
By Francisco Astete, Alex Smith, Karelis Sanchez Alex Ganan.
Upload
opuniteCategory
view
1.103download
0
Coordinating Multiple Stakeholders
April 10-12, 2012 Walt Disney World Swan Resort

Learning Objectives: 1. Describe the relationship between prescription drug morbidity and mortality and the under-treatment of pain. 2. Identify measurement-based care as standard of care in pain medicine and describe how to measure pain, mood and function in every clinical encounter. 3. Evaluate how new state and federal policy changes will likely allow more prudent and safer use of opioids for chronic, non-cancer pain.
Disclosure Statement
• All presenters for this session, Dr. Alex Cahana and Dr. Gary M. Franklin, have disclosed no relevant, real or apparent personal or professional financial relationships.

John J. Bonica
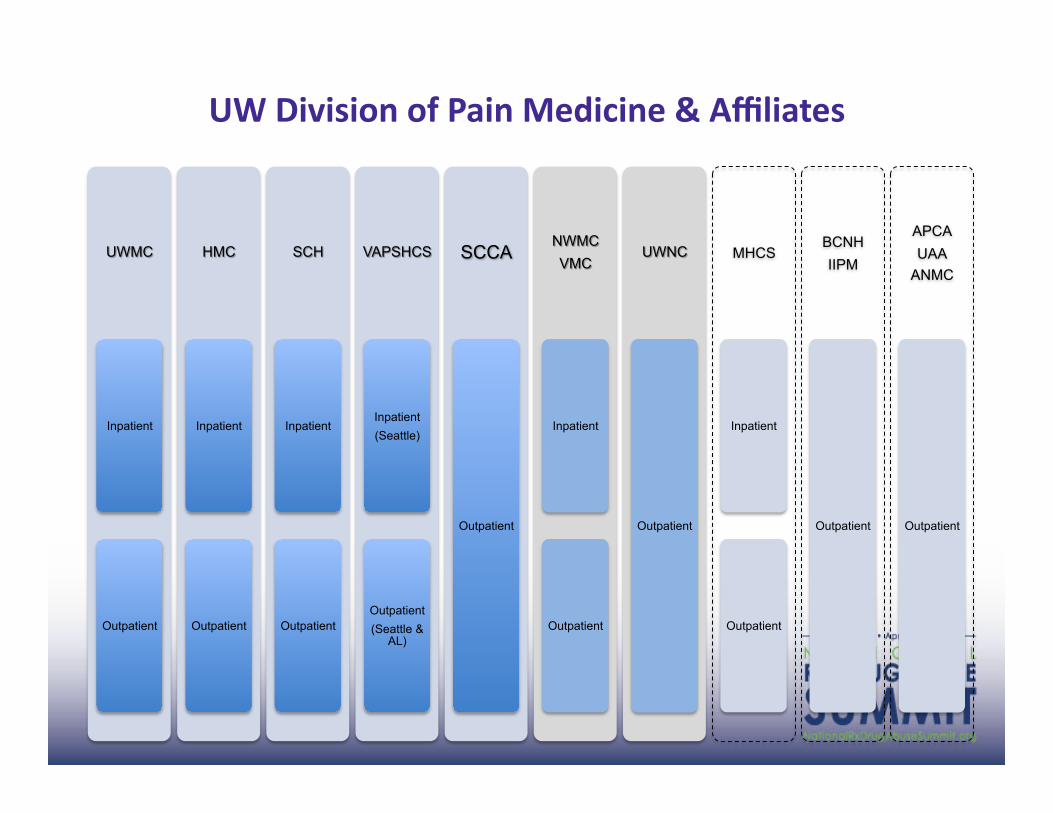
Inpatient
Outpatient
Inpatient
Outpatient
Inpatient
Outpatient
Inpatient (Seattle)
Outpatient (Seattle &
AL)
Outpatient
Inpatient
Outpatient
Outpatient
MHCS
Inpatient
Outpatient
BCNH IIPM
Outpatient
APCA UAA
ANMC
Outpatient
UW Division of Pain Medicine & Affiliates
My disclosures
• I am not opio-‐phobic
• I am not opio-‐philic • I am not needle-‐phobic
• I am not needle-‐philic • I am agnos3c to chi gong and tai chi
• ‘I just wanna know how my pa3ents are doin’
• Because if I don’t measure outcome I believe my prac3ce is not medically, financially or ethically sustainable
• Standard of Care needs to be codified
Today:
• Situa3on • Model of Care
• Value • Future

