Allergy to latex gloves in clinical practice: Case reports
5
General Dentistry Allergy to latex gloves in clinical practice: Case reports F. J. T Burke*/M, A, Wilson7J. F. McCord* iVith increasing incidence qjglove wearing by dental health care workers, there are also increased reports of associated dermatológica! problems. Among these are Type IV allergic reactions, such as contact urticaria, and Type I severe reaction.';. Patients may aho be affected. Three cases of adverse patient reactions to latex or chemicals involved in latex manufacture are reported. Principal areas affected were circumoral and facial skin and the upper lip. A potential adverse reaciion ivas avoided for a third patient following histoiy taking, which identified an adverse reaction to a rubber swimming cap. (Quintessence Int ¡995:26:859-863.) Introduction The wearing of gloves by dental staff during patient treatment has been recommended for some years.'"^ and results of a recent survey in England and Wales have indicated that 83% of dentists wear gloves routinely for all patients and procedures,"* However, some dermatologie problems may be attributed to glove wearing^; twenty-eight percent of the routine glove wearers in the aforementioned survey reported some skin irritation following glove use. Four percent of this group also reported having experienced infec- tions of fingernail beds, which they considered to be a consequence of glove use. Among the skin complaints that may become apparent are hritant contact dermati- tis, allei^ic contact dermatitis, and contact urticaria (Type IV reactions),^ Furthermore, some glove con- stituents, such as thiurams and dithiocarbamates, having been implicated as allergens.^ In that respect, of 542 cases of occupational allergic contact dermatitis reported in a study in Finland, rubber gloves were considered to be responsible for 63 cases,'' In another study comprising 268 operating room nurses, skin tests to latex were positive in 21 nurses ( 10,7%),' Patients may be similariy affected; of routinely glove-wearing dental respondents to a survey 9,7% reported adverse patient reactions, such as mucosal * Department of Restorative Dentistry, Turner Déniai School, Uni- versity Dental Hospital of Manchester, Manchester, England Reprint requests; D r F J . T . Burks, Departmentof Restorative Dentistry. Turner Dental Schooi, LJniversity Dental Hospital of Manchester, Higher Cambridge Street, Manciiester M15 6FH, England. erythema, considered to be caused by the wearing of gloves by the dentist,'' Results of a similar study carried out in 1989^ indicated that 6% of patients had experienced an adverse reaction to latex, this increase demonstrating either an increasing problem per se, or an increasing awareness of the allergic potential of latex. The US Food and Drug Administration received 1,118 reports of reactions to latex over a 4-year period: Rubber dam was implicated in 19 cases, and latex examination gloves were implicated in 407 cases.' The purpose of this article is to highlight patients' allergic reactions to latex gloves through three case reports. Case reports Case I A 76-year-old woman attended the University Dental Hospital of Manchester for preliminary impressions for study casts prior to the provision of a maxillary partial denture. When the patient returned home, her husband noticed a red area on the left side of the patient's neck, and a photograph of the affected area was taken (Fig la). On contacting the dental hospital, the patient was given an immediate appointment. Examination revealed the presence of erythematous areas on the left side of the neck extending forward from the angle ofthe mandible toward the chin and a smaller erythematous area bilaterally at the angle ofthe mouth (Fig lb). Within 24 hours, the area of inflammation had resolved, A diagnosis of allergy to either the impression material or the latex glove material was made. The Quintessence International Volume 26, Number 12/1995 859
Transcript of Allergy to latex gloves in clinical practice: Case reports

General Dentistry
Allergy to latex gloves in clinical practice: Case reports
F. J. T Burke*/M, A, Wilson7J. F. McCord*
iVith increasing incidence qjglove wearing by dental health care workers, there are alsoincreased reports of associated dermatológica! problems. Among these are Type IV allergicreactions, such as contact urticaria, and Type I severe reaction.';. Patients may aho be affected.Three cases of adverse patient reactions to latex or chemicals involved in latex manufacture arereported. Principal areas affected were circumoral and facial skin and the upper lip. A potentialadverse reaciion ivas avoided for a third patient following histoiy taking, which identified anadverse reaction to a rubber swimming cap. (Quintessence Int ¡995:26:859-863.)
