
Alternative puncture site for implantable permanent haemodialysis ...
3
Nephrol Dial Transplant (1996) 11: 2293-2295 Technical Note Nephrology Dialysis Transplantation Alternative puncture site for implantable permanent haemodialysis catheters R. Apsner, G. Sunder-Plassmann, M. Muhm and W. Druml Klinische Abteilung fiir Nephrologie und Dialyse, Universitatsklinik ftir Innere Medizin III, Universitat Wien, Vienna, Austria Abstract Background. Vascular access represents a major prob- lem in long-term haemodialysis patients. In patients without patent internal arteriovenous fistula, the implantation of cuffed catheters to provide a temporary or permanent central venous access is often necessary. Catheterization of the subclavian vein should be avoided because of the high risk of stenosis or throm- bosis. The puncture of the internal jugular vein can be impossible in cases with stenosis or thrombosis due to previous catheterization. To overcome these limitations we evaluated an alternative puncture site for implant- ation of permanent central venous catheters. Methods. The very low, most central jugular approach, first described by Rao et al, with the site of puncture just above the medial notch of the clavicle, was used to introduce Dacron cuffed dialysis catheters into the innominate vein in four chronic dialysis patients with impeded conventional vascular access. Results. In all four patients puncture of the internal jugular vein using Rao's technique was successful at the first attempt. All four catheters were introduced without any problems. Even in a case with thrombosis of the internal jugular vein and the ipsilateral subcla- vian vein, this technique was successfully applied. No complications such as haematoma, pneumothorax, or catheter-associated infection were observed. The cath- eters remained in situ for 2-12 months with excellent blood flow and without clinical evidence of venous stenosis or thrombosis. Conclusions. In case of failure to cannulate the internal jugular vein by a conventional approach, the technique of Rao et al. can be used before sacrificing the subcla- vian vein or changing to exotic techniques such as translumbar, transfemoral or transhepatic methods. Key words: haemodialysis; permanent central venous catheter Correspondence and offprint requests to: Robert Apsner MD, Klinische Abteilung fiir Nephrologie und Dialyse, Universitatsklinik fur Innere Medizin III, Universitat Wien, Vienna, Austria. Introduction Internal arteriovenous fistulae and grafts represent the preferred vascular access in long-term haemodialysis patients. For many reasons (e.g. thrombosis or matura- tion of the fistula) temporary or permanent central venous access with a cuffed catheter may be required for dialysis treatment [1-4]. Because of the high incid- ence of stenosis and/or thrombosis after cannulation of the subclavian vein, which can compromise the patency of an ipsilateral endogenous fistula or graft, the internal jugular vein is considered as the site of first choice for implantation of a central venous access in haemodialysis patients [5-11]. Several studies con- cerning puncture sites of the internal jugular vein have been published using either the central, the anterior, or the posterior approach (for review see [12]). However, puncture of the internal jugular vein may not be feasible because of stenosis or total thrombosis due to previous cannulation or haematoma after arter- ial puncture. Another problem associated with the conventional jugular access can be low blood flow because of kinking of the catheter. In contrast to the above-mentioned classical punc- ture sites of the internal jugular vein, Rao et al. [13] described the most central approach to this vessel at its confluence with the subclavian vein. This technique has several advantages compared to the conventional jugular puncture. The landmark of this approach is the notch located just above the medial end of the clavicle. This notch can be easily identified, even in obese patients, and the vessel is punctured at the site of the largest diameter. The success rate is reported to be about 99% [13]. The catheter enters the vessel in a smooth curve so that kinking is almost impossible (Figure 1). The complication rate reported by Rao et al. is low compared to the conventional jugular and subclavian access, which is probably due to the ease and reliability of identifying the constant bony land- mark. Furthermore, this technique can be successfully applied even in patients with thrombosis or stenosis of the proximal internal jugular vein. In four patients with a complicated conventional S 1996 European Renal Association-European Dialysis and Transplant Association Downloaded from https://academic.oup.com/ndt/article-abstract/11/11/2293/1901353 by guest on 30 January 2018
Transcript of Alternative puncture site for implantable permanent haemodialysis ...