Overtreatment is the new under-‐treatment

132 to 1775
690 to 1,442

Opioid AddicEon Treatment
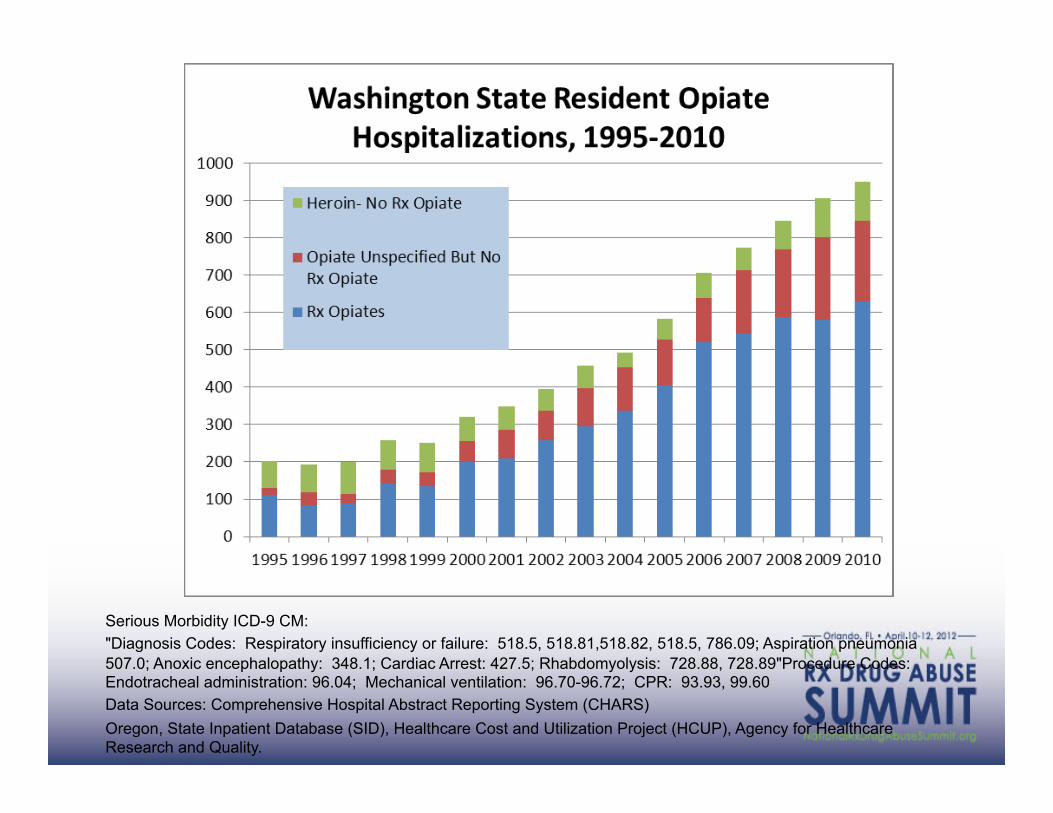
Serious Morbidity ICD-9 CM: "Diagnosis Codes: Respiratory insufficiency or failure: 518.5, 518.81,518.82, 518.5, 786.09; Aspiration pneumonia 507.0; Anoxic encephalopathy: 348.1; Cardiac Arrest: 427.5; Rhabdomyolysis: 728.88, 728.89"Procedure Codes: Endotracheal administration: 96.04; Mechanical ventilation: 96.70-96.72; CPR: 93.93, 99.60 Data Sources: Comprehensive Hospital Abstract Reporting System (CHARS) Oregon, State Inpatient Database (SID), Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality.
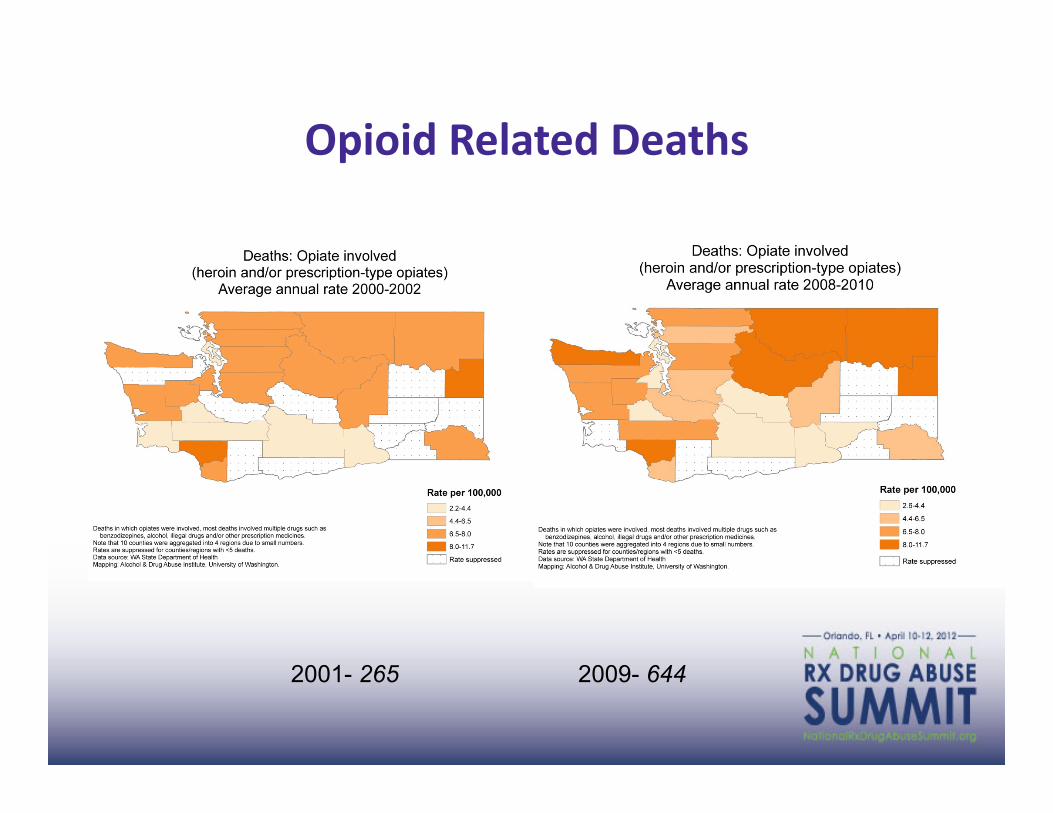
Opioid Related Deaths
2001- 265 2009- 644
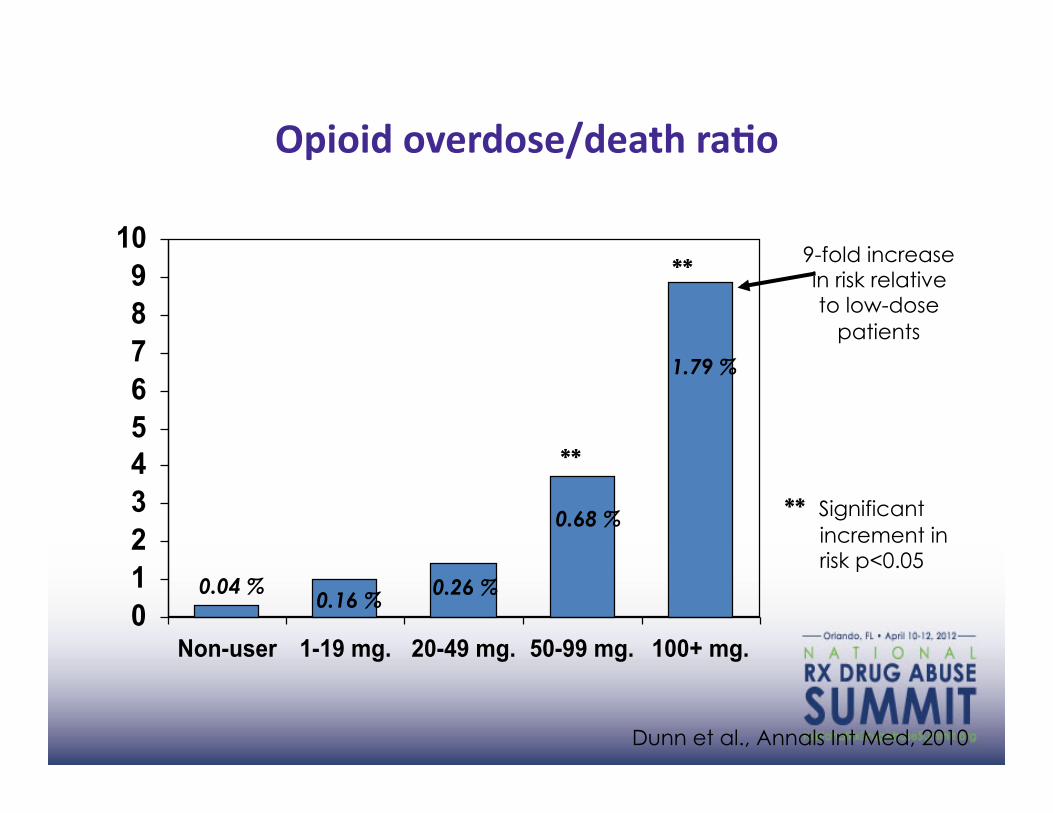
Opioid Overdose Risk (fatal & non-fatal) by Average
Daily Dose of Medically Prescribed Opioids Opioid overdose/death raEo
0123456789
10
Non-user 1-19 mg. 20-49 mg. 50-99 mg. 100+ mg.
1.79 %
0.68 %
0.26 % 0.16 % 0.04 %
9-fold increase in risk relative to low-dose
patients
Dunn et al., Annals Int Med, 2010
**
**
** Significant increment in risk p<0.05

0
0.5
1
1.5
2
2.5
Non-user 1-19 mg. 20-49 mg. 50+ mg.
10.0 %
7.0 %
5.7 % 3.8 %
2-fold increase in risk relative to non-users
Saunders et al., JGIM, 2010
** Significant increment in risk p<0.05
**
Fracture Hazard RaEo

Merrill et al., under review
Adverse selecEon:
26.8%
38.5%
51.7%
61.4%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
1-19 mg 20-49 mg. 50-119 mg. 120+ mg.
1.0 1.4 2.1 2.6
Odds ratios adjusted for pain severity and patient characteristics

Newborns with Drug Withdrawal (GeneraEon Rx) Washington State, 1990-‐2009
0
1
2
3
4
5
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008
Rate per 1,000 live births
Source: Washington State Department of Health, Comprehensive Hospital Abstract Reporting System

WA State Healthy Youth Survey Frequency of Use to Get High Past 30 days Grade 10
Sabel J, Banta-Green C. CSTE 2009