Introduction
The wearing of gloves by dental staff during patienttreatment has been recommended for some years.'"^and results of a recent survey in England and Waleshave indicated that 83% of dentists wear glovesroutinely for all patients and procedures,"* However,some dermatologie problems may be attributed toglove wearing^; twenty-eight percent of the routineglove wearers in the aforementioned survey reportedsome skin irritation following glove use. Four percentof this group also reported having experienced infec-tions of fingernail beds, which they considered to be aconsequence of glove use. Among the skin complaintsthat may become apparent are hritant contact dermati-tis, allei^ic contact dermatitis, and contact urticaria(Type IV reactions),^ Furthermore, some glove con-stituents, such as thiurams and dithiocarbamates,having been implicated as allergens.^ In that respect, of542 cases of occupational allergic contact dermatitisreported in a study in Finland, rubber gloves wereconsidered to be responsible for 63 cases,'' In anotherstudy comprising 268 operating room nurses, skintests to latex were positive in 21 nurses ( 10,7%),'
Patients may be similariy affected; of routinelyglove-wearing dental respondents to a survey 9,7%reported adverse patient reactions, such as mucosal
* Department of Restorative Dentistry, Turner Déniai School, Uni-versity Dental Hospital of Manchester, Manchester, England
Reprint requests; DrFJ.T. Burks, Departmentof Restorative Dentistry.Turner Dental Schooi, LJniversity Dental Hospital of Manchester, HigherCambridge Street, Manciiester M15 6FH, England.
erythema, considered to be caused by the wearing ofgloves by the dentist,'' Results of a similar study carriedout in 1989^ indicated that 6% of patients hadexperienced an adverse reaction to latex, this increasedemonstrating either an increasing problem per se, oran increasing awareness of the allergic potential oflatex. The US Food and Drug Administration received1,118 reports of reactions to latex over a 4-year period:Rubber dam was implicated in 19 cases, and latexexamination gloves were implicated in 407 cases.'
The purpose of this article is to highlight patients'allergic reactions to latex gloves through three casereports.
Case reports
Case I
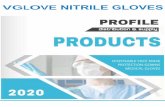
A 76-year-old woman attended the University DentalHospital of Manchester for preliminary impressionsfor study casts prior to the provision of a maxillarypartial denture. When the patient returned home, herhusband noticed a red area on the left side of thepatient's neck, and a photograph of the affected areawas taken (Fig la). On contacting the dental hospital,the patient was given an immediate appointment.Examination revealed the presence of erythematousareas on the left side of the neck extending forwardfrom the angle ofthe mandible toward the chin and asmaller erythematous area bilaterally at the angle ofthemouth (Fig lb). Within 24 hours, the area ofinflammation had resolved,
A diagnosis of allergy to either the impressionmaterial or the latex glove material was made. The
Quintessence International Volume 26, Number 12/1995 859

General Dentistry
Fig la Case 1, Erythematous area on the lelt side ot theneck extending forward trom Ihe angle of the mandibletoward the chin.
Fig 1b Case 1. Smaller erythematous area bilaterally atthe angle of the mouth.
latter was considered to be most likely, in view of tbearea of tbe face affected, because tbis corresponded totbe area likely to be in contact witb a gloved handduring tbe recording of maxillary impression. Thediagnosis of latex allergy was confirmed by patcb tests,and tbe patient was successfully treated on subsequentvisits by an operator wbo wore vinyl gloves.
Case 2
A 42-year-old woman attended the dental hospital fora restoration In ber maxillary left first molar. Duritigtreatment, it was noted tbat the left side ofthe patient'slip was becoming increasingly swollen (Figs 2a and2b). The affected area was not related to the injectionsite, nor had it been traumatized. Tbe swelling spreadacross the midline within 1 hour, but no ftirtherincrease in size occurred after this time. After 6 hours,the swelling abated. On examination 24 hours later,the patient's lip had returned to normal. The patientthen recalled that her lip had become slightly swollenfollowing treatment on a previous occasion, but thatshe had not considered it necessary to report thisoccurrence.