Nephrol Dial Transplant (1996) 11: 2293-2295
Technical Note
NephrologyDialysis
Transplantation
Alternative puncture site for implantable permanenthaemodialysis catheters
R. Apsner, G. Sunder-Plassmann, M. Muhm and W. Druml
Klinische Abteilung fiir Nephrologie und Dialyse, Universitatsklinik ftir Innere Medizin III, Universitat Wien, Vienna,Austria
AbstractBackground. Vascular access represents a major prob-lem in long-term haemodialysis patients. In patientswithout patent internal arteriovenous fistula, theimplantation of cuffed catheters to provide a temporaryor permanent central venous access is often necessary.Catheterization of the subclavian vein should beavoided because of the high risk of stenosis or throm-bosis. The puncture of the internal jugular vein can beimpossible in cases with stenosis or thrombosis due toprevious catheterization. To overcome these limitationswe evaluated an alternative puncture site for implant-ation of permanent central venous catheters.Methods. The very low, most central jugular approach,first described by Rao et al, with the site of puncturejust above the medial notch of the clavicle, was usedto introduce Dacron cuffed dialysis catheters into theinnominate vein in four chronic dialysis patients withimpeded conventional vascular access.Results. In all four patients puncture of the internaljugular vein using Rao's technique was successful atthe first attempt. All four catheters were introducedwithout any problems. Even in a case with thrombosisof the internal jugular vein and the ipsilateral subcla-vian vein, this technique was successfully applied. Nocomplications such as haematoma, pneumothorax, orcatheter-associated infection were observed. The cath-eters remained in situ for 2-12 months with excellentblood flow and without clinical evidence of venousstenosis or thrombosis.
Conclusions. In case of failure to cannulate the internaljugular vein by a conventional approach, the techniqueof Rao et al. can be used before sacrificing the subcla-vian vein or changing to exotic techniques such astranslumbar, transfemoral or transhepatic methods.
Key words: haemodialysis; permanent central venouscatheter
Correspondence and offprint requests to: Robert Apsner MD,Klinische Abteilung fiir Nephrologie und Dialyse, Universitatsklinikfur Innere Medizin III, Universitat Wien, Vienna, Austria.
Introduction
Internal arteriovenous fistulae and grafts represent thepreferred vascular access in long-term haemodialysispatients. For many reasons (e.g. thrombosis or matura-tion of the fistula) temporary or permanent centralvenous access with a cuffed catheter may be requiredfor dialysis treatment [1-4]. Because of the high incid-ence of stenosis and/or thrombosis after cannulationof the subclavian vein, which can compromise thepatency of an ipsilateral endogenous fistula or graft,the internal jugular vein is considered as the site offirst choice for implantation of a central venous accessin haemodialysis patients [5-11]. Several studies con-cerning puncture sites of the internal jugular vein havebeen published using either the central, the anterior,or the posterior approach (for review see [12]).However, puncture of the internal jugular vein maynot be feasible because of stenosis or total thrombosisdue to previous cannulation or haematoma after arter-ial puncture. Another problem associated with theconventional jugular access can be low blood flowbecause of kinking of the catheter.