!"#$%&$'(()*$+('$',(-.$/.(*0.-/'-%)$1.2+*$&.%3$&.-()1*$4)1$&43-567$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$!
!"#$%&"'()%&"#*#%+,-.*%/,#%0*/1#23%4-&%'(%&"#%5,6(.%"/(+*7%
&"#$8,#%(6&2$!!"#$%&'!()*!("+,-."/,0'!#$1&2'"/'3$#4'56&',/7'*&,0-8'9!&:-&;<&$'=>>?@"
84'-%)45$943-56$:4.')(.*,-/$
$
#$%&"$'(")($*%&)"+%,-"$."/0(-&1(,2""""""""
$84'-%)45$943-56$:4.')(.*,-/"
3456"7$(0+"809":%0;%<"=+$(%>0""??@4A"BC$&12""?6AD534D44@6"=0E2"?6ADFAGD4F@A"***D+$HI9$'(;1>,D$()"
;)<-'(*$6%2$'%$:4.'-0-/4'($-)$-'*$
=&&-5-4'($>(?-)[email protected])-)+$
"
@,2.*146A$B2)($C.1$
J0-%$&0+"K&-($>'H-%$&"-$"-C1""
L$HI"M$'(":1>,"70;/0%)&"
"
@,2.*146A$B256$D',$
L$HI"M$'(":1>,"70;/0%)&""
K;/+1;1&-0-%$&"N%-"
"
@,2.*146A$B256$EF',$$
:1>%0"O(0%&%&)"
P$*"-$"Q1H'(1":1>%0"7$R1(0)1""
%&"M$'(":0(I1-""
"
@,2.*146A$=2+2*'$GE',$
S..%+%0-1,"T1,-"B(0H-%H1,""
!"#$%&"'(%)*+,%-.('/%01$*%21#$3%
UR1&-2"=10-'(%&)"V(1)$&"B0(-&1(,C%/"
"
$$$$$$$$$$$$$$$$$$$@-3(*$?6$H%)(I$$$$$$$$$$$$$$$$$$$$$$$$$$$$GI""JEI""$/3$(*'$
$$$$$$$$$$$$$$$$$$$$$$$$$$$GEI""JGI""$/3$0*'$$
$$$$$$$$$$$$$$$$$$$$$$$$$$$GGI""$43JGEI""$/3$3*'$
$$$$$$$$$$$$$$$$$$$$$$$$$$$G"I""$43JGGI""$43$/*'$
@%$KLM:$NJ34-5$2*$4'I$
&W(1&,$&X&./D$()"
Q/$&,$(1>"W9""

More opioids, more addicEon, more deaths
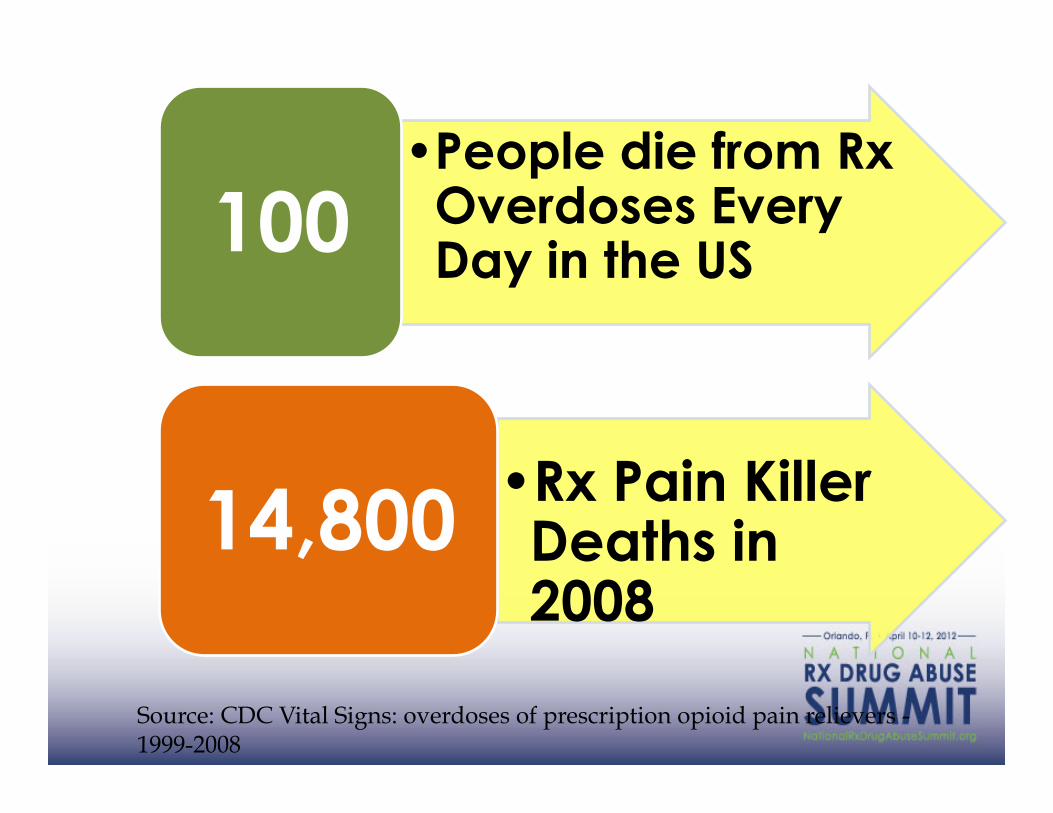
• People die from Rx Overdoses Every Day in the US 100
• Rx Pain Killer Deaths in 2008
14,800
Source: CDC Vital Signs: overdoses of prescription opioid pain relievers - 1999-2008
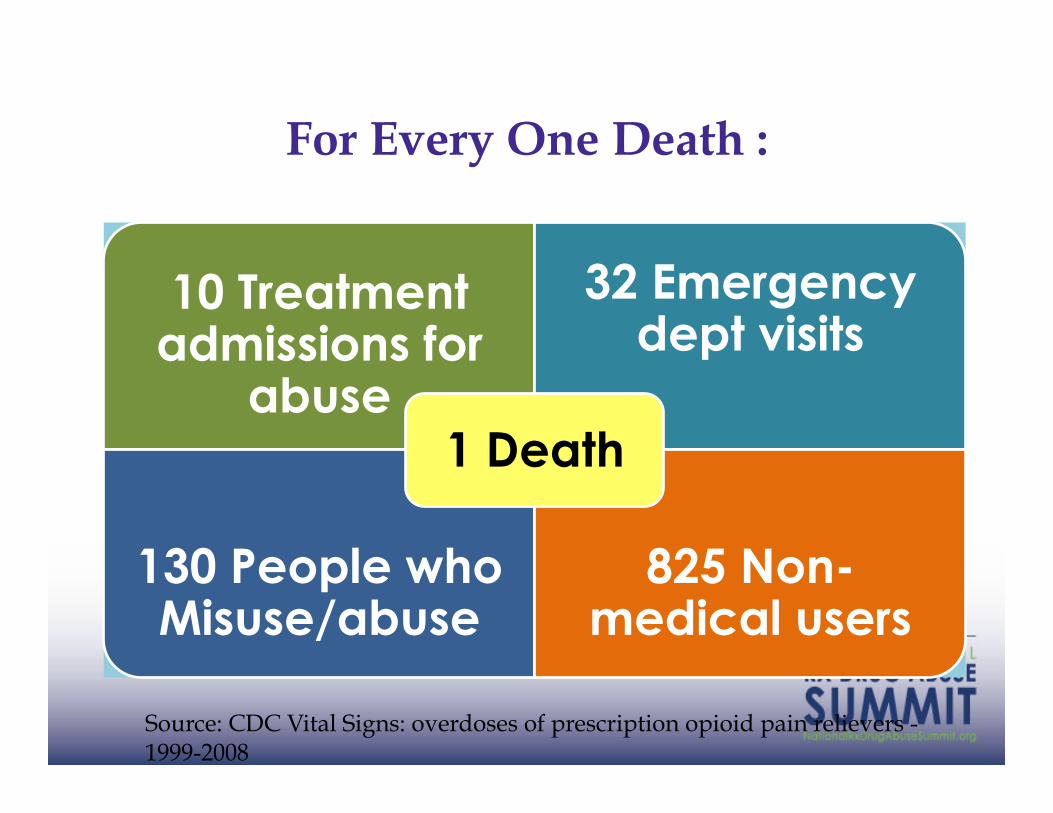
For Every One Death :
10 Treatment admissions for
abuse
32 Emergency dept visits
130 People who Misuse/abuse
825 Non-medical users
1 Death
Source: CDC Vital Signs: overdoses of prescription opioid pain relievers - 1999-2008

