
Amol cranio vertebralanomalies-21-10-14
117
Cranio-Vertebral Cranio-Vertebral Anomalies Anomalies DR. AMOL GULHANE DR. AMOL GULHANE
-
Upload
amol-gulhane -
Category
Health & Medicine
-
view
93 -
download
0
Transcript of Amol cranio vertebralanomalies-21-10-14

Cranio-Vertebral Cranio-Vertebral AnomaliesAnomalies
DR AMOL GULHANEDR AMOL GULHANE
ClassificationClassificationII Bony AnomaliesBony Anomalies
AA Major AnomaliesMajor Anomalies
1 Platybasia1 Platybasia
2 Occipitalization2 Occipitalization
3 Basilar Invagination3 Basilar Invagination
4 Dens Dysplasia4 Dens Dysplasia
5 Atlanto- axial dis5 Atlanto- axial dis
B Minor Anomalies1Dysplasia of Atlas2Dysplasia of occipital condyles clivus etc
II Soft Tissue anomalies1 Arnold-Chiari Malformation2 Syringomyelia Syringobulbia
OSSIFICATION CENTRESOCCIPUT amp BASIOCCIPUT2 occipital squamous portions ndash2 centresBasiocciput(clivus) -1 centre2 Jugular tubercles ndash2 centres2 Occipital condylesndash2 centres
ATLAS ossifies from 3 centresEach half of post Arch with lateral mass unites at 3 ndash4 yearsAnterior arch unites with lateral mass at 6 ndash8 years
AXIS ossifies from 5 primary amp 2 secondary centres
2 Neural arches ndash2 centres appear at 7 ndash8 wkBody of axis ndash1 centre appear at 4 ndash5 monthsBody of dens ndash2 centres appear at 6 ndash7 months4 pieces (at birth) unite at 3 ndash6 years
Tip of odontoid appears at 3 ndash6 years unites with the body of odontoid at 12 years
Cerebellar tonsils
medulla
Vertebral artery
basion
Medulla oblongata
basion
Anterior arch of atlas
Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ClassificationClassificationII Bony AnomaliesBony Anomalies
AA Major AnomaliesMajor Anomalies
1 Platybasia1 Platybasia
2 Occipitalization2 Occipitalization
3 Basilar Invagination3 Basilar Invagination
4 Dens Dysplasia4 Dens Dysplasia
5 Atlanto- axial dis5 Atlanto- axial dis
B Minor Anomalies1Dysplasia of Atlas2Dysplasia of occipital condyles clivus etc
II Soft Tissue anomalies1 Arnold-Chiari Malformation2 Syringomyelia Syringobulbia
OSSIFICATION CENTRESOCCIPUT amp BASIOCCIPUT2 occipital squamous portions ndash2 centresBasiocciput(clivus) -1 centre2 Jugular tubercles ndash2 centres2 Occipital condylesndash2 centres
ATLAS ossifies from 3 centresEach half of post Arch with lateral mass unites at 3 ndash4 yearsAnterior arch unites with lateral mass at 6 ndash8 years
AXIS ossifies from 5 primary amp 2 secondary centres
2 Neural arches ndash2 centres appear at 7 ndash8 wkBody of axis ndash1 centre appear at 4 ndash5 monthsBody of dens ndash2 centres appear at 6 ndash7 months4 pieces (at birth) unite at 3 ndash6 years
Tip of odontoid appears at 3 ndash6 years unites with the body of odontoid at 12 years
Cerebellar tonsils
medulla
Vertebral artery
basion
Medulla oblongata
basion
Anterior arch of atlas
Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

OSSIFICATION CENTRESOCCIPUT amp BASIOCCIPUT2 occipital squamous portions ndash2 centresBasiocciput(clivus) -1 centre2 Jugular tubercles ndash2 centres2 Occipital condylesndash2 centres
ATLAS ossifies from 3 centresEach half of post Arch with lateral mass unites at 3 ndash4 yearsAnterior arch unites with lateral mass at 6 ndash8 years
AXIS ossifies from 5 primary amp 2 secondary centres
2 Neural arches ndash2 centres appear at 7 ndash8 wkBody of axis ndash1 centre appear at 4 ndash5 monthsBody of dens ndash2 centres appear at 6 ndash7 months4 pieces (at birth) unite at 3 ndash6 years
Tip of odontoid appears at 3 ndash6 years unites with the body of odontoid at 12 years
Cerebellar tonsils
medulla
Vertebral artery
basion
Medulla oblongata
basion
Anterior arch of atlas
Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Cerebellar tonsils
medulla
Vertebral artery
basion
Medulla oblongata
basion
Anterior arch of atlas
Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Medulla oblongata
basion
Anterior arch of atlas
Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Atlas (anterior arch)
Transverse lig atlasDens of axis
Medulla oblongata
Vertebral artery
Atlas posterior arch
Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Atlas lateral mass
Transverse ligament of atlas
Transverse process and foramen transversarium
Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Anterior longitudinal ligament
Apical ligament of dens
Tectorial membrane
Transverse ligament of atlas
Anterior arch of atlas
Dens of axis (C2)
Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Clivus
Anterior atlanto-occipital membrane
Atlas (lateral mass)
Axis
Int carotid artery
Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Alar ligaments
Atlanto-axial jointAtlanto-occipital joint
Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Anatomical and Radiological AspectsAnatomical and Radiological Aspectsbull Anatomical LandmarksAnatomical Landmarks
bull Nasion Nasion -the middle point of the junction of the frontal and the two nasal bones (fron-the middle point of the junction of the frontal and the two nasal bones (frontonasal suturetonasal suture
bull Clivus Clivus bull BasionBasion --the midpoint of the anterior border of the foramen magnumthe midpoint of the anterior border of the foramen magnumbull OpisthionOpisthion-- posterior margin of the foramen magnum posterior margin of the foramen magnum bull
bull Lines angles and indexesLines angles and indexesbull Chamberlainrsquos LineChamberlainrsquos Linebull McGregorrsquos LineMcGregorrsquos Linebull McRaersquos LineMcRaersquos Linebull Klaus Height IndexKlaus Height Indexbull AT IndexAT Index
bullBasal AnglebullBoogardrsquos anglebullBullrsquos anglebullA-O intervalbullEDFM
CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

