ALS And ICE Bucket Challenge Under supervise of : Dr. Hassan Darami Faris Alosaimi “435031635”...
28
ALS And ICE Bucket Challenge Under supervise of : Dr. Hassan Darami Faris Alosaimi “435031635” Salim Alhakami “435031615 ” Yasser Aleliwi “435032849” Mohammed Almakdob “435031639 ” Abdulrahman Badr Alwallan “435031645 ”
-
Upload
mae-gardner -
Category
Documents
-
view
218 -
download
0
Transcript of ALS And ICE Bucket Challenge Under supervise of : Dr. Hassan Darami Faris Alosaimi “435031635”...

ALS And ICE Bucket Challenge
Under supervise of: Dr. Hassan Darami
Faris Alosaimi “435031635” Salim Alhakami “435031615”
Yasser Aleliwi “435032849” Mohammed Almakdob “435031639”
Abdulrahman Badr Alwallan “435031645”
ALS And
ICE Bucket Challenge
What is ALS?
• Amyotrophic lateral sclerosis (ALS) "Lou Gehrig's Disease," is a progressive neurodegenerative disease that affects nerve cells in the brain and the spinal cord.• Motor neurons reach from the brain to the spinal cord and from the
spinal cord to the muscles throughout the body. The progressive degeneration of the motor neurons in ALS eventually leads to their death. When the motor neurons die, the ability of the brain to initiate and control muscle movement is lost. With voluntary muscle action progressively affected, patients in the later stages of the disease may become totally paralyzed.
