameter has proven
the chronic toxicity considered to be the safest and no mortality and physical unevenness
shown .
The Linkus syrup, a poly herbal combination was studied for its acute toxicity in Albino rats.
The drug was administered orally at the dose of 4 gms/kg. After treatment there were no
abnormalities observed in behavior of the animals. Also no changes in functions of respiratory
system, cardiovascular system, central nervous system, gastrointestinal system and excretory
system were seen. Average values of different biochemical parameters in the test group were
comparable to average values of respective biochemical parameters in control group of
animals. The Linkus lozenges are safe when given orally at the Dose of 4 gms/kg, which is 20
times the normal therapeutic dose
114
Herbal and allopathic products as an OTC medication have widely distributed .This
investigation sought that the herbal treatment Linkus were more superior as compare to the
other investigational market drug (A & B).The sleep quality of children and parents were
relatively high in poly herbal Linkus cough syrup and the disturbance due to cough has
reduced. Disappointment was with Group A & B which were used extensively throughout the
globe.
Published research on asthma, chronic cough or cystic fibrosis [267, 268] but its first on its
kind of research on school going children in Pakistan .In addition children’s quality of sleep
in every interventional group were evaluated. However, the limitation of the study is the co-
operation and understanding of the parents/guardians. Phone calls and patient’s home visit
was the only tool to minimize loss to follow up.
Cough is the most frustrating symptoms and lead absentees affects due to sleep disturbance of
parents and children. The diphenhydramine was used in both allopathic medication causes
restlessness, insomnia, acute dystonia, increased risk of severe injury and nervousness with in
therapeutic doses (209, 210).
The Pharmacovigilance report of linkus cough syrup will be the call for physicians and
researchers. OTC products should be addressed in market with the keen observatory hands.
Pharmacist’s presence on retail Pharmacy should be more noticeable.
The current study intended to look the interquartile relationship between Linkus and other
marketed allopathic brands for acute cough and its impact on child and parents sleep. The
results of the study showed that the medication on different interquartile ranges have
significant reduction on cough and its impact on sleep .However on Linkus therapy the side
effects were less as compare to other allopathic medication include Acefyllin Piperazine and
Aminophylline Diphenhydramine.
Herbal medicine data base explains that the consumption of traditional medicine reached in
2.1 to 2.3 billion (211).Conversely the knowledge about side effects of pharmacological
medications has been increased which convert a consumer more towards traditional and
herbal medicine (212). The biggest challenges of alternate and comprehensive medicine are
to convert into complete sciences. This study aimed to prove the effects of herbal medicine

115
interquartile ranges and its impact on cough with the comparison of other successful marketed
multinational pharmaceutical brands. Significant relationship found on all treatment groups on
indication of cough and other associated problems. Linkus syrup have possess the therapeutic
value for the treatment of Cough and its related problems with other standard conventional
therapies .The side effects as compare to the conventional therapy found less .
Findings of the current therapy demonstrate that that the herbal syrup Linkus possesses
therapeutic ranges on cough on different interquartile ranges as compare to other market best
sale conventional pharmaceutical medication .Linkus will be the best herbal medication with
no side effects on children under 2 to 11 years of age. Safety and efficacy of the targeted
syrup has been proven previously and maintaining the practitioner confidence on traditional
herbal medicines.
5.2. Conclusion and Future Prospects
Current trend of herbal market and the visible financial growth with evident therapeutic graph
have confirmed and prove the effectiveness of Linkus. Minimum side effects make the herbal
and alternative medication and more attractive for the end users.
o The manufacturing process of Linkus was found to be reproducible and complying
with the standard specification and validation.
o The poly herbal Linkus Syrup and Lozenges Quantitative and Qualitative estimation
have proven the quality by both protocols via organoleptic attributes and HPTLC and
spectrophotometry. The biomarkers Vasicine, Piperine and Glycyrrhizin have been
standardized and quantify with HPTLC for Linkus Kids Syrup.
o In vitro Linkus dosage form has a good anti-oxidant and reducing ability. Linkus has
displayed moderate activity of urease, lipoxygenase and ACE inhibition as compared
to standards. These biological activities of polyherbal formulation Linkus might be
helpful for reducing the cough and related symptoms.
o Linkus cough syrup shows strong sensitivity against Staphylococcus aureus,
Streptococcus pyogenes and Salmonella spp in both disc and well diffusion method
and showed resistivity against Pseudomonas aeruginosa. However with the
comparison of amoxicillin and ampicillin, linkus showed more sensitivity against

116
Salmonella spp and Streptococcus pyogenes. The poly herbal blend of Linkus syrup
can be used as an anti-microbial agent on cough and associated symptoms related to
upper respiratory tract infections.
o Another study was established on efficacy and toxicity of poly herbal Linkus lozenges
in experimental animal. After treatment there were no abnormalities observed in
behavior also no changes in elements of respiratory framework, cardiovascular
framework, focal sensory system, gastrointestinal framework and excretory
framework were seen. Average values of different biochemical parameters in test
groups were comparable to average values of respective biochemical parameters in
control group of animals. No mortality and no abnormality were seen in linkus
lozenges and suggested it to be the safest choice.
o Polyherbal syrup Linkus shows better results in treatment of cough including side
effects as compare to the other parallel groups B and C (Aminophylline with
Diphenhydramine and Acefyllin Piperazine with Diphenhydramine). For nocturnal
sleep Linkus providing better results in cough and associated problems. Pain were
significantly reduce on day 14 with the herbal Linkus syrup group A (<0.001). Group
B and C found less effective with more side effects as compared to Linkus syrup .The
interquartile ranges of Linkus before and after the treatment was significant down.
Poly herbal Linkus syrup could substantially improve the clinical effect and relieves
coughs and benefit lung functions and better sleep facilitation.