CRANIOMETRYCraniometry of the CVJ uses a series of lines planes amp angles to define the normal anatomic relationships of the CVJ
These measurements can be taken on plain X rays 3D CT or on MRI
The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The Chamberlainrsquos lineThe Chamberlainrsquos line
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Chamberlain lsquos line Palato-occipital line
Posterior pole of hard palate to the Opisthion
Tip of the dens usually below and upto 3 mm above this line
Dens gt 6mm in basilar impression
H O
Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Significance
An abnormal superior position of the odontoid indicates basilar impression
Common precipitating causes include platybasia atlas occipitalization and bone-softening diseases of the skull base (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
Occasionally rheumatoid arthritis may also precipitate this deformity
A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

A drawn from the posterosuperior margin of the hard palate to the most inferior surface of the occipital bone
The McGregorrsquos line
The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The McGregorrsquos lineThe McGregorrsquos line
H
Low occiput
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Mc Gregorrsquos lineBasal lineMOST ACCURATE
Postero-superior margin of Hard palate ndash most inferior surface of occipital bone
Odontoid apex shouldnrsquot lie above lt 5mm
Superior lie of odontoid indicates basilar impression(gt5mm)
Low occiput
The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The McRaersquos lineThe McRaersquos line
B O
Mc Raersquos lineFormen magnum line
Anterior and posterior ends of formen magnum(Basion and Opisthion)
Inf margin of occiput should lie at below this line Tip of dens does not exceed this line Perpendicular line along odontoid intersects 1st line in its anterior quadrant
Inf margin of occiput lies superior ndash Basilar imp
If sagittal diameter lt 20mm neurological symptoms (+) (foramen magnum stenosis)
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
Significance
If the inferior margin of the occipital bone is convex in a superior direction andor lies above this line then basilar impression is present
Predisposing causes include platybasia occipitalization rheumatoid arthritis and bone-softening diseases (eg Pagetrsquos disease osteomalacia and fibrous dysplasia)
If the odontoid apex does not lie in the ventral quarter of this line a dislocation of the atlanto-occipital joint or a fracture or dysplasia of the dens may be present
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
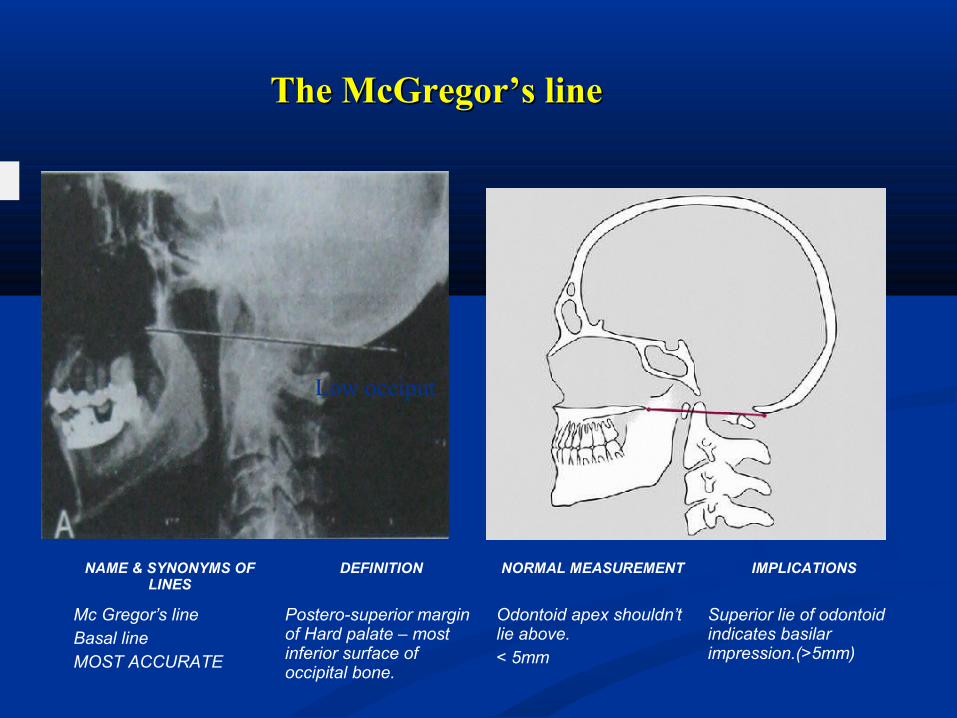
Clivus-Canal lineClivus-Canal line
C
B
OC2
H
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Wackenhiersquos lineClivus canal line
Drawn along clivus into cervical canal
Odontoid tip is ventral and tangential to line
Odontoid transects the line in basilar imp
Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Basilar AngleWelckerrsquos basilar angle Martinrsquos basilar angle sphenobasilar angle
LandmarksThree points are located and joined together by two lines the subsequent angle is measured
The three points are the nasion (frontal-nasal junction) the center of the sella turcica (midpoint between the clinoid processes) and the basion (anterior margin of the foramen magnum)
The average normal angle subtended by these two lines is 137deg with a normal variation of 123-152deg
Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Significance
The measurement is an index of the relationship between the anterior skull and its base
The angle will increase beyond 152deg in platybasia in which the base is elevated in relation to the rest of the skull
This may or may not be associated with basilar impression
The deformity may be congenital (isolated impression occipitalization) or acquired (Pagetrsquos disease rheumatoid arthritis fibrous dysplasia)
Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Basilar AngleBasilar Angle
Mid sella
B
N
S
B
N
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Basilar angle Welckerrsquos Martinrsquos Spheno-BA
Nasion ndash Centre of the sella ndash Basion
Angle 1370 (123-1520)
gt1520 Platybasia(Base is elevated)+- Basilar impression
Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Modified MRI techniqueThis technique described by Koenigsbert et al yields a normal value range (95 CI) 116deg - 118deg for adults and 113deg - 115deg for children Angle formed by line extending across the anterior cranial fossa to the tip to the dorsum sellae line drawn along the posterior margin of the clivus
The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The Boogardrsquos lineThe Boogardrsquos line
N
O
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Line Nasion to Opisthion Basion should lie below this line
Altered in basilar impression
Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Boogardrsquos angleBoogardrsquos angle
Tuberculum sellaTuberculum sella
B o
N
Mc Ray
s
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Boogard lsquos Angle Angle intersected by1st line between Dorsum sellae to Basion amp Mc Raersquos line
119-1350
Average - 1220
gt 1350
Basillar impression
Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Boogardrsquos angle
MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