Sign and Symptoms of ALS
• The initial clinical manifestation of ALS may occur in any body segment (bulbar, cervical, thoracic or lumbosacral) and may manifest as upper motor neuron or lower motor neuron symptoms or signs.
Upper motor neuron symptoms
• Loss of upper motor neurons (UMNs) results in slowness of movement, incoordination and stiffness with relatively little overt weakness. Arm or hand UMN symptoms include poor dexterity with resulting difficulty performing activities of daily living. Leg UMN symptoms manifest as a spastic gait with poor balance and may include spontaneous leg flexor spasms and ankle clonus.
Lower motor neuron symptoms
•Loss of LMNs results in weakness, usually accompanied by atrophy and fasciculations. Cramps are also common.
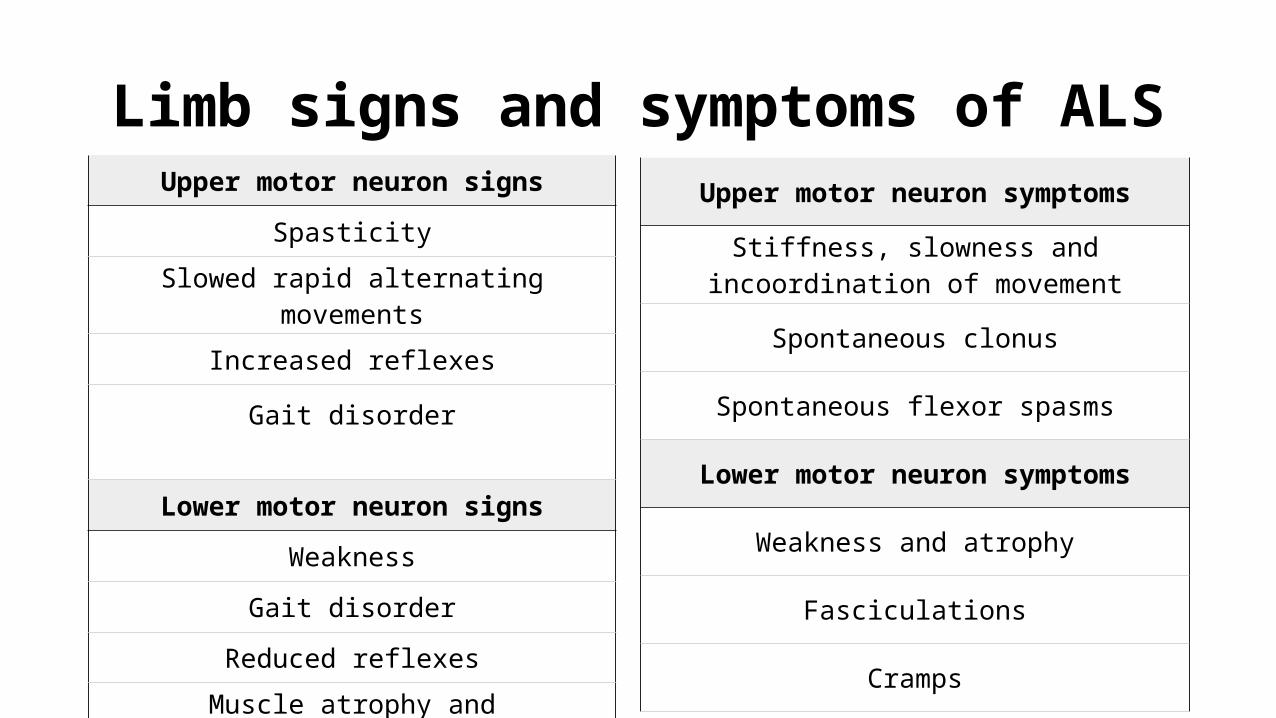
Limb signs and symptoms of ALS
Upper motor neuron signs
Spasticity
Slowed rapid alternating movements
Increased reflexes
Gait disorder
Lower motor neuron signs
Weakness
Gait disorder
Reduced reflexes
Muscle atrophy and fasciculations
Upper motor neuron symptoms
Stiffness, slowness and incoordination of movement
Spontaneous clonus
Spontaneous flexor spasms
Lower motor neuron symptoms
Weakness and atrophy
Fasciculations
Cramps
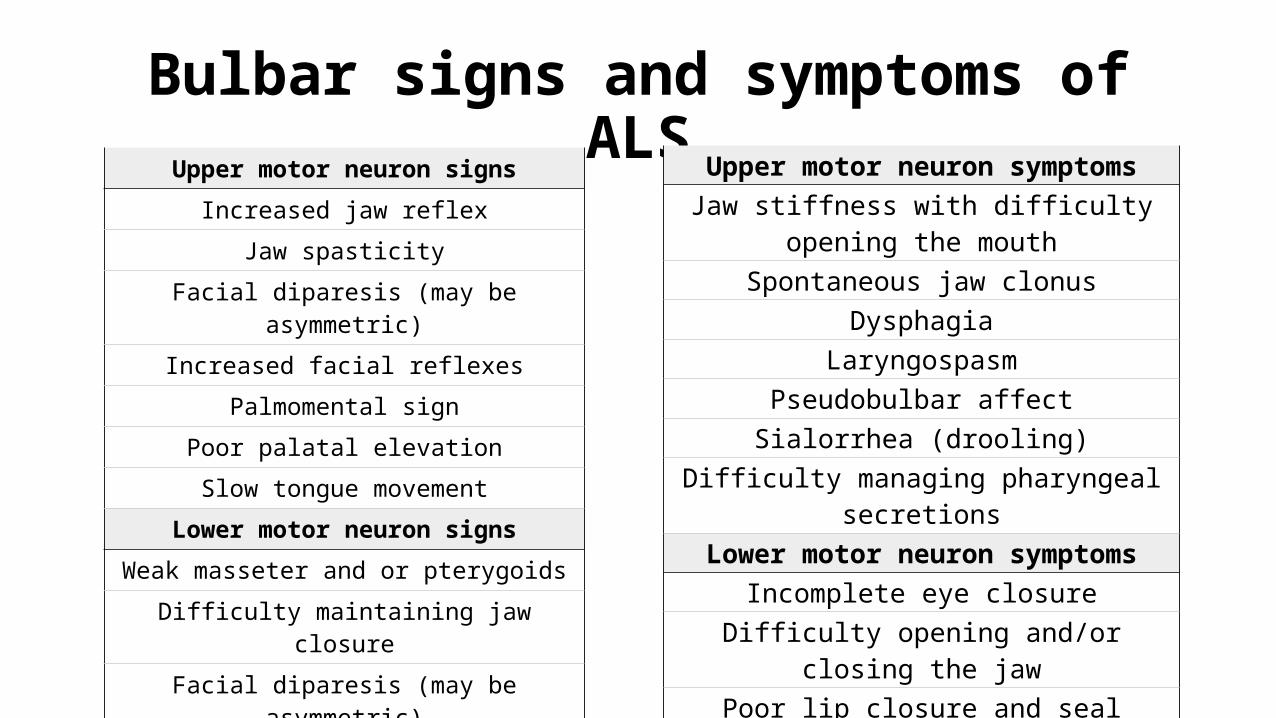
Bulbar signs and symptoms of ALSUpper motor neuron signs