Cultural Transformation

Today:
• Situa3on • Model of Care
• Value • Future

Revise our pracEce model
• System is fragmented
• Care is inconsistent
• Cost is unsustainable
• Coordinated care (PCMH) Patient activation
• Collaborative care (Telepain/ECHO)
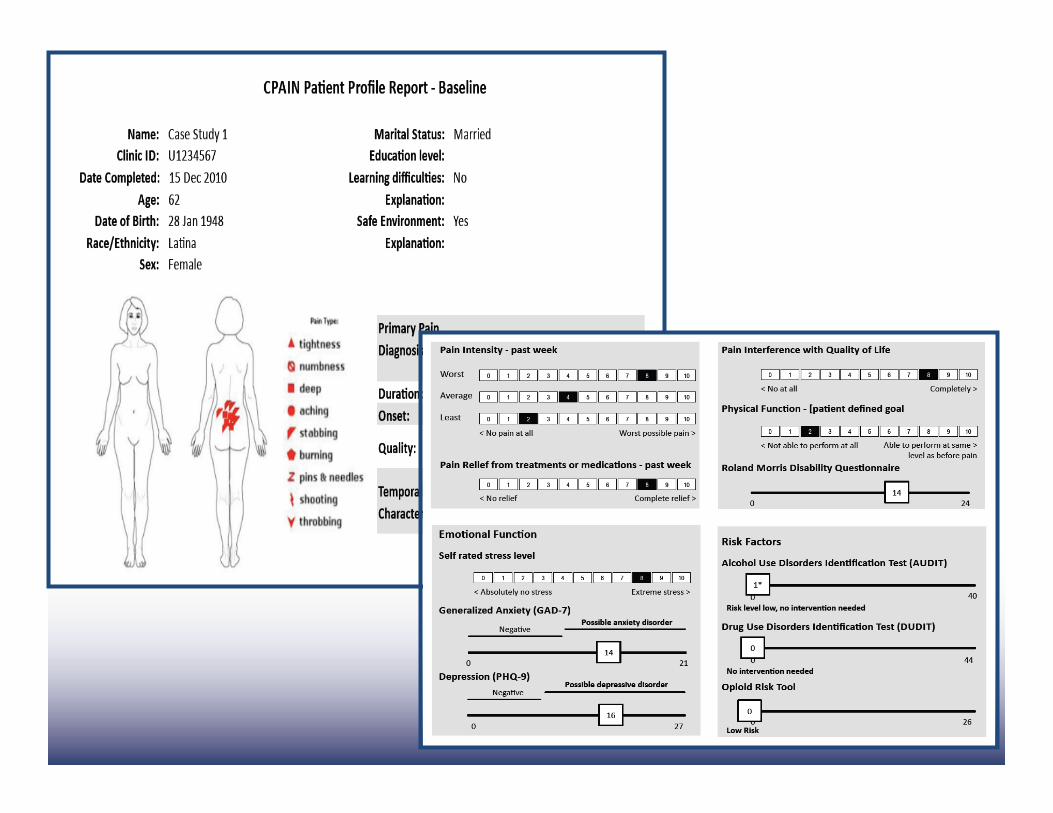
• Measurement based care (CPAIN / PainTracker)
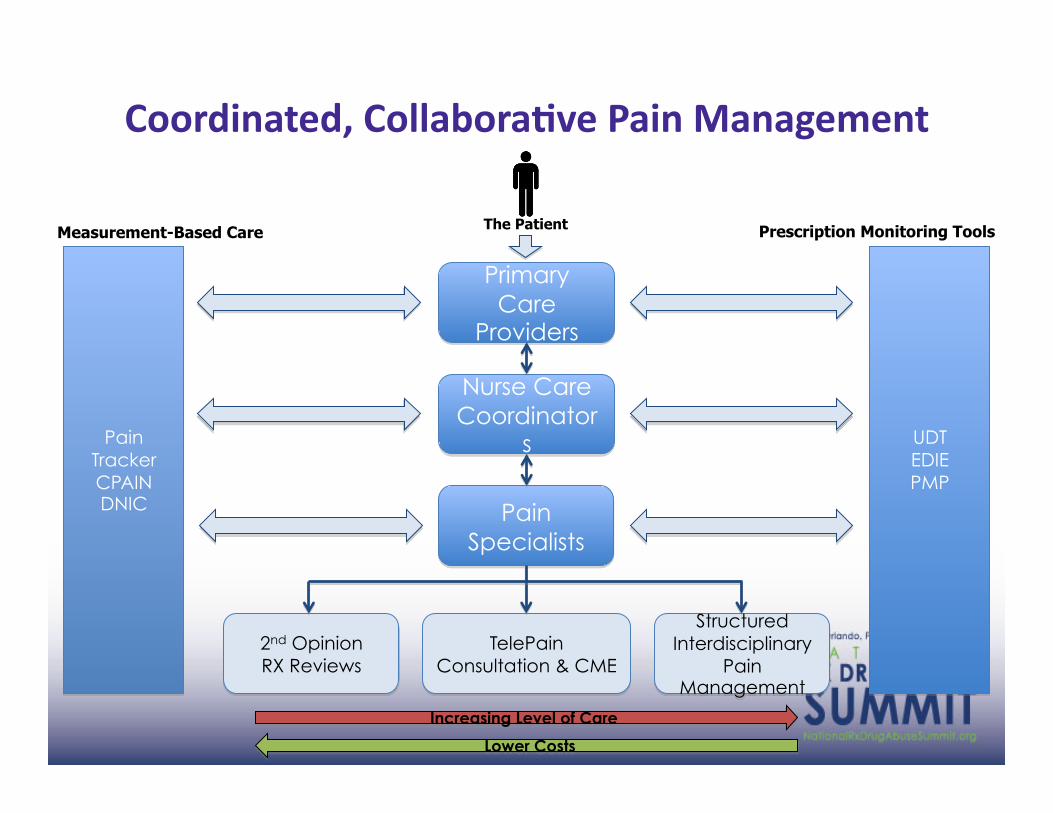
Primary Care
Providers
Nurse Care Coordinator
s
Pain Specialists
TelePain Consultation & CME
Structured Interdisciplinary
Pain Management
2nd Opinion RX Reviews
Pain Tracker CPAIN DNIC
UDT EDIE PMP
Increasing Level of Care
Measurement-Based Care Prescription Monitoring Tools The Patient
Lower Costs
Coordinated, CollaboraEve Pain Management
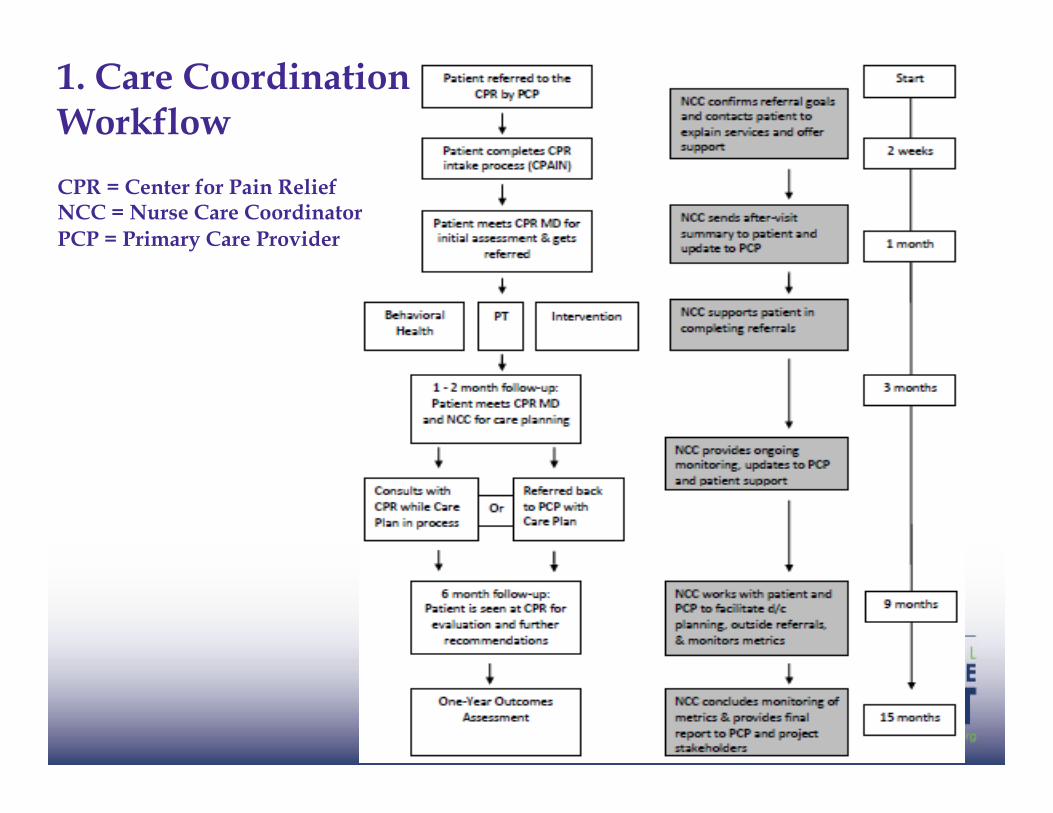
1. Care Coordination Workflow
CPR = Center for Pain Relief NCC = Nurse Care Coordinator PCP = Primary Care Provider