MethodMethod of Bull of Bull
C2
Atlas plane
Chamberlain
Bull lsquos angle Atlanto-palatine angle
Posterior Angle betn 1st line from Post tip of hard palate to post margin of foramen magnum 2nd line betn ant amp post tubercles of atlas
Post angle lt130 If odontoid is tilted posteriorly or in case of change of atlas position The angle gt 130
Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Ranawat methodRanawat method
C2
C1
Ranawat method Line joining center of the anterior arch of C1 to post ring amp another line along the axis of the odontoid from the centre of the pedicle of C2 to 1st line
Normal distance between C-1 and C-2 in Men averages 17 mm (plusmn2 mm SD) Women 15 mm (plusmn 2 mm SD)
A decrease in this distance indicates cephalad migration of C-2
C2
C1
C2
C1
PEDICLE
Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Schmidt ndash Fischer AngleSchmidt ndash Fischer Angle (ATLANTO-OCCIPITAL JT AXIS ANGLE)(ATLANTO-OCCIPITAL JT AXIS ANGLE)
O
C2AA JT
AO JT
C1 C1
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Schmidt ndash Fischer Angle
Angle of axis of Atlanto-Occipital joint
125 +- 2 degrees Angle is wider in condylar hypoplasia
CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

CRANIO-VERTEBRAL ANGLECRANIO-VERTEBRAL ANGLE
ax
C
NAME amp SYNONYMS OF LINES
DEFINITION NORMAL MEASUREMENT IMPLICATIONS
Cranio vertebral angle Between clivus line and post axial line
Flexion ndash 1500
Extension - 1800
lt1500 Platybasiacord compressionBasilar impression
bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

bullBDI less than 85 mm compared with 12 mm on data from plain radiographs
bullAn ADI less than 2 mm compared with 3 mm previously accepted
Midsagittal MDCT image of the craniocervical junction demonstrates the BDI(basion-dental interval) as the distance from the most inferior portion of the basion to the closest point of the superior aspect of the dens
MDCT VS PLAIN RADIOGRAPHY IN CRANIOMETRYhellip
MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

MDCT image of the craniocervical junction demonstrates the ADI which is calculated by drawing a line from the posterior aspect of the anterior arch of C1 to the most anterior aspect of the dens at the midpoint of the thickness of the arch in craniocaudal dimension
Atlantodental Interspace (ADI)SynonymsAtlas-odontoid space predental interspace atlas-dens interval
Flexion is the optimum view to assess the interspace because in this position the most stress is placed on the transverse ligament of the atlas
Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Normal Values for Atlantodental Interspace
Adults 1 to 3 mm
Children1 to 5 mm
Significance
A decreased space is to be expected with advancing age because of degenerative joint disease of the atlantodental joint
A more significant change is an abnormally widened space with reduction in the neural canal size
The most frequent causes include trauma occipitalization Downrsquos syndrome pharyngeal infections and inflammatory arthropathies (eg ankylosing spondylitis rheumatoid arthritis psoriatic arthritis and Reiterrsquos syndrome)
Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Sagittal CT images right measures the basion-posterior axial line interval which is denoted by the small horizontal red line
The left image demonstrates measurement of the basion-dental interval which is denoted by the vertical red line
If either of these distances are greater than 12 mm then the diagnosis of occipitocervical dissocation is fairly certain
The basion-posterior axial line interval (BAI) is drawn along the posterior aspect of the dens (the posterior axial line) and a measurement between this line and the tip of the basion is performed
Harris Lines or the Rule of Twelve
The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The Powers ratio can be measured to determine if there is anterior occipitoatlantal dissociation The Powers ratio is the distance between the basion and the posterior spinolaminar line of C1 (BC) divided by the distance between the anterior arch of C1 and the opisthion (AO) If the Powers Rule (BC)(AO) is greater than 1 then anterior occipitoatlantal dissocation has likely occurred
The accuracy of the Powers ratio is controversial since it can be difficult to locate the position of the basion and the opisthion on the lateral skull radiograph It is easier to obtain on sagittal CT
Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Sagittal MDCT image of the craniocervical junction demonstrates the AOI which is calculated by drawing a line perpendicular to the articular surfaces of the occipital condyle and the lateral mass of C1 This line is drawn at the center of the articulation by correlating the sagittal and coronal images
bullThe AOI demonstrated 95 of the population ranged between 05 mm and 14 mm
AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

AP open mouth
If the lateral margin of the atlas lateral mass lies lateral to the lateral axis margin this may be a radiologic sign of Jeffersonrsquos fracture odontoid fracture alar ligament instability or rotatory atlantoaxial subluxation
Atlantoaxial Alignment
ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ATLANTOAXIAL ALIGNMENT
A Normal Alignment
B Abnormal Alignment The abnormality (arrow) is the result of a Jeffersonrsquos fracture of the atlas
Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Table Lines and angles used in radiologic diagnosis of CV anomalies
Parameter Normal range limits
A PLATYBASIA
B BASILAR INVAGINATION
C ATLANTO-AXIAL DISLOCATION
bull Basal angle lt 150 degree
bull Boogardrsquos angle lt 136 degree
bull Bullrsquos angle lt 13 degree
bull Chamberlainrsquos line lt one third of odontoid above this linebull Mcgregorrsquos line lt 5 mmbull Mcrae line odontoid lies below thisbull Klaus height index gt 35 mmbull Atlanto-temporo gt 22mm mandibular index
bull Atlanto-odontoid space upto 3 mm in adults upto 5 mm in childrenbull EDFM gt 19mm
RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