Increased jaw reflexJaw spasticity
Facial diparesis (may be asymmetric)
Increased facial reflexesPalmomental sign
Poor palatal elevationSlow tongue movement
Lower motor neuron signsWeak masseter and or pterygoidsDifficulty maintaining jaw closure
Facial diparesis (may be asymmetric)
Poor palatal elevationTongue weakness
Muscle atrophy and fasciculations
Upper motor neuron symptomsJaw stiffness with difficulty opening the mouth
Spontaneous jaw clonusDysphagia
LaryngospasmPseudobulbar affectSialorrhea (drooling)
Difficulty managing pharyngeal secretionsLower motor neuron symptoms
Incomplete eye closureDifficulty opening and/or closing the jaw
Poor lip closure and sealDysarthria
Slurred, nasal and/or hoarse speechHoarseness
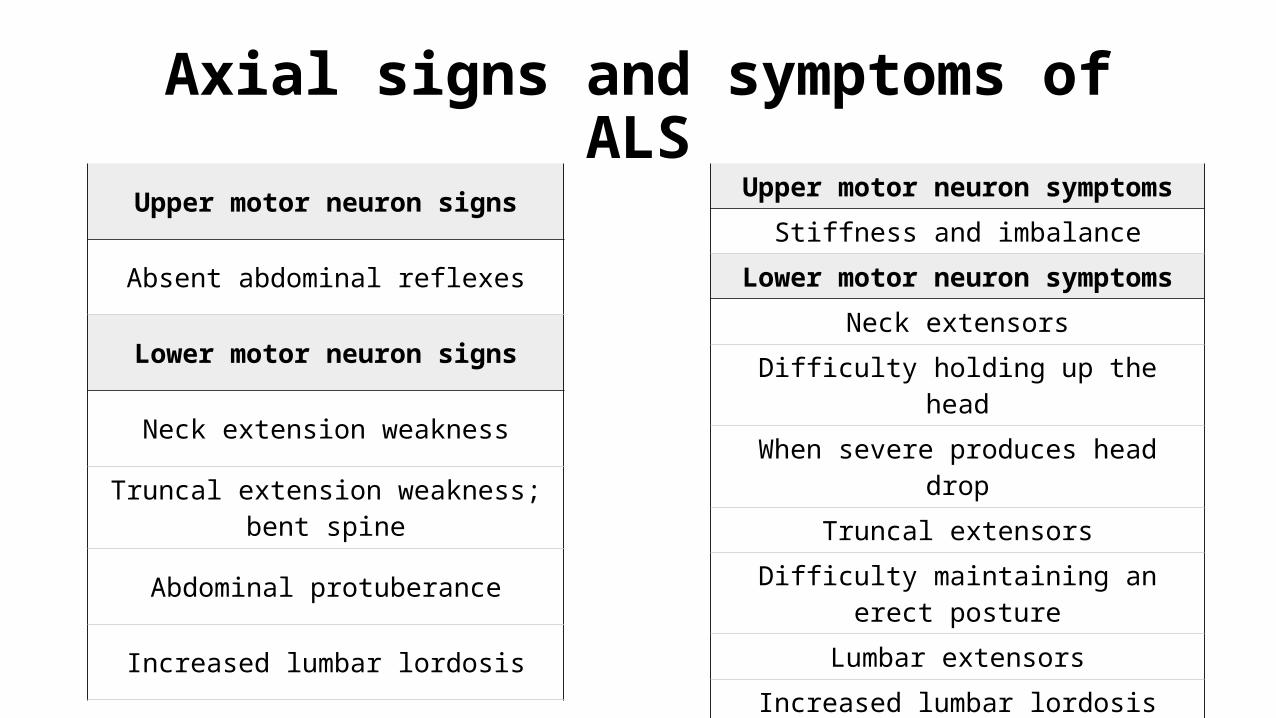
Axial signs and symptoms of ALS
Upper motor neuron signs
Absent abdominal reflexes
Lower motor neuron signs
Neck extension weakness
Truncal extension weakness; bent spine
Abdominal protuberance
Increased lumbar lordosis
Upper motor neuron symptomsStiffness and imbalance
Lower motor neuron symptomsNeck extensors
Difficulty holding up the headWhen severe produces head drop
Truncal extensorsDifficulty maintaining an erect posture
Lumbar extensorsIncreased lumbar lordosisAbdominal wall musclesAbdominal protuberance
Cramps
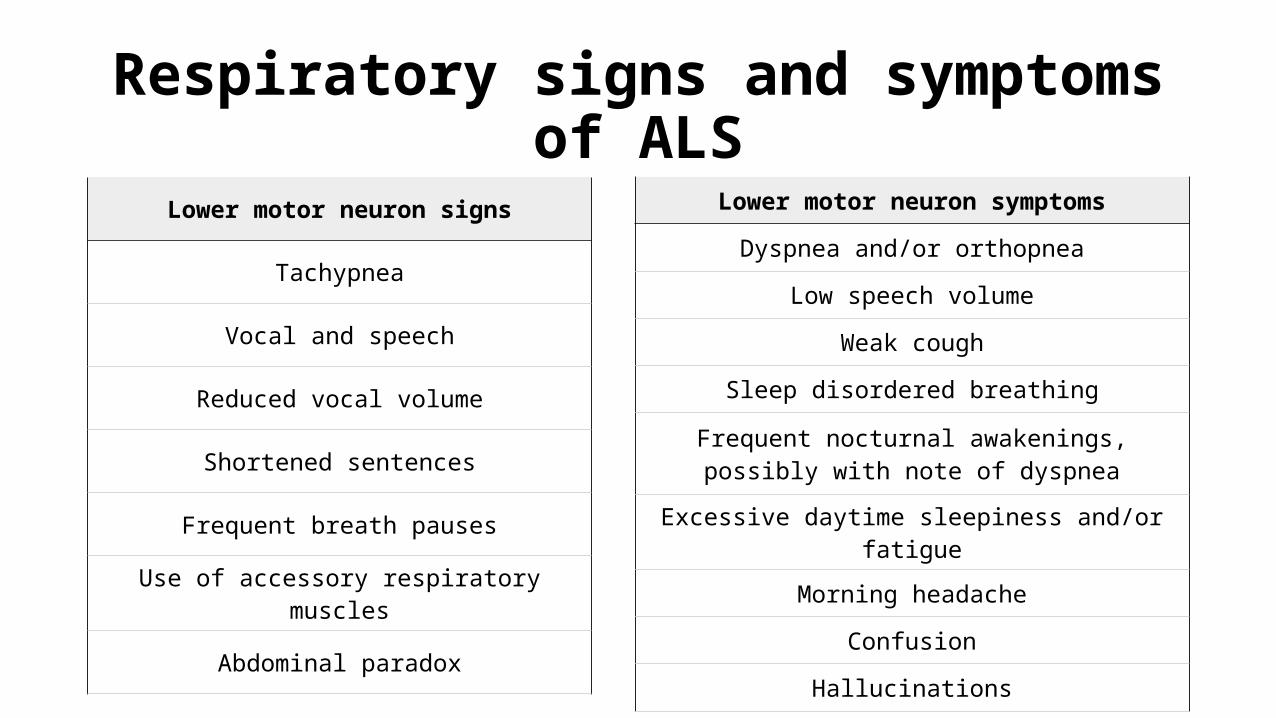
Respiratory signs and symptoms of ALS
Lower motor neuron signs
Tachypnea
Vocal and speech
Reduced vocal volume
Shortened sentences
Frequent breath pauses
Use of accessory respiratory muscles
Abdominal paradox
Lower motor neuron symptoms
Dyspnea and/or orthopnea
Low speech volume
Weak cough
Sleep disordered breathing
Frequent nocturnal awakenings, possibly with note of dyspnea
Excessive daytime sleepiness and/or fatigue
Morning headache
Confusion
Hallucinations
Probable Causes of ALSFree radicals
The inherited form of ALS often involves a mutation in a gene responsible for producing a strong antioxidant enzyme that protects your cells from damage caused by free radicals — the byproducts of oxygen metabolism
GlutamatePeople who have ALS typically have higher than normal levels of glutamate, a chemical messenger in the brain, in their spinal fluid. Too much glutamate is known to be toxic to some nerve cells
Protein mishandling Mishandled proteins within the nerve cells may lead to a gradual accumulation of abnormal forms of these proteins in the cells, eventually causing the nerve cells to die.
Probable Causes of ALS
Autoimmune responsesSometimes, a person's immune system begins attacking some of his or her body's own normal cells, and scientists have speculated that such antibodies may trigger the process that results in ALS. Thus ALS is not contagious.