2. ECHO/TelePain/ROAM

!"#$#%#&$'
!"#$#%#&$'
(&)*$+'!&,*,'
(-*,*$+*.'+/'0!12'
3..#)/$&"'(&)*$+,'#$'(-&%)%*'
“MulEplier Effect”
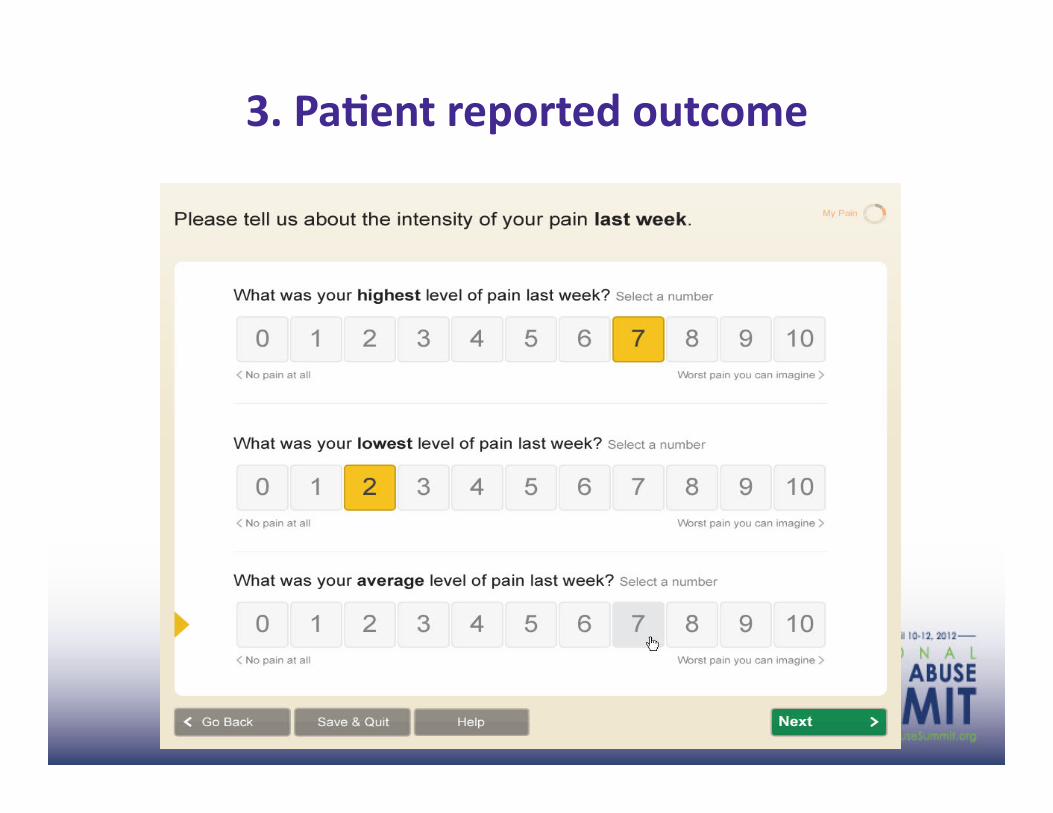
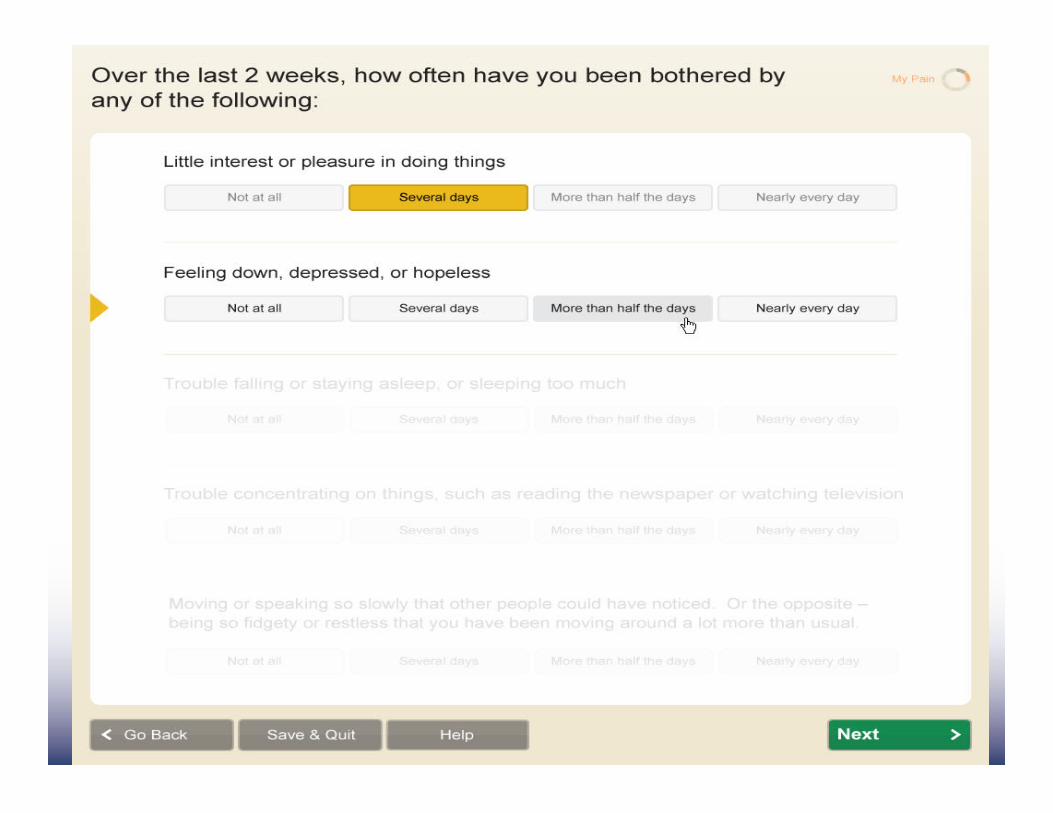
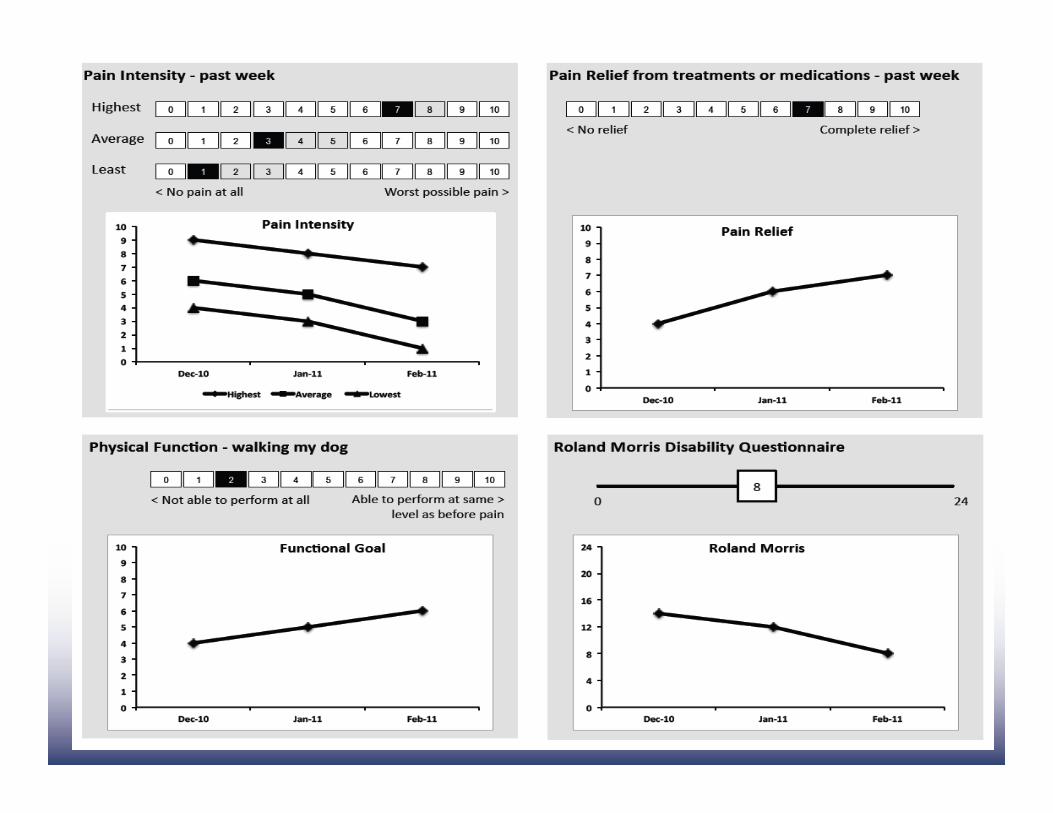
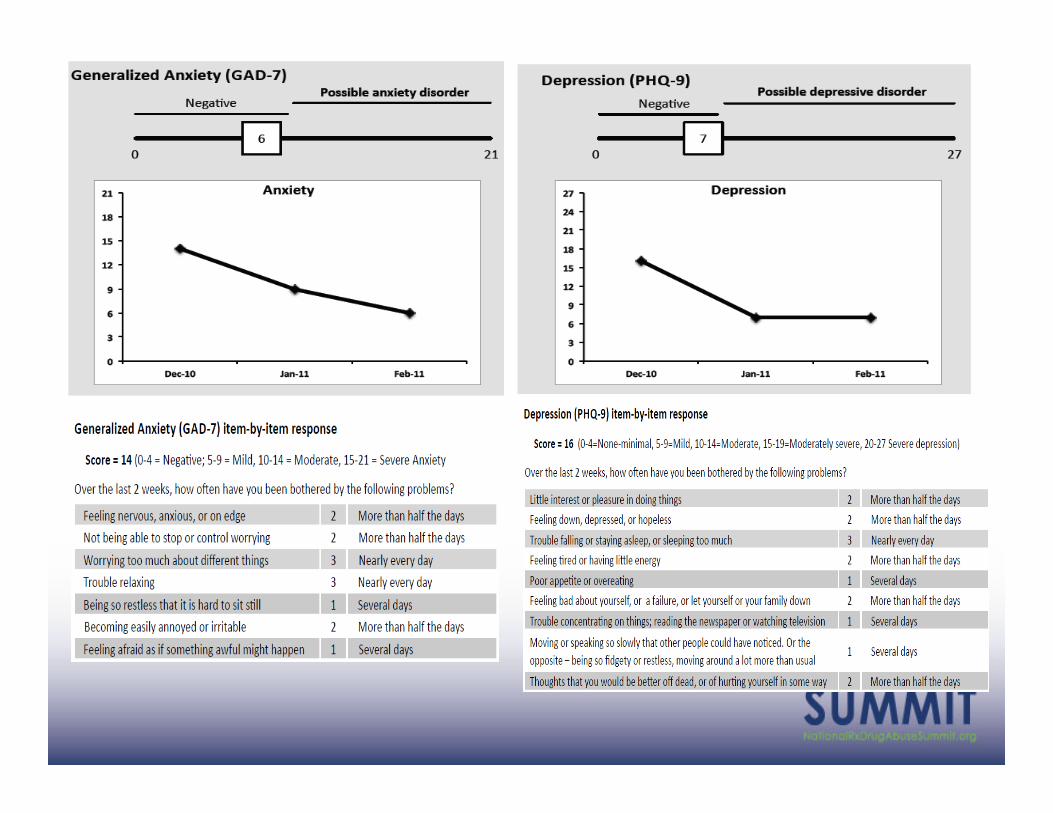
3. PaEent reported outcome
Today:
• Situa3on • Model of Care
• Value • Future