117
REFRENCES
1. Shields MD, Bush A, Everard ML, McKenzie S, Primhak R. Recommendations for
the assessment and management of cough in children. Thorax. 2008;63(Suppl 3):iii1-
iii15.
2. Goldsobel AB, Chipps BE. Cough in the pediatric population. The Journal of
pediatrics. 2010;156(3):352-8. e1.
3. Vernacchio L, Kelly JP, Kaufman DW, Mitchell AA. Pseudoephedrine use among US
children, 1999–2006: results from the Slone Survey. Pediatrics. 2008;122(6):1299-
304.
4. Goldman RD. Codeine for acute cough in children. Canadian Family Physician.
2010;56(12):1293-4.
5. Rosendahl I. Expense of physician care spurs OTC, self-care market. Drug Topics.
1988;132(15):62-3.
6. Morice AH, Menon MS, Mulrennan SA, Everett CF, Wright C, Jackson J, et al.
Opiate therapy in chronic cough. American journal of respiratory and critical care
medicine. 2007;175(4):312-5.
7. Fahey T, Stocks N, Thomas T. Quantitative systematic review of randomised
controlled trials comparing antibiotic with placebo for acute cough in adults. Bmj.
1998;316(7135):906-10.
8. Bridges-Webb C, Britt H, Miles D, Neary S, Charles J, Traynor V. Morbidity and
treatment in general practice in Australia. Australian family physician.
1993;22(3):336-9, 42-6.
9. Irwin RS, Madison JM. The diagnosis and treatment of cough. New England Journal
of Medicine. 2000;343(23):1715-21.
10. Mello CJ, Irwin RS, Curley FJ. Predictive values of the character, timing, and
complications of chronic cough in diagnosing its cause. Archives of Internal Medicine.
1996;156(9):997-1003.
11. Craven V, Everard ML. Protracted bacterial bronchitis: reinventing an old disease.
Archives of disease in childhood. 2013;98(1):72-6.

118
12. Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics: ACCP
evidence-based clinical practice guidelines. Chest Journal. 2006;129(1_suppl):260S-
83S.
13. Hay AD, Wilson A, Fahey T, Peters TJ. The duration of acute cough in pre-school
children presenting to primary care: a prospective cohort study. Family Practice.
2003;20(6):696-705.
14. Butler CC, Hood K, Kinnersley P, Robling M, Prout H, Houston H. Predicting the
clinical course of suspected acute viral upper respiratory tract infection in children.
Family practice. 2005;22(1):92-5.
15. Karakoç F, Karadağ B, Akbenlioğlu C, Ersu R, Yıldızeli B, Yüksel M, et al. Foreign
body aspiration: what is the outcome? Pediatric pulmonology. 2002;34(1):30-6.
16. Piirila P, Sovijarvi A. Objective assessment of cough. European Respiratory Journal.
1995;8(11):1949-56.
17. Hashimoto Y, Murata A, Mikami M, Nakamura S, Yamanaka E, Kudoh S. Influence
of the rheological properties of airway mucus on cough sound generation.
Respirology. 2003;8(1):45-51.
18. Korpáš J, Widdicombe J, Vrabec M. Influence of simulated mucus on cough sounds in
cats. Respiratory medicine. 1993;87(1):49-54.
19. Chang AB, Robertson CF, van Asperen PP, Glasgow NJ, Masters IB, Teoh L, et al. A
cough algorithm for chronic cough in children: a multicenter, randomized controlled
study. Pediatrics. 2013;131(5):e1576-e83.
20. Fogari R, Zoppi A, Tettamanti F, Malamani G, Tinelli C, Salvetti A. Effects of
nifedipine and indomethacin on cough induced by angiotensin-converting enzyme
inhibitors: a double-blind, randomized, cross-over study. J Cardiovasc Pharmacol.
1992;19(5):670-3.
21. McEwan JR, Choudry NB, Fuller RW. The effect of sulindac on the abnormal cough
reflex associated with dry cough. Journal of Pharmacology and Experimental
Therapeutics. 1990;255(1):161-4.
22. Malini PL, Strocchi E, Zanardi M, Milani M, Ambrosioni E. Thromboxane
antagonism and cough induced by angiotensin-converting-enzyme inhibitor. The
Lancet. 1997;350(9070):15-8.

119
23. Hargreaves M, Benson M. Inhaled sodium cromoglycate in angiotensin-converting
enzyme inhibitor cough. The Lancet. 1995;345(8941):13-6.
24. Poe RH, Harder RV, Israel RH, Kallay MC. Chronic persistent cough. Experience in
diagnosis and outcome using an anatomic diagnostic protocol. CHEST Journal.
1989;95(4):723-8.
25. Morice A. The diagnosis and management of chronic cough. European Respiratory
Journal. 2004;24(3):481-92.
26. Gilberg S, Njamkepo E, Du Châtelet IP, Partouche H, Gueirard P, Ghasarossian C, et
al. Evidence of Bordetella pertussis infection in adults presenting with persistent
cough in a French area with very high whole-cell vaccine coverage. Journal of
Infectious Diseases. 2002;186(3):415-8.
27. Asilsoy S, Bayram E, Agin H, Apa H, Can D, Gulle S, et al. Evaluation of chronic
cough in children. CHEST Journal. 2008;134(6):1122-8.
28. Irwin RS. Introduction to the diagnosis and management of cough: ACCP evidence-
based clinical practice guidelines. CHEST Journal. 2006;129(1_suppl):25S-7S.
29. Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice
guidelines. CHEST Journal. 2006;129(1_suppl):72S-4S.
30. Curley FJ, Irwin RS, Pratter MR, Stivers DH. Cough and the Common Cold1-3. Am
Rev Respir Dis. 1988;138:305-11.
31. Prasad AS, Fitzgerald JT, Bao B, Beck FW, Chandrasekar PH. Duration of symptoms
and plasma cytokine levels in patients with the common cold treated with zinc acetate:
a randomized, double-blind, placebo-controlled trial. Annals of Internal Medicine.
2000;133(4):245-52.
32. Higenbottam T. Cough induced by changes of ionic composition of airway surface
liquid. Bulletin europeen de physiopathologie respiratoire. 1983;20(6):553-62.
33. Barbee RA, Halonen M, Kaltenborn WT, Burrows B. A longitudinal study of
respiratory symptoms in a community population sample. Correlations with smoking,
allergen skin-test reactivity, and serum IgE. CHEST Journal. 1991;99(1):20-6.
34. Gilchrist VJ, Stange KC, Flocke SA, McCord G, Bourguet C. A comparison of the
National Ambulatory Medical Care Survey (NAMCS) measurement approach with
direct observation of outpatient visits. Medical care. 2004;42(3):276-80.