Pathogenesis
current hypotheses include:SOD1 mutation
similarities between sporadic and familial ALS suggest relationship to SOD1mutation may cause toxic gain of function of SOD1 enzyme leading to
generation of free radicals, cell injury, and cell deathglutamate-induced excitotoxicity results in activation of calcium-
dependent enzyme pathways leading to increased neuronal destruction
TDP-43 (also called TARDBP) is major component of cytoplasmic protein aggregates (including ubiquitin) in patients with sporadic ALS
Pathogenesis
pathologic features of ALS on histological exam:degree of loss of both of neuronal systems including:
large motor neurons of anterior horn cells of spinal cord and motor nuclei of brainstem (motor nuclei of cranial nerves V, VII, IX, X [somatic], XII)
large pyramidal neurons of motor cortex and/or large myelinated axons of corticospinal tracts
cellular pathologic changes in involved areas:neuronal atrophy with relative increase in lipofuscin and loss of Nissl substanceevidence should be seen of different stages of process of neuronal degeneration
including normal-appearing neuronsevidence of degeneration of corticospinal tracts at same level
Pathogenesis
other histologic findings commonly found include:lack of pathologic change in motor neurons of cranial nerves III, IV, VI, the
intermediolateral column of spinal cord, or Onuf's nucleus in sacral region of cord.occurrence of ≥ 1 of the following cellular pathologic changes in large motor
neurons of anterior horn cells of spinal cord and motor nuclei of brainstem, and large pyramidal neurons of motor cortex and/or large myelinated axons of corticospinal tracts:
ubiquitinated intracytoplasmic inclusions in motor neurons (skeins, Lewy body-like structures)Bunina bodies (cystatin C-containing inclusion found in cell bodies of motor neurons in
patients withALS)aggregates of neurofilaments in perikarya of motor neurons (hyaline conglomerate inclusions)axonal spheroids with accumulation of masses of neurofilaments and Wallerian-like
degeneration in anterior roots
DiagnosisThere is no specific test that can diagnose the disease as known , but that affected the upper and lower motor neuron in one party is likely to strongly signs of disease. Therefore, the diagnosis depends primarily on the signs and symptoms observed by the physician to the patient and a series of tests to rule out other diseases.
Because the symptoms of this disease are similar to the symptoms of many other diseases
of these experiments is to draw electrical muscle, There is another famous test that measures the speed of nerve conduction valuable
Differential Diagnosis:•
Multifocal motor neuropathy with conduction block
Cervical spondylotic myelopathy with polyradiculopathy
Spinal stenosis with compression of lumbosacral nerve roots
Chronic inflammatory demyelinating polyneuropathy with
central nervous system lesions
Syringomyelia
Syringobulbia
Differential Diagnosis:Foramen magnum tumorMeningeal carcinomatosis Spinal muscular atrophy Polyglucosan body disease Bulbospinal muscular atrophy (Kennedy disease)Monomelic amyotrophy ALS-like syndromes have been reported in the setting of lead intoxication, HIV,
hyperparathyroidism, hyperthyroidism, lymphoma, and vitamin B 12 deficiency.
Management
Nonpharmacologic Therapy Noninvasive positive-pressure ventilation may increase tracheostomy-
free survival in patients with respiratory difficulty (defined by orthopnea or FVC 50% of predicted may improve quality of life).
Percutaneous endoscopic gastrostomy (PEG) tube placement improves nutritional intake, promotes weight stabilization, and eases medication ADMINISTRATION. Some studies suggest PEG placement may prolong life 1 to 4 mo, particularly when placed before FVC falls to ≤50% of predicted value.
Nutrition, speech therapy, physical and occupational therapy services.
Suction device for sialorrhea.
drugs to treat this disease:
The Food and Drug Administration (FDA) approved the first drug to treat the disease: Riluzole (Rilutik). It is believed that Rilozul limits of motor neuron damage by reducing the secretion of glutamate through activation of glutamate carriers. In addition, many other effects garrison nerve offers by closing sodium channels and calcium channel stoppers, inhibition of protein kinase C, and stimulate the receptors prone to substance NMDA. Clinical trials of the drug on patients Rilozul proved that prolongs survival for several months, and could have a greater benefit for the survival of patients with bulbar beginning. Property lengthen the time before a patient needs a respirator.
HISTORY OF ALS
Jean- Marie Charcot (1825-1893) noted the first research of the character of ALS in 1874, and name the fatal syndrome based on what he found. He was a noted French neurologist who called “the Father of Neurology”, and .explained nervous system works
Famous People with ALS Disease
Henry Louis "Lou Gehrig" was an American baseball
first baseman who played 17 seasons in Major League
Baseball (MLB) for the New York Yankees (1923–1939).
Stephen William Hawking is an English theoretical physicist,
cosmologist, author and Director of Research at the
Centre for Theoretical Cosmology within the
University of Cambridge.