n=3500
1. Coordinated Care
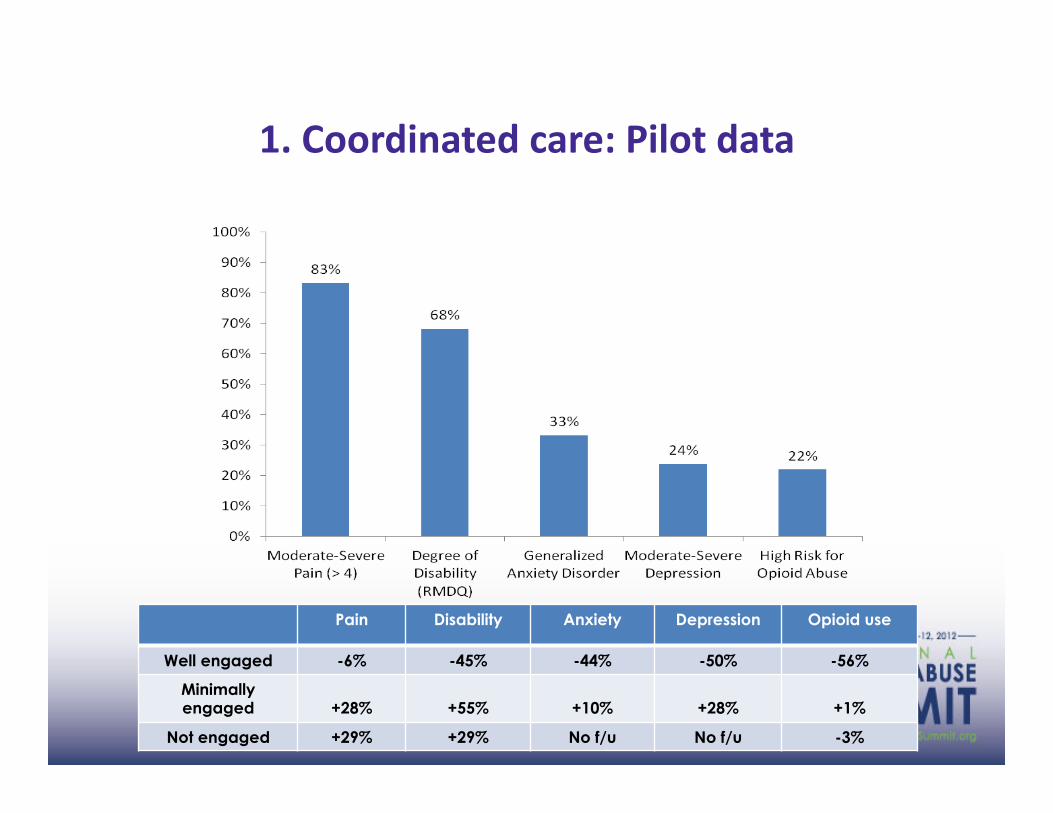
1. Coordinated care: Pilot data
Pain Disability Anxiety Depression Opioid use
Well engaged -6% -45% -44% -50% -56%
Minimally engaged +28% +55% +10% +28% +1%
Not engaged +29% +29% No f/u No f/u -3%
2. ECHO/TelePain/ROAM
• 40-‐50 dial-‐ins each session • 1500 providers • 76 loca3ons • 2240 CME hours
• Regional ‘Pain champions’ (meta-‐ECHO)

N = 94 Mean = 4.7 SD = 0.6
N = 95 Mean = 4.5
SD = 0.7
N = 94 Mean = 4.3
SD = 0.7
0
1
2
3
4
5
6
Learning best practice care
Developing clinical expertise
Comfortable teaching others what I've learned
Mea
n R
atin
g
Participants Rated Level of Agreement on a 5-point Scale: 1 = Not At All, 5 = To a Large Degree
2. ECHO/TelePain/ROAM