120
35. Irwin RS, Curley FJ. The treatment of cough. A comprehensive review. CHEST
Journal. 1991;99(6):1477-84.
36. French CL, Irwin RS, Curley FJ, Krikorian CJ. Impact of chronic cough on quality of
life. Archives of Internal Medicine. 1998;158(15):1657-61.
37. Irwin RS, Boulet L-P, Cloutier MM, Fuller R, Gold PM, Hoffstein V, et al. Managing
cough as a defense mechanism and as a symptom: a consensus panel report of the
American College of Chest Physicians. CHEST Journal.
1998;114(2_Supplement):133S-81S.
38. Gwaltney Jr JM, Phillips CD, Miller RD, Riker DK. Computed tomographic study of
the common cold. New England Journal of Medicine. 1994;330(1):25-30.
39. Puhakka T, Lavonius M, Varpula M, Svedström E, Terho E, Ruuskanen O. Pulmonary
imaging and function in the common cold. Scandinavian journal of infectious diseases.
2001;33(3):211-4.
40. Hing E, Cherry DK, Woodwell DA. National Ambulatory Medical Care Survey: 2004
summary. Advance data. 2006(374):1-33.
41. Aylward M, Maddock J, Davies D, Protheroe D, Leideman T. Dextromethorphan and
codeine: comparison of plasma kinetics and antitussive effects. European journal of
respiratory diseases. 1984;65(4):283-91.
42. Azizullah A, Khattak MNK, Richter P, Häder D-P. Water pollution in Pakistan and its
impact on public health—a review. Environment International. 2011;37(2):479-97.
43. Nasreen N, Jalaluddin M. Indoor fungal allergens. International Journal of Biology
and Biotechology. 2005;2:707-10.
44. Rao TA, Siddiqui BA, Shaikh MA, Ahmed M, Shaikh AH, Ahmed F. Dynamics of
some common epidemics in Karachi, Pakistan. JPMA-Journal of the Pakistan Medical
Association. 2011;61(11):1072.
45. Rao NA, Mahfooz Z, Irfan M. Online Submission. Dynamics. 2011.
46. Mustafa G, Khan PA, Iqbal I. Nocturnal asthma in school children of south Punjab
Pakistan. J Ayub Med Coll Abbottabad. 2008;20(3):36-9.
47. Shaikh S, Nafees AA, Khetpal V, Jamali AA, Arain AM, Yousuf A. Respiratory
symptoms and illnesses among brick kiln workers: a cross sectional study from rural
districts of Pakistan. BMC Public Health. 2012;12(1):1.

121
48. Nafees AA, Fatmi Z, Kadir MM, Sathiakumar N. Pattern and predictors for respiratory
illnesses and symptoms and lung function among textile workers in Karachi, Pakistan.
Occupational and environmental medicine. 2013;70(2):99-107.
49. Akhtar S, White F, Hasan R, Rozi S, Younus M, Ahmed F, et al. Hyperendemic
pulmonary tuberculosis in peri-urban areas of Karachi, Pakistan. BMC Public Health.
2007;7(1):1.
50. Gulsvik A, Refvem O. A scoring system on respiratory symptoms. European
Respiratory Journal. 1988;1(5):428-32.
51. Ellul-Micallef R. Effect of terbutaline sulphate in chronic" allergic" cough. Br Med J
(Clin Res Ed). 1983;287(6397):940-3.
52. Bickerman Ha, Barach Al, Drimmer F. The Experimental Production Of Cough In
Human Subjects Induced By Citric Acid Aerosols. Preliminary Studies On The
Evaluation Of Antitussive Agents*. The American journal of the medical sciences.
1954;228(2):156-63.
53. Morris D, Shane S. Human bioassay of a new antitussive agent. Canadian Medical
Association journal. 1960;83(21):1093.
54. Prime F. The assessment of antitussive drugs in man. British medical journal.
1961;1(5233):1149.
55. Calesnick B, Christensen JA, Munch JC. ANTITUSSIVE ACTION OF L-
PROPOXYPHENE IN CITRIC ACID-INDUCED COUGH RESPONSE. The
American Journal of the Medical Sciences. 1961;242(5):560-4.
56. Chernish S, Lewis G, Kraft B, HOWELL H. Clinical evaluation of a new antitussive
preparation. Annals of allergy. 1963;21:677.
57. Eccles R, Morris S, Jawad M. Lack of effect of codeine in the treatment of cough
associated with acute upper respiratory tract infection. Journal of clinical pharmacy
and therapeutics. 1992;17(3):175-80.
58. Fuller P, Picciotto A, Davies M, McKenzie S. Cough and sleep in inner-city children.
European Respiratory Journal. 1998;12(2):426-31.
59. Khoshoo V, Edell D, Mohnot S, Haydel R, Saturno E, Kobernick A. Associated
factors in children with chronic cough. CHEST Journal. 2009;136(3):811-5.

122
60. Schmidt BM, Ribnicky DM, Lipsky PE, Raskin I. Revisiting the ancient concept of
botanical therapeutics. Nature Chemical Biology. 2007;3(7):360-6.
61. Guitart D, Pickering C, Byrne J. Past results and future directions in urban community
gardens research. Urban Forestry & Urban Greening. 2012;11(4):364-73.
62. Ekor M. The growing use of herbal medicines: issues relating to adverse reactions and
challenges in monitoring safety. Front Pharmacol. 2013;4:177.
63. Fetrow CW, Avila JR. The complete guide to herbal medicines: Simon and Schuster;
2000.
64. Shaw D. Risks or remedies? Safety aspects of herbal remedies in the UK. Journal of
the Royal Society of Medicine. 1998;91(6):294.
65. Schultz V, Hänsel R, Tyler VE. Rational phytotherapy: a physician's guide to herbal
medicine: Psychology Press; 2001.
66. Li L. Opportunity and challenge of traditional Chinese medicine in face of the
entrance to World Trade Organization. Chin Inform Trad Chin Med. 2000;7:7-8.
67. Saito H. Regulation of herbal medicines in Japan. Pharmacological Research.
2000;41(5):515-9.
68. Orisatoki R, Oguntibeju O. The role of Herbal Medicine use in HIV/AIDS treatment.
Archives of Clinical Microbiology. 2010;1(3).
69. Tyler VE. Herbal medicine: from the past to the future. Public health nutrition.
2000;3(4a):447-52.
70. Allison DB, Fontaine KR, Heshka S, Mentore JL, Heymsfield SB. Alternative
treatments for weight loss: a critical review. Critical reviews in food science and
nutrition. 2001;41(1):1-28.
71. Warburton DE, Katzmarzyk PT, Rhodes RE, Shephard RJ. Evidence-informed
physical activity guidelines for Canadian adults This article is part of a supplement
entitled Advancing physical activity measurement and guidelines in Canada: a
scientific review and evidence-based foundation for the future of Canadian physical
activity guidelines co-published by Applied Physiology, Nutrition, and Metabolism
and the Canadian Journal of Public Health. It may be cited as Appl. Physiol. Nutr.
Metab. 32 (Suppl. 2E) or as Can. J. Public Health 98 (Suppl. 2). Applied physiology,
nutrition, and metabolism. 2007;32(S2E):S16-S68.