A provisional diagnosis of angioedema because oflatex allergy was made. Tests for allergy to localanesthetic solution and latex confirmed this diagnosis.The patient's medical history included asthma, hay
fever, eczema, and allergies to shellfish, melons,pineapples, bananas, oats, chocolate, antioxidant foodadditives, and aspirin. When the patient was treated onsubsequent visits, tbe dentist wore vinyl gloves.
Case 3
A 60-year-old man suffered circumoral erythemafollowing treatment with a general dental practitioner(Eig 3). The patient was then referred to the dentalhospital for treatment, when his medical historyindicated that the patient had previously displayedmultiple allergies. The patient was also asked if he hadever suffered any reaction, such as itching or skinreddening, to rubber articles, such as balloons orcondoms. The patient stated that he had notedreddening of his scalp following the wearing of arubber swimming cap.
Accordingly, prior to tbe commencement of treat-ment, the patient was referred for patch testing. Theresults showed that he had an allergic reaction to twoof the constituents of carba mix and three of theconstituents of thiuram mix, thereby indicating anallergy to a number of chemicals used in the manu-facture of latex gloves. The patient was successfullytreated by an operator who used poLyvinyl gloves tocover the latex gloves.
860 Quintessence International Volume 26, Number 12/1995

General Dentistry
Figs 2a and 2b Case 2. Sweiling of the left side of the iip foiiowing contact wifh iatex.
Discussion
These cases demonstrated the potential for adverseresponses to latex in patients following contact withgloves worn during dental treatment. In the patientdescribed in case 1, the mucosal reaction was minimal,while the skin reaction was considerable; the converseoccurred in the patient described in case 2. A similarreaction was described by March,'" who reported thedevelopment ofa red, swollen, and tender mucosa in apatient following crown preparation and impressiontaking. In that patient, allergy to the impressionmaterial was initially suspected, but patch tests in-dicated a severe allergic response to latex. At the timeofthat report, it was considered that such cases wererare, since few had been reported. However, thereappears to be potential for an increasing incidence ofthe problem, given tbe increasing level of glove use inthe dental and medical fields.
More than 600 serious reactions to latex have nowbeen reported to the US Food and Drug Administra-tion, including at least 16 fatalities attributed toanaphylaxis." Anaphylactic episodes are now knownto have complicated a variety of common medical andsurgical procedures, as well as oral, vaginal, and rectalexaminations in which latex gloves were used. It maybe that the affected patients had displayed, but had notreported, some previous signs of latex allergy, such asitching or erythema, on contact with everyday itemscontaining latex, such as balloons, contraceptives,baby pacifiers, and envelope adhesives. In anotherease, an obstetrics and gynecology physician, whonormally wore cotton and vinyl liners under glovesbecause ofa history of contact urticaria associated withlatex gloves, donned latex gloves without liners for
Fig 3 Case 3. CIrcumoral erythema 24 hours after denfaltreatment.
treatment of an emergency and developed an anaphy-lactic reaction.''
A variety of rubber-containing devices have beenimplicated in the production of iatrogenic reactions inpatients'^
• Latex gloves• Condoms• Urinary catheters• Tourniquets« Wheelchair tires• Adhesive tapes and bandages• Hot water bottles• Sheets and pillows• Dental rubber dam• Endotracheal tubes• Hemodialysis units• Electrocardiographic strips
International '^"'"mp Oft Number 12/1995 861

General Dentistry
Patients suffering from a number of conditions orundergoing certain operations have been consideredto be pariicuiariy at risk for intraoperation anaphylac-tic response to latex'':
1. Patients suffering from spina bifida abnormalities.Slater et al '̂ identified this group because of theirfrequent exposure to iatex gloves from an earlyage.
2. Women undergoing cesarian section or episiotomysuturing. Turjanmaa et al'^ reported on four pa-tients who had previously experienced locai whealand fiare reactions when latex gloves were used.Two patients experienced aliergic reactions afterthe episiotomy was sutured, while in the otherpatients, one of whom was a dentist, anaphylacticsymptoms occurred immediately after the sameoperation.