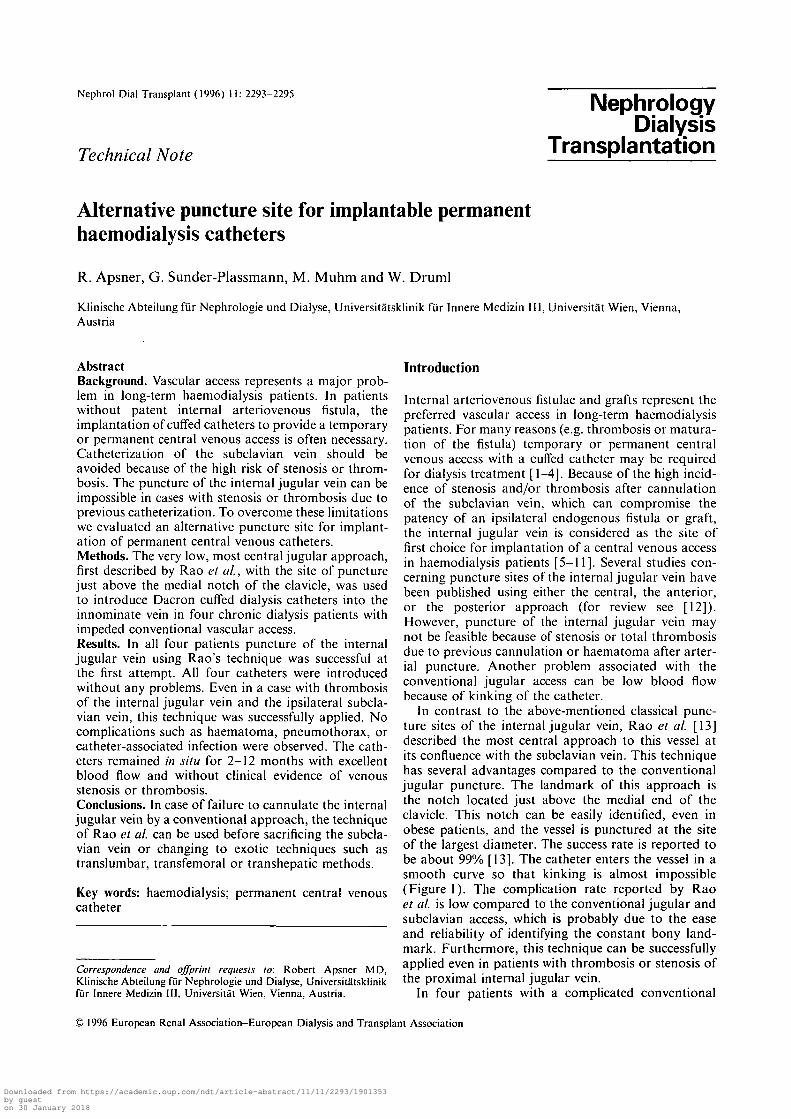
In contrast to the above-mentioned classical punc-ture sites of the internal jugular vein, Rao et al. [13]described the most central approach to this vessel atits confluence with the subclavian vein. This techniquehas several advantages compared to the conventionaljugular puncture. The landmark of this approach isthe notch located just above the medial end of theclavicle. This notch can be easily identified, even inobese patients, and the vessel is punctured at the siteof the largest diameter. The success rate is reported tobe about 99% [13]. The catheter enters the vessel in asmooth curve so that kinking is almost impossible(Figure 1). The complication rate reported by Raoet al. is low compared to the conventional jugular andsubclavian access, which is probably due to the easeand reliability of identifying the constant bony land-mark. Furthermore, this technique can be successfullyapplied even in patients with thrombosis or stenosis ofthe proximal internal jugular vein.
In four patients with a complicated conventional
S 1996 European Renal Association-European Dialysis and Transplant Association
Downloaded from https://academic.oup.com/ndt/article-abstract/11/11/2293/1901353by gueston 30 January 2018
2294 R. Aspner et al.
Fig. 1. Chest X-ray showing a permanent dialysis catheter intro-duced according to Rao's technique
vascular access, permanent Dacron cuffed haemodia-lysis catheters were introduced using the methoddescribed above after previous attempts of insertion atconventional sites had failed.