123
72. Organization WH. Research guidelines for evaluating the safety and efficacy of herbal
medicines: Manila: WHO Regional Office for the Western Pacific; 1993.
73. Annex II W. Guidelines for the Assessment of Herbal Medicines (WHO Technicaln
Report Series No. 863). Geneva; 1996.
74. Humans IWGotEoCRt, Organization WH, Cancer IAfRo. Some traditional herbal
medicines, some mycotoxins, naphthalene and styrene: World Health Organization;
2002.
75. Castot A, Djezzar S, Deleau N, Guillot B, Efthymiou M. [Pharmacovigilance off the
beaten track: herbal surveillance or pharmacovigilance of medicinal plants]. Therapie.
1996;52(2):97-103.
76. Keller K. Legal requirements for the use of phytopharmaceutical drugs in the Federal
Republic of Germany. Journal of Ethnopharmacology. 1991;32(1-3):225-9.
77. Hussain S, Malik F, Riaz H, Qayyum MA, Khalid N. Alternative and Traditional
Medicines Systems in Pakistan: History, Regulation, Trends, Usefulness, Challenges,
Prospects and Limitations: INTECH Open Access Publisher; 2012.
78. Gangwar AK, Ghosh AK. Medicinal uses and pharmacological activity of Adhatoda
vasica. Int J Herbal. 2014;2:88-91.
79. Gangwar AK, Ghosh AK. Medicinal uses and Pharmacological activity of Adhatoda
vasica. International Journal of herbal medicine. 2014;2(1):88-91.
80. Kumar KS, Bhowmik D, Tiwari P, Kharel R. Indian traditional herbs Adhatoda vasica
and its medicinal application. Journal of Chemical and Pharmaceutical Research.
2010;2(1):240-5.
81. Pandita K, Bhatia M, Thappa R, Agarwal S, Dhar K, Atal C. Seasonal variation of
alkaloids of Adhatoda vasica and detection of glycosides and N-Oxides of vasicine
and vasicinone. Planta medica. 1983;48(2):81-2.
82. Shrivastava N, Srivastava A, Banerjee A, Nivsarkar M. Anti-ulcer activity of
Adhatoda vasica Nees. Journal of herbal pharmacotherapy. 2006;6(2):43-9.
83. Maikhuri R, Gangwar A. Ethnobiological notes on the Khasi and Garo tribes of
Meghalaya, Northeast India. Economic botany. 1993;47(4):345-57.
84. Dhar K, Jain M, Koul S, Atal C. Vasicol, a new alkaloid from Adhatoda vasica.
Phytochemistry. 1981;20(2):319-21.
124
85. Shanmugasundaram P, Maheswari R, Vijayaanandhi M. Quantitative estimation of
Piperine in herbal cough syrup by HPTLC method. Rasayan J Chem. 2008;1(02):212-
7.
86. Majeed M, Badmaev V, Rajendran R. Use of piperine as a bioavailability enhancer.
Google Patents; 1999.
87. Khushbu C, Roshni S, Anar P, Carol M, Mayuree P. Phytochemical and therapeutic
potential of Piper longum Linn a review. IJRAP. 2011;2(1):157-61.
88. Mehra P, Puri H. Pharmacognostic studies on Piplamul. XXII. Indian J Pharm.
1970;32:184.
89. Kapoor L. Handbook of Ayurvedic medicinal plants: Herbal reference library: CRC
press; 2000.
90. Chatterjee A, Dutta C. Alkaloids of Piper longum Linn—I: Structure and synthesis of
piperlongumine and piperlonguminine. Tetrahedron. 1967;23(4):1769-81.
91. Chatterjee A, Dutta C. The structure of Piper longumine, a new alkaloid isolated from
the roots of Piper longum Linn.(Piperceae). Sci Cult. 1963;29:568.
92. Singh O, Ali M, Akhtar N. Phenolic acid glucosides from the seeds of Entada
phaseoloides Merill. Journal of Asian natural products research. 2011;13(8):682-7.
93. Ammosov A, Litvinenko V. Triterpenoids of Plants of Glycyrrhiza L. and
Meristotropis Fisch. et Mey Genuses (A Review). Pharmaceutical Chemistry Journal.
2003;37(2):83-94.
94. Saxena S. Glycyrrhiza glabra: Medicine over the millennium. Nat Prod Rad.
2005;4(5):358-67.
95. Amaral AJ, Ferretti L, Megens H-J, Crooijmans RP, Nie H, Ramos-Onsins SE, et al.
Genome-wide footprints of pig domestication and selection revealed through massive
parallel sequencing of pooled DNA. PloS one. 2011;6(4):e14782.
96. Sharma V, Agrawal R. Glycyrrhiza glabra: A plant for the future. Mint J Pharm Med
Sci. 2013;2(3):15-20.
97. Duke J. Handbook of Legumes of World Economic ImportancePlenum Press. New
York. 1981:345.
98. Bergquist RR, Nubel DS, Thompson DL. Production method for high-oil corn grain.
Google Patents; 1998.