3. Patients receiving a barium enema with a latexballoon tip."
4. Patients with occupational exposure, such as thoseinvolved in the manufacture of iatex gloves orcatheters."
5. Health care workers and others who wear iatexgloves. Because of generalized usage, they maybecome sensitized.
Furthermore, the majority of patients who developlatex hypersensitivity have a liistory of another allergiccondition, such as hay fever," as did the patients incases 2 and 3.
As a result of the reported increase in allei^y tolatex, the US Food and Drug Administration issuedthe following Medical Alert in March 1991 ":
Allergic Reactions to Rubber Latex-containingMedical Devices
Because of reports of severe allei^ic reactions to medicaldevices containing laiex (natural rtibbcr). the Food andDrug Administration is advising health care professionalslo identify those latex-sensitive patients and be prepared totreat allergic reactions promptly. Patients'^ reactions tolatex have ranged from contact urticaria lo systemicanaphylaxis. Latex is a component of many medicaldevices, including surgical and examination gioves, cathe-ters, intubation tubes, anesthesia niasks. and dental rubberdams.
It is therefore important that patients who have alatex allergy be identified, and, just as patients arerourinely asked about allergy to medications, a carefulhistory should be taken from every patient regardingcontact with iatex. Among questions that may be askedare those concerning itching, rash, or rhinitis follow-ing contact with latex-containing objects, such asballoons or condoms. Additionally, an unexplained
aliergic or anaphylactic reaction during a medicalprocedure may indicate sensitization. Health careworkers should also be asked if they have suffered areaction of any type to latex gloves. Suspect patientsshould be referred for further testing.
For those patients who are subsequently found fodemonstrate an allergic response to latex, gloves madeof vinyl may be appropriate, although some brandshave demonstrated poor puncture resistance'^ andhigh stiffness, '̂ or polyvinyl overgloves may be used asdescribed in case 3. Recently introduced nonlatex,nonvinyl gloves made from synthetic copolymers orstyrene butadiene block polymers {Tactyion, SmartPracrice; Elastyren, Allerderm Labs) may also be ofvalue. Furthermore, manufacturers should be encour-aged to avoid the use of potentially irritant chemicalsduring manufacture of gioves because it has heenconsidered that additives are the main allergens inrubber materials.'* The thiuram group, the mercaptobe-zothiazole group, and the carbamates are aliergensoften utilized as latex accelerators, while amines areallergens commonly present as antioxidants. Naturaland synthetic rubber polymers are rarely contactallergens, but natural rubber may cause contact urti-caria with immediate wheal and flare reactions. How-ever, proteins from natural iatex appear to be the causeofthe most serious type of allergic reactions.-"
Summary
Three cases have been described in which patientsdisplayed allei^y to latex or chemicals involved inmanufacture of latex gloves, and a review of theliterature has indicated that increasing numbers ofpatients may be allergic to latex devices. Dental healthcare workers should be aware ofthe aliergic potentialof latex and should include questions regarding thiscondition during history taking. Dentists should beaware ofthe potential for an anaphylactic reaction tolatex, however rare, and should be prepared to treat itaccordingly.
References
1. British Dental Association. Guide to Blood Borne VirJSes and theControl of Cross-Infection in Dentistry. London: British DentalAssociation. 19S7.
2. Council on Denial Malerials, Instruments and Equipment. Infectioncontrol recommendations for the dental office and the dentallaboratory. J Am Dent Assoc 1988; i 16:241-248.
.1. Crawford JJ. State-oft he-art practicai infection control in dentistryJ Am Dent Assoc 1985:110:629-633.