RADIOLOGY OF CVJ(NORMAL VARIANTS amp ANOMALIES)
THE OCCIPUT The basiocciput forms the lower portion of the clivus
The upper portion of the clivusis formed by the basisphenoid separated from the basiocciput by the sphenooccipital synchondrosis
The age at which this synchondrosis fuses ranges from ldquoafter the twelvth yearrdquoto 14-16 years for girls and 16-185 years for boys
Most occipital anomalies are associated with decreased skull base height and basilar invagination
Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Condylus Tertius
Anomalies and malformations of the most caudal of the occipital sclerotomes are collectively termed lsquo lsquomanifestations of occipital vertebraerdquo
When the hypochordal bow of the fourth occipital sclerotome (proatlas) persists or when the proatlas fails to integrate an ossifledremnant may be present at the distal end of the clivus called the condylus tertius or third occipital condyle
This third condyle may form a joint or pseudojoint with theodontoid process or with the anterior arch of the atlas and may lead to limitation in therange of motion of the CVJ
There is an increased prevalence of os odontoideum associatedwith this abnormality
The occipital bone is composed of asioccipital exoccipital and supraoccipital portions enclosing the foramen magnum
Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Condylus tertius and platybasia Midsagittal Ti-weighted MR image revealsmarked skull base flattening with a Welcher basal angle of 150 dotted line) Note the marked bowstring deformity of the cervicomedullary junctionThe C-1 arch (A) lies directly above the tip of the odontoid process (0) Marrow within accessory ossification centers (condylus tertius)
Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Condylar Hypoplasia
In condylar hypoplasia the occipital condyles are underdeveloped and have a flattened appearance leading to basilar invagination (violation of the Chamberlain line) and widening of the atlantooccipital joint axis angle
The tip of the odontoid process and the lateral masses of the atlas typically lie below a line connecting the mastoid tips (bimastoid line) this relationship is violated in condylar hypoplasia
The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The lateral masses of the atlas may be fused to the hypoplastic condylesfurther accentuating the basilar invagination
Clinically condylar hypoplasia limits or may even abolish movements at the atlantooccipital joint and may occasionally lead tocompression of the vertebral artery secondaryto excessive posterior gliding of the occiput inrelation to the atlas
image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

image
PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

PLATYBASIA
BASILAR IMPRESSION
BASILAR INVAGINATION
These terms are not synonymous
PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

PLATYBASIAMartinrsquos anamoly
Flattening of angle between the clivus and the body of the sphenoid CFPRIMARY- Isolated or in conjunction with other dysplasias like Achondroplasia Osteogenesis imperfecta
SECONDARY - Pagetrsquos disease bone softening degenerative diseaseBasilar angle gt 152deg(N=123-1520)
Craniovertebral = clivus-canal angle becomes acute (lt150deg) MC associated changes - Basilar invagination anomalies of C1(occipitalisation)block vertebra Klippel-Feil syndrome
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
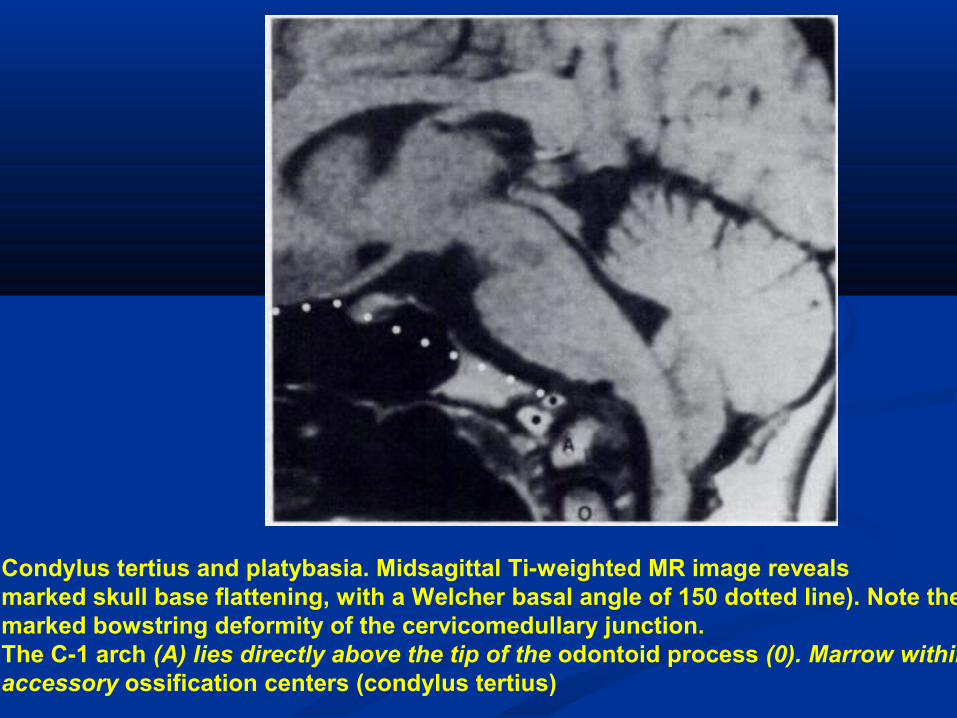
BASILAR INVAGINATION
Basilar invagination implies that the floor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
There are two types of basilar invagination primary invagination which is developmental and more common secondary invagination which is acquired
Primary invagination can be associated with occipitoatlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies
In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

In BI all three parts of the occipital bone (basiocciput exoccipitalamp squamous occipital bone) are deformed
Topographic types of BI Anterior BI hypoplasia of the basilar process of the occipital boneBI of the occipital condyles(ParamedianBI)ndashCondylar hypoplasiaBI in the lateral condylar areaPosterior BI posterior margin of the FM is invaginatedUnilateral BIGeneralised BI
BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