N = 85 Mean = 4.6
SD = 0.7
N = 84 Mean = 4.3
SD =0.7
N = 84 Mean = 4.4
SD = 0.7
N = 85 Mean = 4.4
SD = 4.5
N = 86 Mean = 4.5
SD = 0.6
0
1
2
3
4
5
6
Reduced patient travel for specialty care
and testing
Reduced emergency room visits
Provider's appropriate use
of testing
Decreased visits by
patients to specialists
Through early and effective
patient interventions
Mea
n R
atin
g
Providers Rated Agreement on a 5-point Scale: 1 = Strongly Disagree, 5 = Strongly Agree
2. ECHO/TelePain/ROAM

2. ECHO/TelePain/ROAM
0
5
10
15
20
25
State Clallam Grant Jefferson Kitsap Okanogan
2007-‐2009
2008-‐20010
34%
41% *
63% * 54% *
43% *
29%
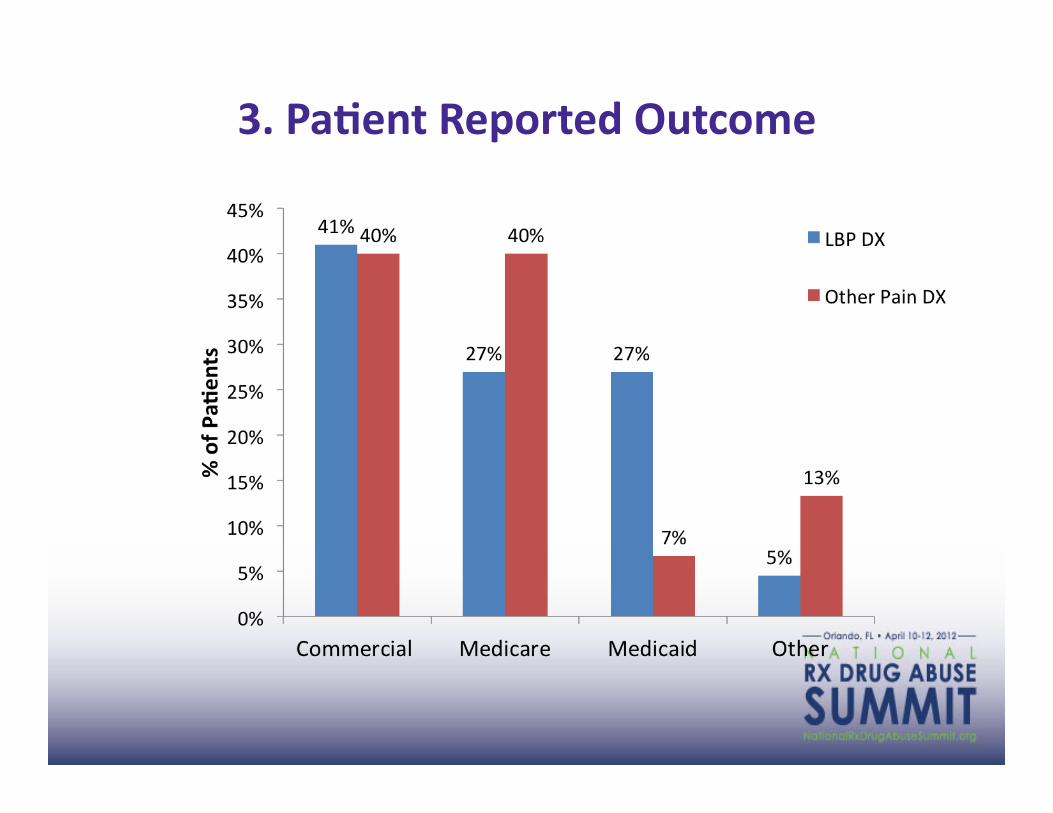
3. PaEent Reported Outcome

3. PaEent Reported Outcome
3. PaEent Reported Outcome
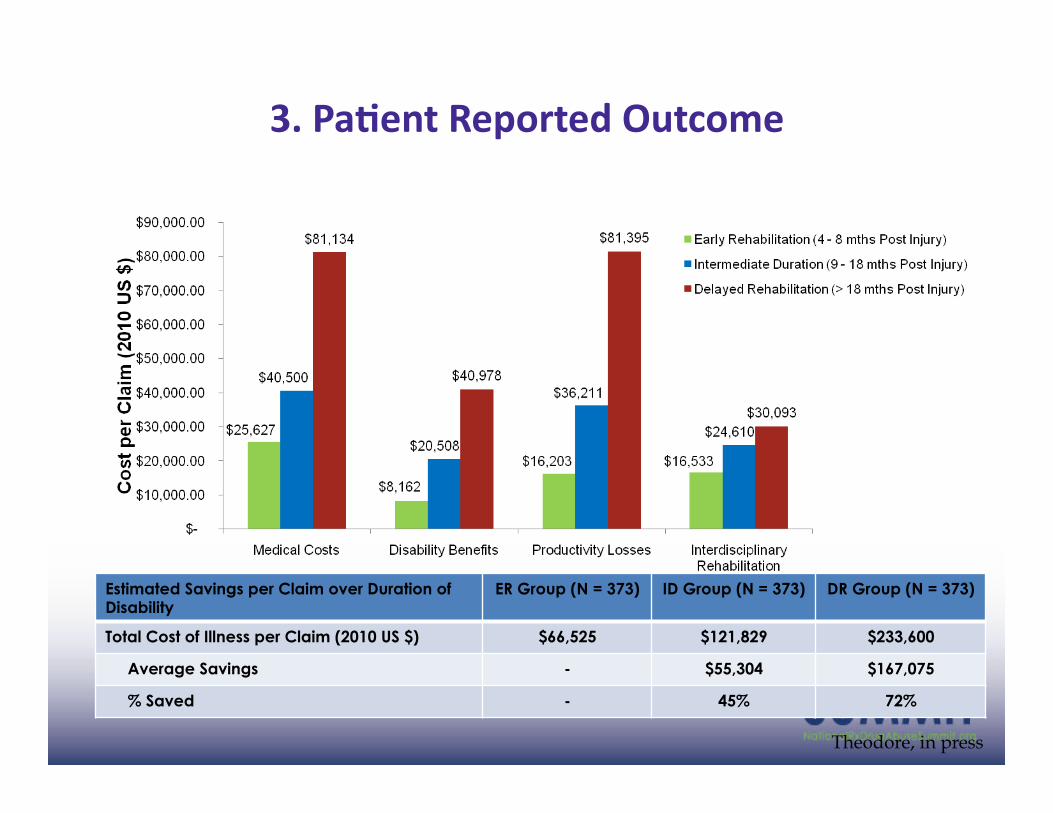
Estimated Savings per Claim over Duration of Disability
ER Group (N = 373) ID Group (N = 373) DR Group (N = 373)
Total Cost of Illness per Claim (2010 US $) $66,525 $121,829 $233,600
Average Savings - $55,304 $167,075
% Saved - 45% 72%
Theodore, in press
Today:
• Situa3on • Model of Care
• Value • Future