125
99. Bradley PR. British herbal compendium. Volume 1. A handbook of scientific
information on widely used plant drugs. Companion to Volume 1 of the British Herbal
Pharmacopoeia: British Herbal Medicine Association; 1992.
100. Do Monte FcHM, dos Santos JG, Russi M, Lanziotti VMNB, Leal LKAM, de
Andrade Cunha GM. Antinociceptive and anti-inflammatory properties of the
hydroalcoholic extract of stems from Equisetum arvense L. in mice. Pharmacological
research. 2004;49(3):239-43.
101. Obolentseva G, Litvinenko V, Ammosov A, Popova T, Sampiev A. Pharmacological
and therapeutic properties of licorice preparations (a review). Pharmaceutical
Chemistry Journal. 1999;33(8):427-34.
102. Yamamura Y, Kawakami J, Santa T, Kotaki H, Uchino K, Sawada Y, et al.
Pharmacokinetic profile of glycyrrhizin in healthy volunteers by a new
high‐performance liquid chromatographic method. Journal of pharmaceutical
sciences. 1992;81(10):1042-6.
103. Sinha SC. Medicinal plants of Manipur. 1996.
104. Kr BR, Sk S, Murugan M. ANTIMICROBIAL ACTIVITY AND
PHYTOCHEMICAL STUDY OF MEDICINAL PLANT ALPINIA GALANGA.
Asian Journal of Pharmaceutical and Clinical Research. 2016:364-6.
105. Saraswathy A, Meena A, Shakila R, Kumar KS, Ariyanathan S. Pharmacognostic
studies on Alangium salvifolium (Linn. f.) Wang. root bark. Pharmacognosy Journal.
2010;2(11):374-80.
106. Akhtar AH, Ahmad KU. Anti-ulcerogenic evaluation of the methanolic extracts of
some indigenous medicinal plants of Pakistan in aspirin-ulcerated rats. Journal of
ethnopharmacology. 1995;46(1):1-6.
107. Hamedi S. The Scientific Name of Zoufa, a Traditional Persian Medicinal Plant: Is it
Hyssopus officinalis L. or Nepeta bracteata Benth.? Traditional and Integrative
Medicine. 2016;1(2):79-81.
108. Kahkeshani N, Farahanikia B, Mahdaviani P, Abdolghaffari A, Hassanzadeh G,
Abdollahi M, et al. Antioxidant and burn healing potential of Galium odoratum
extracts. Res Pharm Sci. 2013;8(3):197-203.

126
109. Naghibi F, Mosaddegh M, Mohammadi Motamed M, Ghorbani A. Labiatae family in
folk medicine in Iran: from ethnobotany to pharmacology. Iranian Journal of
Pharmaceutical Research. 2010:63-79.
110. Blumenthal M. Therapeutic guide to herbal medicines. 1998.
111. Ahmad MA, Ansari S, Aslam M, Bhat JU, Khanam R, Nizami Q, et al. Anti-seizure
activity of flower extracts of Nepeta bractaeta in Swiss albino mice. 2012.
112. Ody P. The complete medicinal herbal. London: Dorling Kindersley 192p ISBN
156458187X En. 1993;120.
113. Hornok L. Cultivation and processing of medicinal plants: John Wiley & Sons Ltd.;
1992.
114. Garg S, Naqvi A, Singh A, Ram G, Kumar S. Composition of essential oil from an
annual crop of Hyssopus officinalis grown in Indian plains. Flavour and fragrance
journal. 1999;14(3):170-2.
115. Dinda KA, Craker LE. Growers guide to medicinal plants: HSMP Press; 1998.
116. Wang N, Yang X-W. Two new flavonoid glycosides from the whole herbs of
Hyssopus officinalis. Journal of Asian natural products research. 2010;12(12):1044-
50.
117. Hernandez T, Canales M, Teran B, Avila O, Duran A, Garcia AM, et al. Antimicrobial
activity of the essential oil and extracts of Cordia curassavica (Boraginaceae). Journal
of Ethnopharmacology. 2007;111(1):137-41.
118. Chopra I. The glossary of Indian medicinal plants. New Delhi, CSIR. 1956;74.
119. Tiwari R, Srivastava K, Shukla S, Bajpai R. Chemical examination of the fixed oil
from the seeds of Cordia myxa. Planta medica. 1967;15(3):240-4.
120. Abro G, Syed T, Dayo Z. Varietal resistance of cotton against Earias spp. Pak J Biol
Sci. 2003;6(21):1837-9.
121. Ifzal S, Qureshi A. Studies on Cordia myxa. Part I. The monosaccharide and
polysaccharide components of fruits of Cordia myxa. Pakistan Journal Scientific and
Industrial Research. 1976;19(2):64-5.
122. Karawya M, Wassel G, Baghdadi H, Ammar N. Mucilagenous contents of certain
Egyptian plants. Planta medica. 1980.

127
123. Saxena AK. Organotin compounds: toxicology and biomedicinal applications. Applied
organometallic chemistry. 1987;1(1):39-56.
124. Wohlfarth C, Wohlfahrt B. References for Pure Organic Liquids. Pure Organic
Liquids: Springer; 2002. p. 1044-85.
125. Srivastava SK, Srivastava SD. Taxifolin 3, 5-dirhamnoside from the seeds of Cordia
obliqua. Phytochemistry. 1979;18(12):2058-9.
126. Dhawan B, Rastogi R. Recent developments from Indian Medicinal plants. The
Medicinal Plant Industry CRC Press, Boca Raton. 1991:185-208.
127. Chauhan J, Srivastava S, Sultan M. Hesperetin 7-rhamnoside from Cordia obliqua.
Phytochemistry. 1978;17(2):334.
128. Chauhan JS, Srivastava SK. Lupa-20, 29-ene-3-o-β-D-maltoside from the roots of
Cordia Obliqua. Phytochemistry. 1978;17(5):1005-6.
129. Srivastava S, Srivastava S, Nigam S. Lupa-20 (29)-ene-3-O-alpha-L-
rhamnopyranoside from the roots of Cordia obliqua. Journal of the Indian Chemical
Society. 1983.
130. Karnick C. Pharmacology of Ayurvedic medicinal plants: Sri Satguru Publications;
1996.
131. Kloss J. The Handbook of Herbal Medicine, Natural Foods, and Home Remedies: Sri
Satguru Publications; 2001.
132. Vishal A, Parveen K, Pooja S, Kannappan N, Kumar S. Diuretic, laxative and toxicity
studies of Viola odorata aerial parts. Pharmacol online. 2009;1:739-48.
133. Ammon H, Anazodo M. 1992. Curcumin: A potent inhibitor of leukotriene B4
formation in rat peritoneal polymorphonuclear neutrophils (PMNL). Planta Medica.
58: 226. Ammon, HPT, Safayhi, H., Mack, T. and Sabieraj, J. 1993. Mechanism of.
Medica. 1991;57:1-7.
134. Bibi S, Dastagir G, Hussain F, Sanaullah P. Elemental composition of Viola odorata
Linn. Pak J Pl Sci. 2006;12:141-3.
135. Muhammad N, Saeed M, Barkatullah IM, Khan H. Pharmacognostic studies of Viola
betonicifolia. African Journal of Pharmacy and Pharmacology. 2012;6(1):43-7.