Mao Zedong was a Chinese Communist
revolutionary and the founding father of the
People's Republic of China.
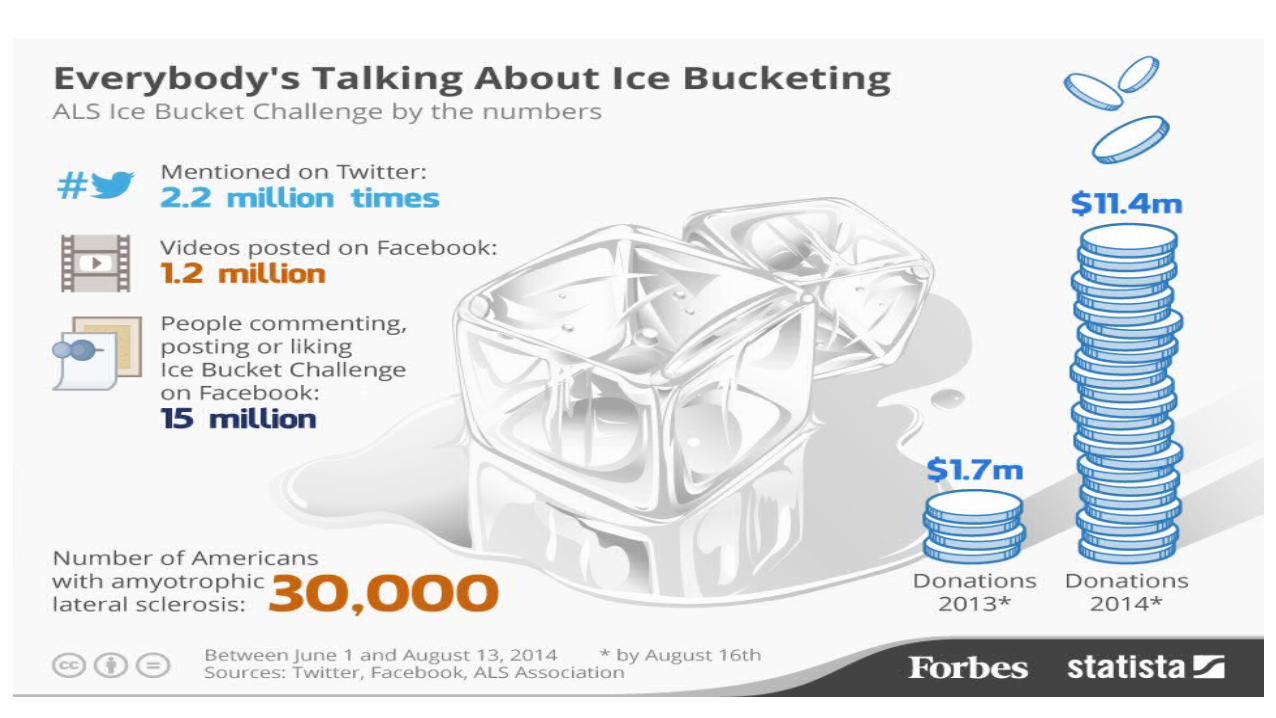
What is Ice Bucket Challenge ?
• The Ice Bucket Challenge for ALS/MND is a social media campaign that was initiated by Pete Frates, a former Boston College captain who is living with motor neurone disease (MND) in the US. Since Peter Frates posted his challenge online, the Ice Bucket Challenge quickly went viral and is now spreading across the world MND, sporting and entertainment communities.
The rules:Mandatory:1. Fill a bucket (or larger container) with water and ice2. Tip it over your head3. Challenge three other people to take the Ice Bucket Challenge within 48 hours4. If nominees don't take the Ice Bucket Challenge within 48 hours they make a donation to an MND charity.• Of course you can take the challenge AND make a donation and ask the people
you nominate to do the same! Optional:1. Add your own personal touch by creating a ice bucket tipper like Bill Gates.2. Post your video/photos on Facebook, Twitter, YouTube and Instagram. Use the hashtags #icebucketchallenge and #MND.

How to get involved?
• Take the Ice Bucket Challenge and challenge your friends and family to do the same.
Resources:
DynamedMayo clinicClinicalkeyUptodateEssentials of pathophysiology page (913+914)Pathophysiology clinical concepts of disease processes page (847) Professional guide to Pathophysiology page (297+298+299)http://www.disabled-world.com/artman/publish/famous-als.shtml