Scalability and sustainability
• State (WA, AK) • DoD/VA • Large employers (UW, GE)
• CMS/CMMI
WA State legislaEon (2876):
• Mandates Educa3on and Guidelines
• Mandates TeleHealth
• Mandates Opioid tracking
• Mandates Measurement at each encounter
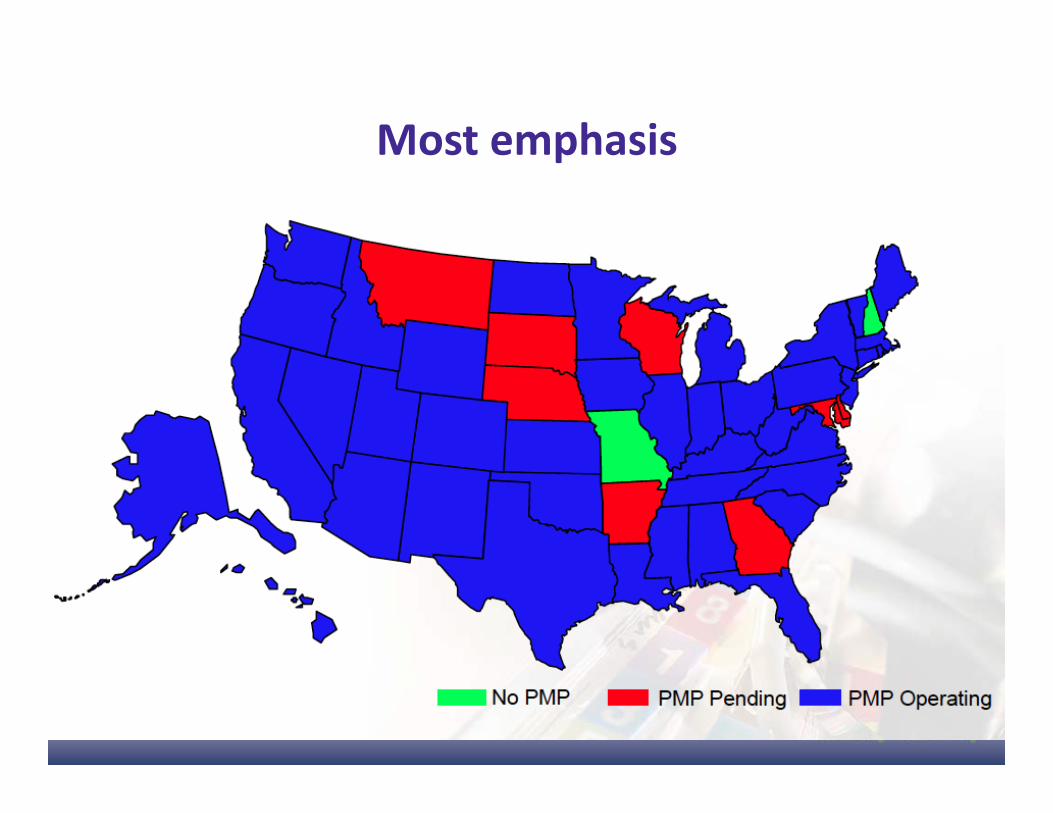
Most emphasis
NaEonal legislaEon
• Educa3on -‐ 7 (CA, FL, ME, NY, UT, WA, WV)
• TeleHealth -‐ 5 (KS, ME, MN, NM, WA) • Monitoring Program -‐ 48 (NH, MS pending) • Outcome tracking -‐ 1 (WA)
Mandatory guidelines:

2009-‐2010: Deaths from opioids decreased by 50%

Registration Reveals Patient on EDIE Patient’s ED chart
flagged for doctor
Physician reviews ED care guidelines
Patient Discharged
medical screening exam by ED physician
No controlled substances
ED case manager talks to patient prior to discharge
State ED informaEon exchange
Usual Triage

State ED informaEon exchange “Please review Jane Doe”
24 hour referral line compiled and researched.
Reviewed for appropriateness Program Coordinator calls PCP
Patient’s Primary Care Physician
PCP Recommendations
ED Care Guidelines Committee Chaplin ED Nurse ED Physicians Psych Nurse Pharmacist Medical Director
ED Care Guidelines
ED Physician

EDIE: Reducing Non-‐Emergent ED UElizaEon

Revise our pracEce model
• System is fragmented
• Care is inconsistent
• Cost is unsustainable
• Coordinated care (PCMH) Patient activation
• Collaborative care (TelePain/ECHO)
• Measurement based care (CPAIN/PainTracker)

EducaEon is important
Rosenblatt, 2011
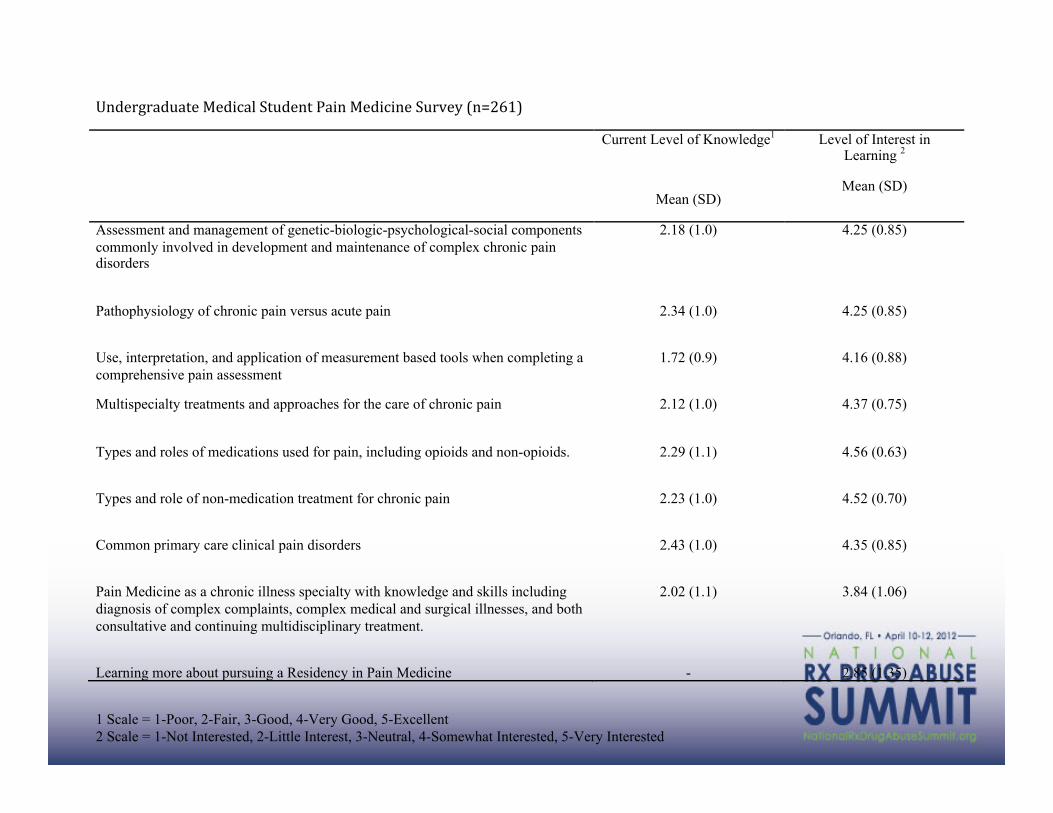
!"#$%&%'#(')$*+$#,-'.*/)(#$")*0',"*+$#,-,"$*/(%1$2*3"45678** Current Level of Knowledge1
Mean (SD)
Level of Interest in Learning 2
Mean (SD)
Assessment and management of genetic-biologic-psychological-social components commonly involved in development and maintenance of complex chronic pain disorders
2.18 (1.0) 4.25 (0.85)
Pathophysiology of chronic pain versus acute pain
2.34 (1.0) 4.25 (0.85)
Use, interpretation, and application of measurement based tools when completing a comprehensive pain assessment
1.72 (0.9) 4.16 (0.88)
Multispecialty treatments and approaches for the care of chronic pain
2.12 (1.0) 4.37 (0.75)
Types and roles of medications used for pain, including opioids and non-opioids.
2.29 (1.1) 4.56 (0.63)
Types and role of non-medication treatment for chronic pain
2.23 (1.0) 4.52 (0.70)
Common primary care clinical pain disorders
2.43 (1.0) 4.35 (0.85)
Pain Medicine as a chronic illness specialty with knowledge and skills including diagnosis of complex complaints, complex medical and surgical illnesses, and both consultative and continuing multidisciplinary treatment.
2.02 (1.1) 3.84 (1.06)
Learning more about pursuing a Residency in Pain Medicine - 2.85 (1.35) *!1 Scale = 1-Poor, 2-Fair, 3-Good, 4-Very Good, 5-Excellent 2 Scale = 1-Not Interested, 2-Little Interest, 3-Neutral, 4-Somewhat Interested, 5-Very Interested

But not enough

Take Home Message:
• Coordinated, collabora3ve, measurement based model:
• 50% decrease in deaths from opioids
• 65% decrease in coun3es par3cipa3ng in TelePain • 56% decrease in opioid prescrip3on rate • 56% decrease in opioid related ER visits • 50% increase in(see attached, for North American
Spine Society 2012 Outstanding Paper Award) global health ra3ng 1 year aker treatment
It ain't what you don't know that gets you into trouble.
It's what you know for sure that just ain't so.
Mark Twain