BI is associated with high incidence of vertebral artery anomaliesAbnormal curvature of VA is due to the fact that they are of normal length amp course through a reduced bone space (wide angle bw 3rd amp 4th part of VA)
SIGNS SYMPTOMS usually occur in 2nd or 3rd decade
Short neck(78)torticollis (68)
ss of associated ACM (cerebellaramp vestibular disturbances) amp syringomyelia(25 to 35)
Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Motor amp sensory disturbances (85)
Lower cranial nerves involvement
Headache amp pain in the nape of neck (greater occipital N)
ss of raised ICP (HCP) due to posterior encroachment which causes blockage of aqueduct of sylvius
Compression of cerebellum amp vestibular apparatus leading to vertical or lateral nystagmus(65) (not due to direct pressure from post rim of FM but rather due to a thickened band of dura)
Vertebral artery insufficiency ss
bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

bullBASILAR INVAGINATION
bullFloor of the skull is indented by the upper cervical spine amp hence the tip of odontoid is more cephalad protruding into the FM
bullPrimary invagination can be associated with occipito atlantal fusion hypoplasia of the atlas a bifid posterior arch of the atlas odontoid anomalies bullBI is associated with high incidence of vertebral artery anomalies
Chamberlainrsquos line- tip of dens is gt6mm above this line Mc Gregorrsquos line- tip of dens is gt 5mm above this line Mc Raersquos line- tip of dens is above this line Boogardrsquos line- basion is above this line
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
bull Basilar impression refers to secondary or acquired forms of BI
bull due to softening of the bone amp is seen in conditions such as rickets hyperparathyroidism osteogenesis imperfecta Pagets disease neurofibromatosis skeletal dysplasias and RA amp infection producing bone destruction with or without ligamentous laxity
bullMay be associated with developmental cervical canal stenosis amp also fibrous bands amp dural adhesions at the dorsal cervicomedullary junction
BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

BASILAR IMPRESSION (SECONDARY BASILAR INVAGINATION
Pagetrsquosdisease Usually symptomatic after 40 years of ageCT shows irregular thick bones with a ldquomoth eatenrdquoappearance of the calvaria
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
AchondroplasiaGenetically dominant disorder characterized by inhibition of endochondral bone formation
The base of the skull is affected but the membraneous convexity skull bone grows normally
This differential bone growth results in large calvarium on a small baseThe mortality is high in the 1st year of life due to cervicomedullary dysfunction at the FM
A small FM with hypertrophic bone amp a posterior dural shelf results in compression of neural structures
Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Atlantooccipital Assimilation
failure of segmentation between the skull and first cervical vertebra results in assimilation of the atlas
The assimilation may be cornplete or partial
It invariably results in basilar invagination
Although the Wackenheim clivus baseline may be normalthe clivus-canal angle may be decreased
When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

When incompletely assimilated the atlas arches appeartoo high on the lateral plain radiographor when completely assimilated are not visibleat all
There is an increased prevalence of associated fusion of the axis and third cervical vertebra in association with atlantooccipitalAssimilation
When this is present gradual loosening of the atlantodental jointwith progressive atlantoaxial subluxation mayoccur reported in approximately 50 of cases
TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

TOPOGRAPHIC FORMS (WACKENHEIM)
Type I Occipitalization(generally subtotal) associated with BI
Type II Occipitalization(generally subtotal) associated with BI amp fusion of axis amp 3rdcervical vertebrae
Type III Total or subtotal occipitalizationwith BI amp maldevelopment of the transverse ligament
Type III may be associated with various malformations like C2-C3 fusion hemivertebra dens aplasia tertiary condyle etc
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
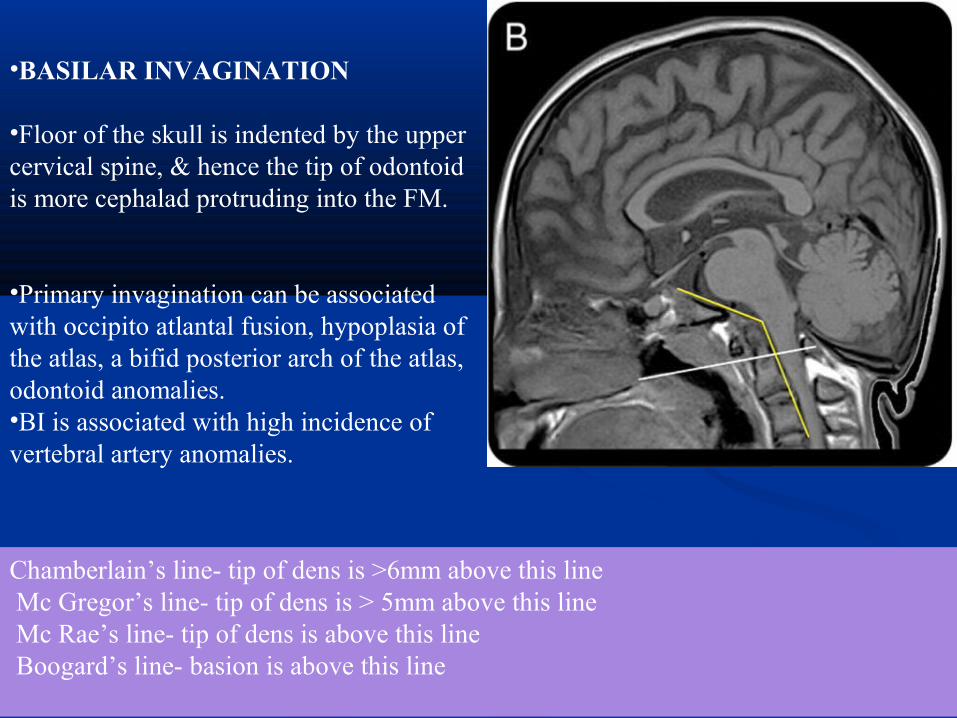
The neurological symptoms are not caused by occipitalization proper but rather by the fact that in the absence of a free atlas TL fails to develop which causes posterior displacement of axis amp compression of the spinal cord
Instability bw atlas amp axis is reducible in patients lt15 yrrsquos but after that irreducible state occurs
ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ATLAS With the exception of the various atlantooccipital assimilations most atlas anomalies when isolated produce no abnormal CVJ relationships and are not associated with basilar invagination
The vast majority of anomalies consist of various arch clefts aplasias and hypoplasias
Arch anomalies are frequently mistaken for fractures in the evaluation of plain radiographs of patients with a history of cervical spine trauma
The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The irregular fragments located inferior to the Anterior arch of the atlas may be
mistaken for fracture fragments The clear cortical margins and characteristic location
help to differentiate this variant from a fracture
Accessory ossification centre for the anterior arch of the atlashelliphellip
PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