128
136. Muhammad N, Saeed M, Gilani SN. Analgesic and anti-inflammatory profile of n-
hexane fraction of viola betonicifolia. Tropical Journal of Pharmaceutical Research.
2013;11(6):963-9.
137. Mittal P, Gupta V, Goswami M, Thakur N, Bansal P. PHYTOCHEMICAL AND
PHARMACOLOGICAL POTENTIAL OF VIOLA ODORATA.
138. Halliwell B. Free radicals, antioxidants, and human disease: curiosity, cause, or
consequence? The lancet. 1994;344(8924):721-4.
139. Oyaizu M. Studies on products of browning reaction--antioxidative activities of
products of browning reaction prepared from glucosamine. Eiyogaku zasshi= Japanese
journal of nutrition. 1986.
140. Das N, Kayastha AM, Srivastava PK. Purification and characterization of urease from
dehusked pigeonpea (Cajanus cajan L.) seeds. Phytochemistry. 2002;61(5):513-21.
141. Wiegand I, Geiss HK, Mack D, Stürenburg E, Seifert H. Detection of extended-
spectrum beta-lactamases among Enterobacteriaceae by use of semiautomated
microbiology systems and manual detection procedures. Journal of clinical
microbiology. 2007;45(4):1167-74.
142. LaRocco M, Murray P, Baron E, Jorgensen J, Landry M, Pfaller M. Reagents, stains,
and media: mycology. Manual of clinical microbiology: Volume 2. 2006(Ed. 9):1737-
44.
143. Rockville M, editor United States of Pharmacopeia-National Formulary. USP30-
NF25, The United States Pharmacoepial Convention; 2007.
144. Messer SA, Moet GJ, Kirby JT, Jones RN. Activity of contemporary antifungal
agents, including the novel echinocandin anidulafungin, tested against Candida spp.,
Cryptococcus spp., and Aspergillus spp.: report from the SENTRY Antimicrobial
Surveillance Program (2006 to 2007). Journal of clinical microbiology.
2009;47(6):1942-6.
145. Forbes B, Sahm D, Weissfeld A, Bailey Ss. Diagnostic microbiology 12th Edition:
Mosby Elsevier, St. Louis, MO. 2007:778-81.
146. MacFaddin J. Media for Isolation-Cultivation-Identification-Maintenance of Medical
Bacteria, Vol. 1, Williams and Wilkins, Baltimore Disclaimer: User must ensure
suitability of the product (s) in their application prior to use. 1985.
129
147. Perez C, Pauli M, Bazerque P. An antibiotic assay by the agar well diffusion method.
Acta Biol Med Exp. 1990;15:113-5.
148. Srinivasan D, Nathan S, Suresh T, Perumalsamy PL. Antimicrobial activity of certain
Indian medicinal plants used in folkloric medicine. Journal of Ethnopharmacology.
2001;74(3):217-20.
149. Noh J-R, Kim Y-H, Gang G-T, Yang K-J, Lee H-S, Nguyen PH, et al. Chestnut
(Castanea crenata) inner shell extract inhibits development of hepatic steatosis in
C57BL/6 mice fed a high-fat diet. Food chemistry. 2010;121(2):437-42.
150. Warda S, Fathia M, Amel O. Antibacterial activity of Tamarindus indica fruit and
Piper nigrum seed. Research journal of microbiology. 2007;2(11):824-30.
151. Pundir RK, Jain P. Comparative studies on the antimicrobial activity of black pepper
(Piper nigrum) and turmeric (Curcuma longa) extracts. International Journal of
Applied Biology and Pharmaceutical Technology. 2010;1(2):492-500.
152. Nirmala P, Selvaraj T. Anti-inflammatory and anti-bacterial activities of Glycyrrhiza
glabraL. Journal of Agricultural Technology. 2011;7(3):815-23.
153. Kizil S, Uyar F. Antimicrobial Activities of Some Thyme (Thymus, Staureja,
Origanum and Thymbra) Species against ImportantPlant Pathogens. Asian Journal of
Chemistry. 2006;18(2):1455.
154. Kumari AAG, Promwichit P. In vitro antimicrobial evaluation of Zingiber officinale,
Curcuma longa and Alpinia galanga extracts as natural food preservatives. American
Journal of Food Technology. 2009;4(5):192-200.
155. Azmi AA, Jamali S, Murad R, Zaidi AH. Antibacterial activity of Joshanda: a
polyherbal therapeutic agent used in common cold. Pakistan Journal of Pharmacology.
2010;27(1):25-8.
156. Hassan S, Khan MA. In vitro biological activity of decoction of Joshanda. Pak J
Pharm Sci. 2014;27(2):239-43.
157. Claeson UP, Malmfors T, Wikman G, Bruhn JG. Adhatoda vasica: a critical review of
ethnopharmacological and toxicological data. Journal of Ethnopharmacology.
2000;72(1):1-20.
158. Bown D. The Royal Horticultural Society encyclopedia of herbs & their uses: Dorling
Kindersley Limited; 1995.