Subjects and methods
Puncture technique
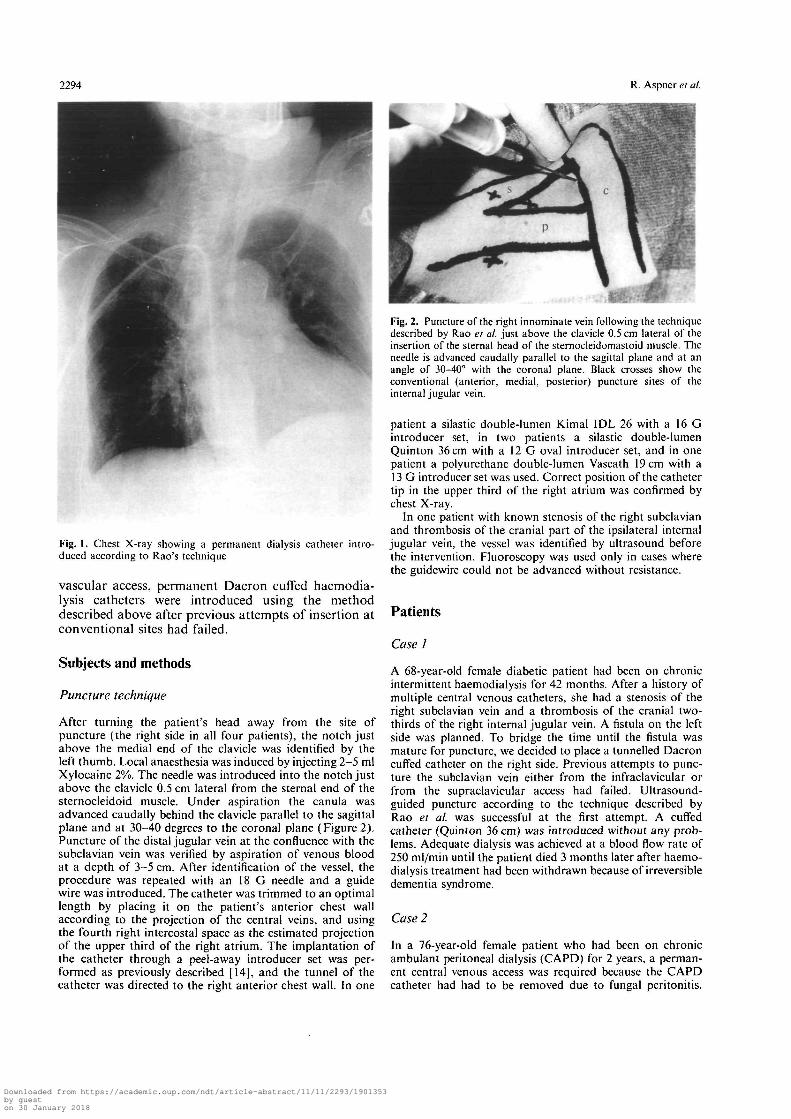
After turning the patient's head away from the site ofpuncture (the right side in all four patients), the notch justabove the medial end of the clavicle was identified by theleft thumb. Local anaesthesia was induced by injecting 2-5 mlXylocaine 2%. The needle was introduced into the notch justabove the clavicle 0.5 cm lateral from the sternal end of thesternocleidoid muscle. Under aspiration the canula wasadvanced caudally behind the clavicle parallel to the sagittalplane and at 30-40 degrees to the coronal plane (Figure 2).Puncture of the distal jugular vein at the confluence with thesubclavian vein was verified by aspiration of venous bloodat a depth of 3-5 cm. After identification of the vessel, theprocedure was repeated with an 18 G needle and a guidewire was introduced. The catheter was trimmed to an optimallength by placing it on the patient's anterior chest wallaccording to the projection of the central veins, and usingthe fourth right intercostal space as the estimated projectionof the upper third of the right atrium. The implantation ofthe catheter through a peel-away introducer set was per-formed as previously described [14], and the tunnel of thecatheter was directed to the right anterior chest wall. In one
Fig. 2. Puncture of the right innominate vein following the techniquedescribed by Rao et al. just above the clavicle 0.5 cm lateral of theinsertion of the sternal head of the sternocleidomastoid muscle. Theneedle is advanced caudally parallel to the sagittal plane and at anangle of 30-40° with the coronal plane. Black crosses show theconventional (anterior, medial, posterior) puncture sites of theinternal jugular vein.
patient a silastic double-lumen Kimal IDL 26 with a 16 Gintroducer set, in two patients a silastic double-lumenQuinton 36 cm with a 12 G oval introducer set, and in onepatient a polyurethane double-lumen Vascath 19 cm with a13 G introducer set was used. Correct position of the cathetertip in the upper third of the right atrium was confirmed bychest X-ray.
In one patient with known stenosis of the right subclavianand thrombosis of the cranial part of the ipsilateral internaljugular vein, the vessel was identified by ultrasound beforethe intervention. Fluoroscopy was used only in cases wherethe guidewire could not be advanced without resistance.