PONTICULUS POSTICUS KIMMERLErsquoS DEFORMITY
It is a bony ridge projecting posteriorly from the articular edge of the atlas superior articular facet
The bony projection may be only a few mm long or may elongate to unite with the adjacent neural arch of the atlas to produce an ldquoARCUATE CANALrdquothrough which the vertebral artery passes
This is due to ossification of a portion of the oblique A-O ligament
Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Posterior Arch Anomalies (MC atlas anomaly)
Total or partial aplasia of the posterior atlas arch is rare
Although absence of the posterior arch when isolated is usually asymptomatic but may be associated with anterior atlantoaxial subluxation
Bilateral atlantoaxial subluxation may be associated with both total and partial aplasias simulating the Jefferson fracture
In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

In contrast to the aplasias and hypoplasias clefts of the atlas arches are much more common
Posterior rachischisis most common is observed in 4 of adults
The majority of posterior atlas clefts (97) are midline whereas lateral clefts through the sulcus of the vertebral artery account for the remaining 3
Posterior arch rachischisis may be superimposed on the odontoid process or the axis body on the open-mouth odontoid view simulating a fracture
Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Posterior arch hemiplasia
Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Split Atlas
In contrast to posterior arch rachischisis anterior arch rachischisisis quite rare (0 1 )
It is typically encountered in association with posterior rachischisis-ldquosplit atlasrdquo
Normally on a lateral radiograph the anterior arch of the atlas appears crescentic or half-moon-shaped with dense cortical bone surrounding the medullary cavity and a well-defined predental space
In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

In anterior arch rachischisis the anterior arch appears fat or plump and rounded in configuration appearing to lsquolsquooverlaprsquolsquo the odontoid process (making identification of the predental space impossible) the arch may have unsharp duplicated anterior margins
CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

CONGENITAL ODONTOID ANOMALIES OR DYSPLASIAS
Types of dens dysplasia
Type 1 (Os odontoideum) separate odontoid process
Type 2 (Ossiculum terminale) failure of fusion of
apical segment with its base
Type 3 ndash Agenesis of odontoid base amp apical segment
lies separately
Type 4 ndash Agenesis of odontoid apical segment
Type 5 ndashTotal agenesis of odontoid process
Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Persistent OssiculumTerminaleAlso called Bergman ossicle results from failure of fusion of the terminal ossicle to the remainder of the odontoid process
The fusion typically is accomplished by 12 years of age
Bergman ossicle may be confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) and absolute differentiation between the two diagnoses may be difficult
Whether traumatic or congenital in origin this anomaly is stable when isolated and of relatively little clinical significance
The odontoid process is usually normal in height
the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

the normal dense secondary ossification center for the odontoid process tip which exhibits a characteristic symmetrical V-shaped lucent zone of separation from the body of the dens COMMENT This is a normal finding of the odontoid seen in 25 of patients lt 12 years of age but it is usually not seen after this age at which time it constitutes non-union (ossiculum terminale of Bergmann)
OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

OdontoidAplasia
Total aplasia of the odontoid process is extremely rare
A true aplasia is associated with an excavation defect into the body of axis
may simulate os odontoideum as the os fragment may be perfectly projected over the atlas arch on the open mouth odontoid view
AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

AP Open Mouth Here the odontoid process exists as an abbreviated remnant stump therefore it is not true agenesis The lateral shift of the atlas relative to the axis C1 on C2 indicates instability
OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

OS ODONTOIDEUM
This term first introduced by Giacominiin 1886 refers to an independent osseous structure lying cephalad to the axis body in the location of the odontoid process
The anterior arch of the atlas is rounded and hypertrophic but the posterior arch is hypoplastic
As the gap between the os odontoideum and the axis body usually extends above the level of the superior articular facet of the axis cruciate ligament incompetence and A-A instability are common
The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

The margins of the axis body the os and anterior arch are all well corticated
Type 2 odontoid fracture is typically associated with a flattened sharp uncorticated margin to the upper axis body and a normal half moon-shaped appearance to the anterior atlas arch with a narrow gap in bw segments
Etiology ndashEmbryologic Traumatic ampor Vascular
Types ndashOrthotopicamp Dystopic
Instability is more common with dystopic type
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
Reduciblendashon flexion dorsal compression of the cord occurs
on extension ventral compression occurs secondary to increased angulation anteriorly
Irreduciblendashdue to displacement of TL ventral to the ossicle
Treatment
Reducible ndashOccipitocervical PF in neutral positionIrreducible ndashTransoral resection of the os odontoidremnant amp surrounding granulation tissue
Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Os odontoideum is defined as non-union of the dens with the axis body A transverse radiolucent cleft separates an ossicle of variable size from the axis body
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
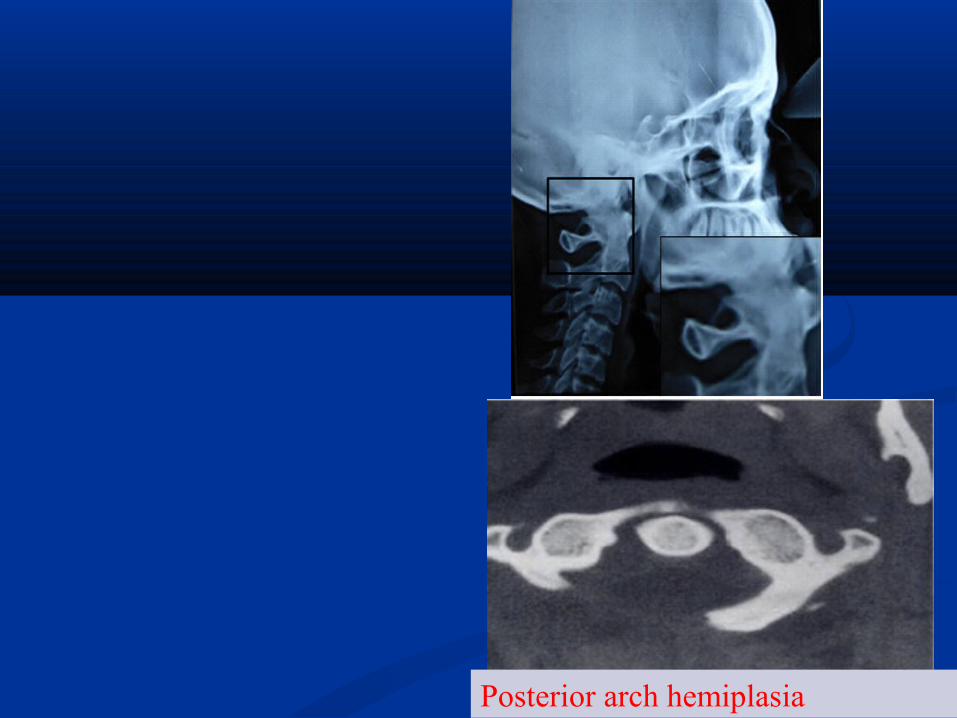
Os odontoideumOs odontoideum
OS ODONTOIDEUMOS ODONTOIDEUM Dens hypoplastic amp Dens hypoplastic amp
separate from ossicle by separate from ossicle by variable distancevariable distance
Incompetent cruciate Incompetent cruciate ligmt ligmt Unstable
Corticated smooth Corticated smooth roundround
FRACTUREFRACTURE Narrow gap between Narrow gap between
fractured fragmentsfractured fragments Fracture may lie caudal Fracture may lie caudal
to superior facetto superior facet Jagged edge no cortexJagged edge no cortex
Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Subluxation
Os odontoideum
Fracture
Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Atlanto-Axial Instability
bullA RotationalndashAround the dens
bullB TranslationalndashTranslation between C1ndashC2 where transverse lig is disrupted
bullC DistractionndashIndicating craniocervical dissociation
Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Non-traumatic conditions associated with increase in the atlanto axial distanceDown syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities (PsoriasisLupus)
On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