130
159. NUMAZAKI K, UMETSU M, CHIBA S. Effect of glycyrrhizin in children with liver
dysfunction associated with cytomegalovirus infection. The Tohoku journal of
experimental medicine. 1994;172(2):147-53.
160. Parvez L, Vaidya M, Sakhardande A, Subburaj S, Rajagopalan T. Evaluation of
antitussive agents in man. Pulmonary pharmacology. 1996;9(5):299-308.
161. Sheikh ZA, Zahoor A, Khan SS, Usmanghani K. Design, Development and
Phytochemical Evaluation of a Poly Herbal Formulation Linkus Syrup. Chinese
Medicine. 2014;2014.
162. Khan TA, Madni SA, Zaidi A. Acute respiratory infections in Pakistan: have we made
any progress? Journal of the College of Physicians and Surgeons--Pakistan: JCPSP.
2004;14(7):440-8.
163. Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K, Campbell H. Epidemiology and
etiology of childhood pneumonia. Bulletin of the World Health Organization.
2008;86(5):408-16B.
164. Berlin Jr C, McCarver-May D, Notterman D, Ward R, Weismann D, Wilson G, et al.
Use of codeine-and dextromethorphan-containing cough remedies in children.
Pediatrics. 1997;99(6):918-20.
165. Litovitz T, Manoguerra A. Comparison of Pediatric Poisoning Hazards: An Analysis
of 3.8 Million Exposure Incidents A Report from the American Association of Poison
Control Centers. Pediatrics. 1992;89(6):999-1006.
166. Health UDo, Services H. US Food and Drug Administration Protecting and Promoting
Your Health. Recuperado de http://www fda gov/[Links].
167. Desai L, Oza J, Khatri K. Prospective process validation of polyherbal cough syrup
formulation. Journal of Advanced Pharmacy Education & Research Oct-Dec.
2012;2(4).
168. Blumenthal M. Harvard study estimates consumers spend $5.1 billion on herbal
products. Herbal Gram. 1999;45:68.
169. Tyler VE. A Sensible Guide to the Use of Herbs and Related Remedies: Haworth
Press, Incorporated; 1993.
170. Barlow SM. Toxicological aspects of antioxidants used as food additives. Food
antioxidants: Springer; 1990. p. 253-307.
131
171. Barnes NC, Piper PJ, Costello JF. Comparative effects of inhaled leukotriene C4,
leukotriene D4, and histamine in normal human subjects. Thorax. 1984;39(7):500-4.
172. Schuler P. Natural antioxidants exploited commercially. Food antioxidants: Springer;
1990. p. 99-170.
173. Chu YH, Chang CL, Hsu HF. Flavonoid content of several vegetables and their
antioxidant activity. Journal of the Science of Food and Agriculture. 2000;80(5):561-
6.
174. Koleva II, van Beek TA, Linssen JP, Groot Ad, Evstatieva LN. Screening of plant
extracts for antioxidant activity: a comparative study on three testing methods.
Phytochemical analysis. 2002;13(1):8-17.
175. Mantle D, Eddeb F, Pickering AT. Comparison of relative antioxidant activities of
British medicinal plant species in vitro. Journal of Ethnopharmacology.
2000;72(1):47-51.
176. Meir S, Kanner J, Akiri B, Philosoph-Hadas S. Determination and involvement of
aqueous reducing compounds in oxidative defense systems of various senescing
leaves. Journal of agricultural and food chemistry. 1995;43(7):1813-9.
177. Gutteridge J. Lipid peroxidation and antioxidants as biomarkers of tissue damage.
Clinical chemistry. 1995;41(12):1819-28.
178. Mahdi W. 17 Linguistic data on transmisston if Southeast Asian cultigens to India and
Sri Lanka. 1998.
179. Rubin RN, Navon L, Cassano PA. Relationship of serum antioxidants to asthma
prevalence in youth. American journal of respiratory and critical care medicine.
2004;169(3):393-8.
180. FD G,李郁芬, Peters J. Children's lung function and antioxidant vitamin, fruit, juice,
and vegetable intake. 2003.
181. Holroyde M, Cole M, Altounyan R, Dixon M, Elliott E. Bronchoconstriction produced
in man by leukotrienes C and D. The Lancet. 1981;318(8236):17-8.
182. Rahman I, Morrison D, Donaldson K, MacNee W. Systemic oxidative stress in
asthma, COPD, and smokers. American journal of respiratory and critical care
medicine. 1996;154(4):1055-60.

132
183. Pundir RK, Jain P. Comparative studies on the antimicrobial activity of black pepper
(piper nigrum) and turmeric (curcuma longa) extracts. 2010.
184. Kumari A, Promwichit P. In vitro antimicrobial evaluation of Zingiber officinale,
Curcuma longa and Alpinia galanga extracts as natural food preservatives. Am J Food
Technol. 2009;4(5):192-200.
185. Gadomski A, Rubin J. Cough and cold medicine use in young children: a survey of
Maryland pediatricians. Maryland medical journal (Baltimore, Md: 1985).
1993;42(7):647.
186. Pandolfini C, Impicciatore P, Bonati M. Parents on the web: risks for quality
management of cough in children. Pediatrics. 2000;105(1):e1-e.
187. Kogan MD, Pappas G, Stella MY, Kotelchuck M. Over-the-counter medication use
among US preschool-age children. Jama. 1994;272(13):1025-30.
188. Agrawal S, Paridhavi M. Herbal drug technology: Hyderabad: Universities Press
Private Limited; 2007.
189. Thakkar K, Parmar V, Patel D, Meshram D. Recent advances in herbal drug
standardization-a review. Int J Adv Pharm Res. 2013;4(8):2130-8.
190. Chawla R, Thakur P, Chowdhry A, Jaiswal S, Sharma A, Goel R, et al. Evidence
based herbal drug standardization approach in coping with challenges of holistic
management of diabetes: a dreadful lifestyle disorder of 21st century. Journal of
Diabetes & Metabolic Disorders. 2013;12(1):1.
191. Houssen ME, Ragab A, Mesbah A, El-Samanoudy AZ, Othman G, Moustafa AF, et
al. Natural anti-inflammatory products and leukotriene inhibitors as complementary
therapy for bronchial asthma. Clinical biochemistry. 2010;43(10):887-90.
192. Samy RP, Pushparaj PN, Gopalakrishnakone P. A compilation of bioactive
compounds from Ayurveda. Bioinformation. 2008;3(3):100.
193. Subhose V, Srinivas P, Narayana A. Basic principles of pharmaceutical science in
Ayurveda. Bulletin of the Indian Institute of History of Medicine (Hyderabad).
2004;35(2):83-92.
194. Ali MA, Alam N, Yeasmin M, Khan A, Sayeed M, Rao V. Antimicrobial screening of
different extracts of Piper longum Linn. Research Journal of Agriculture and
Biological Sciences. 2007;3(6):852-7.