Patients
Case 1
A 68-year-old female diabetic patient had been on chronicintermittent haemodialysis for 42 months. After a history ofmultiple central venous catheters, she had a stenosis of theright subclavian vein and a thrombosis of the cranial two-thirds of the right internal jugular vein. A fistula on the leftside was planned. To bridge the time until the fistula wasmature for puncture, we decided to place a tunnelled Dacroncuffed catheter on the right side. Previous attempts to punc-ture the subclavian vein either from the infraclavicular orfrom the supraclavicular access had failed. Ultrasound-guided puncture according to the technique described byRao et al. was successful at the first attempt. A cuffedcatheter (Quinton 36 cm) was introduced without any prob-lems. Adequate dialysis was achieved at a blood flow rate of250 ml/min until the patient died 3 months later after haemo-dialysis treatment had been withdrawn because of irreversibledementia syndrome.
Case 2
In a 76-year-old female patient who had been on chronicambulant peritoneal dialysis (CAPD) for 2 years, a perman-ent central venous access was required because the CAPDcatheter had had to be removed due to fungal peritonitis.
Downloaded from https://academic.oup.com/ndt/article-abstract/11/11/2293/1901353by gueston 30 January 2018

Permanent haemodialysis catheters
Placement from the left jugular and subclavian vein failedbecause the guide wire could not be advanced into thesuperior vena cava despite fluoroscopic guidance. Two dayslater another attempt through the right subclavian vein (fromthe supraclavicular and infraclavicular approach) failed forthe same reason. Failure was probably due to an abnormalintrathoracal course of the central vessels caused by pleuraladhesions and severe kyphoskoliosis. Puncture at the sitedescribed by Rao et al. was successfull at the first attempt.The guide wire and the cuffed catheter (Quinton 36 cm)could be advanced without difficulty. Dialysis was performedat a blood flow rate of 250 ml/min without complicationsuntil the catheter was removed 2 months later when CAPDwas restarted.
Case 3
A 63-year-old male patient suffering from diabetic nephro-pathy and severe atherosclerosis required dialysis treatment.Previous attempts to create an internal fistula had failed.Implantation of a permanent dialysis catheter into the rightjugular vein was scheduled. Following accidental punctureof the carotid artery, a haematoma developed and thepuncture site was shifted to the very low jugular access.Puncture was at once successful. The catheter (Kimal IDL26) was introduced following standard procedures.Uncomplicated dialysis has now been performed for 12months at a blood flow rate of 280 ml/min.
Case 4
A 40-year-old female patient who had recieved a renalallograft 4 years ago had to restart dialysis treatment becauseof transplant failure. Since the creation of an internal fistulahad been scheduled on the left side, the right side was chosenfor insertion of a permanent dialysis catheter. At the rightjugular and subclavian region, there were multiple scars fromprevious permanent catheters and the patient reported thatplacement of central venous catheters on this side had oftenfailed. Puncture according to Rao et al. was successful andthe catheter (Vascath 19 cm) was introduced without com-plication. Dialysis has been now performed for 2 monthswith a blood flow rate of 250 ml/min.
Discussion
Our data show that the most central jugular access asfirst described by Rao et al.[13] represents a promisingtechnique for placement of tunnelled Dacron cuffedcatheters in haemodialysis patients with compromisedconventional vascular access. Even in patients withstenosis of the jugular vein and the ipsilateral subcla-vian vein (case 1), introduction of a permanent dialysiscatheter was possible. Because of the straight line tothe right atrium, the guide wire could be advancedeasily, even in the presence of intrathoracal abnormalit-ies (case 2). In case of thrombosis or haematoma (case3) the very low jugular access is feasible and allowspreservation of the subclavian vein for arteriovenousfistulae and grafts. In our small series of permanenthaemodialysis catheters introduced according to thetechnique described by Rao et al., neither puncture-associated nor long-term complications were observed.The complication rate for insertion of infusion lines in
2295
the original paper of Rao et al. was very low. In aseries of 376 paediatric and adult patients, one pneumo-thorax, three accidental arterial punctures, and twoaccidental punctures of the thoracic duct (from the leftside), all without clinical relevance, have been described[13]. However, ultrasound-guided cannulation isrecommended for less experienced physicians and theleft side should be avoided because of the danger ofchylothorax due to accidental puncture of the thoracicduct. We believe that this method is applicable forpatients with difficult vascular anatomy and should beused prior to 'exotic' techniques such as transfemoral,transhepatic, or translumbar access [15-18].