On the open mouth odontoid view the combined spread of the lateral masses of C1 greater than 69 mm would indicate rupture of the transverse ligamentAn atlantoaxial distance greater than 4-5 mm by lateral radiographs is indicative of AAI Posterior atlanto dental interval (PADI) Normal range is 19 ndash32 mm in male amp 19 ndash30mm in femalesBelow 19mm neurological manifestations occur
WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

WADIA CLASSIFICATION Group I AAD with occipitalization of atlas amp fusion of C2 amp C3Group II odontoid incompetence due to its maldevelopment with no occipitalization of atlasGroup III odontoid dislocation but no maldevelopment of dens or occipitalization of atlas
Incidence of AAD ndash
57 of all CVJ anomalies83 of all causes of cervical compression
ATLANTO-AXIAL DISLOCATION OR INSTABILITY
Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Posterior atlanto dental interval (PADI) measured from the posterior border of the dens to the anterior border of the posterior tubercle
This index may be more important because it more directly assesses the space available to the spinal cord
Normal range for the distance behind the dens is 19 ndash32 mm in male amp 19 ndash30mm in females
Below 19mm neurological manifestations occur
Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Rotatory displacement (Fielding and Hawkins classification)Type I is simple rotatory displacement with an intact transverse ligamentType II injuries involve anterior displacement of C1 on C2 of 3-5 mm with one lateral mass serving as a pivot point and a deficiency of the transverse ligamentType III injuries involve greater than 5 mm of anterior displacementType IV injuries involve the posterior displacement of C1 on C2
Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Type I injuries (stable subluxations) ndashCollar
Type II injuries may be potentially unstable
Type III and IV rotatory displacements that are unstable are treated surgically with a reduction and C1-2 fusion
Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Non-traumatic conditions associated with increase in the atlantoaxial distance
Down syndrome Due to laxity of the transverse ligament Grisel syndrome Atlantoaxial subluxation associated with inflammation of adjacent soft tissues of the neck Rheumatoid arthritisFrom laxity of the ligaments and destruction of the articular cartilage Osteogenesis imperfectaNeurofibromatosis Morquio syndrome Secondary to odontoid hypoplasia or aplasiaOther arthridities(PsoriasisLupus)
RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

RHEUMATOID ARTHRITIS amp CVJ
First described by Garrodin 189020 of the patients with RA have AAD
AAD is due to loss of tensile strength amp stretching of TL due to destructive inflammatory changes as well as secondary degenerative changes in tissues from vasculitis
Similar changes occur in the median amp lateral joints which result in erosive changes in adjacent bone amp formation of granulation tissue in the synovial joints
Odontoid process ndashosteoporosis angulation
OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

OCCIPITO-ATLANTAL INSTABILITY1048708Traumatic non traumatic
1048708Traumatic usually fatal 8 incidence in RTA1048708Seen with cardiorespiratory arrest quadriplegia loss of autonomic function VA insufficiency etc
1048708Traynelis classification1048708Type I anterior displacement of occiput on atlas1048708 Type II vertical displacement bw occiput amp cervical spine1048708Type III posterior displacement of occiput on atlas
TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

TRAUMATIC LESIONS OF CVJ
OF ATLASPosterior arch 23rdof all occur at the junction of posterior arch amp lateral mass (hyperextension injury)Anterior arch rareJefferson s burst of atlas 1st described by Geoffrey jefferson in 1920
Axial loading ndashdownward displacement of condyles with separation of lateral mass of C1Classically 4 part -2 each in ant amp post archneck pain amp stiffnessCervical collar Halo immobilizationNon union ndashocciputto C2 fusion
open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

open-mouth show lateral spine dispalcement of lateral masses of C1
CT scan of C1 shows fratures through anterior and posterior rings of C1
HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