862 Quintessence International Volume 26, Number 12/1995

General Dentistry
4, Burt;s FJT, Wilson NHF. Ctieting SW. Giove use by dentists inEngland and Wales; Results of a 2-year follow-up stirvey. Br Dent J1994;176:337-341
5. Field EA, King CM. Skin probtems assoeiated with routine wearingofprotective gloves in dental praetiee, BrDent J t99Ü; 168:281-285,
6, Estlander T. Jolanki R, Kanerva L, Dertnatitis and urticaria fromrubber and plastic gloves. Contact Dermatitis t986;14;2O-25,
7. Lagrer F, Vereudoet D. Lhermet t. Poyen D, Ctiarpin D, Prevatenceof tatex altergy in operating room nurses. J Allergy Clin tmmunoll992;9O;3t9-322.
S. Burtce F]T, Wilson NHF, Wastell DG, Cheung SW, Glove use indinieat practice; A survey of 2000 dentists in Engiand and Wales. BrDentJ 199t;171:128-t:2.
9. Couneit on Dentat Materials, Cotincit on Dentai Therapeutics,Couneit on Dental Researeti. Reactions to tatc\ in a heidth caresetting: Deating with patient/worker coneerns. J Am Dent Assoet993:124:9t-92,
10, March PJ. An ailergic reaction to latex rubber gioves. J Am DentAssoc t9S8;117;590-591,
11, American Coilege of Altergy and tmmunoiogy. interim Recommen-dations to tieaitti Professionais and Organizations. AmericanColtege of Aitergy and Immunotogy, t992.
12, Chen MD, Greenspoon JS, Long JZ. Latex anaphytaxis in anobstetrics and gynecology physician. Am J Obstet Gynecol 1992;
13, Fistier AA. tatrogenic attergic rubber reactions in medicai anddental patients. Part tL CurT Contact News t992;49:8t-82,
14, Fislier AA. tatrogenic (intraoperative) rubber glove aiiergy andanapliyiaxis. Part L Curr Contaet News t992;49;17-18.
15, Slater JE, Mostelto LA. Shaer C, Honsinger RW. Type I hypersen-sitivity to rubber. Arm AJlergy 1990;6S;4t 1-414.
16, Tuijanmaa K, ReunataT, Tuimata R, Karkkainen J. Allergy to tatexgtovei: Unusuai complications during delivery. Br Med J 1988:297:1029.
17, LJS Food and Drug Administration. Allergic Reaetions to Latex-Containiris Medieat Devices. hVA Medical Aiert MD.A9t-l. 29Mar t991.
iS. Burke FJT. Wiison NHF. The incidence of undiagnosed punctures inno n-steriie gloves. Br DentJ t990;t68:67-7t.
¡9. Burke FJT, Watts DC, Wüson NHF, Some physieai factors influenc-ing taetiie pereeption with disposabte non-sterite gloves. J Dentt989;17;72-76.
20. Tuijanmaa K. Laurila K, Malden-tiiijunen S, Reunala T. Rubbereontact urtiearia. Contact Dermatitis 1988;i9;362-3â7, D
Quintessence International Volume 26, Number 12/1995
J.Thomas Lambrecht
3-D Modeling Technologyin Oral atid Maxillofacial Surgery
US$140145 pp; 292 Illus(227 in color¡ISBN 0-8S715-287-7
This book explores 3-D trtodeling of indi-xdilital patients undergoitig oral atid max-
illofacial .surgeiy/recotistruction. Modelsfacilitate treatment pliitinitig and surger)-' byallowitig surgeons to st;ndy a patient's bofiystructure. In addition to applications in pre-prosthetic and tumor surgery, 3-D modelingcan assist in surgical correction of malocclu-sion atid congenital deformities. An introduc-tion to the 3-D tnodchtig process—includingcomputed tomography, jnagnetic resonance(ojnography, and model fabricatioti—andnutnerous case studies are presented.
Contents includes:/ Gi^ncra! History" of 3-D Technologyi/ Visualization/ Model Constructioti/ Limitations and Potential Applications/ Coinpnterized Tomography/ Model Fabrication/ Magnetic Resonance Tomography/ Utilities/ Nineteen Case Studies/ Bibliography/ Manrifacturers and Related
Information
Order TodayToll free 1-800-621-0387
Fax 708 682-3288quinl«0enccbook/