References
1. Pourchez Th, Moriniere Ph, Fournier A. Pietri J. Use ofPermcath (Quinton) catheter in uremic patients in whom thecreation of conventional vascular access for hemodialysis isdifficult. Nephron 1989: 53: 297-302
2. Swartz RD, Messana JM, Boyer CJ, Lunde NM, Weitzel WF,Hartman TL. Successful use of cuffed central venous hemodia-lysis catheters inserted percutanously. J Am Soc Nephrol 1993;4: 1719-1725
3. Shusterman NH, Kloss K, Mullen JL. Successful use of double-lumen, silicone rubber catheters for permanent hemodialysisaccess. Kidney Int 1989; 35: 887-890
4. McDowel DE, Moss AH, Vasilakis C, Pillai L. Percutanouslyplaced dual-lumen silicone catheters for long-term hemodialysis.Am Surg 1993; 59: 569-573
5. Bander SJ, Schwab SJ. Central venous angioaccess for hemodia-lysis and its complications. Semin Dial 1992; 5: 121-128
6. Barrett N. Spencer S, Mclvor J, Brown EA. Subclavian stenosis:a major complication of subclavian dialysis catheters. NephrolDial Transplant 1988; 3: 423-425
7. Schillinger F, Schillinger D, Montagnac R, Milcent T. Postcatheterization vein stenosis in haemodialysis: comparative angi-ographic study of 50 subclavian and 50 internal jugular accesses.Nephrol Dial transplant 1991; 6: 722-724
8. Schwab SJ, Quarles LD, Middleton JP, Cohan R, Saeed M,Dennis VW. Hemodialysis-associated subclavian vein stenosisKidney Int 1988; 33: 1156-1159
9. Chimochowski GE, Worley E, Rutherford WE, Sartain j ,Blondin J, Harter H. Superiority of the internal jugular over thesubclavian access for temporary dialysis. Nephron 1990; 54:154-161
10. Uldall R. Subclavian cannulation is no longer nessessary orjustified in patients with end-stage renal failure. Semin Dial1994; 7: 161-164
11. (Conner K. Subclavian haemodialysis access: is it still justifiedin 1995. Nephrol Dial Transplant 1995; 11: 1988-1991
12. Rosen M, Latto P, Ng S. Handbook of percutaneous centralvenous catheterisation. Saunders, London, 1992; 115-170
13. Rao TL, Wong A, Salem MR. A new approach to percutaneouscatheterisation of the internal jugular vein. Anesthesiology 1977;46: 362-364
14. Cohen AM, Wood WC. Simplified technique for placement oflong term central venous silicone catheters. Surg Gynecol Obstet1982; 154: 721-724
15. Weitzel WF, Boyer CJ, El-Khatib MT, Swartz RD. Successfuluse of indwelling cuffed femoral vein catheters in ambulatoryhemodialysis patients. Am J Kidney Dis 1993; 22: 426-429
16. Po CL. Koolpe HA, Allen S, Alvez LD, Raja RM. TranshepaticPermCath for hemodialysis. Am J Kidney Dis 1994; 24: 590-591
17. Lund G, Trerotola SO, Scheel PJ. Percutaneous translumbarinferior vena cava cannulation for hemodialysis. Am J KidneyDis 1995; 25: 732-737
18. Gupta A, Karak PK., Daddekni S. Translumbar inferior venacava catheter for long-term hemodialysis. J Am Soc Nephrol1995; 5: 2094-2097
Received for publication: 27.3.96Accepted in revised form: 18.6.96
Downloaded from https://academic.oup.com/ndt/article-abstract/11/11/2293/1901353by gueston 30 January 2018


