133
195. Ojha N. Management of respiratory allergic disorders (rads) in children: some clinical
and experimental evidences from ayurveda. Journal of Herbal Medicine and
Toxicology. 2011;5(1):103-9.
196. Rakesh SU, Salunkhe V, Dhabale P, Burade K. HPTLC method for quantitative
determination of gallic acid in hydroalcoholic extract of dried flowers of Nymphaea
stellata Willd. Asian Journal of Research in Chemistry (AJRC). 2009;2(2):131-4.
197. Slaveska-Raicki R, Rafajlovska V, Rizova V, Spirevska I. HPTLC determination of
gallic acid and tannin in extracts of bearberry leaves. JPC-Journal of Planar
Chromatography-Modern TLC. 2003;16(5):396-401.
198. Patel DK, Patel K, Dhanabal S. Standardization of Berberis aristata extract through
conventional and modern HPTLC techniques. Asian Pacific Journal of Tropical
Disease. 2012;2:S136-S40.
199. Angaji EBSA, Angaji SM. Antimicrobial effects of four medicinal plants on dental
plaque. Journal of Medicinal Plants Research. 2009;3(3):132-7.
200. Grassmann J, Hippeli S, Vollmann R, Elstner EF. Antioxidative properties of the
essential oil from Pinus mugo. Journal of agricultural and food chemistry.
2003;51(26):7576-82.
201. Altman RD, Marcussen K. Effects of a ginger extract on knee pain in patients with
osteoarthritis. Arthritis & Rheumatism. 2001;44(11):2531-8.
202. Daswani G, Brijesh S, Birdi J, editors. Preclinical testing of medicinal plants:
advantages and approaches. Workshop Proceedings on Approaches towards
Evaluation of Medicinal Plants Prior to Clinical Trial; 2006: Citeseer.
203. Ogbonnia S, Mbaka G, Anyika E, Osegbo O, Igbokwe N. Evaluation of acute toxicity
in mice and subchronic toxicity of hydroethanolic extract of Chromolaena odorata (L.)
King and Robinson (Fam. Asteraceae) in rats. Agriculture and Biology Journal of
North America. 2010;1(5):859-65.
204. Stewart M, Moar J, Steenkamp P, Kokot M. Findings in fatal cases of poisoning
attributed to traditional remedies in South Africa. Forensic science international.
1999;101(3):177-83.
205. Saad B, Azaizeh H, Abu-Hijleh G, Said O. Safety of traditional Arab herbal medicine.
Evidence-Based Complementary and Alternative Medicine. 2006;3(4):433-9.

134
206. Colson CR, De Broe ME. Kidney injury from alternative medicines. Advances in
chronic kidney disease. 2005;12(3):261-75.
207. Cheng C-W, Bian Z-X, Wu T-X. Systematic review of Chinese herbal medicine for
functional constipation. World J Gastroenterol. 2009;15(39):4886-95.
208. Archer L, Simpson H. Night cough counts and diary card scores in asthma. Archives
of disease in childhood. 1985;60(5):473-4.
209. Hamutcu R, Francis J, Karakoc F, Bush A. Objective monitoring of cough in children
with cystic fibrosis. Pediatric pulmonology. 2002;34(5):331-5.
210. Michelson AL, Lowell FC. Antihistaminic drugs. New England Journal of Medicine.
1958;258(20):994-1000.
211. Finkle WD, Adams JL, Greenland S, Melmon KL. Increased risk of serious injury
following an initial prescription for diphenhydramine. Annals of Allergy, Asthma &
Immunology. 2002;89(3):244-50.
212. Ventegodt S, Orr G, Merrick J. The need for evidence-based, non-drug medicine.
2012.

LIST OF PAPERS IN PUBLICATION
1. Rehman, H., Shaikh, Z. A., Naveed, S., Latif, M., & Usmanghani, K.
(2016). Evaluation of in vitro antioxidant, reducing, lipoxygenase and ACE
inhibition activity of polyherbal drug linkus. African Journal of Pharmacy
and Pharmacology, 10(44), 945-953.
2. Rehman, H., Naveed, S., & Usmanghani, K. (2016). Efficacy and safety of
Linkus, Aminophylline diphenhydramine and acefyllin piperazine for the
treatment of cough in children. Pakistan Journal of Pharmaceutical
Sciences, 1(29), 1027-1032.
3. Rehman, H., Naveed, S., & Usmanghani, K. (2016). An Interquartile
Relationship betweenPolyherbal Extract Based lozenges Linkus –A Phase
IV Comparative Randomised Control Trial. Accepted Pakistan Journal of
Pharmaceutical Sciences.
4. Rehman, H., Zahoor A., Naveed, S., & Usmanghani, K. (2017). Polyherbal
Extract Based Linkus Lozenges for Symptomatic Relief: Design,
Development and Evaluation. American Journal of Advanced Drug
Delivery. AJADD[5][01][2017]011-018
5. Evaluation of Efficacy and toxicity of poly herbal lozenges –Linkus in
experimental animals. Accepted African Journal of Traditional,
Complementary and Alternative Medicines
6. Quantitative determination of piperine and glycyrrhizine via a noval
HPTLC method in poly herbal formulation. Submitted
7. Polyherbal Extract Based Linkus Lozenges for Symptomatic Relief:
Design, Development and Evaluation. Submitted- on imedped publications
9. Missed Opportunities in Pakistan: The Never-ending struggles and
Challenges in Clinical Research.Submitted
10. Challenging Status about Patient Centricity among Health Care Profession
in Pakistan.Submitted
135
8. Antimicrobial analysis of polyherbal formulation linkus cough
syrup..Submitted





![+DPLUSXU + 3 'HSDUWPHQW RI &KHPLFDO (QJLQHHULQJ14.139.56.3/wp-content/uploads/2017/07/B.-Tech...Shashi Chawla, A Text Book of Engineering Chemistry. COMMUNICATION SKILLS [CHH-113]](https://static.fdocuments.us/doc/165x107/60edce1ab1015a78a07aa1a3/dplusxu-3-hsduwphqw-ri-khplfdo-qjlqhhulqj14139563wp-contentuploads201707b-tech.jpg)
![&RPSDUDWLYH GHWHUPLQDWLRQ RI UXVFRJHQLQV …acgpubs.org/JCM/2018/Volume 12/Issue 1/7-17-JCM-1805-094.pdf · 'hwhuplqdwlrq ri uxvfrjhqlqv frqwhqw lq %xwfkhu¶v %urrp ukl]rph vdpsohv](https://static.fdocuments.us/doc/165x107/5e0cef6c7decb3076e791cbd/rpsdudwlyh-ghwhuplqdwlrq-ri-uxvfrjhqlqv-12issue-17-17-jcm-1805-094pdf.jpg)