HANGMANrsquoS ( TRAUMATIC SPONDYLOLISTHESIS OF AXIS )ldquoJudicial Hangingrdquo-submental knots causes dislocation of neural arch of axisToday majority due to RTA
Two basic mechanisms
Hyperextension amp distractionHyperextension amp compression
Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Type I are either non-displaced or have no angulationamp lt3mm of displacement (stable injury with uncommon neurological deficits)
Type II with significant angulationamp translation of anterior fragment
Type III with severe angulationamp displacement along with concomitant UL or BL facet dislocation
Neck pain but neurological deficits lessSurgical Rx seldom required due to high chances of spontaneous interbody fusion amp healingMost managed by reduction amp external immobilization
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
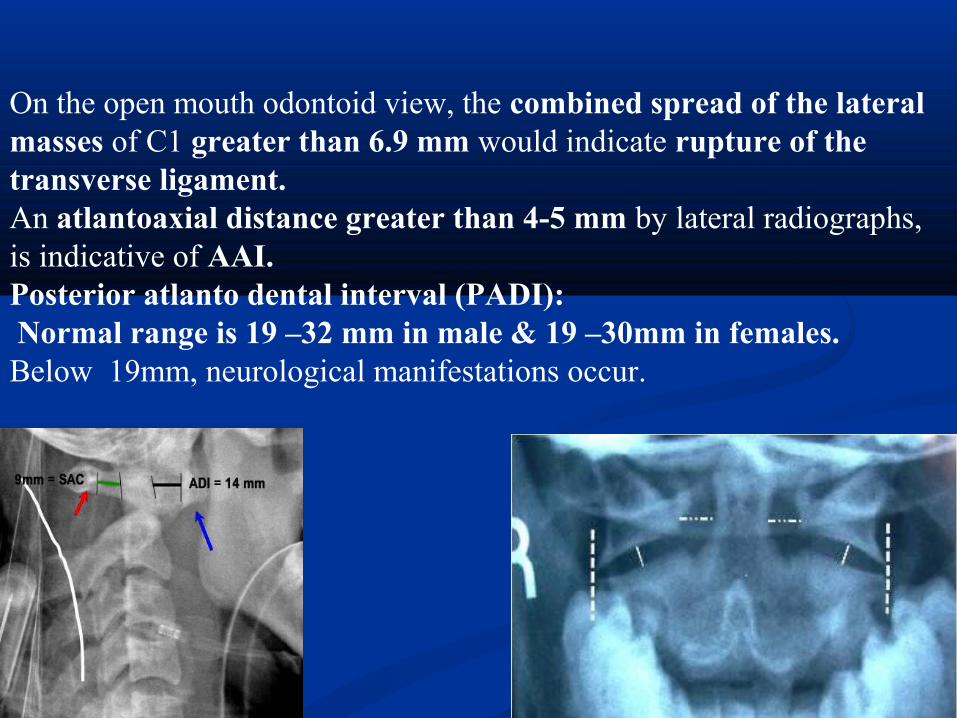
Radiographic features (best seen on lateral view)
1 Prevertebral soft tissue swelling2 Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament3 Anterior dislocation of the C2 vertebral body4 Bilateral C2 pars interarticularis fractures
Hangmans Fracture- through pars of c2
Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Hangmans Fracture
Traumatic spondylolisthesis of C2 Fractures of the lamina articular facets pedicles or pars interarticulares of C2 with disruption of C2-C3 junction
Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Axial CT image of the cervical spine at C2 level shows fractures of bilateral C2 pars interarticulares The fracture on the right extends to the transverse foramen where the right vertebral artery is located
ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ODONTOID Constitute about 7 ndash14 of cervical spine Flexion is the MC mechanism of injury causing anterior displacement of C1 on C2
Anderson amp DrsquoAlonzo classificationndashType I oblique avulsion through the upper part of the odontoid process at the point of alar ligament attachmentType II occur at the junction of the odontoid process amp the body of axisType III extend down in to the body of axis
ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ODONTOID
Type I are stable amp heal well if immobilised in a collar or brace
Type III are usually stable skull traction fb halo or brace for 3 ndash4 months results in fusion
Type II are prone to non union with a failure rate of 30 -60 with conservative measuresIndications for Sxndashdisplacement gt= 5mm nonunion age gt7 years disruption of the TLOdontoid compression screws (acute type II ) C1-2 arthrodesis(wiring fusion transarticular screws)
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU
CHIARI MALFORMATION
The Chiari malformations are a group of hindbrain herniation syndromes initially described by Austrian pathologist Hans Chiari in 1891
Types of Chiari malformations Type I Caudal descent of cerebellar tonsils in cervical spine Osseous anomalies of posterior skull base and spine
It presents in early adulthood rather than at birthAssociated with syringomyelia in 50 to 70
Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

Type II Caudal descent of cerebellar vermis and brain stem into cervical spine
Open spinal dysraphismHydrocephalusMultiple neuroaxis anomalies
Type III Craniocervical encephalocele containing portions of cerebellum and brain stem
HydrocephalusType IV (Controversial not commonly accepted as a Chiarimalformation)
Aplasiahypoplasia cerebellum
ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ARNOLD-CHIARI MALFORMATION I Present in adulthood =cerebellar tonsillar ectopia Herniation of cerebellar tonsils gt 5mm below a line connecting Basion with Opisthion (= foramen magnum)
Causesbull small posterior fossabullcerebellar overgrowthbulldisproportionate CSF absorptionAssociated with1 Syringohydromyelia (30-56)2 Hydrocephalus (25-44)3 Malformation of skull base
NECTEffaced Posterior Fossa cisterns Crowded Foramen Magnum Lateral3rd ventricles usually normal
ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ARNOLD-CHIARI MALFORMATION II
Radiography Lucken shadel -Craniolacunia = Lacunar Skull = mesenchymal dysplasia of calvarial ossificationAbsent Hypoplastic posterior arch of C1
Myelography Tethered cord
NECT Small posterior fossa Large funnel-shaped foramen magnum Scalloped petrous pyramid notched clivus Absent falx cerebelli
ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

ARNOLD-CHIARI MALFORMATION III
bull High cervical occipital meningoencephalocele + intracranial Chiari 2malformation
NECTo Occipital squamo defectPosterior spina bifida at the P1ndashP2 levelo Bony features of Chiari 2Small posterior cranial fossa scalloped clivus lacunar skullMR FindingsTIWI Sac contentsbull Meninges cerebellum plusmn brain stembull Cisterns 4th ventricle dural sinuses o HydrocephalusT2WI Tissues in sac may be bright (gliosis)MRV plusmn Veins in cephalocele
NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

NEOPLASMS OF CVJ
Unusual Metastatic malignancies such as carcinoma of the breast lung prostate kidney and thyroid in adults
and neuroblastoma Ewingrsquos tumor leukemia hepatoma and retinoblastoma in children are most commonPrimary malignancies involving the craniocervical junction are rare(multiple myeloma)
Benign tumors are very rare
THANK YOUTHANK YOU

THANK YOUTHANK YOU


















